
How older adults’ health beliefs affect intention to perform COVID-19 self-examination: A reasoned action approach
Abstract
BACKGROUND:
COVID-19 self-examination is a significant part of the national recovery plan against the virus. Although it is easier to perform COVID-19 self-examination (CSE), only a small percentage of people prefer it. There are no precise statistics on CSE in Malaysia, but informal data from news agencies imply low CSE. Lack of awareness and conflicting information about the reliability of CSE results may have raised concerns about CSE’s efficacy and effectiveness.
OBJECTIVE:
This study investigates how Malaysian older adults’ health beliefs influence their intention to perform CSE. The study developed a framework combining illness threats (ITH), perceived barriers (PBA), medical motivations (MMO), and control over illness (COI) from the Health Belief Model (HBM) with the Reasoned-Action Approach’s attitude (ATT), perceived control (PCO), and intention (INT).
METHODS:
Structural Equation Modelling (SEM) analyses were conducted with AMOS 26 software to determine the influence of HBM on older adults’ attitude, perceived control, and intention. The study collected 200 data for the pilot study and 400 data for hypotheses testing.
RESULTS:
ITH, MMO, and COI have positive effects, whilst PBA affects ATT negatively. ITH and COI positively impact PCO, and PCO has a greater significant effect on INT than ATT.
CONCLUSION:
Given the HBM’s role in influencing older adults’ intention to perform COVID-19 self-examination, providing different levels of care and emphasising the perception of knowledge of illness are especially beneficial. Several recommendations are made to ensure that CSE remains relevant for older adults’ well-being, although COVID-19’s impact has become more stabilised.
 Dr. Kim Piew Lai graduated from the National University of Malaysia with a B.A. in Communication (1996) and an M.Sc. in Quality and Productivity Improvement (1997). He worked in the manufacturing and service industries, focusing on telecommunications, automotive supplies, and healthcare management from 1998 to 2007. Since 2008, Dr Lai has been with Multimedia University, Malaysia as a lecturer at the Faculty of Business where he earned his Ph.D. in 2016. He is an active researcher and has published articles in the areas of health communication, servicescape, branding, and management.
Dr. Kim Piew Lai graduated from the National University of Malaysia with a B.A. in Communication (1996) and an M.Sc. in Quality and Productivity Improvement (1997). He worked in the manufacturing and service industries, focusing on telecommunications, automotive supplies, and healthcare management from 1998 to 2007. Since 2008, Dr Lai has been with Multimedia University, Malaysia as a lecturer at the Faculty of Business where he earned his Ph.D. in 2016. He is an active researcher and has published articles in the areas of health communication, servicescape, branding, and management.
 Dr. Siong Choy Chong is currently the Chief Technical Officer (Quality Assurance) at Finance Accreditation Agency, Malaysia. Prior to that, he was a Professor and Deputy Vice-Chancellor for Academic Affairs and Research in one of the higher education institutions in Malaysia. Dr Chong has published over 150 articles in international refereed journals, conference proceedings, and book chapters. His research interests include quality assurance in higher education, accreditation of prior experiential learning, and micro-credentials. He received his PhD from Multimedia University, Malaysia.
Dr. Siong Choy Chong is currently the Chief Technical Officer (Quality Assurance) at Finance Accreditation Agency, Malaysia. Prior to that, he was a Professor and Deputy Vice-Chancellor for Academic Affairs and Research in one of the higher education institutions in Malaysia. Dr Chong has published over 150 articles in international refereed journals, conference proceedings, and book chapters. His research interests include quality assurance in higher education, accreditation of prior experiential learning, and micro-credentials. He received his PhD from Multimedia University, Malaysia.
 Dr. Binshan Lin is the BellSouth Professor in College of Business at Louisiana State University Shreveport (LSUS). He received his Ph.D. from the Louisiana State University. Currently he serves as Director of Research in College of Business, and Chair of LSUS Faculty of Research and Development Committee. Dr. Lin has published over 280 articles in refereed journals.
Dr. Binshan Lin is the BellSouth Professor in College of Business at Louisiana State University Shreveport (LSUS). He received his Ph.D. from the Louisiana State University. Currently he serves as Director of Research in College of Business, and Chair of LSUS Faculty of Research and Development Committee. Dr. Lin has published over 280 articles in refereed journals.
1Introduction
1.1Background of the study
COVID-19 Self-Examination (CSE) refers to self and portable antigen tests that help detect the presence of coronavirus [54]. It is regarded as an early detection method that aids in reducing COVID-19 fatalities and supplementing precautions of wearing masks, social distancing, frequent handwashing, and staying safe at home.
CSE is especially critical for older adults, particularly those with underlying health conditions, which are classified as a high-risk group for severe COVID-19-related illnesses [1]. According to the Malaysian Ministry of Health’s dashboard [2], the country recorded 4,792,942 cases, with those aged 60 and older accounting for 8.6% to 12.4% of the weekly cases over the 16 weeks period (June to September 2022). Although the percentage is small, it is a cause for concern when the fatality rate is considered. An average of 66.6% to 86.7% of weekly cases resulted in deaths amongst older adults over the said period. The rate is even more concerning, given that the number of older adults infected increased by 88.16% between June 2022 (152 cases) and August 2022 (286 cases) [2]. Older adults (60 years old and above) make up only 7% of Malaysia’s 33 million population, and many may die before being admitted for treatment due to COVID-19 [3]. These figures highlight the importance of taking all necessary precautions and administering CSE regularly.
When performed correctly and regularly with a nasal swab and saliva antigen self-test kit, CSE is an early detection method to reduce fatalities. Although it is easier to use and less expensive than the Polymerase Chain Reaction (PCR) test, only a small percentage of people prefer it. Goggolidou et al. (2021) [55] found that 62% of participants had no preference for the occurrence of COVID-19 self-test. There are no precise statistics on CSE conducted at home in Malaysia, and informal data from news agencies imply low CSE use [4]. Lack of awareness and conflicting information about the reliability of CSE results [5] may have raised concerns about CSE’s efficacy and effectiveness.
Malaysia has implemented restricted movement control orders (MCO) on the economy and social activities from March 18, 2020, to June 28, 2021, followed by National Recovery Plan until December 2021 [90]. Individuals must pay RM30 to RM150 (approximately USD6.66 to USD33.30) for COVID-19 tests during the MCO [91].
Given that the government is gradually relaxing control over measures to curb COVID-19 amidst the daily cases, increasing older adults’ awareness about CSE appears to be a viable strategy for reducing fatalities and increasing the likelihood that they will trust, learn, and perform self-testing regularly.
1.2Research objectives
The Health Belief Model (HBM) refers to a set of health perceptions that guide individuals’ health behaviours [56]. HBM suggests that perceptions about illness threats, barriers, motivations, and control over illness can influence a person’s decision to prevent the health problem [6]. This study uses the HBM to investigate how Malaysian older adults’ health beliefs influence their intention to perform CSE. Although there are studies examining the influences of HBM on behaviours [21, 22, 24, 63], none of them looked at older adults’ behaviour and their acceptance of COVID-19 self-tests. Therefore, it has become elusive to conclude how HBM affects older adults’ decision to perform CSE and how HBM shapes perceived control and attitude towards CSE. The reasoned-action approach [7] is used to investigate the relationships between older adults’ health beliefs and their intention to perform CSE, with attitude and perceived control acting as mediators. The findings suggest formulating appropriate strategies to promote proper and widespread CSE use.
2Theoretical background
2.1The health belief model
The HBM, often referred to as a health-experience model, is widely accepted in healthcare and, more recently, in the Internet [8] and marketing [9] literature. The HBM suggests that a person’s health experience will result in behavioural changes such as the intention to receive vaccination. Such health-related experience provides the knowledge to form a perceptual belief and aid decision-making.
Specifically, the HBM has been discussed as the precursor to prosocial behaviour in the self-examination behavioural context. Shahnazi et al. (2020) [10] found that illness threats (perceived severity and susceptibility), barriers to taking action (perceived barriers and cues to act), medical motivations (trust), and control over illness (perceived self-efficacy) play essential roles in shaping COVID-19’s preventive health behaviour.
Although other models, such as the Relapse-Prevention Model [57] and Transtheoretical model of health behaviour change [58], can be used to examine behaviours, we chose HBM for the following reasons: 1) HBM has been shown to be useful in examining health behaviours [59]; 2) HBM has been widely used in health- [60], and non-health related studies [61, 62]; and 3) HBM provides multi-dimensional perceptions for understanding health behaviours [6, 56].
However, many studies using the HBM to predict health behaviour yielded inconsistent results. Mercadante and Law (2021) [11] found that illness threats and control over illness affect health behaviour, whereas Panahi et al. (2022) [12] discovered that perceived barriers could predict health behaviours. Despite these studies, whether the same beliefs apply to older adults in predicting their health behaviours towards CSE remains elusive. Further, little attention has been paid to the awareness of how the HBM influences older adults’ intention to perform CSE. Studies to date have focused on breast and HIV self-examination, with findings suggesting that illness threats, perceived barriers, medical motivations, and control over illness have either direct or indirect influences on the intention to perform self-examination [13, 15].
Illness threats, a combination of perceived severity and susceptibility, refer to individuals’ perception of health risks due to COVID-19 [6]. Although studies have examined perceived severity and susceptibility separately, Jones et al. (2015) [14] contend that the two are inextricably linked and separating them would not affect behavioural outcomes. When older adults, in particular, have the ability to perceive all severe illnesses (including COVID-19 fatality) that pose a potential threat to their physical health and well-being, it will lead them to perform self-examination [65].
Perceived barriers are perceived obstacles to achieving a desired outcome or status, such as obstacles to improving an individual’s health conditions [14]. Previous research on self-examination behaviour suggests that examining perceived barriers is critical since they may be the most significant reason for not participating in a specific prevention programme [15]. Hence, improving a person’s ability to understand, identify, and mitigate specific barriers can enhance older adults’ intention to perform CSE.
Medical motivations include trust in medical practitioners and medical care [6]. Given the higher risk associated with healthcare services, motivations are linked to credence attributes such as trust and risk. Older adults who are susceptible to COVID-19 infection tend to engage in trusting behaviour and translate their behaviour by consuming certain medical services for better outcomes [66]. Because older adults are vulnerable, the presence of motivations would more likely increase their consumption of healthcare services, including CSE [67]. Medical motivations are significant because they can facilitate cooperative behaviour and boost confidence, resulting in better adherence to a medical programme and improved patient health [16].
Control over illness reflects individuals’ beliefs about their approach to sickness. Individuals who endorse control over illness believe that they can manage the progression of diseases in some ways [17]. This factor is crucial because it influences people’s attitudes toward the healthcare prevention programme. When older adults have some degree of control over their illnesses, it could be interpreted as having some degree of control over COVID-19 illness and being able to control its consequences. Numerous studies have concluded that having control over illnesses is essential for reducing depression, demoralisation and anxiety, and improving the quality of life [18, 64].
2.2Reasoned-action approach theory
The behavioural decision-making literature also highlights the use of Stimulus-Orgasm-Response (SOR) [68] and Means-End-Chain (MEC) [69] approaches to explain individuals’ decision-making. For instance, Lai and Chong (2020) [16] used SOR to understand older adults’ intention to recover, and [70] used the MEC to explore patients’ health experiences.
However, the use of the reasoned-action approach to explaining health decisions in our study can be justified for two reasons. First, this approach provides a heuristic value for explaining CSE and can predict future behaviour. Its heuristic value is evident in many health-related studies that support this approach as a conceptual framework [7, 19]. Second, this approach is parsimonious, comprising a limited number of variables that provide reliable predictive health decision-making [7, 20]. These are evident in past studies [27, 36, 37, 47, 48].
The reasoned-action approach was initially introduced to explain the underlying factors influencing attitude on behaviour. Accordingly, the likelihood of older adults making health-related decisions can be determined by their attitude, subjective norms, and perceived control as the underlying factors.
Attitude refers to how older adults think and feel about their health decisions. Subjective norms are associated with social influence [19], whereas perceived control refers to the older adults’ capability to make a difference in reducing COVID-19 spread, for example, by performing CSE. Given that this study is designed to explain health behaviour during the COVID-19 pandemic, in which older adults are aware of COVID-19 fatalities and are expected to behave in a particular manner to prevent such illness, the effects of subjective norms (individual awareness about COVID-19 fatality and compliance during the pandemic) may have been moderated. Numerous studies have excluded subjective norms based on contexts (see [21]) since this factor may be redundant in well-known and widely understood situations, such as privacy and security risks. Likewise, Hevey et al. (2009) [22] found that subjective norms are irrelevant in a situation when an individual’s beliefs outweigh those of others. Thus, in the COVID-19 context, a person’s high level of CSE awareness may lead to the belief that his or her views outweigh others. This is also consistent with the reasoned-action approach, which is adaptable to different contexts and situations.
Although studies claimed that health beliefs strongly influenced intentional behaviour [23], they could not conclude whether health beliefs influence attitude and perceived control. This is because there is no common understanding of how health beliefs affects other variables [24]. Further, limited studies have examined the relationships between health beliefs and perceived control [21, 22].
2.3Attitude towards CSE and intention to perform CSE
The reasoned-action approach views the relationship between attitude and intention in determining behaviour as voluntary and uncompelled. However, people may experience grief, anxiety, stress, and worry over COVID-19, where a negative attitude toward disconfirming their behaviour may occur [25]. Citing Fishbein and Ajzen’s (2011) [7] reasoned action approach, older adults may feel and think unfavourably about COVID-19 when they perceive a loss and are pessimistic about its fatality. However, given the long-term effects of coronavirus, most people rarely see COVID-19 fatality positively, especially in older adults [26], prompting them to react to behavioural intentions about health prevention programmes [27]. Consistent with previous research [26, 43, 44], it appears plausible to hypothesise that although older adults have negative feelings about COVID-19, probably due to conflicting information [89] and lack of awareness [55], they are required to participate in the health-promoting programme, such as COVID-19 vaccination. Based on this premise, we anticipate that older adults will react similarly to CSE as a form of health promotion. The following hypothesis is constructed:
H1: Negative attitude toward CSE increases the intention to perform CSE. 2.4 Health beliefs and attitude towards CSE
We conceptualise that illness threats reflect older adults’ beliefs associating their health with COVID-19 due to an increased likelihood of infection. We contend that the perception of illness threats precedes attitude towards CSE. We follow the evidence from past studies [28, 71, 72] that offer health belief constructs as the antecedents explaining individual attitudes. Illness threats can become a critical component linking to attitude because it constantly reminds older adults of the seriousness of the illness. If older adults believe performing CSE can minimise their illness, this should directly influence their attitude [28]. Hence, we propose that severity and susceptibility drive older adults’ concerns about COVID-19 illness.
Perceived barriers should elicit increased feelings and deliberative thinking since any estimation of personal obstacles would justify the causal relationships on attitude toward infection control [29]. A significant contributor to perceived barriers is the challenges experienced by individuals, i.e. self-challenges and their desired behavioural outcomes. This is essential in this study since perceived barriers are a collection of challenges, and their presence could affect positive attitudes [30]. We interpret that personal challenges associated with COVID-19 illness, such as confusion and anxiety, could be the main contributors to a positive attitude towards CSE. However, since limited studies have investigated the role of perceived barriers on attitude (see [29] for example), identifying this would contribute to the health literature.
High medical motivations, which are related to trust, should promote positive thoughts and feelings because trust in healthcare justifies the positive effect of an individual participating in disease prevention programmes. Tzeng and Ho (2002) [31] found that the medical motivations aspect of trust reinforces patients’ attitudes toward dietary promotion programmes. An important insight into this effect is that trust may lead individuals, even if they are less familiar, to believe in the knowledge acquired through news, social media or friends and not to question the programme’s effectiveness [13]. This reinforcement of acquired knowledge amongst older adults is essential to boosting positive attitudes since their assurance can be earned through mass media, relationships with doctors, and healthcare programmes [73–75].
We also anticipate that perceived control over illness will influence an individual’s attitude toward CSE in the same way trust influences attitude. When an individual perceives control over illness positively, his or her behaviour should also be positive [32]. Since perceived control over illness reflects not only the ability but also beliefs in capacity [18], self-efficacy should also be viewed as a form of control. Whenever a person uses his or her capacity to prevent or control illness (e.g. preventing contact, getting medical attention or controlling own behaviour), it reinforces his or her belief in living a healthy life. In other words, participating in a disease prevention programme would increase a person’s capacity to attain the desired outcomes and his or her ability to achieve health goals. However, few studies have examined the direct effect of control over illness on attitude. We propose the following hypotheses:
H2: Increased perceived illness threat increases positive attitude towards CSE.
H3: Increased perceived barriers increase positive attitude towards CSE.
H4: Increased medical motivations increase positive attitude towards CSE.
H5: Increased perceived control over illness increases positive attitude toward CSE.
2.5Perceived behavioural control of CSE and intention to perform CSE
Another factor that predicts intention is the individual’s behavioural control, particularly beliefs about using tools as a form of control [21] to achieve the desired outcome, i.e. older adults’ control over CSE use. We contend that behavioural control can help shift the focus of control away from the ability and capacity of individuals (inner), i.e. handling personal illness, to other forms of personal control (external), i.e. dealing with devices, i.e. self-test kit, to achieve desired outcomes. We regard this factor as perceived behavioural control to use CSE, given that older adults who intend to perform CSE for health reasons are more likely to analyse and integrate any conflicting perceptions about self-examination kits. This is evident from previous studies [36, 37, 48], which suggest that individuals’ confidence to perform a task (as a form of perceived control) may serve as a reliable predictor of behavioural intention. Aligned with Ebnehoseini et al. (2020) [33], older adults who perceive that they will prevent COVID-19 illness to avoid health-related expenses are more likely to engage in controlling behaviour by using specific devices such as self-test kits to increase their ability to control their surroundings or outcomes. This leads to the following proposition:
H6: Increased perceived behavioural control of CSE increases intention to perform CSE.
2.6Health beliefs and perceived behavioural control of CSE
Studies have shown that perceived illness threats affect patients’ readmissions, recovery, and stress [34]. Despite the clear behavioural support, empirical evidence linking illness threats and perceived behavioural control are scarce (see [35] for example). If appropriately assessed, perceived illness threats can become an important antecedent reflecting health beliefs, leading to increased adherence to treatment programmes. Higher perceived illness is also hypothesised to lead to greater participation in other psychological determinants, such as behavioural control.
The recognition of perceived barriers associated with perceived behavioural control in the healthcare literature is expected to motivate individuals to achieve the desired outcome, thereby reducing their risk of illness [36]. We expect that increased perceived barriers will increase the perceived behavioural control, i.e. encourage older adults to exert control over their CSE use. When an individual perceives any existence of barriers, such perception generates a motivation to adopt alternative methods to obtain equivalent outcomes [37]. However, studies on the relationship between perceived barriers and behavioural control have received little attention and produced contradictory results. This is evident in the studies [77, 78] that examine perceived barriers and behavioural control exclusively. In another case, reduced perceived barriers were found to increase perceived behavioural control [76], contradicting another empirical finding [37].
We regard past and current experience-based medical motivations for promoting positive perceptions of a healthy life, that of trust and risk, as the primary focus of many health practitioners [38]. Tzeng and Ho (2022) [31] claimed that trust, which is akin to motivation, reflects the overall beliefs of certainty and risk experiences over time, which increase expectations and lead to controlling behaviour. A similar proposition is suggested in Yu et al.’s (2020) [39] motivation-cognition-behaviour model, implying that motivation enhances individuals’ need for behavioural control and ensures positive health outcomes.
Further, since perceived control over illness is largely a personal level of self-control over the aspects of one’s health, we propose that control over illness could directly impact perceived behavioural control by extending a person’s self-efficacy in using tools to practice COVID-19 mitigation. Thus, high levels of control over illness reflect an individual’s ability and capacity to reduce COVID-19 illness over time, which drives him or her to employ tools, such as CSE, as preventative measures. Nevertheless, studies on the relationship between control over illness and perceived behavioural control have found mixed results (see [40, 41]). Given the distinctive nature of how individuals perceive control, we propose a positive link between control over illness and perceived behavioural control. The following hypotheses thus ensue:
H7: Increased illness threat increases perceived behavioural control of CSE.
H8: Increased perceived barriers increase perceived behavioural control of CSE.
H9: Increased medical motivations increases perceived behavioural control of CSE.
H10: Increased control over illness increases perceived behavioural control of CSE.
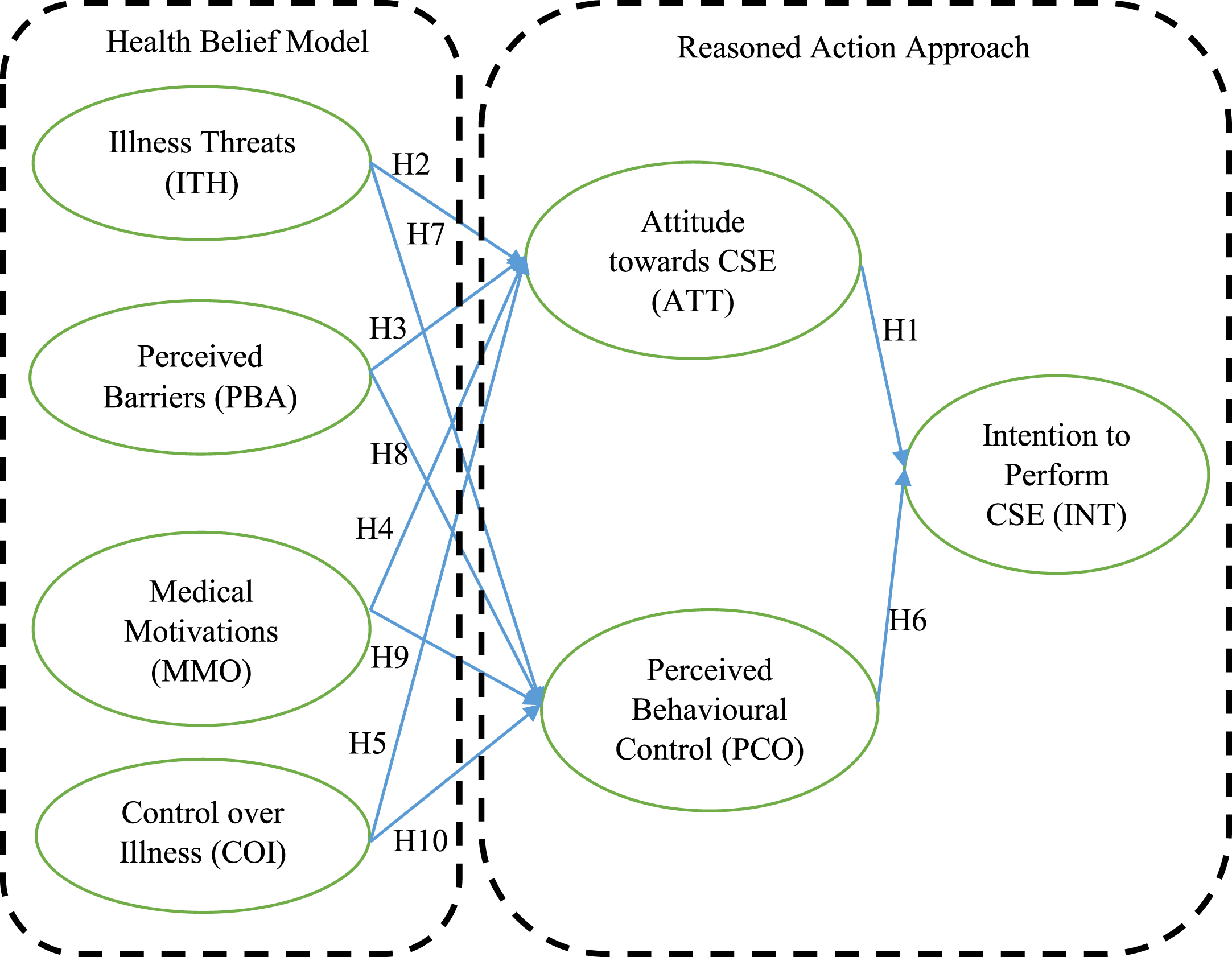
2.7Research model
We present a theoretical model with four HBM factors (ITH, PBA, MMO, and COI) as antecedents and three reasoned-action approach factors (ATT, PCO and INT). We developed hypotheses linking the HBM to attitude and perceived behavioural control, which in turn link to intention but not directly to intention, for two reasons: 1) to align with the understanding of the reasoned-action approach that attitude and perceived behavioural control could provide a reliable predictive behavioural outcome; and 2) to understand the indirect role of attitude better and perceived behavioural control in linking the HBM and intention. Figure 1 depicts the model.
Fig. 1
Research framework.
3Research methodology
3.1Sample selection
We selected individuals aged 60 years and above who are healthy and free from COVID-19 illness as our respondents, i.e. participants with no reported symptoms of coronavirus illness (fever, chills, cough, shortness of breath etc.) in the 14 days preceding the survey. We employed an online survey to avoid physical contact with them. Respondents were introduced and snowballed to reach 200 responses for the pilot and another 400 for hypothesis testing. Online survey questionnaires were distributed via social media platforms, such as Facebook, WhatsApp, WeChat, Messenger, and other real-time messaging apps. Potential respondents were sent a link and invited to complete the survey voluntarily. We included two preliminary questions to ensure that the respondents were legitimate by asking them about their prior experiences with CSE and their most recent self-examination date.
3.2Scale measures
We adapted previous research measures to represent the constructs in the framework. The sources of the survey items are indicated in Table 1. To reduce the possibility of inflated and false estimated relationships amongst constructs, i.e. common method error and variance, we used different scales and pointers to assist respondents in distinguishing the constructs. INT and PCO were measured using 7-point Likert scales, whereas ATT, ITH, PBA, MMO, and COI were assessed using 8-point scales.
Table 1
Details of measures used
| Construct | Items | Pilot (N = 200) | Mass (N = 400) | |
| Intention to perform CSE | INT1 - I intend to perform COVID-19 self-examination once a month. | 0.743 | 0.878 | |
| (INT) | INT2 - I will attempt to perform COVID-19 self-examination in the next month. | 0.644 | 0.745 | |
| INT3 - I have decided to perform COVID-19 self-examination in the next month. | 0.774 | 0.822 | ||
| Source: [96] | ||||
| Attitude towards CSE (ATT) | ATT1 - Performing COVID-19 self-examination is a (bad/good) decision. | 0.896 | 0.923 | |
| ATT2 - Performing COVID-19 self-examination is a (foolish/wise) decision.++ | 0.684 | 0.516 | ||
| ATT3 - I (dislike/like) the idea of performing COVID-19 self-examination. | 0.844 | 0.880 | ||
| ATT4 - Performing COVID-19 self-examination would be (unpleasant/pleasant). | 0.642 | 0.894 | ||
| Source: [97] | ||||
| Perceived Control of CSE (PCO) | PCO1 - I think I understand what problem brought me to do COVID-19 self-examination.+ | 0.242 | ||
| PCO2 - By performing COVID-19 self-examination, I feel I know the meaning of the problem for my family’s future and me.++ | 0.736 | 0.626 | ||
| PCO3 - By performing COVID-19 self-examination, I think I know what caused the problem.+ | 0.444 | |||
| PCO4 - By performing COVID-19 self-examination, I feel I have the tools to make decisions that will influence my future. | 0.827 | 0.825 | ||
| PCO5 - By performing COVID-19 self-examination, I feel I can make a logical evaluation of the various options available to me in order to choose one of them. | 0.842 | 0.818 | ||
| PCO6 - By performing COVID-19 self-examination, I feel I can make decisions that will change my family’s future. | 0.579 | 0.715 | ||
| PCO7 - By performing COVID-19 self-examination, I feel there are certain things I can do to prevent the problem from recurring.+ | 0.498 | |||
| PCO8 - By performing COVID-19 self-examination, I feel I know what to do to ease the situation. | 0.740 | 0.758 | ||
| PCO9 - By performing COVID-19 self-examination, I think I know what my next steps should be. | 0.806 | 0.783 | ||
| Source: [98] | ||||
| Illness Threats (ITH) | ITH1- My current condition will lead to serious long-term health problems.++ | 0.605 | 0.630 | |
| ITH2 - My current condition is causing me a lot of worry and concern. | 0.873 | 0.874 | ||
| ITH3 - The illnesses I get worry me a great deal. | 0.863 | 0.863 | ||
| ITH4 - Whenever I get sick, it seems to be serious. | 0.853 | 0.886 | ||
| ITH5 - My current condition will interfere a great deal with my normal activities. | 0.686 | 0.752 | ||
| ITH6 - I will become very sick as a result of my current condition. | 0.601 | 0.562 | ||
| ITH7 - I get sick more easily than other people my age.++ | 0.663 | |||
| ITH8 - I am concerned about the possibility of becoming seriously ill. | 0.837 | 0.905 | ||
| Source: [6] | ||||
| Perceived Barriers | PBA1 - I worry that taking medicine may cause problems. | 0.863 | 0.896 | |
| (PBA) | PBA2 - The trouble with medicine is that you can get too dependent on them. | 0.890 | 0.873 | |
| PBA3 –Often, the side effects from medications are worse than the illness.++ | 0.823 | 0.763 | ||
| Source: [6] | ||||
| Medical Motivations | MMO1 - Doctors know best for you when you are ill. | 0.820 | 0.727 | |
| (MMO) | MMO2 - When I follow my doctor’s advice usually feel better. | 0.813 | 0.833 | |
| MMO3 - I trust my own feelings about my health rather than a doctor’s advice.+ | 0.483 | |||
| Source: [6] | ||||
| Control Over Illness | COI1 - When I get sick, I just keep going as usual. | 0.775 | 0.694 | |
| (COI) | COI2 - I do not let illness interfere with my life. | 0.789 | 0.767 | |
| COI3 - When I think I am going to be sick, I fight it. | 0.687 | 0.702 | ||
| Source: [6] |
+Italicised - Items were deleted because of factor loadings below 0.50. ++Italicised - Items were deleted because of cross-loadings.
3.3Refinement, reliability and validation of measures
To test the applicability of survey measures in the context of Malaysian older adults, a pilot test of 200 samples was conducted. About 33 items were assessed and refined to align with the study’s objective. For example, item PBA1 was changed from “I worry that taking tablets may cause problems . . . ” to “ . . . taking medicine may . . . ”, and item INT1 from “I intend to perform illness self-examination once a month” to “ . . . perform COVID-19 self-examination . . . ”.
Our initial response rate was low (54 of 200 responses, or 27%). We then contacted the respondents and sought their permission to forward the survey link to their known friends, relatives, and social contacts aged 60 and above. The responses were evaluated once the 200 complete responses had been collected. Data were collected from June to August 2021. The male-to-female ratio was 53 : 47. The respondents’ ethnicity was referred to as “race” by Chinese (69%), Malays (18.5%), and Indians (12.5%). Their ages ranged from 61 to 65 (77.7%), 66 to 70 (15.0%) and over 71 (7.5%). The majority of respondents (68.5%) are retirees who have stopped working, whilst the remaining 31.5% have returned to work as part-timers or self-employed. We used AMOS version 24.0 to compute the constructs’ Cronbach’s alpha and confirmatory factor analysis to assess the construct’s factor loadings (Table 1). The preliminary results indicated that four items (PCO1, PCO3, PCO7 and MMO3) had factor loadings below the threshold of 0.50 with one cross-loaded item (ITH7). Following Hair et al. (2010) [42], we removed all misfit items to improve the representation of the intended construct structure. The items were re-tabulated, and all constructs’ reliability ranged from 0.765 (INT) to 0.912 (ITH). The average variance extracted values met the minimum 0.50 threshold, with a range of 0.522 (INT) to 0.738 (PBA). Having established the constructs’ reliability and validity, we proceed with the remaining 28 items for mass sampling.
4Results
We followed the same procedure of approaching respondents and soliciting their responses through an online survey. Due to the low initial response rate (67 of 400 participants, or 16.75%), we followed up and obtained 400 usable responses from September 2021 to February 2022. All items were within the acceptable kurtosis (+/- 2) and skewness (+/- 5) tolerances. The goodness-of-fit indexes were tabulated to determine how well the data structure fits the structural model. We assessed the measurement model indexes and eliminated four items (ATT2, PCO2, ITH1 and PBA3) because of cross-loadings (see Table 1). The refined measurement model indexes demonstrated an adequate model fit (χ2 = 606.167 (df = 231, n = 400), p <0.001, CFI = 0.942, GFI = 0.880, TLI = 0.930, χ2/df = 2.624; RMSEA = 0.064). The constructs’ reliability and validity met the minimum threshold (Table 2), and the results were further supported by HTMT analysis (Table 3).
Table 2
Constructs’ reliability, validity and correlation coefficient value
| CR | AVE | MSV | MaxR (H) | INT | ATT | PCO | ITH | PBA | MMO | COI | |
| INT | 0.857 | 0.667 | 0.452 | 0.870 | 0.817 | ||||||
| ATT | 0.928 | 0.811 | 0.234 | 0.931 | 0.484 | 0.900 | |||||
| PCO | 0.890 | 0.620 | 0.452 | 0.895 | 0.672 | 0.358 | 0.787 | ||||
| ITH | 0.922 | 0.667 | 0.488 | 0.942 | 0.464 | 0.249 | 0.445 | 0.817 | |||
| PBA | 0.883 | 0.790 | 0.488 | 0.891 | 0.421 | 0.190 | 0.425 | 0.699 | 0.889 | ||
| MMO | 0.757 | 0.610 | 0.338 | 0.769 | 0.462 | 0.448 | 0.396 | 0.402 | 0.391 | 0.781 | |
| COI | 0.765 | 0.521 | 0.379 | 0.768 | 0.616 | 0.414 | 0.572 | 0.361 | 0.538 | 0.581 | 0.721 |
Italicised and bold: Squared root of AVE.
Table 3
HTMT analysis
| INT | ATT | PCO | ITH | PBA | MMO | COI | |
| INT | |||||||
| ATT | 0.484 | ||||||
| PCO | 0.693 | 0.360 | |||||
| ITH | 0.470 | 0.258 | 0.456 | ||||
| PBA | 0.441 | 0.201 | 0.430 | 0.703 | |||
| MMO | 0.474 | 0.444 | 0.403 | 0.417 | 0.396 | ||
| COI | 0.618 | 0.411 | 0.576 | 0.372 | 0.551 | 0.578 |
We then examined the structural model and assessed the ten hypotheses. The structural model indicated that INT has a 53% ability to explain its variance caused by ATT and PCO. The results also showed mixed support for all the hypotheses (Fig. 2 and Table 4). Two of the ten hypotheses were not supported because of contradicting directional relationships (H1 and H3), and the other two were not significant (H8 and H9). Our findings confirmed that ATT and PCO have dominant effects on INT (explanatory power of 53%), confirming Fishbein and Ajzen’s (2011) [7] reasoned-action approach that a small number of variables (ATT and PCO) is sufficient to explain individuals’ health decision making.
Fig. 2
Structural path standardised coefficients.
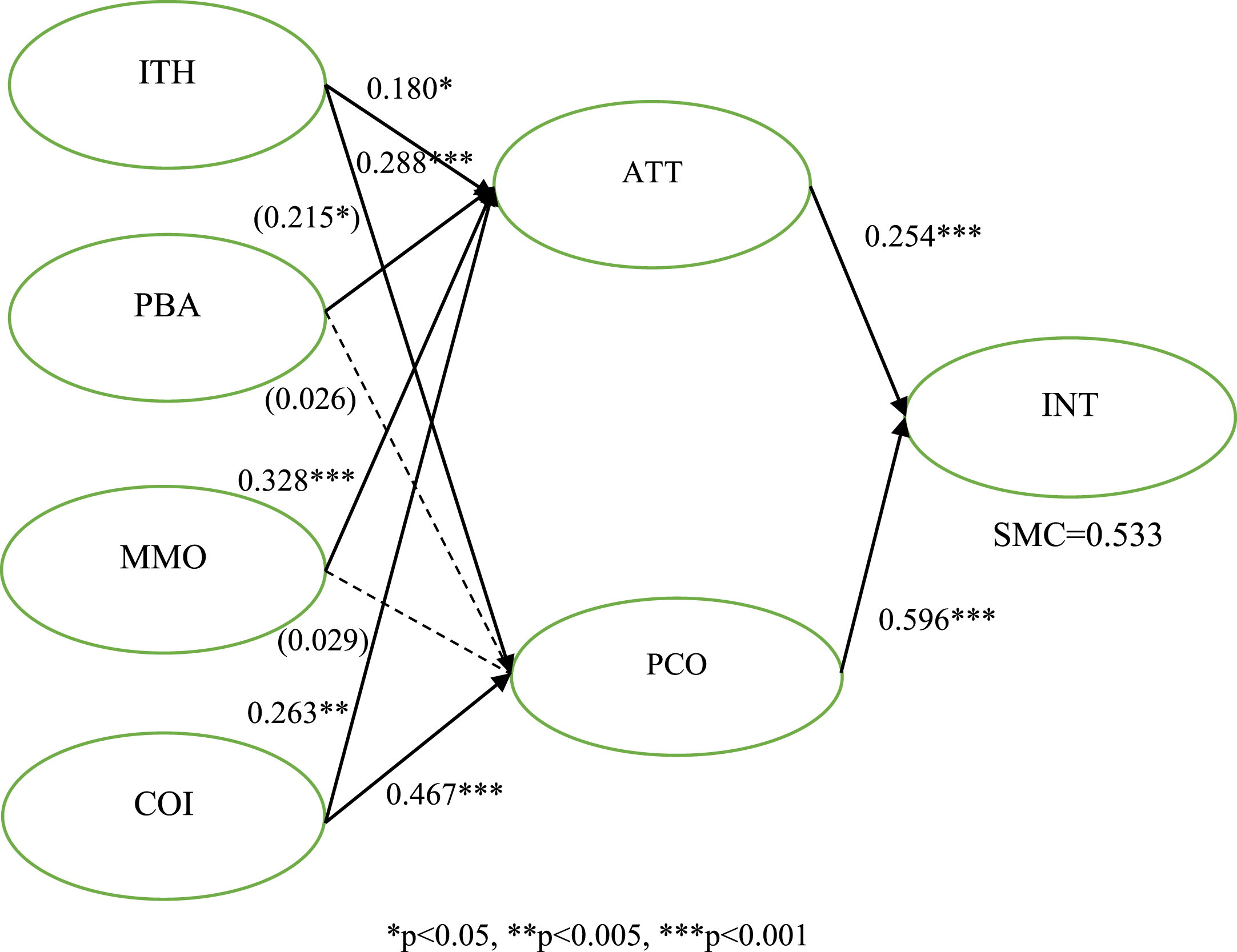
Table 4
Path estimated for research framework
| Relationship | Standardised Co-efficient | Remarks |
| H1: ATT → INT (-) | 0.254*** | Significant but not supported |
| H2: ITH → ATT (+) | 0.180* | Significant, Supported |
| H3: PBA →ATT (+) | (0.215)* | Significant but not supported |
| H4: MMO → ATT (+) | 0.328*** | Significant, Supported |
| H5: COI → ATT (+) | 0.263** | Significant, Supported |
| H6: PCO → INT (+) | 0.596*** | Significant, Supported |
| H7: ITH → PCO (+) | 0.288*** | Significant, Supported |
| H8: PBA → PCO (+) | (0.026) | Not supported |
| H9: MMO → PCO (+) | (0.029) | Not supported |
| H10: COI → PCO (+) | 0.467*** | Significant, Supported |
*p <0.05, **p <0.005, ***p <0.001.
Whilst ATT shows a direct role in channelling a strong effect on INT (H1), the dominant positive influence of ATT comes through the HBM, where ITH, MMO, and COI have direct and positive impacts on ATT, supporting H2, H4, and H5. Although PBA has a direct effect on ATT, the relationship is negative. Thus, H3 is not supported. PCO has a dominant positive impact on INT derived from strong health beliefs to enhance older adults’ behavioural control of CSE, supporting H6. ITH and COI both serve to strengthen PCO amongst older adults, supporting H7 and H10. However, PBA and MMO are more likely to channel moderate effects on ATT compared to PCO. The insignificant relationships of PBA (H8) and MMO (H9) on PCO were unexpected. Another key finding is that ITH, PBA, MMO, and COI play more dominant roles in enhancing PCO than ATT (the variance explained in PCO is 43%, against TT’s 27%).
5Discussion
Our findings suggest that the more concerned older adults are about their health issues, the more they believe, think and consider ways to improve their health, and the greater their attitude and perception of control are, the more likely is their intention to perform CSE. These findings could indicate that older adults who are often concerned about their health tend to think and feel more optimistic about ways to improve their medical conditions and participate in screening programmes.
Surprisingly, older adults show a positive attitude towards CSE, although most people would view COVID-19 fatality negatively. Regarding their attitude towards CSE, we initially hypothesised that the direction of its relationship to intention to perform CSE was negative since past studies in the healthcare [92:page 304, 95:page 168], ethics [93:page 493], and online service [44:page 249] literature suggested a possible negative relationship. We hypothesised this negative relationship based on the findings of a group of respondents who expressed their willingness to participate in health-promoting programmes but perceived their participation to be less efficient. However, the positive effect of attitude on intention, although based on a health concern in the COVID-19 situation, may only partially reflect older adults’ attitudes, given that attitude comprises cognitive and affective attitudes. Indeed, few studies have focused on the distinct effects of older adults’ cognitive and affective attitudes. This is evident in some studies [45, 79, 80], which discovered that different components, i.e. emotional-based and cognitive-based attitudes, affect intention differently. Thus, this study may pave the way for future research into the influence of attitude components on health outcomes.
The link between older adults’ perceived illness threats and attitude suggests the supporting role of severity and susceptibility (H2). Illness threats act as a moderate predictor of attitude, given that the link coefficient is the lowest in this study. This is most likely due to the nature of health concerns, in which illness threats reflect older adults’ fears of becoming ill easily and their belief that they lack self-inspection skills, leading them to be concerned about performing CSE to detect symptoms of illness [46].
The negative relationship between perceived barriers and attitude (H3) is compelling. Our result contradicts previous studies [29, 30], which found that the more concerned older adults are about perceived barriers, the more positive their attitude toward treatments would be. In our study, however, older adults are not motivated to have a positive attitude toward CSE when they sense challenges or confusion. From the healthcare standpoint, older adults may believe CSE could produce false positive results, forcing them to undergo unnecessary medical and quarantine procedures.
Medical motivations have a positive impact on attitude (H4), implying that trust has a far greater influence in shaping older adults’ attitudes toward CSE [13, 31]. Hence, believing in the truth can encourage older adults to think and feel positive about performing self-examination to detect signs of COVID-19 illness.
Similarly, the positive interaction between perceived control over illness and attitude (H5) indicates that an individual’s capacity or efficacy is another crucial aspect of health beliefs that influences attitude. This suggests that having a strong control over illness can generate a positive affirmation, such as confidence or a sense of determination, to protect against disease exposure. Such illness can be prevented in the context of older adults’ health beliefs [18, 33].
In terms of the effects of behavioural control on CSE (H6), we extend prior findings [7, 21, 33] that older adults intend to perform CSE once they gain control of the devices or tools, i.e. self-test kits. The result also shows that PCO, which represents individuals’ ability to use CSE, plays a vital role in directly influencing intention and confirming the reasoning-action approach as the main driver (43% of explanatory power), which contradicts the PCO’s weak effects in some studies [47, 48]. The fact that PCO exerts a strong influence on intention in this study can be explained in several ways. As a new normal practice, CSE awareness may increase an individual’s knowledge and beliefs about COVID-19 protective measures (about his or her intention to perform CSE). Further, the self-testing nature of CSE can enhance cognitive factors (learning about self-testing, using the kits, interpreting, and acting on results), which may precede how attitude influences intention formation. Moreover, the strong influence of PCO on intention is probably due to the existence of COVID-19, which motivates older adults to believe that performing CSE can help them make better healthcare decisions.
Regarding the influence of illness threats (H7), this belief motivates older adults to engage in CSE-related behaviour. This is to be expected given that the COVID-19 nature, which puts older adults at a higher risk [1], can add significance to CSE use based on their perceptions of the seriousness of their current health (e.g. they may think of performing CSE to help them make a better health decision). Moreover, the perceived illness threats that typically occur in older adults magnify the manifestation of health conditions (diseases and illness), raising concerns about the importance of health value [81], as the physical and mental well-being they would gain from participating in a health programme, leading them to engage in health deterioration prevention behaviours [16].
Prior studies have found a possible link between perceived barriers and health examination intention [36, 37], and we expect the same outcome. However, our research shows that PBA does not have any link to PCO (H8). This is intriguing and plausible, given that when older adults face challenges (i.e. fewer skills to learn and less health knowledge to detect signs of illness), such barriers may push them further away from engaging in good health behaviours. Further, we believe that a lack of skills in using and detecting illness cues may impair perception of ability and resources, which presupposes control of intended behaviour.
Similarly, no significant link between medical motivations and perceived behavioural control is established. Like perceived barriers to attitude, older adults supposedly should be swayed by their trust to use CSE. However, they are not motivated to take their trust and risk experiences into account when making health decisions (H9). The weak effect suggests that most interactions about healthcare (e.g. providers, procedures, and medicines) may contain considerable ambiguity, which may increase the unintentional bias assimilation towards healthcare products or services [49]. Moreover, in real life, older adults may become less attentive to remain interested in preserving good health and, therefore, may lose faith in possible healthcare [82]. Thus, ageing may dissuade individuals from seeking help and treatment, which would otherwise increase their trust in healthcare.
Perceived control over illness is positively linked to PCO (H10), leading us to believe that personal self-control, which is similar to self-efficacy, does not impede but instead helps older adults address their needs with health-related devices or tools, i.e. CSE, to sustain a good health condition or control a health-threatening event. We concur with a study [41] that an individual with a strong sense of self-control over illness is more likely to focus on applying solutions to maintain his or her health conditions. This finding supports another study [28] that self-efficacy is a significant factor shaping behavioural care. This is possible, given that COVID-19 acts as a stressor, prompting older adults to seek alternative means of sustaining or controlling their healthcare needs. Thus, introducing self-test kits may have increased older adults’ sense of self-efficacy.
6Conclusion, implications and future research directions
6.1Theoretical implications
We have extended the theoretical and empirical work on older adults’ health beliefs by investigating the roles of illness threats, perceived barriers, medical motivations, and control over illness, as well as attitude, behavioural control, and intention to CSE. The research has also applied the reasoned-action approach, demonstrating that attitude and behavioural control could affect the intention to perform CSE through the HBM variables.
The findings provide new insights into the prominent role of behavioural control over attitude regarding HBM with CSE, which contradicts two prior studies [50, 51]. Our findings show that heightened perceptions of health beliefs help develop behavioural control more than improve their attitude, which increases older adults’ intention to perform CSE. The growing influence of behavioural control may also be associated with advanced age, revealing what older adults want, which is to control their concerns (feelings). This is evidenced by the unexpectedly high level of behavioural control (43% of explanatory power), indicating that older adults’ responses to health beliefs also include the need to control their health outcomes.
This study has also responded to calls from past studies to investigate the impact of health beliefs on older adults’ reasoned actions [77, 83]. The findings support the link between the HBM and the reasoned-action approach, where predicting self-testing behaviour can be more likely if older adults can extend their control over CSE [21]. Some studies consider Fishbein and Ajzen’s intention formation solely from attitude to perceived behavioural control, although HBM variables can be directly linked to intention [27]. In this study, we present a perspective that aligns the reasoned-action approach with HBM. Health beliefs, which represent older adults’ experiential assessments in the same way that behavioural and control beliefs do, are regarded as background factors that indirectly shape intention through perceived behavioural control and attitude. Our study demonstrates that HBM can be linked to individuals’ background factors when it comes to making sense of their health conditions.
Although attitude can predict behaviour [7], it has the most influential impact on healthcare decisions [19] or vaccine intention [51] in non-urgent emergency conditions. Our study indicates that the presence of attitude in life-threatening COVID-19 situations may not primarily influence intention, but it may play a role in establishing a connection between health beliefs and behavioural decisions. The secondary role of attitude may correspond to Casidy et al.’s (2016) [44] study. However, the premise of the non-primary influence of attitude has not been established in the healthcare literature. We propose a future avenue for testing the role of attitude in various situations, such as urgent-life-threatening versus non-urgent-life-threatening conditions.
6.2Managerial implications
Older adults are particularly vulnerable to coronavirus-related illnesses. Thus, they may face the dilemma of sustaining and improving their health to meet some of their primary care needs. Our research provides healthcare practitioners, volunteers, and marketers with a conceptual framework for understanding how older adults perceive health as well as a tool to analyse, measure and improve it within their health experience’s context. Understanding health beliefs as part of a multi-health experience will aid them in detecting and managing high-risk COVID-19 groups.
Regarding healthcare barriers, i.e. conflicting information [89] and low awareness [55], our findings can contribute to the pressing need to transform healthcare organisations through a change in the system as a result of COVID-19 [29]. Healthcare organisations can use the HBM scales to segment older adults based on their prior health experiences and identify the most desired health experience. This is prevalent, given that about 11% of older adults maintain good confidence to age healthily [94].
One common issue in today’s COVID-19 healthcare is that older adults may be anxious and refuse treatment. This means that medical doctors and health officials may have difficulty distinguishing older adults who are more likely to resist treatments from others. Categorising older adults based on their health experiences can assist practitioners in identifying the most vulnerable older age group, i.e. older adults who are optimistic, sceptical or anti-vaccine, and pinpointing what motivates them to acquire information for substantial health benefits. Indeed, the ability to categorise older adults could become a new standard of central competence for healthcare organisations. Medical practitioners may work in this direction collectively to align with the healthcare organisations’ vision, mission and strategy. Besides, health volunteers may take on a new role in promoting and assisting with this effort [88]. These insights can be combined with demographic and psychographic profiles to optimise healthcare campaign exposure and differentiate the level of care for older age groups.
In our research, older adults demonstrate a positive attitude, suggesting they are optimistic about the COVID-19 situation. Thus, their positive attitude can be used as a friendly treatment service blueprint to improve the healthcare organisations’ strategies. For example, health practitioners can promote positive communication, engage with colleagues, and forge information sharing entirely with patients. Healthcare organisations can cultivate a positive healthcare culture by allowing patients to express their treatment decisions with the management staff, medical officers or volunteers via non-personal communication channels such as real-time chats, social media or text messages. Every aspect of treatment decisions in a healthcare organisation involves everyone working as a team. A good service blueprint may not be profitable if the organisation, staff, health practitioners and volunteers are not working together to achieve the shared strategy.
Our findings also demonstrate how health beliefs predict behaviour. We identified two types of HBM - illness threats and control over illness –which are strongly linked to perceived behavioural control and attitude, and related to older adults’ illness perception. This observation is consistent with calls for a greater focus on illness perception regarding treatment convenience. It implies that if practitioners provide opportunities for older adults to participate in activities that help them perceive CSE as a tool for managing their illness, they may be more likely to perform CSE. This is likeable by shifting the promotion of COVID-19 awareness to a stigma-free virtual environment at the right time. Indeed, O’Connor et al. (2014) [52] proposed that older adults should openly discuss their illness perceptions and share and demonstrate community support virtually. After all, virtual venues like virtual cooking classes, virtual conferences, and virtual exercise activities can help reduce older adults’ social isolation.
A human systems perspective may suggest that healthcare organisations develop a new set of core values to serve as the foundation for friendly medication creation. This may encourage health practitioners and volunteers to make a commitment that aligns with the organisational value, i.e. promoting a positive attitude and perceived control. Health practitioners may shift their insistence on treatment decisions with older adults. Likewise, health volunteers may take a new approach to promote a positive attitude and a shift of control that allows older adults to choose their health treatments. However, it would require a collective commitment and responsibility from health practitioners and volunteers at all levels to forge a new friendly value.
We also advocate that health practitioners reverse our suggestion. Practitioners should emphasise the importance of illness perception and not expect older adults to openly talk, share, and seek support as they would in a physical, social gathering setting. Instead, they should let the older adults decide who, when, and what topics they would like to share privately. Put differently, practitioners should reconsider their roles. Instead of concentrating on healthcare, providers of virtual environments should emphasise the virtual environment as a place to meet others, overcome negative beliefs, and so on, which can also offer advice on illness prevention devices or tools such as CSE. In this way, the virtual environment can serve as an alternative source of information for older adults.
Our findings also highlight the importance of behavioural control in predicting intention to perform CSE. As a result, the CSE awareness campaign may need improvement. Older adults may have declining learning abilities and little support to conduct self-examination [46]. Most of the self-kits available to the general public on how to test for COVID-19 are predicated on those who already have the knowledge and skills to perform the test themselves. The self-examination may involve preparing the test area, setting up the test content, taking a swab sample, and processing the sample, which may be complicated for older adults. Practitioners should pay special attention to tools that enable more uncomplicated and simplified control of testing procedures. It is possible to develop a lightweight box with a powerful coronavirus detection method that bypasses all the complicated steps. Practitioners could also consider artificial intelligence (AI) to create a simple user interface for self-examination, allowing older adults to engage actively in protecting themselves. One example is incorporating QR codes with AI assistance into self-kits. We also suggest that healthcare organisations provide education with simplified control of testing procedures to assist older adults in using CSE. In conjunction with this, healthcare organisations could also develop new user-friendly tools that help health practitioners and volunteers employ environment-friendly practices in treatment decisions.
Social media interactions can also improve older adults’ attitudes toward CSE and help them determine where and how to choose self-kit tools. Adopting certification from a government-appointed agency for market approval may help older adults make wiser choices and push manufacturers to improve their test features. By expanding the channels available (social media, campaigns, and COVID-19 safety briefings), practitioners can better gauge older adults’ attitudes toward CSE. However, for these to be effective, older adults must desire to be part of it and be actively engaged with trustworthy information whilst considering and accessing support.
Healthcare organisations can no longer rely on the government’s initiative and directive for COVID-19 recovery. By adopting a swift transformation of the healthcare belief model, the management of healthcare organisations can truly reflect the COVID-19 healthcare reactions. Healthcare organisations should not restrict incorporating innovative ideas to only medical practitioners. Ideas from health volunteers and non-medical practitioners may promote more patient-oriented values on the pressing concerns for unified thinking and action in healthcare.
Another implication for health volunteers stemming from this study is the importance of HBM as a platform that can help increase health promotion and awareness amongst older adults. Health volunteers can fit the issues of ITH, PBA, MMO, and COI into their health promotion campaigns and avoid focusing on the issues of negative-health conditions or negative attitudes such as feelings of anger, frustration, and isolation [84] by carefully designing and identifying important health message older adults appreciate the most. We urge health volunteers to employ a foolproof promotion strategy [85], such as identifying possible communication barriers and better volunteers-older adults’ engagement, as a strategy to help older adults understand the importance of a state of healthy well-being and CSE.
Our findings also suggest the older adults’ positive attitudes and perceived control toward CSE as outcomes of HBM. Given the importance of COVID-19 recovery, health volunteers should consider that HBM increases older adults’ willingness to perform CSE. Such willingness needs to be encouraged and not taken lightly. Health volunteers can establish formal and informal communication channels [86] to elicit older adults’ concerns, raise their awareness, and enhance their CSE intention. Health volunteers can set up CSE work environment stations based on HBM-related terms that can improve CSE awareness and benefit volunteers, healthcare organisations, and practitioners in terms of satisfaction, involvement, and performance [87]. Health volunteers can add value to doctors and medical officers by better understanding older adults’ needs and focusing more on a positive attitude about CSE to improve long COVID-19 conditions in different ways.
6.3Limitations and future research directions
The study has some limitations, which may provide opportunities for improvement and new avenues for future research. First, the validation of health beliefs - illness threats, perceived barriers, medical motivations, and control over illness - suggests that older adults have different health perceptions regarding COVID-19. This raises the question of whether older adults perceive health beliefs differently in life vs non-life-threatening situations. We conducted the study during COVID-19 when older adults have been considered a life-threatening high-risk group. Future studies could broaden and generalise health beliefs to various healthcare conditions.
Our respondents were identified based on their social media presence. This is reasonable, given that at least 60% of older adults have adequate digital literacy [53]. However, we urge practitioners to consider the implications of health beliefs for various older adults with digital versus non-digital literacy. The current study focuses on a specific age group, namely older adults over 60. We recommend testing the HBM’s validity for different age groups.
The majority of HBM research is in the healthcare context. It is worth broadening the concept to explore if the typology of health beliefs can be applied to other settings dealing with healthcare experiences, such as preference for preferred healthcare practitioners, green products, and intention to purchase high-end intelligent workout equipment.
Future studies could also extend our model to the post-pandemic era to determine whether the results can be generalised. This is because older adults’ concerns may differ during and after the COVID-19 situation. Further studies could also examine the model fit for other medical conditions such as non-communicable diseases. Although our results suggest that medical motivations of trust enhance positive attitudes [31], more research is needed to determine whether the same effects occur in crisis and non-crisis situations. We note that in different contexts, i.e. attitude towards illegal drug use, binge drinking, and smoking addictions [46] may not be the same as CSE. We propose that studies be conducted to investigate this phenomenon.
Acknowledgments
The authors would like to express their gratitude to the Centre of e-Services, Entrepreneurship, and Marketing (CESEM) Faculty of Business, Multimedia University, for their support and guidance.
Author contributions
CONCEPTION: Siong Choy Chong and Binshan Lin.
DATA COLLECTION: Kim Piew Lai.
INTERPRETATION OR ANALYSIS OF DATA: Kim Piew Lai.
PREPARATION OF THE MANUSCRIPT: Kim Piew Lai.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Kim Piew Lai Siong Choy Chong and Binshan Lin.
SUPERVISION: Siong Choy Chong and Binshan Lin.
References
[1] | Mustaffa N , Lee SY , Nawi SNM , Rahim MJC , Chee YC , Besari AM , Lee YY , COVID-19 in the elderly: A Malaysian perspective, Journal of Global Health (2020) ;10: (2):020370. |
[2] | Covidnow. Cases by age group: Data for Malaysia/data for past 6 months. Ministry of Health. 2022; March 2;Available from: https://covidnow.moh.gov.my/cases/. |
[3] | Bosman J , Harmon A , Sun A As U.S. nears 800,000 virus deaths, 1 of every 100 older Americans has perished. The New York Times. 2022; March 2; Available from: https://www.nytimes.com/2021/12/13/us/covid-deaths-elderly-americans.html. |
[4] | Nadirah HR More people in Malaysia self-test for COVID-19 before attending gatherings. The Straits Times. 2022; March 2; Available from: https://www.straitstimes.com/asia/se-asia/more-people-in-malaysia-self-test-for-COVID-19-before-attending-gatherings. |
[5] | The Star. Latest COVID-19 test kit needs wider sampling, say health experts. The Star Online. 2022; March 2; Available from: https://www.thestar.com.my/news/nation/202202/11/latest-COVID-19-test-kit-needs-wider-sampling-say-health-experts. |
[6] | Cockburn J , Fahey P , Sanson-Fisher RW , Construction and validation of a questionnaire to measure the health beliefs of general practice patients, Family Practice (1987) ;4: (2):108–116. |
[7] | Fishbein M , Ajzen I , Predicting and Changing Behaviour: The Reasoned Action Approach. New York: Psychology Press. 2011. |
[8] | Willis E , Applying the health belief model to medication adherence: The role of online health communities and peer reviews, Journal of Health Communication (2018) ;23: (8):743–750. |
[9] | Alagarsamy S , Mehrolia S , Predicting intention to buy organic food during the COVID-19 pandemic: A multigroup analysis based on the Health Belief Model. Journal of International Food & Agribusiness Marketing. 2022; Available from: https://doi.org/10.1080/08974438.2022.2035881. |
[10] | Shahnazi H , Ahmadi-Livani M , Pahlavanzadeh B , Rajabi A , Hamrah MS , Charkazi A , Assessing preventive health behaviours from COVID- A cross sectional study with Health Belief Model in Golestan Province, Northern of Iran, Infectious Diseases of Poverty (2020) ;9: (6):91–99. |
[11] | Mercadante AR , Law AV , Will they, or won’t they? Examining patients’ vaccine intention for flu and COVID-19 using the Health Belief Model, Research in Social and Administrative Pharmacy (2021) ;17: (9):1596–1605. |
[12] | Panahi R , Ramezankhani A , Tavousi M , Osmani F , Niknami S , Predictors of adoption of smoking preventive behaviours among university students: Application of Health Belief Model, Journal of Education and Community Health (2022) ;4: (1):35–42. |
[13] | Khiyali Z , Aliyan F , Kashfi SH , Mansourian M , Jeihooni AK , Educational intervention on breast self-examination behaviour in women referred to health centres: Application of Health Belief Model, Asian Pacific Journal of Cancer Prevention (2017) ;18: (10):2833–2838. |
[14] | Jones CL , Jensen JD , Scherr CL , Brown NR , Christy K , Weaver J , The health belief model as an explanatory framework in communication research: Exploring parallel, serial, and moderated mediation, Health Communication (2015) ;30: (6):566–576. |
[15] | Julinawati S , Cawley D , Domegan C , Brenner M , Rowan NJ , A review of the perceived barriers within the Health Belief Model on pap smear screening as a cervical cancer prevention measure, Journal of Asian Scientific Research (2013) ;3: (6):677–690. |
[16] | Lai KP , Chong SC , The influence of servicescape and service credibility on older adults’ intention to recover: A study of rehabilitation services in Malaysia, Journal of Health Organisation and Management (2020) ;34: (2):101–122. |
[17] | Griffin KW , Rabkin JG , Perceived control over illness, realistic acceptance, and psychological adjustment in people with AIDS, Journal of Social and Clinical Psychology (1998) ;17: (4):407–424. |
[18] | Zaleta AK , Miller MF , Olson JS , Yuen EY , LeBlanc TW , Cole CE , Buzaglo JS , Symptom burden, perceived control, and quality of life among patients living with multiple myeloma, Journal of the National Comprehensive Cancer Network (2020) ;18: (8):1087–1095. |
[19] | Molloy BK , Stock M L , Dodge T , Aspelund JG , Predicting future academic willingness, intentions, and Nonmedical Prescription Stimulant (NPS) use with the Theory of Reasoned Action and prototype/willingness model, Substance Use & Misuse (2019) ;54: (14):2251–2263. |
[20] | Ezati Rad R , Kahnouji K , Mohseni S , Shahabi N , Noruziyan F , Farshidi H , Aghamolaei T , Predicting the COVID-19 vaccine receive intention based on the Theory of Reasoned Action in the south of Iran, BMC Public Health (2022) ;22: (1):1–13. |
[21] | Klobas JE , McGill T , Wang X , How perceived security risk affects intention to use smart home devices: A reasoned action explanation, Computers & Security (2019) ;87: :101571. |
[22] | Hevey D , Pertl M , Thomas K , Maher L , Chuinneagain SN , Craig A , The relationship between prostate cancer knowledge and beliefs and intentions to attend PSA screening among at-risk men, Patient Education and Counselling (2009) ;74: (2):244–249. |
[23] | Sheppard J , Thomas CB , Community pharmacists and communication in the time of COVID- Applying the Health Belief Model, Research in Social and Administrative Pharmacy (2021) ;17: (1):1984–1987. |
[24] | Firouzbakht M , Hajian-Tilaki K , Bakhtiari A , Comparison of competitive cognitive models in explanation of women breast cancer screening behaviours using structural equation modelling: Health belief model and theory of reasoned action, European Journal of Cancer Care (2021) ;30: (1):e13328. |
[25] | Karani A , Deshpande R , Jayswal M , Trivedi P , Breach of employer obligation and employee well-being during COVID-19 unlock phase, Human Systems Management (2022) ;41: (2):237–250. |
[26] | Monahan C , Macdonald J , Lytle A , Apriceno M , Levy SR , COVID-19 and ageism: How positive and negative responses impact older adults and society. American Psychologist (2020) ;75: (7):887. |
[27] | Shmueli L , Predicting intention to receive COVID-19 vaccine among the general population using the Health Belief Model and the Theory of Planned Behaviour Model, BMC Public Health (2021) ;21: (1):1–13. |
[28] | Upadhyay N , Upadhyay S , Abed SS , Dwivedi YK , Consumer adoption of mobile payment services during COVID- Extending meta-UTAUT with perceived severity and self-efficacy, International Journal of Bank Marketing (2022) ;40: (5):960–991. |
[29] | Saqlain M , Munir MM , Rehman SU , Gulzar A , Naz S , Ahmed Z . &Mashhood M. Knowledge, attitude, practice and perceived barriersamong healthcare workers regarding COVID- A cross-sectionalsurvey from Pakistan. Journal of Hospital Infection (2020) ;105: (3):419–423. |
[30] | Moore Z , Price P , Nurses’ attitudes, behaviours and perceived barriers towards pressure ulcer prevention, Journal of Clinical Nursing (2004) ;13: :942–951. |
[31] | Tzeng SY , Ho TY , Exploring the effects of product knowledge, trust, and distrust in the health belief model to predict attitude toward dietary supplements, SAGE Open (2022) ;12: (1):21582440211068855. |
[32] | Repka I , Kieda A , Puto G , Zurzycka P , Illness perception in patients suffering from systemic lupus erythematosus, Journal of Public Health, Nursing and Medical Rescue (2020) ;4: (4):34–39. |
[33] | Ebnehoseini Z , Tara M , Tabesh H , Dindar FH , Hasibian S , Understanding key factors affecting on hospital electronic health record (EHR) adoption, Journal of Family Medicine and Primary Care (2020) ;9: (8):4348–4352. |
[34] | Sawyer AT , Harris SL , Koenig HG , Illness perception and high readmission health outcomes, Health Psychology Open (2019) ;6: (1):2055102919844504. |
[35] | Hagger MS , Hardcastle SJ , Hingley C , Strickland E , Pang J , Watts GF , Predicting self-management behaviours in familial hypercholesterolemia using an integrated theoretical model: The impact of beliefs about illnesses and beliefs about behaviours, International Journal of Behavioural Medicine (2016) ;23: (3):282–294. |
[36] | Rahmafitria F , Suryadi K , Oktadiana H , Putro HPH , Rosyidie A , Applying knowledge, social concern and perceived risk in Planned Behaviour Theory for tourism in the COVID-19 pandemic, Tourism Review (2021) ;76: (4):809–828. |
[37] | Damalas CA , Farmers’ intention to reduce pesticide use: The role of perceived risk of loss in the model of the Planned Behaviour Theory, Environmental Science and Pollution Research (2021) ;28: (26):35278–35285. |
[38] | Chen X , Hay JL , Waters EA , Kiviniemi MT , Biddle C , Schofield E , Orom H , Health literacy and use and trust in health information, Journal of Health Communication (2018) ;23: (8):724–734. |
[39] | Yu L , Liu H , Diabate A , Qian Y , Sibiri H , Yan B , Assessing influence mechanism of green utilisation of agricultural wastes in five provinces of China through farmers’ motivation-cognition-behaviour, International Journal of Environmental and Public Health (2020) ;17: (10):3381. |
[40] | Bender B , Milgrom H , Rand C , Ackerson L , Psychological factors associated with medication nonadherence in asthmatic children, Journal of Asthma (1998) ;35: (4):347–353. |
[41] | Dzielska A , Mazur J , Nałecz H , Oblacińska A , Fijałkowska A , Importance of self-efficacy in eating behaviourand physical activity change of overweight and non-overweightadolescent girls participating in healthy me: A lifestyleintervention with mobile technology, Nutrients (2020) ;12: (7):2128. |
[42] | Hair JF , Black WC , Babin BJ , Anderson RE , Multivariate Data Analysis. Seventh Edition. New Jersey: Pearson Prentice Hall. 2010. |
[43] | Lawton R , Conner M , McEachan R , Desire or reason: Predicting health behaviours from affective and cognitive attitudes, Health Psychology (2009) ;28: (1):56–65. |
[44] | Casidy R , Phau I , Lwin M , The role of religious leaders on digital piracy attitude and intention, Journal of Retailing and Consumer Services (2016) ;32: :244–252. |
[45] | Cho H , Li C , Wu Y , Understanding sport event volunteers’ continuance intention: An environmental psychology approach, Sport Management Review (2020) ;23: (4):615–625. |
[46] | Motta ACF , da Hora Rodrigues KR , Could we benefit from oral self-examination during the COVID-19 pandemic? Oral Oncology (2020) ;107: :104840. |
[47] | Foon PY , Ganesan Y , Iranmanesh M , Foroughi B , Understanding the behavioural intention to dispose of unused medicines: An extension of the Theory of Planned Behaviour, Environmental Science and Pollution Research (2020) ;27: (22):28030–28041. |
[48] | Patel J , Kulkarni S , Doshi D , Reddy BS , Reddy MP , Buunk-Werkhoven YA , Determinants of oral hygiene behaviour among patients with moderate and severe chronic periodontitis based on the Theory of Planned Behaviour, International Dental Journal (2019) ;69: (1):50–57. |
[49] | Hall WJ , Chapman MV , Lee KM , Merino YM , Thomas TW , Payne BK , Coyne-Beasley T , Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: A systematic review, American Journal of Public Health.e60-e (2015) ;105: (12):76. |
[50] | Bae SY , Chang PJ , The effect of coronavirus disease-19 (COVID-19) risk perception on behavioural intention towards ‘untact’tourism in South Korea during the first wave of the pandemic (March Current Issues in Tourism (2021) ;24: (7):1017–1035. |
[51] | Matute J , Palau-Saumell R , Meyer J , Derqui B , Jimenez-Asenjo N , Are you getting it? Integrating theories to explain intentions to get vaccinated against COVID-19 in Spain. Journal of Risk Research. 2021; https://doi.org/10.1080/13669877.2021.1958044. |
[52] | O’Connor MF , Arizmendi BJ , Kaszniak AW , Virtually supportive: A feasibility pilot study of an online support group for dementia caregivers in a 3D virtual environment, Journal of Aging Studies (2014) ;30: (1):87–93. |
[53] | Oh SS , Kim KA , Kim M , Oh J , Chu SH , Choi J , Measurement of digital literacy among older adults: Systematic review, Journal of Medical Internet Research (2021) ;23: (2):e26145. |
[54] | Centre for Disease Control and Prevention.COVID-19 Testing: What You Need to Know September 6, 2022. Available at: https://www.cdc.gov/coronavirus/2019ncov/symptomstesting/testing.html. |
[55] | Goggolidou P , Hodges-Mameletzis I , Purewal S , Karakoula A , Warr T , Self-testing as an invaluable tool in fighting the COVID-19 pandemic. Journal of Primary Care &Community Health. 2021 Jan-Dec;12:21501327211047782. doi: 10.1177/21501327211047782. PMID: 34583571; PMCID: PMC8485257. |
[56] | Rosenstock IM , The health belief model and preventive health behaviour, Health Education Monographs (1974) ;2: (4):354–386. |
[57] | Larimer ME , Palmer RS , Marlatt GA , Relapse prevention, An overview of Marlatt’s cognitive-behavioural model. Alcohol Research & Health.151-60. PMID: PMCID: PMC (2014) ;23: (2):6760427. |
[58] | Prochaska JO , Velicer WF , The transtheoretical model of health behaviour change, American Journal of Health Promotion (1997) ;12: (1):38–48. doi: 10.4278/0890-1171-12.1.38.PMID: 10170434 |
[59] | Conner M , Norman P , Predicting long-term healthy eating behaviour: Understanding the role of cognitive and affective attitudes, Psychology & Health (2021) ;36: (10):1165–1181. |
[60] | Tehrani H , Dadashi N , Movahedzadeh D , Khorasani EC , Jafari A , The predictors of the use of complementary and alternative medicine among type 2 diabetes patients based on the Health Belief Model. Journal of Diabetes & Metabolic Disorders. 2022;1-8. . |
[61] | Daragmeh A , Sagi J , Zeman Z , Continuous intention to use e-wallet in the context of the Covid-19 pandemic: Integrating the Health Belief Model (HBM) and Technology Continuous Theory (TCT), Journal of Open Innovation: Technology, Market, and Complexity (2021) ;7: (2):132. |
[62] | Alagarsamy S , Mehrolia S , Predicting intention to buy organic food during the COVID-19 pandemic: A multigroup analysis based on the Health Belief Model. Journal of International Food & Agribusiness Marketing. 2022;1-27. |
[63] | Morowatisharifabad MA , Momayyezi M , Ghaneian MT , Health Belief Model and Reasoned Action Theory in predicting water saving behaviours in Yazd, Iran, Health Promotion Perspectives (2012) ;2: (2):136. |
[64] | Husain MO , Dearman SP , Chaudhry IB , Rizvi N , Waheed W , The relationship between anxiety, depression and illness perception in tuberculosis patients in Pakistan, Clinical Practice and Epidemiology in Mental Health (2008) ;4: (1):1–5. |
[65] | Kachanoff FJ , Bigman YE , Kapsaskis K , Gray K , Measuring realistic and symbolic threats of COVID-19 and their unique impacts on well-being and adherence to public health behaviours, Social Psychological and Personality Science (2021) ;12: (5):603–616. |
[66] | Johnson DS , Grayson K , “Sources and dimensions of trust in service relationships”, in Swartz, T.A. and Iacobucci, D. (Eds), Handbook of Services Marketing and Management, Sage Publications, London. 2000;357-370. |
[67] | LoCurto J , Berg GM , Trust in healthcare settings: Scale development, methods, and preliminary determinants, SAGE Open Medicine (2016) ;4: :2050312116664224. |
[68] | Mehrabian A , Russell JA , An Approach to Environmental Psychology. The MIT Press. 1974. |
[69] | Gutman J , A means-end chain model based on consumer categorization processes, Journal of Marketing (1982) ;46: (2):60–72. |
[70] | Ku GC , Shang IW , Li MF , How Do Location-based augmented reality games improve physical and mental health? Evaluating the meanings and values of Pokémon Go users’ experiences through the Means-End Chain Theory, InHealthcare (2021) ;9: (7):794. |
[71] | Zhao Y , Ni Q , Zhou R , What factors influence the mobile health service adoption? A meta-analysis and the moderating role of age, International Journal of Information Management (2018) ;43: :342–50. |
[72] | Alam MM , Melhim LKB , Ahmad MT , Jemmali M , Public attitude towards COVID-19 vaccination: Validation of COVID-vaccination attitude scale (C-VAS), Journal of Multidisciplinary Healthcare (2022) ;29: (15):941–954. |
[73] | Lin YP , Lee YL , Hung CY , Chang CF , Chen Y , Detection of adulterated drugs in traditional Chinese medicine and dietary supplements using hydrogen as a carrier gas, PloS One (2018) ;13: (10):e0205371. |
[74] | Peng Y , Yin P , Deng Z , Wang R , Patient-physician interaction and trust in online health community: The role of perceived usefulness of health information and services, International Journal of Environmental Research and Public Health (2020) ;17: (1):139. |
[75] | Zhou Y , Chen S , Liao Y , Wu Q , Ma Y , Wang D , Wang X , Li M , Wang Y , Wang Y , Liu Y , General perception of doctor-patient relationship from patients during theCOVID- 19 pandemic in China: A cross-sectional study. Frontiers in Public Health. 2021;9. |
[76] | Rispoli KM , Norman MZ , Hicks E , Early childhood educators’ knowledge and attitudes about developmental screening for Autism Spectrum Disorder, Journal of Early Childhood Teacher Education (2022) ;43: (2):291–306. |
[77] | Yastica TV , Salma SA , Caesaron D , Safrudin YN , Pramadya AR , Application of Theory Planned Behaviour (TPB) and Health Belief Model (HBM) in COVID-19 prevention: A literature review. In 2020 6th International Conference on Interactive Digital Media (ICIDM), IEEE. 2020;1-4. |
[78] | Hossain MB , Alam MZ , Islam MS , Sultan S , Faysal MM , Rima S , Hossain MA , Mamun AA , Health belief model, theory of planned behaviour, or psychological antecedents: What predicts COVID-19 vaccine hesitancy better among the Bangladeshi adults? Frontiers in Public Health (2021) ;9: :711066. |
[79] | Saleem F , Zhang YZ , Gopinath C , Adeel A , Impact of servant leadership on performance: The mediating role of affective and cognitive trust, Sage Open (2020) ;10: (1):2158244019900562. |
[80] | Jang WM , Kim UN , Jang DH , Jung H , Cho S , Eun SJ , Lee JY , Influence of trust on two different risk perceptions as an affective and cognitive dimension during Middle East respiratory syndrome coronavirus (MERS-CoV) outbreak in South Korea: Serial cross-sectional surveys, BMJ Open (2020) ;10: (3):e033026. |
[81] | Lau RR , Hartman KA , Ware JE , Health as a value: Methodological and theoretical considerations, Health Psychology (1986) ;5: (1):25–43. |
[82] | Lichtenberg PA , Gross E , Ficker LJ , Quantifying risk of financial incapacity and financial exploitation in community-dwelling older adults: Utility of a scoring system for the Lichtenberg Financial Decision-Making Rating Scale, Clinical Gerontologist (2020) ;43: (3):266–280. |
[83] | Barattucci M , Pagliaro S , Ballone C , Teresi M , Consoli C , Garofalo A , De Giorgio A , Ramaci T , Trust in science as a possible mediator between different antecedents and COVID-19 booster vaccination intention: An integration of Health Belief Model (HBM) and Theory of Planned Behaviour (TPB), Vaccines (2022) ;10: (7):1099. |
[84] | Griffith J , Relationships of deployment and combat experiences to postdeployment negative health conditions among Army National Guard soldiers, Military Psychology (2019) ;31: (2):128–37. |
[85] | Patra NK , Tripathy JK , Choudhary BK , Implementing the office total productive maintenance (“Office TPM”) program: A library case study, Library Review (2005) ;54: (7):415–24. |
[86] | Gurung G , Derrett S , Gauld R , Hill PC , Why service users do not complain or have ‘voice’: A mixed-methods study from Nepal’s rural primary health care system, BMC Health Services Research (2017) ;17: (1):1–0. |
[87] | Sirca NT , Babnik K , Breznik K , Towards organisationalperformance: Understanding human resource management climate, Industrial Management & Data Systems (2013) ;113: (3):367–384. |
[88] | Shahriari M , Abzari M , Nasr Isfahani A , Kianpour M , Learning, innovation and high performance in knowledge-based firms, Human Systems Management (2017) ;36: (4):285–95. |
[89] | Tan PT , Covid-19 –to test or not to test?. Borneo Post Online. March 2, 2022. Available at: https://www.theborneopost.com/2020/05/29/covid-19-to-test-or-not-to-test/. |
[90] | The Edge Markets. Highlights of the National Recovery Plan. June 15, 2021. Available at: https://www.theedgemarkets.com/article/highlights-national-recovery-plan. |
[91] | The Malay Mail Online. New rules: Malaysians to pay RM30-RM150 for Covid-19 test upon return abroad; foreigners pay RM60-RM250. June 29, 2020. Available at: https://www.malaymail.com/news/malaysia/2020/06/29/new-rules-malaysians-to-pay-rm30-rm150-for-covid-19-test-upon-return-abroad/1879742. |
[92] | Wulfert E , Wan CK , Safer sex intentions and condom use viewed from a health belief, reasoned action, and social cognitive perspective, Journal of Sex Research (1995) ;32: (4):299–311. |
[93] | Goles T , Jayatilaka B , George B , Parsons L , Chambers V , Taylor D , Brune R , Softlifting: Exploring determinants of attitude, Journal of Business Ethics (2008) ;77: (4):481–99. |
[94] | Boo SL , Only one in 10 Malaysian elderly is healthy, expert says. CodeBlue. September 24, 2019. Available at: https://codeblue.galencentre.org/2019/09/24/only-one-in-10-malaysian-elderly-is-healthy-expert-says/. |
[95] | Rana J , Paul J , Health motive and the purchase of organic food: A meta-analytic review, International Journal of Consumer Studies (2020) ;44: (2):162–71. |
[96] | Huang HT , Kuo YM , Wang SR , Wang CF , Tsai CH , Structural factors affecting health examination behavioural intention, International Journal of Environmental Research and Public Health (2016) ;13: (4):395. |
[97] | Taylor S , Todd PA , Understanding information technology usage: A test of competing models, Information Systems Research (1995) ;6: (2):144–76. |
[98] | McAllister M , Wood AM , Dunn G , Shiloh S , Todd C , The perceived personal control (PPC) questionnaire: Reliability and validity in a sample from the United Kingdom, American Journal of Medical Genetics Part A (2012) ;158: (2):367–72. |


