
Organizational and psychosocial environmental work factors associated with self-rated exhaustion disorder among municipal employees in rural northern Sweden
Abstract
BACKGROUND:
Research indicates that good organizational and psychosocial environments are vital to well-functioning workplaces and employee health. Working in the municipal sector and in the rural context may contribute to more health problems, poorer organizational and psychosocial work environments, and higher sick-leave rates.
OBJECTIVE:
The aim of this study was to explore organizational and psychosocial environmental work factors among municipal employees with or without self-rated exhaustion disorder (s-ED) in rural northern Sweden.
METHODS:
The Modern Work Life Questionnaire and the Self-Rated Exhaustion Disorder Scale were used among 1093 municipal employees.
RESULTS:
The results showed that there were significant differences between the s-ED and the non–s-ED group in all but one of the organizational and psychosocial environmental work factors. Various demands, i.e. quantitative, emotional, intellectual, and IT demands were some factors associated with the s-ED group. Social support, resources, and time for work and reflection were some factors associated with the non–s-ED group. Both the s-ED and the non–s-ED groups assessed significantly higher emotional demands and less resources compared to national reference values.
CONCLUSION:
Findings from this study are relevant to a better understanding what organizational and psychosocial work environmental work factor the employer need to pay extra attention to. Addressing risk and protective factors in the work environment could tribute to promote occupational well-being, preventing exhaustion disorder and long-term sick leave among municipal employees in rural northern Sweden.
1Introduction
Organizational and psychosocial environmental risk factors in the workplace can exhaust employees’ mental and physical resources and are associated with ill health [1], and long-term sick leave [2]. Extensive work for a longer period of time can affect the work-life balance [3], and cause stress-related health problems [4]. According to one of the most commonly used occupational stress models, the job demands-resources (JD-R) model [5], employees’ health and well-being depend on a balance of positive and negative organizational and psychosocial factors (resources vs. demands) in the work environment. High demands can exhaust employee’s mental and physical resources, and therefore lead to health problems, and considered to be the main causes of burnout. In contrast, sufficient resources foster employee engagement and may buffer the impact of demands on stress. The JD-R model can be used to understand, explain, and make predictions about employee burnout, work engagement, and outcomes, and is considered a useful framework for monitoring the workplace [6–8].
Burnout can be defined as a ‘syndrome conceptualized as resulting from chronic workplace stress that has not been successfully managed’, included in the International Classification of Diseases 11th edition (ICD). Three symptoms are included; feelings of energy depletion or exhaustion, increased mental distance from one’s job or feelings of negativism or cynicism related to one’s job, and reduced professional efficacy. Burnout is classified as an occupational phenomenon and not a medical condition, bound to the occupational context, and not applied to describe experiences in other areas of life [9]. One of the most used definition of burnout was presented by Maslach and co-workers [10], who defined it as a syndrome of emotional exhaustion, depersonalization and reduced professional accomplishment, mainly afflicting employees in helping professions. Burnout is an unspecific term, with various definitions and of psychological origin, unlike exhaustion disorder (ED), which is a more specific term and a clearly defined clinical diagnosis. The Swedish Board of Health and Welfare introduced the medical diagnosis of (ED) to facilitate the classification of patients seeking health care due to exhaustion caused by prolonged stress. The stressors can be caused by work, private life, and often a combination of both. Exhaustion disorder was accepted as a formal diagnosis in the Swedish version of the 10th revision of the ICD (F43.8A). The diagnostic criteria involve exhaustion symptoms, which have developed in response to stressors, and existed for at least six months. Lack of mental energy, reduced initiative, reduced endurance, or prolonged recovery time after mental strain are also important elements. Other symptoms such as concentration difficulties or memory problems, reduced ability to manage demands, sleep disturbances, gastrointestinal symptoms are also present. The symptoms cause clinically significant suffering or reduced ability to function at work, socially, or in other important situations [11, 12]. Exhaustion disorder has been proposed as the most valid clinical equivalent of burnout [13]. Research has shown that the majority (93%) of patients who fulfilled the criteria for ED also scored clinical burnout [14]. Research has shown that patients with exhaustion disorder appear to consult their general practitioner numerous times with stress-related complaints in the years preceding their diagnosis [15].
In Sweden, a large proportion of sick leave can be linked to occupational stress, and its association with the organizational and psychosocial work environment has increased over time. Exhaustion disorder (ED) is a common cause of sick leave, which for this diagnosis often exceeds 6 months [16]. Job insecurity, low influence of work-related decisions, high effort for low reward, and lack of support are important organizational and psychosocial factors related to ED [17]. People with ED have reported private relationship conflicts to be almost as important as work demands and usually attribute the onset of their illness to a combination of work and non-work stressors [18]. Self-rated ED is based on the Swedish diagnostic criteria for ED, but it is not a medical diagnosis. It is rather a measure of a stressed individual’s recognition of their condition and perception of its severity and effects on their well-being. The s-ED scale is a screening instrument, developed for assessment of ED, and the s-ED scale strives to be compliant with the diagnostic criteria for ED [19]. Previous studies have found s-ED prevalence rates of 7.8% to 21% among working people [19–22]. This study will focus on s-ED among municipal employees in rural northern Sweden.
Excessive workload and psychologically stressful work are associated with working in the municipal sector in Sweden [23], Norway [24], and Finland [25]. Research on the Swedish municipal sector has shown that high workload is associated with mental health problems, especially in those who have low social support [26]. A study among municipal school principals showed that almost one in three reported signs of possible ED [27]. Research has described shortages in work health promotion, where municipal organizations focus on individual health, rather than factors related to the work environment, and also a lack of follow-up after e.g. the annual employee survey [28]. Municipal employees have the highest sick-leave rates in the country, most commonly for stress-related disorders and with a twofold prevalence in women over men [29]. Among municipal employees, where the major occupational groups in the municipal sector are social workers, preschool and school staff, and elderly care employees, lack of recovery time is thought to be an important link between working conditions, ill health, and sick leave [30]. The importance of having time and energy for both private life and work have been described as essential among home help service nurses, and shift work and part time work as two resources contributing to flexibility and a prerequisite to better work-life balance [31]. General work experience such as joy, a good atmosphere, feedback and meaningfulness in work has found to be the strongest predictor of health among municipal health care staff [32], and poor health has been associated with high rates of long-term sick leave, and found in municipalities with a population decline [33].
A population decline is often found in Sweden’s rural municipalities, where young and highly educated people move, leaving the population older and low educated. Rural municipalities are often small in population but large in land area, and located far away from the growth regions [34]. Research in the Nordic countries, Denmark, Finland, and Norway report poorer self-reported health and higher prevalence of obesity, and physical inactivity in rural areas compared to urban areas; however, the opposite pattern was reported in Sweden [35, 36]. Mortality has been reported higher in municipalities with low population density in Sweden, Norway and Finland [37]. Research in northern Sweden has shown higher level of cardiovascular risk factors as obesity, high cholesterol and sedentary lifestyle when living in rural areas, compared to urban areas [38], but lower risk of mental disorder sick leave in sparsely populated areas than urban areas [39]. Recent results from a study conducted in northern Sweden’s rural municipalities showed an s-ED prevalence of 21.5% among rural municipal employees [40].
The results mentioned above indicate employees’ health and well-being depend on a balance of positive and negative organizational and psychosocial environmental work factors, that is demands and resources. In Sweden, a large proportion of sick leave can be linked to occupational stress, and its association with the organizational and psychosocial work environment has increased over time. Exhaustion disorder (ED) is a common cause of sick leave, which for this diagnosis often exceeds 6 months. Job insecurity, low influence of work-related decisions, high effort for low reward, and lack of support are important organizational and psychosocial factors related to ED. Working in the municipal sector and in the rural context could both contribute to health problems, poorer organizational and psychosocial work environments, and higher sick-leave rates. Little is known about s-ED among working municipal employees in rural northern Sweden. To our knowledge, no research has focused on associations between the organizational and psychosocial work environment and s-ED. This cross-sectional study can therefore contribute to increased knowledge and inform future interventions to promote healthy workplaces, increase well-being, and prevent long-term sick leave due to ED.
1.1Aim
The aim of this study was to explore organizational and psychosocial environmental work factors among municipal employees with or without self-rated exhaustion disorder (s-ED) in rural northern Sweden.
1.2Research questions
What organizational and psychosocial environmental work factors are associated with municipal employees with s-ED, and what factors are associated with employees without s-ED?
Are there between-group differences in organizational and psychosocial environmental work factors among employees with or without s-ED?
Are there differences in organizational and psychosocial environmental work factors in the two groups compared to national reference values?
2Methods
2.1Study design and procedure
We performed this cross-sectional study in 2018 in two rural municipalities in northern Sweden, using a web-based questionnaire to collect data from March to June. All municipal employees in the two municipalities received a link to the questionnaire by e-mail. For employees without a known e-mail address, data were collected through a paper-based questionnaire. Three reminders were sent to non-responders by e-mail or paper mail as appropriate. The questionnaire asked for background variables and included instruments measuring participants’ organizational and psychosocial work environment and s-ED. This study was performed on behalf of a coordination association in the area, selecting the two municipalities and municipal employees included in this study.
2.2Settings and subjects
The Swedish Board of Agriculture [41] defines rural areas in terms of population density and proximity to a city. There could, however, be large between-country differences in definitions of rural areas, despite apparent similarities among the defining factors used to describe rural areas in research [42]. In the present study, municipality 1 (1600 square kilometres, ∼618 square miles) has about 3100 inhabitants, and municipality 2 (5500 square kilometres, ∼2125 square miles) has about 12 200 [43]. Of 2077 municipal employees asked to participate in the study, 1093 (52.6%) answered the questionnaire. Three persons could not be categorized as s-ED or non–s-ED because of missing internal values, thus 1090 persons completed the s-ED scale. The dataset in this study and demographic characteristics of the employees of the two municipalities have been previously reported [40]. Regarding professions in Table 1, ‘nursing staff’ and, ‘educational staff’ refers to having a human service profession in each sector. ‘Office staff’ refers to employees with a desk or administrative work, managers excluded. ‘Managers’ refers to having a leading role and being responsible for subordinates. ‘Non-office staff’ refers to other employees with a practical work, e.g. cleaner, janitor, construction worker and cashier.
Table 1
Characteristics of participants with or without s-ED (n = 1090)
| s-ED | non–s-ED | p value | Effect size | |
| 234 (21.5) | 856 (78.5) | |||
| Municipality | ||||
| Municipality 1 | 69 (29.5) | 195 (22.8) | 0.034 | φ= –0.064 |
| Municipality 2 | 165 (70.5) | 661 (77.2) | ||
| Sex | ||||
| Male (%)* | 35 (15.0) | 224 (26.2) | <0.001 | φ= 0.108 |
| Female (%)* | 199 (85.0) | 632 (73.8) | ||
| Age (range 19–67) | ||||
| Mean years±SD* | 42.4±12.3 | 45.8±11.9 | <0.001 | d = 0.281 |
| Employment | ||||
| Work full time (%) | 154 (65.8) | 631 (73.7) | 0.015 | φ= 0.074 |
| Work part time (%) | 80 (34.2) | 223 (26.1) | ||
| Time at current workplace (range 0–42) | ||||
| Mean years±SD | 7.8±7.6 | 9.0±8.9 | 0.057 | d = 0.145 |
| Time as municipal employee (range 0–45) | ||||
| Mean years±SD | 13.3±10.3 | 15.7±11.3 | 0.003 | d = 0.206 |
| Long-term sick leave | ||||
| No (%) | 199 (85.0) | 825 (96.4) | <0.001 | φ= 0.195 |
| Yes (%) | 35 (15.0) | 31 (3.6) | ||
| Children living at home | ||||
| Yes (%) | 108 (46.2) | 414 (48.4) | 0.555 | φ= –0.018 |
| No (%) | 125 (53.4) | 439 (51.3) | ||
| Working schedule | ||||
| Day/evening (%) | 178 (76.1) | 702 (82.0) | 0.041 | φ= 0.062 |
| Night (%) | 56 (23.9) | 154 (18.0) | ||
| Marital status | ||||
| Living with a partner (%) | 173 (73.9) | 685 (76.9) | 0.050 | V = 0.074 |
| Living apart together (%) | 12 (5.1) | 22 (2.6) | ||
| Single (%) | 49 (20.9) | 149 (17.4) | ||
| Education | ||||
| Compulsory school (%) | 6 (2.6) | 35 (4.1) | 0.339 | V = 0.045 |
| Upper secondary school (%) | 122 (52.1) | 409 (47.8) | ||
| University (%) | 106 (45.3) | 412 (48.1) | ||
| Living | ||||
| Urban area (%) | 178 (76.1) | 628 (73.4) | 0.404 | φ= –0.025 |
| Rural area (%) | 56 (23.9) | 228 (26.6) | ||
| Home | ||||
| House (%) | 149 (63.7) | 619 (72.3) | 0.024 | V = 0.084 |
| Apartment (%) | 84 (35.9) | 229 (26.8) | ||
| Other (%) | 1 (0.4) | 7 (0.82) | ||
| Profession | ||||
| Nursing staff (%) | 96 (41.0) | 280 (32.7) | 0.001 | V = 0.133 |
| Educational staff (%) | 107 (45.7) | 349 (40.8) | ||
| Managers (%) | 12 (5.1) | 65 (7.6) | ||
| Office staff (%) | 11 (4.7) | 107 (12.5) | ||
| Non-office staff (%) | 8 (3.4) | 53 (6.2) |
*These figures have earlier been published [40].
2.3Instruments
2.3.1S-ED scale
The s-ED scale [19] was used to assess municipal employees’ self-rated levels of exhaustion. The scale is based on the Swedish diagnostic criteria for ED. Being classified as having s-ED requires a Yes statement to questions 1, 2, and 4 and affirmation of at least four of the six symptoms in question 3. An individual must 1) feel physically and/or mentally exhausted for more than two weeks; 2) consider this exhaustion to be caused by long-term stress exposure (6 months or more); 3) experience symptoms for the last 2 weeks such as concentration or memory problems, markedly reduced capacity to tolerate demands or to work under time pressure, emotional instability or irritability, sleeping problems, physical weakness or being more easily fatigued, physical symptoms such as muscular pain, chest pain, palpations, gastrointestinal problems, vertigo, or increased sensitivity to sounds; 4) the complaints above have markedly decreased well-being and/or functional capacity. The s-ED scale distinguishes between light/moderate and pronounced s-ED in question number four with the response options ‘yes, to a great extent’, ‘yes, somewhat’ or ‘no, not at all’. The instrument has been validated in a study of health and medical staff in Sweden, which showed good construct validity [19].
2.3.2Organizational and psychosocial work environment
The Modern Work Life Questionnaire (MWQ) [44] measures organizational and psychosocial work environmental factors (e.g., demands, control, and support), and is based on questions that has been found to be both theoretically and empirically important. During the initial validation of the questionnaire, principal component analysis (PCA) was used to analyses the construct validity. The MWQ has been judged as valid and sufficiently reliably for mapping the organizational and psychosocial work environment [44, 45]. The Modern Work Life Questionnaire contains 127 questions (i.e. items) about organizational and psychosocial work environment and health. The 127 items in the MWQ form a total of 77 factors, and every factor consists of one or several items. Of the total of 77 factors, 32 factors were included in this study, focusing on the organizational and psychosocial environmental work factors considered most important in relation to ED based on theory and empirical data, such as demands, social support, resources, and conflicts. One example is the factor quantitative demands (QD), which consists of three questions ‘Does your job demand that you work very fast?’ ‘Does your job demand that you work very hard?’ ‘Does your work demand too much effort?’ (‘yes, often’, ‘yes, sometimes’, ‘no, rarely’, or ‘no, never’). The number of response options on different questions range from two to seven. The time period for the questions varies from latest week, 3 months to 2 years (e.g., organizational changes), while some questions do not specify a time period [44, 45]. The results from an individual workplace can be compared with reference values from a representative large sample of the working population in Sweden reported in the national Swedish Longitudinal Occupational Survey of Health (SLOSH). The SLOSH is a longitudinal survey with focus on the association between organization, work environment, and health. The national Swedish Longitudinal Occupational Survey of Health (SLOSH) is based on a representative large sample of the working population in Sweden, from which national reference values has been obtained. These reverence values of SLOSH are representative mean values and proportions for the working population in Sweden, and the same corresponding values for other sub-groups can be calculated in contrast to the working population [46, 47]. The scoring directions of all factors are clarified in Table 2.
Table 2
Differences in factors in organizational and psychosocial work environments among municipal employees with and without s-ED (n = 1090)
| s-ED | non–s-ED | Reference value | Effect size | |
| 234 (21.5) | 856 (78.5) | |||
| Quantitative demands (QD)*(range 1–4), mean±SD (95% CI) | 1.70±0.53 (1.63–1.77) | 2.08±0.57 (2.04–2.12) | 2.10 | d = 0.678 |
| Emotional demands (EmD)*(range 1–4), mean±SD (95% CI) | 1.44±0.49 (1.38–1.51) | 1.78±0.68 (1.73–1.82) | 2.28 | d = 0.574 |
| Intellectual demands (ID)*(range 1–4), mean±SD (95% CI) | 1.34±0.45 (1.28–1.40) | 1.51±0.51 (1.48–1.55) | 1.54 | d = 0.374 |
| Social competence (SC)*(range 1–4), mean±SD (95% CI) | 1.14±0.38 (1.09–1.19) | 1.25±0.50 (1.21–1.28) | 1.48 | d = 0.248 |
| IT demands (ITD)*(range 1–5), mean±SD (95% CI) | 2.90±0.95 (2.78–3.02) | 3.21±0.80 (3.15–3.26) | 2.87 | d = 0.353 |
| Physical demands (PD)*(range 1–6), mean±SD (95% CI) | 4.19±1.75 (3.96–4.42) | 4.74±1.44 (4.65–4.84) | 4.77 | d = 0.343 |
| Social support (SOC)**(range 1–4), mean±SD (95% CI) | 1.97±0.73 (1.88–2.06) | 1.60±0.55 (1.56–1.63) | 1.84 | d = 0.572 |
| Possibilities to influence (PI)**(range 1–4), mean±SD (95% CI) | 2.07±0.73 (1.98–2.17) | 1.77±0.64 (1.72–1.81) | 1.80 | d = 0.437 |
| Resources (RES)**(range 1–4), mean±SD (95% CI) | 2.10±0.68 (2.01–2.19) | 1.68±0.60 (1.64–1.72) | 1.5 | d = 0.655 |
| Time**(range 1–4), mean±SD (95% CI) | 2.51±0.75 (2.41–2.60) | 1.92±0.70 (1.87–1.97) | 2.1 | d = 0.813 |
| Knowledge** (KNOW)(range 1–5), mean±SD (95% CI) | 3.00±0.85 (2.89–3.11) | 3.05±0.73 (3.00–3.09) | 2.93 | d = 0.063 |
| Working autonomy (WA)**(range 1–4), mean±SD (95% CI) | 2.43±0.76 (2.33–2.53) | 2.07±0.68 (2.02–2.11) | 2.35 | d = 0.499 |
| Opportunities to influence working hours (OIWH)*(range 1–6), mean±SD (95% CI) | 2.41±1.16 (2.26–2.56) | 2.90±1.22 (2.82–2.99) | 2.88 | d = 0.412 |
| Participation in decisions (PID)**(range 1–5), mean±SD (95% CI) | 3.04±0.84 (2.94–3.15) | 2.77±0.84 (2.71–2.82) | 2.56 | d = 0.321 |
| Workplace democracy (WD)**(range 1–3), mean±SD (95% CI) | 2.08±0.55 (2.01–2.15) | 1.78±0.49 (1.75–1.83) | 2.02 | d = 0.576 |
| Manifested freedom of expression (MFE)** (range 1–4), mean±SD (95% CI) | 1.93±0.85 (1.82–2.04) | 1.72±0.69 (1.67–1.76) | 1.94 | d = 0.271 |
| Belonging (BEL)**(range 1–5), mean±SD (95% CI) | 2.05±0.95 (1.93–2.17) | 1.70±0.68 (1.65–1.74) | 1.82 | d = 0.424 |
| Human beings versus profitability (HUP)**(range 1–4), mean±SD (95% CI) | 2.53±0.84 (2.43–2.64) | 2.11±0.75 (2.06–2.16) | 2.30 | d = 0.527 |
| Values (VAL)**(range 1–5), mean±SD (95% CI) | 2.36±0.89 (2.24–2.47) | 1.98±0.69 (1.93–2.03) | 2.11 | d = 0.477 |
| Salary (SAL)**(range 1–4), mean±SD (95% CI) | 3.04±0.81 (2.94–3.15) | 2.59±0.80 (2.54–2.64) | 2.46 | d = 0.559 |
| Confidence in management (CM)** (range 1–4), mean±SD (95% CI) | 2.61±0.92 (2.49–2.73) | 2.11±0.78 (2.06–2.16) | 2.38 | d = 0.586 |
| Relation to immediate manager (RIM)** (range 1–4), mean±SD (95% CI) | 2.21±0.88 (2.09–2.32) | 1.86±0.68 (1.81–1.90) | 2.19 | d = 0.445 |
| Coordination (COR)**(range 1–4), mean±SD (95% CI) | 2.38±0.99 (2.26–2.51) | 1.99±0.78 (1.93–2.04) | 2.39 | d = 0.438 |
| Presence of immediate manager (PM)** (range 1–4), mean±SD (95% CI) | 2.51±0.98 (2.39–2.64) | 2.28±0.93 (2.22–2.34) | 1.63 | d = 0.241 |
| Organizational structure (OS)**(range 1–4), mean±SD (95% CI) | 2.30±0.70 (2.21–2.39) | 1.91±0.52 (1.88–1.95) | 2.00 | d = 0.632 |
| Organizational barriers (OB)*(range 1–4), mean±SD (95% CI) | 2.43±0.85 (2.32–2.54) | 2.74±0.75 (2.69–2.79) | 2.78 | d = 0.387 |
| Downsizing and relocation (DAR)* (range 1–5), mean±SD (95% CI) | 3.22±0.95 (3.10–3.35) | 3.64±0.98 (3.57–3.71) | 3.94 | d = 0.435 |
| Reorganization (REORG)**(range 1–4), mean±SD (95% CI) | 2.21±0.92 (2.09–2.33) | 1.89±0.82 (1.83–1.94) | 1.71 | d = 0.367 |
| Conflicts with managers (CWM) % (n) (95% CI) | 26.1% (61) (20.40–31.73%) | 10.3% (88) (8.24–12.32) | 18.3 | φ= –0.189 |
| Conflicts with co-workers (CWC) % (n) (95% CI) | 35.5% (83) (29.29–41.65) | 19.2% (164) (16.52–21.80) | 20.3 | φ= –0.160 |
| Conflicts with others (CWO) % (n) (95% CI) | 36.8% (86) (30.53–42.98) | 23.5% (201) (20.64–26.33) | 24.4 | φ= –0.124 |
| Violence or threat of violence (VTV) % (n) (95% CI) | 32.1% (75) (26.02–38.07) | 23.1% (198) (20.30–25.96) | 16.1 | φ= 0.085 |
*Lower values indicate more negative experienced factors of the organizational and social environment. **Lower values indicate more positive experienced factors of the organizational and social environment.
2.4Statistical analyses
Statistical analyses were performed using SPSS version 25.0 [48], and programming language R (R version 3.5.1, 2018-07-02). Cronbach’s alphas where calculated for all factors (subscales) under study when applicable. The factor intellectual demands (ID) had a Cronbach’s alpha of 0.51 and the factor Downsizing and relocation (DR) had a Cronbach’s alpha of 0.55. The Cronbach’s alphas regarding the other factors ranged from 0.71 (Time) to 0.91 (IT demands, ITD). Descriptive statistics are presented as mean scores, standard deviations (SDs), and frequency distributions when applicable. Group comparisons regarding the characteristics of participants were made using t-test and chi-square depending on the characteristics of the variable (Table 2). Group comparisons were made using 95% confidence intervals to compare means and proportions. The 95% confidence intervals (CI) were also used to make comparisons to the reference values. The factor means of the Modern Work Life Questionnaire were calculated according to the instructions from one of the responsible for the questionnaire (J. Gustafsson, personal communication by e-mail, December 5, 2017). That is, individual means to each factor was first calculated by summarizing all items to each factor in the MWQ, and then divide with the number of items related to the factor. Secondly, mean values were calculated based on these individual means as instructed. In addition to statistical significance, effect sizes were analysed using Cohen’s d (d), phi coefficient (φ), and Cramer’s V (V). Cohen’s criteria consider the effect sizes for d value of 0.2 as representing a small effect, a value of 0.5 as representing a medium effect, and a value of 0.8 as representing a large effect. Effects of φ values of 0.10 are considered small, 0.30 moderate, and 0.5 large [49]. The criteria for the effect size measured by V varies depending on the number of categories; the criteria described by Pallant was used [50].
Partial least square regression (PLSR) was used to assess the most important predictive factor(s) in municipal employees’ belonging to the with s-ED or without s-ED group. Factor scores were received by calculating the total scores for each of the 32 factors (i.e. the sum of all scores from all the items within each factor). Before performing the PLSR, some factors were reversed in order to facilitate interpretation of the results. The number of components in the PLSR models was selected by examining validation plots for mean square error of prediction (MSEP), root mean square error of prediction (RMSEP), coefficient of multiple determination (R2) and by leave-one-out cross-validation as recommended by Mevik and Cederkvist [51]. Two components were regarded as sufficient. To facilitate the interpretation of the results of the PLSR model, a figure was produced showing the predictive patterns of the factors in the MWQ in relation to the response variables (s-ED/non-s-ED). In other words, a figure containing each regression coefficient for each factor with jackknife 95% confidence intervals (CIs) surrounding the regression coefficients (Fig. 1).
Fig. 1
Plots of jackknife 95% confidence intervals around the regression coefficients from PLSR for organizational and social environment factors in the MWQ. Important factors for belonging to the non–s-ED group are presented to the left. Important factors for belonging to the s-ED group are presented to the right. The abbreviations are explained in Table 3.
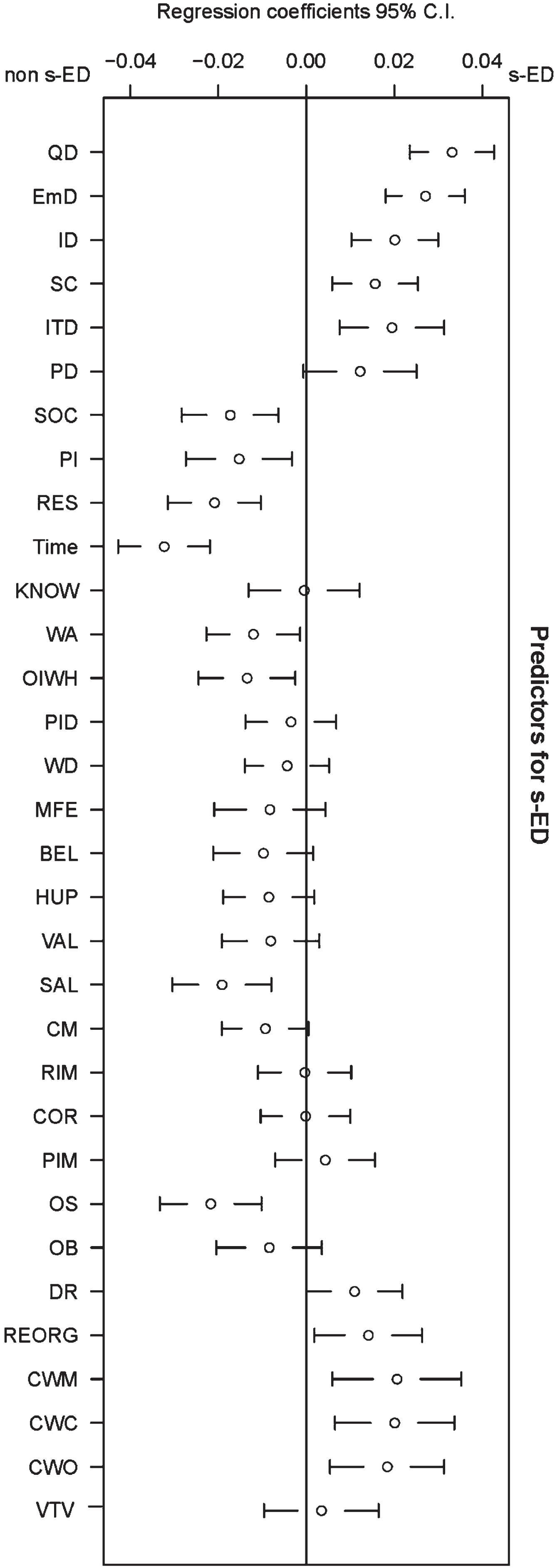
Table 3
Description of the 32 organizational and psychosocial environmental work factors in the PLSR model
| Factor | Abbreviation | Summary |
| Quantitative demands | QD | Working too fast, working too hard |
| Emotional demands | EmD | Understanding others’ situations, being exposed to difficult emotional situations at work |
| Intellectual demands | ID | Constantly learning new things, problem solving |
| Social competence | SC | Work requiring great social skills |
| IT demands | ITD | Being stressed by too many phone calls and e-mails, being interrupted, give quick replies |
| Physical demands | PD | Physically heavy work |
| Social support | SOC | Team cohesion at work, support from co-workers |
| Possibilities to influence | PI | Freedom to decide what to prioritize in work and how the work should be performed |
| Resources | RES | Enough staff, economic resources, and equipment |
| Time | Time | Enough time for work and for reflection |
| Knowledge | KNOW | Enough work-related knowledge and skills |
| Working autonomy | WA | Freedom at work to decide what to do |
| Opportunities to influence working hours | OIWH | Opportunities to affect working hours (start, stop, and break times and days at work) |
| Participation in decisions | PID | Involvement in decision making in the immediate workplace and overall organization |
| Workplace democracy | WD | Feeling opinions matter at work, having enough information before important decisions, shared participation in discussions |
| Manifested freedom of expression | MFE | Ability to express to the manager thoughts, feelings, and wishes about work |
| Belonging | BEL | Sense of belonging in the workplace |
| Human beings versus profitability | HUP | Caring for human beings as much as profitability |
| Values | VAL | Match between workplace and personal values |
| Salary | SAL | Satisfaction with salary |
| Confidence in management | CM | Confidence in workplace management |
| Relation to immediate manager | RIM | Relationship with immediate manager (does the manager listen, and give confirmation?) |
| Coordination | COR | Ability of manager to coordinate overall work operations |
| Presence of immediate manager | PIM | Presence of immediate manager in the workplace |
| Organizational structure | OS | Clear working rules and roles |
| Organizational barriers | OB | Obstacles to work created by organizational structures |
| Downsizing and relocation | DR | Downsizing and relocations in the workplace |
| Reorganization | REORG | Any workplace reorganization in the past 2 years |
| Conflicts with managers | CWM | Conflicts with managers in the past 2 years |
| Conflicts with co-workers | CWC | Conflicts with co-workers in the past 2 years |
| Conflicts with others | CWO | Conflicts with others in the past 2 years |
| Violence or threat of violence | VTV | Exposure to violence or threats of violence at work |
2.5Ethics
This study was approved by the Swedish Ethical Review Authority, Dnr 2017/495-31. Before we emailed the link to the questionnaire to potential participants, we informed them in an introductory letter about the voluntary nature of their participation and our assumption that their completion of the questionnaire would signify their consent to participate. Thereby, informed consent was obtained by all participants.
3Results
There were a total of 1093 municipal employees in the two rural areas of northern Sweden. Of these, 261 were men (23.9%) and 831 women (76.2%). The mean age was 45.1 years, and nearly half of the municipal employees had a university education (47.5%). The majority lived in Municipality 2 (75.8%), and the mean time as municipal employee was 15.2 years. Most employees worked in nursing (34.6%) or education (41.8%). Table 1 shows comparisons of background characteristics between municipal employees with or without s-ED. The s-ED group had a significantly lower mean age (mean = 42.4) compared to the non–s-ED group (mean = 45.8; p < 0.001; d = 0.281). Within the s-ED group, there was significantly higher proportion of women (85.0%) than men (15%; p < 0.001; φ= 0.108). A significantly higher proportion of employees in the non–s-ED group worked full time (73.7%), compared to the s-ED group (65.8%; p = 0.015; φ= 0.074).
Results of the univariate analyses are presented in Table 2. There were significant differences between the two groups regarding all factors except the knowledge factor. The s-ED group reported significantly higher quantitative (m = 1.70, CI: 1.63–1.77) and emotional demands (m = 1.44, CI: 1.38–1.51) than the non–s-ED group (m = 2.08, CI: 2.04–2.12; m = 1.78, CI: 1.73–1.82, d = 0.678). Social support from workplace colleagues was significantly higher among employees in the non–s-ED group (mean = 1.60, CI: 1.56–1.63) than in the s-ED group (mean = 1.97, CI: 1.88–2.06, d = 0.572). The employees in the non–s-ED group assessed having significantly more resources (m = 1.68, CI: 1.64–1.72) (i.e. enough staff, economic resources, and equipment) than the s-ED group (m = 2.10, CI: 2.01–2.19, d = 0.655). The employees in the non–s-ED group assessed having significantly more time for work and reflection (mean = 1.92, CI: 1.87–1.97) than the s-ED group (mean = 2.51, CI: 2.41–2.60, d = 0.813). Univariate results also showed that a significantly larger proportion of employees in the s-ED group reported conflicts with managers (21%, CI: 20.40–31.73) and co-workers (35%, CI: 29.29–41.65) compared to the non–s-ED group (managers: 10.3%, CI: 8.24–12.32; co-workers: 19.2%, CI: 16.52–21.80). The differences were small (managers: φ= –.189, co-workers: φ= –.160).
Compared to the national reference values (NRV) both the s-ED and the non–s-ED groups in this study assessed significantly higher emotional demands (NRV EmD = 2.28) and fewer resources (NRV RES = 1.5) as there were no overlapping CI; s (see above). Both groups also assessed being more frequently exposed to violence or threats of violence compared to the NRV (16.1%). In the S-ED group 32.1% of the employees assessed being exposed to violence or threats (CI: 26.02–38.07) and the corresponding figures for the employees in the non–s-ED group was (23.1%, CI: 20.30–25.96).
Compared to the national reference values the s-ED group reported less time for work (NRV Time = 2.1) and the non–s-ED group reported more time for work, as there were no overlapping CI; s. Compared to the national reference values the s-ED group assessed significantly higher quantitative demands (NRV QD = 2.10). Compared to the national reference values the s-ED group reported less social support (NRV SOC = 1.84), and the non–s-ED group reported more perceived social support, as there were no overlapping CI; s (see above). The s-ED group reported higher proportional exposure to conflicts with managers (26.1%, CI: 20.40–31.73%) and co-workers (35.5%, CI: 29.29–41.65) compared to the NRV; s (CWM = 18.3%, CWC = 20.3%).
The organizational and psychosocial environmental work factors in the PLSR model (Fig. 1) explained 21.0% of the variance in the response variable (s-ED/non–s-ED). Important factors of belonging to the s-ED group were different types of demands: quantitative, emotional, intellectual, and IT demands. Quantitative demands (having to work too fast or too hard) and emotional demands (understanding and being exposed to others’ often difficult emotional situations) were the most important types of demands belonging to the s-ED group. Other important factors were low social competence, reorganization, conflicts with managers, co-workers, and with others. Important factors for belonging to the non–s-ED group were social support, possibilities to influence, resources, time, work autonomy, opportunities to influence working hours, salary and organizational structure. All 32 factors (organizational and psychosocial work environmental factors) in the PLSR are summarized in Table 3. Regression coefficients, standard errors and p-values from jackknife t-tests are described in Table 4.
Table 4
Regression coefficients, standard errors and p-values from jackknife t-tests
| Factor | Regression coefficient | Standard error | p-value |
| QD | 0.0331 | 0.0049 | 1.7e-11 |
| EmD | 0.0271 | 0.0046 | 4.7e-09 |
| ID | 0.0201 | 0.0050 | 6.9e-05 |
| SC | 0.0157 | 0.0049 | 0.0017 |
| ITD | 0.0195 | 0.0061 | 0.0014 |
| PD | 0.0122 | 0.0066 | 0.0627 |
| SC | –0.0173 | 0.0056 | 0.0021 |
| PI | –0.0153 | 0.0062 | 0.0132 |
| RES | –0.0209 | 0.0054 | 0.0001 |
| Time | –0.0323 | 0.0053 | 1.6e-09 |
| KNOW | –0.0005 | 0.0064 | 0.9399 |
| WA | –0.0121 | 0.0054 | 0.0269 |
| OIWH | –0.0135 | 0.0056 | 0.0164 |
| PID | –0.0035 | 0.0053 | 0.5055 |
| WD | –0.0044 | 0.0049 | 0.3680 |
| MFE | –0.0083 | 0.0065 | 0.2001 |
| BEL | –0.0098 | 0.0058 | 0.0926 |
| HUP | –0.0085 | 0.0053 | 0.1063 |
| VAL | –0.0081 | 0.0056 | 0.1516 |
| SAL | –0.0192 | 0.0057 | 0.0008 |
| CM | –0.0093 | 0.0050 | 0.0630 |
| RIM | –0.0004 | 0.0054 | 0.9461 |
| COR | –0.0002 | 0.0052 | 0.9740 |
| PIM | 0.0043 | 0.0058 | 0.4573 |
| OS | –0.0218 | 0.0059 | 0.0002 |
| OB | –0.0084 | 0.0061 | 0.1695 |
| DR | 0.0109 | 0.0056 | 0.0499 |
| REORG | 0.0141 | 0.0062 | 0.0239 |
| CWM | 0.0206 | 0.0075 | 0.0060 |
| CWC | 0.0201 | 0.0069 | 0.0038 |
| CWO | 0.0184 | 0.0066 | 0.0055 |
| VTV | 0.0034 | 0.0067 | 0.6055 |
4Discussion
This cross-sectional study explored organizational and psychosocial environmental work factors among municipal employees with or without self-rated exhaustion disorder (s-ED) in rural northern Sweden. The results showed that there were significant differences between the s-ED and the non–s-ED group in all but one of the organizational and psychosocial environmental work factors. Various demands were associated with the s-ED group, and resources were associated with the non–s-ED group. Both groups assessed assess higher emotional demands and less resources compared to the national reference values.
An overall understanding is that the results from this study conform with the JD-R model [5], that demands can give rise to health impairment and burnout, while job resources buffer the health-impairing impact of demands and burnout model [7]. The overall results also point toward that access to various resources and lower demands can be protective factors against s-ED. One reflection is that it can be important for those working with improving occupational health in municipalities to be aware of these potentially protecting factors against ED. Such knowledge can be used in order to promote well-being among municipal employees. A recent review has described that ED is highly unexplored internationally, and that the medical diagnosis of exhaustion disorder has not yet been accepted into international versions of the ICD [52]. This means that straight forward comparisons to previous research of ED is limited. However, research has shown that ED overlaps with the concept of clinical burnout [13], consequently it seems reasonable to make comparisons to burnout and other stress-related disorders.
Both univariate and multivariate results showed that employees in the s-ED group reported higher quantitative and emotional demands than those in the non–s-ED group. These results are in line with previous results from several reviews concluding that quantitative and emotional demands are associated with increased emotional exhaustion and stress-related disorders [53, 54]. Multivariate results showed that the factor quantitative demands had the strongest association to the group of municipally employees with s-ED out of all factors in the present study. This is in accordance with a previous longitudinal study, that showed quantitative demands to have the largest impact on perceived effort (stress) compared to all the other job demands. Perceived effort in turn significantly increases burnout among nurses [55]. This can be problematic as results have shown that burnout is a significant factor of several negative physical and psychological consequences on workers well-being and health [56]. Burnout has also been shown to be associated with an increased intention to leave the nursing profession [55], decreased quality of care [57], negatively affect children’s academic skills if teachers suffer from feelings of burnout [58]. The results from a longitudinal study among working employees in Sweden showed that high demands were associated with greater risk of burnout, regardless of whether employees were working in a supportive or unsupportive work environment [59]. A cross-sectional and longitudinal study found that increased emotional demands were associated with increased exhaustion among Danish public service employees. Furthermore, high levels of quantitative demands were found to increase the effect of emotional demands on exhaustion [60]. Thus, in order to counteract such negative effects, it seems important to decrease levels of s-ED among municipal employees by organizing the workplaces in such a way that demands are decreased. It can be fruitful to try and specifically reduce quantitative demands. This may improve the well-being and health of those municipally employees at risk of becoming sick of ED and by extension improve the quality of their work in schools and in residential care of older people.
Univariate and multivariate results in the present study show that employees in the s-ED group reported more conflicts with managers and co-workers than those in the non–s-ED group. Between-group differences in exposure to conflict with managers and co-workers were small. A previous cross-sectional study among Finnish municipal employees showed that psychological harassment, workplace bullying, and injustice in the workplace were associated with exhaustion [61]. Workplace conflicts have also been reported in Sweden as important contributors to stress-related illness among people on sick leave for ED [18]. The present study also showed that both groups assessed being exposed to more violence or threats of violence compared to the NRV;s. Among municipal employees in Sweden, 27% (13% of the total labour market) have reported being exposed to violence or threat of violence [23]. A previous cross-sectional study showed that one third of public sector employees in Sweden were exposed to violence or threats of violence showed a relationship between work-related violence and poorer health [62]. Other research among human service sector occupations has found psychosocial work environment factors e.g. high quantitative and emotional demands, low organizational justice, and low level of influence over own work-situation to be were associated with work-related threats. High emotional demands, low quality of leadership and low support from nearest supervisor were some factors associated with workplace violence [63]. The results of the present study indicate how important it is for employers to deal with adverse organizational climates to limit risk factors for employees’ developing ED and consequently taking long-term sick leave.
Both univariate and multivariate results showed that the non–s-ED group reported having more social support, resources and time for work than the s-ED group. The between-group differences in mean scores for social support and resources were moderate, but large for the time factor. In addition, the results also showed that S-ED group reported less time for work and social support in contrast to the NRV;s. Furthermore, the non-s-ED group assessed more time for work and social support than the NRV;s. Previous reviews have concluded that employees who felt unsupported in the workplace developed more symptoms of ED [17, 64], and that good support at work can protect against ED [53]. Results of a previous cross-sectional study have shown an association between low social support and exhaustion among working employees in Sweden [65]. Findings from a qualitative study has found that people with ED on long-term sick leave consider the support of supervisors and co-workers important to their chances of regaining their ability to work [66]. Qualitative research among school principals has also shown the importance of social support from both managers and co-workers for occupational well-being [25], and the availability of workplace resources has been found to improve both employee well-being and work performance [67]. Time pressures, overtime requirements, lack of time for reflection at work or recovery after (all described as common in human service occupations), and lack of resources at work to meet these demands can upset employees’ work/life balance [68], and cause stress and exhaustion. Using the JD-R model, job resources (e.g., social support, autonomy) were negatively related to burnout [69], and positively related to employee well-being in Norway [70]. It seems important to focus on organizational and psychosocial protective factors: that is, to organize work such that employees have enough time both to perform and to reflect upon their work tasks. It is also important to provide sufficient economic and staff resources, as well as access to a supportive and present manager, to prevent s-ED in the vulnerable rural municipal services sector.
Interestingly, compared to the NRV;s both the s-ED and the non–s-ED groups in this study assessed higher emotional demands and fewer resources. Results also showed that s-ED group assessed higher quantitative demands than the NRV;s. Possible explanations for these results may partly be the population decline facing many rural areas both in Europe [71] and Sweden, and its consequences. Some financial and organizational consequences as centralise the care of the elderly, school closure, extensive budget cuts, shortage in the workforce in certain sectors, and difficulties recruiting for example certified nurses and teachers, which could in turn put added pressure on municipal employees in school and elderly care who are asked to do more with less. It may also be difficult change employers in a rural municipality [34]. Furthermore, employees in rural areas have been reported to have a different work situation than those in urban areas [72]. However, some of the challenges described above has also been reported to be present in municipalities in urban areas with a population increase [73, 74], and it is known that working in municipal sector is associated with stressful work environments [23]. Consequently, it is possible that the high demands and lack of resources is a consequence of the challenges facing municipalities, regardless if they are located in rural areas or not. Future studies are needed in order to explore this issue.
4.1Methodological discussion
It has been suggested that Cronbach’s alpha should be somewhere between 0.7–0.95 [75]. Two factors had Cronbach’s alpha values below the recommended interval: intellectual demands (α= 0.51) and downsizing and relocation (α= 0.55). However, it should be noted that these two factors only contain two items each and the low values can be an indication that some additional items are needed. Cronbach’s alpha values regarding the other factors where within the recommended interval and points toward satisfactory scale reliability. It should be noted that the response rate in this study of 52.6% is a cause of concern since it could indicate that non-response bias can be present. There were differences between responders and non-responders regarding profession and municipal belonging, but the effect sizes were small. Nursing staff, and non-office staff had the highest number of non-responders (58.4% and 61.1%). This was partly expected since previous research among healthcare professions has shown a similar response rate (56%) in postal surveys [76]. Research has shown that non-respondents had 20–30% higher sick-leave rate compared to respondents [77]. It is possible that the non-responders working as nursing staff, and non-office staff could suffer from more ill-health compared to other professions, and that the prevalence of s-ED was slightly underestimated in the current study. However, the results point towards the opposite. There was a significantly higher proportion of responders in municipal 1, and a significantly larger proportion of municipal employees with s-ED. This indicates that the potential problem of underestimating s-ED might be a limited problem. The response rate in this study is slightly higher than could be expected for web-based studies [78]. The sample can be regarded as nationally representative in terms of sex and age [79]. A limitation of this study is the cross-sectional design as no insights about causality can be provided. In addition, it should be noted that the NRV;s is based on a representative large sample of the working population in Sweden while the current study is based on a selected sample solely consisting of municipal employees in rural northern Sweden. Consequently, it is not possible to make a direct comparison and use proposed reference values based on the NRV data. It also should be noted that the current study may be at risk of common method variance (CMV) [80]. However, research has found that a relatively high level of CMV must be present to bias a true correlation between variables [81]. Many regression techniques perform poorly with large number of variables and when there are high co-variance values as the case in the current study. However, a strength with PLSR is that it works well with small samples and many variables and is robust with inadequacies such as high co-variance values [82].
5Conclusion
The results from this study are relevant to a better understanding what organizational and psychosocial work environmental factors the employer need to pay extra attention to, since this study provides increased knowledge of various work factors associated with s-ED and non-s-ED. This study shows that municipal employees with s-ED rated their total organizational and psychosocial work environment as poorer than did employees in the non–s-ED group, and that municipal employees in rural northern Sweden assess higher emotional demands and less resources compared to the national reference values. These are new insights, since such comparisons have not been made previously to our knowledge. Increased workplace awareness is important in identifying employees who experience adverse working conditions at an early stage. Addressing risk and protective factors in the work environment could tribute to promote occupational well-being, preventing exhaustion disorder and long-term sick leave. The risk and protective work factors could also be targets of future preventive workplace interventions among employees in the municipal sector in rural northern Sweden.
Ethical approval
This study was approved by the Regional Ethical Review Board in Sweden, Dnr 2017/495-31.
Informed consent
Informed consent was obtained from all participants.
Conflict of interest
The authors report no conflict of interest.
Funding
This study was funded by a Coordination Association of municipalities in northern Sweden.
Acknowledgments
The authors thank the participants in the two municipalities involved in this study.
References
[1] | Jood K , Karlsson N , Medin J , Pessah-Rasmussen H , Wester P , Ekberg K . The psychosocial work environment is associated with risk of stroke at working age. Scand J Work Environ Health. (2017) ;43: (4):367–74. |
[2] | Holmgren K , Fjällström-Lundgren M , Hensing G . Early identification of work-related stress predicted sickness absence in employed women with musculoskeletal or mental disorders: A prospective, longitudinal study in a primary health care setting. Disabil Rehabil. (2013) ;35: (5):418–26. |
[3] | Brown M . Responses to work intensification: Does generation matter? Int J Human Res Manage. (2012) ;23: (17):3578–95. |
[4] | Jacobsen S , Bramming P , Holt H , Larsen HH . Quality in modern nordic working life-investigating three related research perspectives and their possible cross-fertilization. Nordic J Work Life Stud. (2013) ;3: (3):47–80. |
[5] | Demerouti E , Bakker AB , Nachreiner F , Schaufeli WB . The job demands-resources model of burnout. J Appl Psychol. (2001) ;86: (3):499–512. |
[6] | Schaufeli WB , Taris TW . A critical review of the job demands-resources model: Implications for improving work and health. In: Bridging Occupational, Organizational and Public Health: A Transdisciplinary Approach. (2014) , pp. 43–68. |
[7] | Bakker A , Demerouti E , Sanz-Vergel A . Burnout and work engagement: The JD-R approach. Annu Rev Organ Psychol Organ Behav. (2014) ;1: (1):389–411. |
[8] | Schaufeli WB . Applying the job demands-resources model. Organ Dyn. (2017) ;46: (2):120–32. |
[9] | World Health Organization. Burn-out an “occupational phenomenon”. International Classification of Diseases. 2019. [cited 2022 March 22]. Available from: https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases |
[10] | Maslach C , Schaufeli W , Leiter M . Job burnout. Annu Rev Psychol. (2001) ;52: (1):397–422. |
[11] | Swedish National Board of Health andWelfare. Exhaustion disorder: Stress related mental ill health. 2003. No 2003-123-18 |
[12] | Swedish National Board of Health and Welfare. International statistical classification of diseases and related healh problems. 2022. [cited 2022 September 7]. Available from: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/klassifikationer-och-koder/2022-1-7717.pdf |
[13] | Grossi G , Perski A , Osika W , Savic I . Stress-related exhaustion disorder - clinical manifestation of burnout? A review of assessment methods, sleep impairments, cognitive disturbances, and neuro-biological and physiological changes in clinical burnout. Scand J Psychol. (2015) ;56: (6):626–36. |
[14] | Glise K , Ahlborg G Jr , Jonsdottir IH . Course of mental symptoms in patients with stress-related exhaustion: Does sex or age make a difference? BMC Psychiatry. (2012) ;12: :18. |
[15] | Adamsson A , Bernhardsson S . Symptoms that may be stress-related and lead to exhaustion disorder: A retrospective medical chart review in Swedish primary care. BMC Fam Pract. (2018) ;19: (1):172. |
[16] | Swedish Social Insurance Agency. Social Insurance Report 2020:8. Mental disorder sick leave – A register study of the Swedish working population in ages 20 to 69 years. 2020. [cited 2022 March 22]. Available from: https://www.forsakringskassan.se/wps/wcm/connect/e12b777c-e98a-488d-998f-501e621f4714/sjukfranvaro-i-psykiatriska-diagnoser-socialforsakringsrapport-2020-8.pdf?MOD=AJPERES&CVID= |
[17] | Swedish Agency for Health Technology Assessment of Social Services. Occupational exposures and symptoms of depression and exhaustion disorder. Report no. 223. Stockholm: SBU. 2014. [cited 2022 March 22]. Available from: https://www.sbu.se/contentassets/800ad7aecf9146c795d3a89c7a957048/arbetsmiljo_depression_2014.pdf |
[18] | Hasselberg K , Jonsdottir IH , Ellbin S , Skagert K . Self-reported stressors among patients with Exhaustion Disorder: An exploratory study of patient records. BMC Psychiatry. (2014) ;14: (1):66–66. |
[19] | Glise K , Hadzibajramovic E , Jonsdottir IH , Ahlborg G . Self-reported exhaustion: A possible indicator of reduced work ability and increased risk of sickness absence among human service workers. Int Arch Occup Environ Health. (2010) ;83: (5):511–20. |
[20] | Ahlborg G Jr , Hultberg A , Hadžibajramović E , et al. The KART-study. Work environment, stress and health among employees in the region of Västra Götaland. ISM Report no. 17. Stockholm: Institute of Stress Medicine. 2016. [cited 2022 March 22]. Available from: https://www.vgregion.se/ov/ism/isms-forskning/arbetsliv/organisation-och-ledarskap/kart-studien/ |
[21] | Lexén A , Kåhlin I , Erlandsson LK , Håkansson C . Occupational health among swedish occupational therapists: A cross-sectional study. Int J Environ Res Public Health. (2020) ;17: (10):3379. |
[22] | Persson R , Österberg K , Viborg N , Jönsson P , Tenenbaum A . The Lund University Checklist for Incipient Exhaustion-a cross-sectional comparison of a new instrument with similar contemporary tools. BMC Public Health. (2016) ;16: (1):350. |
[23] | Swedish Municipalities and Regions. Work environment in municipalities and regions. 2021. [cited 2022 June 22]. Available from: https://skr.se/skr/tjanster/rapporterochskrifter/publikationer/arbetsmiljonikommunerochregioner.64608.html |
[24] | Skaalvik EM , Skaalvik S . Job satisfaction, stress and coping strategies in the teaching profession-what do teachers say? Int Educ Stud. (2015) ;8: (3):181–92. |
[25] | Elomaa M , Eskelä-Haapanen S , Pakarinen E , Halttunen L , Lerkkanen MK . Work-related stress of elementary school principals in Finland: Coping strategies and support. Educ Manag, Adm & Lead. (2021) ;1–21. |
[26] | Sjöberg A , Pettersson-Strömbäck A , Sahlén KG , Lindholm L , Norström F . The burden of high workload on the health-related quality of life among home care workers in Northern Sweden. Int Arch Occup Environ Health. (2020) ;93: (6):747–64. |
[27] | Persson R , Leo U , Arvidsson I , Håkansson C , Nilsson K , Österberg K . Prevalence of exhaustion symptoms and associations with school level, length of work experience and gender: A nationwide cross-sectional study of Swedish principals. BMC Public Health. (2021) ;21: (1):331. |
[28] | Larsson R , Akerlind I , Sandmark H . Managing workplace health promotion in municipal organizations: The perspective of senior managers. Work. (2016) ;53: (3):485–98. |
[29] | Swedish Association of Local Authorities and Regions. Sick absence in municipalities and regions. 2017. [cited 2022 March 22]. Available from: https://skr.se/tjanster/merfranskr/rapporterochskrifter/publikationer/sjukfranvaroikommunerochlandsting.27519.html |
[30] | Aronsson G , Astvik W , Gustafsson K . Work Conditions, Recovery and Health: A Study among Workers within Pre-School, Home Care and Social Work. British J Soc Work. (2014) ;44: (6):1654–72. |
[31] | Agosti MT , Andersson I , Ejlertsson G , Janlöv AC . Shift work to balance everyday life - a salutogenic nursing perspective in home help service in Sweden. BMC Nurs. (2015) ;14: (1):2. |
[32] | Persson SS , Lindström PN , Pettersson P , Andersson I . Workplace relationships impact self-rated health: A survey of Swedish municipal health care employees. Work. (2018) ;60: (1):85–94. |
[33] | Åkerlind IL , Ljungblad RC . Leadership, social climate, health promotion measures and sick leave a comparative study in health and care in 60 municipalities. Socialmedicinsk Tidskrift. (2013) ;90: (6):799–809. |
[34] | Syssner J . Pathways to Demographic Adaptation: Perspectives on Policy and Planning in Depopulating Areas in Northern Europe. 1st ed. Cham: Springer International Publishing; (2020) . |
[35] | Eurostat. Self-assessment of health, by degree of urbanization. 2013. [cited 2022 March 22]. Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=File:Self-assessment_of_health,_by_degree_of_urbanisation,_2013_(%C2%B9)_(%25_of_persons_aged_18%E2%80%9364_assessing_their_own_health_as_bad_or_very_bad)_RYB15.png |
[36] | Eurostat. Eurostat regional yearbook. 2017. [cited 2022 June 22]. Available from: https://ec.europa.eu/eurostat/documents/3217494/8222062/KS-HA-17-001-EN-N.pdf/eaebe7fa-0c80-45af-ab41-0f806c433763 |
[37] | Bremberg S . Rural-urban mortality inequalities in four Nordic welfare states. Scand J Public Health. (2020) ;48: (8):791–3. |
[38] | Lindroth M , Lundqvist R , Lilja M , Eliasson M . Cardiovascular risk factors differ between rural and urban Sweden: The Northern Sweden MONICA cohort. BMC Public Health. (2014) ;14: (1):825. |
[39] | Lidwall U , Bill S , Palmer E , Olsson Bohlin C . Mental disorder sick leave in Sweden: A population study. Work. (2018) ;59: (2):259–72. |
[40] | Asplund S , Åhlin J , Åström S , Hedlund M , Lindgren BM , Ericson-Lidman E . Self-rated exhaustion disorder and associated health-related factors among municipal employees in rural areas of northern Sweden. Int Arch Occup Environ Health. (2020) ;94: (4):659–68. |
[41] | Swedish Board of Agriculture. Our definition of rural areas. 2015. [cited 2022 March 22]. Available from: https://jordbruksverket.se/stod/programmen-som-finansierar-stoden/var-definition-av-landsbygd |
[42] | Muilu T . Needs for rural research in the northern Finland context. J Rural Stud. (2010) ;26: (1):73–80. |
[43] | Statistics Sweden. Municipalites in numbers. 2021. [cited 2022 March 22]. Available from: https://kommunsiffror.scb.se/ |
[44] | Oxenstierna G , Widmark M , Finnholm K , Elofsson S . A new questionnaire and model for research into the impact of work and the work environment on employee health. Scand J Work Environ Health. (2008) ;(Suppl 6):150–62. |
[45] | Oxenstierna G , Widmark M , Finnholm K , Elofsson S . Psychosocial factors in today‘s working life, and how to measure and describe them. Stress Research Report no. 320. (2008) . Stockholm: Stress Research Institute. |
[46] | Kinsten A , Magnusson Hanson L , Hyde M , Oxenstierna G . SLOSH – Swedish Longitudinal Occupational Survey of Health – a nationally representative psychosocial survey of the Swedish working population. Stress Research Report No 321. (2007) . Stockholm: Stress Research Institute. |
[47] | Magnusson Hanson LL , Leineweber C , Persson V , Hyde M , Theorell T , Westerlund H . Cohort profile: The Swedish longitudinal occupational survey of health (SLOSH). Int J Epidemiol. (2018) ;47: (3):691-692i. |
[48] | IBM. IBM SPSS statistics for Windows. Version 25.0. Armonk, NY: IBM Corp; 2017. |
[49] | Cohen J . Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates; (1988) . |
[50] | Pallant J . SPSS survival manual: A step by step guide to data analysis using IBM SPSS. 5th ed. Maidenhead: Open University Press; (2016) . |
[51] | Mevik BH , Cederkvist HR . Mean squared error of prediction (MSEP) estimates for principal component regression (PCR) and partial least squares regression (PLSR). J Chemomet. (2004) ;18: (9):422–9. |
[52] | Lindsäter E , Svärdman F , Wallert J , Ivanova E , Söderholm A , Fondberg R , et al. Exhaustion disorder: Scoping review of research on a recently introduced stress-related diagnosis. BJPsych Open. (2022) ;8(5). |
[53] | Aronsson G , Theorell T , Grape T , Hammarström A , Hogstedt C , Marteinsdottir I , et al. A systematic review including meta-analysis of work environment and burnout symptoms. BMC Public Health. (2017) ;17: (1):264–264. |
[54] | Seidler A , Thinschmidt M , Deckert S , Then F , Hegewald J , Nieuwenhuijsen K , et al. The role of psychosocial working conditions on burnout and its core component emotional exhaustion - a systematic review. J Occup Med Toxicol. (2014) ;9: (1):10. |
[55] | Van der Heijden B , Brown Mahoney C , Xu Y . Impact of job demands and resources on nurses’ burnout and occupational turnover intention towards an age-moderated mediation model for the nursing profession. Int J Environ Res Public Health. (2019) ;16: (11):1–22. |
[56] | Salvagioni DAJ , Melanda FN , Mesas AE , et al. Physical, psychological and occupational consequences of job burnout: A systematic review of prospective studies. PLoS ONE. (2017) ;12: (10):e0185781. |
[57] | Tawfik DS , Scheid A , Profit J , Shanafelt T , Trockel M , Adair KC , et al. Evidence relating health care provider burnout and quality of care a systematic review and meta-analysis. Ann Intern Med. (2019) ;171: (8):555–67. |
[58] | Klusmann U , Kunter M , Trautwein U , Lüdtke O , Baumert J . Teachers’ occupational well-being and quality of instruction: the important role of self-regulatory patterns. J Educ Psychol. (2008) ;100: (3):702–15. |
[59] | Fagerlind Ståhl AC , Ståhl C , Smith P . Longitudinal association between psychological demands and burnout for employees experiencing a high versus a low degree of job resources. BMC Public Health. (2018) ;18: (1):915. |
[60] | Vammen MA , Mikkelsen S , Forman JL , Hansen ÅM , Bonde JP , Grynderup MB , et al. Emotional demands and exhaustion: Cross-sectional and longitudinal associations in a cohort of Danish public sector employees. Int Arch Occup Environ Health. (2019) ;92: (5):639–50. |
[61] | Helkavaara M , Saastamoinen P , Lahelma E . Psychosocial work environment and emotional exhaustion among middle-aged employees. BMC Res Notes. (2011) ;4: (1):101. |
[62] | Vaez M , Josephson M , Vingård E , Voss M . Work-related violence and its association with self-rated general health among public sector employees in Sweden. Work. (2014) ;49: (1):163–71. |
[63] | Andersen LP , Hogh A , Biering K , Gadegaard CA . Work-related threats and violence in human service sectors: The importance of the psycho-social work environment examined in a multilevel prospective study. Work. (2018) ;59: (1):141–54. |
[64] | Nieuwenhuijsen K , Bruinvels D , Frings-Dresen M . Psychosocial work environment and stress-related disorders, a systematic review. Occup Med. (2010) ;60: (4):277–86. |
[65] | Lindeberg SI , Rosvall M , Choi B , Canivet C , Isacsson SO , Karasek R , et al. Psychosocial working conditions and exhaustion in a working population sample of Swedish middle-aged men and women. Euro J Public Health. (2011) ;21: (2):190–6. |
[66] | Norlund S , Fjellman-Wiklund A , Nordin M , Stenlund T , Ahlgren C . Personal resources and support when regaining the ability to work: An interview study with exhaustion disorder patients. J Occup Rehabil. (2013) ;23: (2):270–9. |
[67] | Nielsen K , Nielsen MB , Ogbonnaya C , Känsälä M , Saari E , Isaksson K . Workplace resources to improve both employee well-being and performance: A systematic review and meta-analysis. Work and Stress. (2017) ;31: (2):101–20. |
[68] | Corin L , Björk L . Job demands and job resources in human service managerial work: An external assessment through work content analysis. Nordic J Work Life Stud. (2016) ;6: (4):3–28. |
[69] | Kaiser S , Patras J , Adolfsen F , Richardsen AM , Martinussen M . Using the job demands–resources model to evaluate work-related outcomes among norwegian health care workers. SAGE Open. (2020) ;10(3). |
[70] | Langseth-Eide B , Vittersø J . Ticket to ride: A longitudinal journey to health and work-attendance in the jd-r model. Int J Environ Res Public Health. (2021) ;18: (8):4327. |
[71] | Hospers G-J . Coping with shrinkage in Europe’s cities and towns. Urban Des Int. (2013) ;18: (1):78–89. |
[72] | Abelsen B , Strasser R , Heaney D , Berggren P , Sigurðsson S , Brandstorp H , et al. Plan, recruit, retain: A framework for local healthcare organizations to achieve a stable remote rural workforce. Human Res Health. (2020) ;18: (1):63. |
[73] | Nyström K . Recruitment of scarce competences to rural regions: Policy perspectives. Rev Reg Res. (2021) ;41: :211–27. |
[74] | Swedish Association of Local Authorities and Regions. Urbanization - challenges for municipalities with a growing and declining population. 2015. [cited 2022 March 22]. Available from: https://skr.se/skr/tjanster/rapporterochskrifter/publikationer/urbaniseringutmaningarforkommunermedvaxandeochminskandebefolkning.65685.html |
[75] | Peterson RA . A meta-analysis of cronbach’s coefficient alpha. The Journal of Consumer Research. (1994) ;21: (2):381–91. |
[76] | Cook JV , Dickinson HO , Eccles MP . Response rates in postal surveys of healthcare professionals between and An observational study. BMC Health Serv Res. (2009) ;9: (1):160. |
[77] | Martikainen P , Laaksonen M , Piha K , Lallukka T . Does survey non-response bias the association between occupational social class and health? Scand J Public Health. (2007) ;35: (2):212–5. |
[78] | Blumenberg C , Barros AJD . Response rate differences between web and alternative data collection methods for public health research: a systematic review of the literature. Int J Public Health. (2018) ;63: (6):765–73. |
[79] | Swedish Association of Local Authorities and Regions. Municipal employees. 2018. [cited 2022 March 22]. Available from: https://skr.se/skr/arbetsgivarekollektivavtal/uppfoljninganalys/personalstatistik/personalenisiffror/tabellerkommunalpersonal2021/tabellerkommunalpersonal2018.47122.html |
[80] | Podsakoff PM , MacKenzie SB , Lee JY , Podsakoff NP . Common method biases in behavioral research: A critical review of the literature and recommended remedies. J Appl Psychol. (2003) ;88: (5):879–903. |
[81] | Fuller CM , Simmering MJ , Atinc G , Atinc Y , Babin BJ . Common methods variance detection in business research. J Bus Res. (2016) ;69: (8):3192–8. |
[82] | Haenlein M , Kaplan AM . A beginner’s guide to partial least squares analysis. Understanding Statistics. (2004) ;3: (4):283–97. |


