
Improving awareness of the HCR-20 and risk assessment process
Abstract
BACKGROUND:
In 2011 Mrs A assaulted two people, one who died. In the hours prior to the attack she made multiple attempts to gain help including attending accident and emergency, contact with an inpatient service and the police. Subsequent investigation highlighted that her risk was not well documented or understood.
OBJECTIVE:
This quality improvement project aimed to improve knowledge and awareness of HCR-20 risk assessments amongst mental health professionals.
METHOD:
The Quality Improvement approach was taken and various initiatives were introduced to improve knowledge of the location and purpose of the HCR-20 and to ensure that these risk assessments were regularly updated.
RESULTS:
The results indicated that knowledge relating to the HCR-20 significantly improved amongst staff and breaches of deadlines for updating these risk assessments dramatically declined after the induction of the interventions.
CONCLUSION:
Including the ‘risk formulation’ and ‘scenarios’ from the HCR-20 in clients’ crisis plans, introducing training relating to the HCR-20, and including discussions relating to the HCR-20 at the beginning of CPA meetings resulted in improved MDT awareness and knowledge of the HCR-20. A broader understanding and awareness of risk factors enabled the service to move towards a culture of risk being everyone’s business.
1.Background
In 2011, Ms A attacked Ms B at a bus stop, which resulted in Ms B being stabbed in the hand. Following this, Ms B took a knife from a shop and fatally stabbed Ms C. In the hours prior to the attack, Ms A made numerous attempts to seek help. This included contact with the police, two nurses at Accident and Emergency, and staff at an inpatient service. Subsequent investigation highlighted that Ms A’s risk of violence in the community was not appropriately considered by her care team, nor were the factors associated with increments in risk appropriately documented [1].
One of the critical duties of forensic mental health teams concerns assessing service-users’ current and future risks, to implement appropriate risk management strategies and protect the public. The Historical Clinical Risk Management-20 Version 3 (HCR-20) is the most commonly used forensic risk assessment in the UK [2] and evaluates an individual’s risk of violence, the relevance of the risk to their current situation and the appropriate risk management strategies [3]. Table 1 details the items included on the HCR-20.
Table 1
HCR-20 items
| Historical risk factors | Current risk factors | Future risk factors |
| H1 Violence | C1 Insight | R1 Professional services and plans |
| H2 Other antisocial behaviour | C2 Violent intent or ideation | R2 Living situation |
| H3 Relationships | C3 Symptoms of major mental disorder | R3 Personal support |
| H4 Employment | C4 Instability | R4 Treatment or supervision response |
| H5 Substance use | C5 treatment or supervision response | R5 stress or coping |
| H6 Major mental disorder | OC-C Other considerations | OC-R Other considerations |
| H7 Personality disorder | ||
| H8 Traumatic experiences | ||
| H9 Violent attitudes | ||
| H10 Treatment or supervision response | ||
| OC-H Other historical considerations |
The HCR-20 has been demonstrated to accurately predict violent behaviour both during treatment [4,5] and subsequent to discharge [6,7] in individuals with psychological difficulties. Ratings on this assessment have also been demonstrated to predict readmission to a psychiatric ward, following discharge from medium-secure facilities [8].
Multidisciplinary involvement in implementing the HCR-20 has been demonstrated to be effective in risk management, highlighting the importance of communicating these assessments to mental health teams and integrating them into practice [2]. Nevertheless, despite evidence that multidisciplinary risk management strategies can reduce the risk of reoffending [9], research aimed at developing guidance on the communication and integration of the HCR-20 into clinical practice is largely absent.
The purpose of this paper can be summarised by the following statement by Haque and Webster “A risk management plan is only as good as the time and effort put into communicating its findings to others” [10]. Whilst the literature supports the validity and reliability of the HCR-20 as a measure of risk, there are serious problems concerning the communication of this information both within and between mental health teams.
2.Methods
2.1.Interventions
Change ideas were identified, implemented and subsequently evaluated using the Plan-Do-Study-Act (PDSA) cycle [11]. Firstly, psychologists included the ‘risk formulation’ and ‘scenarios’ from the HCR-20 in clients’ crisis plans on Rio, to increase the extent to which the risks were readily identifiable for staff. Secondly, an HCR-20 tab on the summary page of a client’s Rio record was added, to improve the accessibility of risk information. Thirdly, training in accessing and using the HCR-20 was offered to all forensic inpatient staff; the duration of this training was reduced from one hour to 30 minutes following staff feedback. Fourthly, a system was developed to monitor breaches of deadlines for HCR-20 reviews. Finally, procedures were implemented requiring the MDT to review the HCR-20 at the beginning of care planning approach (CPA) meetings, rather than at the end, to afford protected time to and promote greater MDT involvement in the creation of this risk assessment; this has now become standard practice. These interventions were introduced in a sequential order, to determine whether they had a causal relationship with outcomes.
To ensure that these interventions were sustainable, monitoring completion of HCR-20s was embedded into the duties of the assistant psychologists on the wards, HCR-20 training was included in pre-existing annual security training and details of accessing HCR-20s would be included in Rio training for new staff.
2.2.Measures
Firstly, a survey was used to evaluate MDT awareness of the use and location of the HCR-20 on Rio; this survey was administered on a weekly basis to different wards. Secondly, a pre-existing informatics report was used to identify the number of breached deadlines per week, to examine whether breaches declined consequential to the induction of the interventions. If an HCR-20 was approaching a deadline, an email was sent to staff to remind them to complete the risk assessment. Additionally, all of the HCR-20s on one of the wards were audited to ensure that the documents were completed to an appropriate standard.
3.Results
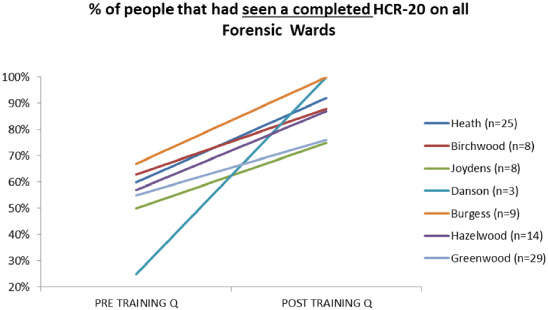
The interventions resulted in an increased awareness of the existence, purpose and location of the HCR-20. As shown in Fig. 1, the percentage of staff members that had seen a completed HCR-20 significantly increased after training. Indeed, paired samples t tests indicated that the intervention resulted in a statistically significant increase in both the percentage of people that had heard of the HCR-20,p (6) = −5.523, p = 0.001, and that had seen an HCR-20, p (6) = −4.950, p = 0.003. Participants noted that HCR-20 training was particularly effective in increasing knowledge and awareness of these risk assessments.
Fig. 1.
Percentage of staff that had seen a completed HCR-20 across all forensic wards.
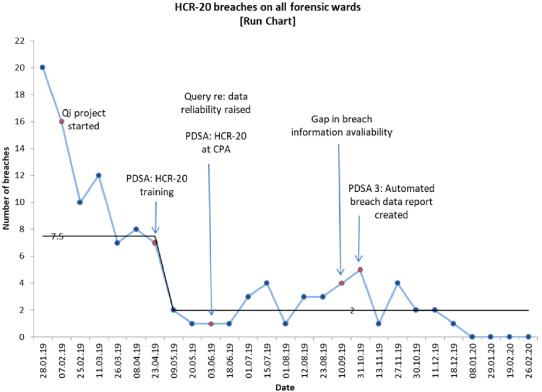
The interventions produced a sustained reduction in HCR-20 breaches by 73%. As shown in Fig. 2, the HCR-20 breaches across all forensic wards declined subsequent to the induction of the interventions, indicating that the interventions maintained an influence over HCR-20 breaches.
Fig. 2.
HCR-20 breaches across all forensic wards.
4.Conclusion
Overall, this QI project indicated that including the ‘risk formulation’ and ‘scenarios’ from the HCR-20 in clients’ crisis plans, adding a tab on the summary page of a client’s Rio record, introducing training relating to the HCR-20, monitoring breaches of HCR-20 reviews and including discussions relating to the HCR-20 at the beginning of CPA meetings resulted in improved MDT awareness and knowledge of the location of the HCR-20 on Rio and reduced HCR-20 breaches. A broader understanding and awareness of risk factors enabled the service to move towards a culture of risk being everyone’s business. This approach is likely to lead to more effective management of risk, compared to it being held in isolation by one or two professionals (usually psychology and psychiatry). Adding a tab of the HCR-20 onto the main summary page enables others (such as Community Mental Health Teams or accident and emergency services) to quickly identify someone’s risk history. These results provide a critical insight into the initiatives that can be used to increase knowledge and awareness of HCR-20s, which will support mental health professionals in making risk-informed clinical decisions.
Some of the interventions were more effective than others. Psychologists reported that copying the ‘risk formulation’ and ‘scenarios’ from the HCR-20 into clients’ crisis plans was a time consuming and ineffective task, as other staff would delete the information from Rio. Additionally, as the risk formulation in crisis plans is generally updated more regularly than the HCR-20, copying the formulation from the HCR-20 may result in out-dated information. Therefore, the team worked with the IT department to develop a system that would automatically update the formulation, negating the need to manually update this. This intervention led to the removal of human error, and saved significant time resources on clinicians.
4.1.Limitations
This project did not provide guidance on approaches to improve the quality of this assessment. Future research must critically examine the quality of HCR-20’s completed in practice. Moreover, whilst this study ascertained evidence for the efficacy of these interventions over a period of months, it is unclear whether the effects would be sustained over a longer period of time, such as years.
4.2.Implications
These results strongly advocate MDT involvement in both the construction and use of the HCR-20. Increasing MDT awareness of risk information in forensic settings is critical in preventing the occurrence of serious further offences, and supporting culture change. Moreover, increasing awareness of the HCR-20 will likely increase general understanding of risk factors and consequently risk management.
Conflict of interest
There were no known conflicts of interest in the completion of this quality improvement project.
References
[1] | Shirley P, Green P, Romily C , External investigation into the case of Ms A. Caring Solutions, NHS England. 2016. Available from: http://oxleas.nhs.uk/site-media/cms-downloads/Report-of-the-independent-investigation-into-the-care-and-treatment-of-Ms-A.pdf. |
[2] | Beazley P, Carter A, Stewart SJ, Renton J. Practicalities of HCR-20 implementation within secure psychiatric services. Journal of Psychiatric Intensive Care. (2017) ;13: (1):47–56. doi:10.20299/jpi.2017.003. |
[3] | Douglas KS, Hart SD, Webster CD, Belfrage H, Guy LS, Wilson CM. Historical-clinical-risk management-20, version 3 (HCR-20V3): Development and overview. International Journal of Forensic Mental Health. (2014) ;13: (2):93–108. doi:10.1080/14999013.2014.906519. |
[4] | De Vogel V, De Ruiter C. Structured professional judgment of violence risk in forensic clinical practice: A prospective study into the predictive validity of the Dutch HCR-20. Psychology, Crime & Law. (2006) ;12: (3):321–36. doi:10.1080/10683160600569029. |
[5] | Belfrage H, Fransson R, Strand S. Prediction of violence using the HCR-20: A prospective study in two maximum-security correctional institutions. The Journal of Forensic Psychiatry. (2000) ;11: (1):167–75. doi:10.1080/095851800362445. |
[6] | Arbach-Lucioni K, Andres-Pueyo A, Pomarol-Clotet E, Gomar-Sones J. Predicting violence in psychiatric inpatients: A prospective study with the HCR-20 violence risk assessment scheme. Journal of Forensic Psychiatry & Psychology. (2011) ;22: (2):203–22. doi:10.1080/14789949.2010.530290. |
[7] | Gray NS, Taylor J, Snowden RJ. Predicting violent reconvictions using the HCR-20. The British Journal of Psychiatry. (2008) ;192: (5):384–87. doi:10.1192/bjp.bp.107.044065. |
[8] | Dolan M, Khawaja A. The HCR-20 and post-discharge outcome in male patients discharged from medium security in the UK. Aggressive Behavior: Official Journal of the International Society for Research on Aggression. (2004) ;30: (6):469–83. doi:10.1002/ab.20044. |
[9] | Dernevik M, Grann M, Johansson S. Violent behaviour in forensic psychiatric patients: Risk assessment and different risk-management levels using the HCR-20. Psychology, Crime and Law. (2002) ;8: (1):93–111. doi:10.1080/10683160208401811. |
[10] | Haque Q, Webster CD. Staging the HCR-20: towards successful implementation of team-based structured professional judgement schemes. Advances in Psychiatric Treatment. (2012) ;18: (1):59–66. doi:10.1192/apt.bp.110.008367. |
[11] | Langley GJ, Moen RD, Nolan KM, Nolan TW, Norman CL, Provost LP. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. John Wiley & Sons; (2009) . |


