
Wireless handheld focused ultrasound in student teaching during the COVID-19 pandemic: Initial results of a pilot study1
Abstract
OBJECTIVE:
The study aim was to investigate the use of a novel device, the Vscan Air™, for rapidly and effectively performing ultrasound in student teaching during the COVID-19 pandemic.
MATERIAL AND METHODS:
As part of the ultrasound practical course with integrated hands-on activity required by the regular medical curriculum, 100 medical students were instructed in the use of the Vscan Air™, including duplex mode. They then evaluated the quality of the ultrasound images obtained by the Vscan Air™ from previously selected organs.
RESULTS:
100 students were interviewed (female n = 68, male n = 32; age >18 years n = 100). The rated image quality never fell below a mean of 3 for the examined organs and portal vein flow (liver 4,58; spleen 3,99; kidneys 4,29; aorta 4,16; Douglas/rectovesical space 4,14; portal vein 4,43; pancreas 3,53; Focused Assessment with Sonography for Trauma 4,38). Scores below 3 were found sporadically in ultrasounds of the spleen (n = 4), kidneys (n = 3), Douglas/rectovesical space (n = 2), and pancreas (n = 15). The liver was rated the lowest for 59 ratings. The portal vein was evaluated in 68 cases. The hepatic artery and hepatic veins could be also visualized in all 68 examinations. The aorta was evaluated in 62 cases.
CONCLUSION:
The Vscan Air™ technology offered adequate image quality and provided a new, fast and patient-oriented technique to support continuous ultrasound examinations and education of students, especially during a pandemic. Particularly noteworthy is the uncomplicated compliance with the required high level of hygiene.
1Introduction
Ultrasound diagnostics is a globally widespread and very frequently used examination method in almost all disciplines of medicine [1]. Particular advantages are the lack of ionizing radiation exposure in ultrasound compared with computed tomography and the rapid availability of ultrasound technology since the majority of medical facilities have at least one ultrasound machine available. As several studies have already shown, deficits remain in the handling and education of ultrasound equipment among students and representatives of the various specialist groups in some cases or there is a lack of appropriate training concepts [2–4], which is why internships in ultrasound diagnostics are important and already increasingly being integrated into medical studies [5–7].
Previous ultrasound devices have high image resolutions and high-end sonographic features, such as Contrast Enhanced UltraSound or elastography. However, these high-end devices are uncomfortable because of their size, the limited-movement monitor screen, and the existing cable connection to the corresponding ultrasound probes. These characteristics limit the possible group size of students participating in the class as well as the available classroom space, among other things. The required disinfection time after contact with infectious patients is particularly long, and the necessary personnel effort is high. In the context of the COVID-19 pandemic, this consideration, in addition to the need to maintain adequate medical care for isolated patients, becomes a high priority [8].
The novel Vscan Air™ ultrasound device enables use of a modern convenient method for optimizing student teaching in the application of medical ultrasound. The Vscan Air™ has two fixed integrated probes (linear and convex) and offers the possibility of wireless image transmission to a compatible display. The possibility of using a duplex mode for flow display is also available [1, 9].
The study aim was to evaluate the experience of using the Vscan Air™ device by medical students with no prior ultrasound experience using the VScan Air technique under the hygienically required conditions during the COVID-19 pandemic as part of their regular ultrasound clerkship. The students were asked to assess to what extent the quality of images produced during a Vscan Air™ ultrasound examination of the abdomen were suitable for ultrasound training.
2Material and methods
No ethics vote was required for this study after consultation with the ethics committee of the University of Regensburg. All examinations were performed as part of the regular ultrasound internship or a practical activity (clinical traineeship, practical year [PJ]) as part of medical studies. Study participation was offered on a voluntary basis over a total of 3 months to all students with no relevant previous ultrasound experience and who were working in the ultrasound center of the participating university hospital. The surveys were conducted completely anonymously without the possibility of drawing conclusions about the participants.
Because of the lack of ultrasound examination experience of the students, any influence on the image quality evaluation of the Vscan Air™ (GE Healthcare, USA) could be avoided. The students performed each other’s ultrasonography using the Vscan Air™ so that images of healthy subjects were obtained throughout. Instruction of the students in the use of the Vscan Air™ and subsequent supervision of the performance of the ultrasound examinations was provided by an experienced examiner (>3000 examinations per year, >20 years of ultrasound experience, and available DEGUM level III), who, however, did not influence the evaluation of the image quality but only assisted in an advisory capacity. Each examination also used the duplex mode integrated into the Vscan Air™ System for blood-flow imaging.
2.1Ultrasound device used
2.1.1Vscan Air™
The ultrasound model Vscan Air™ (GE Healthcare, USA) was used. This is a new type of ultrasound technology that uses a transducer with two permanently integrated probes (a convex probe providing 2–5 MHz imaging and a linear probe providing 3–12 MHz imaging) with wireless image transfer to a mobile display device when used with the compatible software (Table 1). The mobile device used for the image display was a mobile iOS (Apple’s mobile operating system) device on which the corresponding function app was installed. Additionally, an integrated duplex mode could be used [1, 9].
Table 1
VScan Air – compatible display devices and compatible operating systems; Two compatible devices with device softwares are displayed in each case
| Device | Operating system |
| Apple iPhones | |
| iPhone 13 Pro Max | iOS 15.4 |
| iPhone X | iOS 13.7 |
| Apple iPads | |
| iPad Pro 5th Gen | iPadOS 15 |
| iPad Air 4th Gen | iPadOS 14.2 |
| Samsung Mobile | |
| Samsung Galaxy S22 Ultra | Android 12 |
| Samsung Galaxy S20 Tactical Edition | Android 10 |
| Samsung Tablets | |
| Samsung Galaxy Tab S8 Ultra 5G | Android 12 |
| Samsung Galaxy Tab Active Pro | Android 10 |
| Google Mobile | |
| Google Pixel 6 | Android 12 |
| Google Pixel 3 | Android 12 |
The maximum battery capacity was 50 min, which guaranteed sufficient time for the respective investigations by the students. To avoid delays (e.g., loading times) in the course of the examinations, two Vscan Air™ models were used alternately, so that one of the two models could always be charging while the other was in use.
2.1.2Examination procedure
The examinations took place in an examination room provided for this purpose by the participating ultrasound center. All hygiene rules in place at the time of the study, including those concerning COVID-19, were followed.
The basic prerequisite for an adequate evaluation of the images by the students was the training of the students in the use of the Vscan Air™ prior to starting the examinations. The correct use of the device during the ultrasound examination was guaranteed by an appropriate supervisor.
The procedure of the investigation was systematically given and adequately performed by all students. For this purpose, the abdomen to be examined was divided into four quadrants, and defined organs were sonicated in each case (Table 2).
Table 2
Presentation of the division of the abdomen to be examined with description of the organs examined in each case
| Left upper quadrant |
| - Spleen |
| - Koller-Pouch |
| - Left kidney |
| - Recessus costodiaphragmaticus |
| Right upper quadrant |
| - Liver |
| - Morison-Pouch |
| - Recessus costodiaphragmaticus |
| - Right kidney |
| Middle upper quadrant |
| - Pancreas |
| - Large abdominal vessels |
| Lower quadrant |
| - Free fluid in the lower abdomen |
All examinations were performed in the classic B-scan mode. Duplex mode could be added if needed. The images were stored in our Picture Archiving and Communication System (PACS).
Proper disinfection of the Vscan Air™ probe in compliance with the DEGUM hygiene recommendations was performed after each examination [10].
2.1.3Image quality rating scale
To assess the quality of the produced ultrasound images of the individual scanned organs, a scoring system from 0 to 5 points was assigned: 0 = no rating possible (e.g., in case of technical errors or too many artifacts), 1 = Focused Assessment with Sonography for Trauma (FAST) clearly limited, organ assessment not adequately possible, 2 = FAST possible, but organ assessment clearly limited, 3 = FAST possible with good quality, but organ assessment in B-mode slightly limited, 4 = good ultrasound assessment for FAST, low artifacts in B-mode and color-mode, 5 = excellent image quality (clear artifact-free representation of the organ and FAST), and X = no evaluation was performed.
3Results
A total of 100 students (68 females, 32 males; age >18 years; n = 100) (Table 3) participated in the study as part of their regular ultrasound clerkship.
Table 3
Epidemiological data of the participating subjects
| Epidemiological parameter | Result |
| Survey period | 3 months |
| Total number | n = 100 |
| Male | n = 32 |
| Female | n = 68 |
| Students in the clinical study section | n = 100 |
| Students active in PJ | n = 8 |
| Students active in clinical traineeship | n = 12 |
| Age >18 years | n = 100 |
A total of seven structures (liver, spleen, kidneys, aorta, Douglas space/rectovesical space, portal vein, pancreas) and the technique of FAST ultrasound were examined (Table 2). Standardized documentation of the Morison and Koller pouch, paravesical region, diaphragm with basal lung and pleura, epicardial recess with four-chamber section, and para-aortic region was used [11]. The aorta, portal vein, hepatic veins and hepatic artery were additionally examined in duplex mode (Fig. 1). Not every organ was evaluated by every student, however. Table 4 summarizes the number of ratings given to the individual structures examined and the FAST sonography with corresponding mean values and standard deviations. The standard deviations of the individual organs are shown graphically in Fig. 2.
Fig. 1
Examples of acquired ultrasound images using VScan Air by the students.
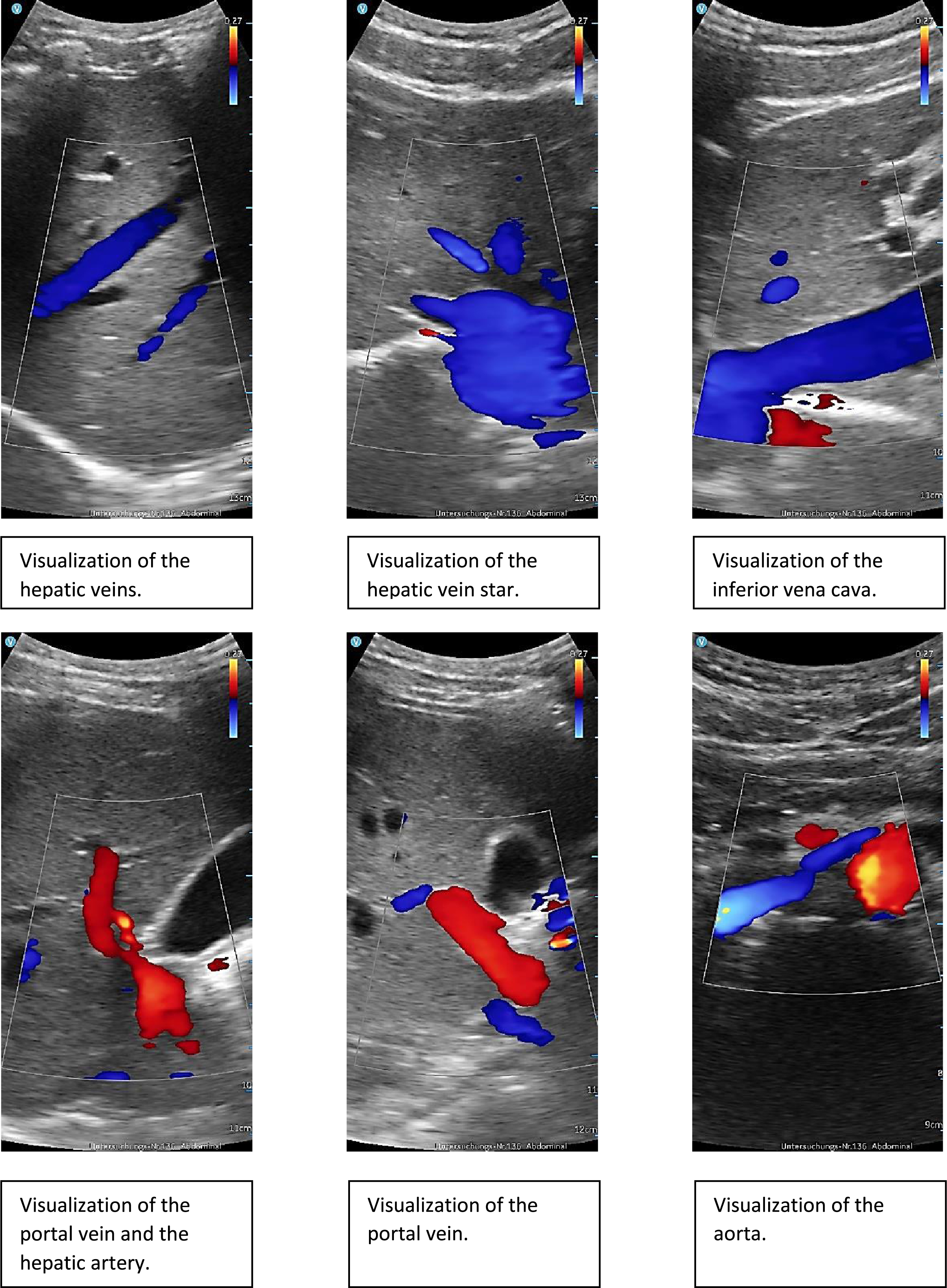
Fig. 2
Presentation of the respective mean values with associated standard deviations of the evaluations of the individual organs examined.
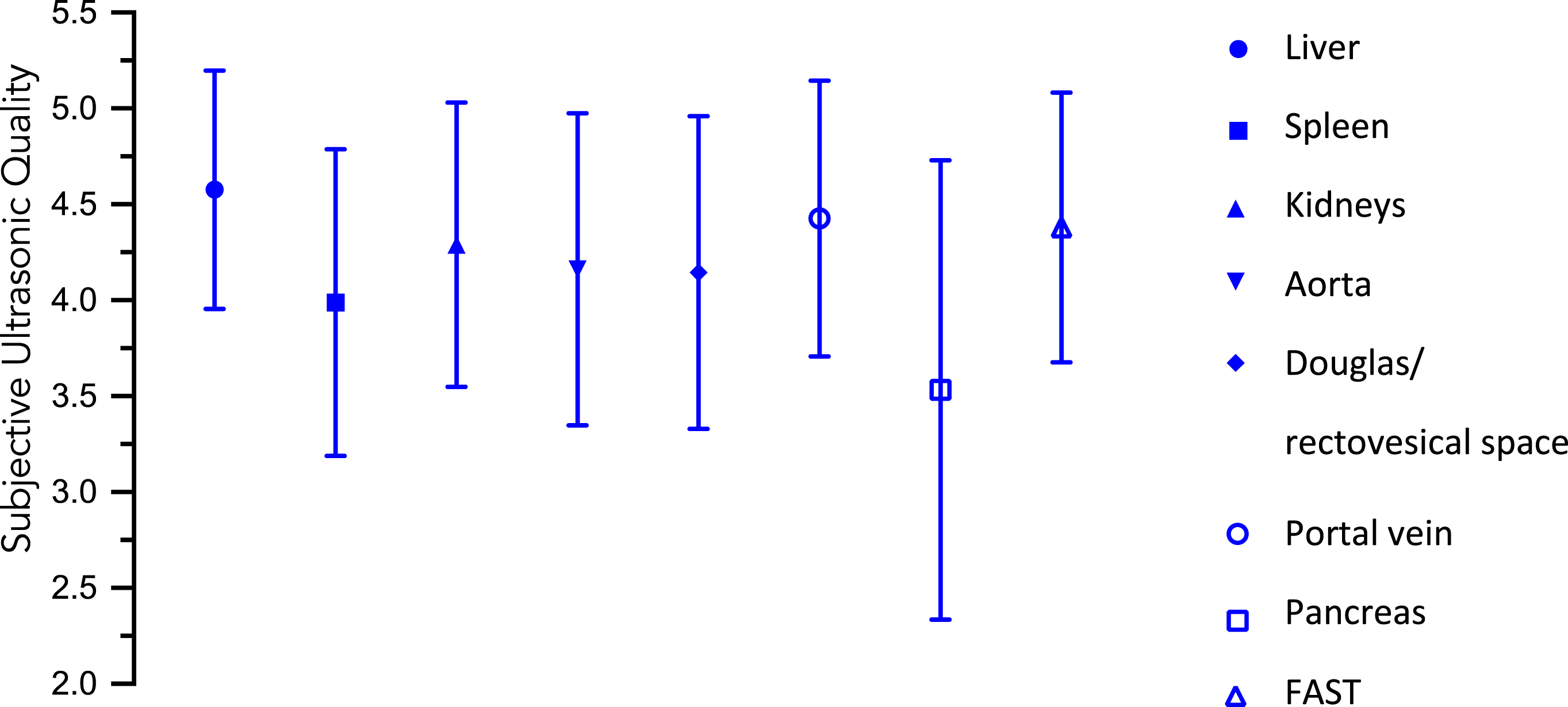
Table 4
Representation of the number of evaluations performed as well as the mean values and corresponding standard deviations of the evaluated image qualities of the individual organs examined
| Liver | Spleen | Kidneys | Aorta | Douglas-Space Rektovesical-Space | Portal vein | Pancreas | FAST | |
| Number of evaluations performed | 59 | 84 | 83 | 62 | 90 | 68 | 62 | 79 |
| Number of evaluations not performed | 41 | 16 | 17 | 38 | 10 | 32 | 38 | 21 |
| Total | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| Mean value image quality | 4,58 | 3,99 | 4,29 | 4,16 | 4,14 | 4,43 | 3,53 | 4,38 |
| Standard deviation | 0,62 | 0,79 | 0,74 | 0,81 | 0,82 | 0,72 | 1,19 | 0,70 |
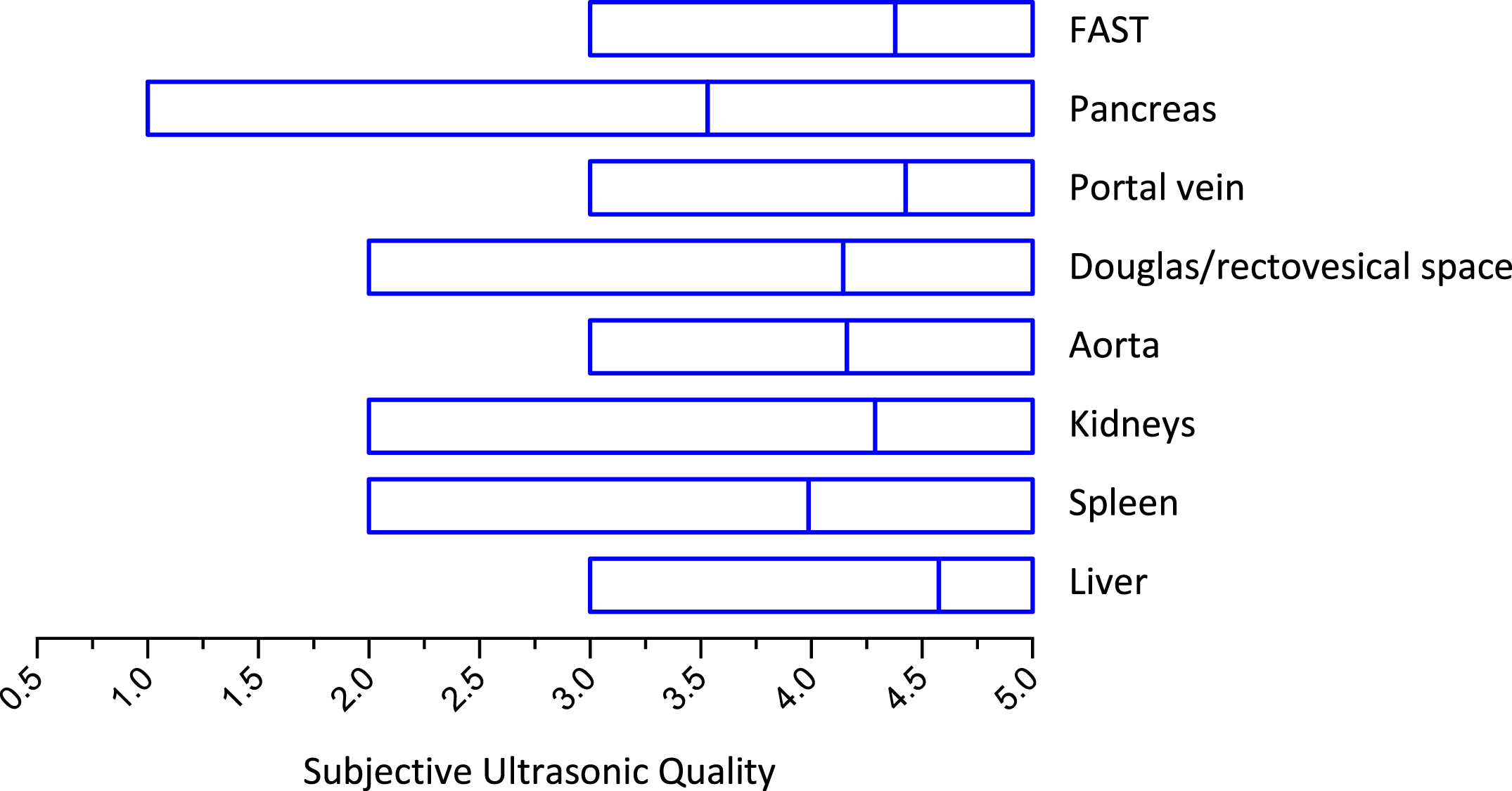
Overall, the rated image quality never fell below a total average score of 3. Individual assessments <3 were found in the spleen (n = 4), kidney (n = 3), Douglas/rectovesical space (n = 2), and pancreas (n = 15) assessments (Fig. 3).
Fig. 3
Presentation of the collected evaluations (minimum value, mean value, maximum value) of the image quality including the respective mean value of the individual organs.
The problems with the performance of ultrasound involved adequate visualization of the intercostal incisions, the location of the spleen and the appropriate incorporation of respiratory/positioning maneuvers.
Adequate adjustment and evaluation of the ultrasound images by the students was guaranteed by the initial instruction of the students in the use of the Vscan Air™ and their ability to ask questions of an experienced ultrasound examiner who was always present.
4Discussion
Given the diagnostic importance and worldwide distribution of ultrasound technology, good knowledge in the application of this technique is mandatory. However, this knowledge is often acquired during residency and there are no uniform standards for ultrasound training yet [12]. Therefore, required integration of ultrasound training into medical studies is increasingly demanded [5, 6].
Many ultrasound models, especially the so-called high-end devices, often pose a challenge to students inexperienced in ultrasound technology during the usually time-limited ultrasound internship because of the complexity of their operation and limit the time available for actual hands-on sonographic activities. Additionally, the group size of the students and choice of the appropriate examination room are limited by the relatively large high-end models.
By means of the Vscan Air™, because of the small size of the device, high ease of use and wireless image transmission to a monitor that is not positionally fixed [1, 13], the above-mentioned problems can be reduced. The Vscan Air™ device has already been described in other studies as a fundamentally effective model [1, 9, 14], but the device also can be used to perform more difficult examinations, such as duplex examination of the veins to exclude thrombosis [9]. However, for adequate training of medical students, sufficient quality of the generated images of the examined structures is also required.
In this study, the evaluation of the surveyed students showed overall consistently adequate image quality (Table 4, Fig. 3) of the representation of the investigated structures. Since healthy subjects were used throughout, a more difficult assessment of the images, e.g., due to pathological findings, could be avoided. This is in line with existing results regarding sufficient image quality of the VScan Air™ [1].
Scores below 3 were awarded in isolated cases, particularly for the spleen and pancreas. Since the participating students had no previous experience in ultrasonography, the lower scores can be explained by the usually difficult localization/demarcation of the spleen and pancreas in the beginning. The ability to visualize portal vein flow in duplex mode suggests that the Vscan Air™ has the basic potential to adequately visualize and evaluate blood flow in vessels. Further development of this technology, such as by integrating CEUS, Elastography, a pulse-wave mode or power-Doppler, could further increase the application potential [1]. In comparison with the high-end devices, the VScan Air is therefore currently still inferior in these points [15–17].
The COVID-19 pandemic, in particular, continues to place high hygienic demands on the conduct of patient treatment and medical school clerkships [18]. The Vscan Air™ offers a clear advantage for this purpose because of its size and nature, as it can be disinfected much more easily and more effectively than other high-end devices, which are rather unwieldy. In addition, unlike large high-end devices, the space-saving Vscan Air™ allows students to be taught in small groups.
Interestingly, we found that the liver was rated the lowest by the students surveyed (Table 4) even though it is one of the organs that is easier to find and delineate on ultrasound. Possibly, this can be attributed to the aforementioned uncertainty of the students to present an optimal sectional image in the intercostal section. This also underscores the need for more intensive integration of ultrasound training into medical studies.
In summary, the Vscan Air™ potentially could be used for better student ultrasound education. Especially, the time factor, fast hygienic preparation, wireless connection and satisfactory image quality show the benefits of training of students on mobile ultrasound systems.
Especially in times of global pandemics and crises, that require mobile ultrasound, this is an important device for obtaining optimized imaging, which will benefit the greater number of patients needing care. A logistical problem that remains to be solved is the need to completely comply with the currently applicable data protection law when transferring images to the PACS. Already in student education, awareness has special importance precisely because of the supposed ease of use with any display device. However, data protection is only ensured with clinical material that is prepared for this in terms of software and organization. Personal devices such as cell phones or tablets are a taboo in patient care, but a must in education in many places. In this context, the establishment of a potential image database for teaching purposes should also be aimed at and attention should be paid to the availability of a secure and stable W-LAN connection.
Since this was a pilot study with a small cohort, this issue should be investigated and evaluated in more detail in further studies. In particular, the aspect of how far a possible training including therapy planning for vascular interventions by means of VScan Air™ could be an important topic area here, which requires further investigations, since valid data already exist in this context for ultrasound high-end techniques [19, 20].
5Limitations
Because the present study is a pilot study with a small cohort, the results collected have limited validity and should be examined in further studies with larger cohorts. The maximum battery capacity of 50 min is still a limiting factor for the use of the VScan Air™ in the daily routine. An increase in battery capacity could remedy the situation. The lack of Doppler function limits the ability to assess hemodynamics. The implementation of a Doppler function would lead to an increase in the potential of the VScan Air™. In the era of COVID-19, the possibility of mobile lung ultrasound is an important consideration. Despite existing indications of a basic feasibility of these investigations using VScan [14], however, the additional use of high-end technology, such as CEUS, would be absolutely necessary for optimal performance [21, 22].
Conflicts of interest
The authors have no potential conflicts of interest to declare.
References
[1] | Jung EM , Dinkel J , Verloh N , Brandenstein M , Stroszczynski C , Jung F , et al. Wireless point-of-care ultrasound: First experiences with a new generation handheld device. Clin Hemorheol Microcirc. (2021) ;79: (3):463–74. DOI: 10.3233/ch-211197 |
[2] | Michels G , Zinke H , Möckel M , Hempel D , Busche C , Janssens U , et al. Empfehlungen zur Ultraschallausbildung in der internistischen Intensiv- und Notfallmedizin: Positionspapier der DGIIN, DEGUM und DGK. Medizinische Klinik - Intensivmedizin und Notfallmedizin. (2017) ;112: (4):314–9. DOI: 10.1007/s00063-017-0285-x. |
[3] | Sohaey R , Di Salvo DN , Bluth EI , Lockhart ME , Cohen HL , Pellerito JS , et al. Medical student ultrasound education: The radiology chair weighs in. Ultrasound Q. (2021) ;37: (1):3–9. DOI: 10.1097/ruq.0000000000000557 |
[4] | Mullen A , Kim B , Puglisi J , Mason NL . An economical strategy for early medical education in ultrasound. BMC Med Educ. (2018) ;18: (1):169. DOI: 10.1186/s12909-018-1275-2 |
[5] | Blechschmidt V , Recker F . Die Zukunft der Ultraschallausbildung im Fokus des NKLM 2020. Jahrestagung der Gesellschaft für Medizinische Ausbildung (GMA); 18.11.2020; Zürich Schweiz. Düsseldorf: German Medical Science GMS Publishing House. (2020) . DOI: 10.3205/20gma080 |
[6] | Dietrich CF , Hoffmann B , Abramowicz J , Badea R , Braden B , Cantisani V , et al. Medical student ultrasound education: A WFUMB position paper, part I. Ultrasound in Medicine and Biology. (2019) ;45: (2):271–81. DOI: 10.1016/j.ultrasmedbio.2018.09.017 |
[7] | Barth G , Recker F , Lo H , Haverkamp N , Kravchenko D , Raupach T , et al. Students’ Perspectives on curricular ultrasound education at german medical schools. Ultrasound in Medicine and Biology. (2022) ;48: :S75. doi:10.1016/j.ultrasmedbio.2022.04.207 |
[8] | ACEP guideline on COVID-19: Ultrasound machine and transducer cleaning. Ann Emerg Med. (2020) ;76: (4):e95–e7. |
[9] | Kaiser U , Herr W , Greiner B , Stroszczynski C , Jung EM . Mobile handheld ultrasound with VScan Air for the diagnosis of deep vein thrombosis. Clin Hemorheol Microcirc. (2022) . DOI: 10.3233/ch-221598 |
[10] | Müller T , Martiny H , Merz E , Döffert J , Wüstner M , Lessel W , et al. DEGUM recommendations on infection prevention in ultrasound and endoscopic ultrasound. Ultraschall in Med. (2018) ;39: :284–304. DOI:https://doi.org/10.1055/s-0044-10200 |
[11] | Scalea TM , Rodriguez A , Chiu WC , Brenneman FD , Fallon WF Jr , KatoK, et al. Focused Assessment with Sonography for Trauma (FAST): Results from an international consensus conference. J Trauma. (1999) ;46: (3):466–72. DOI: 10.1097/00005373-199903000-00022 |
[12] | DEGUM. Wer führt Ultraschall-Untersuchungen durch? Deutsche Gesellschaft für Ultraschall in der Medizin; 2022 [cited 2022 08.11.2022]. Available from: https://www.degum.de/service/patienten/wer-macht-ultraschall-untersuchungen.html |
[13] | Le MT , Voigt L , Nathanson R , Maw AM , Johnson G , Dancel R , et al. Comparison of four handheld point-of-care ultrasound devices by expert users. Ultrasound J. (2022) ;14: (1):27. DOI: 10.1186/s13089-022-00274-6 |
[14] | Güney T , Gürsel G , Özdemir U , Tekin Ö , Çimen M , Mamadova A , et al. Are pocket sized ultrasound devices sufficient in the evaluation of lung ultrasound patterns and aeration scoring in pulmonary ICU patients? J Clin Monit Comput. (2021) ;35: (6):1491–9. DOI: 10.1007/s10877-020-00617-5 |
[15] | Wiesinger I , Jung F , Jung EM . Contrast-enhanced ultrasound (CEUS) and perfusion imaging using VueBox®. Clin Hemorheol Microcirc. (2021) ;78: (1):29–40. DOI: 10.3233/ch-201040 |
[16] | Zhang HJ , Zheng BW , Gu SJ , Wu T , Wu LL , Lian YF , et al. Doppler ultrasonography and contrast-enhanced ultrasonography to evaluate liver allograft discard: A pilot prospective study. Clin Hemorheol Microcirc. (2021) ;77: (1):107–14. DOI: 10.3233/ch-200950 |
[17] | Shao S , Yao M , Li X , Li C , Chen J , Li G , et al. Conventional and contrast-enhanced ultrasound features in sclerosing adenosis and correlation with pathology. Clin Hemorheol Microcirc. (2021) ;77: (2):173–81. DOI: 10.3233/ch-200943 |
[18] | RKI. Empfehlungen des RKI zu Hygienemaβnahmen im Rahmen der Behandlung und Pflege von Patienten mit einer Infektion durch SARS-CoV-2: Robert Koch Institut; 2022 [cited 2022 08.11.2022]. Available from: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Hygiene.html |
[19] | Teusch VI , Piehler AP , Uller W , Müller-Wille R , Prantl L , Stroszczynski C , et al. Value of different ultrasound elastography techniques in patients with venous malformations prior to and after sclerotherapy. Clin Hemorheol Microcirc. (2017) ;66: (4):347–55. DOI: 10.3233/ch-179106 |
[20] | Wiesinger I , Schreml S , Wohlgemuth WA , Stroszczynski C , Jung EM . Perfusion quantification of vascular malformations using contrast-enhanced ultrasound (CEUS) with time intensity curve analysis before and after treatment: First results. Clin Hemorheol Microcirc. (2015) ;62: (4):283–90. DOI: 10.3233/ch-151962 |
[21] | Li Q , Nie F , Yang D , Dong T , Liu T . Contrast-enhanced ultrasound (CEUS) - A new tool for evaluating blood supply in primary peripheral lung cancer. Clin Hemorheol Microcirc. (2022) . DOI: 10.3233/ch-221484 |
[22] | Jung EM , Stroszczynski C , Jung F . Contrast enhanced ultrasound (CEUS) to assess pleural pulmonal changes in severe COVID-19 infection: First results. Clin Hemorheol Microcirc. (2020) ;75: (1):19–26. DOI: 10.3233/ch-209005 |


