
The diagnostic value of contrast-enhanced ultrasound for cervical tuberculous lymphadenitis
Abstract
OBJECTIVE:
To investigate the value of contrast-enhanced ultrasound (CEUS) for the diagnosis of cervical tuberculous lymphadenitis (CTL).
METHODS:
The cohort study included 203 consecutive patients diagnosed with cervical lymph node. Before pathological or laboratory confirmation, all patients underwent CEUS examination, and the imaging findings were analyzed afterward. The diagnostic efficiency of the CEUS imaging findings of CTL was evaluated.
RESULTS:
Nighty-seven patients of the 203 (47.8%) were pathologically or laboratory confirmed with a CTL diagnosis while the remainder (52.2%) were diagnosed with non-tuberculous lymphadenitis. Regarding the imaging findings of CEUS, it was more common in CTL patients to find a pattern of heterogeneous enhancement inside the lymph nodes relative to non-tuberculous patients [81.44% (79/97) vs 15.09% (16/106), P < 0.01]. The sensitivity of the feature in diagnosis for CTL was 81.44% and the specificity was 84.91%, resepectively. Furthermore, a pattern of peripheral rim-like enhancement had been notable in CTL patients compared with non-tuberculous patients [86.60% (84/97) vs 12.26% (13/106), P < 0.01], associating with a diagnostic sensitivity of 86.60% and a specificity of 87.74%. When it came to the combination of both imaging findings mentioned above, the features were more prominent in CTL patients than compared with non-tuberculous patients [74.23% (72/97) vs 5.66% (6/106), P < 0.01], with a diagnostic sensitivity of 74.23% and a high specificity of 94.34%. Regarding area under curve (AUC) for the ROC analysis, the feature of internal heterogeneous enhancement, peripheral rim-like enhancement, and both features were 0.832, 0.872, and 0.843.
CONCLUSIONS:
CEUS patterns of heterogeneous enhancement and peripheral rim-like enhancement of lymph nodes are helpful characteristics for the diagnosis of CTL.
1Introduction
Globally, an estimate of 10 million people are infected with tuberculosis (TB) and 1.4 million die annually from the infection according to the World Health Organization (WHO) [1]. TB remains the top cause of death worldwide from a single infectious agent (prior to HIV/AIDS or COVID-19) [2]. Although TB typically affects the lungs (pulmonary TB), it could also affect other sites (extrapulmonary TB) [3]. Tuberculous lymphadenitis is a common manifestation of extrapulmonary TB which accounts for more than 10% of total the world’s TB infections [4]. Furthermore, it is even more common in countries such as China, where tuberculosis is endemic [5]. Cervical tuberculous lymphadenitis (CTL) is often caused by Mycobacterium tuberculosis by infecting the mucous membrane at sites such as the oral or nasal cavities, and subsequently spreading to the lymph nodes along the lymphatic vessels [6]. CTL holds the highest morbidity rate in tuberculous lymphadenitis, with a long infection duration and complicated clinical manifestations, and remains challenging to distinguish from other lymph node diseases [7, 8]. Therefore, there is an urgent need for imaging methods that can assist in making fast and accurate diagnosis.
In clinical practice, the manifestations of CTL varies. It often shows matting, heterogeneous inside the lymph node, and hilum absence in conventional ultrasound (US). Due to the lack of characteristic imaging signs in US for CTL, it is commonly misdiagnosed or diagnosed late, which affects treatment [9]. Although there are some findings in CT, which helps in better anatomical localization of lymph nodes not usually detected on clinical examination, it is not commonly used in clinical practice because of its radiation and little help in biopsy of lymph node [10, 11]. Elastography which reflects the stiffness of organs can provide additional stiffness information of the lymph node, but it is apt to be influenced by calcification and necrosis of the lesion [12].
Contrast-enhanced ultrasonography (CEUS) is an ultrasound diagnostic technique using intravenous injection of microbubble contrast agents and real-time harmonic gray-scale sonography [13–16], which can effectively evaluate blood perfusion in tissue and partial microcirculation for solid organs [17–19]. It is reported that CEUS showed preferable diagnostic value for superficial lymph nodes [20, 21]. YANG et al found that the CEUS enhancement patterns of tuberculous lymphadenitis were mainly heterogeneous inside the lymph node and rim-like periphery [22].
Though the potential for CEUS to distinguish CTL from other lymph node diseases has been noticed according to previous studies, few studies evaluate the diagnostic value for CTL itself. Therefore, the present study retrospectively analyzed the CEUS imaging features of CTL to explore its value and role in diagnosing CTL.
2Materials and methods
2.1Patients
This retrospective study involved patients that presented to our hospital with enlarged cervical lymph nodes between January 2019 and December 2020. The eligibility criteria were listed as follows: 1. Enlargement of cervical lymph nodes; 2. Complete dynamically records of CEUS examination; 3. The patient was clinically confirmed by pathology or laboratory inspection. While the exclusion criteria were listed as follows: 1. The patient with incomplete information; 2. The patient who refused CEUS examination because of personal reasons such as allergic constitution; 3. Undiagnosed patients. Finally, A total of 203 patients were enrolled, aged 18–56 years old (mean 36.2±9.4 yrs). Among them, 106 were females while 97 were males. This study was approved by the ethics committee of our hospital (approval number 2021-298). All the enrolled patients gave informed consent.
2.2CEUS examination
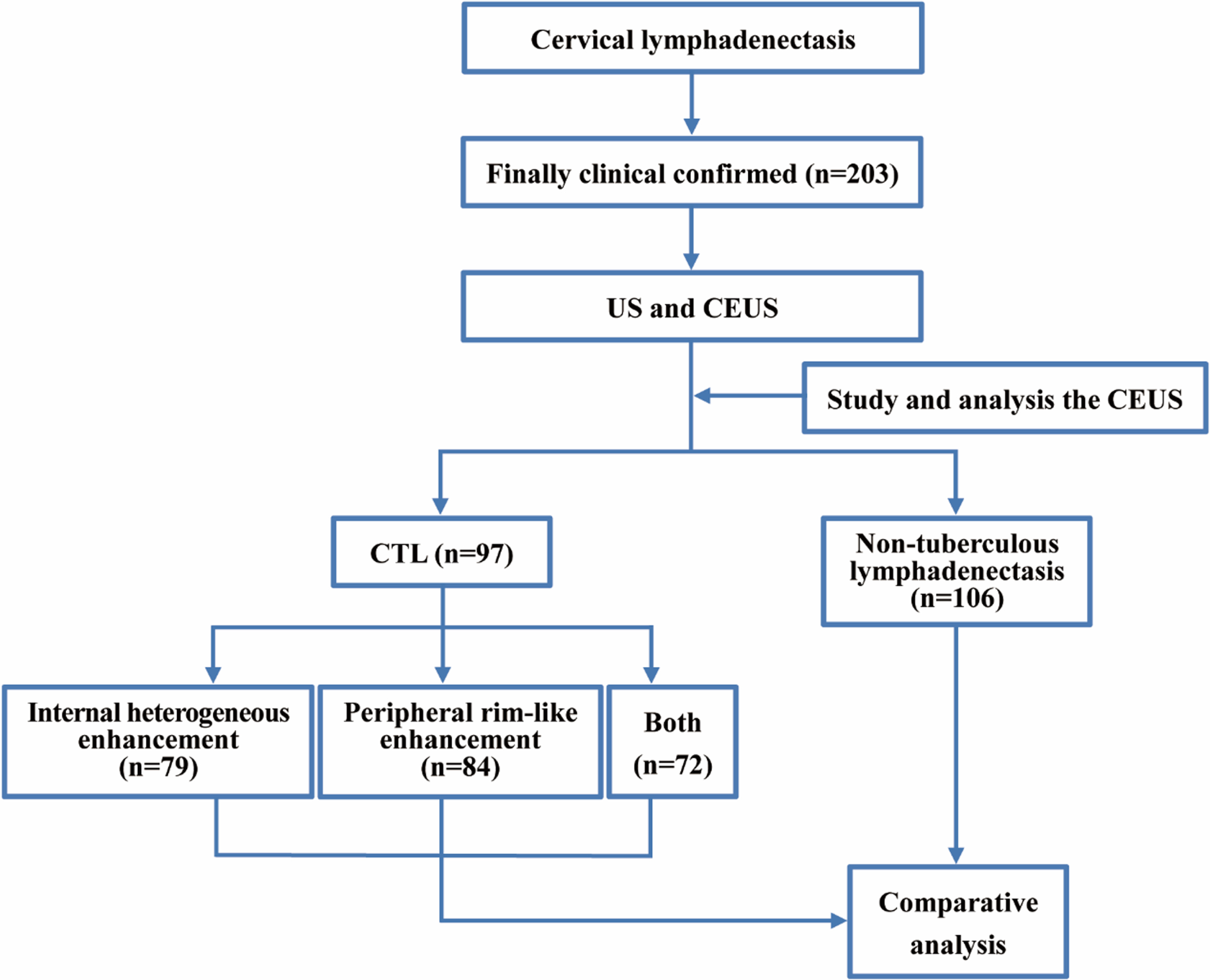
The Philips iU-Elite ultrasound system (Washington, USA) was used for the whole procedure, while a L12-5 linear array transducer (frequency range, 5.0–12.0 MHz) was applied in the US. Each patient took a supine position with the neck fully exposed. All cervical lymph node levels were checked carefully and the larger lymph nodes were selected, of which the most typical lymph node was examined for CEUS after comprehensive assessment with the patient’s prior consent. A L9-3 linear array transducer (frequency range, 3.0–9.0 MHz) was applied in the CEUS, with a real-time contrast imaging software (supported by the Philips Healthcare System), which allows contrast-enhanced imaging with low acoustic power (Mechanical Index, MI is 0.06). A bolus of 2.4 ml of contrast agent (SonoVue, Bracco, Italy), which was diluted with 5 ml of normal saline (NS) and shaken well before use, was injected intravenously via the superficial vein of the elbow, followed by a flush with 10 ml of NS. CEUS was displayed on a split-screen mode by optimizing settings and focus was placed under the level of the lesion to minimize the destruction to microbubbles. The complete CEUS examination was dynamically recorded over 3 minutes and stored in the hard disk of the ultrasonic apparatus. Finally, the perfusion patterns of the lesions in CEUS were analyzed, classified, and documented by the same two senior radiologists. When the analyses from the two radiologists were inconsistent, a third senior radiologist would review the imaging and draw a final conclusion via discussion with the two previous radiologists. The process of the study is shown in Fig. 1.
Fig. 1
The flowchart of case classification and comparision.
2.3Statistical analysis
The statistical analysis was performed with SPSS 19.0 software (IBM Corp, NY, USA). Comparison of enhancement patterns of different lymph node lesions in CEUS was performed by Chi-square test and Fisher’s exact test. The difference was considered statistically significant when P was below 0.05. The receiver operating characteristics (ROC) curve was used to analyze the diagnostic value of CEUS for CTL.
3Result
3.1Confirmed diagnosis
Of the 203 patients who were confirmed with cervical lymph node enlargement by pathology or laboratory examination, 97 patients were tuberculous lymphadenitis (CTL group) while 106 patients were non-tuberculous (non-tuberculous group, included 39 cases of reactive hyperplastic lymphadenopathy, 27 cases of lymphoma, 33 cases of cervical lymph node metastasis of malignant tumors, and 7 cases of histiocytic necrotizing lymphadenitis). The average maximum diameter of the largest typical lymph node was 26.69±4.436 mm, and the basic characteristics of the patients and the conventional ultrasound features of the lesions were present in Table 1.
Table 1
Basic characteristics of the patients and ultrasound features of the lesions
| Characteristics | CTL (n = 97) | Non-tuberculous (n = 106) | P value |
| Patient | |||
| Mean age (yrs) | 35.00±9.281 | 37.24±9.482 | 0.092 |
| Gender (Female/male) | 60/37 | 46/60 | 0.009* |
| History of pulmonary tuberculosis | 31 | 28 | 0.385 |
| PPD test positive | 93 | 52 | 0.000* |
| US | |||
| Maximum diameter (mm) | 26.16±3.710 | 27.17±4.979 | 0.107 |
| Echo | |||
| Hyperechoic | 8 | 7 | 0.655 |
| Isoechoic | 13 | 18 | 0.479 |
| Hypoechoic | 48 | 51 | 0.845 |
| Heterogeneous | 28 | 30 | 0.929 |
| Lymph node hilum | 0.236 | ||
| Presence | 18 | 27 | |
| Absence | 79 | 79 | |
| Internal vascularity | 0.001* | ||
| Presence | 48 | 29 | |
| Absence | 49 | 77 | |
| Internal calcification | 0.004* | ||
| Presence | 29 | 14 | |
| Absence | 68 | 92 | |
| Margin | 0.299 | ||
| Circumscribed | 51 | 48 | |
| Not Circumscribed | 46 | 58 | |
| Matting | 0.006* | ||
| Presence | 59 | 44 | |
| Absence | 38 | 62 | |
| CEUS | |||
| Inside lymph node | |||
| Homogeneous enhancement | 5 | 84 | 0.000* |
| Heterogeneous enhancement | 79 | 16 | 0.000* |
| Non-enhancement | 13 | 6 | 0.059 |
| Peripheral rim-like enhancement | 0.000* | ||
| Presence | 84 | 13 | |
| Absence | 13 | 93 |
PPD: purified protein derivative. CTL: cervical tuberculous lymphadenitis. US: conventional ultrasound. CEUS: contrast-enhanced ultrasonography. * indicates statistically significant difference.
3.2Characteristics of CEUS imaging and ROC analysis
In CEUS imaging, a classification of CTL by YANG, et al. was applied (Fig. 2) [8]. The enhancement patterns of all lymph node lesions in CEUS were shown in Table 2.
Fig. 2
Images present general appearance of CTL for CEUS imaging patterns. (A1, A2) Pattern 1: peripheral rim-like enhancement (⟶) with internal homogeneous enhancement. (B1, B2) Pattern 2: peripheral rim-like enhancement (⟶) and internal heterogeneous enhancement (▵), like “honeycomb”. (C1, C2) Pattern 2: peripheral rim-like enhancement (⟶) and internal heterogeneous enhancement (▵), like “dead wood”. (D1, D2) Pattern 3: peripheral rim-like enhancement (⟶) with non-enhancement inside the lesion.
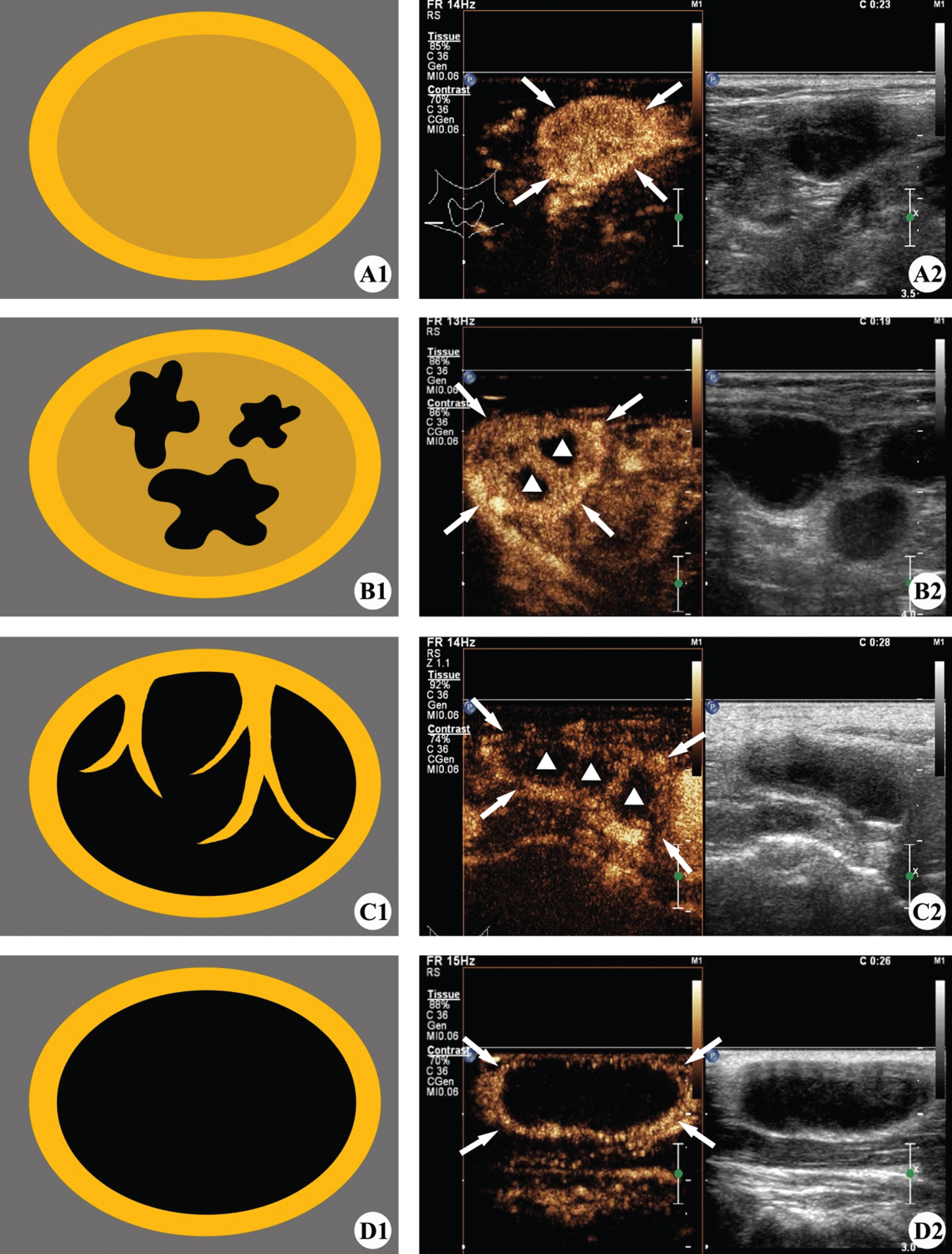
Table 2
Enhancement patterns of cervical tuberculous lymphadenitis and non-tuberculous lesions in CEUS
| Lymph node type | Internal heterogeneous enhancement | Peripheral rim-like enhancement | Internal heterogeneous enhancement + peripheral rim-like enhancement |
| Cervical tuberculous lymphadenitis | 81.44% (79/97)* | 86.60% (84/97)* | 74.22% (72/97)* |
| Non-tuberculous lesions | 15.09% (16/106) | 12.26% (13/106) | 5.66% (6/106) |
| Reactive hyperplastic lymphadenopathy | 10.26% (4/39) | 20.5% (6/39) | 7.69% (3/39) |
| Lymphoma | 11.11% (3/27) | 3.70% (1/27) | 0.00% (0/27) |
| Metastasis of malignant tumors | 24.24% (8/33) | 12.12% (4/33) | 9.09% (3/33) |
| Histiocytic necrotizing lymphadenitis | 14.29% (1/7) | 28.57% (2/7) | 0.00% (0/7) |
*P < 0.05 when it was compared with non-tuberculous lesions.
It was more common to find a pattern of heterogeneous enhancement inside the lymph nodes at arterial phase relative to non-tuberculous patients (P < 0.01), with 81.44% (79/97) in the CTL group compared to 15.09% (16/106) in the non-tuberculous group. ROC analysis showed that using internal heterogeneous enhancement as a feature for diagnosis, the sensitivity, the specificity, the positive predictive value, the negative predictive value, and the area under the curve (AUC) were 81.44 %, 84.91%, 83.16%, 83.33%, and 0.832, respectively.
Furthermore, a pattern of peripheral rim-like enhancement at arterial phase had been notable in CTL patients (86.60%, 84/97) compared with non-tuberculous patients (12.26%, 13/106), associating with the statistically significant difference (P < 0.01). When taking peripheral rim-like enhancement as a feature for CTL diagnosis, the sensitivity, the specificity, the positive predictive value, the negative predictive value, and the AUC were 86.60%, 87.74%, 86.60%, 87.74%, and 0.872, respectively.
When it came to the combination of both imaging findings mentioned above, the features were more prominent in CTL (74.23%, 72/97) compared with non-tuberculous patients (5.66%, 6/106), while the difference was statistically significant (P < 0.01). ROC analysis showed that the combination of the two features can result in diagnostic sensitivity, specificity, positive predictive value, negative predictive value, and AUC of 74.23%, 94.34%, 92.31%, 80.00%, and 0.843, respectively.
All results were presented in Table 3 and Fig. 3. CTL mainly exhibited internal heterogeneous enhancement and peripheral rim-like enhancement (Fig. 4).
Table 3
Diagnostic performance of CEUS for cervical tuberculous lymphadenitis
| Enhancement Pattern | Sensitivity | Specificity | Positive predictive value | Negative predictive value | Youden index | AUC | Z | P |
| Internal heterogeneous enhancement | 81.44% | 84.91% | 83.16% | 83.33% | 0.6635 | 0.832 | 12.550 | 0.000 |
| Peripheral rim-like enhancement | 86.60% | 87.74% | 86.60% | 87.74% | 0.7433 | 0.872 | 15.728 | 0.000 |
| Internal heterogeneous enhancement and peripheral rim-like enhancement | 74.23% | 94.34% | 92.31% | 80.00% | 0.6857 | 0.843 | 13.710 | 0.000 |
Fig. 3
Receiver operating characteristic (ROC) curves for the diagnostic accuracy of CEUS in CTL.
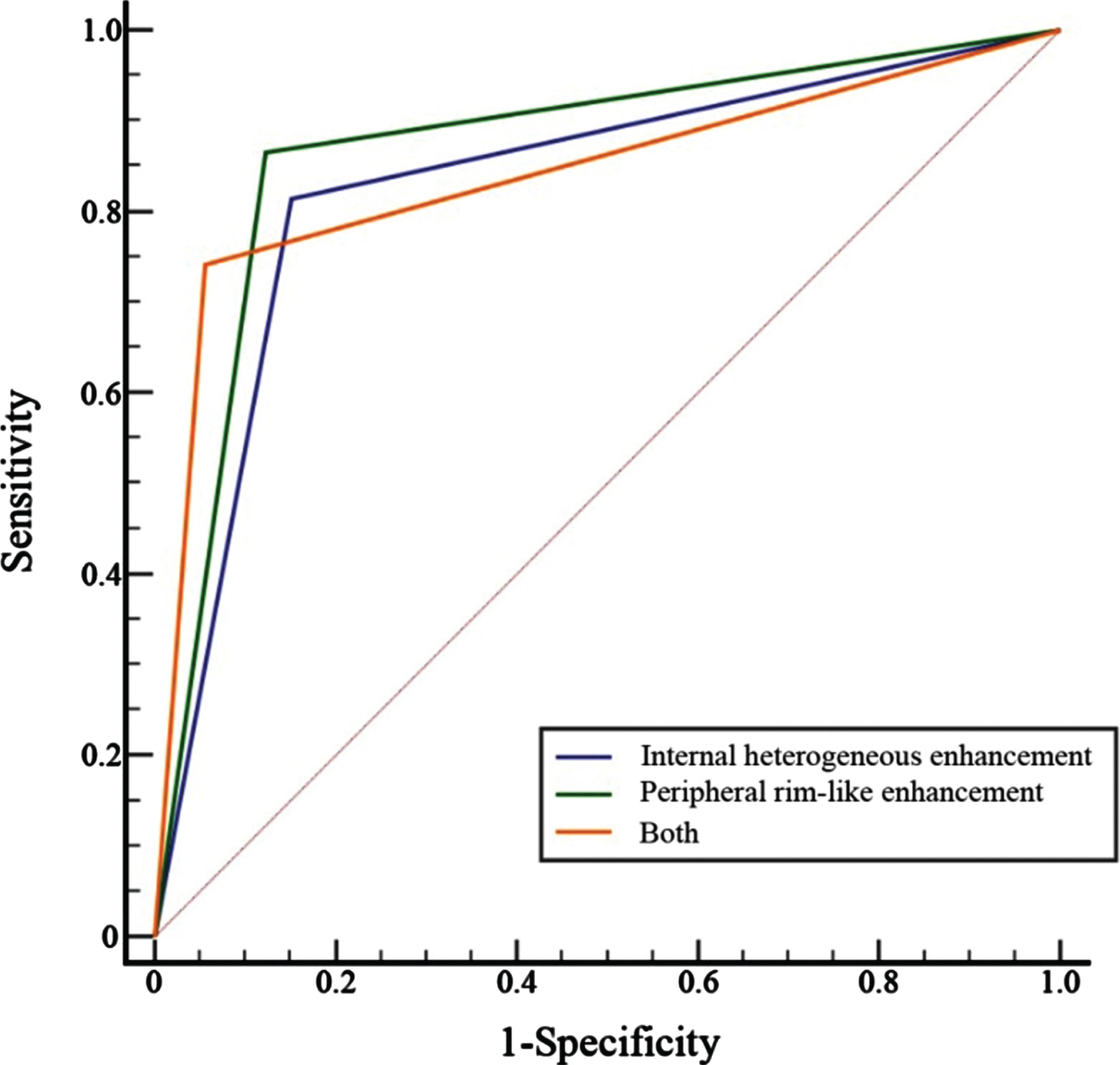
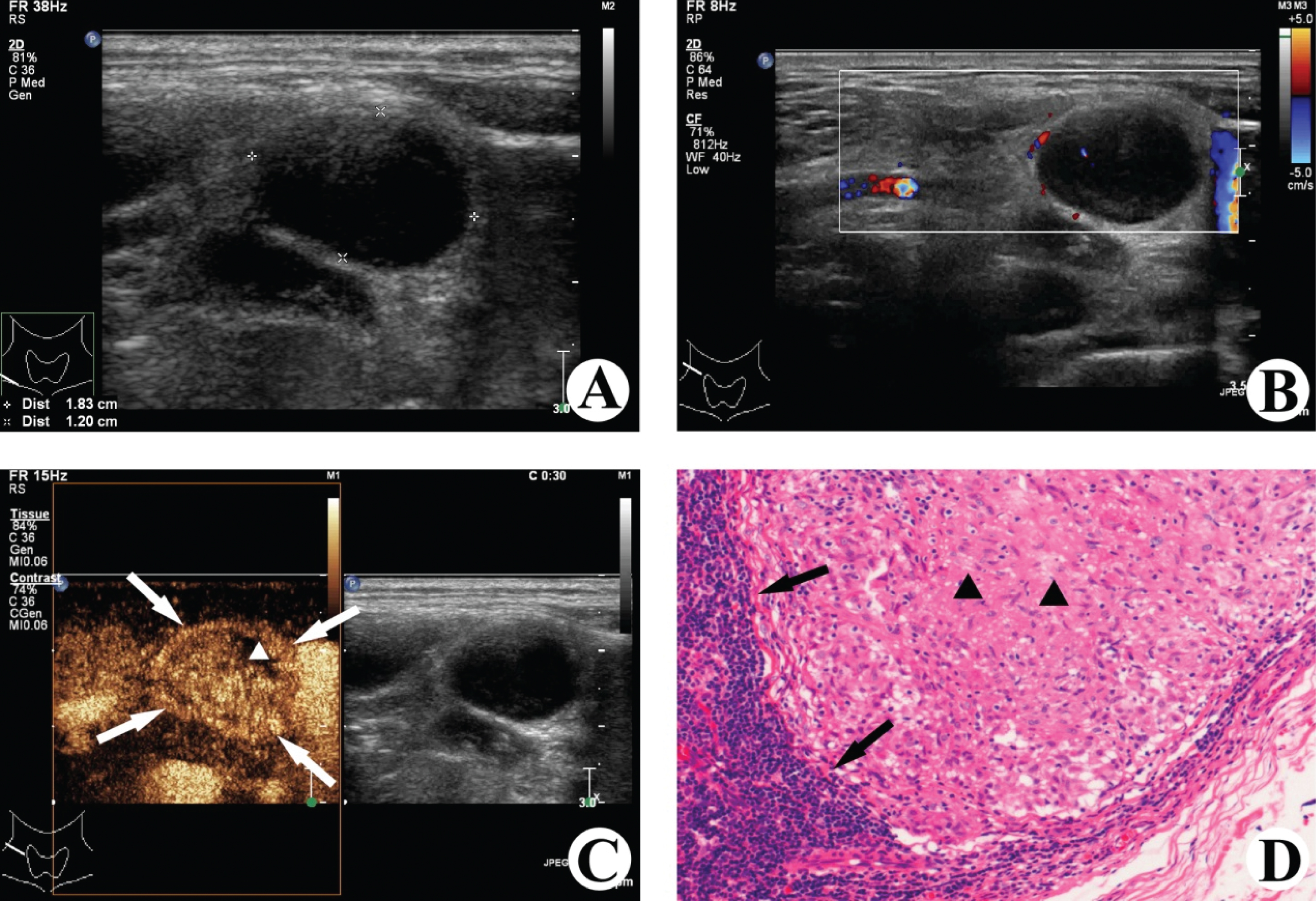
Fig. 4
Images of a 35-years-old woman with tuberculosis in the right cervical lymph node. (A) Gray-scale ultrasound shows the hypoechoic enlarged lymph nodes with clear boundary, and the lymph node hilum is absent. (B) Color Doppler ultrasound detects few color signals of blood flow in and around the lymph node lesion. (C) CEUS image shows internal heterogeneous enhancement (▵ non-enhancing area) and peripheral rim-like enhancement (⟶). (D) The lymph node was surgically removed, and caseous necrosis (▴) and local granulation tissue hyperplasia (⟶) in the lymph node were observed under the microscope (HE×200).
4Discussion
Tuberculous lymphadenitis is the most common form of extrapulmonary tuberculosis, with the neck being the most common site [3]. On account of its complicated clinical manifestations, a rapid and minimally invasive imaging examination method is urgently needed for the screening of CTL. In clinical practice, the accuracy of CEUS was much higher than conventional ultrasound in the diagnosis of cervical lymphoma and lymph node metastasis [9, 23], since CEUS has been widely used to evaluate microperfusion and microcirculation in various tissues and organs [24]. Furthermore, combined with the application of CEUS, the accuracy of lymph node biopsy was greatly improved [25]. A previous study found that CTL was mostly manifested as heterogeneous enhancement inside the lymph node and peripheral rim-like enhancement in CEUS enhanced pattern [22]. Therefore, the cohort study included 203 consecutive patients with the confirmed cervical lymphadenopathy who underwent CEUS, in order to evaluate the role of CEUS in the diagnosis of CTL after analyzing the diagnostic performance of characteristic enhancement pattern of CTL.
In the present study, it showed that the internal heterogeneous enhancement of the lymph nodes, peripheral rim-like enhancement, and the combination of two features were all more common in the CTL group than that in the non-tuberculous group. In particular, the specificity of the diagnosis of CTL with both the features of internal heterogeneous enhancement and peripheral rim-like enhancement combined, was as high as 94.34%. This may be related to the pathological changes of CTL [3, 26]. A comparison of the pathological results of surgically removed CTL and CEUS results verified that the unenhanced region of CEUS images in the lymph nodes indicated caseous necrosis, the internal enhancement area indicated the hyperplasia of lymphocytes and granulation tissue, and the peripheral rim-like enhancement area indicated inflammation at the edge of the lymph node and the hyperplasia of granulation tissue. Various inflammatory chemokines due to inflammatory reactions around lymph nodes caused abnormal hyperplasia of granulation tissue and capillaries around lymph nodes, resulting in a rim-like enhancement in CEUS images [27]. However, in the CEUS images of a few CTL cases, there was no typical enhancement of CTL observed, which may be related to the stage of the disease. Several cases that were still at an early stage of the disease, when the hyperplasia was evident in the lymph nodes, showed only sporadic or inconspicuous necrosis. Therefore, the typical features of internal heterogeneous enhancement in CEUS were not observed under the influence of the partial volume effect of CEUS. It showed homogeneous enhancement inside the lymph nodes. Additionally, the hyperplasia of granulation tissue around lymph nodes was not obvious at this stage, due to the absence of aggregation of inflammatory chemokines. Some cases were at the end stage or the stage of recuperation, when extensive necrosis or dispersed dystrophic calcifications were noted inside the lymph node, leading to the sign of non-enhancement in lymph nodes [28].
On the other hand, some of the non-tuberculous lesions showed internal heterogeneous enhancement and/or peripheral rim-like enhancement, which mimicked CTL. It is acknowledged that the CEUS manifestations of various cervical lymph node diseases may be related to their pathological changes. For example, the reactive hyperplastic lymphadenopathy is dominated by the hyperplasia of lymphoid tissues, necrosis in the lymph nodes is rare, and the boundaries around the lymph nodes are clear. Therefore, reactive hyperplastic lymphadenopathy usually presents with homogeneous enhancement in the lymph nodes [29]. Necrosis is also rarely presented in lymphoma, a group of heterogeneous neoplastic diseases originating from a single mutated lymph node cell, but mostly occurred after chemotherapy [30, 31]. As a result, with very minimal inflammation at the junction of the lymphoma and surrounding tissues, CEUS showed homogeneous hyperenhancement inside the lymph node and no rim-like enhancement around in most cases. In the present study, only one lymphoma case showed peripheral rim-like enhancement, which may be associated with non-specific infection. Lymph node metastasis of malignant tumors presents many similarities with tuberculous lymphadenitis in US findings [32]. For example, cervical lymph nodes metastasis of nasopharyngeal carcinoma are prone to liquefactive necrosis in the lymph nodes, and inflammation surrounding the lesions may occur when complicated with infection [33]. As a result, an enhancement pattern similar to that of CTL was produced. However, the majority of other metastatic lymph nodes did not show typical internal heterogeneous enhancement combined with peripheral rim-like enhancement in CEUS. Furthermore, studies found that the increase in blood vessel volume and density precedes an increase in lymph node size in the early stages of lymph node metastasis [34], which has been hypothesized that detection of these changes by CEUS may allow early diagnosis of lymph node metastasis [35]. It was also reported that metastatic lymph nodes exhibit characteristic enhancement patterns such as centripetal perfusion, and the absence of hilum after enhancement, which were helpful for differential diagnosis [36]. In addition, although it was prone to necrosis in the lymph nodes with the disease of histiocytic necrotizing lymphadenitis, most of which were pinpoint foci, it still showed homogeneous enhancement due to the limited resolution and partial volume effect of CEUS [37, 38].
Several limitations in the current study cannot be ignored. Firstly, the study only compared the features of CEUS imaging in CTL with non-tuberculous cases, while it did not compare among the various diseases in the non-tuberculous group, which may lead to selection bias. Secondly, only CTL and certain common cervical lymph node conditions presented with lymph node enlargement were compared, rare cervical lymph node diseases with lymph node enlargement were not reviewed. Thirdly, some biases such as CTL concomitant with other diseases might be mixed up in the case enrollment in the current retrospective study. Moreover, the present study only briefly evaluated the diagnostic efficacy of CEUS in CTL, and it is believed that multimodal ultrasonography including CEUS will be more valuable for the diagnosis of CTL. These issues require further study.
5Conclusions
In conclusion, CEUS is useful in directly and objectively detecting the hyperplasia and necrosis in and around cervical lymph nodes. Internal heterogeneous enhancement and peripheral rim-like enhancement are the characteristic features of CEUS for CTL diagnosis along with preferable diagnostic performance.
Conflicts of interest
All the authors certify that there is no actual or potential conflict of interests in this article.
Acknowledgments
This study was supported by grant LGF20H180003 from Basic public welfare research program of Zhejiang Province, grant 2019KY511 from Zhejiang medical and health science and technology project, grant 20190101A09 from the Agriculture and Social development plan of Hangzhou, and grant 20191231Y045 from Hangzhou science and technology guidance project.
References
[1] | Harding E . WHO global progress report on tuberculosis elimination. The Lancet Respiratory Medicine. (2020) ;8: (1):19. |
[2] | The Lancet Public Health. Renewing the fight to end tuberculosis. Lancet Public Health. (2021) ;6: (5):e260. |
[3] | Hegde S , Rithesh KB , Baroudi K , Umar D . Tuberculous lymphadenitis: Early diagnosis and intervention. Journal of International Oral Health. (2014) ;6: (6):96–8. |
[4] | Mohapatra PR , Janmeja AK . Tuberculous lymphadenitis. The Journal of the Association of Physicians of India. (2009) ;57: :585–90. |
[5] | Lazarus AA , Thilagar B . Tuberculous lymphadenitis. Disease-a-month: DM. (2007) ;53: (1):10–5. |
[6] | Reede DL , Bergeron RT . Cervical tuberculous adenitis: CT manifestations. Radiology. (1985) ;154: (3):701–4. |
[7] | Handa U , Mundi I , Mohan S . Nodal tuberculosis revisited: a review. Journal of Infection in Developing Countries. (2012) ;6: (1):6–12. |
[8] | Mathiasen VD , Lillebaek T , Wejse C . Tuberculous lymphadenitis: a forgotten and delayed diagnosis in low-incidence countries. Infection. 2021;[Epub ahead of print]. |
[9] | Rubaltelli L , Corradin S , Dorigo A , Tregnaghi A , Adami F , Rossi CR , et al. Automated quantitative evaluation of lymph node perfusion on contrast-enhanced sonography. AJR. American Journal of Roentgenology. (2007) ;188: (4):977–83. |
[10] | Gupta KB , Kumar A , Sen R , Sen J , Vermas M . Role of ultrasonography and computed tomography in complicated cases of tuberculous cervical lymphadenitis. The Indian Journal of Tuberculosis. (2007) ;54: (2):71–8. |
[11] | Sathekge M , Maes A , D’Asseler Y , Vorster M , Gongxeka H , Van de Wiele C . Tuberculous lymphadenitis: FDG PET and CT findings in responsive and nonresponsive disease. European Journal of Nuclear Medicine and Molecular Imaging. (2012) ;39: (7):1184–90. |
[12] | Fu Y , Shi YF , Yan K , Wang YJ , Yang W , Feng GS . Clinical Value of Real Time Elastography in Patients with Unexplained Cervical Lymphadenopathy: Quantitative Evaluation. Asian Pacific Journal of Cancer Prevention: APJCP. (2014) ;15: (13):5487–92. |
[13] | Wilson SR , Burns PN . Microbubble-enhanced US in body imaging: what role? Radiology. (2010) ;257: (1):24–39. |
[14] | Ajmal S . Contrast-Enhanced Ultrasonography: Review and Applications. Cureus. (2021) ;13: (9):e18243. |
[15] | Wiesinger I , Jung F , Jung EM . Contrast-enhanced ultrasound (CEUS) and perfusion imaging using VueBox®. Clin Hemorheol Microcirc. (2021) ;78: (1):29–40. doi: 10.3233/CH-201040. |
[16] | Dong Y , Qiu Y , Yang D , Yu L , Zuo D , Zhang Q , Tian X , Wang WP , Jung EM . Potential application of dynamic contrast enhanced ultrasound in predicting microvascular invasion of hepatocellular carcinoma. Clin Hemorheol Microcirc. (2021) ;77: (4):461–9. |
[17] | Eisenbrey JR , Gabriel H , Savsani E , Lyshchik A . Contrast-enhanced ultrasound (CEUS) in HCC diagnosis and assessment of tumor response to locoregional therapies. Abdominal Radiology (New York). (2021) ;46: (8):3579–95. |
[18] | Spiesecke P , Fischer T , Friedersdorff F , Hamm B , Lerchbaumer MH . Quality Assessment of CEUS in Individuals with Small Renal Masses-Which Individual Factors Are Associated with High Image Quality? Journal of Clinical Medicine. (2020) ;9: (12):4081. |
[19] | Hashimoto M , Ohkuma K , Akita H , Yamada Y , Nakatsuka S , Mizuno R , et al. Usefulness of contrast-enhanced ultrasonography for diagnosis of renal cell carcinoma in dialysis patients: Comparison with computed tomography. Medicine (Baltimore). (2019) ;98: (47):e18053. |
[20] | Stramare R , Scagliori E , Mannucci M , Beltrame V , Rubaltelli L . The role of contrast-enhanced gray-scale ultrasonography in the differential diagnosis of superficial lymph nodes. Ultrasound Quarterly. (2010) ;26: (1):45–51. |
[21] | Yu M , Liu Q , Song HP , Han ZH , Su HL , He GB , et al. Clinical application of contrast-enhanced ultrasonography in diagnosis of superficial lymphadenopathy. Journal of ultrasound in medicine: official journal of the American Institute of Ultrasound in Medicine. (2010) ;29: (5):735–40. |
[22] | YANG Gao-yi , ZHANG Ying , ZHAO Dan , HUANG Jin-yu , ZHANG Wen-zhi , WANG Da-li , et al. Contrast-enhanced ultrasonographic features of cervical tuberculous lymphadenitis. Chinese Journal of Infectious Diseases. (2010) ;3: (5):277–9. |
[23] | Dudau C , Hameed S , Gibson D , Muthu S , Sandison A , Eckersley RJ , et al. Can contrast-enhanced ultrasound distinguish malignant from reactive lymph nodes in patients with head and neck cancers? Ultrasound in Medicine & Biology. (2014) ;40: (4):747–54. |
[24] | Sidhu PS , Cantisani V , Dietrich CF , Gilja OH , Saftoiu A , Bartels E , et al. The EFSUMB Guidelines and Recommen-dations for the Clinical Practice of Contrast-Enhanced Ultrasound (CEUS) in Non-Hepatic Applications: Update (Long Version). Ultraschall in der Medizin (Stuttgart, Germany. (2014) ;35: (3):259–66. |
[25] | Zhao D , Shao YQ , Hu J , Liu D , Tang W , He N . Role of contrast-enhanced ultrasound guidance in core-needle biopsy for diagnosis of cervical tuberculous lymphadenitis. Clinical Hemorheology and Microcirculation. (2021) ;77: (4):381–9. |
[26] | Park JH , Kim DW . Sonographic diagnosis of tuberculous lymphadenitis in the neck. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. (2014) ;33: (9):1619–26. |
[27] | Moon IS , Kim DW , Baek HJ . Ultrasound-based diagnosis for the cervical lymph nodes in a tuberculosis-endemic area. The Laryngoscope. (2015) ;125: (5):1113–7. |
[28] | De Backer AI , Mortelé KJ , Van Den Heuvel E , Vanschoubroeck IJ , Kockx MM , Van de Vyvere M . Tuberculous adenitis: comparison of CT and MRI findings with histopathological features. European Radiology. (2007) ;17: (4):1111–7. |
[29] | Yin SS , Cui QL , Fan ZH , Yang W , Yan K . Diagnostic Value of Arrival Time Parametric Imaging Using Contrast-Enhanced Ultrasonography in Superficial Enlarged Lymph Nodes. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. (2019) ;38: (5):1287–98. |
[30] | Weber AL , Rahemtullah A , Ferry JA . Hodgkin and non-Hodgkin lymphoma of the head and neck: clinical, pathologic, and imaging evaluation. Neuroimaging Clinics of North America. (2003) ;13: (3):371–92. |
[31] | Aiken AH , Glastonbury C . Imaging Hodgkin and Non-Hodgkin Lymphoma in the Head and Neck. Radiologic clinics of North America. (2008) ;46: (2):363–78, ix-x. |
[32] | Choi EC , Moon WJ , Lim YC . Case report. Tuberculous cervical lymphadenitis mimicking metastatic lymph nodes from papillary thyroid carcinoma. The British Journal of Radiology. (2009) ;82: (982):e208–11. |
[33] | Li L , Mori S , Kodama M , Sakamoto M , Takahashi S , Kodama T . Enhanced sonographic imaging to diagnose lymph node metastasis: Importance of blood vessel volume and density. Cancer Research. (2013) ;73: (7):2082–92. |
[34] | Oikawa SI , Shiga K , Saito D , Katagiri K , Ikeda A , Tuchida K , et al. Association between contrast-enhanced ultrasonography and histopathological findings of the metastatic lymph nodes of patients with head and neck cancer: A preliminary study. Oncology Letters. (2018) ;15: (4):4171–76. |
[35] | Ling W , Nie J , Zhang D , Yang Q , Jin H , Ou X , et al. Role of Contrast-Enhanced Ultrasound (CEUS) in the Diagnosis of Cervical Lymph Node Metastasis in Nasopharyngeal Carcinoma (NPC) Patients. Frontiers in Oncology. (2020) ;10: :972. |
[36] | Wang B , Zhang MK , Zhou MP , Liu Y , Li N , Liu G , et al. Logistic Regression Analysis of Conventional Ultrasound, and Contrast-Enhanced Ultrasound Characteristics: Is It Helpful in Differentiating Benign and Malignant Superficial Lymph Nodes? Journal of Ultrasound in Medicine :Official Journal of the American Institute of Ultrasound in Medicine. 2021;[Epub ahead of print]. |
[37] | Park S , Kim JY , Ryu YJ , Lee H . Kikuchi Cervical Lymphadenitis in Children: Ultrasound Differentiation From Common Infectious Lymphadenitis. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. (2021) ;40: (10):2069–78. |
[38] | Park SG , Koo HR , Jang K , Myung JK , Song CM , Ji YB , et al. Efficacy of Ultrasound-Guided Needle Biopsy in the Diagnosis of Kikuchi-Fujimoto Disease. The Laryngoscope. (1519) ;131: (5):E1519–E1523. |


