
Labor of love, or love of labor? Psychological capital’s mitigating role in the relationship between workaholism and work stress
Abstract
BACKGROUND:
Workaholism is conceptualized as a compulsive need to work incessantly, and it is related to numerous detrimental organizational and individual consequences. For that reason, it is imperative that researchers uncover possible variables that can alleviate its potentially harmful effects.
OBJECTIVE:
This study aims to examine the relationship between workaholism, psychological capital (PsyCap), physical health, and work stress. The potential mitigating role that PsyCap could play between workaholism and physical health, as well as work stress, was also examined.
METHODS:
Data on workaholism, PsyCap, physical health, and work stress were collected from 343 full-time faculty and staff from a large Southeastern university.
RESULTS:
Results showed workaholism negatively related to physical health and positively related to work stress. Additionally, PsyCap had a positive relationship with physical health and a negative relationship with work stress. Moreover, PsyCap moderated the relationship between workaholism and work stress, such that as PsyCap increased, the relationship between workaholism and work stress weakened.
CONCLUSIONS:
PsyCap may be a fairly simple and cost-effective intervention for organizations to implement, as it can be learned through short training sessions. By incorporating PsyCap, organizations may be able to help mitigate levels of stress in their employees, specifically among those who suffer from workaholism.
1Introduction
According to the American Psychological Association [1], 70% of survey respondents noted work was either somewhat or a significant source of stress. A British survey found 57% of work-day loss could be attributed to work stress, anxiety, and depression [2]. Evidently, work stress has negative implications for both the employee and the organization, thus, researchers are interested in studying how it arises among employees. A common antecedent (and correlate) of work stress is workaholism. Originally, workaholism was deemed an addiction to work, with a compulsive need to work incessantly [3]. Consensus among the literature indicates it is the compulsive need to work excessively hard [4]. Research has found workaholism to be linked to many adverse outcomes, including poor overall health [5], as well as work-stress, work-life conflict, and burnout [4]. Although correlates of workaholism (and subsequent outcomes) have been widely studied, there is a dearth in the research literature regarding potential variables that could mitigate these relationships.
In the current study, we wanted to identify a construct (i.e., psychological capital; PsyCap) that might subdue the negative association between workaholism and employee health and stress. PsyCap is comprised of four positive psychological resources—hope, efficacy, resilience, and optimism [6]. It draws from the field of positive psychology, or the study of positive human functioning. There is substantial research to support that PsyCap has a positive influence on one’s well-being [7, 8] and quality of work life [9]. Essentially, integrating it into the workplace can have positive implications for employees. Given that PsyCap is state-like in nature, it can change over time and can even be learned through training [6].
We examined the relationships among workaholism, physical health, and work stress, while considering PsyCap as a potential moderator. Workaholism is negatively correlated with several components of well-being including work stress [10], overall physical health [5], and psychological ailments such as burnout and depression [11]. Conversely, PsyCap is largely correlated with desirable work attitudes and behaviors including satisfaction, commitment, and psychological well-being [12]. Furthermore, it is positively correlated with overall well-being [7]. Thus, investigating PsyCap in relation to workaholism would strongly contribute to the current literature by identifying a valuable, moderating construct that targets unhealthy work behaviors.
Research, though scarce, supports PsyCap as a moderator. For example, PsyCap moderated the relationship between surface acting and emotional exhaustion, as well as between deep acting and depersonalization, in a sample of 416 working professionals [13]. This finding illustrates both the mitigating role PsyCap can play, as well as the positive implications it has for well-being. The current study aims to address the gap in the extant literature directly examining PsyCap as a moderator between workaholism and physical health, as well as overall work stress. With employees working increasingly longer hours, and employers expecting more of their labor force, workers are put at a higher risk for work stress, burnout, and other negative effects [4]. The results of the current study provide research that better informs organizations on ways to reduce work stress and physical ailments stemming from workaholism.
1.1Workaholism overview
The definition of workaholism has evolved over time. For instance, Spence and Robbins [14] identified three different dimensions of workaholism: high work involvement, high work drive, and low work enjoyment. More recently, results of a meta-analysis posited workaholism is comprised of behaviors that result from an internal drive to work, as well as issues with disconnecting from work and surpassing the expected requirements in one’s work role [4]. Based on the vast literature, workaholism is the culmination of both excessive and compulsive work driven by internal motivations, whereby the employee does not enjoy their work and experiences work-life imbalance [15–17]. Thus, in the current study, workaholism was conceptualized as a compulsive need to work excessively.
Workaholism is related to personality traits such as perfectionism and Type A personality [4] as well as low self-esteem [13]. Workaholics, especially females, are more likely to experience negative affect [18, 19] and anxiety [19, 20]. Workaholism is also positively associated with job demands, role conflict, and job control, and negatively related to role clarity [21]. Notably, it is driven by an intrinsic desire to work, rather than extrinsic factors such as financial needs [4]. Workaholism is positively linked to work stress, work-life imbalance, and decreased life satisfaction [4] as well as burnout and depression [11]. It is also comorbid with psychiatric disorders such as obsessive-compulsive disorder and attention deficit hyperactivity disorder [22].
Workaholism is also related to poor overall health [5]. For example, workaholics experience higher systolic blood pressure compared to non-workaholics [18]. Aziz et al. [23] found a link between workaholism and a family history of metabolic diseases, such as hypercholesterolemia and heart disease. This research indicates workaholism and such diseases could share common causes (i.e., genetic or environmental factors). Finally, workaholism can lead to sleep problems, which can result in additional mental and physical ailments [24] such as cardiovascular problems [25].
1.2Psychological capital overview
PsyCap was conceptualized after the emergence of positive organizational behavior, which aims to examine strengths and capacities related to performance [26]. Luthans et al. [27] aimed to measure positive psychological factors that would precede positive work outcomes. Thus, PsyCap is comprised of hope, efficacy, resilience, and optimism [12]. Hope is one’s goal-directed energy and the methods one chooses to pursue those goals [28]. Efficacy is one’s ability to adequately perform based on intrinsic motivation and cognitive abilities [29]. According to Southwick et al. [30] resilience encompasses social, psychological, and biological factors which determine how one responds to stressful experiences. Finally, optimism reflects how much a person anticipates positive events to occur [31].
PsyCap is correlated with many positive occupational outcomes, including attitudes of satisfaction, commitment, job performance, and psychological well-being [12]. In recent research, PsyCap predicted several positive outcomes in the workplace, including work engagement [32] and autonomous motivation [33]. Additionally, PsyCap predicted commitment and job satisfaction in a Turkish study of 260 aircraft mechanics [34].
Due to its positive correlates, PsyCap has been studied as a moderator in relationships that examine employee metrics. For example, in a sample of U.S. employees, Probst et al. [35] found PsyCap attenuated the relationship between job insecurity and job performance. Additionally, PsyCap influences perceptions of harsh job demands, such that those high in PsyCap have more positive outlooks about their occupations [36]. Aziz and colleagues [13] found PsyCap moderated the relationship between types of emotional labor (i.e., surface acting and deep acting) and facets of burnout (e.g., depersonalization and emotional exhaustion). Furthermore, PsyCap mitigates the relationship between work stress and workplace incivility [37]. Hence, the existing literature demonstrates that PsyCap has great potential to attenuate the relationship between work stress and a multitude of negative outcomes.
1.3Physical health overview
While physical health is a broad concept that encompasses many factors, Capio et al. [38, p. 4805] define it as “ ... the ability to perform physical activities and carry out social roles that are not hindered by physical limitations and experiences of bodily pain, and biological health indicators.” When examining physical health in psychological research, researchers often use one or more of the following variables in their definition: sleep [39, 49], chronic health conditions, [41] viruses, [42] and immune system complications [43]. In the current study, physical health is conceptualized as a state of physical well-being with regard to digestive and respiratory health, as well as the absence of headaches and sleep problems.
Excessive work negatively influences one’s physical health, which can in turn affect one’s ability to work. For example, employees who do not get enough sleep experience lower levels of job performance, productivity, and safety behaviors at work compared to those with a normal amount of sleep [39]. Additionally, employees with chronic physical health conditions face significantly more problems with work abilities and work production compared to those without such conditions [41].
Stress influences the progression of diseases of the immune system given that disease occurs due to a compromised host function [44]. For example, stress can affect the onset and the progression of autoimmune diseases such as rheumatoid arthritis [43] and cancer [45]. Additionally, in a trial of 420 adults, Cohen and colleagues [41] found perceived stress and negative affect significantly predicted the probability of developing a cold. Work stress is also a risk factor for poor overall health [40]. Based on these findings, it is in the organization’s best interest to invest in the physical well-being of its employees by combatting components of work stress.
1.4Work stress overview
The physical and mental strain individuals feel as a product of their job demands not aligning with their available resources, is called work stress [46]. Work stress is a multifaceted symptom of work with varying precursors and outcomes, thus, there are various ways in which one’s work can lead to stress. Ganster and Perrewé [47] outline the job demands-control (JD-C) theory in which the individual has an unfavorable relationship between their job’s demands or required tasks and their perceived locus of control (i.e., internal or external). Additionally, the job demands-resources (JD-R) model of work stress posits employees may not have adequate mental and physical resources to complete their job demands which, in turn, causes them stress [48]. Finally, the conservation of resources (COR) theory puts forth that stress stems from perceived or actual loss of resources such as objects, energy, or other conditions valued by the individual [47]. Accordingly, the current study hypotheses that pertain to work stress have different theoretical underpinnings.
Work stress has positive relationships with a multitude of negative variables. For example, it has been linked to many physical health problems including hypertension and diabetes, [49] as well as sleep problems [50]. Work stress also has an unfavorable impact on one’s mental health—it is linked to anxiety and depression, [50] major depressive episodes, [51] and burnout [46]. Additionally, work stress is negatively related to overall job performance, [7] absenteeism, [52] and turnover intention [53], thus, organizations should invest in the psychological health and well-being of their employees.
2Current study
The primary goal of the current study is to examine the relationships between workaholism, physical health, work stress, and PsyCap. Additionally, it is proposed that PsyCap will moderate the relationship between workaholism and physical health, in addition to work stress, such that greater levels of PsyCap will weaken the association between workaholism and these variables. Given that workaholism affects an estimated 10% of all U.S. workers, [54] it is imperative for us to develop novel ways to abate its outcomes and contribute to future interventions. In addition to the mental and physical toll they take on employees, work stress and diminished physical health also cost organizations millions of dollars, mostly due to reduced productivity [55]. If PsyCap moderates the relationship between workaholism and the aforementioned variables, then employers can begin to promote it in the workplace in an effort to build a happier, healthier, and more productive workforce.
Workaholism is associated with negative health outcomes, such as increased blood pressure and elevated cholesterol [56, 57]. A link has been found between workaholism and cardiovascular problems, particularly when the individual exhibits Type A personality traits [58]. Moreover, in a Spanish study consisting of 537 hospital employees, workaholism was related to sleep problems which, in turn, mediated the relationship between workaholism and cardiovascular risk [25]. The relationship between workaholism and poor health could be due in part to the fact that workaholics have less time to recover from their exorbitant efforts, or engage in non-work activities, including sleep [5]. Research supports the negative influence workaholism can have on overall health, thus, the following hypothesis is proposed:
Hypothesis 1a (H1a): Workaholism will be negatively related to physical health.
Relationships between workaholism and increased perceived work stress have long been studied [4, 24, 59]. Findings indicate workaholic tendencies are positively associated with work stress based on both the demanding work environment, as well as the workaholic’s drive to work excessively [13]. The demands of one’s job could become overwhelming, especially considering that workaholics do not delegate and would rather take on tasks themselves than distribute them among coworkers, [14] thereby leading to work stress. This notion is based on the JD-C theory of work stress, whereby individuals believe they do not have appropriate control over a given task in terms of how or when it is completed [60]. In turn, this could lead to workaholics taking on more work than they can realistically complete. If they are unable to complete their tasks, it could exacerbate feelings of guilt and other negative emotions that workaholics typically experience regarding their work life. Based on the nature of workaholism and the stress stemming from both working and not working, the following hypothesis is posited:
Hypothesis 1b (H1b): Workaholism will be positively related to work stress.
Luthans et al. [61] found PsyCap was positively associated with satisfaction with one’s health. Hope influences physical health, especially when acting as a buffer between illness and stress or depression [62]. Additionally, resilience and optimism have a positive relationship with physical health [63, 64]. Aspinwall and Tedeschi [65] highlight that positive psychology (e.g., optimism) can lead to behavioral patterns that are considered preventative health measures, including coping and attention to one’s health. It is quite promising that components of PsyCap serve as buffers for physical health, hence, the following hypothesis is expected:
Hypothesis 2a (H2a): PsyCap will be positively related to physical health.
According to the JD-R model, work stress is often a result of perceived insufficiency of resources to accomplish overwhelming job demands [48]. The four components of PsyCap are examples of positive psychological resources. The development of PsyCap may increase the amount of positive psychological resources within an individual, thus, strengthening one’s ability to adhere to job demands and, in turn, diminish the influence of the JD-R model of work stress. Other studies have similarly found results supporting the negative relationship between PsyCap and work stress [29, 66]. Having PsyCap as a resource may act as a buffer between the perception of resources and the resulting work stress. Therefore, the following hypothesis is proposed:
Hypothesis 2b (H2b): PsyCap will be negatively related to work stress.
Workaholics have reported engaging in many unhealthy behaviors such as excessive alcohol, caffeine, and tobacco consumption, as well as overeating [67]. There is also a relationship between workaholism and inadequate sleep [24]. These behaviors and patterns put workaholics at a greater risk for physical health complications. Additionally, immunosuppression could partially explain the link between forms of work stress (e.g., workaholism and its correlates) and impaired physical health [44]. In these instances, stress expends energy that the body would otherwise utilize for basic functioning. This model is representative of the stress response theory [68] in which endocrinological responses can aid survival, but in excess can lead to diseases of adaptation (e.g., high blood pressure, heart disease). If one adopts the components of PsyCap into their cognitions, then the body may expend less energy on stress and, in turn, respond to immunological threats. Accordingly, the following hypothesis is posited:
Hypothesis 3a (H3a): PsyCap will moderate the relationship between workaholism and physical health, such that the higher the level of PsyCap, the weaker the relationship between workaholism and physical health.
Given that work is all-consuming for workaholics, it is no surprise there is a positive correlation between workaholism and work stress. Due to the constant rumination about work, and feelings of guilt when away from work, the workaholic has little to no time to recuperate after the work day. The workaholic expends lots of energy and mental resources on negative thoughts, while leaving little time for leisurely activities. Fortunately, studies have indicated employees higher in PsyCap experience less work stress than those lower in PsyCap [12]. This finding could be due in part to the potentially mitigating influence of PsyCap illustrated by previous research [13, 69]. Based on the JD-R model of work stress, stress is the result of a lack of resources [60]. According to the COR theory, individuals do not want to lose resources and seek to gain them in the future. PsyCap could potentially serve as a positive resource that allows one to recover after the work day. Thus, the following hypothesis is expected:
Hypothesis 3b (H3b): PsyCap will moderate the relationship between workaholism and work stress, such that the higher the level of PsyCap, the weaker the relationship between workaholism and work stress.
3Materials and methods
3.1Participants
Participants (N = 343) were recruited from a large Southeastern university and were eligible for the study if they were at least 18 years old and working full-time. Faculty comprised 41.1% of the sample, while 57.8% were staff. Sixty-nine percent identified as female and 29.3% as male. The majority were Caucasian/White (82.4%), followed by African American or Black (10.3%), Asian or Pacific Islander (1.8%), Hispanic or Latino (1.5%), and other (2.1%). Participants’ ages ranged from 21 to 77 (M = 51.6, SD = 12.5). Sixty-eight percent were married or in a domestic partnership, while 17.2% identified as single/never married. Sixty-three percent reported having children, and some participants (28.5%) had caregiver roles outside of parenting (e.g., caring for an elderly relative). In terms of education, 29.4% had a master’s degree, 28.4% a doctorate degree, 21.1% a bachelor’s degree, 9.1% an associate’s degree, 6.7% a professional degree (e.g., M.D.), and 4.7% a high school diploma. On average, participants worked 11.4 years at their current organization, and 13.6 years in their current position. Including hours spent at work and work done outside the office that supplements one’s job, the average number of hours worked per week was 49.1 hours (SD = 8.47), with participants working from home an average of 25.3 weekly hours (SD = 4.39).
3.2Procedure
The study was approved by the university’s Institutional Review Board (IRB; UMCIRB 19-002684) on 11/4/2019, and ethical standards in the treatment of participants were followed. Participants were recruited via a university-wide faculty and staff listserv that distributed a study invitation email to the university email addresses of faculty and staff listserv subscribers. The email detailed an overview of the topic, the study requirements, the estimated time for completion, and a link to the online survey in Qualtrics. Upon going to the survey web address, they were presented with an informed consent form, which indicated their participation was voluntary, and their responses would be anonymous and confidential. Upon providing consent, participants were assessed on measures of workaholism, PsyCap, physical health, and work stress. Demographic information was also obtained. Participants who met eligibility criteria (i.e., at least 18 years old and working full-time) were included in the analyses.
Data were cleaned using SPSS version 27, with an initial sample size of 437 participants. Ninety-four cases were deleted due to one or more of the following reasons: participants took less than two minutes to complete the survey, participants were missing more than 50% of all data points, or participants were missing responses to an entire scale of the survey. If 10% or more of responses to a scale was missing, composite scores were not calculated for that case. Cases missing fewer than 10% of the items on a scale had scale scores computed by person mean imputation. At the end of this process, 343 participants remained in the study.
3.3Data analysis
Data analyses were conducted utilizing SPSS version 27, with the exception of the slopes for the significant moderation analysis, which were determined using SAS version 9.4. Descriptive statistics were calculated for study variables (see Table 1). Pearson correlations were calculated to test H1a and H1b as well as H2a and H2b. Moderation analyses were conducted to test H3a and H3b. Two separate multiple regression analyses were conducted to test these hypotheses, with workaholism as the predictor, work stress and physical health as criteria, and PsyCap as the potential moderator, with a .05 criterion for statistical significance. First, the main effects of workaholism and PsyCap were examined, followed by their interaction (Workaholism X PsyCap), using Hayes’ PROCESS macro [70] to determine the potential moderating influence of PsyCap.
Table 1
Descriptive statistics and intercorrelations
| Variable | 1 | 2 | 3 | 4 |
| 1. Workaholism | (0.94) | |||
| 2. PsyCap | –0.36** | (0.91) | ||
| 3. Physical Health | –0.44** | 0.23** | (0.89) | |
| 4. Work Stress | 0.55** | –0.30** | –0.39** | (0.87) |
| Range | 1.00–4.21 | 1.38–4.88 | 1.21–7.00 | 1.00–2.00 |
| M | 2.49 | 3.78 | 4.99 | 1.48 |
| SD | 0.66 | 0.51 | 1.10 | 0.34 |
Note. N = 343. Entries on the main diagonal are Cronbach’s alphas. PsyCap = Psychological Capital. *p < 0.05, **p < 0.01.
3.4Measures
3.4.1Workaholism
The Workaholism Analysis Questionnaire [WAQ; 71] was used to assess workaholism. The WAQ is a unidimensional measure that emphasizes work-life imbalance and high work drive [71]. Respondents rate each of the 29 items on the WAQ using a 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). Items are averaged for a total score, with higher scores reflecting greater levels of workaholism. In the current study, a Cronbach’s alpha of .94 was obtained.
3.4.2Psychological capital
The Psychological Capital Questionnaire [PCQ; 27] was used to assess overall levels of PsyCap. The PCQ consists of 24 items that encompass the four dimensions of hope, efficacy, resilience, and optimism. While the PCQ is multidimensional, there is strong evidence to support the four components together create a higher-order construct that is measurable and consistently used in previous literature [26]. Accordingly, we utilized the total PCQ score in our analyses. Participants respond using a six-point scale ranging from 1 (strongly disagree) to 6 (strongly agree) to describe their current feelings [27]. After reverse-scoring three items, items are averaged for a total score, with higher scores indicating greater levels of PsyCap. A Cronbach’s alpha of .85 was obtained in the current study.
3.4.3Physical health
The 14-item Physical Health Questionnaire [PHQ; 72] was used to assess overall physical health. The PHQ assesses four dimensions of physical health: digestion problems, headaches, quality of sleep, and respiratory problems. Participants respond to questions on a scale from 1 (not at all) to 7 (all the time). After reverse-scoring one item, items are averaged for a total score, with higher scores depicting lower levels of physical health. In the current study, internal consistencies for each of the PHQ four dimensions were as follows: 0.77, 0.91, 0.88, and 0.82, respectively. Additionally, the Cronbach’s alpha for the overall physical health scale was .89.
3.4.4Work stress
The Stress in General Revised Scale [SIG-R; 73] was used to assess work stress. This 8-item measure assesses the level of work strain individuals experience. Participants are presented with words or phrases in which they identify whether or not that word or phrase is representative of their work. Responses are based on the following three-point response scale: “yes,”(1) “no,”(2) or “cannot decide”(3), with responses of “3” coded as missing. After reverse-scoring one item, items are averaged, with higher scores representing greater work stress. In the current study, we obtained a Cronbach’s alpha of .87 for the SIG-R.
4Results
Descriptive statistics for study variables are shown in Table 1. Pearson correlations among workaholism, physical health, work stress, and PsyCap were all significant (see Table 1). H1a was supported, as workaholism had a medium-to-large negative correlation with physical health, r = –0.44, 95% CI [–0.52, –0.35], p < .001. There was a large positive correlation between workaholism and work stress, r = 0.55, 95% CI [.47,.62], p < 0.001, hence, H1b was supported. PsyCap had a small-to-medium positive correlation with physical health, r = 0.23, 95% CI [.13,.33], p < 0.001, thereby supporting H2a. H2b was also supported, as PsyCap had a medium negative correlation with work stress, r = –0.30, 95% CI [–0.20, –0.39], p < 0.001.
A multiple regression analysis was used to test the effects of workaholism and PsyCap on physical health. The model was significant and the predictors accounted for 20% of the variance in physical health, F(2, 340) = 41.50, p < 0.001, R2 = 0.20. Workaholism (p < 0.001), but not PsyCap (p = 0.10), had a significant partial effect for predicting physical health. Next, the WAQ and PsyCap variables were standardized and an interaction term was created (WAQ x PsyCap) and then added to the model to test for the potential moderating effect of PsyCap. The addition of the interaction term did not significantly increase the explained variance in physical health, F(1, 339) = 1.14, p = 0.29, ΔR2 = 0.003, thus, H3a was not supported.
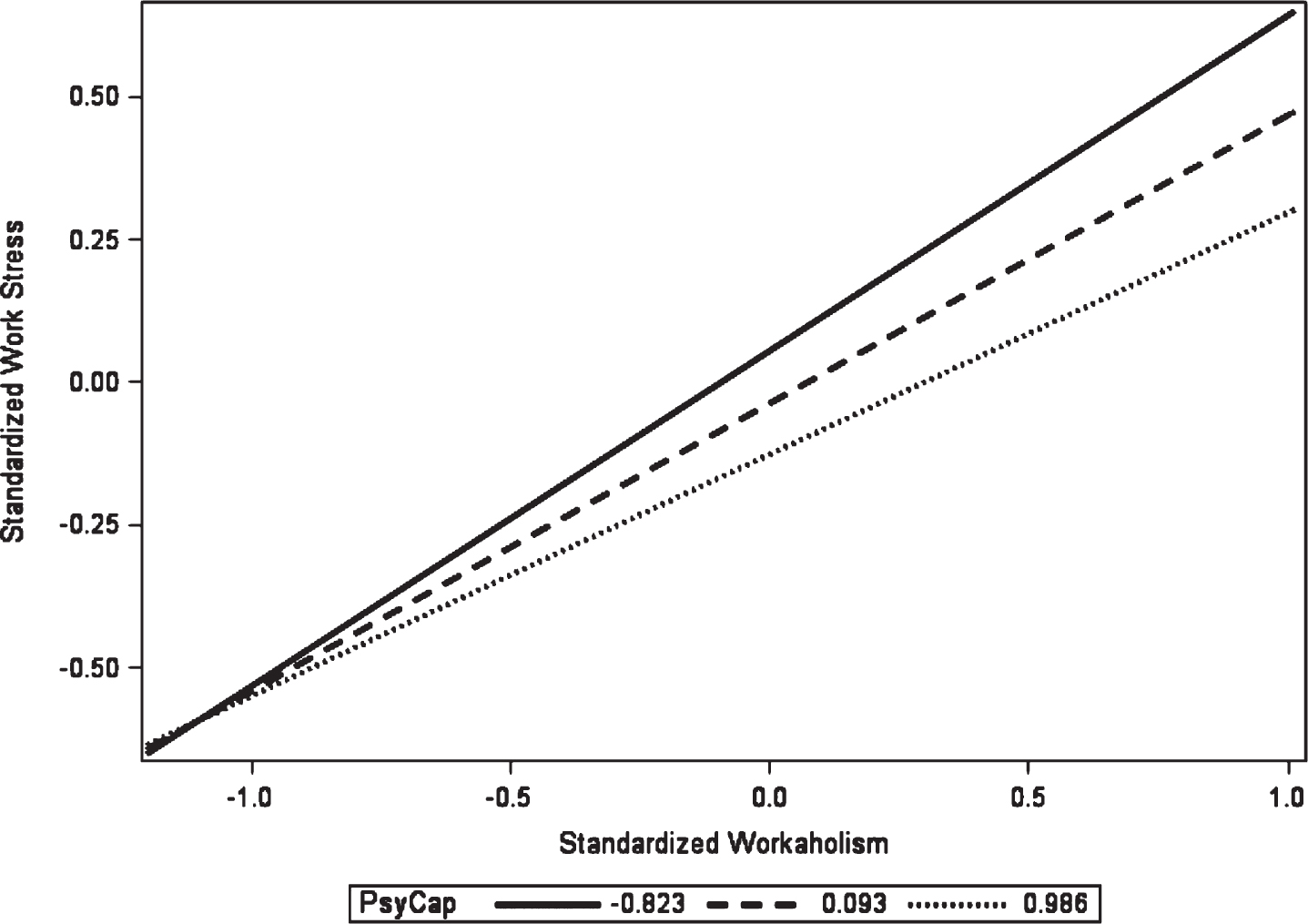
A multiple regression analysis was used to test the effects of workaholism and PsyCap on work stress. This model was significant and the predictors accounted for 32% of the variance in work stress, F(2, 338) = 77.57, p < 0.001, R2 = 0.32. Both workaholism (p < 0.001) and PsyCap (p = 0.02) had significant partial effects for predicting work stress. The addition of the WAQ x PsyCap interaction term to the model significantly increased the explained variance in work stress, F(1, 337) = 4.69, p = 0.03, ΔR2 = 0.009. Figure 1 illustrates the effect of workaholism on work stress at three different levels of PsyCap, showing significant changes in slopes between the lines. The standardized slope for work stress was significant at the 16th percentile (β= 0.59), 50th percentile (β= 0.50), and 84th percentile (β= 0.42). As the level of PsyCap increased, the strength of the relationship between workaholism and work stress decreased. Hence, PsyCap acted as a moderator between workaholism and work stress, therefore, H3b was supported.
Fig. 1
PsyCap as a moderator between workaholism and work stress.
5Discussion
Given the harmful outcomes associated with workaholism, it is imperative to study ways to reduce it. In the current study, we examined PsyCap’s relationship with workaholism, as well as physical health and work stress, to discover potential ways in which the deleterious outcomes of workaholism can be alleviated. A gap in the literature is filled by investigating the possible moderating effect of PsyCap in the relationship between workaholism with physical health and work stress. With wellness programs as a popular benefit to organizations, [74] it could be beneficial to incorporate PsyCap into such trainings, especially given that it can be learned and developed [66].
Our findings add to the current literature that links workaholism to diminished physical health [e.g., lack of sleep, disabling pack pain; 24]. There is also overlap between workaholism and Type A personality traits, [4] which in turn are related to reduced physical health [75]. Substantial research exists that supports a strong link between workaholism and increased work stress [4, 10]. Our research substantiates this relationship, as we found a strong correlation between workaholism and work stress. This association could be explained in part by workaholics’ desire to live up to or exceed unrealistic job demands and expectations [13]. Additionally, perhaps workaholics are drawn to work environments that are high-pressure and demanding. These findings are consistent with the JD-C theory of work stress, which indicates one feels stress at work due to job demands that are out of one’s reach [60].
Our data also revealed a positive relationship between PsyCap and physical health. PsyCap is viewed as a coping mechanism for various ailments [8], thus, perhaps those suffering from physical conditions can heal or recover more successfully if they also display higher levels of PsyCap. The current research also supported a negative relationship between PsyCap and work stress, which is consistent with previous literature [29, 66]. PsyCap likely enables one to better cope with work stress. Personal resources (e.g., optimism) can lead to a more positive appraisal of one’s ability to manage job demands, thereby lowering one’s perceived level of work stress, [69] and PsyCap may act in a similar manner. Moreover, it may mitigate the influence of the JD-R model of work stress by elevating one’s appraisal of their personal resources and boosting their confidence when dealing with demands at work.
The potentially moderating role of PsyCap in the relationship of workaholism with physical health and work stress was also assessed. The results did not support PsyCap as a moderator in the relationship between workaholism and physical health. Given that workaholism is related to unhealthy behaviors, perhaps these behaviors directly influence one’s health and the relationship is unaffected by psychological resources such as PsyCap. However, PsyCap did moderate the relationship between workaholism and work stress. Workaholics spend less time on leisurely activities, which decreases their ability to recover from work and its subsequent stressors [4]. Additionally, the excessive amount of work workaholics engage in may contribute to them feeling as though they do not have sufficient resources to complete their tasks. When employees feel they lack resources, it enhances work stress [76]. Using PsyCap as a positive psychological resource may help mitigate this influence on work stress.
5.1Study limitations
Generalizability may be a limitation given that the study was conducted with employees at a large university and thus 86.6% of respondents had at least a BA degree and 65.2% had at least a MA degree. Furthermore, the majority of respondents self-identified as Caucasian/White (82.5%). Future researchers should sample from individuals who are more diverse in race/ethnicity and education levels, as well as other job settings.
The use of self-report lends itself to the possibility that participants may not report accurately and/or honestly [77]. Nonetheless, it is an important tool to obtain information that peers or observers may not see [78]. This is especially true when studying organizational variables such as workaholism and PsyCap. The use of self-report data can also lead to common method variance, particularly when data are collected at one time point [79]. However, Conway and Lance [80] argue it is an appropriate way to collect data, as it does not always lead to biased responses. Moreover, in the current study, we are interested in the subjective experience of the participant.
Due to the use of a cross-sectional design, causal inferences cannot be made, and the directionality of the relationships between variables cannot be concluded (i.e., reverse causality may exist). Hence, future researchers should examine workaholism and PsyCap in a longitudinal framework to help elucidate the causal and temporal effects workaholism may have on employees. As noted by Andreassen, [81] the short-term influence of workaholism may be beneficial, but the long-term effects are harmful for physical and mental health [4]. Moreover, PsyCap can be developed, [66] so it would be beneficial to examine the influence it may have over time. That said, cross-sectional designs are inexpensive, easy to conduct, and provide the foundation before incorporating longitudinal designs [82].
5.2Organizational implications
Workaholics often self-select into organizations labelled as high-demand or high-stress. While making changes to the organizational climate can be difficult and expensive, enhancing one’s mindset and approach to work may be a better option. By integrating hope, efficacy, resilience, and optimism into one’s psychological resources, one may cope more effectively with their work environment and job demands. Additionally, if the organization opts into a wellness program, it may be beneficial to incorporate PsyCap as a positive psychological resource for its employees. Since PsyCap can be learned through short training sessions [66] it may be a relatively simple and cost-effective intervention for organizations to implement. Our results point to the beneficial role PsyCap may play in mitigating the stressful influence workaholism has on employees.
6Conclusions
The current study results support the relationships of workaholism and PsyCap with physical health and work stress. Moreover, the moderating role of PsyCap in the relationship between workaholism and work stress has promising implications for both employees and organizations. The results shed light on one way workaholism may contribute to increased work stress. Depleted psychological resources exacerbate the relationship between workaholism and work stress, hence, training for PsyCap could mitigate this association. Some organizations use wellness programs as an added benefit for their employees—our findings suggest a way to potentially enhance those programs. By incorporating PsyCap, organizations might be able to help mitigate levels of stress in their employees, specifically among those who suffer from workaholism.
Acknowledgments
The authors have no acknowledgements.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
The authors report no funding.
Informed consent
Informed consent was obtained from all participants prior to enrollment. They were informed as follows:
You are being invited to participate in a research study titled “Workaholism and Well-Being: Psychological Capital as a Potential Moderator” being conducted by Beatrice DeMott, graduate student at East Carolina University in the Psychology Department. The goal is to survey 500 individuals at East Carolina University. The survey will take approximately 10–15 minutes to complete. It is hoped that this information will assist us to better understand the relationship between work styles, well-being, and psychological capital. Your responses will be kept confidential and no data will be released or used with your identification attached. Your participation in the research is voluntary. You may choose not to answer any or all questions, and you may stop at any time. There is no penalty for not taking part in this research study. Please call Beatrice DeMott at 267-280-2484 for any research related questions or the Office of Research Integrity & Compliance (ORIC) at 252-744-2914 for questions about your rights as a research participant.
References
[1] | American Psychological Association. The Impact of stress. [Internet]. American Psychological Association. (2011) . Available from: https://www.apa.org/news/press/releases/stress/2011/impact# |
[2] | Clark. Health and safety at work: Summary statistics for Great Britain. [Internet]. Health and Safety Executive. (2018) . Available from: https://www.hse.gov.uk/statistics/overall/hssh1718.pdf |
[3] | Oates W . Confessions of a workaholic: The facts about work addiction. New York: World. (1971) . |
[4] | Clark MA , Michel JS , Zhandova L , Pui SY , Baltes BB . All work and no play? A meta-analytic examination of the correlates and outcome of workaholism. J Manage. (2016) ;42: (7):786–91. |
[5] | Taris TW , Schaufeli WB , Verhoeven LC . Workaholism in the Netherlands: Measurement and implications for job strain and work-nonwork conflict. Am J Appl Psychol. (2005) ;54: (1):37–60. |
[6] | Luthans F , Youssef-Morgan CM . Psychological capital: An evidence based positive approach. Annu Rev Organ Psychol Organ Behav. (2017) ;4: (17):339–66. |
[7] | Li B , Ma H , Guo Y , Xu F , Zhou Z . Positive psychological capital: A new approach to social support and subjective well-being. Soc Behav Pers. (2014) ;42: (1):135–44. |
[8] | Rabenu E , Yaniv E , Elizur D . The relationship between psychological capital, coping with stress, well-being, and performance. Cur Psych. (2017) ;36: (4):875–87. |
[9] | Nguyen TD , Nguyen TT . Psychological capital, quality of work life, quality of life of marketers: Evidence from Vietnam. J Macromarketing. (2012) ;32: (1):87–95. |
[10] | Aziz S , Zickar MJ . A cluster analysis investigation of workaholism as a syndrome. Int J Workplace Health Manag. (2006) ;11: (1):52–62. |
[11] | Nie Y , Sun H . Why do workaholics experience depression? A study with Chinese University teachers. J Health Psych. (2016) ;21: (10):2339–46. |
[12] | Avey JB , Reichard RJ , Luthans F , Mhatre KH . Meta-analysis of the impact of positive psychological capital on employee attitudes, behaviors, and performance. Hum Resour Dev Q. (2011) ;22: (2):127–52. |
[13] | Aziz S , Widis A , Wuensch KL . The association between emotional labor and burnout: The moderating role of psychological capital. Occup Health Sci. (2018) ;2: (4):365–83. |
[14] | Spence JT , Robbins AS . Workaholism: Definition, measurement, and preliminary results. J Pers Assess. (1992) ;58: (1):160–78. |
[15] | Avanzi L , van Dick R , Fraccaroli F , Sarchielli G . The downside of organizational identification Relations between identification, workaholism, and well-being. Work Stress. (2012) ;26: (3):289–307. |
[16] | Del Libano M , Llorens S , Salanova M , Schaufeli WB . About the dark and bright sides of self-efficacy: Workaholism and work engagement. Span J Psychol. (2012) ;15: (2):688–701. |
[17] | Van Wijhe C , Peeters M , Schaufeli W , Ouweneel E . Rise and shine: Recovery experiences of workaholic and nonworkaholic employees. Eur J Work Organ Psychol. (2013) ;22: (4):476–89. |
[18] | Balducci C , Avanzi L , Fraccaroli F . The individual costs of workaholism: An analysis based on multisource and prospective data. J Manage. (2018) ;44: (7):2961–86. |
[19] | Clark MA , Lelchook AM , Taylor ML . Beyond the big five: How narcissism, perfectionism, and dispositional affect relate to workaholism. Pers Indiv Diff. (2010) ;48: (7):786–91. |
[20] | Serrano-Fernández MJ , Boada-Grau J , Boada-Cuerva M , Vigil-Colet A . Work addiction as a predictor of anxiety and depression. Work. (2021) ;68: (3):779–88. |
[21] | Andreassen CS , Nielsen MB , Pallesen S , Gjerstad J . The relationship between psychosocial work variables and workaholism: Findings from a nationally representative survey. Int J Stress Manag. (2019) ;26: (1):1–10. |
[22] | Andreassen CS , Griffiths MD , Sinha R , Hetland J , Pallesen S . The relationships between workaholism and symptoms of psychiatric disorders: A large-scale cross-sectional study. PLoS One. (2016) ;11: (5). |
[23] | Aziz S , Wuensch KL , Shaikh SR . Exploring the link between work and health: Workaholism and family history of metabolic diseases. Int J Workplace Health Manag. (2017) ;10: (2):153–63. |
[24] | Caesens G , Stinglhamber F , Luypaert G . The impact of work engagement and workaholism on well-being: The role of work-related social support. Career Dev Int. (2014) ;19: (7):813–35. |
[25] | Salanova M , López-González AA , Llorens S , Del Libano M , Vicente-Herrero MT , Tomás-Salvá M . Your work may be killing you! Workaholism, sleep problems and cardiovascular risk. Work Stress. (2016) ;30: (3):228–42. |
[26] | Luthans F . Positive organizational behavior: Developing and managing psychological strengths. Acad Manag J. (2002) ;16: (1):57–72. |
[27] | Luthans F , Avolio BJ , Avey JB , Norman SM . Positive psychological capital: Measurement and relationship with performance and satisfaction. Pers Psychol. (2007) ;6: (3):541–72. |
[28] | Snyder CR , Sympson S , Ybasco F , Borders T , Babyak M , Higgins R . Development and validation of the state hope scale. J Pers Soc Psych. (1996) ;72: (2):321–35. |
[29] | Newman A , Ucbasaran D , Zhu F , Hirst G . Psychological capital: A review and synthesis. J Org Behav. (2014) ;35: (1):120–38. |
[30] | Southwick SM , Bonanno GA , Masten AS , Panter-Brick C , Yehuda R . Resilience definitions, theory, and challenges: Interdisciplinary perspectives. Eur J Psychotraumatol. (2014) ;5. |
[31] | Carver CS , Scheier MF , Segerstrom SC . Optimism Clin Psychol Rev. (2010) ;30: (7):879–89. |
[32] | Alessandri G , Consiglio C , Luthans F , Borgogni L . Testing a dynamic model of the impact of psychological capital on work engagement and job performance. Career Dev Int. (2018) ;23: (1):33–47. |
[33] | Datu JA , King RB , Valdez JP . Psychological capital bolsters motivation, engagement, and achievement: Cross-sectional and longitudinal studies. J Posit Psychol. (2018) ;13: (3):260–70. |
[34] | Gurbuz S , Yildirim HB . Working in the hangar: The impact of psychological capital on work outcomes on among army aircraft mechanics. Mil Psychol. (2019) ;31: (1):60–70. |
[35] | Probst TM , Gailey NJ , Jiang L , Bohle SL . Psychological capital: Buffering the longitudinal curvilinear effects of job insecurity on performance. Saf Sci. (2017) ;100: (Part A):74–82. |
[36] | Grover SL , Teo ST , Pick D , Roche M , Newton CJ . Psychological capital as a personal resource in the JD-R model. Pers Rev. (2018) ;47: (4):968–84. |
[37] | Roberts SJ , Scherer LL , Bowyer CJ . Job stress and incivility: What role does psychological capital play? J Leadersh Organ Stud. (2011) ;18: (4):448–58. |
[38] | Capio CM , Sit CH , Abernathy B . Physical well-being. In MichalosA, (Ed.), Encyclopedia of Quality of Life and Well-Being Research Netherlands: Springer; (2014) , pp. 4805–07. |
[39] | Rosekind MR , Gregory KB , Mallis MM , Brandt SL , Seal B , Lerner D . The cost of poor sleep: Workplace productivity loss and associated costs. J Occup Environ Med. (2010) ;52: (1):91–8. |
[40] | Conway PM , Campanini P , Sartori S , Dotti R , Costa G . Main and interactive effects of shiftwork, age, and work stress on health in an Italian sample of healthcare workers. Appl Ergon. (2008) ;39: (5):630–9. |
[41] | Leitjen FR , van den Heuvel SG , Tbema JF , van der Beek AJ , Robroek SJ , Burdorf A . The influence of chronic health problems on work ability and productivity at work: A longitudinal study among older employees. Scand J Work Environ Health. (2014) ;40: (5):473–82. |
[42] | Cohen S , Tyrell DA , Smith AP . Negative life events, perceived stress, negative affect, and susceptibility to the common cold. J Pers Soc Psychol. (1993) ;64: (1):131–40. |
[43] | Homo-Delarche F , Fitzpatrick F , Christeff N , Nunez EA , Back JF , Dardenne M . Sex steroids, glucocorticoids, stress, and autoimmunity. The Journal of Steroid Biochemistry and Molecular Biology. (1991) ;40: (4-6):619–37. |
[44] | Cohen S , Herbert TB . Health psychology: Psychological factors and physical disease from the perspective of human psychoneuroimmunology. Annu Rev Psychol. (1996) ;47: :113–42. |
[45] | Anderson BL , Kiecolt-Glaser JK , Glaser R . A biobehavioral model of cancer, stress, and disease course. Am Psychol. (1994) ;49: (5):389–404. |
[46] | Ganster D , Schaubroeck J . Work stress and employee health. J Manag. (1991) ;17: (2):235–71. |
[47] | Ganster DC , Perrewé P . Theories of occupational stress. In QuickJC, TetrickLE, (Eds), Handbook of Occupational Health Psychology. Washington, D.C. American Psychological Association; (2011) , pp. 75–93. |
[48] | Bakker AB , Demerouti E . The job demands-resources model: State of the art. J Manag Psychol. (2007) ;22: (3):309–28. |
[49] | Liu MY , Li N , Li WA , Khan H . Association between psychosocial stress and hypertension: A systematic review and meta-analysis. Neurol Res. (2017) ;39: (6):573–80. |
[50] | Shankar J , Famuyiwa OO . Stress among factory workers in a developing country. J Psychosom Res. (1991) ;35: (2-3):163–71. |
[51] | Bonde JP . Psychosocial factors at work and risk of depression: A systematic review of the epidemiological evidence. Occup Environ Med. (2008) ;65: (7):438–45. |
[52] | Heo YS , Leem JH , Park SG , Jung DY , Kim CH . Job stress as a risk factor for absences among manual workers: A 12-month follow-up study. Ind Health. (2015) ;3: (6):542–52. |
[53] | Yong L , Hu X , Huang X , Zhuang X , Guo P , Feng L , et al. The relationship between job satisfaction, work stress, work–family conflict, and turnover intention among physicians in Guangdong, China: A cross-sectional study. BMJ Open. (2017) ;17: (5). |
[54] | Sussman S , Lisha N , Griffiths MD . Prevalence of the addiction: A problem of the majority or the minority? Eval Health Prof. (2011) ;34: (1):3–56. |
[55] | Hassard J , Teoh KR , Viscokaite G , Dewe P , Cox T . The cost of work-related stress to society. A systematic review. J Occup Health Psychol. (2018) ;23: (1):1–17. |
[56] | Yang H , Schnall PL , Jauregui M , Su TC , Baker D . Work hours and self-reported hypertension among working people in California. Hypertension. (2006) ;48: (4):744–50. |
[57] | Thomas WH , Sorensen KL , Feldman DC . Dimensions, antecedents, and consequences of workaholism: A conceptual integration and extension. J Org Behav. (2007) ;28: (1):111–36. |
[58] | Booth-Kewley S , Friedman HS . Psychological predictors of heart disease: A quantitative review. Psychol Bull. (1987) ;101: (3):343–62. |
[59] | Lanzo L , Aziz S , Wuensch KL . Workaholism and incivility: Stress and psychological capital’s role. Int J Workplace Health Manag. (2016) ;9: (2):165–83. |
[60] | Karasek RA . Demand/control model: A social, emotional, and physiological approach to stress risk and active behavior development. In: StellmanJM, (Ed.), Encyclopedia of occupational health and safety. Geneva. ILO; (1998) , pp. 35.06-34.14. |
[61] | Luthans F , Youssel CM , Sweetman D , Harms P . Meeting the leadership challenge of employee well-being through relationship PsyCap and health PsyCap. J Leadersh Organ Stud. (2013) ;20: (1):114–29. |
[62] | Rasmussen HN , O’Byrne KK , Vandament M , Cole BP . Hope and physical health. In GallagherMW, LopezSJ, (Eds.), The Oxford handbook of hope. New York. Oxford University Press; (2018) , pp. 159–68. |
[63] | Hopkins KD , Sheperd CC , Taylor CL , Zubrick SR . Relationships between psychosocial resilience and physical health status of Western Australian urban Aboriginal youth. PLoS One. (2015) ;10: (12). |
[64] | Bouchard LC , Carver CS , Mens MC , Scheier MF . Optimism, health, and well-being. In DunnDS, (Ed,), Positive psychology: Established and emerging issues. New York, NY. Routledge/Taylor & Francis Group; (2018) , pp. 112–30. |
[65] | Aspinwall LG , Tedeschi RG . The value of positive psychology for health psychology: Progress and pitfalls in examining the relation of positive phenomena to health. Ann Behav Med. (2010) ;39: (1):4–15. |
[66] | Avey JB , Luthans F , Jensen SM . Psychological capital: A positive resource for combating employee stress and turnover. Hum Resour Manag J. (2009) ;48: (5):677–93. |
[67] | Seybold KC , Salomone PR . Understanding workaholism: A review of causes and counseling approaches. J Couns Dev. (1994) ;73: (1):4–9. |
[68] | Tache J , Selye H . On stress and coping mechanisms. Issues Ment Health Nurs. (1985) ;7: (1-4):3–24. |
[69] | Huang J , Wang Y , You X . The job demands-resourced model and job burnout: The mediating role of personal resources. Curr Psychol. (2016) ;35: (4):562–9. |
[70] | Hayes F . Introduction to mediation, moderation, and conditional process analysis. A regression-based approach. New York, NY, The Guilford Press; (2014) . |
[71] | Aziz S , Uhrich B , Wuensch KL , Swords B . The Workaholism Analysis Questionnaire: Emphasizing work-life imbalance and addiction in the measurement of workaholism. J Behav Applied Manag. (2013) ;14: (2):71–86. |
[72] | Schat AC , Kelloway EK , Desmarais S . The Physical Health Questionnaire (PHQ): Construct validation of a self-report scale of somatic symptoms. J Occup Health Psychol. (2005) ;10: (4):363–81. |
[73] | Yankelevich M , Broadfoot A , Gillespie JZ , Guidroz A . General job stress: A unidimensional measure and its non-linear relations with outcome variables. Stress Health. (2012) ;28: (2):137–48. |
[74] | Parks KM , Steelman LA . Organizational wellness programs: A meta-analysis. J Occup Health Psychol. (2008) ;13: (1):58–68. |
[75] | Dua JK . The role of negative affect and positive affect in stress, depression, self-esteem, assertiveness, Type A behaviors, psychological health, and physical health. Genet Soc Gen Psychol Monogr. (1993) ;111: (4):515–52. |
[76] | Lazarus RS . Theory based stress measurement. Psychol Inq. (1990) ;1: (1):3–13. |
[77] | Austin EJ , Deary IJ , Gibson GJ , Mcgregor MJ , Dent JB . Individual response spread in self-report scales: Personality correlations and consequences. Pers Indiv Diff. (1998) ;24: (3):421–38. |
[78] | Spector PE . Using self-report questionnaires in OB research: A comment on the use of a controversial method. J Organ Behav. (1994) ;34: (5):125–37. |
[79] | Podsakoff PM , MacKenzie SB , Lee JY , Podsakoff NP . Common method biases in behavioral research: A critical review of the literature and recommended remedies. J Applied Psychol. (2003) ;88: (5):879–903. |
[80] | Conway JM , Lance CE . What reviewers should expect from authors regarding common method bias in organizational research. J Bus Psychol. (2010) ;25: (3):325–34. |
[81] | Andreassen CS . Workaholism: An overview and current status of the research. J Behav Addict. (2014) ;3: (1):1–11. |
[82] | Spector PE . Do not cross me: Optimizing the use of cross-sectional designs. J Bus Psychol. (2019) ;34: (2):125–37. |


