
Validity and reliability of the Pandemic Fatigue Scale (PFS) in the Turkish population
Abstract
BACKGROUND:
The measures developed to fight the COVID-19 pandemic caused fear, stress and anxiety in people over time. It was reported that pandemic fatigue, associated with the gradual loss of motivation to follow the implemented protective measures, emerged in societies.
OBJECTIVE:
This cross-sectional-methodological study aimed to validate the Turkish version of the Pandemic Fatigue Scale, developed by Lilleholt et al. (2020).
METHODS:
A web-based questionnaire was conducted to examine the validity and reliability of the Turkish version of the PFS. 1149 participants from all regions in Turkey participated. Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA) were performed.
RESULTS:
As a result of the KMO and Bartlett’s Test of Sphericity, the scale was suitable for the factor analysis. According to EFA, the scale has two sub-factors. The first sub-factor explained 48.7%, and the second sub-factor explained 16.7% of the total variance. Factor loadings of items varied between 0.67 and 0.89. CFA shows that acceptable fit values were obtained for the RMSEA, GFI, AGFI, CFI, NFI and IFI fit indices.
CONCLUSIONS:
The results support that PFS is a valid and reliable screening tool that can be used to measure the phenomenon of pandemic fatigue.
1Introduction
As of December 27, 2021, 290.363.466 COVID-19 cases and 5.445.713 COVID-19 related deaths were reported around the world. According to data from the World Health Organization (WHO) on the same date, 9.518.390 confirmed COVID-19 cases and 82.506 COVID-19 related deaths were reported in Turkey [1]. Due to its rapid spread and an alarming number of deaths, the COVID-19 pandemic became a clinical threat to the all population and healthcare workers worldwide. However, information about this new virus was quite limited when it first came out. Since there was no treatment or vaccine, in the beginning, controlling the infection was considered to be the only intervention available to prevent the spread of COVID-19 [2].
Accordingly, governments and health policymakers are adopting risk-reducing measures to prevent the spread of the COVID-19, starting with measures that entail obligations such as travel restrictions, partial and complete quarantine, school closures, mandatory quarantine practices at home, wearing face masks, physical distancing and self-isolation. It became tighter over time, depending on the contamination rate [3–5]. For many people, the main reason why rules are broken because of psychological weaknesses is the idea that it is their failure. These people are too weak, too stupid, or immoral to do the right things. For this reason, the term “covidiots” began to be referred to as “pandemic fatigue. “The main reason for the failure of public health practices for the pandemic is pandemic fatigue, which leads to breaking the rules [6].
Besides aiming to control the disease, quarantine also creates adverse effects on the psychosocial health of individuals and societies. This leads to higher prevalence of depression and anxiety, along with fatigue and burnout [7]. Existing restrictions may lead to physical and mental exhaustion in individuals [8] and take fewer precautions and fatigue. However, during the long quarantine practices, compulsory working from home in occupational groups has led to results that provide constant stress from burnout to fatigue [9].
The restrictions caused great economic difficulties even in developed economies, and the decreasing workload brought about problems such as job loss for employees. Various socioeconomic groups were particularly vulnerable to feelings of COVID-19 related anxiety and depression due to the sudden economic recession, increased risk of loneliness from social isolation and current threats of job loss and financial loss [10]. While these practices help prevent the spread of the COVID-19 pandemic, they impose many economic and psychological responsibilities on citizens. In addition, the applicability of the restrictions depends on people’s continuous willingness to comply with the rules [11]. It also caused insensitivity in people, especially towards long-lasting restrictions.
Fatigue is a natural and expected response to constant and unresolved distress in people’s lives. WHO suggested that pandemic fatigue can be perceived as “the loss of motivation in citizens that happens gradually while following the health-protective behaviors, which is influenced by a range of perceptions, experiences and emotions”. Defined as a secret phenomenon that cannot be detected directly, pandemic fatigue was expressed through an increasing number of people who “do not comply with the recommendations and restrictions sufficiently and decrease the expected behavioral state despite the efforts made to keep them informed about the pandemic” [12].
According to the WHO, an individual’s physical and psychological abilities have the power to influence health-protective behaviors. The factors that lead the individual to pandemic fatigue emerge between these two situations. Each of the factors leading to fatigue (perceptions, intentions, experiences, perceived inconvenience, complacency, risk perceptions, values and beliefs) can also be considered as motivating factors that might provide the power to eliminate fatigue in its field [6]. Since December 2019, people all over the world have started to become weary of the protective measures, and it can be observed that this situation, along with pandemic fatigue, has led the individuals not to follow the health-protective behaviors anymore.
It has been stated that the situation that causes the formation of waves in pandemics is the fatigue that occurs in the previous waves. The tendency of pandemics to return in recurrent waves has been known since the 1918 Spanish flu, and it has been stated that COVID-19 will not be the last. For example, the most crucial reason for the second strong wave in Europe in the fall of 2020 was not the loosening of the previously designated measures in the summer, but the general fatigue, caused by these measures emerging in the fall [13].
Some studies suggest that people’s awareness of the pandemic may change over time and, as a result, may affect the spread of the disease [14, 15]. The study results conducted by Lilleholt et al. with a sufficient sample size in many countries, including Germany and Denmark, revealed that pandemic fatigue is a general feeling of unwillingness among citizens to follow health-protective behaviors and demotivation to obtain information regarding COVID-19 [16]. The study was conducted between October 2020-January 2021, when strict rules were reinstated after the gradual normalization in Germany and Denmark in the spring of 2020 [17]. Studies have proved that general fatigue and people are reluctant to comply with the rules. In terms of changing the course of the pandemic, it is vital to determine the level of pandemic fatigue, to ascertain who is experiencing this condition, the feelings and perceptions of the people about pandemic fatigue, and the compliance with the four important health-protective behaviors (distance, hygienic behavior, wearing a mask and information seeking), which are considered to be within the scope of COVID-19 measures. To determine the level of pandemic fatigue and make suggestions to the policymakers, translation of this scale to Turkish was important to ascertain the level of demotivation of the citizens in terms of following the health-protective behaviors after the gradual normalization of the strict measures in our country. In addition, with this scale, it will be possible to determine the level of pandemic fatigue between countries and make comparisons.
This study aims to provide a valid and reliable scale for the Turkish population and future research by analyzing the validity and reliability of the Pandemic Fatigue Scale developed by Lilleholt et al. [18].
2Material and methods
This cross-sectional-methodological study was conducted to evaluate the validity and reliability of the Pandemic Fatigue Scale, which was developed by Lilleholt et al. [18] in accordance with the Turkish language and culture. The research was carried out between 7 and 16 September 2021, with a sample group consisting of individuals from seven different geographical regions of Turkey.
2.1Sample and sampling methods
The population of this study consists of people who live in Turkey. Inclusion criteria were to be a Turkish citizen, to be able to read what was written in Turkish, to be 18 years or older, not to have a psychiatric disorder, and to volunteer to participate in the study. Foreigners living in Turkey were determined as exclusion criteria. Because most of the foreigners in Turkey do not know Turkish, it is impossible for them to fill out the questionnaire. Since it was difficult to reach the entire population, sample selection was made. Accordingly, it was attempted to reach as many people as possible by using purposive and snowball sampling methods, which are convenience sampling methods.
In scale development studies, it is stated that at least five times more people should be contacted [19, 20]. The Pandemic Fatigue Scale is a 6-item scale. However, since the scale included all regions of Turkey, it was thought that it should be conducted with a sample size of at least one thousand people; therefore, the maximum number of people were contacted. Accordingly, 1215 participants were included in the study. However, the data of 66 people who answered the security question incorrectly were deleted, and the study was carried out with the remaining 1149 people. A questionnaire was sent to people in different regions to share the online questionnaire. When the desired number for each region was reached, the data collection process for that region was complete. The data collection process continued until the desired number of participants from each region was reached.
2.2Data collection tools
The questionnaire was used in this study to collect the data. The questionnaire form has two parts. In the first part, the Socio-Demographic Data Collection Form, and in the second part, the Pandemic Fatigue Scale was used. Detailed information about the sections is presented below.
Socio-Demographic Data Collection Form: In this part of the questionnaire, there are eight questions about the gender, marital status, level of education, age, occupation, COVID-19 status of the participants, COVID-19 status of their first-degree relatives, and the geographical region they live in.
Pandemic Fatigue Scale: Pandemic Fatigue Scale was developed by Lilleholt et al. [18]. Pandemic Fatigue Scale is a 7-point Likert-type (1 = Strongly disagree, 2 = Disagree, 3 = Somewhat disagree, 4 = Neither agree nor disagree, 5 = Somewhat agree, 6 = Agree, 7 = Strongly agree), two-factor scale with six items. Information Fatigue Sub-factor: This sub-factor, which has three items, measures the fatigue caused by the news and information about the COVID-19 disease. Behavioral Fatigue Sub-factor: This sub-factor, which has three items, measures the fatigue caused by the desirable and undesirable behaviors and rules in the fight against the COVID-19 pandemic.
This scale aimed to measure the fatigue caused by the determined behavioral patterns, rules, and information in the fight against the COVID-19 disease. High scores from the scale indicate severe pandemic fatigue, and low scores indicate mild pandemic fatigue.
2.3Language validity
The scale was translated from its original English to Turkish by two independent linguists whose native language was Turkish and spoke fluent English. The researchers developed a common scale text by evaluating the scale, translated into Turkish by two independent linguists, vocabulary, semantics and structure. The scale, which two bilingual linguists developed in English and Turkish, was translated back into its original language, English. The text of the scale, which went through a final check, compared to its original version, and its deficiencies were corrected in terms of its compatibility with the Turkish culture and the original scale, and the language validity was ensured.
2.4Data collection process
Data were collected in two stages. The first stage of the study was completed by distributing the Pandemic Fatigue Scale and the Socio-Demographic Questionnaire, which were translated into Turkish, to people with similar characteristics to the sample of the main study for the pilot study. In the second stage, the main research was initiated following the corrections, additions, and deletions made according to the participants’ feedback. In both phases, data was collected with Google Online Forms. The researchers shared the questionnaire link through people residing in seven different regions of Turkey. The data collection process was completed in 10 days.
2.5Content validity
For content validity, the translated and finalized scale draft was sent to a total of five researchers, including a public health expert, a physiotherapist, two healthcare administrators, and a researcher working in the field of health. Expert researchers were asked to analyze the scale draft in language and content. To determine the content validity of the scale items, they were asked to write the appropriate opinion next to each item among the options: i. the item is suitable, ii. review the item, iii. the item is contradictory to the content or not appropriate. The content validity of the scale items was calculated by dividing the number of those who chose options i. and ii. by the total number of experts.
2.6Construct validity
Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA) was performed to evaluate the construct validity.
2.7Determination of reliability
The Cronbach’s Alpha Coefficient was used for the reliability assessment of the scale.
2.8The ethical aspect of research
For the validity and reliability analysis and use of the Pandemic Fatigue Scale by the Turkish language and culture, the necessary permissions were obtained from the article’s corresponding author via e-mail. Before implementing the scale, ethics committee approval was obtained from a state University Social and Human Sciences Ethics Committee (approval date and number: 06.09.2021 – 2021/132). Informed consent was obtained from all participants.
2.9Statistical analysis
The participants’ socio-demographic data were expressed as a percentage and mean values. The EFA and CFA were carried out for the Pandemic Fatigue Scale validity analysis. The Cronbach’s Alpha Coefficient was used to analyze the scale’s internal consistency. The Pearson’s Correlation Coefficient was used to examine the relationship between the scale item-total scores and subscale total scores. Descriptive and confirmatory factor analyses were performed for the content validity index used for the scale. Analyses were carried out with SPSS 25 [21] and AMOS 23 [22] Software Packages. The statistical significance value for the analyses was calculated as 0.05.
3Results
3.1Descriptive results
The findings regarding the socio-demographic information of the participants are presented in Table 1. The table shows that 63.4% (n = 729) of the participants were male and 36.6% (n = 420) were female. It was determined that 63.4% of the participants were married (n = 728). When the distribution of the participants by age groups was examined, the largest number of participants were found to be in the 35–44 age group with a rate of 30.5% (n = 350), while the lowest number of participants were found to be in the 65 years and over the group with a rate of only 1.4% (n = 16). It was seen that at least 150 people and above participated from each region, as planned.
Table 1
The socio-demographic information of the participants (n = 1149)
| Variables | n | % | |
| Gender | Female | 420 | 36.6 |
| Male | 729 | 63.4 | |
| Marital status | Single | 421 | 36.6 |
| Married | 728 | 63.4 | |
| Education | Primary – Secondary school | 45 | 3.9 |
| High school | 99 | 8.6 | |
| Associate’s degree | 110 | 9.6 | |
| Bachelor’s degree | 626 | 54.5 | |
| Master’s degree | 164 | 14.3 | |
| Doctorate | 105 | 9.1 | |
| Age | 18–24 years | 194 | 16.9 |
| 25–34 years | 338 | 29.4 | |
| 35–44 years | 350 | 30.5 | |
| 45–54 years | 200 | 17.4 | |
| 55–64 years | 51 | 4.4 | |
| 65 years and over | 16 | 1.4 | |
| Occupation | Worker | 113 | 9.8 |
| Civil servants | 638 | 55.5 | |
| Retired | 44 | 3.8 | |
| Housewife | 49 | 4.3 | |
| Self-employed | 107 | 9.3 | |
| Student | 198 | 17.2 | |
| COVID-19 status of their first-degree relatives (Have they had it?) | Yes | 662 | 57.6 |
| No | 487 | 42.4 | |
| COVID-19 status of the participants | Yes | 349 | 30.4 |
| No | 800 | 69.6 | |
| Region of residence | Marmara Region | 162 | 14.1 |
| Central Anatolia Region | 156 | 13.6 | |
| Eastern Anatolia Region | 167 | 14.5 | |
| Southeastern Anatolia Region | 160 | 13.9 | |
| Aegean Region | 157 | 13.7 | |
| Black Sea Region | 180 | 15.7 | |
| Mediterranean Region | 167 | 14.5 |
3.2Reliability analysis
3.2.1Reliability of the pandemic fatigue scale with split half method
The split-half analysis method, one of the internal consistency methods, was used to measure reliability. In this method, to estimate test reliability, the test is divided into two equivalent halves. The correlation between the scores of half of them is calculated, and then the reliability of the whole test is estimated based on this calculated correlation [23]. The correlation coefficient was examined between the two parts of the PFS scale, part 1 and part 2. Accordingly, a strong and statistically significant positive relationship was found between part 1 and part 2 (see Table 2).
Table 2
Relationship between the two parts of the Pandemic Fatigue Scale: Split half method (N = 1149)
| Pandemic Fatigue Scale | No. of items | Cronbach’s alpha | Pearson’s r | P value |
| Part 1 | 6 | .859 | .851 | <0.001 |
| Part 2 | 6 | .798 |
In scale development studies, the Cronbach’s alpha coefficient, which is a measure that calculates the internal consistency of the scale items, is used to explain or question the similarity of the items in the scale. The similarity between the items indicates that they measure the same construct.
The Cronbach’s alpha coefficient, which is frequently used for the reliability of Likert-type scales, is 0.70 and above, which is accepted as the threshold value [24]. Internal consistency analysis was conducted for the reliability study of the PFS (see Table 3). The Cronbach’s alpha coefficient was used for the internal consistency of the total scale and sub-factors of PFS. Accordingly, the Cronbach’s alpha coefficient of the total PFS scale was 0.776, and the Cronbach’s alpha coefficient of the two sub-factors of the PFS scale ranged between 0.756 and 0.850. The factors of the PFS scale and the item-total correlation of the total scale were over.50.
Table 3
Reliability of Pandemic Fatigue Scale (N = 1149)
| Factors | No. of items | Standardized item alpha | Corrected item-total correlation range |
| 1 | 3 | .756 | .65–.80 |
| 2 | 3 | .850 | .72–.89 |
| Total scale | 6 | .776 | .67–.79 |
3.2.2Test-retest reliability
Test-retest reliability was used to determine the relationship between the form of the PFS scale after the initial translations and revisions and the main study after the pilot study and test the scale’s stability. The obtained results showed a very strong similarity between the results of the pilot test of the 6-item PFS scale and the results of the main test. Accordingly, it can be stated that the PFS scale maintained the same stability under similar conditions (see Table 4).
Table 4
Test-retest reliability (N = 1149)
| The forms of scale | Pilot test | Interclass correlation coefficient |
| Main test | 0.79** | 0.87 |
| First factor | 0.87** | 0.74 |
| Second factor | 0.78** | 0.92 |
** = p < 0.01.
3.3Validity
3.3.1Content and language validity
For each item of the Pandemic Fatigue Scale, which five different experts evaluated in terms of culture, language and semantics to obtain content and language validity, the fit value was found to be 0.92–1.00; and the fit value for the total scale was found to be 0.97.
3.3.2Construct validity
3.3.2.1 Exploratory Factor Analysis (EFA): EFA was conducted using the SPSS 25 Software Package [21] to determine the factors to which six items in the Pandemic Fatigue Scale are related and the structure of these factors [25]. To conduct the Exploratory Factor Analysis, the required Kaiser-Meyer-Olkin (KMO) value should be 0.60 and above, and Bartlett’s Test of Sphericity (BTS) value should be statistically significant [26]. As a result, the Kaiser-Meyer-Olkin Measure of Sampling Adequacy (KMO) value was found as.785, and Bartlett’s Test of Sphericity (BTS) value was found statistically significant, therefore, the sample was suitable for the factor analysis (x2 = 2178.371, df = 15, p < 001).
The Principal Components Analysis and Orthogonal Varimax Rotation method were used within the scope of the EFA conducted for the Pandemic Fatigue Scale. According to the EFA results, the Pandemic Fatigue Scale exhibited a two-factor structure with six items and an eigenvalue greater than 1. The first sub-factor explained 48.7%, and the second sub-factor explained 16.7% of the total variance. The two-factor structure explained 65.35% of the total variance for the PFS scale. The factor loadings of the first sub-factor varied between 0.80 and 0.89 the factor loadings of the second sub-factor varied between 0.67 and 0.74 (see Table 5). All items were loaded on at least one factor with loading of 0.67 and above. The fifth item in the scale, “I am tired of restricting myself to protect those in the risky group against the pandemic” was loaded on both sub-factors. However, it was decided that the place of this item in the literature should be under the second sub-factor, where it was loaded with a higher factor loading (0.70) since the factor loading in the first sub-factor was low with 0.30. All of the other items were loaded only on the required sub-factor. Communalities for all items in the scale were above 0.50, and these values were above the acceptable value, which is 0.40 [27].
Table 5
Components of the factors and communalities in the pandemic fatigue scale (N = 1149)
| Item | 1 | 2 | h2 |
| Information Fatigue Sub-factor (1) | |||
| 1. I’m tired of the discussions about the pandemic on TV, newspapers and radio. | .887 | .774 | |
| 2. I’m tired of hearing things about the pandemic. | .866 | .831 | |
| 3. Since I don’t want to talk about the pandemic anymore, when the topic of the pandemic comes up among friends and family, I try to change the subject immediately. | .801 | .691 | |
| Behavioral Fatigue Sub-factor (2) | |||
| 4. I feel restricted due to having to exhibit desired behaviors and follow the recommendations about COVID-19. | .737 | .502 | |
| 5. I’m tired of restricting myself to protect those who are in the risky group against COVID-19. | .699 | .580 | |
| 6. I’m losing the courage to fight COVID-19. | .667 | .543 | |
| Eigenvalue | 2.919 | 1.002 | |
| % Variance explained | 48.650 | 16.702 | |
| Cumulative % | 65.353 |
Note: h 2 = communalities.
3.3.2.2. Confirmatory Factor Analysis (CFA):Within the scope of the Pandemic Fatigue Scale construct validity, the CFA analysis was conducted in addition to the EFA to test its compatibility with the original study. The CFA was carried out using the AMOS 23 Software Package [22] to test the structure obtained by the EFA. According to the CFA results conducted for the construct validity of the Pandemic Fatigue Scale, which consists of 6 items and two sub-factors, the goodness-of-fit values of the model and the acceptable values are presented in Table 6. Table 6 shows that the χ2 value was statistically significant (χ2/sd = 2.132; p < 0.001). As a result of the CFA, the factor loadings in the first sub-factor of the PFS, which has a two-factor structure, ranged between 0.72 and 0.91, and factor loadings of the second sub-factor ranged between 0.70 and 0.83 (see Fig. 1). The CFA path diagram and factor loadings regarding the scale are presented in Fig. 1.
Table 6
The goodness of fit values obtained as a result of the CFA
| Reported fit indices | The fit indices obtained as a result of the CFA | Acceptable values |
| X2/df | 2.132 | ≤5 |
| P | <0,001 | |
| RMSEA | 0,031 | ≤0,10 |
| NFI | 0,992 | ≥0,90 |
| CFI | 0,996 | ≥0,90 |
| GFI | 0,995 | ≥0,90 |
| AGFI | 0,987 | ≥0,90 |
| IFI | 0,996 | ≥0,90 |
| TLI | 0,992 | ≥0,95 |
RMSEA = Root Mean Square Error of Approximation, GFI = Goodness-of-Fit Index, AGFI = Adjusted Goodness-of-Fit Index, CFI = Comparative Fit Index, NFI = Normed Fit Index, TLI = Tucker-Lewis Index, IFI = Incremental Fit Index.
Fig. 1
Pandemic Fatigue Scale CFA path diagram. As a result of the CFA, the factor loadings in the first sub-factor of the PFS, which has a two-factor structure, ranged between 0.72 and 0.91, and factor loadings in the second sub-factor ranged between 0.70 and 0.83.
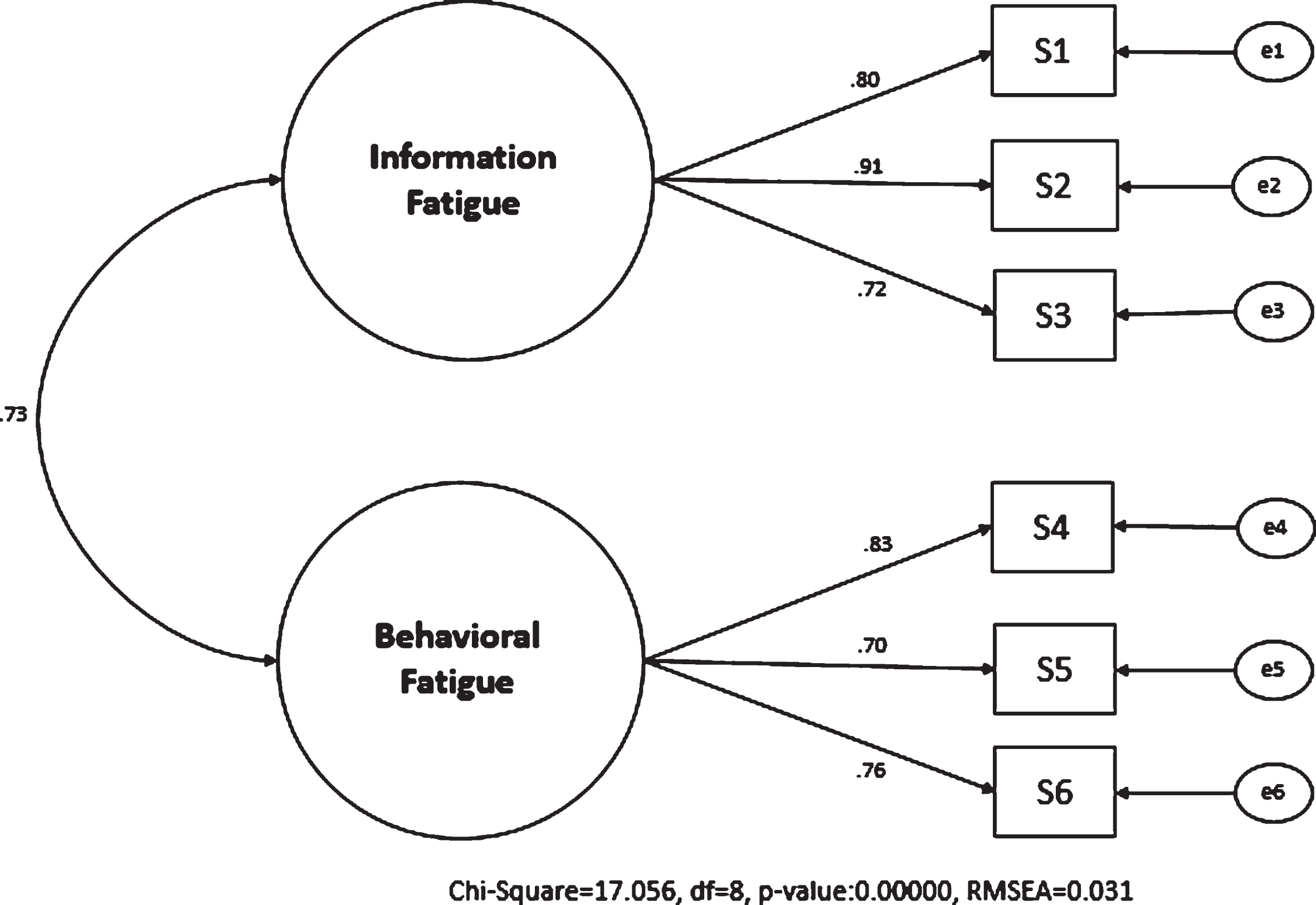
Table 6 shows that the goodness-of-fit values obtained for the model were above the cut-off values; therefore, it could be stated that the model was quite good. According to that, the CFA analysis confirmed the 6-item two-factor Pandemic Fatigue Scale.
4Discussion
Governments and health policymakers worldwide have implemented unprecedented methods to reduce the spread of the Coronavirus disease. They both recommended and mandated obligations such as closing schools, travel restrictions, mandatory quarantine practices at home, wearing masks, physical distancing, and self-isolation [5, 28, 30–32]. While these practices limit the spread of the COVID-19 pandemic, they impose many economic and psychological responsibilities on citizens. In addition, the applicability of restrictions depends on people’s willingness and continued willingness to comply with the rules [10, 11]. In general, despite the intense public support in the fight against the pandemic, it has been reported that there has been an increase in the number of individuals who do not sufficiently comply with the restrictions from some countries and who are at a low level with the information given about the pandemic [29]. The long duration of the pandemic causes pessimism in people. Long-term bans cause people to have a negative attitude towards pandemic rules. For the COVID-19 pandemic, the idea that pandemic fatigue is effective in human behavior and thoughts about the pandemic has emerged [29]. Lilleholt et al. [18] developed a brief self-report for pandemic fatigue based on these considerations. Against the COVID-19 pandemic, which affects the whole world, similar situations are observed at certain intervals in the world’s countries. It seems likely that similar behaviors will be exhibited in different societies for pandemic fatigue. However, different societies may exhibit different behaviors in similar events due to their unique characteristics. This study aims to provide a valid and reliable scale in Turkish that will allow future studies on pandemic fatigue in the Turkish society.
This study was desired to conduct a validity and reliability study of the Turkish version of the Pandemic Fatigue Scale, which was developed to determine the dimensions of pandemic fatigue. With the Turkish version of the Pandemic Fatigue Scale to be obtained as a result of this study, a short and economical measurement tool will be obtained that can be used for the remaining part of the current pandemic in Turkish society and from the beginning of subsequent pandemics.
Lilleholt et al. [18] first designed a ten-item scale in their study and then limited their studies to six items. They found that the one-factor structure did not fit well, but the two-factor structure fits very well. For the two-factor structure obtained, the first factor was named Knowledge Fatigue, and the second factor was named Behavioral Fatigue. The factor loads of the three items in the first factor vary between 0.50 and 0.85, and the factor loads of the three items for the second factor vary between 0.58–0.83. In this study, it was determined that the scale’s reliability was sufficient. As a result of the KMO (Kaiser-Meyer-Olkin Measure of Sampling Adequacy) and Bartlett’s Test of Sphericity, it was determined that the scale was suitable for the factor analysis.
As a result of the EFA, the two sub-factor scale structure was determined. The first sub-factor explained 48.7%, and the second sub-factor explained 16.7% of the total variance. There were three items in the first sub-factor, and the factor loadings of these items varied between 0.80 and 0.89. In the second sub-factor, there were also three items and the factor loadings of these items varied between 0.67 and 0.74. Then, the CFA was performed for the Turkish version, which showed a distribution similar to the original scale incompatibility with the original structure. As a result of the confirmatory factor analysis, acceptable fit values were obtained for the RMSEA, GFI, AGFI, CFI, NFI, IFI and TLI Fit Indices.
The fit of the last two-factor model for the scale developed by Lilleholt et al. [18] was excellent (RMSR = 0.01, RMSEA = 0.02, TLI = 1.00). For the Turkish version of the Pandemic Fatigue Scale, goodness-of-fit measures were found to fit very well (RMSEA = 0.031, GFI = 0.995, AGFI = 0.987, CFI = 0.996, NFI = 0.992, IFI = 0.996 and TLI = 0.992). Therefore, it was determined that the Turkish version of the Pandemic Fatigue Scale is a valid and reliable scale. The scale developed for pandemic fatigue closed a gap in the literature and conceptualized a brief self-report measure of pandemic fatigue.
Thus, this concept was differentiated from other feelings and perceptions related to the pandemic and behavioral responses to the pandemic. The study supported a two-factor structure with similar characteristics to the original. The sub-factors were named information fatigue and behavioral fatigue. Applying the scale to different age groups and people with other socio-demographic characteristics may positively contribute to policymakers.
For example, Labrague [33] conducted a study investigating the effect of pandemic fatigue on nurses’ mental health, sleep quality and job satisfaction among clinical nurses who worked hard during the pandemic period. On the other hand, Petherick et al. [34] examined the fatigue caused by the pandemic in societies during the pandemic process, with data from 14 different countries. It has been found that commitment has a linear increase in relatively low-cost and conventional behavior patterns but decreases in commitment over time insensitive and relatively more costly behavior patterns. Using the Turkish version of the scale in Turkey may help determine the level of pandemic fatigue as the attitudes of Turkish society in terms of pandemic fatigue can be determined. Pandemic fatigue among different occupational groups can be addressed so that the results are compared with the findings obtained in other societies. In addition, with the data obtained in this study, it can be ensured that measures are taken to reduce the effect of pandemic fatigue in terms of Turkish society.
Although this study was conducted in all regions of Turkey, it has limited generalizability because the data were collected by online survey method. At the same time, since the concept of pandemic fatigue has emerged with COVID-19, the effects of this phenomenon may not be revealed by quantitative research methods in the short term. Therefore, future studies should investigate this phenomenon in depth with qualitative studies in the medium and long term. Likewise, since this article is only a methodological study, it is necessary to investigate the pandemic fatigue with regression models in future research, in order to compare the results or investigate the causes.
5Conclusion
The Pandemic Fatigue Scale can be used to determine how the government and health authorities can reduce pandemic fatigue; it can also be used when necessary to determine at what intervals fatigue may occur in terms of public compliance with the rules and enable the preventative measures accordingly.
Ethical approval
Ethics committee approval was obtained from the Dicle University Social and Human Sciences Ethics Committee (approval date and number: 06.09.2021 – 2021/132).
Informed consent
Informed consent was obtained from all participants.
Conflict of interest
The authors declare that there are no conflict of interests.
Acknowledgments
The authors are grateful to all individuals who participated in the study and reviewers for reviewing this article.
Funding
This study did not receive financial support.
Author contributions
All authors contributed to the study’s conception and design, data collection, data analysis and interpretation, drafting of the manuscript, and critical revision of the manuscript. All authors read and approved the final manuscript.
References
[1] | WHO, Coronavirus (COVID-19) Dashboard (2021 Dec 27). https://covid19.who.int/ |
[2] | Lai CC , Shih TP , Ko WC , Tang HJ , Hsueh PR . Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-(COVID-19): The epidemic and the challenges. Int J Antimicrob Agents. (2020) ;55: (3):105924. doi:10.1016/j.ijantimicag.2020.105924 |
[3] | Lin Q , Zhao S , Gao D , et al. A conceptual model for the coronavirus disease (COVID-19) outbreak in Wuhan, China with individual reaction and governmental action. Int J Infect Dis. (2020) ;93: :211–6. doi:10.1016/j.ijid.2020.02.058 |
[4] | De Bruin YB , Lequarre AS , McCourt J , et al. Initial impacts of global risk mitigation measures taken during the combatting of the COVID-19 pandemic. Saf Sci. (2020) ;128: :104773. |
[5] | Chinazzi M , Davis JT , Ajelli M , et al. The effect of travel restrictions on the spread of the novel coronavirus (COVID-19) outbreak. Sci. (2020) ;368: (6489):395–400. |
[6] | Reicher S , Drury J . Pandemic fatigue? How adherence to COVID-19 regulations has been misrepresented and why it matters. BMJ. (2021) ;372: :n137. doi:10.1136/BMJ.n137 |
[7] | Feiz Arefi M , Babaei-Pouya A , Poursadeqiyan M . The health effects of Quarantine during the COVID-19 pandemic. Work. (2020) ;67: (3):523–7. DOI: 10.3233/WOR-203306. PMID: 33164969. |
[8] | Haktanir A , Can N , Seki T , et al. Do we experience pandemic fatigue? Current state, predictors, and prevention. Curr Psychol. (2021) . https://doi.org/10.1007/s12144-021-02397-w |
[9] | Kumaresan A , Suganthirababu P , Srinivasan V , Vijay Chandhini Y , Divyalaxmi P , Alagesan J , Vishnuram S , Ramana K , Prathap L . Prevalence of burnout syndrome among Work-From-Home IT professionals during the COVID-19 pandemic. Work. (2022) ;71: (2):379–84. DOI: 10.3233/WOR-211040. PMID: 35095012. |
[10] | Witteveen D , Velthorst E . Economic hardship and mental health complaints during COVID-19. Proc Natl Acad of Sci. (2020) ;117: (44):27277–84. |
[11] | Bonaccorsi G , Pierri F , Cinelli M , et al. Economic and social consequences of human mobility restrictions under COVID-19. Proc Natl Acad of Sci. (2020) ;117: (27):15530–5. |
[12] | World Health Organization. Regional Office for Europe. Pandemic fatigue: reinvigorating the public to prevent COVID-19: policy considerations for Member States in the WHO European Region [Internet]. World Health Organization. Regional Office for Europe; (2020) . Report No.: WHO/EURO: 2020-1160-40906-55390. Available from: https://apps.who.int/iris/handle/10665/335820 |
[13] | Rypdal K , Bianchi FM , Rypdal M . Intervention fatigue is the primary cause of strong secondary waves in the COVID-19 pandemic. Int J Environ Res Public Health. (2020) ;17: (24):9592. doi: 10.3390/ijerph17249592. PMID: 33371489; PMCID: PMC7767484. |
[14] | Weitz JS , Park SW , Eksin C , Dushoff J . Awareness-driven behavior changes can shift the shape of epidemics away from peaks and toward plateaus, shoulders, and oscillations. Proc Natl Acad of Sci. (2020) . 202009911. doi:10.1073/pnas.2009911117. |
[15] | Funk S , Gilad E , Watkins C , Jansen VAA . The spread of awareness and its impact on epidemic outbreaks. Proc Natl Acad of Sci. (2009) ;106: :6872–7. |
[16] | Böhm R , Lilleholt L , Zettler I . COSMO Denmark Group, Denmark COVID-19 Snapshot Monitoring (COSMO Denmark): Monitoring knowledge, risk perceptions, preventive behaviours, and public trust in the current coronavirus outbreak in Denmark. PsychArch. (2020) . https://doi.org/10.23668/Psycharchives.2795 |
[17] | Betsch C , et al. Germany COVID-19 Snapshot Monitoring (COSMO Germany): Monitoring knowledge, risk perceptions, preventive behaviours and public trust in the current coronavirus outbreak in Germany. PsychArch. (2020) . http://dx.doi.org/10.23668/psycharchives.2776 |
[18] | Lilleholt L , Zettler I , Betsch C , Böhm R . Pandemic Fatigue: Measurement, Correlates, and Consequences. (2020) . https://doi.org/10.31234/osf.io/2xvbr |
[19] | Şencan H . Sosyal ve davranışsal ölçümlerde güvenilirlik ve geçerlilik (reliability and validity in social and behavioral measurement). 1.edition, Ankara: Seçkin Yayınevi; (2005) . |
[20] | Büyüköztürk Ş . Sosyal bilimler için veri analizi el kitabı. 21. Baskı. Pegem Akademi; (2015) . |
[21] | IBM CorReleased. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Cor; (2017) . |
[22] | Arbuckle JL . Amos (Version 23.0) [Computer Program]. Chicago: IBM SPSS; (2014) . |
[23] | Parsons S . Split-half; Robust estimates of split half reliability. (2020) . https://doi.org/10.6084/m9.figshare.5559175.v5 |
[24] | Taber KS . The Use of Cronbach’s Alpha When Developing and Reporting Research Instruments in Science Education. Res Sci Educ. (2018) ;48: :1273–96. https://doi.org/10.1007/s11165-016-9602-2 |
[25] | IBM Corp. Released. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.; (2017) . |
[26] | Kaiser HF . A Second-Generation Little Jiffy. Psychometrika. (1970) ;35: (4):401–15. doi:10.1007/bf022911817 |
[27] | Osborne JW . Best Practices in Exploratory Factor Analysis. Scotts Valley, CA: CreateSpace Independent Publishing; (2014) . |
[28] | Neil M Ferguson , Daniel Laydon , Gemma Nedjati-Gilani , et al. Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand. Imperial College London (16-03-2020). doi:https://doi.org/10.25561/77482 |
[29] | World Health Organization. (2021, August 27). https://apps.who.int/iris/bitstream/handle/10665/335820/WHO-EURO-2020-1160-40906-55390-eng.pdf. Pandemic fatigue Reinvigorating the public to prevent COVID-19. |
[30] | Flaxman S , Mishra S , Gandy A , et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nat. (2020) ;584: (7820):257–61. doi:10.1038/s41586-020-2405-7 |
[31] | Hsiang S , Allen D , Annan-Phan S , et al. The effect of large-scale anti-contagion policies on the COVID-19 pandemic [published correction appears in Nature. 2020 Sep;585(7824):E7]. Nat. (2020) ;584: (7820):262–7. doi:10.1038/s41586-020-2404-8 |
[32] | Kraemer MUG , Yang CH , Gutierrez B , et al. The effect of human mobility and control measures on the COVID-19 epidemic in China. Sci. (2020) ;368: (6490):493–7. doi:10.1126/science.abb4218 |
[33] | Labrague LJ . Pandemic fatigue and clinical nurses’ mental health, sleep quality and job contentment during the COVID-19 pandemic: The mediating role of resilience. J Nurs Manag. (2021) ;29: (7):1992–2001. doi:10.1111/jonm.13383 |
[34] | Petherick A , Goldszmidt R , Andrade EB , et al. A worldwide assessment of changes in adherence to COVID-19 protective behaviours and hypothesized pandemic fatigue. Nat Hum Behav. (2021) ;5: (9):1145–60. doi:10.1038/s41562-021-01181-x |


