
Incidence of commuting accidents among non-physician staff in a large French university hospital centre from 2012 to 2016
Abstract
BACKGROUND:
Traffic road crashes are the leading cause of fatal crashes at work. The circumstances of work-related road accidents have been a regular focus of study, but there is still a lack of knowledge about commuting accidents.
OBJECTIVE:
The aims of this study were to estimate the overall incidence of commuting accidents for non-physician professionals in a major French university hospital, by gender and different professional categories, and to assess its evolution over a 5-year period.
METHODS:
A descriptive analysis was performed on 390 commuting accidents from 2012 to 2016 extracted from the university hospital’s occupational health service. Incidences of commuting accidents were calculated according to gender, occupational categories, and years. Crude relative risk (RR) for the association of commuting accidents with gender, occupational categories, and year of the accident was also estimated using log-binomial regressions.
RESULTS:
The annual incidence ranged from 354 to 581 accidents per 100,000 employees. Compared with administrative staff, the relative risk (RR) for commuting accidents for service agents was 1.6 (95% confidence interval (CI): 1.1–2.4) and for auxiliary nurses and childcare assistants was 1.3 (95% CI: 1.0–1.9). Nursing executives had a non-significantly lower RR of 0.6 (95% CI: 0.3–1.5).
CONCLUSION:
The increased risk observed for the auxiliary nurses and childcare assistants and for the service agents may be related in part to the fatigue caused by work schedules, long commuting distances, physical work, and psychological burden.
1Introduction
Traffic road crashes are the leading cause of fatal crashes at work, accounting for nearly 44% of work-related crash fatalities in France compensated by the French National Health Insurance Fund for Salaried Workers in 2012. Of these, 31% occurred while commuting from home to work [1]. The circumstances of work-related road accidents have been a regular focus of study [2–5], but there is still a lack of knowledge about commuting accidents. In France, commuting-related road crashes have increased by 1.5% from 2001 to 2016 [6]. Commuting road accidents are generally less serious than on-duty road accidents or private road accidents [7]. However, victims of work-related accidents were more often on sick leave and although the length of sick leave was higher for work-related accidents than for private accidents, in a multivariate analysis the type of road accident was not a significant factors to explain the time to return to work [8]. The French occupational accidents and diseases insurance fund (AT/MP) calculated that the part attributable of work accidents to commuting accidents represented almost 11% of the benefits paid by this insurance for workers [9]. In the French hospital sector, there were 2,226 commuting road crashes between home and work in 2015 that resulted in 68,431 days of sick leave, which is an average of 49.6 days per injured employee according to the national pension fund for local government employees [10]. This represents a significant social cost for the individual, the employer and society.
Road crashes are fortunately not very frequent, for example in the French Rhône department, the incidence rate of personal crash (all types of crashes and all degrees of severity) calculated from data from the Rhone Road Accident Victims Register averaged 437 per 100,000 inhabitants between 1996 and 2016. These data showed an over-representation of carers’ professions among victims of work-related road crashes [4]. At the national level, a 16.8% increase in work-related road crashes was also observed between 2001 and 2014 in the health sector [11].
The objective of this study was to estimate the incidence of commuting road crashes for all employees from the university hospital “Hospices Civils de Lyon”, excluding doctors for whom data were not available. This university hospital is the second largest university hospital in France and one of the largest employers in the Lyon region with some 23,000 employees, including 5000 physicians. In addition, we assessed the evolution over five years from 2012 to 2016 and calculated the incidence and its evolution by gender and for different professional categories.
2Materials and methods
2.1Study population and data on commuting road crashes
The dossiers for permanent and contract non-physician staff employed on 01 January each year from 2012 to 2016 were obtained from the hospital’s information technology department (Hospices Civils de Lyon). All commuting road crashes are recorded either during an occupational medicine consultation or by the medical service after reception of the medical certificate and the administrative declaration and this information is available to the occupational medicine physician. Using the occupational health software, Chimed©, data on commuting road crashes for all non-physician hospital workers recorded from 2012 to 2016 were extracted from the medical service file. All work accidents with sick leave are recorded. Work accidents without sick leave could be underreported, mostly for a commuting road crash.
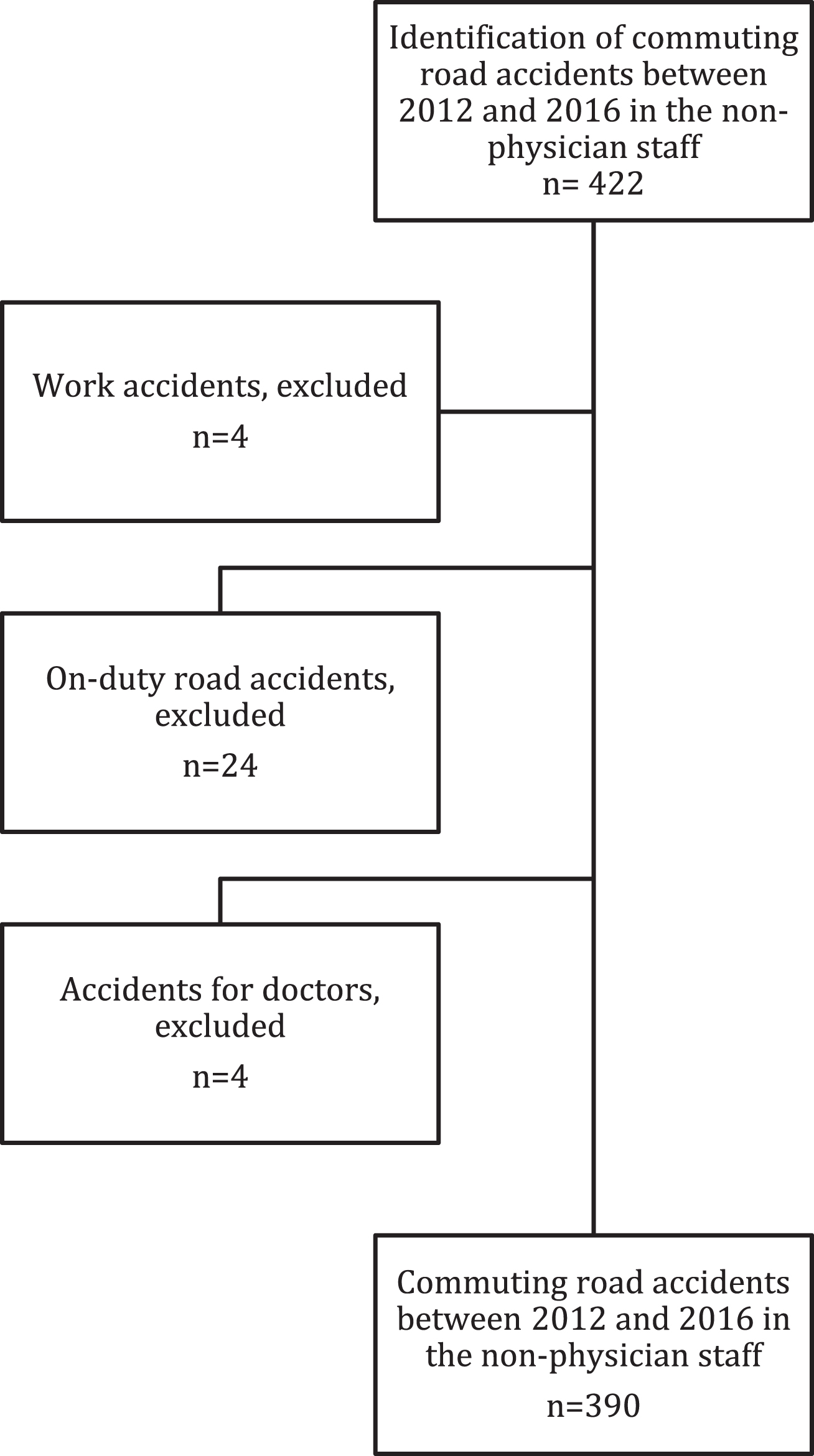
The commuting road crashes file had previously been reviewed to eliminate crash involving medical personnel, and to check that the code for a commuting road crash was correctly assigned (Fig. 1). A commuting road crash was classified as: without a vehicle, with a 4-wheel vehicle, with a 2-wheel vehicle (motorised or not), or pedestrian hit by a vehicle.
Fig. 1
Flowchart of the selection of the study population.
2.2Categories of non-medical staff
Employees in the commuting road crash file were divided into nine homogeneous groups based on occupational risk exposure:
• administrative staff
• service agents
• anaesthetist nurses, operating theatre nurses and midwives
• laboratory and pharmacy staff and their supervisors
• socio-educational, animators, dieticians, occupational therapists, physiotherapists, electro-radiology technicians and all paramedical staff in contact with patients, and their supervisors
• auxiliary nurses and childcare assistants
• nursing executives, specialized nursing executives, midwife managers
• nurses and childcare nurses
• technical staff
This same classification was used to determine the total numbers for each category per year.
2.3Statistical analyses
A descriptive analysis of the commuting road crashes between 2012 and 2016 was performed. Then, the incidence of commuting road crashes was calculated, according to gender, occupational categories and year. The evolution of the number of crashes over the years was assessed by the Cochran-Armitage Chi2 trend test. Finally, crude relative risk (RR) and Wald 95% confidence intervals for the association of commuting road crash with respective to gender, occupational categories and year were estimated on log-binomial regression [12] using the GENMOD procedure in the SAS statistical package (version 9.4) with the DIST = BINOMIAL and LINK = LOG options.
2.4Ethical considerations
The Chimed© file was registered in the National Commission for Data Protection and Liberties (CNIL-France) register under number 07-3. As the personal data contained in the occupational health software were accessible only by the occupational physician, the protocol was approved by the university hospital’s ethics committee and did not require approval by the committee for research involving human subjects. The study was reported on the clinicaltrials.gov registration system: number NCT04600908.
3Results
In this descriptive cross-sectional study, 390 commuting road crashes recorded between 2012 and 2016 for non-medical staff were analysed, for a total population of 17,737 on 1st January 2012 and 17,546 on 1st January 2016 (78% women). The average age of those who had commuting road crash was 41 years, and 78% (305/390) were women (Table 1). The majority of the crashes involved a 4-wheel vehicle (303/390, 78%), 63/390 (16%) involved a motorised or non-motorised 2-wheel vehicle, and 17/390 (4%) were pedestrians. Most of the victims (59%) had one crash during the study period, however, 7.2% had six or more crashes over the period (i.e., more than one crash per year) and 4 (1%) had 8 or 9 crashes. The crashes occurred mostly during the week (86%) with 75% occurring during the day.
Table 1
Description of population and commuting accidents
| n | % | ||
| Gender | Female | 305 | 78.2 |
| Male | 85 | 21.8 | |
| Marital status | Single | 84 | 21,5 |
| Married | 181 | 46,4 | |
| Other | 125 | 32,1 | |
| Professional categories | Administrative staff | 50 | 12.8 |
| Service agents | 44 | 11.3 | |
| Anaesthesia nurses, operating theatre nurses and midwives | 9 | 2.3 | |
| Laboratory or pharmacy staff and their supervision | 20 | 5.1 | |
| Socio-educators, animators, dieticians, occupational therapists, physiotherapists, electro-radiology technicians and all paramedics in contact with patients and their supervisors | 18 | 4.6 | |
| Auxiliary nurses and childcare assistants | 101 | 25.9 | |
| Nursing executives, specialized nursing executives, midwife coordinators | 5 | 1.3 | |
| Nurses and childcare nurses | 101 | 25.9 | |
| Technical staff | 42 | 10.8 | |
| Year of commuting accident | 2012 | 82 | 21.0 |
| 2013 | 75 | 19.2 | |
| 2014 | 69 | 17.7 | |
| 2015 | 62 | 15.9 | |
| 2016 | 102 | 26.2 | |
| Day of commuting accident | Monday | 63 | 16.2 |
| Tuesday | 72 | 18.5 | |
| Wednesday | 59 | 15.1 | |
| Thursday | 71 | 18.2 | |
| Friday | 70 | 17.9 | |
| Saturday | 25 | 6.4 | |
| Sunday | 30 | 7.7 | |
| Time of commuting accident | Day (7am–8pm) | 292 | 74.9 |
| Evening (20 h–24 h) | 67 | 17.2 | |
| Night (00 h–7 h) | 31 | 7.9 | |
| Mode of commuting accident | No vehicle involved | 7 | 1.8 |
| With 4-wheel vehicle | 303 | 77.7 | |
| As a pedestrian hit by a vehicle | 17 | 4.4 | |
| With a motorised or non-motorised 2-wheel vehicle | 63 | 16.1 | |
| Status of commuting accident | Declared | 109 | 27.9 |
| Declared with sick leave | 274 | 70.3 | |
| Received care from the medical service | 7 | 1.8 | |
| Number of accidents | 1 | 230 | 59.0 |
| 2 | 77 | 19.7 | |
| 3 | 29 | 7.4 | |
| 4 | 24 | 6.2 | |
| 6 and more | 30 | 7.7 |
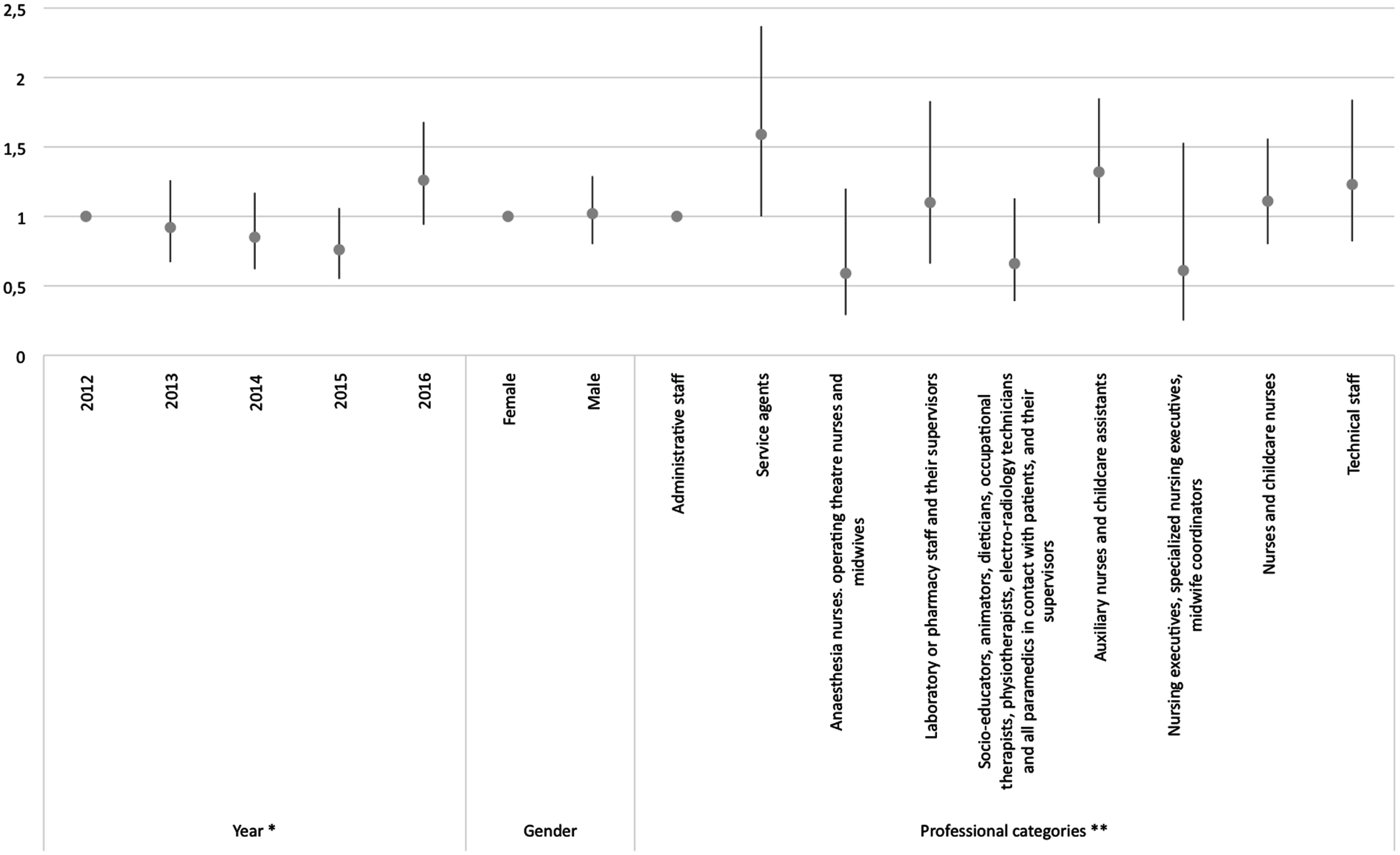
There was a significant decrease in the number of commuting road crashes in the first four years (p = 0.04) with an increase in the last year, although this trend was not significant over the five-year period (p = 0.3) (Table 2). The average annual incidence rate for the period was 443 crashes per 100,000 employees, with significant differences between genders (Fig. 2). For men there was an increased risk in 2016 compared with 2012 (RR = 3.7, 95% CI = 2.0–7.0) (Table 2). The commuting road crash risk for women was stable over the study period, except in 2016, when it increased slightly. The incidence rate varied by professional category, ranging from 156 crashes per 100,000 employees for anaesthetists, operating theatre nurses and midwives (RR = 0.6, 95% CI = 0.3–1.2) to 628 crashes per 100,000 employees for service agents (RR = 1.6, 95% CI = 1.1–2.4) with the administrative staff as a reference. Auxiliary nurses and childcare assistants also have an increased risk of crash (RR = 1.3, 95% CI = 1–1.9).
Table 2
Incidence rate of commuting accidents per 100,000 persons and relative risks by year, gender and occupational categories, from 2012 to 2016
| Incidence rate per | Relative risk | ||
| 100,000 persons | (95% CI) | ||
| (95% CI) | |||
| Year | 2012 | 462 (362–562) | 1 |
| 2013 | 425 (329–521) | 0.92 (0.67–1.26) | |
| 2014 | 393 (300–485) | 0.85 (0.62–1.17) | |
| 2015 | 354 (266–442) | 0.76 (0.55–1.06) | |
| 2016 | 581 (469–694) | 1.26 (0.94–1.68) | |
| Gender | Female | 441 (194–689) | 1 |
| Male | 449 (0–926) | 1.02 (0.8–1.29) | |
| Female | 2012 | 474 (359.6–588.3) | 1 |
| 2013 | 389.7 (285.8–493.7) | 0.82 (0.57–1.18) | |
| 2014 | 391.8 (287.3–496.2) | 0.83 (0.58–1.18) | |
| 2015 | 400 (294.3–505.7) | 0.84 (0.59–1.21) | |
| 2016 | 551.3 (427.4–675.3) | 1.16 (0.84–1.62) | |
| Male | 2012 | 419.7 (214.1–625.4) | 1 |
| 2013 | 552.8 (195.6–596.5) | 1.32 (0.69–2.52) | |
| 2014 | 396.1 (195.6–596.5) | 0.72 (0.35–1.45) | |
| 2015 | 184.8 (47.9–321.8) | 0.47 (0.19–1.13) | |
| 2016 | 691.3 (425.6–957) | 3.74 (2.01–6.96) | |
| Professional categories | Administrative staff | 395 (0–942) | 1 |
| Service agents | 628 (0–1555) | 1.59 (1.07–2.37) | |
| Anaesthesia nurses, operating theatre nurses and midwives | 156 (0–781) | 0.59 (0.29–1.2) | |
| Laboratory or pharmacy staff and their supervisors | 432 (0–138) | 1.1 (0.66–1.83) | |
| Socio-educators, animators, dieticians, occupational therapists, physiotherapists, electro-radiology technicians and all paramedics in contact with patients, and their supervisors | 248 (0–836) | 0.66 (0.39–1.13) | |
| Auxiliary nurses and childcare assistants | 522 (13–1032) | 1.32 (0.95–1.85) | |
| Nursing executives, specialized nursing executives, midwife coordinators | 243 (0–1306) | 0.61 (0.25–1.53) | |
| Nurses and childcare nurses | 457 (20–894) | 1.11 (0.80–1.56) | |
| Technical staff | 484 (0–1216) | 1.23 (0.82–1.84) |
Fig. 2
Crude relative risks and 95% confidence intervals of commuting accidents by year, gender and occupational category.
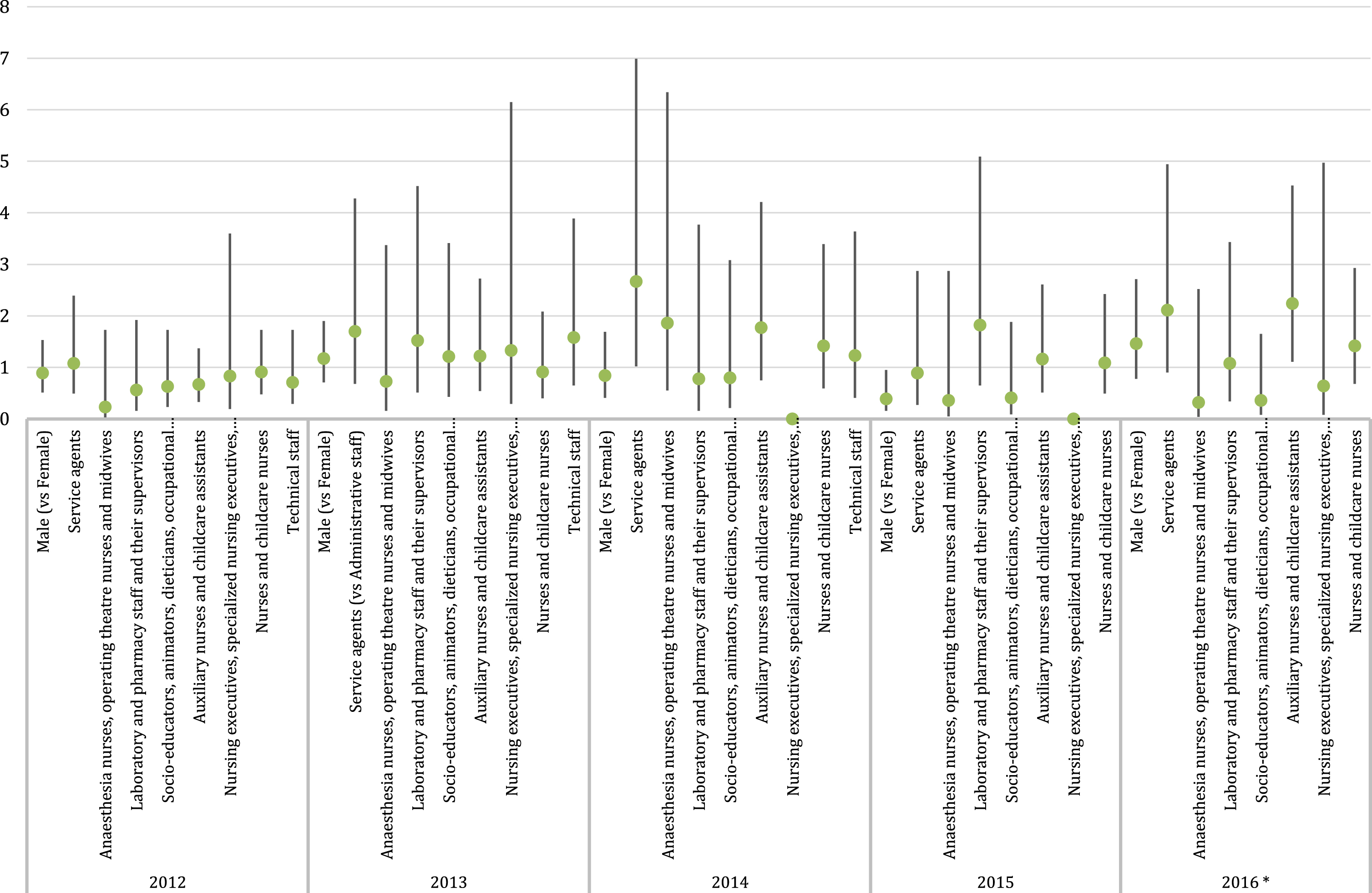
The risk of commuting road crash for service agents was highest in 2014 (RR = 2.7, 95% CI = 1.0–7.0), and in 2016 for auxiliary nurses and childcare assistants (RR = 2.2, 95% CI = 1.1–4.5) (Table 3 and Fig. 3).
Table 3
Incidence rate of commuting accidents per 100,000 employees and relative risks by gender and professional categories by year
| Year | ||||||
| 2012 | 2013 | 2014 | 2015 | 2016 | ||
| Female | Incidence rate (95% CI) | 474 (360–588) | 390 (285–494) | 392 (287–496) | 400 (294–506) | 551 (427–675) |
| Relative risk (95% CI) | 1 | 1 | 1 | 1 | 1 | |
| Male | Incidence rate (95% CI) | 420 (214–625) | 553 (316–789) | 396 (196–597) | 185 (48–322) | 691 (426–957) |
| Relative risk (95% CI) | 0.89 (0.51–1.53) | 1.17 (0.71–1.9) | 0.84 (0.41–1.69) | 0.39 (0.16–0.95) | 1.46 (0.78–2.71) | |
| Administrative staff | Incidence rate (95% CI) | 581 (287–875) | 360 (125–595) | 277 (72–482) | 357 (124–591) | 395 (150–639) |
| Relative risk (95% CI) | 1 | 1 | 1 | 1 | 1 | |
| Service agents | Incidence rate (95% CI) | 626 (238–1014) | 612 (212–1012) | 739 (281–1196) | 317 (06–627) | 831 (340–1322) |
| Relative risk (95% CI) | 1.08 (0.49–2.39 | 1.70 (0.68–4.28) | 2.67 (1.02–6.99) | 0.89 (0.27–2.87) | 2.11 (0.9–4.94) | |
| Anaesthesia nurses, operating theatre nurses and midwives | Incidence rate (95% CI) | 133 (0–395) | 262 (0–626) | 515 (10–1021) | 130 (0–385) | 127 (0–377) |
| Relative risk (95% CI) | 0.23 (0.03–1.73) | 0.73 (0.16–3.37) | 1.86 (0.55–6.34) | 0.36 (0.05–2.87) | 0.32 (0.04–2.52) | |
| Laboratory and pharmacy staff and their supervisors | Incidence rate (95% CI) | 324 (0–690) | 546 (67–1025) | 217 (0–518) | 649 (130–1169) | 426 (09–843) |
| Relative risk (95% CI) | 0.56 (0.16–1.92) | 1.52 (0.51–4.52) | 0.78 (0.16–3.77) | 1.82 (0.65–5.09) | 1.08 (0.34–3.43) | |
| Socio-educators, animators, dieticians, occupational therapists, physiotherapists, electro-radiology technicians and all paramedics in contact with patients, and their supervisors | Incidence rate (95% CI) | 367 (45–688) | 437 (87–787) | 221 (0–472) | 146 (0–347) | 143 (0–341) |
| Relative risk (95% CI) | 0.63 (0.23–1.73) | 1.21 (0.43–3.41) | 0.8 (0.21–3.08) | 0.41 (0.09–1.88) | 0.36 (0.08–1.65) | |
| Auxiliary nurses and childcare assistants | Incidence rate (95% CI) | 389 (192–585) | 437 (230–645) | 491 (270–712) | 413 (211–615) | 885 (587–1182) |
| Relative risk (95% CI) | 0.67 (0.33–1.37) | 1.22 (0.54–2.72) | 1.77 (0.75–4.21) | 1.16 (0.51–2.61) | 2.24 (1.11–4.53) | |
| Nursing executives, specialized nursing executives, midwife coordinators | Incidence rate (95% CI) | 480 (0–1144) | 480 (0–1144) | 0 (0–0) | 0 (0–0) | 252 (0–746) |
| Relative risk (95% CI) | 0.83 (0.19–3.6) | 1.33 (0.29–6.15) | – | – | 0.64 (0.08–4.97) | |
| Nurses and childcare nurses | Incidence rate (95% CI) | 529 (317–741) | 328 (162–494) | 393 (211–574) | 389 (209–569) | 559 (344–774) |
| Relative risk (95% CI) | 0.91 (0.48–1.73) | 0.91 (0.4–2.08) | 1.42 (0.59–3.39) | 1.09 (0.49–2.42) | 1.42 (0.68–2.93) | |
| Technical staff | Incidence rate (95% CI) | 411 (106–715) | 570 (217–923) | 339 (68–611) | 338 (68–608) | 776 (354–1198) |
| Relative risk (95% CI) | 0.71 (0.29–1.73) | 1.58 (0.65–3.89) | 1.23 (0.41–3.64) | 0.95 (0.34–2.65) | 1.97 (0.86–4.47) | |
Fig. 3
Crude relative risks and 95% confidence intervals of commuting accidents by gender and occupational category per year.
4Discussion
The annual incidence of commuting road crashes per 100,000 employees in our university hospital ranged from 354 to 581, with no significant trend over the five-year study period. In the region where the hospital is situated, the average annual incidence of all severity commuting road crash for working-aged individuals (16 to 65 years old) who received care in a public or private hospital during the period 2012 to 2016 was 127 per 100,000, which is three times lower than the average incidence observed in this present paper [13]. The majority of commuting road crashes occurred during the day between 7am and 8pm (74.9%), a trend also found observed in the hospital sector on a national level [10].
Although we did not observed any significant excess risk of commuting road crash by gender in our population, the rate has been reported to be higher for men in other countries, such as Spain or Australia [14, 15]. According to the Rhône Register of Road Traffic Accident Victims, men are more likely to use two-wheelers, a mode of transport more likely to cause crash, a finding also found at the national level [13]. In our population, 16.1% of the commuting road crashes involved a 2-wheel vehicle compared with 77.7% that involved a 4-wheel vehicle, again similar to that found in the Rhône register [13], at a national level for fatal commuting road crash and in Australia [14, 16].
We observed a higher risk of commuting road crashes for 2016 compared with 2012 (RR = 1.3, 95% CI = 0.9–1.7). This is partly due to the higher risk for auxiliary nurses and childcare assistants (RR = 2.2, 95% CI = 1.1–4.5) but also the three times higher risk for males in 2016 compared with 2012 (RR = 3.7, 95% CI = 2–7). There was a 1.2% increase in the rate of commuting road crash in the general population at the national level between 2015 and 2016 and a higher frequency index was also reported for the Rhône Alpes region in 2016 [13]. An increasing frequency index was also reported for the hospital sector at the national level [10].
Over the 5-year study period the RR of commuting road crash for service agents was 1.6 (95% CI = 1.1–2.4) with the highest RR of 2.7 (95% CI = 1.0–7.0) observed in 2014. This increased risk could be due to the particularly high physical constraints and the resulting fatigue caused by this work. Several studies have reported a potential association between road crash and fatigue, lack of sleep, high mental workload at work and work rhythms [17–22]. It is thought that these factors could also explain the excess risk for commuting road crashes observed among nurses in the United States [23–25]. The risk for traffic road crash was reported to be ten times higher at night than during the day, after adjusting for traffic intensity [26]. A quarter of the accidents took place in the evening or at night in our study. In Spain, self-perceived risk as well as accident incidence was higher amongst those in nursing professions [27]. A report published by the French Agency for Food, Environmental and Occupational Health & Safety (ANSES) in 2016 suggested that atypical working hours can lead to more frequent and more severe crashes, with a two-fold increase in the risk of commuting road crash and ‘near accidents’ due to the sleep disorders caused by the atypical working hours [28]. Recently, commuting crashes’ features were found to be associated with demographic and job-related variables of professional drivers in Spain [29].
In France, atypical work rhythms are defined as alternating work in shifts of 2×8 hours (either a morning shift from 6 am to 2 pm or an afternoon shift from 2 pm to 10 pm), with the night shift comprising 10 hours of work. The 2×12 hours shift schedule consists of a maximum of 12 hours per work day, followed by a daily rest period of at least 12 consecutive hours and a weekly rest period of at least 36 consecutive hours. Employees may not work more than three consecutive 12-hour day shifts.
One review published in 1997 suggested that there was a clear circadian rhythm in road crash risk, while a more recent review published in 2011 concluded that while there appeared to be good evidence for circadian influences and the risk of road crash, the peak occurred earlier than would be expected, suggesting confounding from other factors, such as time since waking [30, 31]. However, exposure to risk such as distance from home to work could explain this higher risk for service agents, with a place of residence possibly more distant than others and therefore a higher risk of crash. This is supported by a more recent study that found that primary care professionals who travel more than 30 km per day had a higher accident incidence [27].
We found that 41% of the workers had several road accidents in the studied period. History of accidents is a well-described risk factor [32]. A study of minibus drivers showed that those involved in a second accident shortly after a first had an elevated risk of a third accident [33]. This “accident proneness” [34] is found in road accidents as well as in work accidents in general. In on-duty accidents, however, occupational factors may also be involved [18, 35]. Driving behaviours could explain this history of accidents in a short lap of time.
Our study was carried out in the second largest hospital group in France over a 5-year period. To date, few studies have focused on non-physician healthcare personnel with this detailed level of description. We cannot exclude a possible bias from underreporting of commuting road crashes for the non-physician staff.
Our study included commuting road crash victims who declared their crash to the occupational medicine service. Many of the crash did not require hospital care and were, therefore, probably of low severity, which could partly explain the higher rate observed in this paper compared with the rate in the general population from the Rhône Register. Conversely, the fact that we included crashes with no vehicle involved in our analyses does not explain the higher rate observed, since these crash concern only seven people (less than 2% of all crashes).
5Conclusion
A significantly higher risk of commuting road crashes was observed for service agents and, to a lesser extent, for auxiliary nurses and childcare assistants, compared with administrative employees, which could be due to professional factors such as atypical schedules. Hospitals are changing working patterns; for example, introducing 12-hour shifts, to replace 8-hour ones, to enable 24 h cover while reducing costs. It is important to know whether this contributes to an increased risk of crash [36]. A nested case-control study in the cohort, considering account risk exposure, could help to clarify the influence of these schedules (alternating and night). In addition, the identification of professional categories most at risk would improve the targeting of road crash prevention campaigns in the population. This study allowed us to examine the effects of changes in work rhythm. Will the generalization of the 12-hour shifts both increase the fatigue for workers and road commuting accidents? It will be important in the future to improve the research and knowledge about commuting accidents with these new changes in work rhythms in industrialized countries.
Acknowledgments
The authors would like to thank the IT department at the University Hospital Centre. They also acknowledge translation and editorial services provided by Margaret Haugh, MediCom Consult, Villeurbanne, France.
Conflict of interest
None to report.
References
[1] | French Health Insurance - Occupationnal risks. [Business report - 2012] [Internet]. 2013. Available from: http://www.risquesprofessionnels.ameli.fr/fileadmin/user_upload/document_PDF_a_telecharger/brochures/Rapport_gestion_2012.pdf. |
[2] | Johnston T , Kristman V , Brison R . Descriptive analysis of work and non-work related motor vehicle collisions in Kingston, Ontario. Work. (2012) ;43: :115–21. |
[3] | Thygerson S , Merrill R , Cook L , Thomas A . Comparison of factors influencing emergency department visits and hospitalization among drivers in work and nonwork-related motor vehicle crashes in Utah, 1999-2005. Accid Anal Prev. (2011) ;43: :209–13. |
[4] | Hours M , Fort E , Charbotel B , Chiron M . Jobs at risk of work-related road crashes: An analysis of the casualties from the Rhône Road Trauma Registry (France). Saf Sci. (2011) ;49: (8-9):1270–6. |
[5] | Fort E , Pélissier C , Fanjas A , Charnay P , Charbotel B , Bergeret A , et al. Road casualties in work-related and private contexts: Occupational medical impact. Results from the ESPARR cohort. Work. (2018) ;60: (1). |
[6] | French Health Insurance - Occupationnal risks. [Annual report - 2017] [Internet]. 2018. Available from: https://assurance-maladie.ameli.fr/sites/default/files/2018-12_rapport-annuel-2017–risques-professionnels_assurance-maladie.pdf. |
[7] | Charbotel B , Chiron M , Martin JL , Bergeret A . Work-related road accidents in France. Eur J Epidemiol. (2001) ;17: :773–8. |
[8] | Fort E , Bouffard E , Charnay P , Bernard M , Boisson D , Laumon B , et al. Return to work following road accidents: Factors associated with late work resumption. J Rehabil Med. (2011) ;43: (4):283–91. |
[9] | French Health Insurance - Occupationnal risks. [Annual report - 2016] [Internet]. 2017. Available from: https://www.ameli.fr/sites/default/files/ra-risques-professionnels-2016_assurance-maladie.pdf. |
[10] | National pension fund for local government employees. [2017 Hospital sector statistical report] [Internet]. 2018. Available from: https://www.cnracl.retraites.fr/sites/default/files/celine.thenieres/rapport~Hospitalier~2017.pdf. |
[11] | French Health Insurance. [Commuting accidents] [Internet]. 2015. Available from: https://www.securite-sociale.fr/files/live/sites/SSFR/files/medias/CCSS/2015/FICHE_ECLAIRAGE/CCSS-FICHE_ECLAIRAGE-2015–LES_ACCIDENTS_DE_TRAJET.pdf. |
[12] | Wacholder S . Binomial regression in GLIM: estimating risk ratios and risk differences. Am J Epidemiol [Internet]. 1986 [cited 2021 Sep 14]; 123: (1):174–84. Available from: https://pubmed.ncbi.nlm.nih.gov/3509965/. |
[13] | [The Rhône Registry of road traffic accident victims - Activity report - 2017] [Internet]. 2018. Available from: http://www.revarrhone.org/wp-content/uploads/2018/04/RegistreRapActiv2017_2.pdf. |
[14] | Boufous S , Williamsom A . Work-related traffic crashes: A record linkage study. Accid Anal Prev [Internet]. (2006) ;38: :14–21. Available from: http://www.sciencedirect.com/science?_ob=MImg&_imagekey=B6V5S-4GPW3MK-2-8&_cdi=5794&_user=1697204&_orig=search&_coverDate=01%2F31%2F2006&_sk=999619998&view=c&wchp=dGLbVzW-zSkzk&md5=bb5873975cd19a7f772a784274cbafec&ie=/sdarticle.pdf LB - Manu 105. |
[15] | López-Ruiz M , Martínez JM , Pérez K , Novoa AM , Tobías A , Benavides FG . Impact of road safety interventions on traffic-related occupational injuries in Spain, 2004-2010. Accid Anal Prev [Internet]. (2014) ;66: :114–9. Available from: http://www.sciencedirect.com.docelec.univ-lyon1.fr/science/article/pii/S0001457514000165. |
[16] | Mitchell R , Driscoll T , Healey S . Work-related road fatalities in Australia. Accid Anal Prev [Internet]. (2004) ;36: :851–60. Available from: https://doi.org/10.1016/j.aap.2003.06.002. |
[17] | Philip P , Vervialle F , Le Breton P , Taillard J , Horne JA . Fatigue, alcohol, and serious road crashes in France: factorial study of national data. Br Med J. (2001) ;322: :829–30. |
[18] | Chiron M , Bernard M , Lafont S , Lagarde E . Tiring job and work related injury road crashes in the GAZEL cohort. Accid Anal Prev [Internet]. (2008) ;40: :1096–104. Available from: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=18460378. |
[19] | Di Milia L , Rogers NL , Åkerstedt T . Sleepiness, Long Distance Commuting and Night Work as Predictors of Driving Performance. PLoS One [Internet]. (2012) ;7: :e60045. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3448712/pdf/pone.0045856.pdf. |
[20] | Swanson L , Drake C , Arnedt J . Employment and drowsy driving: a survey of American workers. Behav Sleep Med [Internet]. 2012 Oct [cited 2021 Sep 14]; 10: (4):250–7. Available from: https://pubmed.ncbi.nlm.nih.gov/22946734/. |
[21] | Fort E , Ndagire S , Gadegbeku B , Hours M , Charbotel B . Working conditions and occupational risk exposure in employees driving for work. Accid Anal Prev [Internet]. (2016) ;89: :118–27. Available from: http://www.sciencedirect.com.docelec.univ-lyon1.fr/science/article/pii/S0001457516300227. |
[22] | Kalsi J , Tervo T , Bachour A , Partinen M . Sleep versus non-sleep-related fatal road accidents. Sleep Med [Internet]. 2018 Nov 1 [cited 2021 Sep 14]; 51: :148–52. Available from: https://pubmed.ncbi.nlm.nih.gov/30179735/. |
[23] | Lockley SW , Barger LK , Ayas NT , Rothschild JM , Czeiler CA , Landrigan CP , et al. Effects of health care provider work hours and sleep deprivation on safety and performance. Jt Comm J Qual patient Saf. (2007) ;33: :7–18. |
[24] | Scott LD , Hwang WT , Rogers AE , Nysse T , Dean GE , Dinges DF . The relationship between nurse work schedules, sleep duration, and drowsy driving. Sleep [Internet]. (2007) ;30: :1801–7. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2276124/pdf/aasm.30.12.1801.pdf. |
[25] | Gold D , Rogacz S , Bock N , Tosteson T , Baum T , Speizer F , et al. Rotating shift work, sleep, and accidents related to sleepiness in hospital nurses. Am J Public Health [Internet]. 1992 [cited 2021 Sep 14]; 82: (7):1011–4. Available from: https://pubmed.ncbi.nlm.nih.gov/1609900/. |
[26] | Langlois P , Smolensky M , Hsi B , Weir F . Temporal patterns of reported single-vehicle car and truck accidents in Texas, U.S.A. during 1980-1983. Chronobiol Int [Internet]. 1985 [cited 2021 Sep 14]; 2: (2):131–40. Available from: https://pubmed.ncbi.nlm.nih.gov/3870843/. |
[27] | Díez-Juárez M , Naviero-Rilo J , Pérez-La Orden A . [Road safety in work commuting for primary care profesionals]. Semergen [Internet]. 2013 Apr [cited 2021 Sep 15]; 39: (3):130–8. Available from: https://pubmed.ncbi.nlm.nih.gov/23540985/. |
[28] | Avis de l’Anses - Rapport d’expertise collective. [Assessment of health risks related to night work] [Internet]. 2016. Available from: https://www.anses.fr/fr/system/files/AP2011SA0088Ra.pdf. |
[29] | Llamazares J , Useche S , Montoro L , Alonso F . Commuting accidents of Spanish professional drivers: when occupational risk exceeds the workplace. Int J Occup Saf Ergon [Internet]. 2021 [cited 2021 Sep 15]; 27: (3):754–62. Available from: https://pubmed.ncbi.nlm.nih.gov/31132927/. |
[30] | Folkard S . Black times: temporal determinants of transport safety. Accid Anal Prev [Internet]. 1997 [cited 2021 Sep 14]; 29: (4):417–30. Available from: https://pubmed.ncbi.nlm.nih.gov/9248500/. |
[31] | Williamson A , Lombardi D , Folkard S , Stutts J , Courtney T , Connor J . The link between fatigue and safety. Accid Anal Prev [Internet]. 2011 Mar [cited 2021 Sep 14]; 43: (2):498–515. Available from: https://pubmed.ncbi.nlm.nih.gov/21130213/. |
[32] | Meuser TM , Carr DB , Ulfarsson GF . Motor-vehicle crash history and licensing outcomes for older drivers reported as medically impaired in Missouri. Accid Anal Prev [Internet]. (2009) ;41: :246–52. Available from: http://www.sciencedirect.com/science?_ob=MImg&_imagekey=B6V5S-4V7658M-1-9&_cdi=5794&_user=1697204&_pii=S0001457508002224&_orig=search&_coverDate=03%2F31%2F2009&_sk=999589997&view=c&wchp=dGLbVlz-zSkWA&md5=d52b68810e6c9433da65833fd063381f&ie=/sdarticle.pdf |
[33] | Hamed MM , Jaradat AS , Easa SM . Analysis of commercial mini-bus accidents, Accid Anal Prev [Internet]. (1998) ;30: :555–67. Available from: http://www.sciencedirect.com/science?_ob=MImg&_imagekey=B6V5S-3V728G9-1-P&_cdi=5794&_user=1697204&_pii=S0001457598000219&_orig=search&_coverDate=09%2F30%2F1998&_sk=999699994&view=c&wchp=dGLbVtb-zSkWb&md5=dc1580b74ec4359c7fea88583ba7f1df&ie=/sdarticle.pdf |
[34] | Visser E , Pijl YJ , Stolk RP , Neeleman J , Rosmalen JGM . Accident proneness, does it exist? A review and meta-analysis, Accid Anal Prev [Internet]. (2007) ;39: :556–64. Available from: http://www.sciencedirect.com/science?_ob=MImg&_imagekey=B6V5S-4MBC002-2-1&_cdi=5794&_user=1697204&_pii=S0001457506001746&_orig=search&_coverDate=05%2F31%2F2007&_sk=999609996&view=c&wchp=dGLzVzz-zSkzS&md5=d3c3bfccfd038a28e9eceef0f94a2fa6&ie=/sdarticle.pdf |
[35] | Fort E , Pourcel L , Davezies P , Renaux C , Chiron M , Charbotel B . Road accidents, an occupational risk. Safety Sciences. (2010) ;48: (10):1412–20. |
[36] | Ledoyen JR , Waelli M . [12 hours, time to count...] [Internet]. 2015. Available from: https://documentation.ehesp.fr/memoires/2015/mip/groupe~32.pdf |


