
Postural analysis and ergonomic intervention of unorganized workers in indian construction sectors
Abstract
BACKGROUND:
In India’s fast-growing economy, the construction sector offers significant developments with huge employment opportunities but poses risks due to poor working environments and uncomfortable postures. Traditional methods, such as manual material handling, can lead to health hazards and musculoskeletal disorders such as overexertion, low back pain, etc.
OBJECTIVE:
The purpose of this study was to analyze the working postures of unorganized employees engaged in residential buildings using Ergofellow software and to recommend changes in their unsafe working postures.
METHODS:
Participants’ working positions were video recorded and the postures were analyzed using Rapid Upper Limb Assessment (RULA), Rapid Entire Body Assessment (REBA) and Ovako Working Posture Analysis (OWAS). Paired sample t-tests were used to analyze significant differences between the RULA and REBA scores after the ergonomic interventions were implemented.
RESULTS:
From the analysis of RULA, REBA and OWAS, the working postures showed a high risk of potential injury and required an immediate change in employees’ working postures. The RULA and REBA scores were subsequently lower after the ergonomic interventions, which were based on ergonomic and safety principles. The paired sample t-tests with p-values of less than 0.05 demonstrated decreased risks after ergonomic interventions.
CONCLUSION:
Working postures of the construction workers exposed to musculoskeletal disorders were examined and the ergonomic interventions were implemented. According to the recommendations, working positions were changed, and employee well-being was enhanced by reduced operational risks.
1Introduction
In both developing and developed countries, business people ensure that workplaces encourage engagement, and academicians and human resource specialists are particularly focused on improving employee performance [1, 2]. The human workforce falls into two categories: organized and unorganized workers. A group of organized workers acts as a single unit to achieve its common objectives. Unorganized labour, on the other hand, refers to workers who are unable to work together due to the nature of their employment, such as bonded labourers, migrant workers and casual labourers in construction, agriculture, etc [3, 4]. In a developing country like India, more than 75 per cent of employees work in unorganized sectors and generate around half of the nation’s GDP [5]. The construction industry is the country’s second-largest industry after agriculture, employing a large number of people in unorganized sectors [6]. Building work relies heavily on manual labour and employs a sizeable workforce with a 10% yearly growth rate [7, 8]. The construction industry comprises multiple hazardous operations such as handling materials, and working on elevated and confined workspaces [9]. Construction workers experience more work-related musculoskeletal disorders and workplace absenteeism than workers in other unorganized sectors [10]. Uncomfortable working postures maintained for a long time combined with repetitive motions result in the development of work-related musculoskeletal disorders (WMSDs) [11, 12]. Previous researchers highlighted that 81% of construction workers experience MSDs and low back pain is the most common hazard among 92% of construction workers [9]. Productivity was prioritized over workers’ health by previous researchers, resulting in a lack of ergonomic recommendations that need to be revised by taking into account workers’ activities [13, 14].
Faster urbanization increased construction activities, but unorganized workers in residential construction are less inspected than in the organized sectors by previous researchers, highlighting the need for further research [15, 16]. It is indeed essential to gain a better understanding of the potential risk factors in each unique occupational group to design appropriate methods for the prevention and management of musculoskeletal disorders [17]. An ergonomic assessment is one of the best ways to identify potential MSDs and design appropriate interventions. [18]. This study therefore focuses on working postures by identifying the potential issues and introducing ergonomic interventions. The main goal of this study was to identify and assess the risks faced by construction workers using the Rapid Upper Limb Assessment (RULA), Rapid Entire Body Assessment (REBA) and Ovako Working Posture Analysis (OWAS). After ergonomic interventions and suggestions for these high-risk postures, the working postures were reassessed and scores were recalculated to determine whether the suggestions were effective or not. The differences in scores were statistically analyzed using paired sample t-tests.
2Methods
2.1Study design
Using literature and workers’ interaction, an initial understanding of the construction industry and the postures that were dangerous to the musculoskeletal system were identified and categorized [19]. After a comprehensive assessment of the literature survey and regular site visits, the construction workers were examined using the technique described below. The approach in this case consisted of two steps. The first step was to collect the working postures by video and still photographs for further analysis. The second step was to separate the very high-risk postures and identify the problematic postures using the tools listed below. Data were collected on residential construction sites located in Chennai, India. The work was initiated with a local mason expert and the availability of the number of workers depended on the nature of work and material availability on the workers’ daily schedule. From February 2021 to June 2021 the working postures were sequentially recorded and analyzed based on the construction work taking place at the time [20].
To analyze occupational risks and other musculoskeletal illnesses, a cross-sectional study was conducted on 52 construction employees from various occupational groups, including concrete workers (30%), masons (8%), loading and unloading (16%), flooring workers (34%) and assistance (12%). The responsibilities of a mason include the manipulation of blocks weighing more than 25 kilograms on average, as well as the installation of over 100 blocks and tiles per day. Carrying blocks weighing more than 25 kilograms, as well as the cement and sacks weighing 50 kilograms, were observed as the loading jobs. Excavation work, sieving sand and gravel, mixing cement, transporting mortar, slurry, block and tiles to the job sites, levelling, and tool handling were all done by labourers. Operations such as tying beams, placing, and cutting rods were included in the reinforcement. Manual transport of steel rods weighing more than 25 kilograms required for reinforcement was also carried out.
The hypothesis tested in this study was:
1 H0 – Null Hypothesis – There is no significant difference between Initial and Final RULA and REBA scores.
2 H1 – Alternate Hypothesis – There is a significant difference between Initial and Final RULA and REBA scores.
2.2Data collection methods
The first step is data collection in any kind of experimental study and there are multiple techniques to collect data, however, self-reporting techniques such as questionnaires are particularly time-consuming [9]. Systematic observation is a well-organized method for obtaining reliable data on examining postures [13]. The direct assessment approach, in contrast, has the advantage of being more precise and reliable than other methods [17]. Recognizing the importance and challenges adopted by previous studies, working postures were collected through video recordings and still photos for analysis. In the recorded videos, working postures were separated into individual frames for analysis [21]. For the identification of high-risk postures, previous researchers highlighted using more than one method for risk assessment [22, 23]. Field observation, followed by assessment techniques such as the Rapid Upper Limb Assessment (RULA), etc. was considered an appropriate strategy for working posture analysis [24, 25]. The Ergo Fellow Software includes the RULA, REBA and OWAS techniques for users to utilize. In this study, observational data collection and postural analysis were carried out.
2.3Ergofellow software
Ergofellow is ergonomic software consisting of tools such as RULA and Rapid Entire Body Assessment (REBA) in which working postures are analyzed [26]. RULA and REBA techniques were preferred over other methods because of the observational technique requiring angular deviations and withstanding load for a long time as input data [6]. Initially from video graphic recordings, the risky postures were segregated and the risk was estimated using RULA and REBA. The amount of load and the holding time were recorded during the site observations. Generally, RULA and REBA were carried out after a detailed collection of video recordings and images of participants’ working postures [3]. RULA and REBA have previously been utilized for postural analysis of water fetching activities by women in rural areas and corrective methods for uncomfortable activities were suggested [12].
2.4Rapid upper limb assessment (RULA)
RULA is a viable and accurate observational method for determining the postures and muscle actions of operators whose repetitive tasks are mainly dependent on the upper limb [3, 27]. Manual material handling (MMH) demands activities such as loading and unloading leading to frequent impact on upper limbs [28]. RULA is an analysis tool for the upper limb of the body and it consists of two kinds of group scores (A& B). Group A comprises the upper arm, lower arm, wrist and wrist twist. Group B comprises the neck, trunk and legs. High repetition of the same process results in muscle fatigue, resulting in reduced muscle ability to generate force [5]. Finally, these scores were collectively used to decide the level of risk which the worker had been experiencing during the task for several days. From the video graphic recording data such as bending followed by angular deviation of arms, bending of the trunk, wrist, etc are applied [29]. The conclusive portion contains muscle use and holding of load for a particular position. Finally, the generated score shows whether the posture is to be investigated immediately or later. RULA varies from REBA in terms of the determination of the five types of risk levels such as negligible risk, low risk, medium risk, high risk and very high risk [30].
2.5Rapid entire body assessment (REBA)
REBA is the most widely used method in various studies [31, 32] and it involves examining the postures of the upper limbs (arm, forearm and wrist), trunk, neck, and lower extremities all at once. Furthermore, it distinguishes the type of grip and muscle activity used [13]. Similar to RULA, REBA also consists of Group A and Group B values. Group A score is calculated for the trunk, neck, and legs and the load values are added together [33, 34, 35]. Group B score is added as an additional parameter [36]. The final estimated value identifies five levels of risk, ranging from negligible to extremely high [12]. The low, medium, high and very high-level risks were separated from the derived observations. REBA also shows the risk level from the scores in which a lower value lessens the urgent situation for inspection in the working postures [24]. REBA was reliable in measuring the risk of musculoskeletal disorders from the previous studies by multiple researchers in different areas [37].
2.6APECS application for angle identification
For RULA and REBA, it is necessary to find the angular position of the body parts during participants’ working hours. It was not feasible to use manual input of the angular positions for all working postures [10], therefore AI Posture Evaluation and Correction System (APECS) software (developed by New Body Technology) was used to determine the body positions required for RULA and REBA assessments [38, 39].
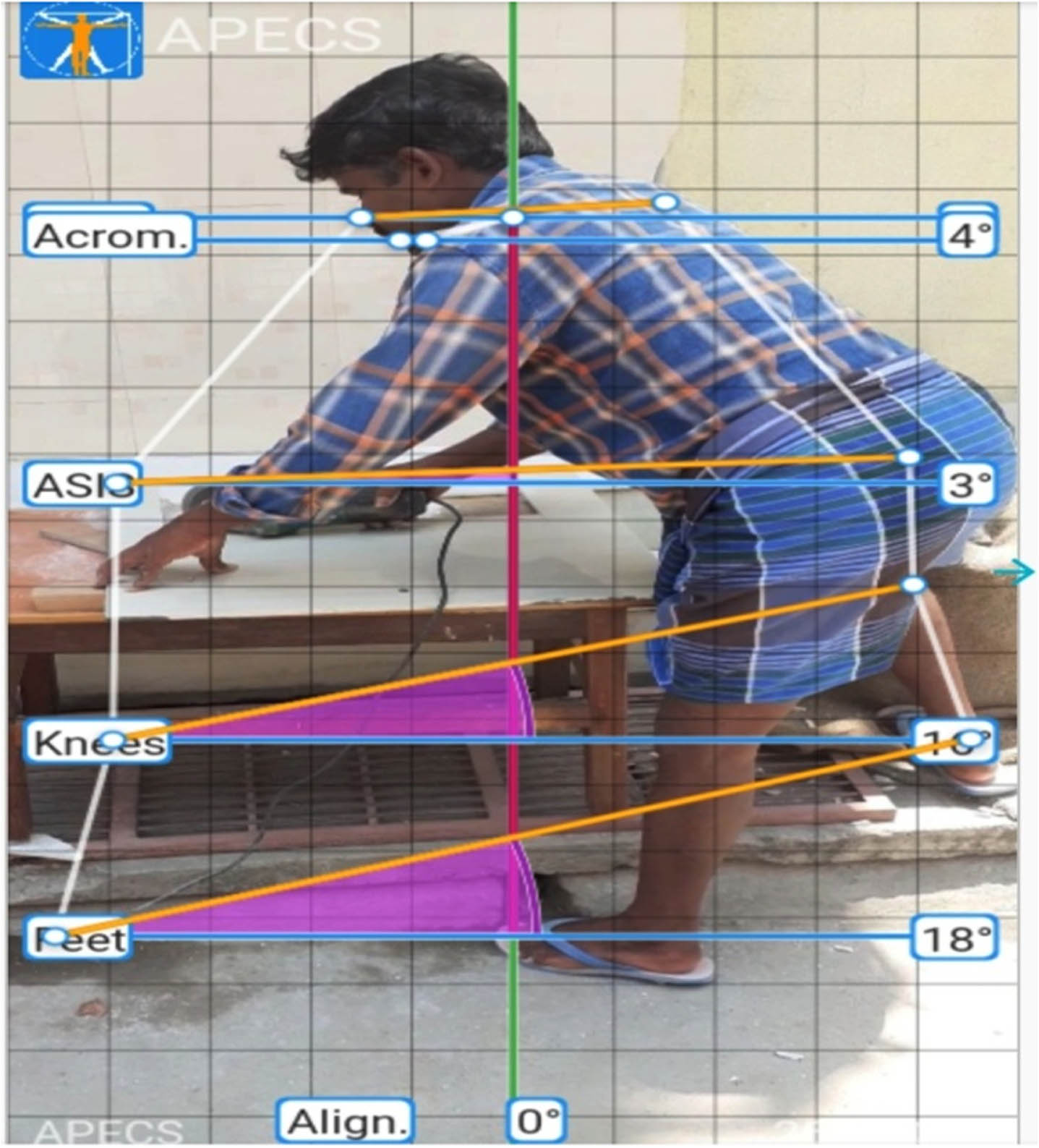
APECS (Version 6.2.00) [38], is an Android mobile application that was used in this study. It allows for identifying the orientation of individual workers in the images used [39]. After uploading the photography, it generates a result for the input values on RULA and REBA tools. The particular angle and body position can be analyzed from both front and side views of the image. A sample image of the workers involved in the flooring operation is displayed in Fig. 1. Anagha et al. [39] used this method to obtain the angle of the complex postures and assess the risk of stances of the building workers.
Fig. 1
Illustration of APECS Application. APECS – AI Posture Evaluation and Correction System.
2.7Ovako working posture analyses (OWAS)
Another common observational tool for assessing the degree of risk for musculoskeletal problems is the Ovako Working Posture Analysis (OWAS) [24]. The most common back positions among workers are identified by OWAS as being 4 postures, 3 postures for the arms, 7 postures for the legs, and 3 categories for the weight of the load carried. Through video recording, risk levels of workers at construction sites were identified and ergonomic measures were offered to lower workplace injury [40]. OWAS requires data such as the position of the back, legs, arms and the amount of load the construction worker is withstanding. By entering these input values, the risk level of the working stance is identified [41]. Similar to RULA and REBA, the working postures were analyzed in the OWAS method and the results were reported.
Finally, all the results of RULA, REBA and OWAS were compared. RULA, REBA and OWAS methods have received numerous citations in pertinent literature, significantly more than any other observational methods [24, 31]. Joshi et al. (2019) observed 18 techniques among which REBA was utilized the most (69%), followed by RULA (64%) and OWAS (33%) [32]. RULA has been utilized in multiple types of research. Similarly, Chatterjee et al. and Jain et al. used RULA to assess the postures of construction workers and suggested remedies after calculating the risk [33, 34].
2.8Data collection and analysis
The data collection process started after obtaining consent from the respective management and the working crew. The routine work was recorded using video cameras. The recorded videos were observed and snapshots of working postures were used for further analysis. Due to the irregular availability of workers during unscheduled working hours, random numbers of workers from different areas were considered for the working sample. Therefore, 52 workers exhibiting different working postures from excavation, masonry work, roofing and flooring activities were prepared for data analysis. It was observed from the individual snapshots that workers were subjected to regular bending, contorting of the body, working above shoulder level and below knee level, lifting and manual handling of irregular loads.
For the sake of upper body assessment, the RULA technique was chosen and for the entire body assessment, the REBA method was preferred. Likewise, OWAS was employed to assess postures with special concern for the duration of individual tasks. RULA and REBA analysis were used to identify high-risk postures, which were then adjusted under ergonomic principles and reassessed and analyzed using paired sample t-tests using the same methodology to see if the alterations lowered the risk. Ergonomic intervention programs were the most well known preventive strategy [33, 42, 43], which boosts productivity by reducing occupational health hazards [19, 44, 45].
2.9Participants
There were 68 construction workers allocated to various jobs at the selected construction site. However due to respective tasks carried out by many people in the same age group, 76% of 68 workers (n = 52) were chosen as the final sample size of this study. In the end, 52 workers who had signed up for the study were involved in the data analysis process after obtaining the workers’ consent. The demographic data of workers are presented in Table 1.
Table 1
Demographic data of workers
| Participants | Min | Max | Mean | Standard Deviation |
| Age (Years) | 18 | 55 | 34.27 | 10.51 |
| Height (cm) | 141 | 182 | 164.94 | 11.28 |
| Weight (kg) | 45 | 83 | 65.19 | 10.66 |
| Work Experience (Years) | 0 | 22 | 7.88 | 4.91 |
3Results
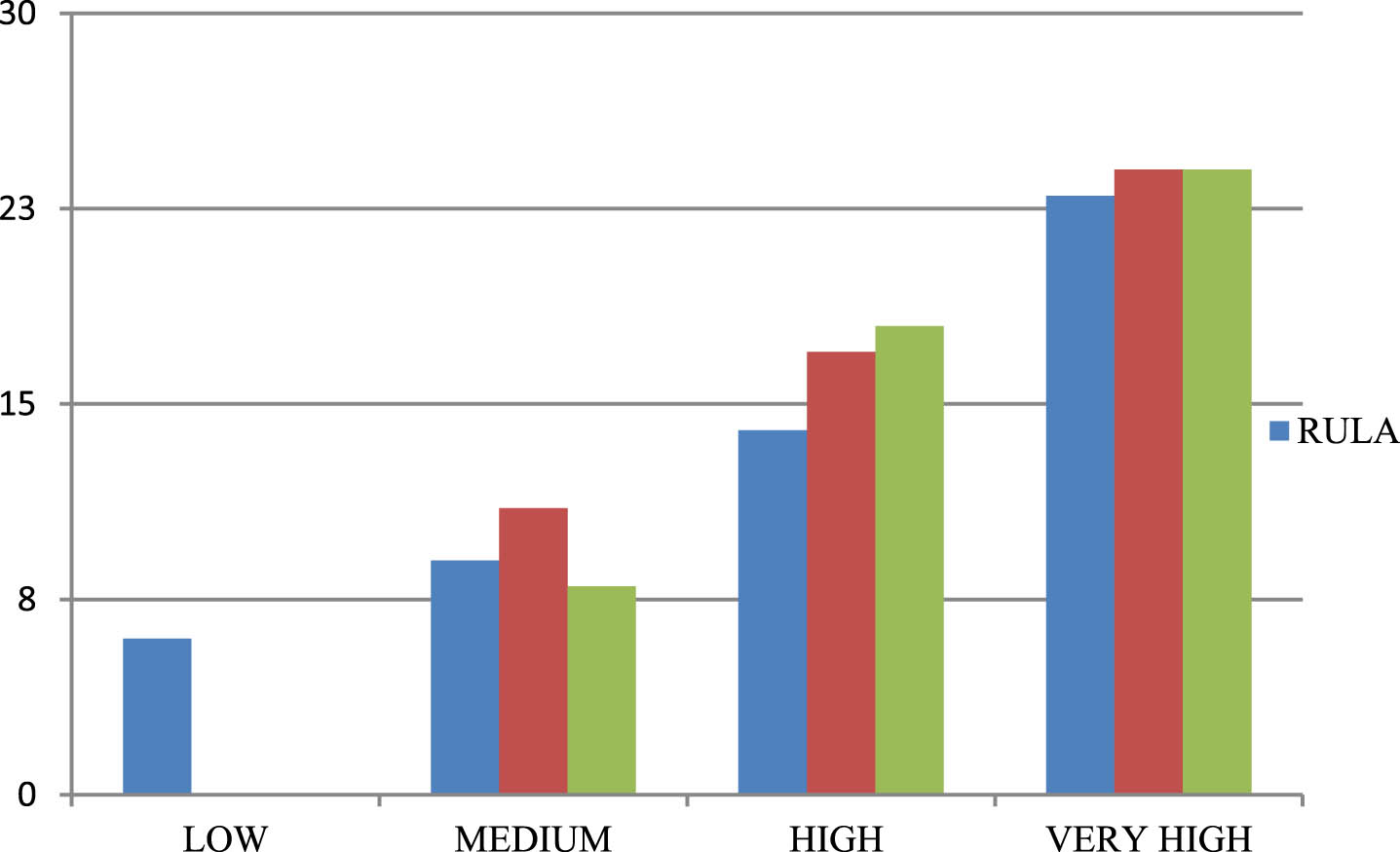
RULA revealed that the majority of the labourers experienced an undeniable degree of risk and revision in their functioning stances was essential. It was found that 45% of workers fell under the ‘very high’ risk level category, 27% of workers made up the ‘high’ level risk category, ‘medium’ risk level constituted 17% of the workers and finally, 11% of workers faced a low level of risk. The risk level of workers from the RULA analysis is displayed in Table 2. The scores were updated through ergonomic interventions for high-risk working postures, with implemented recommendations and revised scores are detailed below.
Table 2
Risk level of workers in terms of RULA
| RULA Score | 1–2 | 3–4 | 5–6 | 7 |
| Risk Level | Low | Medium | High | Very High |
| Required Action | Acceptable | Investigate Further | Investigate further and change soon | Investigate and change immediately |
| Number Of Workers | 6 | 9 | 14 | 23 |
As performed in RULA, the same set of 52 workers exhibiting working postures was carried out for REBA analysis. It was found that the ‘high risk’ level constituted about 47% of workers, 32% of workers fell under the ‘high’ risk level and 21% of workers were facing the ‘medium’ level of risk [20, 43]. The risk levels of workers from the REBA analysis are displayed in Table 3. Similar to RULA, high-risk postures were adapted using ergonomic modifications and then again analyzed using the same methodology. The reassessment scores that were mentioned in the discussion section follow.
Table 3
Risk levels of workers in terms of REBA
| REBA Score | 1 | 2–3 | 4–7 | 8–10 | 11+ |
| Risk Level | Negligible | Low | Medium | High | Very High |
| Required Action | None | Change may be needed | Change needs Soon | Investigate&Implement | Implement Immediate change |
| Number of Workers | Nil | Nil | 11 | 17 | 24 |
Similar to RULA and REBA, the OWAS results closely show the higher level of risk that the workers were experiencing. Fifty per cent of workers showed a high level of risk, 35 per cent of workers showed a medium level of risk and 15 per cent of workers showed a low level of risk from the OWAS analysis. The risk levels of workers identified through OWAS have been presented in Table 4. Due to its limited score categories when compared to RULA and REBA, OWAS was not used for reassessment [24, 46]. Finally, the initial scores of each method indicated that workers were experiencing a high level of risk from the working stances which are displayed in Fig. 2.
Table 4
Risk level of workers in terms of OWAS
| OWAS Score | 1 | 2 | 3 | 4 |
| Risk Level | Negligible | Low | Medium | High |
| Required Action | No Action Required | Corrective Actions required in near future | Corrective actions should be done as soon as possible | Corrective actions should be done and improvement required immediately. |
| Number of workers | Nil | 8 | 18 | 26 |
Fig. 2
Comparison of the risk level of workers in RULA, REBA & OWAS.
For the positions that posed a high risk, recommendations were made and it was urged to adopt these ergonomic remedies. The interventions were applied to working postures and the scores were again recalculated by applying to RULA and REBA. The recalculated scores are displayed in Table 6 for the mentioned posture and this method is applied for all the high-risk postures. The differences in scores were analyzed using paired sample t-tests. The working postures after the implementation of corrective measures were again analyzed with RULA and REBA scores and were reduced when compared to the previous postures score which is represented in Table 8.
3.1Paired sample t-test
The investigation proceeded to identify whether there were significant differences between RULA and REBA scores before and after the implementation of the recommendations. The statistical tests were performed using IBM SPSS software version [47, 48]. The data underwent the Shapiro-Wilk test to examine the normal distribution and the p-value of 0.067, which is greater than 0.05 confirms that the data was normally distributed [49]. A paired sample t-test was conducted to assess potential differences between the values obtained from the two sets of observations, assuming adherence to a normal distribution [50]. The paired sample t-test also known as the dependent sample t-test, is a statistical method for determining if the means of subject obtained from the two sets of data differ [7, 51]. A paired sample t-test was performed to examine the developed hypothesis, with the null hypothesis being rejected only if the p-value is less than 0.05 [5]. The analysis revealed a significant difference (p = 0.0042) between the old and new RULA scores, underscoring the robustness and meaningfulness of the findings. Following adjustments to the working postures, notable changes in score values were observed, including a mean value of 2.04 and a standard deviation of 0.6110, with details presented in Table 5.
Table 5
Paired Sample t-test results on RULA Score
| OLD &NEW RULA Score Analysis | Mean | Standard Deviation | Standard Error | t | df | Sig |
| Values | 2.0400 | 0.6110 | 0.1222 | 16.694 | 24 | 0.0042 |
A paired sample t-test with a sample size of 24, assessed differences between initial and final REBA scores. Before this, the data’s normality was confirmed via the Shapiro-Wilk test. The analysis revealed a significant difference between initial and final scores (p = 0.0066), which is less than 0.05, indicating the null hypothesis is rejected. Also, the mean value of 2.5833 and a standard deviation of 0.8927, detailed results of which are provided in Table 6.
Table 6
Paired Sample t-test on REBA score
| OLD &NEW REBA Score Analysis | Mean | Standard Deviation | Standard Error | t | df | Sig |
| Values | 2.5833 | 0.8297 | 0.1694 | 15.253 | 23 | 0.0066 |
4Discussion
Worldwide, work-related musculoskeletal disorders are a major occupational health issue. This investigation’s key finding was that building employees are susceptible to high-risk WMSDs and immediate ergonomic measures are necessary due to the large percentage of high-risk and extremely high-risk levels in both RULA and REBA assessments [52]. Similarly, Jain et al. [34] analyzed the working postures of farmers and classified the scores with the percentage of workers who fell under the level of risk they were experiencing. Construction workers being the human capital of the construction industry require continuous improvement of skills, reduction of health risks and improving productivity [6]. To avoid these kinds of issues, ergonomic interventions must be implemented to maintain the workers’ capability and reduce the incidence of injuries and accidents in various construction occupations [36]. This study also involved adjusting and changing worker actions and working postures following ergonomic principles. It takes place in collaboration with masonry experts and construction officials to ensure overall productivity remains unaffected. In this approach, both human postures and the entire operation of the organization may also be influenced [29]. This comprehensive strategy could improve system productivity and operator well-being through administrative and engineering interventions and they are explained with appropriate recommendations as illustrated in Table 7.
Table 7
Recalculated score after ergonomic interventions
| Posture No 1 | Recommendations | Scores Before | |
| Before Ergonomic Intervention | Ergonomic | ||
| recommendations | |||
| RULA Score | REBA Score | ||
 Regular Working Posture | Nil | 7 | 12 |
| After Ergonomic Intervention | Recommendations | New Score after | |
| Ergonomic | |||
| recommendations | |||
| RULA score | REBA score | ||
 Corrected Working Posture | Get close to work and use a small seat to sit. | 4 | 10 |
From the analysis using RULA and REBA, it was identified that workers were unaware of ergonomics. The outcome from RULA and REBA showed that working people on the sites were exposed to a high level of disorders and it was planned to reduce these by applying ergonomic interventions [34]. Occupational ergonomics has to do with the design or modification of the workplace, equipment and process to decrease injuries at the workplace and also to improve productivity [40]. Highlighting ergonomic risk control such as proper workplace design and creating awareness through training and education in their working postures with management support enhances worker performance [14]. Especially from the proposals of the site engineer and masonry expert, high-risk postures were analyzed. The postures exhibit an immediate change in their working postures chosen for the implementation of recommendations [22]. After implementing recommendations and revised postures, workers experienced a reduction in muscle fatigue [53], consequently lowering the occurrence of musculoskeletal disorders [54]. The dramatic decrease in RULA and REBA scores displayed in Table 8 confirmed that the suggested recommendations and corrective measures to the work postures reduced the risk of occupational disorders [27]. Similarly, Qureshi et al. applied ergonomic interventions to workers in foundry units who were experiencing occupational hazards, while Drisya et al. analyzed complaints of shoulder knee and upper back issues linked to bar bending operations [7, 52]. Implementing ergonomic interventions in the construction industry was complex because the workflow should not be affected by any cause [55]. Suggestions were organized after a deep literature survey and discussion with the experts. The interventions were applied after practice with a skilled worker in keeping safety as a major issue [50]. From the literature survey and discussion with domain experts, suggestions were given.
Table 8
RULA & REBA score comparison for very high risky postures
| Posture No. | Initial RULA Score | Final RULA Score | Initial REBA Score | Final REBA Score |
| 1 | 7 | 4 | 12 | 10 |
| 2 | 7 | 5 | 11 | 8 |
| 3 | 7 | 4 | 12 | 10 |
| 4 | 7 | 5 | 11 | 8 |
| 5 | 7 | 5 | 11 | 10 |
| 6 | 7 | 5 | 12 | 10 |
| 7 | 7 | 5 | 11 | 8 |
| 8 | 7 | 5 | 14 | 10 |
| 9 | 7 | 5 | 11 | 9 |
| 10 | 7 | 6 | 11 | 8 |
| 11 | 7 | 4 | 12 | 10 |
| 12 | 7 | 5 | 13 | 10 |
| 13 | 7 | 4 | 13 | 10 |
| 14 | 7 | 5 | 13 | 10 |
| 15 | 7 | 5 | 11 | 9 |
| 16 | 7 | 5 | 14 | 10 |
| 17 | 7 | 5 | 12 | 9 |
| 18 | 7 | 4 | 11 | 9 |
| 19 | 7 | 5 | 11 | 7 |
| 20 | 7 | 6 | 13 | 10 |
| 21 | 7 | 5 | 12 | 9 |
| 22 | 7 | 6 | 11 | 10 |
| 23 | 7 | 5 | 12 | 10 |
| 24 | – | – | 11 | 9 |
4.1Control measures on the worker level
Implementing a series of effective control measures at the worker level is essential for minimizing the risks associated with working postures and they are listed as follows.
⊲ Get closer to work and use a stool to sit.
⊲ Replace manual loading with trolleys and conveyor belts for transportation.
⊲ Instead of bending to reach, materials may be kept on a work table to avoid bending.
⊲ Execute short breaks for pain relief.
⊲ Use a ladder to carry out a task at higher elevations.
⊲ Materials should be kept within reach before starting the task.
4.2Control measures on the management level
At the managerial level, it is crucial to establish a set of efficient control measures aimed at reducing the risks linked with working postures as detailed below.
⊲ Workers should be trained on ergonomic principles regularly.
⊲ Make a task plan before carrying it out.
⊲ Overtime work must be compensated by allowances.
⊲ Provide Personal Protective Equipment such as back support belts, knee pads, gloves, safety goggles, and steel-toed boots.
It is evident from Tables 7 and 8, that the suggested ergonomic measures significantly reduced the risk of bad working postures. By instituting a system that involves regulations of the working postures associated concerns can be documented. This documentation serves as the foundation for developing targeted interventions aimed at improving the postural habits serves as the foundation for developing targeted interventions aimed at improving the postural habits of construction workers [56]. The implementation of such as system allows for a proactive approach to addressing and mitigating working posture-related issues within the construction industry. Compared to other industries, the construction industry requires more manpower for each task. Workers frequently exerted themselves beyond their natural physical limits to keep up with the industry’s growing complexity and problems. To avoid the problems in their working postures they were requested to follow these recommendations for health hazards [36]. In integrating proper ergonomics into the company, management should create a proper workplace with adequate lighting, proper tools and equipment [3]. Workers should be allowed to relax with regular breaks and employee endurance should not be tested at all times. Management should have a positive influence on the lives of employees [27]. These recommendations are put into practice after getting adequate approval from the site engineer and masonry expert for the implementation of working postures without reducing their actual job efficiency.
To continue the score differences throughout their work, workers adhered to following these improved postures in their future working projects. Even though industrialized countries have rules in place to protect workers, the situation is poor in developing nations where labour is cheap and the living standards of these workers are rarely taken into account. Most of these workers are unskilled and illiterate, and they migrate to large cities in search of higher pay [9]. A worker’s perception of risk at work increases with their lack of understanding of ergonomics. Workers should be made aware of health issues. Supervisors should urge employees to adopt comfortable postures at work [7]. By predicting and incorporating ergonomic hazards into work-related features, NIOSH’s Prevention through Design (PtD) effort seeks to reduce ergonomic hazards in occupational safety. It entails preventative measures like task redesigning and retrofitting, improving the work environment and ensuring workers’ safety [57]. It is also necessary to modify the working procedures concerning ergonomic guidelines and the introduction of machinery for manual material handling activities. This study implies that the construction sectors should implement workplace interventions like ergonomic guidelines and the introduction of machinery for manual material handling activities. This study implies that the construction sectors should implement workplace interventions like ergonomic adjustments, training programs, and changes in work processes to reduce absenteeism and productivity. Workers must be informed of these ergonomic measures so they can safeguard themselves against workplace health risks [58]. Education on body mechanics, posture awareness, and muscle-strengthening exercises are also recommended. Organizational guidelines should promote safe postures, leading to reduced absenteeism, increased job satisfaction, and enhanced productivity.
5Limitations amd future scope
The study findings are subjected to several limitations that need to be acknowledged. The scope of this study was focused on construction workers in India and selectively on the residential working practices in Chennai city. Additionally, fewer female workers were at the construction site and they avoided the interviews. Due to experimental activity, a systematic observation method is preferred for data collection when collecting worker data on building sites using contact and non-contact sensors was more challenging than in other industries [18, 22]. The working areas were not fixed, so the installation of cameras resulted in discontinuous data and also the workers were engaged in multiple activities [23, 59]. In our forthcoming study, it is planned to analyze larger samples of medium-risk postures and provide recommendations for both medium and low-risk postures. The analysis would be extended to the replacement of other personal protective equipment (PPE) and ergonomic devices to assess working postures. Findings and recommendations were subsequently applied to comparable workplaces in different areas to expand the potential scope for future applications.
6Conclusion
Neglecting worker welfare in developing sectors not only impacts their physical and mental health, it affects their overall well-being. Specifically, construction workers with physically demanding, awkward postures often suffer from musculoskeletal disorders that necessitate lengthy recovery. Our investigation into the working postures of unorganized residential construction workers has provided valuable insights into the pressing issue of occupational health and safety concerns within the industry. Through the utilization of established ergonomic assessment methods such as Rapid Upper Limb Assessment (RULA), Rapid Entire Body Assessment, and Ovako Working Posture Analysis (OWAS) the working postures prevalent among the construction workers were meticulously scrutinized. High rates of harmful postures among workers were identified and the urgent need for interventions was highlighted for the protection of well-being.
Optimized working postures have been achieved following the interventions, incorporating ergonomic best practices rooted in safety principles to reduce musculoskeletal disorders and enhance employee welfare. The post-implementation results demonstrated a promising reduction in RULA and REBA scores, supported by paired sample t-tests, indicating the effectiveness of mitigating workplace hazards and promoting a safer environment. Strong recommendations are made for management and client support in implementing changes, stressing the importance of ergonomics in unorganized sectors. Prioritizing ergonomics is vital for protecting worker’s health and cultivating a resilient safety culture in the construction industry. Ongoing implementation and enhancement of ergonomic interventions are essential for worker well-being and supporting India’s growing construction sector. This study is a valuable resource for academia and practitioners interested in collecting posture-related data for construction workers, aiding in the selection for analysis methods across job types. By collaborating with stakeholders and policymakers, we can prioritize occupational health and safety, ensuring every worker receives the dignity and protection they deserve.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Conflict of interest
The authors declare that they have no conflict of interest.
Acknowledgments
The authors have no acknowledgments.
Funding
The authors report no funding.
References
[1] | Shair EF , Ahmad SA , Marhaban MH , Mohd Tamrin SB , Abdullah AR . EMG processing based measures of fatigue assessment during manual lifting. BioMed Research International. (2017) ;2017: :3937254. |
[2] | Shenje J , Wushe T . An analysis of the relationship between occupational stress and employee job performance in public health care institutions: A case study of public hospitals in Harare. SA Journal of Human Resource Management. (2019) ; 17: (1), 1–1. |
[3] | Kulkarni VS , Devalkar RV . Postural analysis of building construction workers using ergonomics. International Journal of Construction Management. (2019) ;19: (6), 464–71. |
[4] | Biswas D , Mariani A . Problems of Unorganized Workers and their Social Security Measures in India: An Analysis. International Journal of Research and Analytical Reviews. (2020) ; 7: (1):931–40. |
[5] | Rashedi E , Nussbaum MA . Cycle time influences the development of muscle fatigue at low to moderate levels of intermittent muscle contraction. Journal of Electromyography and Kinesiology. (2016) ;28: :37–45. |
[6] | Kulkarni VS , Devalkar RV . Ergonomic analysis of building construction workers using RULA and REBA techniques. NICMAR–J Const Manag. (2017) ;32: :09–15. |
[7] | Drisya S , Das BB , Parida R . Ergonomic evaluation of bar benders in construction industry. Ergonomic Design of Products and Worksystems-21st Century Perspectives of Asia. (2018) ;57–67. |
[8] | Gopalakrishnan G , Brindha G . A study on employee welfare in construction industry. International Journal of Civil Engineering and Technology. (2017) ;8: (10):7–12. |
[9] | Chakraborty T , Das SK , Pathak V , Mukhopadhyay S . Occupational stress, musculoskeletal disorders and other factors affecting the quality of life in Indian construction workers. International Journal of Construction Management. (2018) ;18: (2):144–50. |
[10] | Anwer S , Li H , Antwi-Afari MF , Wong AY . Associations between physical or psychosocial risk factors and work-related musculoskeletal disorders in construction workers based on literature in the last 20 years: A systematic review. International Journal of Industrial Ergonomics. (2021) ;83: :103113. |
[11] | Brandl C , Mertens A , Schlick CM . Ergonomic analysis of working postures using OWAS in semi-trailer assembly, applying an individual sampling strategy. International Journal of Occupational Safety and Ergonomics. (2017) ;23: (1):110–7. |
[12] | Patil SP , Sangle KK . Postural Assessment of Rural Water Fetcher Using Ergonomics. European Journal of Molecular & Clinical Medicine. (2020) ;7: (06):427–33. |
[13] | Hignett S , McAtamney L . Rapid entire body assessment (REBA). Applied Ergonomics. (2000) ;31: (2):201–5. |
[14] | Rajendran M , Sajeev A , Shanmugavel R , Rajpradeesh T . Ergonomic evaluation of workers during manual material handling. Materials Today: Proceedings. (2021) ;46: :7770–6. |
[15] | McAtamney L , Corlett EN . RULA: a survey method for the investigation of work-related upper limb disorders. Applied Ergonomics. (1993) ;24: (2):91–9. |
[16] | Palikhe S , Yirong M , Choi BY , Lee DE . Analysis of musculoskeletal disorders and muscle stresses on construction workers’ awkward postures using simulation. Sustainability. (2020) ;12: (14):5693. |
[17] | Dianat I , Afshari D , Sarmasti N , Sangdeh MS , Azaddel R . Work posture, working conditions and musculoskeletal outcomes in agricultural workers. International Journal of Industrial Ergonomics. (2020) ;77: :102941. |
[18] | Jebelli H , Hwang S , Lee S . EEG-based workers’ stress recognition at construction sites. Automation in Construction. (2018) ;93: :315–24. |
[19] | Yahya NM , Zahid MN . Work-related musculoskeletal disorders (WMDs) risk assessment at core assembly production of electronic components manufacturing company. InIOP Conference Series: Materials Science and Engineering (2018) Mar 1 (Vol. 319: , p. 012036). IOP Publishing. |
[20] | Sukadarin EH , Deros BM , Ghani JA , Mohd Nawi NS , Ismail AR . Postural assessment in pen-and-paper-based observational methods and their associated health effects: a review. International Journal of Occupational Safety and Ergonomics. (2016) ;22: (3):389–98. |
[21] | Satapathy S . Work place discomfort and risk factors for construction site workers. International Journal of System Assurance Engineering and Management. (2022) ;13: (2):668–80. |
[22] | Dev M , Bhardwaj A , Singh S . Analysis of work-related musculoskeletal disorders and ergonomic posture assessment of welders in the unorganized sector: a study in Jalandhar, India. International Journal of Human Factors and Ergonomics. (2018) ;5: (3):240–55. |
[23] | Hita-Gutierrez M , Gomez-Galan M , Díaz-Perez M , Callejon-Ferre AJ . An overview of REBA method applications in the world. International Journal of Environmental Research and Public Health. (2020) ;17: (8):2635. |
[24] | Kee D . Comparison of OWAS, RULA and REBA for assessing potential work-related musculoskeletal disorders. International Journal of Industrial Ergonomics. (2021) ;83: :103140. |
[25] | Qureshi MA , Sohu S , Keerio MA . The impacts of operational risks in the supply chain of construction projects in Malaysia. Tehnicki Vjesnik. (2020) ;27: (6):1887–93. |
[26] | Draskovic D , Prusa P , Cicevic S , Jovcic S . The implementation of digital ergonomics modeling to design a human-friendly working process in a postal branch. Applied Sciences. (2020) ;10: (24):9124. |
[27] | Dasgupta P , Sample M , Buchholz B , Brunette M . Is worker involvement an ergonomic solution for construction intervention challenges: A systematic review. Theoretical Issues in Ergonomic Science. (2017) ;18: (5):433–41. |
[28] | Qzay M , Cakır O , Ucan R , Gul A . Application of RULA and NIOSH Ergonomic Risk Assessment Methods: A Case Study in Construction Industry in Turkey. International Journal of Engineering Research & Technology (IJERT). (2020) ;9: (09):306–12. |
[29] | Micheletti Cremasco M , Giustetto A , Caffaro F , Colantoni A , Cavallo E , Grigolato S . Risk assessment for musculoskeletal disorders in forestry: A comparison between RULA and REBA in the manual feeding of a wood-chipper. International Journal of Environmental Research and Public Health. (2019) ;16: (5):793. |
[30] | Lee G , Choi B , Jebelli H , Lee S . Assessment of construction workers’ perceived risk using physiological data from wearable sensors: A machine learning approach. Journal of Building Engineering. (2021) ;42: :102824. |
[31] | Kumar A , Kamath S . A Study of Reliability and Validity of RULA against REBA Among The Employees Operating Computers In The Bank. Journal of Advances in Sports and Physical Education. (2019) ;2: (07):131–8. |
[32] | Joshi M , Deshpande V . A systematic review of comparative studies on ergonomic assessment techniques. International Journal of Industrial Ergonomics. (2019) ;74: :102865. |
[33] | Chatterjee A , Sahu S . A physiological exploration on operational stance and occupational musculoskeletal problem manifestations amongst construction labourers of West Bengal, India. Journal of Back and Musculoskeletal Rehabilitation. (2018) ;31: (4):775–83. |
[34] | Jain R , Meena ML , Dangayach GS . Prevalence and risk factors of musculoskeletal disorders among farmers involved in manual farm operations. International Journal of Occupational and Environmental Health. (2018) :1–6. |
[35] | Shukriah A , Baba MD , Jaharah AG . REBA evaluation on garage worker: a case study. Journal of Fundamental and Applied Sciences. (2017) ;9: (5S):1080–6. |
[36] | Mishra D , Satapathy S . Ergonomic Study of Construction Workers in Odisha (India): A Case Study in Construction Sites. Trends in Industrial Engineering Applications to Manufacturing Process. (2021) :507–27. |
[37] | Schwartz AH , Albin TJ , Gerberich SG . Intra-rater and inter-rater reliability of the rapid entire body assessment (REBA) tool. International Journal of Industrial Ergonomics. (2019) ;71: :111–6. |
[38] | AEPCS Android application link: www.newbodytechnology.com |
[39] | Anagha R , Xavier AS . Working posture analysis of construction workers using ergonomics. Sustainability, Agri, Food and Environmental Research. (2022) ;10: (1). |
[40] | Wang MH , Chen YL , Chiou WK . Using the OVAKO working posture analysis system in cleaning occupations. Work. (2019) ;64: (3):613–21. |
[41] | Gómez-Galán M , Pérez-Alonso J , Callejón-Ferre ÁJ , López-Martínez J . Musculoskeletal disorders: OWAS review. Industrial Health. (2017) ;55: (4):314–37. |
[42] | Caban-Martinez AJ , Santiago KM , Stillman J , Moore KJ , Sierra DA , Chalmers J , Baniak M , Jordan MM . Physical exposures, work tasks, and OSHA-10 training among temporary and payroll construction workers. Journal of Occupational and Environmental Medicine. (2018) ;60: (4):e159–65. |
[43] | Brandt M , Madeleine P , Samani A , Ajslev JZ , Jakobsen MD , Sundstrup E , Andersen LL . Effects of a participatory ergonomics intervention with wearable technical measurements of physical workload in the construction industry: cluster randomized controlled trial. Journal of Medical Internet Research. (2018) ;20: (12):e10272. |
[44] | Colim A , Faria C , Braga AC , Sousa N , Rocha L , Carneiro P , Costa N , Arezes P . Towards an ergonomic assessment framework for industrial assembly workstations—A case study. Applied Sciences. (2020) ;10: (9):3048. |
[45] | Gyllensten K , Fredriksson S , Widen S , Söderberg M , Waye KP . Nurses’ and preschool teachers’ experiences of taking part in a participatory intervention project in communication-intense working environments. Work. (2022) ;73: (3):857–69. |
[46] | Brandl C , Mertens A , Schlick CM . Ergonomic analysis of working postures using OWAS in semi-trailer assembly, applying an individual sampling strategy. International Journal of Occupational Safety and Ergonomics. (2017) ;23: (1):110–7. |
[47] | Timurtaş E , Avcı EE , Mate K , Karabacak N , Polat MG , Demirbüken İ . A mobile application tool for standing posture analysis: development, validity, and reliability. Irish Journal of Medical Science. (2022) ;191: (5):2123–31. |
[48] | Zhao X , Hwang BG , Lim J . Job satisfaction of project managers in green construction projects: Constituents, barriers, and improvement strategies. Journal of Cleaner Production. (2020) ;246: :118968. |
[49] | Won D , Hwang BG , Chng SJ . Assessing the effects of workforce diversity on project productivity performance for sustainable workplace in the construction industry. Sustainable Development. (2021) ;29: (2):398–418. |
[50] | Shan M , Liu WQ , Hwang BG , Lye JM . Critical success factors for small contractors to conduct green building construction projects in Singapore: identification and comparison with large contractors. Environmental Science and Pollution Research. (2020) ;27: (8):8310–22. |
[51] | Raphael AO , Samuel OS , Dipeolu AA . Evaluation of Service Quality Gaps in Construction Professional Service Firms in Nigeria. Journal of Construction in Developing Countries. (2022) ;27: (1):25–40. |
[52] | Qureshi AM , Solomon DG . Ergonomic assessment of postural loads in small-and medium-scale foundry units. Journal of The Institution of Engineers (India): Series C. (2021) ;102: (2):323–35. |
[53] | Seo J , Lee S . Automated postural ergonomic risk assessment using vision-based posture classification. Automation in Construction. (2021) ;128: :103725. |
[54] | Gallagher S , Schall MC . Musculoskeletal disorders as a fatigue failure process: evidence, implications and research needs. In New Paradigms in Ergonomics (2020) Apr 28 (pp. 105–119). Routledge. |
[55] | Joshi M , Deshpande V . Investigative study and sensitivity analysis of Rapid Entire Body Assessment (REBA). International Journal of Industrial Ergonomics. (2020) ;79: :103004. |
[56] | Zhu Z , Dutta A , Dai F . Exoskeletons for manual material handling–A review and implication for construction applications. Automation in Construction. (2021) ;122: :103493. |
[57] | Nath ND , Akhavian R , Behzadan AH . Ergonomic analysis of construction worker’s body postures using wearable mobile sensors. Applied Ergonomics. (2017) ;62: :107–17. |
[58] | Mosly I . Factors influencing safety performance in the construction industry of Saudi Arabia: an exploratory factor analysis. International Journal of Occupational Safety and Ergonomics. (2022) ;28: (2):901–8. |
[59] | Yu Y , Li H , Yang X , Kong L , Luo X , Wong AY . An automatic and non-invasive physical fatigue assessment method for construction workers. Automation in Construction. (2019) ;103: :1–2. |

