
A descriptive study of knowledge, attitudes, behaviors, and precautions of physiotherapy and rehabilitation students regarding COVID-19
Abstract
BACKGROUND:
Physiotherapy and rehabilitation students need to be aware of the global COVID-19 pandemic and choose the correct interventions.
OBJECTIVES:
To investigate the knowledge, attitudes, behaviors, and precautions of physiotherapy and rehabilitation students regarding COVID-19 during the global pandemic.
METHODS:
A total of 438 physiotherapy and rehabilitation students participated in the study. A web-based descriptive cross-sectional questionnaire was conducted using the “Google Forms” on physiotherapy and rehabilitation students in the months of February, March, and April 2021. The online questionnaire consisted of six main sections containing 130 items: (1) sociodemographic information, (2) knowledge sources and knowledge about COVID-19, (3) attitudes about COVID-19, (4) behaviors, (5) precautions, and (6) being a physiotherapy and rehabilitation student during the COVID-19 pandemic. The collected data were reported in terms of mean, standard deviation, number, frequency, and percentage values.
RESULTS:
The vast majority of the participants (n = 291, 66.5%) often/always accessed information about COVID-19 via social media, 397 (90.6%) of them often/always wear masks. Moreover, 419 (95.6%) of the physiotherapy students knew the symptoms of COVID-19, and 409 (93.4%) of the students have been responded “yes” to the question of whether pulmonary rehabilitation should be applied in intensive care units for COVID-19 infections.
CONCLUSIONS:
Physiotherapy and rehabilitation students have adequate awareness about COVID-19. In this regard, physiotherapy and rehabilitation students should be included in appropriate educational programs to protect themselves, their relatives, and patients against COVID-19, and their knowledge about the treatment methods should be increased.
1Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a new type of coronavirus that emerged in late 2019, and causes the disease defined as COVID-19 (Coronavirus Disease 2019) [1]. The human-to-human transmission of COVID-19 occurs between 2 and 10 days before the cases become symptomatic [1, 2]. Although it is known that there may be asymptomatic cases, the most common symptoms are fever, cough, myalgia, and shortness of breath. In severe cases, incidents of pneumonia, severe acute respiratory syndrome, kidney failure, and even death may occur [3]. COVID-19 patients have different degrees of respiratory, physical, and psychological dysfunction, and that these patients need physiotherapy and rehabilitation both during the treatment of the disease and after discharge [4, 5]. Physiotherapists take part in the acute and chronic periods of the disease in order to minimize the consequences of long-term immobilization and mechanical ventilation, especially in severe cases [6]. Therefore, treatment paradigms need to be evaluated and updated as new information emerges [7]. In this context, the critical role of future physiotherapists in having sufficient competencies and awareness about COVID-19 should be considered with respect to the short and long-term impacts of the disease. The possibility of physiotherapy and rehabilitation students being exposed to infected cases during the treatment process shows how closely they are intertwined with the pandemic conditions. On the other hand, the potential contribution of these students’ (who will work on the front lines in the future) attitudes, behaviors, and low-risk practices in preventing negative impacts of the epidemic highlights the importance of examining these factors more closely.
Although students of physiotherapy and rehabilitation science are not directly involved in the management of COVID-19 patients, they can serve in the delivery of pandemic management and patient education. Physiotherapy students can sensitize people in the community, their close circles, and families about COVID-19 symptoms, personal hygiene, and pandemic prevention. In this sense, physiotherapy students are expected to have basic knowledge of COVID-19 and to make the correct interventions in the face of the global pandemic [8]. The circumstances of the current global pandemic require a significant awareness of the clinical situation, the preventive measures of spreading, and the management of COVID-19. In this context, physiotherapy students are also expected to have sufficient awareness of COVID-19. However, it is important to obtain this awareness and information from the correct channels. In addition, physiotherapy students are expected to have an understanding of the potential changes that may occur physically, mentally, and psychologically during and after the illness and to have an opinion about the physiotherapy program that can be applied [8, 9].
Although there are studies in the literature investigating the knowledge levels, attitudes, behaviors, and preventive measures of medical students and students from different health sciences during the COVID-19 global pandemic [8, 10], the number of studies specifically aimed at physiotherapy and rehabilitation students is limited [11, 12], and it is observed that knowledge, attitude, behavior, and precautions are not all investigated together in these studies. Based on these considerations, the aim of our study was to investigate the knowledge, attitudes, behaviors, and precautions of physiotherapy and rehabilitation students about COVID-19 during the global pandemic.
2Methods
A web-based descriptive cross-sectional questionnaire was conducted using the “Google Forms” on physiotherapy and rehabilitation undergraduate students in the months of February, March, and April in 2021. The study was approved by Akdeniz University Faculty of Medicine Clinical Research Ethics Committee (70904504/38, Decision No: KAEK-42). Physiotherapy and rehabilitation students were asked to participate in the study via the distribution of the questionnaire to universities with physiotherapy and rehabilitation departments, and sharing the link of the questionnaire form on social media groups. Participants were asked to provide written informed consent before answering the questionnaire questions. All participants were asked to provide true answers, and were informed that their personal information would be kept confidential. The Google Forms link used to announce and distribute the questionnaire was open to everyone’s access. Various vocational students and graduate students also reached out and filled the online questionnaire. However, the data coming from these students were excluded from the analyses as they did not constitute the intended sample of the study. Our study was recruited on 438 physiotherapy and rehabilitation undergraduate students aged between 18 and 41 years.
Inclusion criteria for the study was determined; (1) to be a physiotherapy and rehabilitation undergraduate student; (2) to be over 18 years of age; (3) to be voluntarily participating in the study; (4) having read and approved the informed consent form; (5) having internet access to complete the online questionnaire and answering the entire questionnaire. Those who received education in a different department other than the physiotherapy and rehabilitation undergraduate department, those who did not have internet access, and those who did not answer all the questions in the online questionnaire were excluded from the study.
2.1Content of the questionnaire
The questionnaire used in the article study by Khasawneh et al. [10] was redesigned and used for physiotherapy and rehabilitation students. Permissions were obtained from the corresponding author (Dr. Khalid A. Kheirallah) to redesign and use this questionnaire for physiotherapy and rehabilitation students.
The online questionnaire consisted of six main sections containing 130 items: (1) sociodemographic information; (2) knowledge sources and knowledge about COVID-19 (Tables 1 and 2; Fig. 1); (3) attitudes about COVID-19 (Table 3); (4) behaviors (Table 4); (5) precautions (Table 4); and (6) being a physiotherapy and rehabilitation student during the COVID-19 pandemic (Table 5). Sociodemographic information included gender, age, academic level (year of study), and questions about the situation of encountering a patient with COVID-19 [10].
Table 1
Knowledge sources and thoughts on potential modes of transmission of COVID-19
| Knowledge sources | Never/None n (%) | Rarely/Sometimes n (%) | Often/Always n (%) |
| Social media | 15 (3.4) | 132 (30.1) | 291 (66.5) |
| Official website of the Ministry of Health of the Republic of Turkey | 54 (12.3) | 205 (46.8) | 179 (40.9) |
| Official website of the World Health Organization (WHO) | 170 (38.8) | 207 (47.3) | 61 (13.9) |
| Official website of the World Confederation for Physical Therapy (WCPT) | 283 (64.6) | 134 (30.6) | 21 (4.8) |
| Internet search engines | 14 (3.2) | 161 (36.8) | 263 (60.0) |
| Up to date medical literature search sites such as PubMed, PEDro | 253 (57.8) | 131 (29.9) | 54 (12.3) |
| News channels | 22 (5.0) | 209 (47.7) | 207 (47.3) |
| Family and friends | 59 (13.5) | 246 (56.1) | 133 (30.4) |
| Health personnel in the hospital | 125 (28.5) | 225 (51.4) | 88 (20.1) |
| International and national organizations | 161 (36.8) | 193 (44.0) | 84 (19.2) |
| Potential modes of transmission | Not possible n (%) | I don’t know n (%) | Possible n (%) |
| Airborne | 60 (13.7) | 86 (19.6) | 292 (66.7) |
| Inhaling a large droplet | 12 (2.7) | 55 (12.6) | 371 (84.7) |
| From animals | 207 (47.3) | 175 (39.9) | 56 (12.8) |
| Contaminated foods | 52 (11.9) | 203 (46.3) | 183 (41.8) |
| Contacting contaminated surfaces | 16 (3.6) | 70 (16.0) | 352 (80.4) |
| Skin-to-skin contact/Contact with a patient | 30 (6.9) | 32 (7.3) | 376 (85.8) |
| From feces | 195 (44.5) | 185 (42.2) | 58 (13.3) |
| By kissing | 9 (2.0) | 20 (4.6) | 409 (93.4) |
| By handshake | 21 (4.8) | 38 (8.7) | 379 (86.5) |
| From mother to fetus | 56 (12.8) | 226 (51.6) | 156 (35.6) |
| Blood transfusion | 48 (10.9) | 228 (52.1) | 162 (37.0) |
| Breast milk | 69 (15.7) | 246 (56.2) | 123 (28.1) |
Table 2
Levels of knowledge on potential risk factors and virulence of COVID-19
| Knowledge of potential risk factors and virulence | I disagree n (%) | I don’t know n (%) | I agree n (%) |
| COVID-19 has serious effects on the health system and economy | 15 (3.4) | 12 (2.8) | 411 (93.8) |
| The COVID-19 pandemic is under control | 271 (61.9) | 135 (30.8) | 32 (7.3) |
| I consider myself informed about COVID-19 | 59 (13.5) | 137 (31.3) | 242 (55.2) |
| Children are at a greater risk for COVID-19 | 209 (47.7) | 162 (37.0) | 67 (15.3) |
| People with chronic illness are at a greater risk for COVID-19 | 11 (2.5) | 18 (4.1) | 409 (93.4) |
| Pregnant women are at a greater risk for COVID-19 | 19 (4.3) | 123 (28.1) | 296 (67.6) |
| COVID-19 causes pneumonia | 8 (1.8) | 154 (35.2) | 276 (63.0) |
| There is a recovery rate of over 90% in cases of COVID-19 | 57 (13.0) | 199 (45.4) | 182 (41.6) |
| One patient can infect about 4 other people with COVID-19 | 43 (9.8) | 113 (25.8) | 282 (64.4) |
| Health education can prevent the pandemic | 41 (9.4) | 79 (18.0) | 318 (72.6) |
| Regular use of masks prevents catching the disease | 47 (10.7) | 58 (13.3) | 333 (76.0) |
| The media is exaggerating this virus outbreak | 230 (52.5) | 142 (32.4) | 66 (15.1) |
| The COVID-19 outbreak is sufficiently covered in the media in Turkey | 219 (50.0) | 113 (25.8) | 106 (24.2) |
| I talk about the virus without reviewing the literature or being sure of the accuracy of the information | 257 (58.7) | 128 (29.2) | 53 (12.1) |
| I trust the experts in the media who give their opinions on the virus | 107 (24.4) | 217 (49.6) | 114 (26.0) |
| I confirm the information I have read/heard about the virus | 80 (18.3) | 85 (19.4) | 273 (62.3) |
| I stocked up on food and household supplies during the quarantine period | 223 (50.9) | 64 (14.6) | 151 (34.5) |
| I would not want to treat a patient with suspected COVID-19 | 150 (34.2) | 136 (31.1) | 152 (34.7) |
| I do not want to apply a physiotherapy and rehabilitation program to a COVID-19 patient | 218 (49.8) | 144 (32.9) | 76 (17.3) |
| I do not think that physiotherapy and rehabilitation should be applied in COVID-19 | 319 (72.8) | 74 (16.9) | 45 (10.3) |
| Even though protective materials/clothing are used, I do not want to apply the physiotherapy to a patient with COVID-19 | 322 (73.5) | 91 (20.8) | 25 (5.7) |
| To prevent the pandemic, it is sufficient for only sick people to wear masks | 373 (85.2) | 37 (8.4) | 28 (6.4) |
| COVID-19 patients will exceed hospital capacities | 80 (18.3) | 187 (42.7) | 171 (39.0) |
| The spread rate of COVID-19 will decrease in a short time | 138 (31.5) | 225 (51.4) | 75 (17.1) |
| The spread rate of COVID-19 will increase | 92 (21.0) | 185 (42.2) | 161 (36.8) |
Fig. 1
Knowledge about COVID-19.
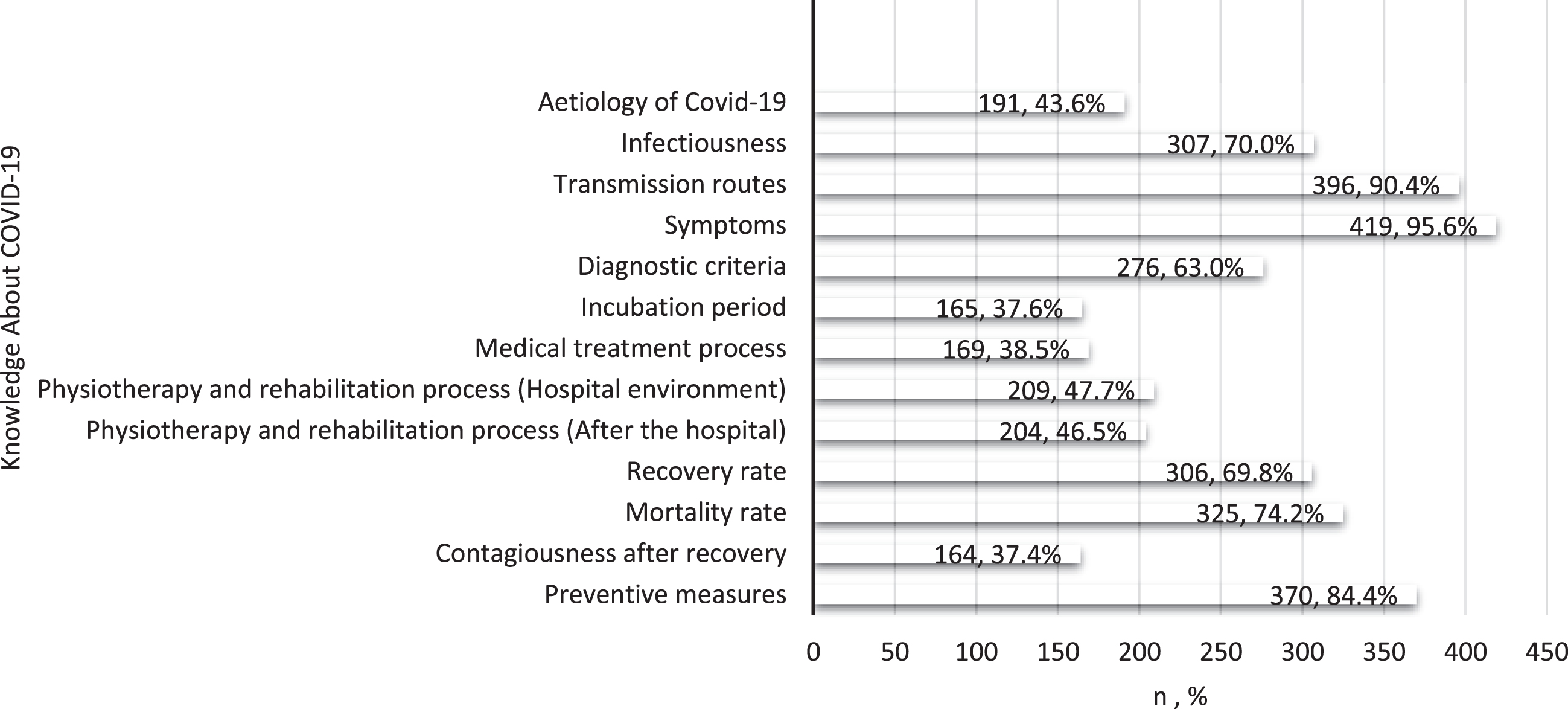
Table 3
Sensitivity perception and importance of COVID-19 and attitudes and stigma towards the test
| Sensitivity perception and importance of COVID-19 | I disagree n (%) | I abstain n (%) | I agree n (%) |
| I am concerned about contracting COVID-19 | 108 (24.7) | 110 (25.1) | 220 (50.2) |
| I am concerned that one of my family members will contract COVID-19 | 32 (7.3) | 54 (12.3) | 352 (80.4) |
| I have a predisposition to contracting COVID-19 | 226 (51.6) | 160 (36.5) | 52 (11.9) |
| My family members have a predisposition to contracting COVID-19 | 123 (28.1) | 155 (35.4) | 160 (36.5) |
| It is possible for me to contract COVID-19 from my inner circle. | 122 (27.9) | 138 (31.5) | 178 (40.6) |
| I could contract COVID-19 in the next 6 months | 103 (23.5) | 238 (54.3) | 97 (22.2) |
| Attitudes and stigma towards the test | |||
| I will consider getting tested if I show signs and symptoms of COVID-19 | 29 (6.6) | 35 (8.0) | 374 (85.4) |
| I would consider getting the vaccine produced for COVID-19 | 56 (12.8) | 106 (24.2) | 276 (63.0) |
| I think the COVID-19 vaccine will prevent the spread of the pandemic | 68 (15.5) | 144 (32.9) | 226 (51.6) |
| You should stay away from a person who contracted COVID-19 | 9 (2.1) | 57 (13.0) | 372 (84.9) |
| You should stay away from the family of a person who contracted COVID-19 | 13 (3.0) | 75 (17.1) | 350 (79.9) |
| If someone in my family contracts COVID-19, I would want to keep it private | 372 (84.9) | 43 (9.8) | 23 (5.3) |
| If I get infected and end up in the hospital, I would be extremely stressed | 83 (18.9) | 127 (29.0) | 228 (52.1) |
| If I get infected, I would do anything to avoid isolation | 376 (85.9) | 43 (9.8) | 19 (4.3) |
Table 4
Behavioral responses and precautions
| Behavioral responses | Decreased n (%) | Did not change/affect, n (%) | Increased n (%) |
| Anxiety | 20 (4.6) | 177 (40.4) | 241 (55.0) |
| Concern | 9 (2.1) | 107 (24.4) | 322 (73.5) |
| Depression | 11 (2.5) | 148 (33.8) | 279 (63.7) |
| Panic | 19 (4.3) | 159 (36.3) | 260 (59.4) |
| Loneliness | 14 (3.2) | 156 (35.6) | 268 (61.2) |
| Irritability | 14 (3.2) | 158 (36.1) | 266 (60.7) |
| Happiness | 274 (62.6) | 159 (36.3) | 5 (1.1) |
| Joy | 264 (60.3) | 170 (38.8) | 4 (0.9) |
| Feeling excited | 215 (49.1) | 186 (42.5) | 37 (8.4) |
| Insomnia | 49 (11.2) | 185 (42.2) | 204 (46.6) |
| Light sleep | 33 (7.5) | 223 (50.9) | 182 (41.6) |
| Seeing nightmares | 24 (5.5) | 278 (63.5) | 136 (31.0) |
| Insufficient sleep | 38 (8.7) | 202 (46.1) | 198 (45.2) |
| Arguing with other people | 27 (6.2) | 228 (52.0) | 183 (41.8) |
| Engaging in a fight with others | 81 (18.5) | 306 (69.9) | 51 (11.6) |
| Smoking | 96 (21.9) | 263 (60.1) | 79 (18.0) |
| Smoking hookah | 126 (28.8) | 282 (64.4) | 30 (6.8) |
| Precautions | Never n (%) | Rarely/Sometimes n (%) | Often/Always n (%) |
| Buying a mask | 15 (3.4) | 63 (14.4) | 360 (82.2) |
| Buying disinfectant/cologne | 31 (7.1) | 72 (16.4) | 335 (76.5) |
| Wearing a mask | 4 (0.9) | 37 (8.5) | 397 (90.6) |
| Regular hand washing | 5 (1.1) | 48 (11.0) | 385 (87.9) |
| Using disinfectant/cologne | 6 (1.3) | 48 (11.0) | 384 (87.7) |
| Paying more attention to personal hygiene | 7 (1.5) | 47 (10.8) | 384 (87.7) |
| Avoiding contact with certain groups | 12 (2.7) | 62 (14.2) | 364 (83.1) |
| Paying attention to a have balanced diet | 33 (7.5) | 191 (43.6) | 214 (48.9) |
| Cleaning the cell phone/tablet/computer | 32 (7.3) | 124 (28.3) | 282 (64.4) |
| Avoiding public meetings | 31 (7.1) | 78 (17.8) | 329 (75.1) |
| Staying home as much as possible | 19 (4.3) | 71 (16.2) | 348 (79.5) |
| Avoiding eating outside | 51 (11.6) | 145 (33.1) | 242 (55.3) |
| Not handshaking when greeting | 14 (3.2) | 69 (15.7) | 355 (81.1) |
| Not kissing when greeting | 15 (3.4) | 37 (8.5) | 386 (88.1) |
| Avoiding public transportation | 36 (8.2) | 105 (24.0) | 297 (67.8) |
| Getting enough sleep | 67 (15.3) | 227 (51.8) | 144 (32.9) |
| Taking care of physical health | 34 (7.8) | 175 (39.9) | 229 (52.3) |
| To make people around me take care of their physical health | 48 (11.0) | 180 (41.1) | 210 (47.9) |
| To invite people around you to comply with preventive measures | 20 (4.6) | 123 (28.1) | 295 (67.3) |
| Complying with social distancing rules | 3 (0.7) | 81 (18.5) | 354 (80.8) |
| Increasing fluid intake | 44 (10.0) | 144 (32.9) | 250 (57.1) |
| To receive education on protective measures against COVID-19 as a physiotherapist candidate | 107 (24.4) | 177 (40.4) | 154 (35.2) |
| Approaching all my patients cautiously during internships or clinical practice courses | 63 (14.4) | 110 (25.1) | 265 (60.5) |
| As a physiotherapy and rehabilitation student, to advise your patients and relatives about the measures that can be taken against COVID-19 | 54 (12.3) | 89 (20.3) | 295 (67.4) |
Table 5
Being a physiotherapy and rehabilitation student during the COVID-19 pandemic process
| Being a physiotherapy and rehabilitation student during the COVID-19 pandemic process | Yes n (%) | No n (%) |
| Have you attended any classes on COVID-19? | 138 (31.5) | 300 (68.5) |
| Would you like to attend more lessons on COVID-19? | 353 (80.6) | 85 (19.4) |
| Have you received any education on physiotherapy and rehabilitation in COVID-19? | 100 (22.8) | 338 (77.2) |
| Have you read a physiotherapy and rehabilitation article about COVID-19? | 199 (45.4) | 239 (54.6) |
| Did you know that you can take part in infectious diseases as a physiotherapist candidate? | 277 (63.2) | 161 (36.8) |
| Physiotherapists should take an active role in the acute period of COVID-19 infection | 329 (75.1) | 109 (24.9) |
| Pulmonary rehabilitation program should be applied in intensive care unit in COVID-19 infection | 409 (93.4) | 29 (6.6) |
| Physiotherapists should take an active role in the discharge period after COVID-19 | 408 (93.2) | 30 (6.8) |
| The global COVID-19 pandemic has elicited the need for physiotherapists | 395 (90.2) | 43 (9.8) |
| Participation in online congresses/symposiums/educations | 229 (52.3) | 209 (47.7) |
2.2Statistical analysis
SPSS for Windows (IBM SPSS Statistics, Version 23.0, Armonk, NY, USA) was used for statistical analysis. It is known that there are approximately twenty thousand physiotherapy and rehabilitation students in Turkey. Accordingly, the sample size for our current study was determined from the Raosoft sample calculator [13]. The number of samples was calculated as 377 in total, with a 5% margin of error, 95% confidence interval, and 50% response distribution [13]. Data were expressed in terms of mean, standard deviation, numbers, frequency, and percentage values.
3Results
A total of 438 physiotherapy and rehabilitation undergraduate students participated in the study, of the students 227 (51.8%) were female and 211 (48.2%) were male, aged between 18 and 41, with a mean age of 20.8±2.2 years. Of the participants, 86 (19.6%) were first-year, 109 (24.9%) were second-year, 119 (27.2%) were third-year, and 124 (28.3%) were fourth-year students. In the part of the questionnaire where the sociodemographic data were examined, and more than one option could be selected as an answer; 39 (8.9%) participants had COVID-19 disease themselves, 252 (57.5%) had family or close friends that had COVID-19 infection, 62 (14.2%) had encountered a COVID-19 patient in the clinic or hospital environment and 171 (39.0%) of them had not encountered a person with COVID-19.
3.1Knowledge sources and knowledge about COVID-19
The majority of the participants (n = 291, 66.5%) often/always access knowledge about COVID-19 via social media, 246 (56.1%) rarely/sometimes receive knowledge from family and friends however, 283 (64.6%) of them have never applied to the official website of the World Confederation for Physical Therapy (WCPT) (Table 1).
In the section of potential transmission routes of COVID-19, which includes questions that investigate the level of knowledge about COVID-19 it was seen that 409 (93.4%) participants answered the question as “possible” to transmission by kissing, 246 (56.2%) marked the option of transmission through breast milk as “I don’t know”, and 207 (47.3%) chose the option that it is not possible to transmit from animals (Table 1).
It was found that 419 (95.6%) of physiotherapy students knew the symptoms of COVID-19 in the section where more than one option could be selected and the knowledge level of the participants about COVID-19 was investigated (Fig. 1).
Based on the knowledge levels about the potential risk factors and virulence of COVID-19, 411 (93.8%) participants responded “I agree” to the question that COVID-19 has serious effects on the health system and economy, 225 (51.4%) chose the option “I don’t know” to the question that the spread of COVID-19 will decrease in a short time, and it was observed that 373 (85.2%) of them gave the answer of “I disagree” to the question that only sick people should wear masks to prevent the pandemic (Table 2).
3.2Attitudes regarding COVID-19
Among the physiotherapy students participating in the study, 352 (80.4%) responded “I agree” to the statement “I am worried that one of their family members will catch COVID-19", 238 (54.3%) “I abstain” to the statement that I can be COVID-19 in the next 6 months, 226 (51.6%) answered “I disagree” to the statement “I have a predisposition to contracting COVID-19” (Table 3).
In the section where we examine attitudes and stigma towards testing for COVID-19, 374 (85.4%) participants “I agree” to the question “I would consider getting tested if I show symptoms”, 144 (32.9%) respondents said “I abstain” to the question “I think the COVID-19 vaccine will prevent the spread of the pandemic”, 376 (85.9%) answered “I disagree” to the question “If I get infected, I will do everything to avoid isolation” (Table 3).
3.3Behaviors
In the section where behaviors related to COVID-19 are evaluated, 322 (73.5%) students stated that their concern increased, 306 (69.9%) students stated that their level of engaging fights with other people did not change/affect, and 274 (62.6%) students stated that their level of happiness decreased (Table 4).
3.4Precautions
In the section where the measures taken against COVID-19 were examined, 397 (90.6%) of the participants “often/always” wear masks, 227 (51.8%) answered “rarely/sometimes” to the question of getting enough sleep, 107 (24.4%) on the other hand, answered the question of getting training on protective measures against COVID-19 as a physiotherapist candidate as “never” (Table 4).
3.5Being a physiotherapy and rehabilitation student during the COVID-19 pandemic process
In the section where questions were asked about being a physiotherapy and rehabilitation student during the COVID-19 global pandemic, while 409 (93.4%) students answered “yes” to the question of whether pulmonary rehabilitation should be applied in intensive care in COVID-19 infection, 338 (77.2%) students answered “no” to the question of whether they received any education on physiotherapy and rehabilitation in COVID-19 (Table 5).
4Discussion
This descriptive study on COVID-19, which is an ongoing global pandemic and affects many different fields and branches of science, evaluated the knowledge, attitudes, behaviors, and precautions of Turkish physiotherapy and rehabilitation students in Turkey about COVID-19.
Our study revealed that most students acquire information about COVID-19 via social media. In a study that included students from fields such as medicine, dentistry, and physiotherapy, it was reported that the level of information intake on social media was 65.17%, similar to our study [8]. Likewise, Khasawneh et al. [10] reported that 83.4% of medical students rely on social media to get information about COVID-19. In the current study, the fact that only 15 (3.4%) students did not use social media to get information about COVID-19 reveals students’ trust in social media as an information source. This situation underlines the importance of using social media correctly and effectively in pandemic management [10]. In addition, one of the important results of our study is that 283 participants never applied to the official website of WCPT in order to get information. Nonetheless, it is noteworthy that references to current medical literature search sites such as PubMed, PEDro, and the official website of WHO is seriously low. In contrast to the lack of interest in the abovementioned websites, the information obtained from the official site of the Ministry of Health of the Republic of Turkey, from internet search engines, and news channels is abundant. This situation presented us that the physiotherapist candidate students refer to social media, internet search engines, news channels before they refer to the current literature, WHO and WCPT, and trust in the official website of the Ministry of Health of the Republic of Turkey, where information about general COVID-19 and specific data (daily cases, number of deaths, number of tests, filiation rate, etc.) for Turkey is presented. We propose that by increasing the information specific to physiotherapy and rehabilitation in COVID-19, in addition to the general COVID-19 information in these areas, which physiotherapy and rehabilitation students prefer more, students will be able to access information about their own fields more easily.
In the current study, it was found that most students know that COVID-19 transmission is possible through contacting contaminated surfaces, inhaling large droplets, skin-to-skin contact/contacting with a patient, handshaking, and kissing. However, 66.7% of the students reported that airborne transmission could also occur. Although airborne viability of COVID-19 has been proven at low levels, airborne transmission has not yet been demonstrated except through inhaling a large airborne droplet [14, 15]. However, in our study, it was determined that the risk of transmission is high in long-term contact with large droplets, touching contaminated surfaces, and contact with inadequately cleaned or uncleaned surfaces, which are among the options marked by students as potential transmission routes [14]. The fact that the majority of the participants did not have information on the point of transmission from mother to fetus, blood transfusion, or breast milk gave similar results to the study conducted with medical students in the questionnaire we revised and used for physiotherapy and rehabilitation students in our current study [10]. It can be stated that this situation is caused by the limited amount of publications on pregnancy, birth, postpartum, and blood transfusion related to COVID-19 [10, 14, 16, 17]. It was determined that 95.6% of the participants knew the symptoms of COVID-19. Moreover, the participants were knowledgeable about transmission routes and preventive approaches. These results were similar to the results of the study by Jangra et al. [11] where 98% of physiotherapy students were knowledgeable about the symptoms of COVID-19 and preventive approaches. Similarly, the results of an article in which medical school students and students from other health-related departments were included also support our study [8]. In the related article, it was reported that only 3.36% of the students did not know the symptoms, and 91.61% of them had knowledge about preventive approaches [8]. In our current study, it was determined that 204 to 209 of the participants had knowledge about the physiotherapy and rehabilitation processes of COVID-19 in the hospital environment, and after the hospital. Since there are no data in the literature to compare these results with, it would not be possible to reach a definite conclusion about the level of knowledge. However, it can be argued that this may be due to the fact that about half of the participants are students who have not yet started clinical courses and have not encountered a patient with COVID-19.
Physiotherapy students gave an ambiguous result by marking almost the same level of different options for the question “I would not want to work with a patient with suspected COVID-19”. However, the number of students who do not want to apply physiotherapy to a patient with COVID-19 using protective materials/clothing is only 25. It can be said that new infectious diseases, with consequences that have not been fully understood or not known, generally cause great fear among the public [10, 18]. In our study, it can be stated that the uncertainty of the students about the future situation of COVID-19 stems from the points that are not yet understood. Likewise, it is seen that students are more sensitive about a family member contracting COVID-19 rather than having contracting the disease themselves. In this context, it can be said that the increasing mortality and morbidity due to COVID-19 with aging [19, 20] increases this sensitivity towards contracting the disease. It was seen that the majority of the participants did not have any reservations about being tested if they showed symptoms, and 63.0% wanted to be vaccinated. An effective vaccine offers the safest way to achieve herd immunity [21]. Assuming that the number of contacts varies significantly among individuals in the same age group, it has been reported that vaccinating 50% of the population may be sufficient for herd immunity [21]. Even if the rate of those who want to be vaccinated among our students is above this rate, that this rate can be considered low is low due to the possibility of contacting a patient with COVID-19, being a health worker candidate, and contacting with their families. Although participants do not want to keep it a secret whether they have COVID-19, it seems that they may be extremely stressed by the possibility of hospitalization. Khasawneh et al. [10] explained the reason for this for medical school students as follows: Although there is minimal stigma in medical students, it is probably because they think that it may lead to a sense of stigma among the general public and other student peers. It can be said that the same may be true for physiotherapy and rehabilitation students.
In our current study, it is shown that there is an increase in anxiety, level of concern, and depression, and a decrease in feelings of happiness and joy in physiotherapy students due to the COVID-19 pandemic. There are many studies in the literature that support our results caused by emotional changes. Strong correlations have been shown between the anxiety levels of psychological and social determinants related to COVID-19 [22]. It has been reported that the current COVID-19 pandemic causes psychological distress, anxiety, and depression in a large part of the general population [22]. It has been stated that there is a relationship between student satisfaction and the prevalence of depression, anxiety, and stress in students who continue their education with online platforms [23]. In our current study, it can be observed that anxiety and depression symptoms increase in physiotherapy students, as in the majority of the population, both during the online education process and during the lockdown periods.
The importance of wearing a mask [24], hand hygiene [25], and following social distance rules [26] are mentioned among the measures taken against COVID-19 are mentioned in the literature [27, 28]. It is seen that the results of our study are in line with the literature. In our study, it was found that 90.6% of the students wore masks, the majority of them paid attention to hand hygiene and 80.8% of them obeyed the social distancing rules. At the same time, as a responsible physiotherapy student, our study demonstrated that only 12.3% of the participants did not make any suggestions about the precautions that can be taken against COVID-19 to the patients and their relatives, while 295 always made suggestions. In this regards, we consider that it is important for physiotherapy students, who are in close contact with the patients, to make suggestions about the use of masks, hand hygiene, and social distance rules in terms of preventing the pandemic.
The importance of physiotherapy and rehabilitation practices in COVID-19 is frequently mentioned in the literature [3, 4, 6, 29–31]. The majority of the participants in our study agreed on the necessity and importance of physiotherapists and physiotherapy and rehabilitation in the acute period of COVID-19 during the intensive care process, and during the discharge period. Smondack et al. [32] stated that with the COVID-19 becoming a global pandemic, the health system adapted very quickly to the changing circumstances, and physiotherapists should be present at every stage of the treatment of patients during process. It has been stated that the aim is to maximize patients’ quality of life, and ensure the return to community participation in post-acute rehabilitation after COVID-19 with a comprehensive assessment and a progressive treatment plan that provides an individualized schedule [33]. In the same study, it was reported that with physiotherapy and rehabilitation, the full recovery of COVID-19 patients could be achieved (31). As seen in these two studies, it can be stated that the thoughts and awareness of the students participating in the study about the importance of physiotherapy and rehabilitation during the COVID-19 period will contribute positively to the treatment processes of patients with COVID-19.
There are some strengths and limitations of our study. Our study is one of the most comprehensive studies evaluating the knowledge, attitudes, behaviors, and precautions of physiotherapy and rehabilitation students about COVID-19 as a whole. Another strength of our study is the questionnaire prepared for medical school students [10], and rearranged for physiotherapy and rehabilitation students after obtaining permission, is the first questionnaire used for students in this field. At the same time, the cost-effectiveness of the survey method used, the short response time, and ease of accessibility by students are among the strengths of our study. Although detailed results of COVID-19 on physiotherapy and rehabilitation students were presented in our study, there are some limitations of our study. These include the fact that the students researched the answers to some questions before answering them, and that some students who had not yet entered the clinic and practice courses answered the questionnaire. At the same time, because of the online structure of the questionnaire used in the study, physiotherapy and rehabilitation students who did not have internet access were not able to participate in the study. Considering the strengths of our study, we believe that these limitations did not affect the study.
5Conclusion
The COVID-19 pandemic has affected the world since the end of 2019, and the persistence of the pandemic requires that physiotherapy and rehabilitation students are aware of the circumstances and consequences of COVID-19. In light of the current findings, we determined that students in our research, who are the future physiotherapist candidates, have satisfactory levels of awareness about COVID-19. Nonetheless, physiotherapy and rehabilitation students need to be included in appropriate educational programs to protect themselves, as well as their inner circle, and their patients against COVID-19, and their knowledge about treatment methods should be increased.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
The authors report no funding.
Acknowledgments
We would like to thank Dr. Khalid A. Kheirallah, who granted us permission to use the questionnaire prepared for medical school students by giving permission to reorganize and adapt it for physiotherapy and rehabilitation students in our study. We also thank the physiotherapy and rehabilitation students who agreed to participate in the study and answered the questionnaire.
References
[1] | World Health Organization, Coronavirus disease 2019 (COVID-19) Situation Report 46 (2020) . |
[2] | Guan WJ , Ni ZY , Hu Y , Liang WH , Ou CQ , He JX , et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. (2020) ;382: (18):1708–20. |
[3] | Thomas P , Baldwin C , Bissett B , Boden I , Gosselink R , Granger CL , et al. Physiotherapy management for COVID-19 in the acute hospital setting: Clinical practice recommendations. J Physiother. (2020) ;66: (2):73–82. |
[4] | Yang LL , Yang T . Pulmonary rehabilitation for patients with coronavirus disease 2019 (COVID-19). Chronic Dis Transl Med. (2020) ;6: (2):79–86. |
[5] | Al Attar WSA , Husain MA . Physiotherapists’ knowledge and the implementation of COVID-19 infection prevention and control measures. Work. (2021) ;69: (2):351–8. |
[6] | Iannaccone S , Castellazzi P , Tettamanti A , Houdayer E , Brugliera L , de Blasio F , et al. Role of rehabilitation department for adult individuals with COVID-19 The experience of the san raffaele hospital of milan. Arch Phys Med Rehabil. (2020) ;101: (9):1656–61. |
[7] | Felten-Barentsz KM , van Oorsouw R , Klooster E , Koenders N , Driehuis F , Hulzebos EHJ , et al. Recommendations for hospital-based physical therapists managing patients with COVID-19. phys ther. (2020) ;100: (9):1444–57. |
[8] | Gohel KH , Patel PB , Shah PM , Patel JR , Pandit N , Raut A . Knowledge and perceptions about COVID-19 among the medical and allied health science students in India: An online cross-sectional survey. Clin Epidemiol Glob Health. (2020) . |
[9] | Srivastav AK , Sharma N , Samuel AJ . Impact of Coronavirus disease-19 (COVID-19) lockdown on physical activity and energy expenditure among physiotherapy professionals and students using web-based open E-survey sent through WhatsApp, Facebook and Instagram messengers. Clin Epidemiol Glob Health. (2020) . |
[10] | Khasawneh AI , Humeidan AA , Alsulaiman JW , Bloukh S , Ramadan M , Al-Shatanawi TN , et al. Medical students and COVID-19: knowledge, attitudes, and precautionary measures. A descriptive study from jordan. Front Public Health. (2020) ;8: :253. |
[11] | Jangra MK , Saxena A , Anurag P . Knowledge and awareness among physiotherapy students to combat COVID-19: A questionnaire based study. Clinical Epidemiology and Global Health. (2021) ;11: :100748. |
[12] | Loweke R . A doctor of physical therapy student’s experience during the COVID-19 pandemic. Home Healthc Now. (2021) ;39: (1):49. |
[13] | Raosoft Inc. RaoSoft® sample size calculator. (2004) . Available from: http://www.raosoft.com/samplesize.html |
[14] | Carraturo F , Del Giudice C , Morelli M , Cerullo V , Libralato G , Galdiero E , et al. Persistence of SARS-CoV-2 in the environment and COVID-19 transmission risk from environmental matrices and surfaces. Environ Pollut. (2020) ;265: (Pt B):115010. |
[15] | Comber L , Murchu EO , Drummond L , Carty PG , Walsh KA , De Gascun CF , et al. Airborne transmission of SARS-CoV-2 via aerosols. Rev Med Virol. (2021) ;31: (3):e2184. |
[16] | Cho HJ , Koo JW , Roh SK , Kim YK , Suh JS , Moon JH , et al. COVID-19 transmission and blood transfusion: A case report. J Infect Public Health. (2020) ;13: (11):1678–9. |
[17] | Karimi-Zarchi M , Neamatzadeh H , Dastgheib SA , Abbasi H , Mirjalili SR , Behforouz A , et al. Vertical transmission of coronavirus disease 19 (COVID-19) from infected pregnant mothers to neonates: A review. Fetal Pediatr Pathol. (2020) ;39: (3):246–50. |
[18] | Person B , Sy F , Holton K , Govert B , Liang A , Garza B , et al. Fear and stigma: The epidemic within the SARS outbreak. Emerging Infectious Disease Journal. (2004) ;10: (2):358. |
[19] | Chen Y , Klein SL , Garibaldi BT , Li H , Wu C , Osevala NM , et al. Aging in COVID-19: Vulnerability, immunity and intervention. Ageing Res Rev. (2021) ;65: :101205. |
[20] | Pence BD . Severe COVID-19 and aging: Are monocytes the key? Geroscience. (2020) ;42: (4):1051–61. |
[21] | Fontanet A , Cauchemez S . COVID-19 herd immunity: Where are we? Nat Rev Immunol. (2020) ;20: (10):583–4. |
[22] | Petzold MB , Bendau A , Plag J , Pyrkosch L , Mascarell Maricic L , Betzler F , et al. Risk, resilience, psychological distress, and anxiety at the beginning of the COVID-19 pandemic in Germany. Brain Behav. (2020) ;10: (9):e01745. |
[23] | Fawaz M , Samaha A . E-learning: Depression, anxiety, and stress symptomatology among Lebanese university students during COVID-19 quarantine. Nurs Forum. (2021) ;56: (1):52–7. |
[24] | Wang J , Pan L , Tang S , Ji JS , Shi X . Mask use during COVID-19: A risk adjusted strategy. Environ Pollut. (2020) ;266: (Pt 1):115099. |
[25] | Ma QX , Shan H , Zhang HL , Li GM , Yang RM , Chen JM . Potential utilities of mask-wearing and instant hand hygiene for fighting SARS-CoV-2. J Med Virol. (2020) ;92: (9):1567–71. |
[26] | Morawska L , Cao J . Airborne transmission of SARS-CoV-2: The world should face the reality. Environ Int. (2020) ;139: :105730. |
[27] | Feiz Arefi M , Babaei-Pouya A , Poursadeqiyan M . The health effects of quarantine during the COVID-19 pandemic. Work. (2020) ;67: (3):523–7. |
[28] | Arefi MF , Poursadeqiyan M . A review of studies on the COVID-19 epidemic crisis disease with a preventive approach. Work. (2020) ;66: (4):717–29. |
[29] | Landry MD , Geddes L , Park Moseman A , Lefler JP , Raman SR , Wijchen JV . Early reflection on the global impact of COVID-19, and implications for physiotherapy. Physiotherapy. (2020) ;107: :A1–a3. |
[30] | Battaglini D , Robba C , Caiffa S , Ball L , Brunetti I , Loconte M , et al. Chest physiotherapy: An important adjuvant in critically ill mechanically ventilated patients with COVID-19. Respir Physiol Neurobiol. (2020) ;282: :103529. |
[31] | Lee AJY , Chung CLH , Young BE , Ling LM , Ho BCH , Puah SH , et al. Clinical course and physiotherapy intervention in 9 patients with COVID-19. Physiotherapy. (2020) ;109: :1–3. |
[32] | Smondack P , Gravier F , Prieur G , Repel A , Muir JF , Cuvelier A , et al. Physiotherapy and COVID-19. From intensive care unit to home care-An overview of international guidelines. Rev Mal Respir. (2020) ;37: (10):811–22. |
[33] | Sheehy LM . Considerations for postacute rehabilitation for survivors of COVID-19. JMIR Public Health Surveill. (2020) ;6: (2):e19462. |


