
Coagulation and hemorheology profile of patient with stroke and COVID-19: A case series during second wave pandemic
Abstract
In 2021 the delta variant was discovered, heralding the start of the second pandemic wave. This case series aims to analyse and compare the coagulation and hemorheology profiles of COVID-19 patients diagnosed with acute stroke during the pandemic’s second wave and ascertain the effect on patient outcomes. This case series reports 4 cases with their respective characteristics. Case 1 reports on COVID-19 patients without comorbidities, Case 2 with comorbidities, Case 3 with strokes in young patients, and Case 4 with strokes in elderly patients. All cases had abnormal coagulation and hemorheology factors with mixed outcomes. Coagulation and hemorheology factors tend to be higher in COVID-19 patients with acute stroke. The value of coagulation and hemorheology factors can be a prognostic outcome in COVID-19 patients with severe disease, especially in patients associated with acute stroke.
1Introduction
In 2020, the World Health Organization declared the COVID-19 pandemic. It was caused by infection with the severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2) coronavirus, with a high global mortality rate of 4.9 million [1]. In 2021, a new strain, the B.1.617.2 variation, often referred to as the delta variant, was discovered, heralding the start of the second pandemic wave [2]. Numerous studies suggest that this strain is associated with increased symptoms, complications, and mortality and is more readily transferred [2].
By systemic stimulation of the coagulation cascade, systemic inflammation has been reported to generate coagulation anomalies in persons with COVID-19. As a consequence, coagulopathy, strokes, and multisystem failure may occur [3]. A spike in the patient’s coagulopathy and hemorheology factors, such as fibrinogen, D-dimer, and blood viscosity, indicates this condition [3].
Numerous studies have proven an association between elevated coagulation factors and poor prognosis in COVID-19 patients [3]. Blood viscosity is also suspected of having an association with this event. However, the significance of these factors in terms of mortality has not been frequently documented, especially in COVID-19 patients who simultaneously have an acute stroke. This case series aims to analyse and compare the coagulation profiles and blood viscosity of COVID-19 patients diagnosed with acute stroke during the pandemic’s second wave and ascertain the effect on patient outcomes.
2Case illustration
2.1Case 1
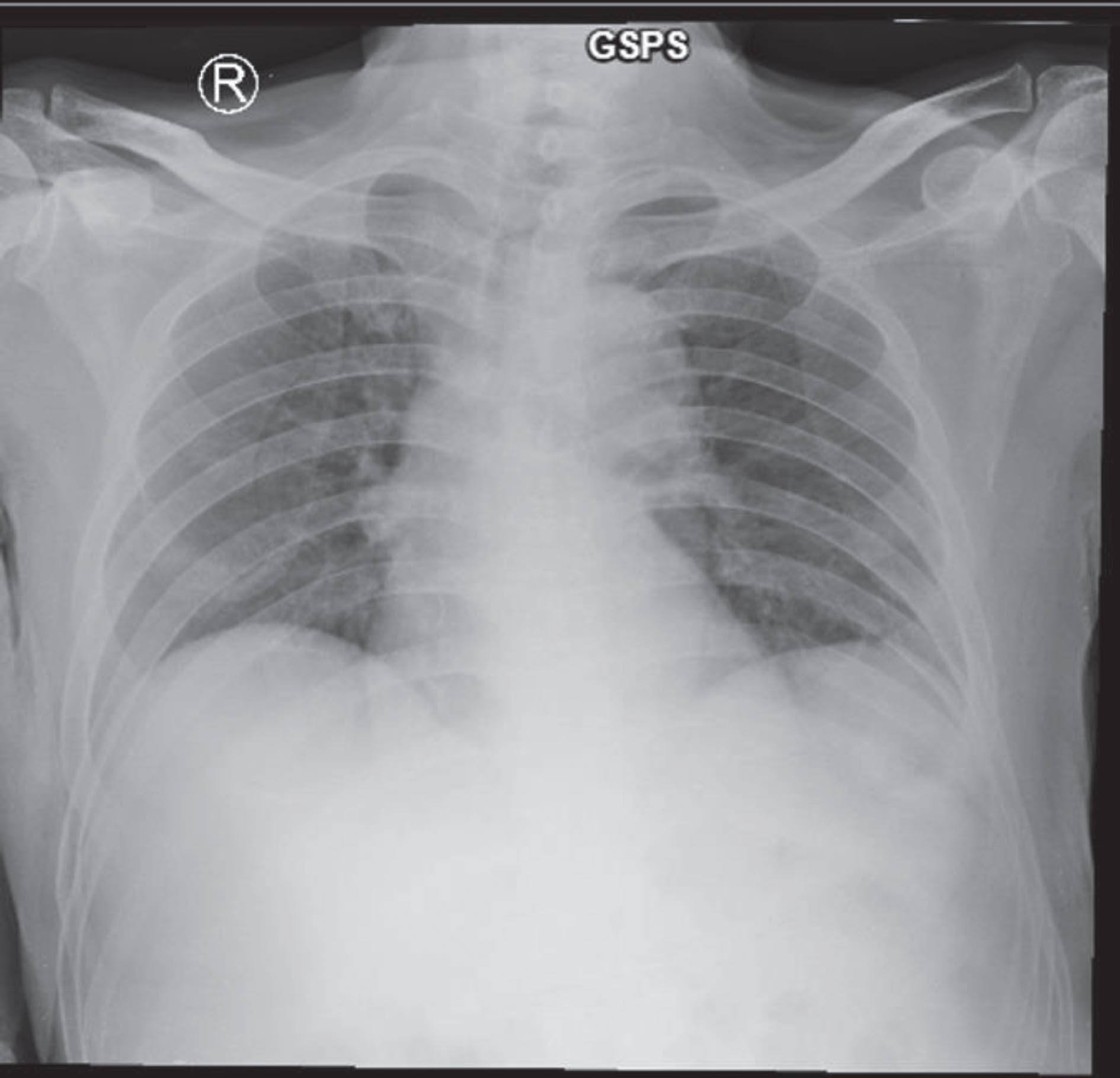
A 67-year-old man arrived with a cough and a high temperature for three days without presenting other symptoms. The patient was hospitalised after being proven positive for COVID-19 by Real Time Polymerase Chain Reaction (RT-PCR) testing. Throughout hospitalisation, the patient remained completely aware with normal vital signs and neurological testing. Chest radiography revealed a lung infiltration in the lower right field, as seen in Fig. 1.
The first laboratory investigations revealed an increase in leukocytes (14,670 cells/microliter), but all other parameters were within normal ranges. Special laboratory tests revealed elevated viscosity (7.19 centipoise), fibrinogen level (486.3 mg/dL), and D-dimer levels (2,280 ng/mL). Other laboratory testing were within normal limits. The patient was hospitalised for seven days and was treated with antiviral treatment. After the patient was ruled negative, he was released since his outpatient viscosity value reduced to 5.07 centipoise, and his modified Rankin scale (mRS) value decreased to 3.
Fig. 1
Chest radiography revealed a lung infiltration in the lower right field for Case 1.
2.2Case 2
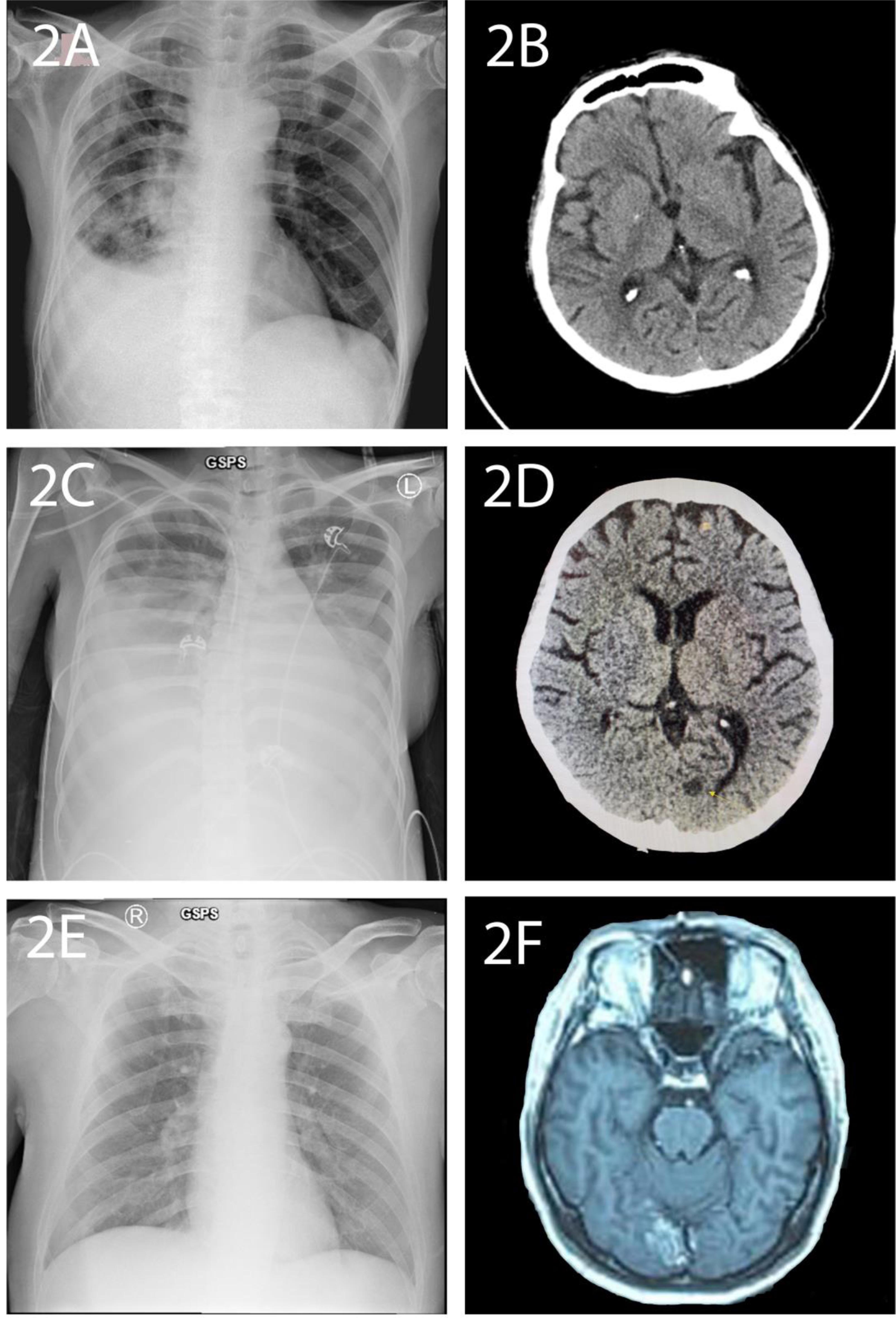
A 68-year-old man was presented with decreased consciousness an hour before admission. The patient was also on chemotherapy for his small cell lung carcinoma. The patient was hospitalised after being proven positive for COVID-19 by RT-PCR testing. Throughout hospitalisation, the patient was delirious with normal vital signs and neurological tests. Chest radiography revealed consolidation in the right perihilar region, infiltration in the upper right lung, and a right pleural effusion (Fig. 2A). Head CT scan revealed no evidence of infarction, haemorrhage, space-occupying lesion, or pathological intracranial mass (Fig. 2B). Basic laboratory tests were within normal limits. A special laboratory test revealed that the sample had a high viscosity (5.58 centipoise), a high D-Dimer concentration (3,960 ng/mL), and a high fibrinogen level (416.6 mg/dL). Other laboratory tests were within normal limits. The patient spent 20 days in a critical care unit before being declared dead.
Fig. 2
Chest radiography and head CT-scan of patients. (A) Chest radiography Case 2, (B) head CT-scan Case 2, (C) Chest radiography Case 3, (D) head CT-scan Case 3, (E) Chest radiography Case 4, (F) head CT-scan Case 4.
2.3Case 3
A 24-year-old woman came 1.5 hours before admission with severe left-sided weakness and stomach discomfort. The central left fascial and hypoglossal nerves were pared during physical examination. Patients have concomitant tuberculous colitis but have no prior history of stroke. Chest radiography revealed bilateral infiltrates in the lower lung fields and bilateral pleural effusions (Fig. 2 C). The code stroke was activated, and a head CT scan revealed infarction in the right lentiform nucleus and posterior crus internal capsule and persistent subcortical infarction in the left occipital lobe (Fig. 2D). The patient was diagnosed with acute ischemic stroke. Additionally, the patient was proven positive for COVID-19 by RT-PCR testing. The patient was later hospitalised following mechanical thrombectomy of the right MCA. Basic laboratory tests were within the normal limit. Special laboratory tests revealed an abnormally high viscosity (5.45 centipoise), high D-Dimer concentration (4,990 ng/mL), and APTT value (34.2 seconds). The results of other laboratory tests were within normal limits. For nine days, the patient was treated with dual antiplatelet treatment. After the patient was ruled negative, she was discharged since her outpatient viscosity value had fallen to 3.22 centipoise and his mRS had decreased to 5.
2.4Case 4
A 53-year-old man was presented with sudden left-sided weakness 1 hour before admission without other accompanying symptoms. Physical examination revealed central left fascial nerve paresis, dysphagia, and dysarthria— patient with no comorbidities and no history of a previous stroke. The results of the chest radiographic examination showed bilateral infiltrates in the lower lung fields (Fig. 2E). Code stroke was activated, and a head CT scan showed right occipital lobe cerebral infarction (Fig. 2F). The patient was diagnosed with acute ischemic stroke. In addition, the patient was also confirmed positive for COVID-19 through RT-PCR examination. The patient was managed by mechanical thrombectomy. Then the patient was hospitalised. During hospitalisation, basic laboratory tests were within normal limits. Special laboratory tests showed high viscosity values (20.38 centipoise), high fibrinogen (560.2 mg/dL), high D-Dimer values (610 ng/mL), and high APTT values (38.2 seconds)— other laboratory tests within normal limits. The patient received dual antiplatelet therapy and was treated for nine days. After the patient was declared negative, the patient was discharged as outpatient viscosity value decreased to 6.56 centipoise and mRS 2.
3Discussion
All patients reported in this case series have interesting characteristics. Although all reported abnormal coagulation and hemorheology factors in COVID-19 patients, each had different comorbidities and clinical characteristics. At the same time, these findings indicate the existence of other factors besides coagulation and hemorheology factors, which also affect patient outcomes.
Case 1 showed an increase in coagulation and hemorheology factors in the form of an increase in blood viscosity, fibrinogen levels, and D-dimer levels. This is a COVID-19 case without comorbidities that shows abnormal coagulation and hemorheology factor values. This case was used as a control case to compare the other 3 cases with these characteristics. In this case, changes in coagulation and hemorheology factors can be explained by the COVID-19 mechanism [3, 4]. COVID-19-infected cells are thought to deplete the ACE2 protein, resulting in an extracellular accumulation of angiotensin II [3, 4]. This accumulation will also form clots due to its interaction with platelets and endothelial cells. Proinflammatory mediators such as IL-6, TNF-a, and activation of AT-II have also been shown to cause damage to microvascular endothelial cells. They activate tissue factors, which strengthen the coagulation cascade and may result in the formation of microthrombus in small blood vessels [3, 4].
Compared to Case 1, Case 2 also showed increased coagulation and hemorheology factors, especially blood viscosity, D-dimer, and fibrinogen level. This vast difference in blood viscosity, D-dimer and fibrinogen level is mainly due to the clinical characteristic of the patient. Even though the patient’s age was almost the same, the patient in Case 2 had severe disease. The degree of disease severity has a close relationship with the profile of coagulation and hemorheology factors [5, 6]. Acute stroke in Case 3 and Case 4 patients also includes severe disease, so this acute stroke also affects coagulation and hemorheology factors with the mechanism described. Interestingly, the stroke patients in Case 3 had very high D-dimer values. This can happen because the younger female patients tend to have higher blood viscosity and are influenced by red-cell aggregation, white-cell mass, plasma fibrinogens, and immunoglobulins [7].
In particular, COVID-19 may induce hematologic abnormalities based on observing and evaluating blood viscosity. This considerable change in blood viscosity can be seen in all patients. At the time of admission, the blood viscosity taken in all patients showed very high values, especially in patients with stroke and severe disease. This shows blood viscosity’s role in describing the severity of patients with COVID-19 in the early stages [8]. The high blood viscosity in stroke patients is in line with the findings in previous studies. An increase in blood viscosity between 1.98 and 4.86 times greater than the control was observed in one investigation [9]. This may result from an underlying process where, in an ischemic stroke, blood flow reduction results in rouleaux production. Fibrinogen’s association with the erythrocyte membrane facilitates its production. The formation of rouleaux will increase the proportion of erythrocytes to plasma, increasing hematocrit. Increases of plasma viscosity or erythrocyte aggregation will lead to an decrease of the perfusion in capillaries [10]. Reduced blood flow will result in diminished delivery of nutrients and oxygen. Eventually, the erythrocytes will grow rigid and lose their deformability [11].
In line with the course of the patient’s illness and the treatment given, it turned out that the patient had improved. This is illustrated by changes in blood viscosity which decrease to normal limits in all patients. Interestingly, the decrease in blood viscosity in stroke patients is greater than in COVID-19 patients who have not had a stroke. This is presumably because the stroke has a major role in increasing blood viscosity. With good management of stroke, patient improvement will lead to more significant changes in blood viscosity [12]. Because the physician has a strong understanding of the impact of coagulation and hemorheology factors on the prognosis of COVID-19 patients with stroke, it seems that coagulation and hemorheology factors have been evaluated in order to provide early therapy. This change in blood viscosity can also be related to patient outcomes where a longer length of stay is obtained in patients with higher blood viscosity. However, the mRS data showed the opposite result. These findings indicate that other factors can affect mRS in patients, namely comorbidities, patient age, and length of stay. This also shows that blood viscosity cannot stand alone to determine patient outcomes but can be a very potential prognostic factor in stroke patients with COVID-19.
4Conclusion
Coagulation and hemorheology profiles tend to be higher in COVID-19 patients with acute stroke. The value of coagulation and hemorheology factors can be a prognostic outcome in COVID-19 patients with severe disease, especially in patients associated with acute stroke.
Acknowledgments
None.
Conflict of interest
The authors declare that there are no conflicts of interest to report.
References
[1] | Zhu N , Zhang D , Wang W , Li X , Yang B , Song J , et al., A Novel Coronavirus from Patients with Pneumonia in China, N Engl J Med (2020) ;382: (8):727–33. |
[2] | Tareq AM , Emran TB , Dhama K , Dhawan M , Tallei TE , Impact of SARS-CoV-2 delta variant (B, 1.617.2) in surging second wave of COVID-19 and efficacy of vaccines in tackling the ongoing pandemic. Hum Vaccin Immunother (2021) ;17: (11):4126–7. |
[3] | Martín-Rojas RM , Pérez-Rus G , Delgado-Pinos VE , Domingo-González A , Regalado-Artamendi I , Alba-Urdiales N , et al., COVID-19 coagulopathy: An in-depth analysis of the coagulationsystem, Eur J Haematol (2020) ;105: (6):741–50. |
[4] | Eslamifar Z , Behzadifard M , Soleimani M , Behzadifard S , Coagulation abnormalities in SARS-CoV-2 infection: overexpression tissue factor, Thromb J (2020) ;18: (1):38. |
[5] | Araya S , Mamo MA , Tsegay YG , Atlaw A , Aytenew A , Hordofa A , et al., Blood coagulation parameter abnormalities in hospitalized patients with confirmed COVID-19 in Ethiopia, PLoS One (2021) ;16: (6):e0252939. |
[6] | Alzoughool F , Alanagreh L , Abumweis S , Atoum M , Cerebrovascular comorbidity, high blood levels of C-reactive protein and D-dimer are associated with disease outcomes in COVID-19 patients, Clin Hemorheol Microcirc (2021) ;77: (3):311–22. |
[7] | Simmonds MJ , Milne N , Ong K , Brotherton E , McNamee AP , Horobin J , et al., Physical Properties of Blood Are Altered in Young and Lean Women with Polycystic Ovary Syndrome, PLoS One (2016) ;11: (11):e0167290. |
[8] | Xing Y , Yang W , Jin Y , Wang C , Guan X , D-dimer daily continuous tendency predicts the short-term prognosis for COVID-19 independently: A retrospective study from Northeast China, Clin Hemorheol Microcirc (2021) ;79: (2):269–77. |
[9] | Joob B , Wiwanitkit V ,. Blood viscosity of COVID-19 patient: a preliminary report, Am J Blood Res (2021) ;11: (1):93–5. |
[10] | Jung F , Mrowietz C , Hiebl B , Franke RP , Pindur G , Sternitzky R , Influence of rheological parameters on the velocity of erythrocytes passing nailfold capillaries in humans, Clin Hemorheol Microcirc (2011) ;48: (1):129–39. |
[11] | Rasyid A , The role of blood viscosity in acute ischemic stroke, Neurona (2014) ;31: (3):192–6. |
[12] | Shaik A , Chen Q , Mar P , Kim H , Mejia P , Pacheco H , et al., Blood hyperviscosity in acute and recent COVID-19 infection. Clin Hemorheol Microcirc. 2022. |


