
Patients’ perception of personal protective equipment during the SARS-Cov-2 pandemic
Abstract
BACKGROUND:
Since the outbreak of the coronavirus (SARS-Cov-2), wearing personal protective equipment (PPE) has become necessary. Patients’ ability to recognize staff is disrupted impacting on the relationship between healthcare worker and patient.
OBJECTIVE:
Assess the patients’ perspective of healthcare workers wearing PPE and its effect on communication.
METHODS:
Admitted Orthopaedic patients during the first wave of SARS-Cov-2 were surveyed about the experience with staff wearing PPE. In response to feedback, individual badges with large pictures and names were introduced to wear over PPE. Patient views and response to the badges was collected from surveying admitted patients.
RESULTS:
Patients encountered staff wearing face masks and felt this was appropriate in the context of the pandemic. 44% responded that they would prefer staff wearing badges with names, roles and pictures more visible. Following the introduction of badges, patients were better able to recognize staff roles and remember names. Hospital staff felt this was a positive change to help improve rapport while wearing PPE.
CONCLUSION:
Wearing PPE affects patients’ ability to recognize individuals in a fast-paced environment such as an acute hospital. Introducing badges was an intervention based on patient feedback and an important adaptation to sustained PPE use to improve the patient’s experience.
1.Background
Personal protective equipment (PPE) covering the face has become essential during the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) pandemic for healthcare workers as a means of infection prevention control. PPE is recognised as being essential for protecting patients, healthcare workers and their families [1]. World Health Organization (WHO) guidance in February 2020 deemed this necessary and in mid-March 2020 this was mandatory for all direct patient interaction in the NHS [2].
This is not only a physical barrier for the virus but can also be for communication between patients and healthcare workers. While the benefits of PPE cannot be ignored, masks challenge both verbal and non-verbal communication between healthcare workers and patients. This during a time of minimised physical contact and with a cohort of patients who are often elderly and need major medical input this can significantly hamper communication and create a distressing environment [3]. PPE effects speech discrimination in healthcare environments as compared to without it, with wearing of face masks alone found to reduce speech intelligibility by 23% and advanced face protection decreasing this by 69% [4,5].
When connecting with patients, it is the non-verbal cues that can be one of the most effective components especially with patients with cognitive impairment [6]. A large study following the SARS outbreak in Hong Kong researched the effect of face masks on empathy and relational empathy. This study demonstrated facemasks had a significant adverse effect on patient’s perception of empathy and the diminished effects of continuity of care [7].
Non-verbal communication was identified as being a key feature to enabling inpatients to progress with rehabilitation and reduce confusion in elderly patients [7].
Non-verbal communication in the therapeutic relationship between healthcare worker and patient facilitates medical advice to be followed, patient satisfaction and positive clinical outcomes [7]. Other similar studies have suggested use of large reusable name badges to help patients better identify staff [8].
This project has sought to assess the patients’ perspective of healthcare workers wearing PPE during the pandemic and its effect on communication.
2.Methods
A list of patients admitted to the Orthopaedics ward in April 2020 was compiled through electronic medical records system. Following this, patients were contacted via telephone; consent was taken for asking about feedback regarding PPE, followed by the questionnaire (Table 1). Exclusion criteria included uncontactable by telephone, lack of capacity, and patient refusal. Questions were kept simple and brief to maximise understanding.
Following the initial questionnaire badges (Fig. 1) were made with assistance from the local MyWiSH Charity and were made available to all staff in the trust in May 2020. After badges became a regular practice of being worn alongside PPE, feedback was sought from patients needing Orthopaedic input in emergency, fracture clinic and inpatient settings. Clinical staff were also asked to provide opinions on the effect of wearing these badges.
To maximise awareness of badges, we advertised this intervention on the staff intranet to increase uptake in other departments.
Patient feedback (Fig. 2) suggested that communication and rapport was not as severely hampered by PPE as we anticipated however most patients felt introduction of badges was preferable. Our anticipation was that patients would prefer to see larger pictures to help reduce issues with non-verbal communication but unexpectedly names on badges were more important.
3.Results
Seventy-eight patients were admitted to the Orthopaedics ward in April 2020. At the time of assessing patient information in June 2020, 8 patients had died, 4 patients had dementia and were unable to communicate their opinion, 25 patients were not contactable, 1 patient refused to complete the questionnaire, 1 patient did not speak English and was not able to communicate with questionnaire administrators. These were excluded from the results. The remaining 39 patients were included.
Table 1
Results of questionnaire about patient perception to PPE
| Question | Yes (%) | No (%) | Other answers |
| Did you encounter doctors/nurses wearing PPE/face masks? | 31 (79.5%) | 4 (10.3%) | 4 Did not remember any details from admission/Did not remember wearing of masks |
| Did you think it was appropriate considering the current situation with the coronavirus? | 33 (84.6%) | 1 (2.6%) | 4 Did not remember any details from admission/Did not remember wearing of masks 1 Did not think about it |
| Did you feel you were able to communicate in the same way when the team looking after you were wearing masks? | 29 (74.4%) | 3 (7.7%) | 2 Sometimes 4 Did not remember any details from admission/Did not remember wearing of masks 1 No answer |
| Does it affect developing a rapport with the doctor? | 4 (10.3%) | 30 (76.9%) | 4 Did not remember any details from admission/Did not remember wearing of masks 1 No answer |
| When your doctors/nurses looking after you were wearing masks did it make you feel scared? | 0 (0%) | 34 (87.2%) | 4 Did not remember any details from admission/Did not remember wearing of masks 1 No answer |
| Would you prefer doctors wearing a badge with their face visible on it? | 17 (43.6%) | 15 (38.5%) | 3 Not bothered/Does not matter 3 Did not remember any details from admission/Did not remember wearing of masks 1 No answer |
Fig. 1.
Example of badge worn by clinical staff with name, role, and photograph.

Fig. 2.
Natural feedback from staff and patients about badges.
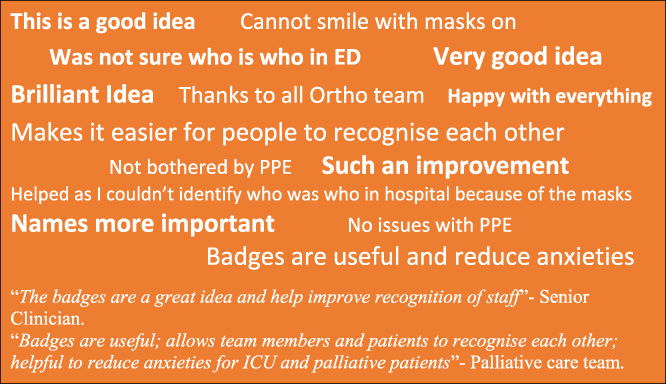
After a four-week period of these badges being worn by Orthopaedic team members in a variety of settings, we invited patients and colleagues to share their thoughts about badges. We were conscious of survey fatigue and were keen for natural feedback to emerge about this intervention to gain a genuine view of badges. We encouraged staff and patients to email their views about the badges if they commented on these during their hospital experience.
Twenty-two patients gave feedback with 68% thinking badges were preferable and beneficial for the patient experience; an increased proportion of patients preferring for staff to wear badges.
The financial cost and assembly of badges was covered by MyWiSH charity.
4.Conclusion
The coronavirus outbreak has had a profound impact on society including healthcare. One major effect of this has been the wearing of PPE. Our project demonstrated that patients thought wearing PPE was not impeding communication. Unexpectedly, they felt that larger name and picture badges would still be helpful in improving the patient experience. Limitations to our project included a small sample size and not accounting for confounding factors. A follow up to this study would include a survey of all patients admitted to hospital within a measurable timeframe.
Being the central component of a healthcare system, patient opinion is a crucial factor to consider following wide-spread changes to clinical practice especially in a system such as the National Health Service where patient-centred care is vital. While not unique, our project showed the willingness of healthcare staff to adapt to seek out a means of supporting our patients during the most challenging of circumstances.
Conflict of interest
None to report.
References
[1] | Chu DK, Akl EA, Duda S, Solo K, Yaacoub S, Schünemann HJ Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. The Lancet. (2020) ;395: (10242). |
[2] | Organization WH , Rational use of personal protective equipment for coronavirus disease (COVID-19): interim guidance, 27 February 2020 [Internet]. Geneva: World Health Organization; 2020. Available from: https://apps.who.int/iris/handle/10665/331215. |
[3] | Sturmey G, Wiltshire M. Patient perspective: Gordon Sturmey and Matt Wiltshire. BMJ. (2020) ). |
[4] | Muzzi E, Chermaz C, Castro V, Zaninoni M, Saksida A, Orzan E. Short report on the effects of SARS-CoV-2 face protective equipment on verbal communication. European Archives of Oto-Rhino-Laryngology. (2021) ). |
[5] | Hampton T, Crunkhorn R, Lowe N, Bhat J, Hogg E, Afifi W The negative impact of wearing personal protective equipment on communication during coronavirus disease 2019. The Journal of Laryngology & Otology. (2020) ;134: (7). |
[6] | Arvanitakis Z, Shah RC, Bennett DA. Diagnosis and management of dementia: Review. JAMA. (2019) ;322: (16). |
[7] | Wong CKM, Yip BHK, Mercer S, Griffiths S, Kung K, Wong MC-S Effect of facemasks on empathy and relational continuity: A randomised controlled trial in primary care. BMC family practice [Internet]. (2013) ;14: (200), Available from: https://pubmed.ncbi.nlm.nih.gov/24364989. |
[8] | Key T, Kulkarni A, Kandhari V, Jawad Z, Hughes A, Mohanty K. The patient experience of inpatient care during the covid-19 pandemic: Exploring patient perceptions, communication, and quality of care at a University Teaching Hospital in the United Kingdom. Journal of Patient Experience. (2021) ;8: . |


