
Cognitive and self-regulation skills for employment among people with brain injury: A comparison of employed and non-employed people using mixed analysis
Abstract
BACKGROUND:
Employment for people with brain injuries is challenging, and identifying the factors that can be improved by rehabilitation and establishing appropriate intervention methods are imperative.
OBJECTIVE:
To examine whether differences in cognitive functions and self-regulation skills exist between employed and non-employed people with brain injuries. In addition, we explored the self-regulation skills characteristic of employed people by qualitatively comparing them to those of non-employed people.
METHODS:
Using a mixed research method, demographic data, neuropsychological tests, self-efficacy, and self-regulation skills were compared between 38 people with brain injuries (16 employed and 22 unemployed) in the community. Subsequently, self-regulation skills were assessed by the Self-Regulation Skills Interview (SRSI), and participants’ responses were qualitatively compared.
RESULTS:
No significant differences were observed in demographic data and neuropsychological tests, but employed people showed significantly better SRSI scores than unemployed people (p < 0.01). The qualitative analysis of the SRSI showed that employed people recognised themselves as having more specific symptoms than unemployed people. For example, they recognised the behaviour ‘when having more than one errand, forgetting it’, whereas non-employed people only recognised the category ‘failure of prospective memory’. Furthermore, employed people reviewed their behaviour and developed ingenious coping strategies, such as ‘looking back on appointments that have been made’, ‘writing down as soon as having a schedule’, whereas unemployed people only exhibited categories such as ‘writing schedules on the cell phone’.
CONCLUSIONS:
Self-regulation skills, such as recognising specific symptoms and developing relevant coping strategies, are effective for gaining employment.
1Introduction
Employment is an important social activity that contributes to people’s well-being. However, maintaining employment for people with brain injuries is challenging [1–5]. Brain injuries cause a variety of sequelae, including physical, cognitive, and behavioural aspects. Therefore, vocational rehabilitation must address these multiple dimensions [4, 5]. At present, vocational rehabilitation techniques for people with brain injuries are not sufficiently developed.
Previous studies have examined factors affecting employment [4–8]. A study conducted by Singh et al. [6] reported associations between employment and factors such as brain injury severity, the number of abnormalities on computed tomography scans, age, and the presence or absence of a psychiatric history. Additionally, Fure et al. [7] reported associations between employment and the quantity of work demanded, compensation, employment status, symptom severity, and sex. DiSanto et al. [8] demonstrated the relevance of age, race, symptom severity, employment status, education, and independence in using public institutions. Importantly, many of these factors do not overlap, suggesting an interplay of a variety of factors impacting employment. In addition, as many of these factors cannot be improved by rehabilitation, identifying the factors that can be improved using rehabilitation and establishing appropriate intervention methods are crucial [9].
Based on a meta-analysis of qualitative studies, interviews with people who had returned to work reported that they felt self-coping behaviours, such as recognizing their own symptoms and developing coping strategies, were important in the return-to-work process [10]. These behaviours are shown in various components, including self-awareness, self-concept, self-esteem, self-efficacy, and metacognitive skills [11]. Among these concepts, self-awareness and metacognitive skills are particularly prominent and widely used in rehabilitation [12]. Self-awareness refers to the ability to recognize one’s own symptoms, understand their impact on various aspects of life, and anticipate when problems may occur [13, 14]. Self-awareness is also related to metacognitive skills, referring to a person’s ability to anticipate the possibility of failure prior to a performance, monitor one’s behaviour during the performance (i.e., self-monitoring), and adjust one’s behaviour to correct problems (i.e., self-regulation) [15, 16]. The aspects of metacognitive skills include multiple self-coping used during complex actions (e.g., problem-solving). For example, in situations that differ from the routine, success is dependent on the person’s ability to perceive what is different, monitor their performance in response to the change, determine a strategy, and execute that strategy. Kennedy and Coelho [17] reported self-regulation as an ongoing relationship between metacognitive beliefs/knowledge, self-monitoring, self-control, and strategy execution. Many people with brain injuries show declines in these metacognitive skills, reducing their achievements in daily living and social activities [18, 19]. Although the need for metacognitive skills has been suggested [10], specific aspects of those for employment have not been studied, and only a few studies have specifically compared them with a control group, such as non-employed people.
We therefore examined whether differences in demographic data, cognitive function, and self-regulation skills exist between employed and non-employed people with brain injuries. In addition, using the mixed research method, self-regulation skills, considered to be key elements to be improved in rehabilitation, were qualitatively analysed using semi-structured interview responses. Our findings may provide suggestions for rehabilitation of the functions needed for employment, allowing for the development of guidelines for targeted behaviours in vocational rehabilitation for people with brain injuries.
This study aimed to examine whether differences in cognitive functions and self-regulation skills exist between employed and unemployed people with brain injuries. Additionally, we aimed to identify specific self-regulation skills characteristic of employed people through qualitative assessment.
2Methods
2.1Setting
This was a cross-sectional observational study, and the information was collected through face-to-face interviews. Participants living in the community were recruited with the cooperation of four facilities: a hospital providing outpatient rehabilitation, a long-term care rehabilitation facility, a day-care welfare facility of care insurance, and a consultation service facility. Interviews and assessments were conducted at each facility, and in all facilities, the patients had the ability to habitually attend the facility on their own. In each facility, one research collaborator, who was not involved in data analysis, widely recruited the participants. The first or second author showed the contents of the research protocol to each participant who applied, and obtained written informed consent from all the participants. Interviews and assessments were conducted by occupational therapists, each with at least 5 years of experience, who were providing support to the participants at each facility.
Data was collected from January 2020 to June 2022, but was suspended between August 2020 and March 2022 because of the COVID-19 pandemic.
2.2Participants
We recruited participants with brain injury who were no longer in the acute phase to reduce symptom fluctuations and psychological burden on the participants. In Japan, people in the post-acute phase are those living in the community after several months of hospitalisation. Furthermore, since the maximum age for job seekers in Japan is often set at 65 years, we targeted people under 65 years. Participants who met the following criteria were included in the study: a history of brain injury or being diagnosed by doctors as having cognitive impairments, at least 6 months have passed following brain injury, aged under 65 years, have language comprehension ability to understand and respond to questions, could attend facilities independently, and could provide informed consent. The exclusion criteria were physical impairments and issues that prevented participation in the interview. The sample size was targeted at 40, which was the estimated number of participants who could be administered at the collaborating institutions during the study period.
2.3Measurement
2.3.1Demographic data
Demographic data on age, sex, diagnosis, number of months since onset or injury, and employment status were collected from facilities information records.
2.3.2Neuropsychological tests
Table 1
Interview items of the SRSI
| Screening question: “Think about the various ways that you may have changed since your injury. Can you tell me one aspect of yourself that has changed which causes you the most distress and holds you back in everyday living?” |
| 1. Emergent awareness: “Can you tell me how you know that you experience (main difficulty); that is, what do you notice about yourself?” |
| Prompt: “What else might you notice?”; “So far, you’ve told me ... , is there anything else?” |
| 2. Anticipatory awareness: “When are you most likely to experience (main difficulty), or, in which situations does it mainly occur?” |
| Prompt: “In what other situations would you expect more or greater (main difficulty)?”; |
| “So far, you’ve told me..., can you think of anything else?” |
| 3. Motivation to change: “How motivated are you to learn some different strategies to help overcome (main difficulty)?” (Encourage self-grading on a scale of 0 to 10) |
| 4. Strategy awareness: “Have you thought of any strategies that you could use to help cope with your (main difficulty)?” and “What are they?” |
| Prompt: “What else could you try that might help?”; “So far, you’ve told me..., can you think of any other strategies?” |
| 5. Strategy use: “What strategies are you currently using to cope with your (main difficulty)?” |
| Prompt: “Can you think of anything else that you are currently using or have tried recently?”; “So far you have said......., are there any other strategies you are using?” |
| 6. Strategy effectiveness: “How well do the strategies that you are using for (main difficulty) work for you?” |
| Prompt: “How do you know that they are helpful/unhelpful?”; “Would you notice any difference if you stopped using the strategies?” |
Item citation from Miyahara et al. 2012(The original version was developed by Ownsworth et al. 2000).
Standardised neuropsychological tests were performed to assess the memory function and the executive function at each facility, which took approximately 1 hour.
1) Rivermead behavioural memory test (RBMT) [20, 21] The RBMT was used to assess various aspects of memory function, including disorientation, short-term memory, long-term memory, prospective memory, and delayed recall. The original version was developed by Wilson et al. [20], and a Japanese version was prepared by Kazui et al. [21]. It includes 11 item questions and required approximately 30 minutes. In a study involving 478 participants with brain injuries and 199 participants without brain injuries in Japan, the RBMT demonstrated high parallel-form reliability, interrater reliability, and correlations with other memory tests [21]. The results are scored using the total screening and standard profile scores. The screening score of each item is converted from a bare score to a score of 1 if the score is perfect and 0 if otherwise. The standard profile score of each item is converted into three levels from 0 to 2 points, considering the difficulty of the lower-level examination. In this study, standard profile scores were used for analysis. The age cut-off points were set at 19/20 points for those aged≤39 years, 16/17 points for those aged 40–59, and 15/16 points for those aged≥60 years [21].
2) Behavioural assessment of the dysexecutive syndrome (BADS) [22, 23] The BADS can assess executive function, which is the ability to make judgments and plan actions in consideration of efficiency and arrangements. The original version was developed by Wilson et al. [22], and a Japanese version was prepared by Kashima et al. [23]. It consists of six different sub-tests using cards and tools and requires approximately 30 minutes. Twenty-six participants in Japan were included in a previous study, and inter-rater reliability and test-retest reliability were confirmed. Additionally, a significant difference in scores was depicted between 92 participants with neurological disease and those without [23]. It comprises six items, each of which has a calculated profile score of 0 to 4. The sum of the resulting profile scores is converted to an age-corrected standardised score [23]. In this study, standard scores were used for analysis.
2.3.3Self-efficacy and self-regulation skills
The self-efficacy and self-regulation skills were assessed using standardised tools at each facility, which took approximately 30 minutes.
1) General self-efficacy scale (GSES) [24] Using the GSES, developed for the Japanese people, participants can self-evaluate whether they are able to perform occupations and whether they contribute to their society [24]. Test-retest reliability, within-item reliability, and high correlations with other self-efficacy tests were confirmed in a study including 121 Japanese university students. Additionally, a significant difference in scores was observed between participants with depressive symptoms [24]. The GSES comprises 16 questions, to which the participant answers ‘yes’ or ‘no’ using a 2-point scale. The results have a score ranging from 0 to 16, with higher scores indicating higher self-efficacy. The sum of raw scores is converted to standardised scores [24]. In this study, standard scores were used for analysis.
2) Self-regulation skills interview (SRSI) [25, 26] (Table 1)
The SRSI can assess the participant’s self-regulation skills through semi-structured interviews. The original version was developed by Ownsworth et al. [25], and a Japanese version was prepared by Miyahara et al. [26] (Table 1). In a study involving 31 and 32 participants with and without brain injuries, respectively, the SRSI demonstrated high interrater reliability, significant differences in scores between the two groups, and associations with other methods of assessing self-awareness [26]. The SRSI is designed to measure a range of metacognitive skills, such as self-awareness and self-regulation skills, relating to specific types of everyday difficulties. The participants’ responses are scored according to the guidelines. The semi-structured interview is used to ask participants about the symptoms experienced in daily life, the situations in which they appeared, their motivation to overcome the symptoms, and the coping strategies they employed to manage difficulties based on six questions: 1. Emergent Awareness, 2. Anticipatory Awareness, 3. Motivation to change, 4. Strategy Awareness, 5. Strategy Use, and 6. Strategy Effectiveness. The evaluator scores the responses on a scale of 1 to 10, according to the guidelines for the content, with lower scores indicating higher awareness. In this study, we used two items: Question 1, labelled as ‘Emergent Awareness’, aimed to ask about participants’ awareness of symptoms occurring in daily life, and Question 5, labelled as ‘Strategy Use’, aimed to ask about the strategies to manage these symptoms. In addition to the usual scoring procedure, we originally transcribed all the participants’ responses to a quantitative and qualitative content analysis.
2.4Data analysis
We used an exploratory sequential design within the mixed research method [27]. Demographic data, scores of neuropsychological tests, self-efficacy, and self-regulation skills were analysed quantitatively. In addition, self-regulation skills of SRSI were analysed quantitatively and qualitatively.
2.4.1Quantitative comparison of demographic data and assessment results between the employed and unemployed people
All participants were categorised into those who were employed and those who were unemployed after the interviews were conducted. We defined an employed person as one who is employed by a firm, whether full- or short-time employment. Descriptive statistics were calculated for both groups. Parametric and nonparametric tests were performed for normally and non-normally distributed data, respectively. SPSS version 28 was used for statistical analysis.
2.4.2Content analysis of the SRSI between employed and unemployed people
In this study, the SRSI responses were analysed using content analysis [28]. Content analysis is a method applicable to both qualitative and quantitative data, involving the transcription and quantification of phenomena to generate new knowledge and insights [28].
1) Quantitative content analysis The verbatim transcripts of the responses to the two SRSI items, ‘Emergent Awareness’ and ‘Strategy Use’, were classified into employed and unemployed groups, and each item was transcribed into a text file for each group. Quantitative text analysis was subsequently conducted using KHCoder software, a computer software widely used for content analysis in Japan [29]. All transcripts are broken down into words, and the frequency of each word was measured. The analysis was conducted for nouns and verbs. The proportion of participants who said a word in the two groups was compared using Fisher’s exact test. The confidence interval was set at 95%, with a two-tailed significance level of 5%.
2) Qualitative content analysis A qualitative content analysis was conducted on words that showed significant differences between the two groups. The KHCoder’s KWIC concordance feature [29] produced lists of sentences and speaker numbers in which each extracted word appeared. We performed open coding of all sentence lists using inductive content analysis [30] and compared them between two groups. Authors 1 and 2 conducted open coding. Author 2 conducted the analysis by blinding the participants to the group to which the statements belonged, and Authors 1 and 2 discussed any differences in content to reach a consensus.
3Results
3.1Participants
Seven facilities were requested to participate in this study, and four of them agreed to participate. Thirty-nine participants applied for this study. One participant who was hospitalised as a result of a fall accident before the interview was excluded. Therefore, data from 38 participants were analysed. Participants regularly attended the facilities and received advice from occupational therapists on daily living and social life. Participants were divided into two groups according to their employment status. Notably, 16 participants were employed, whereas 22 were unemployed.
3.2Demographic data and assessment results between the employed and unemployed groups (Table 2)
Table 2
Demographic data and assessment results for the two groups
| Employment (N = 16) | Non-employment (N = 22) | P-value | Effect size | |
| Age: median (IQR) | 43.0(40.8–48.0) | 45.8(37.5–56.2) | 0.27 | r = 0.18 |
| Sex: males, females (%) | 12(75.0), 4(25.0) | 16(72.7), 6(27.3) | 1.00 | φ= 0.05 |
| Diagnosis: N | ||||
| Traumatic brain injury | 11 | 11 | ||
| Cerebral infarction | 2 | 4 | ||
| Cerebral hemorrhage | 1 | 2 | ||
| Cerebral tumor | 0 | 3 | ||
| Subarachnoid hemorrhage | 0 | 2 | ||
| Hypoxic encephalopathy | 2 | 0 | ||
| Months post-injury: median (IQR) | 42.6(16.0–51.5) | 62.4(18.3–88.5) | 0.55 | r = 0.1 |
| RBMT: median (IQR) | 16.0(6.4) | 15.2(6.6) | 0.68 | r = 0.07 |
| BADS: median (IQR) | 98.3(85.0–108.3) | 91.4(71.8–104.0) | 0.40 | r = –0.08 |
| GSES: mean (SD) | 39.8(9.0) | 44.5(11.6) | 0.84 | d = –0.44 |
| SRSI [Emergent Awareness]: Median (IQR) | 3(3–3) | 6(5–7.3) | < 0.001 | r = 0.82 |
| SRSI [Strategy Use]: Median (IQR) | 3.5(3–5) | 8(6–10) | < 0.001 | r = 0.68 |
SD: standard deviation; IQR: interquartile range; RBMT: Rivermead Behavioural Memory Test; BADS: Behavioral Assessment of the Dysexecutive Syndrome; GSES: General Self-Efficacy Scale; SRSI: Self-Regulation Skills Interview. Two sample test: Comparisons of GSES scores. Mann-Whitney U test: Comparisons of age, months since onset or injury, RBMT, BADS, and SRSI scores. Fisher’s exact test: Comparisons of sex. **: statistically significant difference; P < 0.01.; *: statistically significant difference; P < 0.05. Effect size: r (correlation coefficient) = Z/
A two-sample t-test was performed for GSES scores. The Mann-Whitney U test was performed for age, months since onset or injury, RBMT, BADS, and SRSI scores. The Fisher’s exact test was performed for the sex ratio in the two groups. The significant difference between the employed and unemployed groups was only found in the SRSI score (p < 0.01). No significant differences were found in age, sex, months since onset or injury, RBMT, BADS, and GSES scores.
3.3Content analysis of SRSI between employed and unemployed groups
We measured the frequency of the extracted words for each of the two SRSI items using KHCoder [29] and analysed the words more than 25% of the total number of participants in each group.
3.3.1Quantitative analysis of SRSI between employed and unemployed groups
1) SRSI item ‘Emergent Awareness’ (Fig. 1) The total number of words by the employed group was 150, whereas that for the unemployed group was 87, as the unemployed group had fewer statements. As shown in Fig. 1, the most frequently mentioned word in the employed group was ‘forgetting’, which was mentioned by 75% (n = 12) and 32% (n = 7) of the participants from the employed and unemployed groups, respectively. The second most frequently mentioned word in the employed group was ‘multiple’, which was mentioned by 50% (n = 8) and 9% (n = 2) of the participants from the employed and unemployed groups, respectively. In the unemployed group, no words were mentioned by more than half (50% [n = 11]). The words ‘buying’ (31% [n = 5]) and ‘people’ (25% [n = 4]) were mentioned only in the employed group, whereas the word ‘myself’ (27% [n = 6]) was mentioned only in the unemployed group.
Words that were significantly more frequent in the employed group than in the unemployed group were ‘forgetting’ (p = 0.02), ‘multiple’ (p < 0.01), ‘buying’ (p < 0.01), and ‘people’ (p = 0.02). In contrast, a word that was significantly more frequent in the unemployed group was ‘myself’ (p = 0.03).
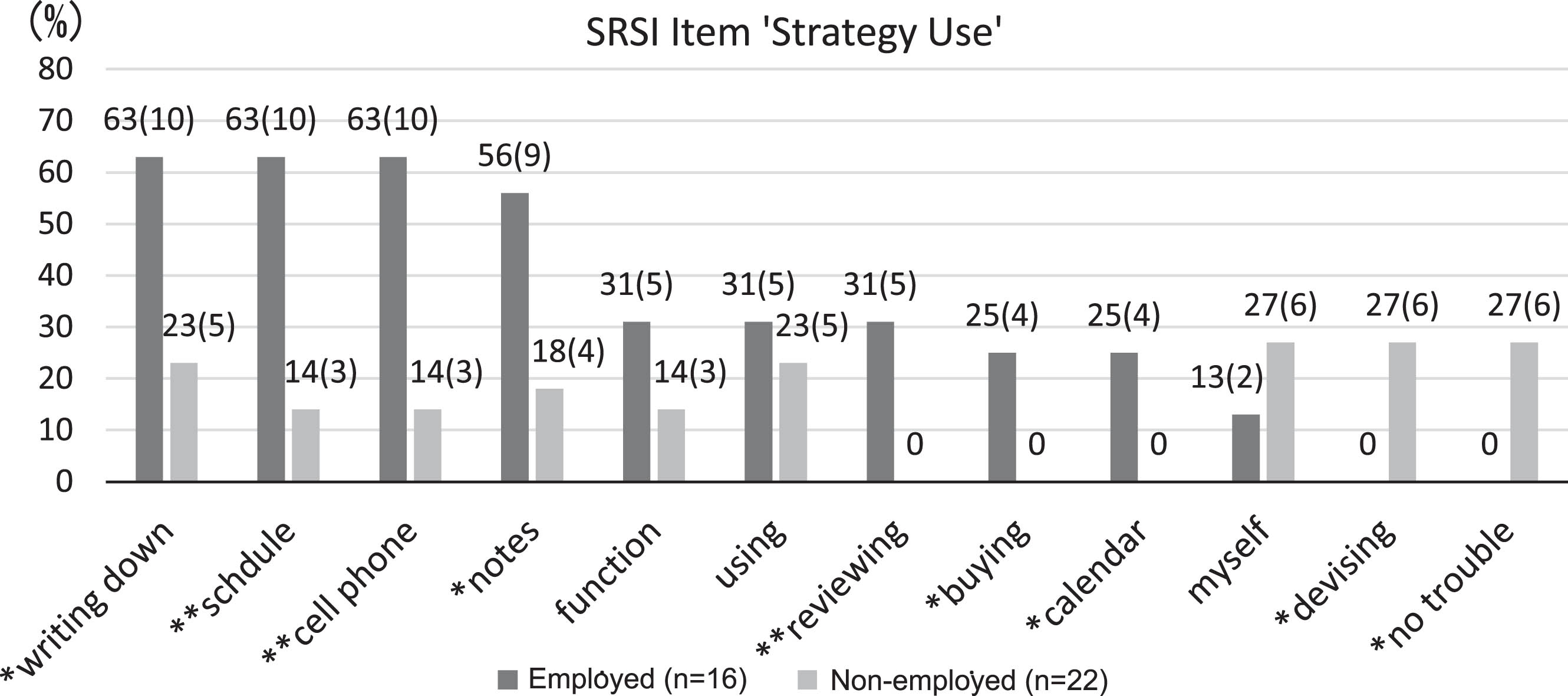
2) SRSI item ‘Strategy Use’ (Fig. 2)
The total number of words by the employed group was 133, whereas that by the unemployed group was 82, with the unemployed group having fewer statements. As shown in Fig. 2, the most frequently mentioned words in the employed group were ‘writing down’, ‘schedule’, ‘cell phone’ (63% [n = 10]), and ‘notes’ (56% [n = 9]). These words often appeared in the same sentence, for example: ‘writing down my schedule in the note application of my cell phone’. In the unemployed group, no words were mentioned by more than half (50% [n = 11]). The words mentioned only in the employed group were ‘reviewing’ (31% [n = 5]), ‘buying’ (25% [n = 4]), and ‘calendar’ (25% [n = 4]). The words mentioned only in the unemployed group were ‘devising’ (27% [n = 6]) and ‘no trouble’ (27% [n = 6]).
Words that were significantly more frequent in the employed group were ‘writing down’ (p = 0.02), ‘schedule’ (p < 0.01), ‘cell phone’ (p < 0.01), ‘notes’ (p = 0.02), ‘reviewing’ (p < 0.01), ‘buying’ (p = 0.02), and ‘calendar’ (p = 0.02). Significantly more frequently used words in the unemployed group were ‘devising’ (p = 0.03) and ‘no trouble’ (p = 0.03).
Fig. 1
Comparison of word rates of “Emergent Awareness” in the two groups. Data represent participants’ rates (n). All transcripts are broken down into words, frequency of each word was measured. The proportion of participants who said words in the two groups was compared using Fisher’s exact test. The confidence interval was set at 95% with a two-tailed significance level of 5%. **: statistically significant difference, P < 0.01. *: statistically significant difference, P < 0.05.
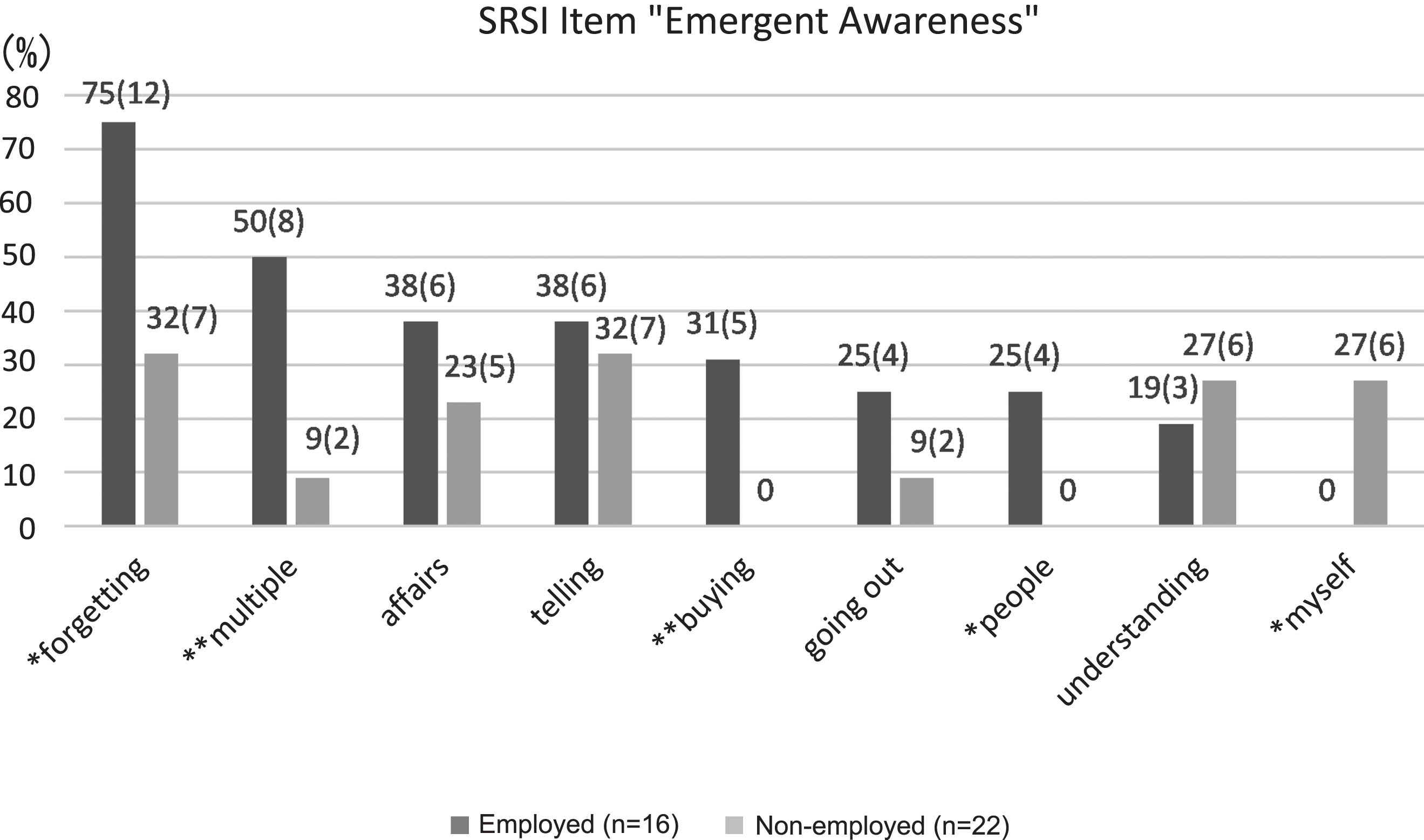
Fig. 2
Comparison of word rates of “Strategy Use” in the two groups. Data represent speaker’s rates (n). All transcripts are broken down into words, frequency of each word was measured. The proportion of participants who said words in the two groups was compared using Fisher’s exact test. The confidence interval was set at 95% with a two-tailed significance level of 5%. **: statistically significant difference, P < 0.01. *: statistically significant difference, P < 0.05.
3.3.2Qualitative analysis of SRSI between employed and unemployed groups (Tables 3 and 4)
Words with significant differences in numbers between the two groups were analysed with the open coding method. Tables 3 and 4 show the results of categorising the statements into categories and words.
1) SRSI item ‘Emergent Awareness’ (Table 3)
‘Forgetting’ was the most frequently mentioned word in both groups. The number statement category of ‘forgetting’ in the employed group was eight, whereas that in the unemployed group was three. The categories ‘failure of prospective memory’ and ‘cannot remember the episodes’ were found in both groups. The unemployed group showed only one additional category, which was ‘cannot remember details’. In contrast, the employed group showed five additional categories of specific episodes of forgetting, for example, ‘when having more than one errand, forgetting it’ and ‘when trying to do it fast, forgetting one of those’. Both the number of speakers and categories were higher in the employed group than in the unemployed group.
(a) Example of the employed group, Participant No. 4 (Pt. 4): ‘When asked to wash non-routine items in addition to routine laundry, I forget to do so. I forget to do my non-routine appointments’.
(b) Example of the unemployed group, Pt. 25: ‘I forget to do errands that I am told to do’.
The second most frequently mentioned word in the employed group was ‘multiple’. The number of coded categories of statements in both groups was two, but more participants in the employed group used this word.
(a) Example of the employed group, Pt. 4: ‘When I do multiple errands, I forget the one I have been doing’.
(b) Example of the unemployed group, Pt. 22: ‘I am not good at doing multiple errands at the same time’.
Words that appeared only in the employed group. The word ‘buying’ was mentioned only by the employed group, such as ‘forgetting what to buy’.
(a) Example of the employed group, Pt. 4: ‘I go shopping and forget what to buy. It takes me a long time to find what I want to buy at a store’.
(b) Pt. 5: ‘I forget what to buy when I buy more than one thing’.
Words that appeared only in the unemployed group. The word ‘myself’ appeared only in the unemployed group. The number of coded categories of statements was three. They meant ‘not feeling any symptoms that interfere with my life’.
(a) Example of the unemployed group, Pt. 18: ‘My wife tells me my memory is declining, but I’m not having much trouble myself’.
(b) Pt. 22: ‘I have no problems in my daily life’.
2) SRSI item ‘Strategy Use’ (Table 4)
The words ‘writing down’, ‘schedule’, ‘cell phone’, and ‘notes’ often appeared in the same sentence, for example: ‘writing down my schedule in the note application of my cell phone’. The number of statements and coded categories was higher in the employed group. The number of coded categories of ‘writing down’ in the unemployed group showed only one category ‘writing down in a note’, but the employed group also presented the perspective of how the participants wrote, such as ‘devising a way to write down in notes’, ‘keeping a consistent place to put notes’ in five categories. Likewise, for the word ‘schedule’, the unemployed group showed only two categories: ‘writing schedules on the cell phone’ and ‘checking schedules ahead’. However, the employed group added the categories ‘looking back on appointments that have been made’, ‘writing down as soon as having a schedule’, ‘focusing on one note to write down’, and ‘telling around people about plans’ in six categories.
(a) Example of the employed group, Pt. 4: ‘When shopping, if I have enough time, I write down the order in which I buy’.
(b) Pt. 5: ‘I try to be creative in the way I take notes, and I write them with the proper (necessary) wording’.
(c) Pt. 8: ‘As soon as I have an appointment, I write it on the calendar. I put notes in the card holder which I always carry with me as soon as I write them’.
(d) Example of the unemployed group, Pt. 27: ‘I write my daily errands in my notebook’.
Words that appeared only in the employed group. The words ‘reviewing’, ‘buying’, and ‘calendar’ appeared only in the employed group. ‘Reviewing’ meant looking back on their own performances and plans.
(a) Example of the employed group, Pt. 2: ‘I write my time schedule on a page for each day. What did I do today? I review what I did all day. I check the schedule for the next day’.
(b) Pt. 4: ‘I review at the notes when I get home’.
(c) Pt. 5: ‘I write notes as soon as a noteworthy event occurs and write them several times a day and review them’.
Words that appeared only in the unemployed group. The words ‘devising’ and ‘no trouble’ only appeared in the unemployed group. All six participants in the unemployed group said, ‘I am not troubled by symptoms, so I did not devise a way to deal with it’.
(a) Example of the unemployed group, Pt. 30: ‘I have no problems in my daily life, so I don’t make any efforts’.
Table 3
Qualitative content of the SRSI responses; Item ‘Emergent Awareness’
| Categories from words | |||
| Word ⌈forgetting⌋ | |||
| Employed group | Pt No. | Non-employed group | Pt No. |
| • failure of prospective memory | 4, 8 | • failure of prospective memory | 25 |
| • cannot remember the episodes | 6, 7, 10, 15 | • cannot remember the episodes | 19, 26, 28, 33, 34, 38 |
| • failure of routines | 4, 16 | • cannot remember details | 25, 26 |
| • failure of non-routines | 3, 5 | ||
| • when having more than one errand, forgetting it | 4, 5, 11, 12 | ||
| • leaving something behind | 1, 8, 11, 16 | ||
| • forgetting what to bring | 6, 7, 10, 12, 15 | ||
| • when trying to do it fast, forgetting one of it | 6 | ||
| Word ⌈multiple⌋ | |||
| Employed group | Pt No. | Non-employed group | Pt No. |
| • cannot do multiple errands at the same time | 2, 3, 4, 5, 10, 11, 13, 14 | • cannot do multiple errands at the same time | 22 |
| • always running multiple errands | 14 | • being tired by conversations with more than one person | 24 |
| Word ⌈buying⌋ | |||
| Employed group | Pt No. | Non-employed group | Pt No. |
| • forgetting what to buy | 4, 5, 6 | none | |
| • buying the same goods twice | 15, 16 | ||
| • time-consuming to buy | 4 | ||
| Word ⌈people⌋ | |||
| Employed group | Pt No. | Non-employed group | Pt No. |
| • Cannot remember people’s names and faces | 1 | none | |
| • Cannot remember the content of conversations with others | 1 | ||
| • Having difficulty in communicating with others | 9, 13 | ||
| Word ⌈myself⌋ | |||
| Employed group | Pt No. | Non-employed group | Pt No. |
| None | • not feeling any symptoms that interfere with my life | 18, 20, 22, 30 | |
| • cannot initiate actions without someone pointing it out to them | 31 | ||
| • alone in family conversations | 33 | ||
From the responses of the SRSI, words with significant differences in word counts between the two groups were categorised. For each word, sentences with similar contents were grouped as ‘category’. Within these categories, the content and participant numbers were compared. Pt No.: Participants in the employment group were designated by numbers 1–16, whereas those in the non-employment group were designated by numbers 17–38, totaling 38 participants
Table 4
Qualitative content of the SRSI responses; Item ‘Strategy Use’
| Categories from words | |||
| Word ⌈writing down⌋ | |||
| Employed group | Pt No. | Non-employed group | Pt No. |
| • writing down in a note | 2, 3, 4, 5, 6, 7, 16 | • writing down in a note | 21, 23, 24, 37, 38 |
| • devising a way to write down in notes | 2, 6, 4, 5, 6, 8, 11, 16 | ||
| • keeping a consistent place to put notes | 8 | ||
| • reviewing the notes | 4 | ||
| • organizing thoughts by writing | 9 | ||
| Word ⌈schedule⌋ | |||
| Employed group | Pt No. | Non-employed group | Pt No. |
| • writing schedules on the cell phone or the notebook | 2, 3, 6, 7, 12, 15, 16 | • writing schedules on the cell phone | 23, 31, 33 |
| • checking schedules ahead | 1, 2, 15 | • checking schedules ahead | 33 |
| • looking back on appointments that have been made | 2, 8 | ||
| • writing down schedules as soon as having them | 5, 8 | ||
| • focusing on one note to write down | 8 | ||
| • telling around people about plans | 12 | ||
| Word ⌈cell phone⌋ | |||
| Employed group | Pt No. | Non-employed group | Pt No. |
| • using the cell phone’s scheduling function | 1, 3, 4, 5, 6, 15, 16 | • using the cell phone’s scheduling function | 23, 33 |
| • checking the cell phone every day | 1, 5, 16 | • checking the cell phone every day | 33 |
| • using functions other than scheduling | 1, 7, 10, 15 | • using functions other than scheduling | 27 |
| • inputting schedules as soon as having them | 5 | ||
| • displaying the schedule on the top screen of the cell phone | 15 | ||
| • using the cell phone and the notes properly | 6, 11 | ||
| Word ⌈notes⌋ | |||
| Employed group | Pt No. | Non-employed group | Pt No. |
| • taking notes | 4, 8, 11 | • taking notes | 25, 27, 34 |
| • devising note-taking methods | 5, 16 | • not taking notes in the daily living | 21, 25, 27 |
| • consolidating where notes are placed | 7, 10, 15 | ||
| • checking notes repeatedly | 5 | ||
| • making a to-do list and checking when finished | 15 | ||
| • using the cell phone and the notes properly | 6, 11 | ||
| Word ⌈reviewing⌋ | |||
| Employed group | Pt No. | Non-employed group | Pt No. |
| • reviewing performances every day | 2, 4, 5, 8 | none | |
| • reviewing behaviours before getting angry | 9 | ||
| Word ⌈buying⌋ | |||
| Employed group | Pt No. | Non-employed group | Pt No. |
| • writing what to buy in a note | 1, 8 | none | |
| • writing the order to buy in a note | 4, 11 | ||
| Word ⌈calendar⌋ | |||
| Employed group | Pt No. | Non-employed group | Pt No. |
| • writing schedules on the calendar | 2, 12 | none | |
| • writing appointments only on the calendar | 8 | ||
| • writing schedules as soon as having an appointment | 8 | ||
| • using the cell phone and the calendar properly | 16 | ||
| Employed group | Pt No. | Non-employed group | Pt No. |
| Word ⌈devising⌋ | |||
| Employed group | Pt No. | Non-employed group | Pt No. |
| none | • having no trouble and not devising a way to deal with it | 18, 20, 22, 28, 30, 36 | |
| Word ⌈no trouble⌋ | |||
| Employed group | Pt No. | Non-employed group | Pt No. |
| none | • having no trouble and not devising a way to deal with it | 18, 20, 22, 28, 30, 36 | |
From the responses of the SRSI, words with significant differences in word counts between the two groups were categorised. For each word, sentences with similar contents were grouped as ‘category’. Within these categories, the content and participant numbers were compared. Pt No.: Participants in the employment group were designated by numbers 1–16, whereas those in the non-employment group were designated by numbers 17–38, totaling 38 participants.
4Discussion
4.1Difference in demographic data and assessment results between the employed and unemployed people
The results of quantitative data showed no significant differences in demographic data and neuropsychological assessments between the employed and unemployed groups. This could be attributed to the fact that participants attending each facility were independent in performing daily activities and attending on their own. Consequently, participants with a certain level of cognitive function may have been selected.
Notably, the only significant difference between employed and unemployed people was observed in the SRSI scores. This implies that self-regulation skills are related to employment, even if there are no differences in cognitive functioning. In a previous study, Wise et al. [31] investigated the relationship between employment status and self-perception and found an association between SRSI scores and employment. Additionally, Douglas et al. [32] investigated self-perceptions focused on communication skills and found that unemployed people perceived less disability, whereas employed people observed their difficulties more frequently. The results of this study also support these previous research findings, suggesting that improving metacognitive skills is effective for employment. Notably, as the sample size of this study was small, examining the effects of multiple variables with a larger sample size and multivariate analysis is necessary.
4.2Specific features of self-regulation in both groups using the content analysis
In this study, we have exploratively identified specific aspects of self-regulation skills characteristic of two groups using content analysis of SRSI. The total number of statements was higher in the employment group for both symptom recognition and coping strategies. The SRSI item ‘Emergent Awareness’ indicates self-awareness of disorders. Specifically, many participants in the employed group recognised more specific and practical symptoms than the unemployed group about ‘forgetting’ and ‘multiple’. For example, participants in the employed group were able to describe specific situations related to ‘forgetting’, whereas those in the unemployed group stated only the fact, such as ‘I forget to do errands’.
The SRSI item ‘Strategy Use’ indicates self-regulation. Specifically, the participants in the employed group reported that they had coped with those symptoms using ingenious strategies realistically. The unemployed group only presented the category ‘writing down in a note’, but the employed group added the perspective of how to use strategies effectively.
Notably, participants in the employed group exhibited the habit of ‘reviewing’ their performances, which was not observed in the unemployed group. In the metacognitive system, self-regulation skills require constant monitoring and adjustment of one’s behaviour to suit the current situation at hand [11, 13–15]. ‘Reviewing’ could be the key action for self-monitoring that leads employees to recognize their symptoms and improve their behaviour, thereby fostering their ability to work independently. People with brain injuries often have difficulty in recognizing and coping with the problems at hand [11, 13–14,19]. These skills are difficult to generalize across multiple situations, and many reports have advocated that self-regulation skills should be improved under each occupational situation [18, 19, 33–34].
The words ‘myself’, ‘devising’, and ‘no trouble’ were used only in the unemployed group in statements such as ‘I don’t have any problems in my life, so I haven’t devised ways to deal with them’. This suggests that getting employment is difficult if one does not have any self-awareness about one’s own symptoms.
Although several reports have revealed the association between employment and self-regulation skills [2, 10], few studies have explicitly provided detailed insights, such as our study. This study provides novel insights for the development of rehabilitation techniques. The relationship between employment and self-regulation skills should be further researched, and specific guidelines for self-regulation skills needed in vocational rehabilitation should be developed.
4.3Limitations of the study and scope for future research
The sample size of this study was small, and participants were recruited from limited areas in Japan. In addition, the sampling process was not randomised, which may have resulted in a bias in the selection of the participants. In the future, we aim to verify whether the present results are also applicable to a broader range of participants. Additionally, since more symptoms may occur in the workplace, coping behaviours in various situations should also be investigated.
Furthermore, this study did not consider the duration of employment as an influencing factor for the participants in the employed group. People with brain injuries face challenges not only in returning to work or getting work but also in maintaining employment. Hence, further investigation is needed to explore how participants’ self-perception differs depending on employment duration.
5Conclusion
Employment for people with brain injuries is often challenging, and clarifying the factors that promote employment and establishing specific techniques for vocational rehabilitation are crucial.
We examined whether differences exist in demographic data, cognitive function, and self-regulation skills between employed and non-employed people with brain injury living in the community in Japan. We also conducted a qualitative analysis of SRSI for self-regulation skills using the mixed research method.
The results showed no significant differences in demographic data and neuropsychological tests between the two groups, but employed participants showed significantly better self-regulation skills according to their SRSI scores than unemployed participants. The qualitative content analysis showed that employed participants recognised more ‘specific’ symptoms occurring in their lives than unemployed participants. For example, ‘when having more than one errand, forgetting it’, and ‘when trying to do it fast, forgetting one of those.’ In contrast, the non-employed people only stated ‘failure of prospective memory’ and ‘cannot remember the episodes’. Further, the unemployed participants mentioned only two coping-related categories ‘writing schedules on the cell phone’ and ‘checking schedules ahead’; however, the employed participants presented the categories ‘looking back on appointments that have been made’, ‘writing down as soon as having a schedule’, and ‘focusing on one note when writing it down’. Moreover, a statement ‘reviewing performances every day’, as a strategy to deal with ‘forgetting’ only appeared in the employment group.
Our results imply that self-regulation skills are related to employment if there are no differences in cognitive functions, and that employed people could recognize more specific symptoms and develop ingenious coping strategies in their lives. This study contributes novel perceptions for the development of rehabilitation techniques for people with brain injuries. The relationship between employment and self-regulation skills should be further researched, as specific guidelines for self-regulation skills need further development.
Ethical approval
This study was conducted in accordance with the Declaration of Helsinki and in compliance with the Ethical Guidelines for Life Sciences and Medical Research Involving Human Subjects. Approval to conduct the study was obtained from the Ethics Review Committee of the Nittazuka Medical Welfare Center (2019-18). The long-term care rehabilitation facility and the day-care welfare facility of care insurance did not have their own ethics review committee structure; prior to the start of the study, the director of each facility and an outside research expert reviewed the common research protocol for this study to ensure that there were no ethical issues.
Informed consent
The authors provided a written explanation of the study to participants. After the written consent were obtained from the participants, data collection began.
Acknowledgments
We would like to acknowledge all participants who participated in this study. We would also like to acknowledge all the facility managers and staff who recruited and interviewed the participants.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Funding
This research project was funded by the 49th Mitsubishi Foundation Social Welfare Program and Research Grant (FY2018) and the JR-West Relief Foundation (FY2023).
References
[1] | Karcz K , Trezzini B , Escorpizo R , Schwegler U , Finger M . Factors associated with sustaining work after an acquired brain injury: a scoping review. Disabil Rehabil. (2022) ;44: (21):6510–30. doi: 10.1080/09638288.2021.1960439. |
[2] | Ownsworth T , McKenna K . Investigation of factors related to employment outcome following traumatic brain injury: a critical review and conceptual model. Disabil Rehabil. (2004) ;26: (13):765–83. doi: 10.1080/09638280410001696700. PMID: 15371049 |
[3] | Thor JA , Mazlan M , Waran V . Employment status after traumatic brain injury and the effect of concomitant injuries on return to work. Brain Inj. (2021) ;35: (8):949–56. doi: 10.1080/02699052.2021.1934729. |
[4] | Vestling M , Tufvesson B , Iwarsson S . Indicators for return to work after stroke and the importance of work for subjective well-being and life satisfaction. J Rehabil Med. (2003) ;35: (3):127–31. doi: 10.1080/16501970310010475. PMID: 12809195 |
[5] | Simpson GK , McRae P , Gates TM , Daher M , Johnston D , Cameron ID . A vocational intervention that enhances return to work after severe acquired brain injury: A pragmatic trial. Ann Phys Rehabil Med. (2023) ;66: (8):101787. doi: 10.1016/j.rehab.2023.101787. Epub ahead of print. PMID: 37890426 |
[6] | Singh R , Dawson J , Basu S , Humphries TJ , Mason S , Lecky F . Vocational outcomes after traumatic brain injury; prevalence and risk factors after 1 year in a multivariable model. J Head Trauma Rehabil. (2022) ;37: (2):104–13. doi: 10.1097/HTR.0000000000000687. |
[7] | Fure SCR , Howe EI , Andelic N , Brunborg C , Olsen A , Rike PO , et al. Workplace factors associated with return to work after mild-to-moderate traumatic brain injury. J Head Trauma Rehabil. (2023) ;38: (1):E1–9. doi: 10.1097/HTR.0000000000000772. |
[8] | DiSanto D , Kumar RG , Juengst SB , Hart T , O’Neil-Pirozzi TM , Zasler ND , et al. Employment stability in the first 5 years after moderate-to-severe traumatic brain injury. Arch Phys Med Rehabil. (2019) ;100: (3):412–21. doi: 10.1016/j.apmr.2018.06.022. |
[9] | Grauwmeijer E , Heijenbrok-Kal MH , Haitsma IK , Ribbers GM . Employment outcome ten years after moderate to severe traumatic brain injury: A prospective cohort study. J Neurotrauma. (2017) ;34: (17):2575–81. doi: 10.1089/neu.2016.4846. |
[10] | Frostad Liaset I , Lorås H . Perceived factors in return to work after acquired brain injury: A qualitative meta-synthesis. Scand J Occup Ther. (2016) ;23: (6):446–57. doi: 10.3109/11038128.2016.1152294. |
[11] | Schmidt J , Ownsworth T . Special issue editorial: The self after brain injury. Neuropsychol Rehabil. (2022) ;32: (8):1669–1675. doi: 10.1080/09602011.2022.2120504. |
[12] | Al Banna M , Redha NA , Abdulla F , Nair B , Donnellan C . Metacognitive function poststroke: A review of definition and assessment. J Neurol Neurosurg Psychiatry. (2016) ;87: (2):161–6. doi: 10.1136/jnnp-2015-310305. |
[13] | Toglia J , Kirk U . Understanding awareness deficits following brain injury. NeuroRehabilitation. (2000) ;15: (1), 57–70. |
[14] | Crosson B , Barco P , Velozo CA , Bolesta MM , Cooper PV , Werts D , et al. Awareness and compensation in postacute head injury rehabilitation. J Head Trauma Rehabil. (1989) ;4: (3):46–54. doi: 10.1097/00001199-198909000-00008. |
[15] | Al Banna M , Redha NA , Abdulla F , Nair B , Donnellan C . Metacognitive function poststroke: A review of definition and assessment. J Neurol Neurosurg Psychiatry. (2016) ;87: (2):161–6. doi: 10.1136/jnnp-2015-310305. |
[16] | Ownsworth T , Fleming J , Desbois J , Strong J , Kuipers P . A metacognitive contextual intervention to enhance error awareness and functional outcome following traumatic brain injury: A single-case experimental design. J Int Neuropsychol Soc. (2006) ;12: (1):54–63. doi: 10.1017/S135561770606005X. |
[17] | Kennedy MR , Coelho C . Self-regulation after traumatic brain injury: a framework for intervention of memory and problem solving. Semin Speech Lang. (2005) ;26: (4):242–55. doi: 10.1055/s-2005-922103. |
[18] | Cicerone KD , Langenbahn DM , Braden C , Malec JF , Kalmar K , Fraas M , et al. Evidence-based cognitive rehabilitation: Updated review of the literature from 2003 through 2008. Arch Phys Med Rehabil. (2011) ;92: (4):519–30. doi: 10.1016/j.apmr.2010.11.015. |
[19] | Cicerone KD , Goldin Y , Ganci K , Rosenbaum A , Wethe JV , Langenbahn DM , et al. Response to: can we successfully improve attentional impairments after brain injury with computer-based interventions? Letter to the Editor on “Evidence-Based Cognitive Rehabilitation: Systematic Review of the Literature From 2009 Through 2014”. Arch Phys Med Rehabil. (2022) ;103: (10):2066–7. doi: 10.1016/j.apmr.2022.05.021. |
[20] | Wilson BA , Cockburn J , Baddeley A , Hiorns R . The development and validation of a test battery for detecting and monitoring everyday memory problems. J Clin Exp Neuropsychol. (1989) ;11: (6):855–70. doi: 10.1080/01688638908400940. PMID: 2592527 |
[21] | Kazui H , Watamori S , Honda R , Tokimasa A , Hakuno N , Mori E . The validation of the Japanese version of the Rivermead Behavioral Memory Test-a test for everyday memory- (in Japanese). Adv Neurol Sci. (2002) ;46: (2):307–18. doi: 10.11477/mf.1431901355. |
[22] | Wilson BA , Alderman N , Burgess PW , Emslie H , Evans JJ Behavioral assessment of the dysexecutive syndrome. Bury St Edmunds (UK): Harcourt Assessment; 1996. |
[23] | Kashima H ,editor. Behavioral Assessment of the Dysexecutive Syndrome JapaneseVersion (in Japanese). Tokyo (JP): Shinkoh Igaku Shuppan; 2003. |
[24] | Sakano Y , Tohjoh M . The general self-efficacy scale (GSES): Scale development and validation (in Japanese). Jpn J Behav Ther. (1986) ;12: 73–82. doi: 10.24468/jjbt.12.1_73. |
[25] | Ownsworth TL , McFarland KM , Young RM . Development and standardization of the Self-regulation Skills Interview (SRSI): A new clinical assessment tool for acquired brain injury. Clin Neuropsychol. (2000) ;14: (1):76–92. doi: 10.1076/1385-4046(200002)14:1;1-8; FT076. |
[26] | Miyahara T , Shimizu H , Hanaoka H , Yamane S , Kawahara K , Moriyama K . Development of Self-Regulation Skills Interview in Japan: reliability and validity (in Japanese). Sogo Rehabili. (2012) ;40: (8):1117–26. doi: 10.11477/mf.1552102632. |
[27] | Creswell JW A concise introduction to mixed methods research. London, Thousand Oaks, New Delhi and Singapore: SAGE Publications; 2015. Translated by Kakai H. A concise introduction to mixed methods research (in Japanese). Tokyo (JP): Japan UNI Agency; 2023 |
[28] | Elo S , Kyngäs H . The qualitative content analysis process. J Adv Nurs. (2008) ;62: (1):107–15. doi: 10.1111/j.1365-2648.2007.04569.x. PMID: 18352969 |
[29] | Higuchi K . A two-step approach to quantitative content analysis: KH Coder tutorial using Anne of Green Gables (Part II). Ritsumeikan Social Science Review. (2017) ;53: (1):137–147[accessed May 6,2022]. Available from:https://khcoder.net/license.html. |
[30] | Sato T , Kasuga H , Kanzaki M Mapping of qualitative research. Tokyo (JP): Shinyosha; 2022. |
[31] | Wise K , Ownsworth T , Fleming J . Convergent validity of self-awareness measures and their association with employment outcome in adults following acquired brain injury. Brain Inj. (2005) ;19: (10):765–75. doi: 10.1080/0269905050019977. |
[32] | Douglas JM , Bracy CA , Snow PC . Return to work and social communication ability following severe traumatic brain injury. J Speech Lang Hear Res. (2016) ;59: (3):511–20. doi: 10.1044/2015_JSLHR-L-15-0025. |
[33] | Tate R , Kennedy M , Ponsford J , Douglas J , Velikonja D , Bayley M , et al. INCOG recommendations for management of cognition following traumatic brain injury, part III: executive function and self-awareness. J Head Trauma Rehabil. (2014) ;29: (4):338–52. doi: 10.1097/HTR.0000000000000068. |
[34] | Jeffay E , Ponsford J , Harnett A , Janzen S , Patsakos E , Douglas J , et al. INCOG 2.0 Guidelines for cognitive rehabilitation following traumatic brain injury, part III: Executive functions. J Head Trauma Rehabil. (2023) ;38: (1):52–64. doi: 10.1097/HTR.0000000000000834. |


