
Complex systems design based on actual system functioning: Coping with variability in a national water ambulances service
Abstract
BACKGROUND:
In Brazil, the Mobile Emergency Medical Service (SAMU) is a model of mobile assistance and care for emergencies standardized throughout the country. The water ambulance service within the SAMU operates in riverside and coastal areas, and faces challenges and peculiarities that increase the complexity of providing a high-quality and safe emergency care service.
OBJECTIVE:
To develop organizational design guidelines aiming to improve resilient performance of complex systems, with an application to riverine and coastal mobile emergency care in Brazil.
METHODS:
Data collection followed an ethnographic approach. Fieldwork was carried in a participatory way, based on worksite technical description, semi-structured interviews with managers and emergency care teams’ professionals, and work observation whenever possible. Five regional SAMU coordinations were visited. Data coding employed content analysis and grouped data excerpts according to concepts of capacity and demand. Interfaces were identified between demand and capacity elements and adaptations led by system agents, orienting the proposal of guidelines for organizational design as solutions to face the verified gaps.
RESULTS:
Design guidelines produced spanned composition and training of both intervention teams and dispatch central teams, uniforms and personal protective equipment (PPE), decentralized water bases, means of communication, intervention protocols, biosafety and inter-sector actions.
CONCLUSION:
The approach enabled framing and assessment of specific design elements according to resilience engineering concepts, which in turn showed paths for improving the service and reconciling work-as-imagined and actual system functioning.
1Introduction
In Brazil, the Mobile Emergency Medical Service (SAMU) is a model of mobile assistance and care for emergencies standardized throughout the country. As first responders within emergency pre-hospital care [1], SAMU is part of the Brazilian Unified Healthcare System (SUS) and covers about 83% of the country’s population (about 170 million people) [2]. Inspired by the French model, it is available 24 hours a day, providing on-scene emergency care for patients instead of just transport to healthcare facilities [3].
Launched in 2003 by the Federal Government as part of the National Emergency Care Policy [4], SAMU provides emergency medical care anywhere: residences, worksites, and public locations. The service operates through toll-free phone calls arriving at an Emergency Dispatch Center (CRU). The calls are received by the Medical Regulation Attendance Technician (TARM), who writes down the description of what happened and the patient’s health conditions. Then they send this information to the regulatory physician who verifies the gravity of the case and the need to send or not a basic ambulance - without the presence of a doctor - or an advanced ambulance - with the presence of a doctor.
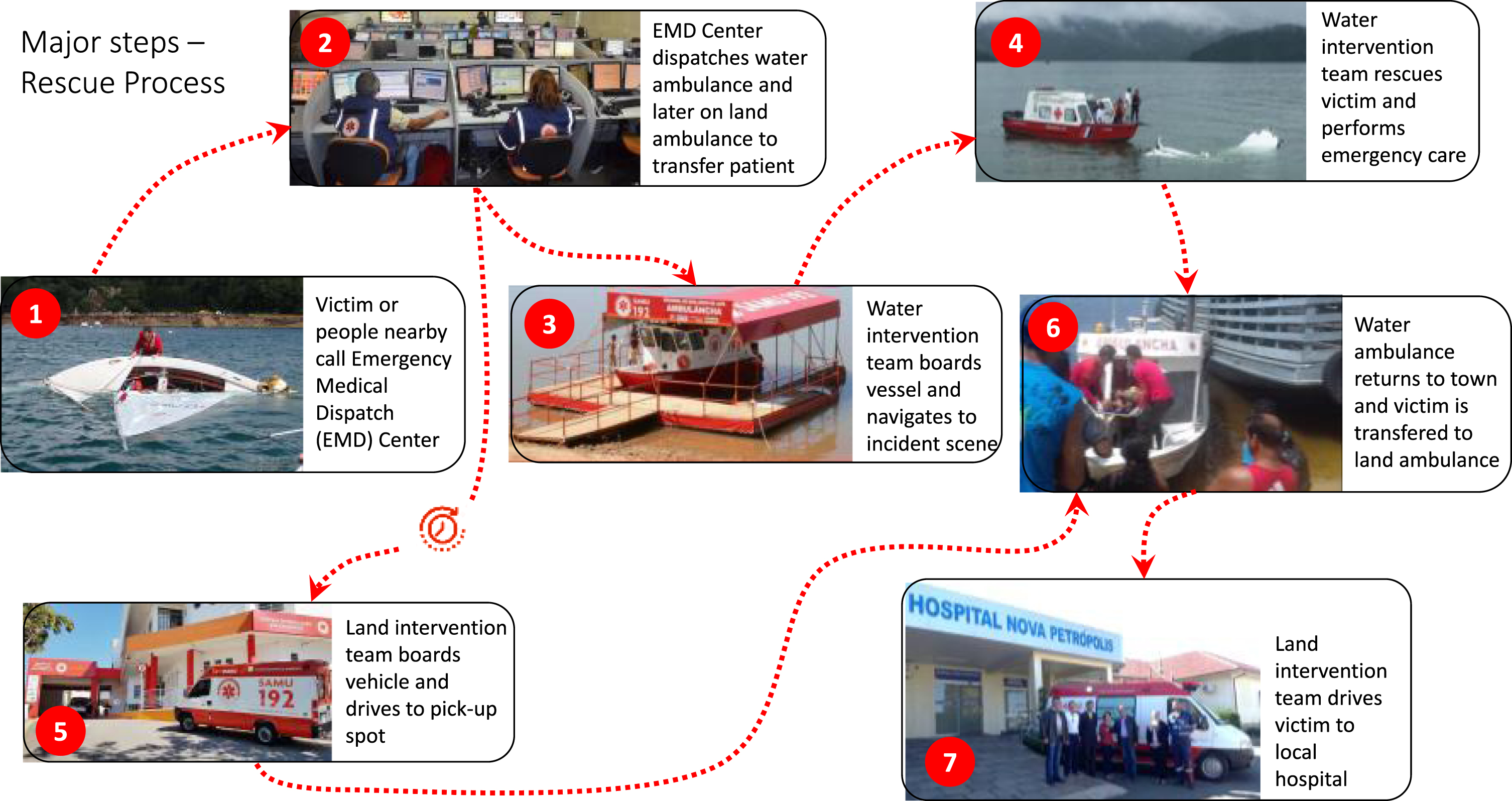
The watercraft modality of the SAMU operates in riverside and coastal areas, and the vessels are commonly called “ambulanchas.” In this article, we will use the term “water ambulances” to refer to these boats. The main process performed by the water ambulance service is the rescue process, illustrated in Fig. 1. This type of service faces challenges and peculiarities such as changing navigability conditions, the difficulty of hiring and retaining qualified workers, adverse geographic conditions and limited communication between teams [5]. These features, as well as other sources of variability internal and external to the service increase the complexity of providing a high-quality and safe emergency care service [5].
Fig. 1
General SAMU rescue process for providing mobile emergency care to riverine and coastal populations.
In this paper we addressed the problem of managing variability in complex socio-technical systems through organizational design. Specifically, we explored how organizational design can offer support to complex and safety-critical domains in coping with complexity by means of variability management to reconcile Work-as-Imagined (WAI) and Work-as-Done (WAD). As a research approach to tackle this problem, we applied a research design combining: (a) fieldwork and data collection using an ergonomic ethnographic approach; and (b) data coding and analysis using content analysis and concepts from resilience engineering [6].
We employed this approach to develop a proposal for organizational design guidelines aiming to improve the resilient performance of riverine and coastal mobile emergency care in Brazil. Resilience Engineering states that one cannot prescribe the system’s performance as policy makers and system designers imagined, and some degrees of variability, flexibility, and adjustments are required to keep the system functioning well. This means that in truly resilient systems, it is not possible to completely realign Work-as-Imagined (WAI) and Work-as-Done (WAD). As such, this gap should be acknowledged, and adaptations that lead to good outcomes should be supported [7, 8]. While WAI can be considered the attempt to align a system’s capacity with its demands by the organization [9, 10], demand and capacity really can never be fully aligned due to the complex dynamic interplay between them. Therefore, WAD comprises adjustment maneuvers needed to cope with mismatches, generally leading to success but sometimes also leading to failures.
In our work, our aim was to understand the gaps between system demands, available resources or capacities, and adaptations by system agents to cope with these gaps, revealing focal points for intervention and enabling the development of guidelines that reconcile or align system demands to possibilities of adaptation, turning the service resilient to circumstances of actual system functioning.
Thus, this work sought to describe the dynamics of actions in this system, making it possible to understand its real operation and proposing useful and applicable guidelines that can support municipalities in the implementation and maintenance of the service, as well as an adequate structuring of the water ambulance service within the framework of urgency and emergency already regulated by the Ministry of Health.
2Methods
This work is part of a research project whose aim was to support the incorporation of the water ambulance service - a part of the Brazilian Mobile Emergency Medical Service (SAMU) – into the country’s National Emergency Care Policy. We visited and interviewed operators and managers of dispatch centrals, decentralized bases, water ambulances, disembark points, and healthcare facilities across five of the six regional SAMU coordinations qualified by the Ministry of Health to operate the water ambulance service.
Research was divided into two stages. In the first stage the diagnosis of the service in different regional coordinations of riverine SAMU was carried out, covering almost all municipalities that have the service enabled in Brazilian territory. At this stage, the characterization of the operation of the service in each region was done, including the production of regional maps of service operation, the characterization and technical drawings of the vessels in operation, and the identification of the main difficulties faced by the teams for the operationalization of the service.
The second stage addressed the formulation of proposals to help incorporate the ambulance component into the National Policy for Emergency Care. At this stage, normative guidelines were produced to support the implementation and maintenance of the service.
2.1Research design
The study followed an exploratory cross-sectional design, based on qualitative data collected following an ethnographic approach to understand the operation of riverine and coastal mobile emergency care. This choice of research design reflected a perspective on complex systems that stems from the fields of participatory ergonomics and resilience engineering. These fields have posed as a cornerstone for analysis and design of such systems, the understanding of how work is really done and how interdependencies between human, technological and organizational factors play out.
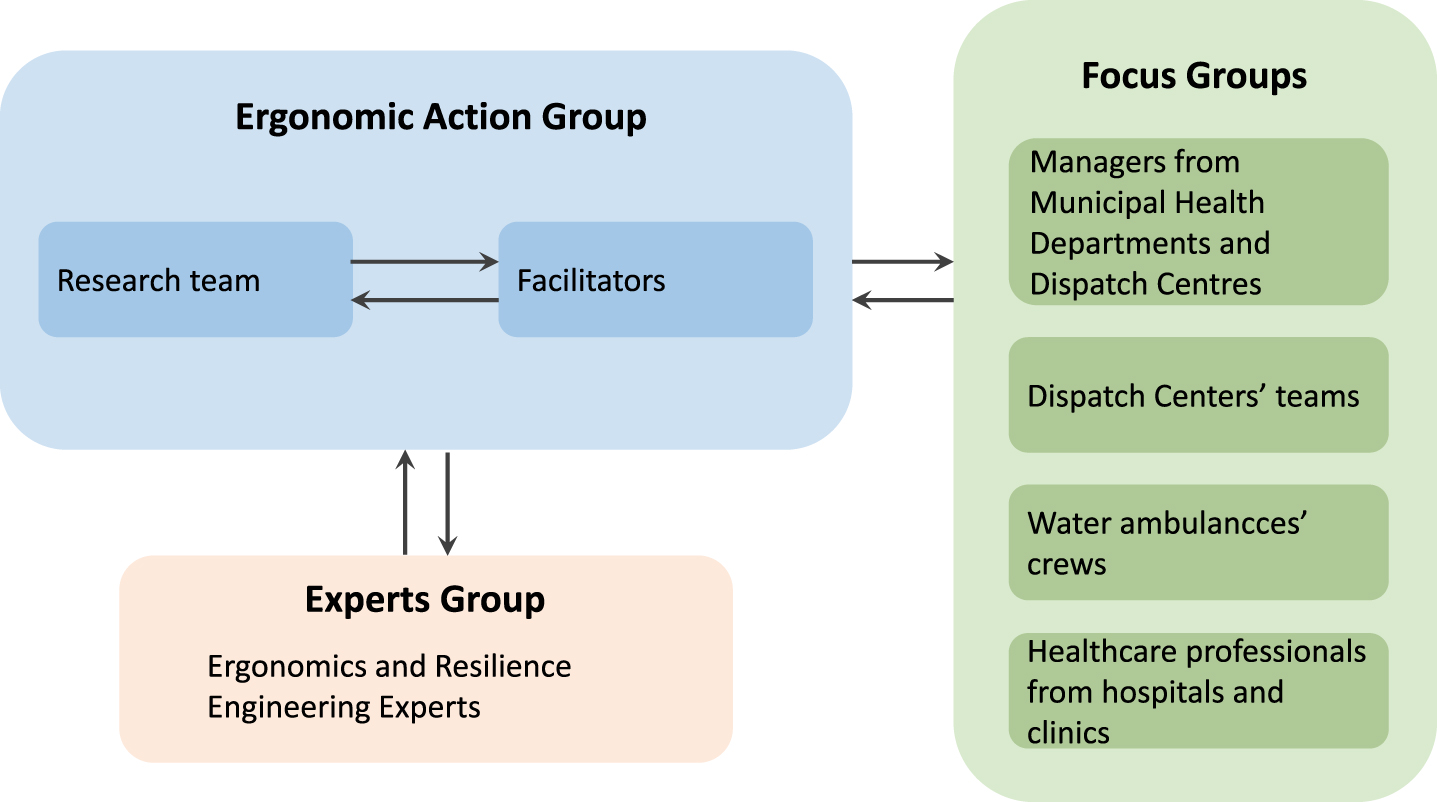
In this context, fieldwork was carried out in a participatory way and was based on semi-structured interviews, worksite technical description and naturalistic work observation whenever possible. Social construction enabled the involvement of the research team with the community of professionals from SAMU across different regional coordinations, as shown in Figure 2.
Fig. 2
Social construction for research activities.
To carry out the study, document analysis was initially carried out on legal and technical documentation regarding Brazilian emergency care, SAMU and the water ambulance service. Then, visits were carried out to five of the six regional coordinations of riverine and coastal SAMU where this service is implemented and authorized by the Ministry of Health in the country. The regional coordinations visited were: Ilha Grande Bay, in Rio de Janeiro, Salvador and Bom Jesus da Lapa, in Bahia, Manaus and Alto Solimões, in Amazonas, totaling nine municipalities visited that operate the SAMU water ambulance service. To assist the team in framing data collection research design, a pilot visit was organized to Ilha Grande Bay, the closest regional coordination to the research team, consisting of a two-day workshop that comprised:
• A presentation of the research project’s aims;
• A brief guided visit to the local SAMU facilities and other healthcare units;
• A series of talks between the researchers, local SAMU managers and water ambulance crews on the main steps of the rescue process and obstacles faced during expeditions;
• Observation of a water ambulance rescue.
2.2Data collection
Fieldwork was conducted by a multidisciplinary research team consisting of the same three researchers across all visits. Researchers were instructed to document as much as possible the interactions through field notes, hot reports, audio/video records, and photos (when allowed). Participants in the study spanned managers from Municipal Health Departments, SAMU, and other local healthcare facilities, as well as emergency care teams’ professionals, such as doctors, nurses, health attendants and boat drivers. 101 professionals were interviewed, including around 80% of SAMU water ambulance crews in Brazil. Approximately 270 hours were needed for fieldwork, spanning a 40-day time period. Participants were selected according to a “snowball” sampling method [11]. We monitored the content of ‘interviews’ outputs and claimed saturation when participants’ responses started showing significant similarities.
Interviewees were classified into four different groups:
• Managers from the regional Dispatch Centre and decentralized bases;
• Professionals from the Dispatch triage team;
• Professionals from water ambulance crews;
• Managers and professionals from healthcare facilities in the regions that receive patients from SAMU mobile teams.
Interviews focused on identifying the difficulties that participants face while carrying out their activities and the main problems concerning the boats and navigability in waterways in which they operate at the coastal and riverine communities in the regions. Interviews also included descriptions of how variability unfolded during service operation and narratives of challenging cases in providing care and dealing with incidents during expeditions. The description of variability was later used to analyze gaps between demand and capacity, and how workers adapt to fill into these gaps, ultimately providing the research team insight into how each misalignment should be coped with.
Data collection took into consideration this system’s organizational context, related to its “blunt end” (administrative structure, relationship with municipal and state management, availability of human and material resources, and local protocols). Additionally, other elements of the work environment were considered, such as those related to its “sharp-end” (communication instances, geographic and climatic factors, and population’s epidemiological aspects). Data collection protocols for the interviews and naturalistic observation can be found elsewhere [5].
Fieldwork was organized into the following steps:
1. Guided visits to the regional Dispatch Centre and decentralized operational bases that host the water ambulance crews in each region’s municipalities;
2. Semi-structured interviews with Dispatch managers, health managers at the municipal level, Dispatch triage team, members of the water ambulance crews, and managers and professionals from healthcare units in the regions;
3. Inspection, description and technical drawing of the water ambulances and their docking locations;
4. Navigation aboard water ambulances; and
5. Simulation of an emergency operation (available at one of the locations);
At all municipalities, guided visits to operational bases and interviews with local managers preceded the other steps, as a first point of contact between the research team and local professionals. The remaining steps were ordered according to availability of crews and other healthcare professionals. At the end of each working day, the three researchers composing the fieldwork research team conducted a meeting where individual field notes went through screening for inconsistencies, discussion and organization.
2.3Data coding and analysis
Field notes and the transcription of interviews underwent content analysis [12] looking for trends, characteristics, and interpretation of the data. Data collected using the inclusion/framework matrix tool [13, 14], following the content analysis guidelines of [12, 15]. Data coding thus employed content analysis conducted along the following phases: (i) organization of collected data and definition of registry unit; (ii) categorization of discourse elements; (iii) contextualization highlighting consensus, controversies and contradictions; (iv) analysis toward tendencies, characteristics and interpretation.
Definition of analysis themes sought to adhere to the main principles for content analysis [15, 16]:
• Formalization: unique and cohesive criteria for establishing the categories;
• Exhaustiveness: categories able to cover the totality of the speech elements to be classified;
• Exclusivity: maximization of inter-group variance;
• Homogeneity: minimization of intra-group variance.
The unit of coding within the statements was defined as the phrase/sentence described by the respondent. Then, the categories were listed in order to allow the alignment of the analysis with the objective of this study, considering that a significant part of the registration units dealt with the alignment or misalignment between the demands imposed on the ambulance service and the capacity available for the operation of the same.
Next, the definition of categories was carried out in two large groups, called Capacity and Demand [9, 17]. A focus question was defined for each category to aggregate speeches. For the Capacity category, the focus question was “What should be the elements to be regulated for the ambulance component of SAMU?” For the Demand category, the focus question was “What are the elements that impact the SAMU indicators regarding the ambulance component?” where the indicators are those applicable to the ambulance service that are described in the National Policy for Emergency Care.
The establishment of categories sought to comply with the principles described by [16, 18, 19], highlighting: (a) formalization - uniqueness in the criteria for establishing categories, allowing a clear definition of them and cohesive rules of inclusion and exclusion; (b) exhaustiveness - coverage of the categories on the totality of the speech elements to be classified; (c) exclusivity – mutually exclusive categories (maximization of between-group variance); and (d) homogeneity – internally as narrow categories as possible (minimization of intra-group variance).
In order to develop the guidelines taking into account the system actual functioning, interfaces were identified in the data between situation demands, capacity elements and adaptations led by system agents, evidencing gaps between demand and capacity, and how workers adapt to fill into such gaps. Three members of the research team independently iteratively screened the data to locate and list these interface points cumulatively, discussing results afterwards. In this way, it was possible to see which incident pressures (demands) on the waterway emergency mobile care system were not well attended by which resources made available for the operation of the system (capacity), and gain insight on how to best cope with them.
Finally, aiming at subsidizing the regulation of the SAMU waterway component, guidelines for the regulation of the ambulance service were proposed as solutions to face the verified misalignments. These ambulance service specifications were created seeking to align capacity with demand and facilitate adaptations when necessary. The following section describes the results obtained in this methodological process and summarizes the elaborated proposals - originally formulated in the form of normative items - for all organizational elements of the service.
All the proposals were finally validated with key members from all the regional coordinations visited.
3Results
Preliminary data coding - aimed to support the research team in modelling and analyzing demand x capacity misalignments - produced: (a) technical drawings of the currently employed water ambulances; (b) description of team composition, main processes carried out and obstacles to the service; and (c) operation maps, comprising delimitation of serviced area, average response time to communities, as well as location of stations and disembark points for each water ambulance team. These spanned coastal areas at islands, open-sea shores, large bays, semi-arid riverine and Amazonian riverine regions. Figure 3 shows the operation map produced for the SAMU regional coordination of Manaus, capital of the state of Amazonas. Figure 4 shows the technical drawings and produced for the main water ambulance in operation in Manaus, while Fig. 5 shows the water ambulance moored at one of the serviced communities.
Fig. 3
Operation map for the regional coordination of Manaus, Amazonas state.
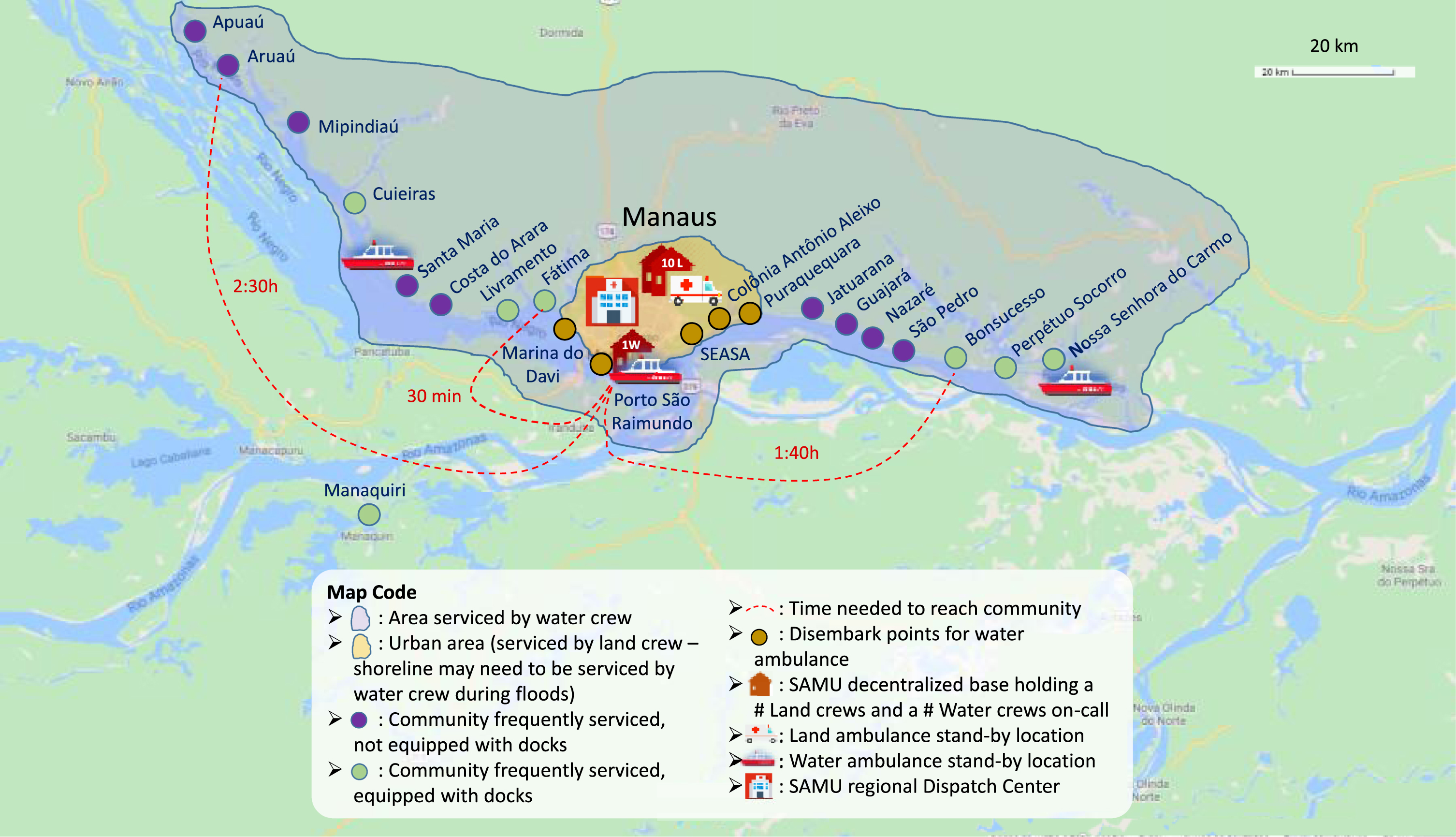
Fig. 4
Technical drawing of the main water ambulance from the regional coordination of Manaus, Amazonas state.
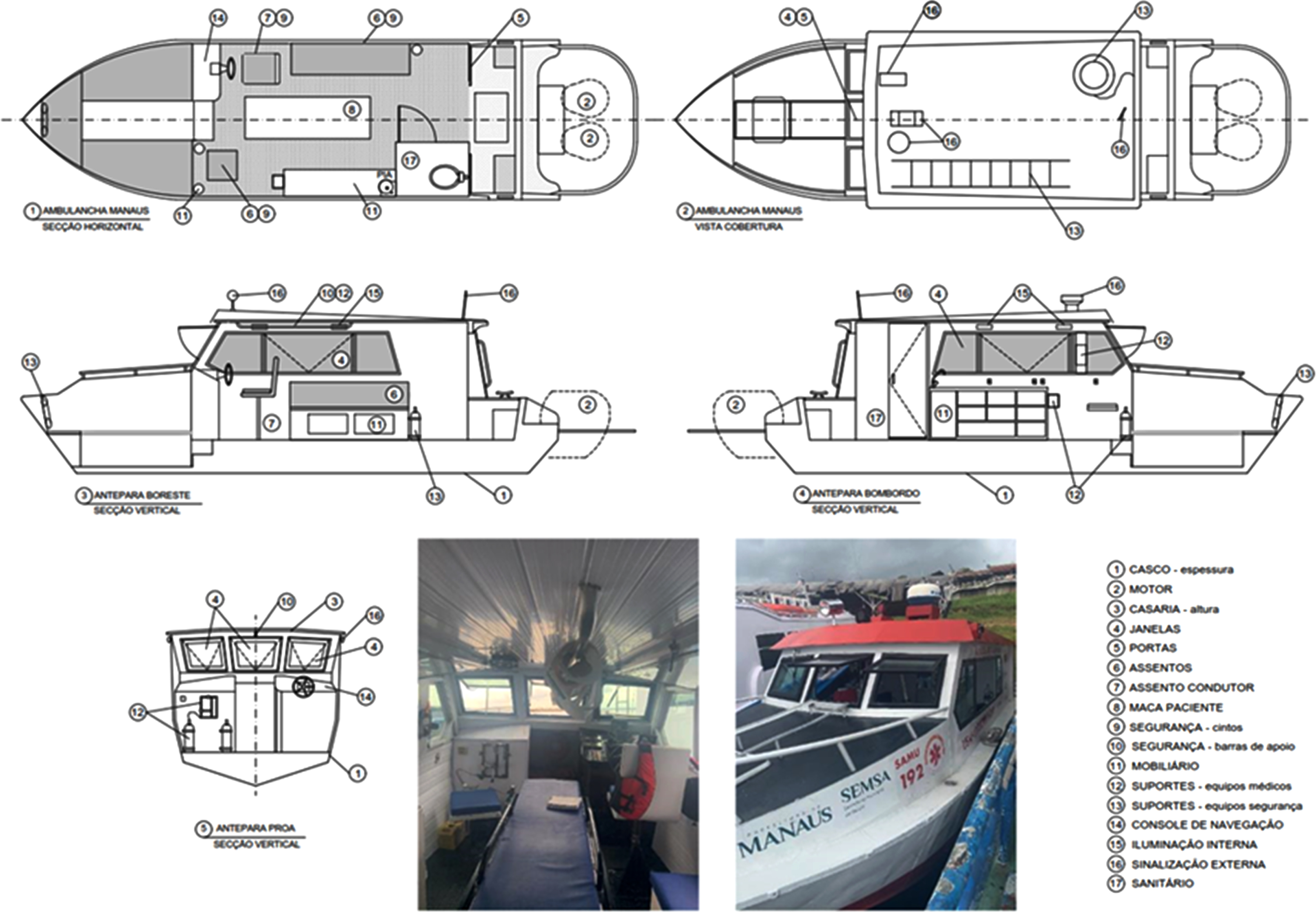
Fig. 5
Water ambulance docked at mooring spot for the community of Fátima, located 30 min upriver from Manaus and one of the few communities with docking sites.

Capacity categories defined at the content analysis (resources made available to accomplish the system’s mission) were: Communication; Base; Care protocols; Rescue teams - composition and training; Dispatch teams - composition and training; Uniforms and PPE; watercraft purchase; Procedures; Biosafety; and actions across levels of care. Detailing over description of emergency care through the lens of demand and capacity categories can be found elsewhere [5].
Design specifications from this systematization produced spanned composition and training of both intervention teams and dispatch central teams, uniforms and personal protective equipment (PPE), decentralized water bases, means of communication, intervention protocols, biosafety and inter-sector actions. Results for all categories are detailed in Tables 1 and 2.
Table 1
Demand×capacity misalignments and design specifications for the water ambulance service (Part 1 of 2)
| Item | Situation | Misalignment demand×capacity | Design specifications for water ambulance service | |
| Capacity | Demand | |||
| Communication | Navigation blind in most of the route; total or partial lack of cellular signal; inoperative operators; radio signal that does not reach the entire route of the expedition | Full communication of the on-board team with the regional Dispatch Center, both for the referral itself and for the reporting of problems or incidents in the expedition and rescue request. | Impossibility of conducting referral during service and transport of the patient, and to ask for rescue in case of incidents or accidents | Fostering the installation of signal relay antennas; availability of cell phones with chips from all operators for the vessel’s team; implementation of emergency positioning radio beacons equipment, to be activated in need of rescue, sending a location signal from anywhere to a registered center |
| Waterway operation bases | Absence or underequipped waterway operation base | Presence of the team close to the vessel and in decent conditions; vessel protected from robbery and theft; suitable place for disembarking victims and maintenance of ambulance | Theft of fuel, engine and equipment; loss of time in commuting and expenses with motorcycle and fuel, often paid for by the team itself; difficulties in disembarking victims and in accessing and maintaining the vessel; team fatigue | Minimum referral of waterway bases in five rooms plus nautical hangar with lifting system for repairs in a dry environment; suggestion of setting up a joint base with other river teams such as Civil Defense, Fire Department and Special Secretariat for Indigenous Health (SESAI). |
| Watercraft purchase, development or rental | Terms of reference for tenders prepared locally and without prior guidance or guidelines | Specifications for the vessel and implementation process aligned with local-regional demands and particularities regarding the operation of the ambulance service Under-specified | Vessel and implementation process with gaps in the necessary expertise, generating difficulties in the operation of the services and maintenance of vessels, impacting the provision of the service. | Formation of a working group to prepare the Terms of Reference for the bids, with the participation of the vessel and referral teams, managers, vessel maintainers and naval engineer; inclusion of the vessel’s maintenance plan with definition of maintenance locations, parts forecast and temporary component replacement plan |
| Protocols | For the basic life support team (BLS) - without a nurse or doctor on board - medications and many procedures need to be authorized by the referral Center; absence of specific protocols such as team rescue in case of incidents and the requester’s own displacement | Shortage of doctors and nurses in regions far from the capitals, generating a shortage of physicians on board; long distances traveled with victims in serious condition without a signal to communicate with the referral; need to reduce response time by meeting the applicant and vessel team midway | In the absence of a communication signal, which can last several hours in an expedition, BLS teams need to decide between acting without legal support or watching the worsening of the victim’s condition; need for teams to have personal contacts or passing vessels for rescue in case of incidents; risk of a midway mismatch between the applicant and the vessel team | Adequacy of the work protocols of basic support teams in regions with proven medical absence and poor communication signal, formalizing procedures such as “pre-referral” in the prescription of procedures and medications; guidelines for the development of new protocols aimed at the rescue of teams and alignment with the particularities of the occurrences attended by water ambulances. |
Table 2
Demand×capacity misalignments and design specifications for the water ambulance service (Part 2 of 2)
| Item | Situation | Misalignment demand x capacity | Design specifications for water ambulance service | |
| Capacity | Demand | |||
| Dispatch teams – Composition and training | Absence of training towards emergency dispatch to coastal and riverine communities; absence of normative guidelines regarding incorporation of teammembers experienced as rescuers in water ambulance service | Need of collecting precise information on events, given disntinct beaches with the same name, remote hard-reaching event locations, absence of cellphone and radio coverage and requesters not fluent in Portuguese | Rescue teams lacking enough information to locate victim and without “pre-authorization” support in events at locations without ways of communication with Dispatch Center; opacity of gravity of event to the SAMU 192 | Training of dispatch teams regarding topics such as: local riverine, maritime and insular geography in both wet and dry seasons; profile of serviced communities including primary care coverage; main mooring spots for water ambulances; local cellphone and radio coverage; navigation distances and response times to commmunities; typical scenarios that require “pre-authorization” of interventions; linguistic regionalisms |
| Rescue teams – Composition and training | Multiple arrangements in the composition of teams between different regional coordinations, with teams often having only 2 members; limitation in specific training | Need for three people to board the victim; complexity of care due to the nature of occurrences and long time to reach the health unit; need for at least two people for patient handling and navigation procedures | Dependence on the victim’s companions to board the ambulance; need to pause the return journey (which in maritime regions can only be done in collisions) to execute the procedure. doctors; need for a nursing technician to stop monitoring the patient to assist in night navigation, or speed reduction | to the minimum BLS team of a health professional or marine, depending on availability for hiring in the region; implementation of intermediate teams, with nurses but no doctors, for regions with a shortage of doctors; divalent training in seamanship and CPR procedures for all team members |
| Biosafety | Guidelines and undifferentiated those biosecurity measures oriented terrestrial component | Exposure of the craft crews to infection by infectious diseases increased relative to land teams, due to extended periods in contact with victims and companions | Increased risk of infection of vessel teams, victims and companions by infectious-contagious diseases; large number of leaves during the COVID-19 pandemic | Design of a curtain system around the stretchers of vessels; equipping the vessel with PPE kits for teams, victims and companions; sanitizing benches on the bases; training of vessel teams in the use of PPE, good isolation practices in shipping and vessel disinfection; training of regulatory staff in identifying suspected cases of COVID-19 and other infectious diseases and pre-referral of victim’s pre-shipment procedures |
| Cross-sectoral actions | regional SAMU Actions 192 in management and training with little coordination with local government agencies and state as Primary Health Care, Civil Defense, Federal Police, Fire Brigade and Municipal Works | Absence of piers in most communities served; inspections of vessels by inspection bodies; occurrences located within riverine and coastal communities; need for articulation with community health workers (CHWs) in the communities | Need for mooring on beaches, rocky shores and ravines, often from the bow, making it difficult for victims to board, especially when planking; increased response time due to ambulance inspections; difficulty in finding victims and transporting them to the coast in internalized events; difficulties in articulating with community health workers (CHW) | Fostering partnerships for the installation of floating piers in communities aiming at greater safety, comfort and speed in the mooring and embarkation of victims; implementation of communication protocols between the referral Center and waterway inspection bodies in order to facilitate and speed up inspections at the ambulance; encouragement of agreements with health units or community residents’ associations to provide land vehicles to help in internalized events; training of CHW’s to support team service |
One of the topics highlighted in our analysis concerns the acquisition process of the watercraft, which is led in a decentralized way by municipalities. It generally does not meet minimum standardization requirements, and often does not consider the local construction experiences or appropriate locations for the acquisition of parts and maintenance of the vessels, which has a direct impact on the system’s resilience, generating variability, and consequently, the interruption of the service. In this case, the demand vs. capacity misalignment could be solved by defining standards and guidelines for purchase, maintenance, and the training of local working groups.
On the topic of communication means and demands, and referring especially to the Upper Amazon (Alto Solimões, in Portuguese) and to the São Francisco River, the communication between the Dispatch teams and the rescue teams is very unstable. One complication presented by most locations is the absence of navigation equipment such as sonar, GPS and low-range radio, on the boats, which increases the tension of conductors, especially in Upper Amazon river, as they increase the risk of vessels colliding. The implementation of these measures would improve the quality of service and mitigate the probability of accidents, making the system more resilient and reducing the possibility of complications during calls and, consequently, interruptions. Although there are standard procedures for patient care, the lack of communication between rescuers and the Patient Referral disturbs the care process. Updating the procedures to include actions to cope with patients’ eventual worsening, or in cases where communication fails, would mitigate variability that negatively impacts the system’s resilience.
Another point noted is the lack of bases to prevent the boats from theft and vandalism, to quicken the access, and to support rescue teams during their breaks. One of the proposals presented to reduce such variability was sharing bases between departments like the Fire Department, Civil Defense, Special Secretariat for Indigenous Health (when applicable) and others.
One of the most important points to be highlighted for the system’s resilience is the selection and training of the teams at the referral centers. Due to the difficulty of hiring qualified professionals in these more remote regions, they need to hire professionals who reside in the capitals and who suffer from the lack of transport infrastructure to travel to smaller cities, in addition to the high cost.
4Discussion
The utilization of a mixed-methods research design allowed for the investigation of multiple themes of demand-capacity misalignments. Such orientation for a research has been shown to offer comprehensive perspectives on understanding functioning of complex socio-technical systems [20, 21].
Results showed that the lack of a national regulation for water ambulance services simultaneously allowed for situated adjustment to meet local challenges but contributed for service under specification. The employed methodology enabled framing and assessment of misalignments between engineered capacities and system demands, as well as framing and assessment of specific design elements to manage variability, which in turn showed paths for improving the service.
Variability was found to be a key-component in system behavior, with different impacts over service outcomes depending on the organizational and technical aspects and restrictions at play at each triggered emergency event, such as the composition of the deployed team and the availability of cell phone and radio coverage at the event location and route – defining availability of communication between the intervention team and the dispatch central.
As verified in previous studies that framed their research design based on demand and capacity elements [22–24], the use of a model of organizational resilience in this study enabled the identification of how demand x capacity misalignments foster adaptation from healthcare professionals towards coping with them while aiming to deliver effective emergency care.
As for methodological limitations, we note that data collection was conducted mainly at micro and meso levels, which is a limitation that has been considered a challenge to studies in resilient health care [25].
The gaps in the mobile emergency care service disclosed by the application of our research design can perhaps be related to the concept of slack and its many uses in the context of complex socio-technical systems [26]. Particularly, the systematization of demand-capacity misalignments as has been carried out in this study might enable useful insight on where to focus slack resources.
In domains as intensive in variability as coastal and riverine mobile emergency care, it could be argued that a pertinent strategy regarding prioritization in designing organizational resources (capacity elements) for slack should account for unexpected variability [27] and breadth of scope [26] – i.e. slack that can be deployed to cope with diverse sources of variability. Particularly for the case of the domain studied, increasing personnel in rescue teams (e.g. adding one health attendant or sailor) could potentially fit such guidelines. Our analysis suggested that this intervention could significantly increase potential for in situ adaptation within teamwork and overall system preparedness to cope with a wide range of challenging situations, such as:
• Navigation and mooring under inclement conditions, including weather and tide conditions, inadequate mooring spots and water bodies with excessive and / or dangerous debris;
• Unavailability of residents from serviced communities when transporting and boarding victims to the water ambulances;
• Victims’ clinical conditions that require support in manipulation (e.g. precision in interventions, body positioning) during navigation;
• Need of attending multiple victims at the scene and during the return expedition.
As described in [5], the current absence of slack in key resources such as intervention teams’ composition often requires adaptations at the sharp-end that include support from primary care personnel (especially community health workers), community residents, and local boat owners, ultimately meaning that resilient performance becomes extra-organizational. In turn, this scenario might mean brittleness to the system in occasions where these informal support networks become more fragile. Therefore, the need for adaptations mixed with the absence of slack resources might create sacrifice dilemmas, similarly to what has been reported in healthcare literature [28] and other safety-critical domains [29, 30], as well as creating potentially excessive workload for crews, jeopardizing workers’ mental health and ultimately patient safety [31].
One of the main limitations of the present study is that “actual system functioning” can never be fully appreciated or disclosed. Although participatory research tools in Ergonomics & Human Factors - and increasingly in the field of resilience engineering – can help us map and understand cognitive adaptations to complexity, there is always a limit to the extent in which we can narrow the gap between work-as-disclosed (or work-as-observed) and work-as-done. [32–35]. Nevertheless, we believe there continues to be opportunities for improving system performance and informing theory development in operationalizing resilient performance in complex systems.
5Conclusion
The use of a conceptual framework for analysis based on elements of system demands, engineered capacities and adaptations from system agents allowed the identification of several points in the system that can overload the teams or the system components. From these points, it was possible to draw up normative guidelines that could help the implementation process of new municipalities that may offer the service and still allow those that are already in operation, the identification of critical points can help to minimize incidents and make the system behave more resiliently. As we move towards engineering ever-more inter-dependable systems we hope we can guide the design of specifications to manage variability, cope with complexity and support systems in sustaining graceful extensibility.
5.1Ethics statement
This study was conducted in accordance with Brazilian regulations concerning research with human subjects. The study was approved by the Oswaldo Cruz Foundation Institutional Review (IRB) Board (approval number 3.775.237, December 19th, 2019).
Informed consent
Not applicable.
Conflict of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Disclaimer
The authors declare that data collection protocols for this study overlap with the study by Jatobá et al. [5]. Notwithstanding this intersection, the research aims, data coding, analysis and findings of this study fundamentally differ from the former, which is reflected on both its distinct conceptual and practical significances. Jatobá et al. [5] presented a diagnosis of the difficulties and challenges of emergency mobile care for riverside and maritime regions in Brazil through methods underpinned by the Grounded Theory [36]. In contrast, the present builds on these findings to produce organizational design guidelines to some focal points for intervention in the system towards both improving the alignment between system demand and engineered resources, and facilitating the necessary adaptations to improve the quality of the service.
Acknowledgments
The authors gratefully acknowledge all healthcare professionals who participated in this study, and particularly the SAMU professionals for their availability and willingness to share their knowledge during the various research phases. Paulo V. R. de Carvalho gratefully acknowledges the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq; grant number 304770/2020-5) and Fundação de Amparo a Pesquisa do Rio de Janeiro FAPERJ (project number 260003/001186/2020).
Funding
Alessandro Jatobá was funded by the National Council for Scientific and Technological Development - CNPq (grants #307029/2021-2 and 402670/2021-3) and the Carlos Chagas Filho Foundation for Supporting Research in the State of Rio de Janeiro - FAPERJ (grant # E-26/201.252/2022). The other authors have no funding to report.
References
[1] | Nevola VR , Lowe MD , Marston CA . Review of methods to identify the critical job-tasks undertaken by the emergency services. WOR. (2019) ;63: :521–36. https://doi.org/10.3233/WOR-192914. |
[2] | Frasão G . População passa a contar com 476 novas ambulâncias do SAMU. 2018;192. https://www.saude.gov.br/noticias/agencia-saude/42892-populacao-passa-a-contar-com-476-novas-ambulancias-do-samu-192 (accessed July 13, 2020). |
[3] | Timerman S , Gonzalez MMC , Zaroni AC , Ramires JAF . Emergency medical services: Brazil. Resuscitation. (2006) ;70: :356–9. https://doi.org/10.1016/j.resuscitation.2006.05.010. |
[4] | Machado CV , Salvador FGF , O’Dwyer G . Mobile Emergency Care Service: Analysis of Brazilian policy. Revista de Saúde Pública. (2011) ;45. |
[5] | Jatobá A , Bellas H , Arcuri R , Bulhões B , Carvalho PVR de . Water ambulances and the challenges of delivering mobile emergency healthcare to riverine and maritime communities. The American Journal of Emergency Medicine. (2021) ;47: :258–66. https://doi.org/10.1016/j.ajem.2021.05.012. |
[6] | Hollnagel E , Woods DD , Leveson N . Resilience Engineering: Concepts and Precepts. Aldershot, England; Burlington, VT: Ashgate; 2006. |
[7] | Clay-Williams R , Hounsgaard J , Hollnagel E . Where the rubber meets the road: Using FRAM to align work-as-imagined with work-as-done when implementing clinical guidelines. Implementation Science. (2015) ;10: :125. https://doi.org/10.1186/s13012-015-0317-y. |
[8] | Hollnagel E . Prologue: Why do our expectations of how work should be done never correspond exactly to how work is done. Resilient health care III: Reconciling work-as-imagined and work-as-done. (2017) , pp. 7–16. |
[9] | Anderson JE , Ross AJ , Jaye P . Modelling Resilience and Researching the Gap between Work-as-Imagined and Work-as-Done. Resilient Health Care, Volume 3: Reconciling Work-as-Imagined and Work-as-Done, Farnham, Surrey; Burlington, VT: CRC Press; (2017) ;, pp. 133–41. |
[10] | Anderson JE , Ross AJ , Macrae C , Wiig S . Defining adaptive capacity in healthcare: A new framework for researching resilient performance. Applied Ergonomics. (2020) ;87: :103111. https://doi.org/10.1016/j.apergo.2020.103111. |
[11] | Goodman LA . Snowball sampling. The Annals of Mathematical Statistics. (1961) ;32: :148–70. |
[12] | Bardin L . L’ analyse de contenu. 5 éd rev et augm Presses Univ de France; (1989) . |
[13] | Másculo FS , Vidal MC , editors. Ergonomia: Trabalho Adequado e Eficiente. Elsevier Brasil; (2011) . |
[14] | Gale NK , Heath G , Cameron E , Rashid S , Redwood S . Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Medical Research Methodology. (2013) ;13: :117. https://doi.org/10.1186/1471-2288-13-117. |
[15] | Selltiz C , Jahoda M , Deutsch M , Cook SW . Research Methods in Social Relations. Revised One-Volume Edition. Holt, Rinehart and Winston; (1959) . |
[16] | Bailey KD . Typologies and taxonomies: An introduction to classification techniques. Sage; (1994) . |
[17] | Dekker S . Drift into failure: From hunting broken components to understanding complex systems. Farnham; Burlington, VT: Ashgate Pub; (2011) . |
[18] | Minayo MC de S , Deslandes SF , Neto OC , Gomes R . Pesquisa Social: Teoria, Método e Criatividade. 21st ed. Vozes; (1994) . |
[19] | Selltiz C . Métodos de pesquisa nas relações sociais. EPU; (1974) . |
[20] | Phipps DL , Morris RL , Blakeman T , Ashcroft DM . What is involved in medicines management across care boundaries? A qualitative study of healthcare practitioners’ experiences in the case of acute kidney injury. BMJ Open. (2017) ;7. https://doi.org/10.1136/bmjopen-2016-011765. |
[21] | Fylan B , Marques I , Ismail H , Breen L , Gardner P , Armitage G , et al. Gaps, traps, bridges and props: A mixed-methods study of resilience in the medicines management system for patients with heart failure at hospital discharge. BMJ Open. (2019) ;9. https://doi.org/10.1136/bmjopen-2018-023440. |
[22] | Back J , Ross AJ , Duncan MD , Jaye P , Henderson K , Anderson JE . Emergency department escalation in theory and practice: A mixed-methods study using a model of organizational resilience. Annals of Emergency Medicine. (2017) ;70: ;659–71. https://doi.org/10.1016/j.annemergmed.2017.04.032. |
[23] | Ross A , Sherriff A , Kidd J , Gnich W , Anderson J , Deas L , et al. A systems approach using the functional resonance analysis method to support fluoride varnish application for children attending general dental practice. Applied Ergonomics. (2018) ;68: :294–303. https://doi.org/10.1016/j.apergo.2017.12.005. |
[24] | Arcuri R , Bulhões B , Jatobá A , Bellas HC , Koster I , d’Avila AL , et al. Gatekeeper family doctors operating a decentralized referral prioritization system: Uncovering improvements in system resilience through a grounded-based approach. Safety Science. (2020) ;121: :177–90. https://doi.org/10.1016/j.ssci.2019.08.023. |
[25] | Berg SH , Akerjordet K , Ekstedt M , Aase K . Methodological strategies in resilient health care studies: An integrative review. Safety Science. (2018) ;110: :300–12. https://doi.org/10.1016/j.ssci.2018.08.025. |
[26] | Saurin TA , Werle NJB . A framework for the analysis of slack in socio-technical systems. Reliability Engineering & System Safety. (2017) ;167: :439–51. https://doi.org/10.1016/j.ress.2017.06.023. |
[27] | Hollnagel E . FRAM: The Functional Resonance Analysis Method: Modelling Complex Socio-technical Systems. Ashgate; 2012. |
[28] | Perry SJ , Wears RL , Anderson B . Extemporaneous Adaptation to Evolving Complexity: A Case Study of Resilience in Healthcare. Proceedings of the second resilience engineering symposium, Juan-Les-Pins, France: (2006) . |
[29] | Gomes JO , Woods DD , Carvalho PVR , Huber GJ , Borges MRS . Resilience and brittleness in the offshore helicopter transportation system: The identification of constraints and sacrifice decisions in pilots’ work. Reliability Engineering & System Safety. (2009) ;94: :311–9. https://doi.org/10.1016/j.ress.2008.03.026. |
[30] | Woods DD . Creating foresight: Lessons for enhancing resilience from Columbia. Organization at the limit: Lessons from the Columbia disaster, Blackwell; 2005. |
[31] | Durand A-C , Bompard C , Sportiello J , Michelet P , Gentile S . Stress and burnout among professionals working in the emergency department in a French university hospital: Prevalence and associated factors. WOR. (2019) ;63: :57–67. https://doi.org/10.3233/WOR-192908. |
[32] | Gattola V , Patriarca R , Tomasi G , Tronci M . Functional resonance in industrial operations: A case study in a manufacturing plant. IFAC-Papers On Line. (2018) ;51: :927–32. https://doi.org/10.1016/j.ifacol.2018.08.489. |
[33] | Ward P , Hoffman RR , Conway GE , Schraagen JM , Peebles D , Hutton RJB , et al. Editorial: Macrocognition: The science and engineering of sociotechnical work systems. Frontiers in Psychology. (2017) ;8. |
[34] | Patriarca R , Falegnami A , Costantino F , Di Gravio G , De Nicola A , Villani ML . WAx: An integrated conceptual framework for the analysis of cyber-socio-technical systems. Safety Science. (2021) ;136: :105142. https://doi.org/10.1016/j.ssci.2020.105142. |
[35] | Moppett IK , Shorrock ST . Working out wrong-side blocks. Anaesthesia. (2018) ;73: :407–20. https://doi.org/10.1111/anae.14165. |
[36] | Corbin JM , Strauss AL . Basics of qualitative research: Techniques and procedures for developing grounded theory. Fourth edition Los Angeles: SAGE; (2015) . |


