
Knowledge, attitude, and behaviour of dentists working during the COVID-19 pandemic: A cross-sectional survey
Abstract
BACKGROUND:
The coronavirus disease 2019 (COVID-19) has immensely affected the world’s population at physical and psychosocial levels. Dentists are no different from other healthcare providers, as they are equally if not more exposed to the threat of getting infected.
OBJECTIVE:
To assess the experience and behavior of public and private sector dentists practicing during the COVID-19 pandemic and their knowledge about it.
METHODS:
A cross-sectional survey was conducted online by sharing google forms through email, WhatsApp, and Facebook. The survey included questions on the knowledge, attitude, and behavior of dentists practicing during COVID-19. The data was interpreted by SPSS 24 using a chi-square test, and a value of p < 0.05 was considered significant.
RESULTS:
A considerable number of general dentists (26.9%) and specialists (39.4%) adopted partial suspension of clinics. Restriction’s ease allowed 50.2% of the clinicians to resume their duties. 67.9% of the patients were medicated online during the lockdown phase. There was no significant difference regarding years of experience and willingness to treat/care (p-value 0.648). Personal protective equipment (PPE) was readily available for use in public or private practices, and the respondents agreed with its efficacy in protecting the operators. Compliance with PPE wear was 50% in all the respondents.
CONCLUSION:
The psychosocial repercussion of the pandemic continues to affect dental practices. Our attitude needs to improve as far as PPE is concerned, with regular training workshops and continuous updates of the developing Knowledge on COVID-19.
1Introduction
The coronavirus disease 2019 (COVID-19) originated first in Wuhan, China’s city was declared a global pandemic by WHO in March 2020. Much time has elapsed since the outbreak of this disease surfaced on 24th November 2019, dentists. The symptoms of the coronavirus range from flu-like symptoms to respiratory failure, and the vaccine is far from getting available, and the care is mainly palliative. Health care professionals are at the highest risk of contracting this virus from their patients or co-workers [1, 2]. Dentists are also close to their staff and patients, and they are considered one of the high-risk category health workers [3]. In-depth analysis of the transmission mode of virus highlighted that in dentistry, transmission is through airborne inhalation and touch through contaminated surfaces [4, 5]. Oral manifestations of burning mouth syndrome-like symptoms, loss of taste, and smell are essential for dentists as they might see patients with these complaints [6, 7]. COVID-19 virus is present in saliva for around one month, although active symptoms subside in 16–18 days [8]. This further intensifies the risk of dentists getting infected because of the nature of the work. Thus, extra preventive measures are necessary to avoid it [9].
The growing fear of COVID-19 infection transmission has mandated the development of new guidelines and recommendations by health authorities [4, 10]. dental practice suspended [11], and only emergency services rendered through triage to prevent transmission of disease through dental offices and hospitals [12–15].
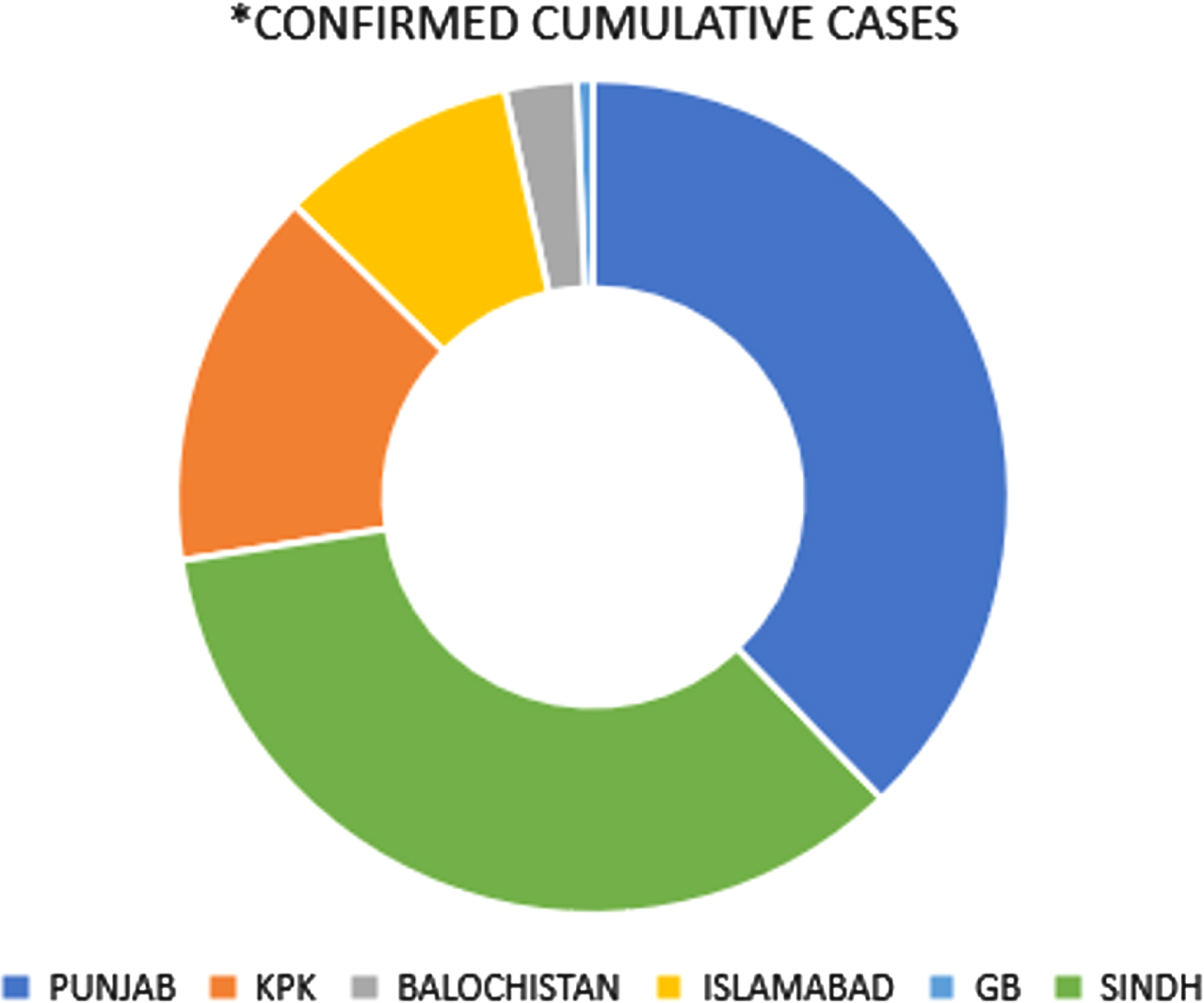
Figure 1 illustrates the number of current cases in Pakistan as the country heads to another smart lockdown for the third time. Initially, all dental teaching colleges and their hospitals were closed throughout the country with a primary focus on emergency dental services, e.g., to alleviate pain, stop bleeding, manage trauma and stop the spread of recurrent infections [16, 17]. The idea was to redirect all personal protective equipment to doctors taking care of COVID-19 patients [18, 19]. National policy since 23rd March 2020 has been for primary care triage to focus initially on the provision of the three As Advice; Analgesia; Antimicrobials where appropriate [16, 20]. Unless urgent or emergency care is required, mild and moderate dental symptoms were managed remotely by providing advice and analgesics and antimicrobials where applicable. Azithromycin, paracetamol, and ibuprofen commonly prescribed in dentistry also identified as potentially beneficial in defense against the virus at least helpful in dealing with the complications [20].
Fig. 1
Confirmed cumulative cases. Data Source: Government of Pakistan, https://covid.gov.pk/stats/pakistan. Updated on May 9th, 2021.
The knowledge related to the virulence of the COVID-19 virus is critical in understanding the effects, even though the information is limited. Knowledge is scarce in less than fifty percent of staff working in Orthodontic clinics than what they perceive concerning the COVID-19 pandemic. Only two-thirds of the team was willing to work after the resumption of work after lockdown finished. Recommendations for training programs plan to increase healthcare workers’ understanding regarding the virus and the sufficient protection required before treating patients [21]. Hand hygiene is essential not only for health professionals but also for basic domestic activities [22]. Government-issued a detailed document regarding correct PPE (personal protective equipment) usage in and around patients either in a hospital setting or doing quarantine at home. However, its application and importance in dentistry are vital to prevention and care [23].
The survey highlights dentists’ preparedness and perception towards combating the COVID-19 pandemic in clinical practice white adhering to recommended safety protocols. Despite the positive attitude of dental professionals and proper practice of “transmission-based precautions” in general, the current situation of COVID-19 in the country is not up to the mark with a shortage of training and facilities [14, 18, 25]. Moreover, if not allowed to work or choose not to work in the current COVID-19 situation, most people find it quite hard to make ends meet [24, 25].
2Methods
This was a convenience-sample survey conducted among dentists working in different sectors from and was conducted between 10 and 22 January 2021. Ethical approval was obtained from Rashid Latif College Lahore (RLDC/00517/20). Participants informed in the online survey of the ethical considerations, especially voluntary participation, respondent anonymity, and data usage. Submission considered as consent to participate.
The inclusion criteria include General Dentists and specialists working in public and private sector dental practices, hospitals, and academic institutions. Exclusion criteria included non-practicing dentists or undergraduate dental students and questionnaires with incomplete answers and apparent mistakes. As a pilot project, the survey is given to a small group of clinicians to check for validity and reliability. The survey form starts with a brief introduction keeping the anonymity of the participants intact, and the submission of the survey form was considered consent to participate.
The survey (Appendix) included a forty-item questionnaire developed with modification for general dentists to assess the knowledge, behavior, and attitude of healthcare professionals [24, 25]. Questions #1-8 were about the demographics and general information of the participants, with Questions #3 and #5 met in light of Pakistan’s educational and practice environments. Questions #16 added to add all the procedures performed in general dentistry. Questions #9–14 were about workplace information, and #15-18 were related to individual experiences in practice during the pandemic. Four questions were in the knowledge section (#19 to #22), with #19 and #21 following the Likert scale. The following four questions were about their readiness to treat/care for patients confirmed or suspected with COVID-19. The last fourteen questions assessed the knowledge, general attitude, and practice of cross infection control and personal protective equipment measures.
The public and private sector dentists attempt the survey after the pilot estimate, using a purposive sampling technique. The sample size was 244, with a margin of error at 5% and a confidence level set at 95%.
The questionnaires exclude all questions with incomplete answers and apparent mistakes. Google Forms is used to collect the survey form and send it to the participants through WhatsApp, Facebook messenger, and email. The result is downloaded as a Microsoft excel sheet and put in SPSS 24 for statistical interpretation at the end of the study.
The data analysis uses descriptive statistics and counts and percentages categorical show data. The Chi-square test investigated the correlation between specific, definite groups important to the study [19].
3Results
An exalted percentage of female participants and age group 31-40 years participated in this survey (53.4%). Moreover, more significant percentages of the participants were doing private practice (43.3%) and were living with their parents (29.7%). Moreover, as many as 50.2 % of respondents did not have online consultation at work during the COVID-19 pandemic.
The highest percentage of specialists went for a partial suspension of their dental practices during the pandemic compared to general dentists. A low percentage also were specialists who did not suspend their practices (p-value < 0.05). Moreover, many dentists having up to 5 years of dental practice partially suspended their clinics. No one with over 20 years of dental practice opted for ‘no suspension’ of their clinical practices (Table 1). However, the highest percentage of respondents have partially resumed dental services at work (50.2%). The exact rate continued dental service at their private practices.
Table 1
Table1
| Characteristics | Category | Count (N) and Percentage (%) | What was the status of the dental services in your workplace during the pandemic? | P-value | ||
| Complete suspension | Partial suspension | No suspension | ||||
| Highest academic | General Dentist | N % | 45 (18.1%) | 67 (26.9%) | 9(3.6%) | 0.001 |
| degree | Specialist | N % | 23(9.2%) | 98 (39.4%) | 7(2.8%) | |
| Years of dental | ≤5 years | N % | 35(14.1%) | 64(25.7%) | 10(4%) | 0.036 |
| practice (including | 6 to 10 years | N % | 5(2%) | 35(14.1%) | 4(1.6%) | |
| postgraduate | 11 to 15 years | N % | 23(9.2%) | 47(18.9%) | 2(0.8%) | |
| education period) | > 20 years | N % | 5 (2%) | 19(7.6%) | 0 (0%) | |
67.9% of the patients were medicated online during the lockdown phase. Out of these, the highest percentage of dental service providers (44.6%) medicated less than five patients per week on the phone during the pandemic. Dental professionals frequently suggested only medication rather than a procedure during the COVID-19 pandemic. The most considerable number of dentists had acquired prior knowledge from the patients regarding the symptoms of Covid-19 by contacting them through the phone (59.4%).
The highest percentage of general dentists agree, and specialists agree to understand the relevant Knowledge of COVID-19 (p-value <,0.05, Table 2). TV, internet, and medical journals accounted for the most Knowledge about COVID-19 (19.3%). The highest percentage of dentists who did not complete the COVID-19 training still agree that they understand the relevant Knowledge of COVID-19, but lesser percentages agree. Moreover, the higher percentages of dentists who completed the COVID-19 training agree that they know the relevant knowledge of COVID-19. In contrast, lesser portions agree (p-value < 0.05). A considerable number of dentists also decided that they understood the risks and relevant Knowledge of COVID-19 (p-value 0.000, Table 2).
Table 2
| Characteristics | Category | Count (N) and Percentage (%) | Do you understand the relevant knowledge of COVID-19? | P-value | ||
| Agree | Completely agree | Neither agree nor disagree | ||||
| Have you completed the training | No | N % | 98 (39.4%) | 46 (18.5%) | 18 (7.2%) | 0.001 |
| program about COVID-19? | Yes | N % | 40 (16.1%) | 44 (17.7%) | 3 (1.2%) | |
| You are confident that you understand | Agree | N % | 102 (41 %) | 22 (8.8%) | 4 (1.6%) | 0.000 |
| the risks of the COVID-19 pandemic | Completely agree | N % | 23 (9.2%) | 66 (26.5%) | 5 (2%) | |
| for patients and health care workers. | ||||||
Both general dentists and specialists were willing to treat/ and care for patients, showing no significant difference (p-value 0.523). Moreover, there was no significant difference regarding years of experience and willingness to treat/care for the COVID-19 patients (p-value 0.648). This finding highlight that all the dental service providers with any number of dental experiences are willing to provide dental treatment to the COVID-19 patients (Table 3). A low percentage of respondents (33.3 %) had treated or cared for patients with COVID-19. Moreover, very few dentists (23.3 %) have an established clinic where suspected or confirmed COVID-19 patients get treatment, and most do not know where they should refer for urgent treatment during the COVID-19 outbreak.
Table 3
| Characteristics | Category | Count (N) and Percentage (%) | Are you willing to treat or care for patients confirmed or suspected with COVID-19 if you have the opportunity? | p-value | |
| No | Yes | ||||
| Highest academic degree | General Dentist | N | 67 | 54 | 0.523 |
| % | 26.9% | 21.7% | |||
| Specialist | N | 76 | 52 | ||
| % | 30.5% | 20.9% | |||
| Years of dental practice | ≤5 years | N | 58 | 51 | 0.648 |
| (including postgraduate | % | 23.3% | 20.5% | ||
| education period) | 6 to 10 years | N | 28 | 16 | |
| % | 11.2% | 6.4% | |||
| 11 to 15 years | N | 43 | 29 | ||
| % | 17.3% | 11.6% | |||
| > 20 years | N | 14 | 10 | ||
| % | 5.6% | 4.0% | |||
A high percentage of practitioners agreed that they understood how to protect themselves and patients from COVID-19, with general practitioners a little more so (p-value < 0.05). Based on years of experience, a significantly higher number of dental practitioners with experience of up to 5 years are more confident in protecting themselves from COVID-19 (p-value < 0.05, Table 4). The highest percentage use correct personal protective equipment (PPE) includes (37.3%). Dentists wear goggles and a face shield simultaneously during an aerosol-generating procedure. The highest percentage of dentists only wear a surgical mask during precheck triage / dental radiology and oral examination / low-risk procedures.
Table 4
| Characteristics | Category | Count (N) and Percentage (%) | You are confident that you understand how to protect yourself and your patients during the COVID-19 pendemic | p-value | |||
| Agree | Completely agree | Neither agree nor disagree | Disagree | ||||
| Highest academic degree | General Dentist | N | 70 | 35 | 11 | 5 | 0.02 |
| % | 28.1% | 14.1% | 4.4% | 2.0% | |||
| Specialist | N | 60 | 53 | 15 | 0 | ||
| % | 24.1% | 21.3% | 6.0% | 0.0% | |||
| Years of dental practice | ≤5 years | N | 67 | 27 | 10 | 5 | 0.000 |
| (including postgraduate | % | 26.9% | 10.8% | 4.0% | 2.0% | ||
| education period) | 6 to 10 years | N | 26 | 16 | 2 | 0 | |
| % | 10.4% | 6.4% | 0.8% | 0.0% | |||
| 11 to 15 years | N | 27 | 40 | 5 | 0 | ||
| % | 10.8% | 16.1% | 2.0% | 0.0% | |||
| > 20 years | N | 10 | 5 | 9 | 0 | ||
| % | 4.0% | 2.0% | 3.6% | 0.0% | |||
Most dentists clean their hands using soap and water or an alcohol-based hand rub (92%). A significantly greater number of general and specialist dentists agree that it is not adequate to use only alcohol-based hand rub if hands are visibly soiled. However, the highest percentage of young dental practitioners with up to 5 years of experience agree that alcohol-based hand rubs are adequate if hands are visibly soiled (Table 5). A small percentage of both general and specialist dental surgeons perceive that correct PPE usage eliminates the need for hand hygiene. Still, the insignificant p-value highlighted that both have the almost same opinion that the proper use of PPE does not eliminate the need for hand hygiene. Similarly, an exceedingly small percentage in all categories of dental practice has the perception that correct PPE removes the need for hand hygiene. Still, the insignificant p-value emphasized that all sorts of years of dental practice point to a similar opinion that the correct use of PPE does not eliminate the need for hand hygiene (Table 6).
Table 5
| Characteristics | Category | Count (N) and Percentage (%) | It is adequate to use an alcohol-based hand rub if the hands are visibly soiled | p-value | |
| TRUE | FALSE | ||||
| Highest academic degree | General Dentist | N | 50 | 71 | 0.055 |
| % | 20.1% | 28.5% | |||
| Specialist | N | 38 | 90 | ||
| % | 15.3% | 36.1% | |||
| Years of dental practice | ≤5 years | N | 54 | 55 | 0.000 |
| (including postgraduate | % | 21.7% | 22.1% | ||
| education period) | 6 to 10 years | N | 14 | 30 | |
| % | 5.6% | 12.0% | |||
| 11 to 15 years | N | 15 | 57 | ||
| % | 6.0% | 22.9% | |||
| > 20 years | N | 5 | 19 | ||
| % | 2.0% | 7.6% | |||
Table 6
| Characteristics | Category | Count (N) and Percentage (%) | Use of correct PPE eliminates the need for hand hygiene | p-value | |
| TRUE | FALSE | ||||
| Highest academic degree | General Dentist | N | 13 | 108 | 0.202 |
| % | 5.2% | 43.4% | |||
| Specialist | N | 8 | 120 | ||
| % | 3.2% | 48.2% | |||
| Years of dental practice | ≤5 years | N | 14 | 95 | 0.11 |
| (including postgraduate | % | 5.6% | 38.2% | ||
| education period) | 6 to 10 years | N | 2 | 42 | |
| % | 0.8% | 16.9% | |||
| 11 to 15 years | N | 5 | 67 | ||
| % | 2.0% | 26.9% | |||
| > 20 years | N | 0 | 24 | ||
| % | 0.0% | 9.6% | |||
The majority of the dentists (42%) agree that the recommended PPE is readily available in their hospital or clinic. The highest percentage of dentists agree to use PPE for keeping dental staff from getting COVID-19 (53.8%), but inconvenient to use recommended PPE when treating/caring for patients (33.3%). However, the highest percentage of general dentists, as well as specialists, agree to remove PPE immediately before leaving the treatment room, and an insignificant p-value presenting the same opinion in both general dentists and specialists towards removing PPE immediately before leaving the treatment room (p-value –0.089, Table 7). The highest percentage of specialists disagree to forget often to change PPE, and the second-highest percentage of general dentists agree to forget often to change PPE between patients. The significant p-value presents an important perception towards ignoring PPE change between patients (Table 7).
Table 7
| Characteristics | Category | Count (N) and percentage (%) | Highest academic degree | p-value | |
| General dentist | Specialist | ||||
| Do you understand | Agree | N | 82 | 56 | 0.001 |
| the relevant knowledge | % | 32.9% | 22.5% | ||
| of COVID-19? | Completely agree | N | 30 | 60 | |
| % | 12.0% | 24.1% | |||
| Neither agree nor disagree | N | 9 | 12 | ||
| % | 3.6% | 4.8% | |||
| You will remove your PPE | Agree | N | 64 | 55 | 0.089 |
| immediately when you | % | 25.7% | 22.1% | ||
| leave the treatment room | Completely agree | N | 42 | 41 | |
| % | 16.9% | 16.5% | |||
| Neither agree nor disagree | N | 6 | 16 | ||
| % | 2.4% | 6.4% | |||
| Disagree | N | 7 | 9 | ||
| % | 2.8% | 3.6% | |||
| Completely disagree | N | 2 | 7 | ||
| % | 0.8% | 2.8% | |||
| You often forget to change | Agree | N | 38 | 26 | 0.018 |
| PPE between patients | % | 15.3% | 10.4% | ||
| Completely agree | N | 12 | 10 | ||
| % | 4.8% | 4.0% | |||
| Neither agree nor disagree | N | 34 | 26 | ||
| % | 13.7% | 10.4% | |||
| Disagree | N | 25 | 40 | ||
| % | 10.0% | 16.1% | |||
| Completely disagree | N | 12 | 26 | ||
| % | 4.8% | 10.4% | |||
Moreover, most dentists said head nurses or attending doctors would reprimand them if they failed to use protective equipment when treating or caring for patients (45.8%). Furthermore, most believe that compliance can be improved if they follow recommended safety measures. Most of the respondents estimated 50% compliance to recommended PPE during treatment or care of patients after work resumption.
4Discussion
A significant number of participants (both general dentists and specialists) responded with an increasing trend to a partial suspension of their clinics, showing the pandemic’s impact on dental services. It is in line with the literature published before, keeping the health and safety of the people in mind to prevent human-human transmission in dental setup [1, 5, 14, 15]. Moreover, very few respondents (33.3 %) had treated or cared for patients with COVID-19, with an insignificant correlation between general dentists and specialists, showing the hesitancy in their behavior to treat such patients. Furthermore, very few dentists (23.3 %) have an established clinic were suspected or confirmed COVID-19 patients get treatment. Most do not know where they should refer for urgent treatment during the COVID-19 outbreak. These results align with a previous study in Pakistan, as many dentists face challenging situations and financial loss during this pandemic due to inflation, low patient flow, and lack of protective equipment, forcing them to close their clinics [26]. Many dental practitioners did not have the financial backing to improve the facilities in their clinics or take extra precautionary measures according to COVID-19 cross infection control protocols implemented by WHO or American Dental Association (ADA, 27).
COVID-19 infodemic involved the circulation of misinformation and disinformation involving many aspects of the disease, including vaccination, lack of teamwork, lack of access to COVID-19 tools like diagnostic kits or PPE kits in private or hospital setup [28, 29]. A negligible number of participants supported COVID-19 designated hospitals (14.5%) or community work (9.6%), a lot of them did not participate in any anti- pandemic activity (65.9%). There is generalized fear or hesitancy among the dentists to work collectively in the dental clinics or do community work, which shows the psychological impact of the current pandemic among the health care workers worldwide, which was accompanied by an infodemic [28].
Interestingly, a significant percentage of participants did not do online consultation (63.5%) in the lockdown phase. A small number of participants (44.6%) medicated less than five patients during the closure, contrary to the literature recommendation to prevent complications [20]. The probable reason might be that dentistry requires intervention to relieve the patients’ pain, whereas just medicating the patient has a small but vital role. Lack of facilities and preparation for online consultations could be a formative factor because Pakistan, still being a developing country, lags in technology as compared to other developing countries of the South Asia region [29, 30].
There is an insignificant correlation between specialists and general dentists showing a willingness to practice on COVID-19 confirmed/suspected patients. The participants give preliminary information before the appointment (59.4%). The majority of the dentists preferred medicating the patients and reappointing them if there was no emergency. However, besides medication, the most common procedure was dental extraction and prosthetic work. It is in line with the previous literature recommendation to defer or reduce aerosol-generating procedure to the minimum [1, 5].
A considerable number of respondents who underwent training for COVID-19 showed a greater understanding of its risk, further highlighting the need for increased knowledge in the respective field. It matches the previous recommendation of enhancing the training of health care professionals related to a better understanding of the COVID-19 pandemic [19, 21]. General dentists showed a better understanding of protecting themselves and the patients than the specialists. Moreover, practitioners with little experience are more confident in protecting themselves and the patients. Our study highlights that higher academic degree holders and experience displayed more apprehension of the cause and effect of understanding and practice. A recent study shows that older health care workers experienced more significant anxiety about their own and their family’s safety (along with their patients) but maintained the professional obligation to complete their work effectively. The authors also observed that older staff had increased stress related to (lack of) PPE and longer work hours [11, 31, 32].
Several participants, specialists, and general dentists equitably believe that correct PPE does not eliminate the need for hand hygiene. Many dental practitioners believe alcohol-based hand rub is insufficient to ensure hand hygiene if hands are soiled. However, dentists with five years and less experience think otherwise. Past literature has handed out detailed guidelines and recommendations regarding hand hygiene, and the results of our study are in line with it [22]. 37.3% of the participants choose the correct protocol of PPE. Still, the authors believe the number is not enough and a lot more people need to get the right concept and training. Many specialists agree more than the general dentists to remove the PPE before leaving the surgery. However, a substantial number still fail to change PPE between patients, showing the prevailing attitude. This attitude towards wearing PPE is typical in the past literature [33]. Either they feel it as an extra burden during practice [29], or they are casual about it, which is not agreeable.
The limitation of the present study was the use of self-reported data, which can underestimate or overestimate the study participants’ responses. Our study collected data in a limited period during which the pandemic spread rapidly, and vaccination programs started among healthcare professionals in Pakistan. However, in light of emerging new variants of the virus and anticipated treatment of COVID-19, dentists’ knowledge, attitudes, and practices may change
5Conclusion
In the alleviation stage of the COVID-19 pandemic, when dental services are gradually resuming, a good percentage of dentists believe that they understand the COVID-19-related risks. Although our research implies improvement in knowledge, confidence and preparedness require more work. Training programs are essential to ensure safety and proper protection. The aim is to balance the health and well-being of the dentists and, at the same time, guarantee the highest and safest dental care for the public.
Conflict of interest
None to report.
Acknowledgements
We would like to thank all the Pakistani dentists who took precious time out of their busy schedule to participate in the survey.
Funding
None to report.
Supplementary materials
[1] The appendix is available from https://dx.doi.org/10.3233/WOR-211018.
References
[1] | Barabari P , Moharamzadeh K , Novel coronavirus (covid-19) and dentistry–a comprehensive review of literature, Dent J (2020) ;8: (2):1–18. |
[2] | Mahase E , Covid-19: WHO declares pandemic because of “alarming levels” of spread, severity, and inaction. BMJ [Internet]. (2020) ;368: (March):m1036. Available from: https://dx.doi.org/doi:10.1136/bmj.m1036. |
[3] | Gamio L , The workers who face the greatest coronavirus risk. New York Times. 2020;. |
[4] | Bhumireddy J , Mallineni SK , Nuvvula S , Challenges and possible solutions in dental practice during and post COVID-19, Environ Sci Pollut Res (2021) ;28: (2):1275–7. |
[5] | Bourley J , Jian G , Lubamba G , Yu W , Milolo A , Bushabu F , et al., Covid-19-Related Considerations in Stomatology: Short Communication, Int J Med Rev Case Reports (2020) ;4: (0):1. |
[6] | Arefi MF , Poursadeqiyan M , A review of studies on the COVID-19 epidemic crisis disease with a preventive approach, Work (2020) ;66: (4):717–29. |
[7] | Odeh ND , Babkair H , Abu-Hammad S , Borzangy S , Abu-Hammad A , Abu-Hammad O , COVID- 19 Present and future challenges for dental practice, Int J Environ Res Public Health (2020) ;17: (9). |
[8] | Alharbi A , Alharbi S , Alqaidi S , Guidelines for dental care provision during the COVID-19 pandemic. Saudi Dent J [Internet]. (2020) ;32: (4):181–6.Available from: https:// doi.org/10.1016/j.sdentj.2020.04.001. |
[9] | Baghizadeh Fini M , What dentists need to know about COVID-19. Oral Oncol [Internet]. 2020;105(April): 104741. Available from: https://doi.org/10.1016/j.oraloncology.2020.104741. |
[10] | Lai J , Ma S , Wang Y , Cai Z , Hu J , Wei N , et al., Factors associated with mental health outcomes among health care workers exposed to coronavirus disease, JAMA Netw Open (2039) ;3: (3):e203976–e203976. |
[11] | Ahmed MA , Jouhar R , Ahmed N , Adnan S , Aftab M , Zafar MS , et al., Fear and practice modifications among dentists to combat novel coronavirus disease (COVID-19) outbreak, Int J Environ Res Public Health (2020) ;17: (8). |
[12] | Omidi L , Moradi G , Mostofi Sarkari N , Risk of COVID-19 infection in workplace settings and the use of personal protective equipment, Work (2020) ;66: (2):377–8. |
[13] | Banaee S , Claiborne DM , Akpinar-Elci M , Occupational health practices among dental care professionals before and during the COVID-19 pandemic, Work (2021) ;68: (4):993–1000. |
[14] | Kh Mahmud P , Ali SM , Khdr Sabir D , Impacts of novel pandemic coronavirus (COVID-19) outbreak on dental practice: A review of the current literature, Edorium J Dent [Internet].40-1. Available from (1000) ;7: (May).http://www.edoriumjournalofdentistry.com. |
[15] | Cotrin P , Peloso RM , Oliveira RC , de Oliveira RCG , Pini NIP , Valarelli FP , et al., Impact of coronavirus pandemic in appointments and anxiety/concerns of patients regarding orthodontic treatment, Orthod Craniofacial Res (2020) ;23: (4):455–61. |
[16] | NHS Education for Scotland. Management 499 of Acute Dental Problems. Scottish Dent Clin Eff Progr. 2020;(March):22-3. |
[17] | Yang Y , Zhou Y , Liu X , Tan J , Health services provision of 48 public tertiary dental hospitals during the COVID-19 epidemic in China, Clin Oral Investig (2020) ;24: (5):1861–4. |
[18] | Waris A , Atta UK , Ali M , Asmat A , Baset A , COVID-19 outbreak: current scenario of Pakistan, New Microbes New Infect (2020) ;35: (20):100681. |
[19] | Putrino A , Raso M , Magazzino C , Galluccio G , Coronavirus (COVID-19) in Italy: Knowledge, management of patients and clinical experience of Italian dentists during the spread of contagion, BMC Oral Health (2020) ;20: (1):1–15. |
[20] | Dental S , Drugs for the Management of Dental Problems During COVID-19 Pandemic. Scottish Dent Clin Eff Progr. 2020;(April):1-15. |
[21] | Hua F , Qin D , Yan J , Zhao T , He H , COVID-19 Related Experience, Knowledge, Attitude, and Behaviors Among 2,669 Orthodontists, Orthodontic Residents, and Nurses in China: A Cross-Sectional Survey, Front Med (2020) ;7: (August):1–13. |
[22] | Boyce JM , Pittet D , Guideline for hand hygiene in healthcare settings: Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force, Am J Infect Control (2002) ;30: (8). |
[23] | Robbins L , National Guidelines, Am J Health Plann (1978) ;3: (1). |
[24] | Shi Y , Wang J , Yang Y , Wang Z , Wang G , Hashimoto K , et al., Knowledge and attitudes of medical staff in Chinese psychiatric hospitals regarding COVID-19. Brain, Behav Immun - Heal [Internet].(1000) ;4: (March):100064. Available from: https://doi.org/10.1016/j.bbih.2020.100064. |
[25] | Daugherty EL , Perl TM , Rubinson L , Bilderback A , Rand CS , Survey Study of the Knowledge, Attitudes, and Expected Behaviors of Critical Care Clinicians Regarding an Influenza Pandemic, Infect Control Hosp Epidemiol (2009) ;30: (12):1143–9. |
[26] | Farooq I , Ali S , COVID-19 outbreak and its monetary implications for dental practices, hospitals and healthcare workers, Postgrad Med J (2020) ;96: (1142):791–2. |
[27] | Abrar E , Abduljabbar AS , Naseem M , Panhwar M , Vohra F , Abduljabbar T , Evaluating the Influence of COVID-19 Among Dental Practitioners After Lockdown, Inq J Heal Care Organ Provision, Financ (2021) ;58: :004695802110607. |
[28] | Mahendran K , Patel S , Sproat C , Psychosocial effects of the COVID-19 pandemic on staff in a dental teaching hospital, Br Dent J (2020) ;229: (2):127–32. |
[29] | Plessas A , Paisi M , Baines R , Wheat H , Delgado MB , Mills I , et al., Frontline experiences and perceptions of Urgent Dental Care centre staff in England during the COVID-19 pandemic: a qualitative study. Br Dent J. 2021;1-10. |
[30] | Subhan R , Ismail WA , Musharraf S , Khan M , Hafeez R , Alam MK , Teledentistry as a Supportive Tool for Dentists in Pakistan. Biomed Res Int. 2021;2021. |
[31] | Cai H , Tu B , Ma J , Chen L , Fu L , Jiang Y , et al , Psychological impact and coping strategies of frontline medical staff in Hunan between January and March during the outbreak of coronavirus disease (COVID) in Hubei, China, Med Sci Monit (2020) ;26: :1–16. |
[32] | Almas K , Khan AS , Tabassum A , Nazir MA , Afaq A , Majeed A , Knowledge, Attitudes, and Clinical Practices of Dental Professionals during COVID-19 Pandemic in Pakistan, Eur J Dent (2020) ;14: :S63–9. |
[33] | Meng L , Hua F , Bian Z , Coronavirus Disease (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine, J Dent Res (2020) ;99: (5):481–7. |


