
Interventions for workplace violence against health-care professionals: A systematic review
Abstract
BACKGROUND:
Workplace violence (WPV) against health-care professionals has been a concern worldwide as it strains the relationship between the patient and healthcare professionals. Implementing mitigation interventions to help the healthcare professionals to prevent and manage these violent episodes might make the workplaces more secure.
OBJECTIVE:
This study aimed to synthesize the recent evidence on intervention strategies for workplace violence.
METHOD:
Four electronic databases (PubMed, Wiley, Cochrane and Google Scholar) were searched for peer-reviewed intervention studies published in the last 11 years to mitigate workplace violence. A qualitative synthesis of the findings from included studies was done.
RESULT:
A total of 17 studies were identified based on prevention and management of workplace violence. The interventions were mainly educational in nature based on a workshop format. These interventions were found to be effective in improving the perceived ability to deal with situations that lead to violence.
CONCLUSION:
Strategies to mitigate violent episodes could be helpful to health-care professionals and administrators in their attempts to make safer workplaces in the health-care settings.
1Introduction
Globally, workplace violence against health-care professionals is identified as a significant problem for administrators and health-care managers [1–3]. Such violence occurs across the world, in different health-care settings and scenarios, and in both the developed and developing countries [1, 3, 4]. These episodes of violence reduce the feeling of safety for the health-care providers and raises concerns about the client and care provider relationship. It also reduces the effectiveness of care provided by the health-care personnel. If unchecked, workplace violence has the potential to adversely affect the reputation of the health-care system [5–7]. Thus, the need has been felt to systematically address workplace violence in health-care settings.
Various studies have looked at methods to curb and reduce violent episodes at the workplace [8–10]. Such measures have included de-escalation methods, simulation methods, and changes in health-care processes. The implementation of these measures has been evaluated critically for the impact produced in terms of the perceived safety and reduction in incidents of violence. Synthesis of such emerging literature would be of use to health-care professionals, administrators, and policymakers in getting information about which measures are likely to be of use in their settings. It is expected that health-care scenarios might vary across countries and across services in a country. Yet, a systematic review would be helpful to draw upon the experience of others who have worked in this area.
Several systematic reviews have looked at interventions to address workplace violence [11–13]. A comprehensive systematic review on doctors reported moderate effects of integrated workplace violence interventions in reducing patient-led aggressive episodes [14]. These interventions are specific to a setting such as the emergency department or group of healthcare professionals such as doctors or nurses. The findings of these reviews cannot be generalized to all the healthcare professionals, and thus a systematic review on healthcare professionals is desirable. Thus, this systematic review was planned to collate and synthesize the intervention studies for addressing workplace violence against health-care professionals.
2Method
The aim of this systematic review was to study the interventions that tried to address the occurrence of workplace violence against health-care professionals in the world literature. This review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [15]. The SPIDER formulation was considered for defining the key elements of the review question and is presented in Table 1.
Table 1
Key elements of the research question
| SPIDER tool components | Key elements of the research question |
| S- Sample | The sample includes healthcare practitioners such as general practitioner, clinicians, physicians, surgeons, residents, interns and nurses working at any healthcare setting involved with patient care. |
| PI- Phenomenon of interest | Any form of violence: physical or verbal. Incidences of abuse, threat or assault related to the workplace that can compromise the safety, wellbeing, or health of the workers. |
| D- Design | Training and intervention providing education and /or hands-on-training on techniques to prevent and manage episodes of workplace violence. |
| E- Evaluation | Reduction in frequency of violent episodes. |
| Differences in the pre and post intervention scores to assess the efficacy of intervention to mitigate workplace violence. | |
| R- Research type | Quantitative and Mixed Method Study |
| Intervention based studies with the following designs were selected: quasi-experimental, case-control, pre-post (longitudinal), cohort, or randomized controlled trial |
2.1Literature search
Search terms were identified through literature review, in-depth discussion and expert opinions. The authors devised a search strategy combining keywords pertaining to violence, health-care professionals and interventions in the form: (aggression OR violence) AND (Surgeon OR Resident OR Intern OR physician OR doctor OR “general practitioner” OR “health care practitioner” OR Nurses OR Clinicians) AND (workplace) AND (prevent*OR strateg*OR intervent*). This keyword string was searched on PubMed, Wiley Online Library, Cochrane Library and Google Scholar electronic databases. Hand searches and contacting researchers were not carried out as a part of this study.
Searches were limited to: intervention-based studies in peer-reviewed journals published in English language journals in eleven-year period between October 2009 and September 2020. Case reports, case series, reviews, opinion pieces, commentaries or editorials were excluded.
2.2Data extraction
The studies included according to inclusion and exclusion criteria were evaluated in detail. The details that were extracted from the identified studies included the country, type of study, sample size and characteristics, intervention and the findings. The details were extracted by two researchers (SC and TK) and discrepancies were resolved through consensus with the third author (PR).
2.3Methodological quality
The included studies were critically appraised for methodological quality by Johanna Briggs Institute Critical Appraisal Tools for quasi-experimental studies and randomized control trials [16]. A nine-item checklist (cause and effect, control group, outcome measurement, follow-up, statistical analysis) was used to evaluate the quality of the included studies by marking each item in the checklist as ‘Yes’, ‘Unclear’ or ‘No’. The responses on each item were used to evaluate overall quality. The methodological quality was independently assessed by two reviewers (SC and TK) and disagreements were sought to be resolved with the help of a third reviewer (PR). A risk of bias graph was made using Cochrane Collaboration Tool Review Manager Version 5.3 for randomised control trials included in this review [17]. Quantitative synthesis (meta-analysis) was not performed, due to heterogeneity in study designs and outcome measures.
3Results
The selection of articles according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart is depicted in Fig. 1. A total of 17 studies were identified and extracted data is presented in Table 2.
Fig. 1
Study selection.
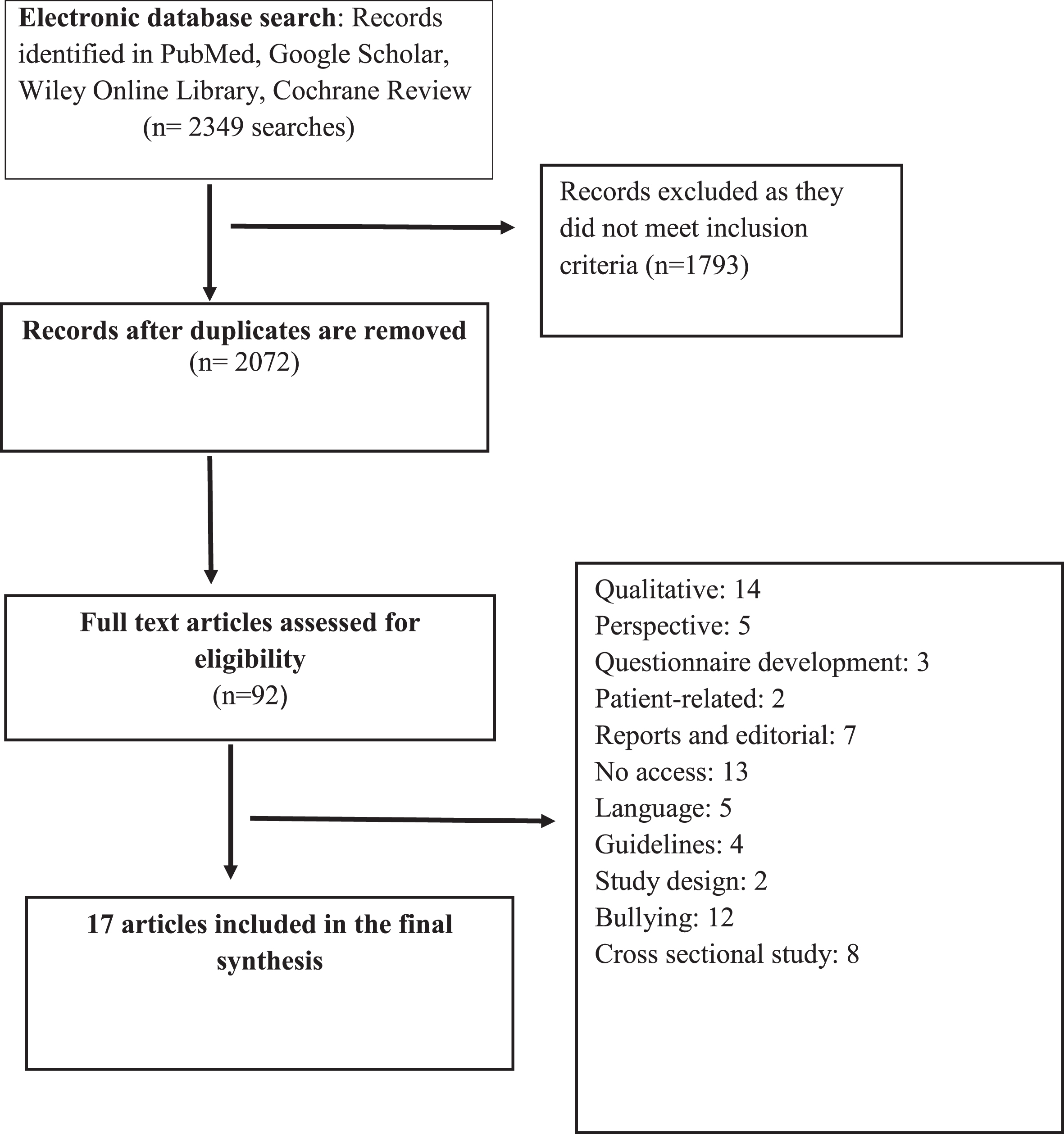
Table 2
Intervention studies on managing workplace violence
| Author, year | Country | Type of study, sample size and characteristics | Intervention | Findings | Methodological Quality* |
| 1. Hsieh et al. [18] | Taiwan | Quasi-experimental study design. 135 nurses, age 35.61±8.18 years, female 88.10% | Participants were given two hours of resilience-enhancing training. | Significant improvement in both the intervention groups in comparison to the control group in depressive symptoms, occupational stress and resilience | Good |
| Participants were divided into three groups: “Biofeedback Training”, “Smartphone Delivered Biofeedback Training”and “control group” | |||||
| 2. Ming et al. [19] | Taiwan | Quasi experimental in national medical centre, 66 participants, mean age 32±9 years, female 87.9%, work experience 10.1±8.9 years | Educated about workplace violence by use of strategies like simulation-based communication, discussions, management techniques | Significant improvement in self-perception and confidence of participants was observed in intervention group | Fair |
| 3. de la Fuente et al. [20] | USA | Pre-post study design in 5 hospital system 31 nurses, female 95.2%, 57.2% had more than 11 years’ experience | Behaviour management training (4 hours): information on alarming signals of violent behaviour, communication skills, and maintenance of personal safety, hands-on training and didactic training | Significant improvement in scores for confidence in handling patient aggression | Fair |
| 4. Coneo et al. [21] | Northern Uganda | A pre-post, convergent mixed-methods design study, 97 participants, males (n = 28) and females (n = 69) | Training program consisted of prevention (70%), de-escalation (20%) and reactive strategies (10%) | Change in staffs’ view towards aggression | Fair |
| 5. Layne et al. [22] | South Carolina | Pre-post study design Pre-survey: 1,980 participants in 2012 Post-survey: 1,423 participants in 2014 | Workshop-based training consisting | Reduction in lateral aggression and vertical aggression | Fair |
| Brain writing techniques to eliminate unprofessional attitude, ensure accountability technique: strategy involving silently sharing written ideas in groups | |||||
| 6. Baby et al. [23] | New Zealand | Cluster randomised, active controlled, single-blinded design 127 healthcare support workers, intervention (n = 63) and controlled condition (n = 64) | Group intervention: communication skills Control condition: four workshops on mindfulness, once in a week facilitated by non-clinical facilitators | No statistical difference between intervention and control group | Fair |
| 7. Hemati-Esmaeili et al. [24] | Iran | Action research study, 49 nurses from emergency department in 5 hospitals, female 95.9%, 87.8% had work experience of less than 5 years | “Prevention of violence in the emergency plan” to brief participants about workplace violence and its dimensions, educate on domains such as anger and stress management and conflict resolution | Verbal violence decreased after implementing the programme Fear of violence decreased significantly | Fair |
| The managerial component of the program administered in three phases i.e. before, during, and after the violence interventions | |||||
| 8. Baig et al. [8] | Pakistan | Quasi-experimental study at a teaching hospital 141 health care providers, 70.4% doctors, female 64.8% | Training for prevention and de-escalation of violence by health-care providers | Confidence in coping with patient aggression was higher in the intervention group | Fair |
| 9. Sanner-Stiehr et al. [25] | USA | Longitudinal, quasi-experimental design-pre and post,129 nursing students Age: 20–25 years old (69.8%), Caucasian (82.2%) Females (82.2%; n = 106) | Training on disruptive behaviors and consequences, roleplay for effective and ineffective response techniques by facilitator, participants invited for cognitive rehearsal, debriefing targeting the affective domain | Statistically significant increase in overall self-efficacy and knowledge | Fair |
| 10. Lamont and Bruner [2] | Australia | Quasi experimental design 78 emergency department nurses, age 41.7±10.9 years, female 72%, experience 16.6±10.7 years | One day workshop with following objectives: | Behaviour intention scores were significantly increased in 14 out of 15 constructs | Fair |
| 1) Developing risk assessment and management plans for workplace violence | |||||
| 2) Applying de-escalation strategies to ease down the escalating aggression | |||||
| 3) Use of breakaway techniques when tackling violent people | |||||
| Techniques included enquiry-based learning and simulation methodology and supervised psychomotor skills | |||||
| 11. Arnetz et al. [26] | USA | Pre-post randomised control trial mixed-methods approach, 2863 participants Intervention group (n = 1,612) and controlled group (n = 1,251) | Total duration of study: 5 years (Pre-intervention: 3 years and post-intervention: 2 years) Intervention: violence data to develop action plan for violence prevention Control Group: no data | Significant decrease was reported in the incident rate ratio (IRR) of violent events in the intervention group after 6 months intervention | Fair |
| Significant decrease in risk of violence-related injury among participants receiving the intervention | |||||
| 12. Martinez [10] | USA | Pilot study, pre-post design 15 nurses, female 80%, age 18 to 54 | Simulation based workshop on WPV and different phases of the assault cycle; | Confidence level significantly increased from pre- to post- training | Fair |
| 13. Kang et al. [27] | South Korea | A Randomized Controlled Trial, n = 40 nurses; Intervention group (n = 20) | “Cognitive rehearsal program” (CRP), a 20-hour intervention on bullying episodes, standard communication, and role-play | Significant differences in interpersonal relationships and turnover intention in intervention group | Fair |
| Mean Age = 32.25±8.48 | |||||
| Wait-List Group (n = 20) | |||||
| Mean Age = 31.25±8.03 | |||||
| 14. Al-Ali et al. [28] | Jordan | Pre-post design | 3-day workshop involving training on different aspects of workplace violence | Significant impact on nurses towards workplace violence | Good |
| 97 nurses, age 28.65±5.23 years, female 60.8%, experience more than 3 years 63% | |||||
| 15. Wong et al. [29] | USA | Pre-post curriculum implementation design, 162 emergency department staff members | 10 case-based simulations sessions for de-escalation and personal defense techniques and 3 hour session on team-based interprofessional approaches, | Significant improvement in internal and external factors and perspectives on patient aggression | Fair |
| 16. Björkdahl et al. [30] | Sweden | Pre-post, prospective non-randomized intervention study, 260 staff and 156 patients completed the intervention in psychiatry department | Training programme containing preventive approach and theoretical nursing framework includes factors as appreciation, emotional regulation and structure | Perception on the questionnaire was significantly more positive among the trained staff in comparison to other staff | Fair |
| 17. Inoue et al. [31] | Japan | Randomized Controlled Trial, n = 62 nurses; intervention group (n = 30) and control group (n = 32) | 90 minutes session, once a week for 4 weeks, Psychotherapy-based discussion to cope with various aspects of WPV and behavioral therapy | Significant differences between the two groups in the domains such as flashback, avoidance behavior, IES-R score, anxiety and depression | Fair |
Methodological Quality for Quasi-Experimental Studies: Total Score: 9 (Refer Table 3). ≥75% (≥6.75) critical appraisal scores- Good. 75% -50% (6.75- 4.5) critical appraisal scores- Fair. ≤50% (≤4.5) critical appraisal scores- Poor. Methodological Quality for Randomised Control Trial: Total Score: 13 (Refer Table 4). ≥75% (≥9.75) critical appraisal scores- Good. 75% -50% (9.75- 6.5) critical appraisal scores- Fair. ≤50% (≤6.5) critical appraisal scores- Poor.
3.1Study design
Studies originated from various countries with six of them being from the USA, two from Taiwan and one each from Australia, Iran, Jordan, Pakistan, New Zealand, Uganda, South Korea, Sweden and Japan. All the studies were described as quasi-experimental and/or pre-post design, except one, which was described as an action research study by the authors [24].
3.2Defining workplace violence
The definition of workplace violence differed in the included studies. Four studies defined workplace violence as incivility, abuse, threat, assault, harassment and bullying leading to physical injury or mental distress. Five studies defined workplace violence in terms of behaviors. Of which, three studies defined workplace violence as patients’ aggressive/violent behavior which might turn into an assault potentially harming the healthcare professional [8, 20, 24]. Other two defined workplace violence as disruptive behavior including lack of civil behavior, horizontal violence, and discord that might lead to distress, anxiety, depression, and even medically unexplained physical symptoms [22, 25]. One study discussed workplace violence in terms of “violent speech/violence” consisting of physical violence, sexual violence, and verbal abuse [31]. Another study defined it as behavioral emergencies/acute agitation which could be due contributed by a number of factors such as rapid metabolic decline, toxic and drug ingestions and psychiatric derangement in the emergency department [29].
3.3Participant characteristics
Participants included only nurses or nursing students in twelve studies [2, 8, 10, 18–20, 24, 25, 27–29, 31], while other five studies included a mixed population consisting of doctors, nurses and ancillary staff as participants [21–23, 26, 30]. The sample size ranged markedly from 15 to 2863 participants, with female preponderance (58.5% –97%) [10, 26]. A majority of participants belonged to the age category of 18–59 years. The participants were recruited from different departments such as emergency, surgical wards, psychiatry, medicine, gynecology, neuroscience, critical care and outpatient settings. Only four studies recruited exclusively from the emergency department [2, 24, 29, 30], two studies from the psychiatry department [18, 31] and two from surgical wards [20, 28].
3.4Intervention characteristics
The studies used two main techniques to limit the number of violent incidents at the workplace. The first technique was based on strategies to prevent violent episodes and the second technique was based on management of violent episodes. The interventions given in the studies were based on either one of these techniques or a combination of these two techniques. One study focused on the preventive aspect of workplace violence by giving intervention on improving awareness and risk assessment skills, while another study used de-escalation methods and communication skills for aggression management among patients [19, 29]. Five studies used a combination of different preventive and management techniques in which participants learned about the preliminary signs of violent behaviour, communication skills for diffusing a violent episode, and means to maintain personal safety [2, 8, 10, 20, 24].
Interventions in the form of resilience training and cognitive rehearsals were also given in a few studies consisting of episodes of bullying, role-plays to mitigate violent behaviour in healthcare systems [18, 25, 27]. Another study included psychotherapy discussion on means of coping with violence and stress management with behavioural therapy [31]. Three studies from the psychiatry and emergency department, included a Simulation-based Training program for managing agitated patients [10, 19, 29].
Most of the interventions were conducted in groups, except one which was conducted through in-person training [20]. The duration of intervention ranged from 3.5 hour seminars to 4 day workshops. The methods used for dissemination of prevention and management techniques were mainly based on didactics and hands-on-training. All the studies used a combination of these techniques, starting with didactics through seminars, power-point presentations, group discussion on real or fictional case scenarios and experiences, brainstorming followed by hands-on-training sessions including role play, video-based simulations, cognitive rehearsal, practicing de-escalation and debriefing techniques and feedback. Only one study provided the participants with a workplace violence training manual as supplementary education material [28].
3.5Instrument and scales: Assessment of outcome measures
Most of the studies used validated scales with high internal consistency (Cronbach α> 0.70) for measuring improvement in healthcare professionals’ ability to manage workplace violence in terms of attitude, confidence and self-efficacy, except one study which measured changes in frequency of workplace violence episodes in the post-intervention period [24]. Four studies used Confidence in Coping Patient Aggression Scale, a 10-item questionnaire used to measure confidence in coping with aggressive situations using likert-scale responses for assessment of outcomes [2, 8, 19, 20]. Another study used Mental Health Nursing Clinical Confidence Scale (MHNCCS) to measure nursing students’ confidence before and after the simulation intervention [10]. Two studies assessed improvement in attitude while dealing with violent episodes using different scales like Attitude Towards Patient Physical Assault questionnaire and Management of Aggression and Violence Attitude Scale (MANVAS) [21, 29]. Self-efficacy to respond to disruptive behavior (SERDB), a self-reported scale assessing domains of previous behavior, motivation, and situational self-efficacy was used to assess improvement in self-efficacy in one of the studies [25].
One study used Perception of Patient Aggression Scale-New Zealand (POPAS-NZ), a 12-item outcome questionnaire to measure the perceived level of patient aggression during violent episodes, stalking and litigation [23] while another study used a 28-item scale “Negative Behaviors in Healthcare (NBHC) instrument” to measure negative behaviours in the healthcare system. To assess the level of psychological stress, depression, anxiety and emotional state of the participants studies used scales such as “Kessler Psychological Distress Scale (K 10)”, Korean version of “Brief Symptom Inventory-18”, “Profile of Mood States (POMS) self-assessment questionnaire” and “Centre for Epidemiologic Studies Depression scale (CES-D)” [18, 23, 27, 31].
3.6Outcomes measures
The reduction in frequency of violent episodes and changes in pre and post intervention scores was used to assess the efficacy of intervention to mitigate workplace violence. A reduction in cases of verbal and physical abuse was reported by 76% nurses [19]. The same study also found a significant increase in the confidence to cope with aggressive behavior, especially among participants with higher education status and willingness to receive training to manage workplace violence [24]. Nurses’ attitudes toward their perceived performance in handling patient aggression also showed significant improvement [28]. After three-month follow-up, an improvement in knowledge about response strategies and self-efficacy to respond to disruptive behaviour was observed among the participants who underwent the intervention [25]. Significant reduction in depressive episodes, distress and increase in resilience was seen among both the intervention groups in comparison to the control group [18]. After attending psychotherapy discussions as an intervention, participants gained confidence in their capability to manage situations involving verbal or physical violence appropriately in the future [31].
3.7Risk of bias assessment
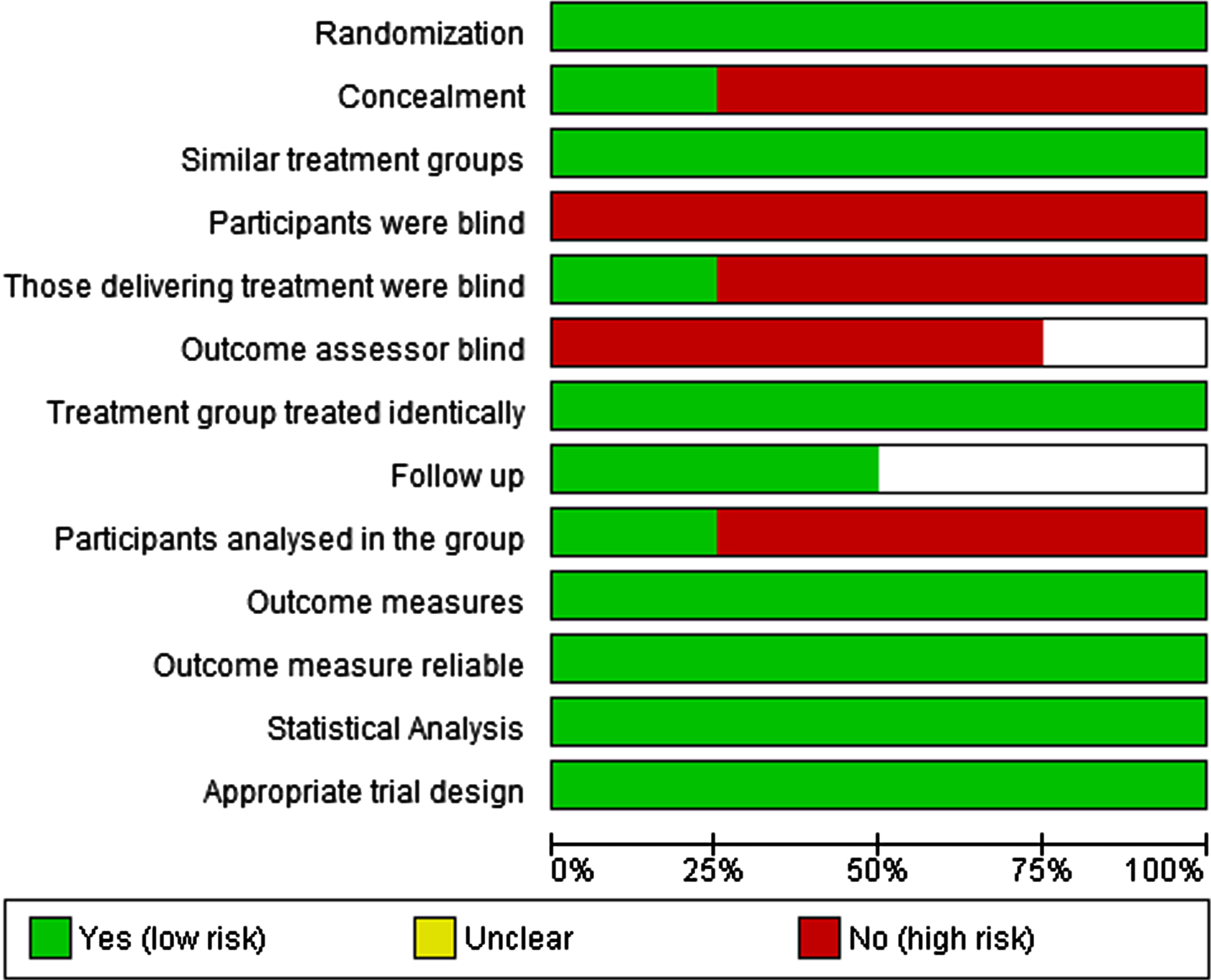
The critical appraisal of the studies was done (as shown in Table 3 and 4) and risk of bias graph was made as shown in Fig. 2 and 3 for Quasi-experimental and RCTs, respectively. All the studies had fair methodological quality, except for the three studies by Al Ali et al., Hsieh et al. and Baig et al., which had good methodological quality [8, 18, 28]. All quasi-experimental studies (n = 9) had low risk for some items such as defined cause and effect, similar interventions to all recruited participants, multiple outcome measurements, reliable measurements and appropriate statistical analysis. All studies had high risk of bias with respect to similar comparison of groups, inclusion of control group and follow up, only one had a control group [8]. Similarly, low risk of bias was found in the RCTs (n = 4) with respect to randomization, similar treatment group, identical treatment of groups, follow-up, outcome measure and its reliability, statistical analysis and appropriate trial design. Four RCTs were found to have high risk for items such as concealment, blinding and participants analysed in the group.
Table 3
Critical Appraisal of the quasi-experimental studies
| Study | 1 - Cause and effect | 2 - Similar comparison of groups | 3 - Similar treatment other than exposure of interest | 4 - Control group | 5 - Multiple outcome measurements | 6 - Follow up | 7 - Participants included in any comparisons measured in same way | 8 - Outcome measurement reliable | 9 - Statistical analysis | Final Score |
| Hsieh et al. [18] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | 8 |
| Ming et al. [19] | Yes | No | Yes | No | Yes | Unclear | No | Yes | Yes | 5 |
| De la Fuente et al. [20] | Yes | No | Yes | No | Yes | Yes | No | Yes | Yes | 6 |
| Coneo et al. [21] | Yes | No | Yes | No | Yes | No | Yes | Yes | Yes | 6 |
| Hemati-Esmaeili et al. [24] | Yes | No | Yes | No | Yes | No | No | Yes | Yes | 5 |
| Baig et al. [8] | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | 8 |
| Sanner-Stiehr et al. [25] | Yes | No | Yes | No | Yes | Yes | No | Yes | Yes | 6 |
| Lamont and Brunero [2] | Yes | No | Yes | No | Yes | Unclear | No | Yes | Yes | 5 |
| Layne et al. [22] | Yes | No | Yes | No | Yes | No | Yes | Yes | Yes | 6 |
| Martinez[10] | Yes | No | Yes | No | Yes | Unclear | No | Yes | Yes | 5 |
| Al-Ali et al. [28] | Yes | Yes | Yes | No | Yes | Unclear | Yes | Yes | Yes | 7 |
| Wong et al. [29] | Yes | No | Yes | No | Yes | Unclear | No | Yes | Yes | 5 |
| Björkdahl et al. [30] | Yes | No | Yes | No | Yes | Unclear | Yes | Yes | Yes | 6 |
Joanna Briggs Critical Appraisal Checklist for Quasi-experimental Studies.
Table 4
Critical Appraisal of Randomised Control Trials
| Study | 1 -Randomisation | 2 -Concealment | 3 -Similar treatment groups | 4 -Participants blinded | 5 -Interventionist blinded | 6 -Outcome assessor blind | 7 -Treatment group treated identically | 8 -Follow-up | 9 -Participants analysed in the group | 10 -Outcome Measures | 11 -Outcome measure reliable | 12 -Statistical analysis | 13 -Appropriate trial design | Final Score |
| Baby et al. [23] | Yes | Yes | Yes | No | Yes | Unclear | Yes | Unclear | No | Yes | Yes | Yes | Yes | 9 |
| Arnetz et al. [26] | Yes | No | Yes | No | No | No | Yes | Yes | No | Yes | Yes | Yes | Yes | 8 |
| Kang et al. [27] | Yes | No | Yes | No | No | No | Yes | Unclear | No | Yes | Yes | Yes | Yes | 7 |
| Inoue et al. [31] | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 9 |
Joanna Briggs Critical Appraisal Checklist for Randomised Control Trials.
Fig. 2
Risk of Bias Graph for Quasi- Experimental Studies.
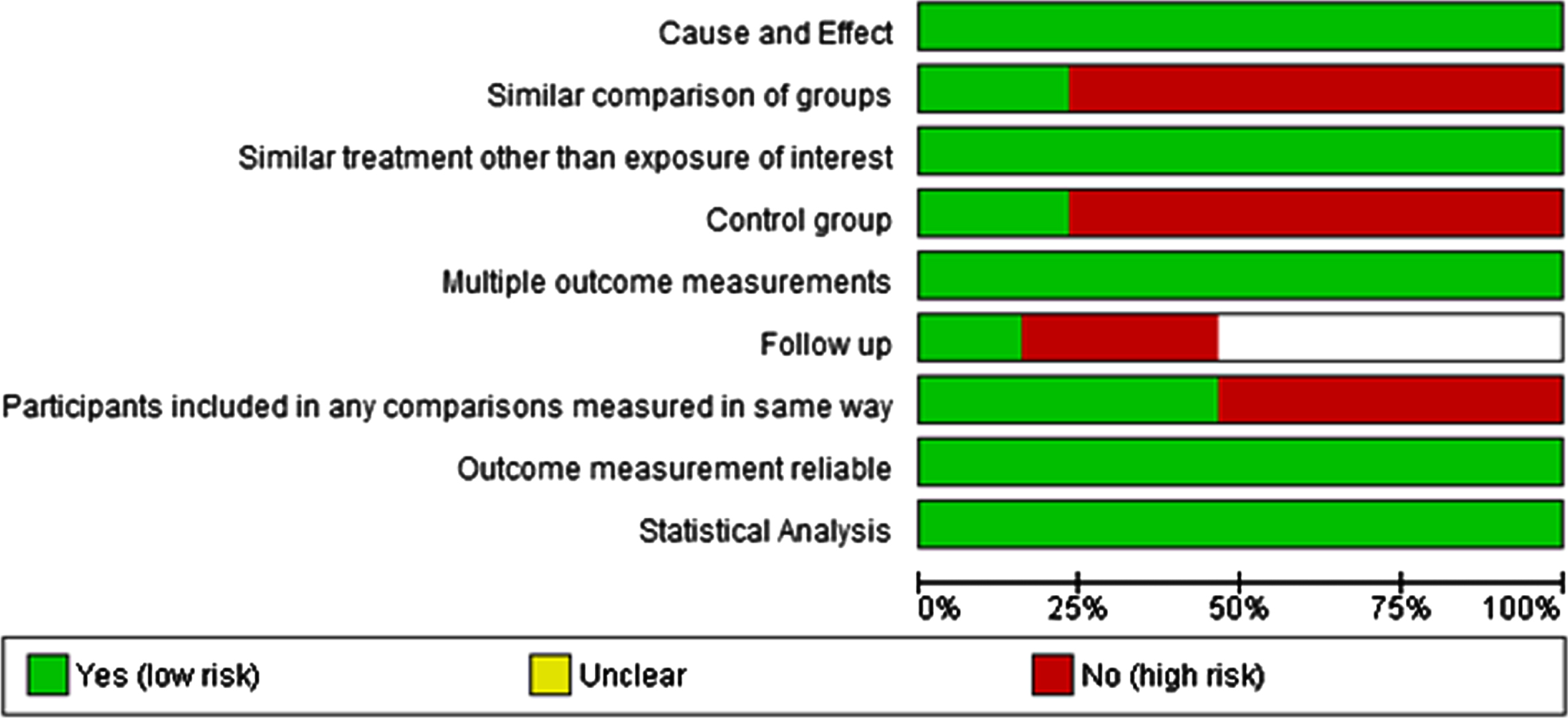
Fig. 3
Risk of Bias Graph for Randomised Control Trials.
4Discussion
The literature in this review is mainly drawn from fair quality quasi-experimental intervention studies with a pre-post design and randomised control trials to compare the improvement in healthcare professionals’ ability in terms of self-efficacy, confidence and/or attitude to prevent and cope with violent episodes at the workplace. Most of the studies recruited nurses working in emergency departments to undergo didactic and hands-on-training in a workshop or seminar format to impart skills on risk assessment of violent episodes and implementable strategies to mitigate these episodes.
This systematic review was based on quasi-experimental studies, a realistic study design to understand different aspects of workplace violence, given the inherent difficulty in researching multidimensional aspects of violence. Only four RCTs were used as the study design. In future, studies should incorporate a control group or opt for an experimental design to derive at more robust conclusions. An inconsistency was observed across studies in defining ‘workplace violence’, which might make cross comparison across studies difficult. Besides, accurately defining workplace violence may be challenging as incivility, assault, aggressive/disruptive behavior and abuse may all be used in combination to define ‘violence’ [32]. The inconsistencies in defining and conceptualization of workplace violence has been identified in literature. A consensus on certain factors that act as criteria for defining an episode of violence should include any or all of the following: intentionality, underlying ideology of perpetrator, hurt, inter-categorical group dynamics and role of environment [33].
We also found that the interventions were targeted to nurses in the emergency department. This behavior is motivated by inter-category dynamics as patients and/or visitors identify themselves as transitory groups attacking an individual (nurses) from hospital staff to attain some objective, mostly related to patient care [34]. Another meta-analysis on prevalence of workplace violence in healthcare settings also reported that nurses working in emergency or psychiatry departments were most prone to episodes of violence [35]. Nurses are primary care providers, who are more closely involved with daily patient care, which might make them more prone to patient/visitor-led violent episodes [36, 37]. In addition, another systematic review demonstrated substantial exposure of emergency department staff to workplace violence with a pooled incident rate of 36 violent cases 10,000 cases [38, 39]. High incidence rate might be contributed by cases presenting with different symptoms such as metabolic decline, brain damage, illicit drug ingestions and psychiatric cases in an emergency department.
The role performance (of patients and healthcare professionals) happens in a specific environment decided by various organisational and psychological factors such as organisational climate, management style, support etc which indirectly contribute to the occurrence of these episodes [40]. It is advised that early assessment of the risk factor that leads to violence should be done for prevention of violent episodes. Our review also highlighted the intervention strategies used to prevent and mitigate workplace violence were inadequate in addressing all the perpetuating factors that lead to patient led violence [39]. In turn, a violent episode also leads to a level of disengagement in the care given to patients [41]
The results of this study point towards some major themes. Firstly, the literature suggested that workshop-based format has been frequently used as a method to educate about workplace violence and has focused on de-escalation techniques and rehearsals with simulated patients. This suggests that communication-based strategies are useful to reduce the incidents of aggressive interactions and enhance confidence of the care providers in dealing with potentially threatening situations. Some interventions based on universal precautionary strategies like ways to correctly approach a patient, keeping safe distance and using the codes during violent episodes were not included in our review, due to their qualitative nature [27, 39].
Secondly, in our review the efficacy of the intervention was measured by the level of improvement in different professional related core skills such as confidence, self-efficacy, intention, and resilient attitude to prevent and manage violent encounters. A significant improvement was observed in all core skills across studies. These skills were measured using different validated tools, which made cross comparisons and pooling of data for quantitative analysis difficult for the authors.
Thirdly, the core skills can be enhanced by using classroom courses, audio-visual simulation, real case scenario-based exercises, and training on de-escalation techniques. Our results are congruent with previous literature which showed that simulation techniques helped the professionals to understand the concept of violence, communication techniques helped to identify early predictors of a violent episode, and de-escalation techniques improved attitude and temperament towards violent episodes [28, 29, 42, 43]. Although studied less frequently, we also found that measures to improve the healthcare processes and systems also have led to reduction in aggressive behaviors and better safety perception of the work environment.
This review elucidated that effective communication can be considered as an initial step to reduce the incidence of patient-led aggression, improve healthcare workers’ experiences in managing these episodes and help them to maintain psychological well-being in the long-term.
4.1Clinical implications
The implications of the abovementioned findings can help to strengthen the communication training of the health-care professionals including doctors, nurses and paramedics. This is quite pertinent in the emergency health-care setting, where communication difficulties are frequently encountered due to constraints of time [44, 45]. Health-care professionals need to continually enhance their communication skills, and participate in teaching methods using hands-on skills to better engage in the learning process [46, 47]. The efficacy of these methods leads to improved ability to deal with difficult situations. The other implication lies in the consideration of mechanisms to streamline patient flow, provide appropriate information to patients and develop strategies and resources to deal with ‘escalated’ situations. These require forethought about the service delivery characteristics and mechanisms, cultural nuances and dynamics of relationships between the health-care provider and the patient. Health-care administrators and managers need to play a balanced role safeguarding the needs of the patients to ensure that they are served properly, and the needs of the health-care staff so that they do not feel threatened or experience burn-out [48].
4.2Limitations
While interpreting findings from this review, certain caveats need to be considered. Firstly, the search was limited to only 11 years and had only English language articles. There could be more literature on the topic in different languages. Secondly, we looked at only two databases for identifying the studies. Additionally, the studies were heterogeneous in design and had used different outcome measures. Hence, summary measures were not computed. Consequently, publication bias could not be commented upon.
5Conclusion
This systematic review presents recent studies which have looked at interventions to address workplace violence among health-care professionals. Though there is emergent literature looking at the ways in which workplace violence could be reduced, more needs to be done and evaluated. The components of the interventions could be looked at, and multi-centric clustered randomized controlled designs could be entertained. Also, different categories of healthcare personnel can be assessed in terms of the efficacy of the interventions. Process indicators like feasibility and acceptance of the methods could also be incorporated. One could hope that attention to workplace violence and addressing it through suitable mechanisms can improve the patient-healthcare provider interaction and improve the safety in the care processes.
Acknowledgments
None to report.
Conflict of interest
The authors declare that they have no conflict of interests.
References
[1] | Gillespie GL , Gates DM , Miller M , Howard PK . Workplace violence in healthcare settings: risk factors and protective strategies. Rehabilitation Nursing. (2010) ;35: (5):177–84. |
[2] | Lamont S , Brunero S . The effect of a workplace violence training program for generalist nurses in the acute hospital setting: A quasi-experimental study. Nurse Education Today. (2018) ;68: :45–52. |
[3] | Tadros A , Kiefer C . Violence in the emergency department: a global problem. Psychiatric Clinics. (2017) ;40: (3):575–84. |
[4] | Taylor JL , Rew L . A systematic review of the literature: workplace violence in the emergency department. Journal of clinical Nursing. (2011) ;20: (7-8):1072–85. |
[5] | Arnetz JE , Arnetz BB . Violence towards health care staff and possible effects on the quality of patient care. Social Science & Medicine. (2001) ;52: (3):417–27. |
[6] | Baydin AK , Erenler AK . Workplace violence in emergency department and its effects on emergency staff. Int J Emerg Ment Health. (2014) ;16: (2):288–90. |
[7] | Lanctôt N , Guay S . The aftermath of workplace violence among healthcare workers: A systematic literature review of the consequences. Aggression and Violent Behavior. (2014) ;19: (5):492–501. |
[8] | Baig L , Tanzil S , Shaikh S , Hashmi I , Khan MA , Polkowski M . Effectiveness of training on de-escalation of violence and management of aggressive behavior faced by health care providers in a public sector hospital of Karachi. Pakistan Journal of Medical Sciences. (2018) ;34: (2):294. |
[9] | Kowalenko T , Cunningham R , Sachs CJ , Gore R , Barata IA , Gates D , Hargarten SW , Josephson EB , Kamat S , Kerr HD , McClain A . Workplace violence in emergency medicine: current knowledge and future directions. The Journal of Emergency Medicine. (2012) ;43: (3):523–31. |
[10] | Martinez AJ . Implementing a workplace violence simulation for undergraduate nursing students: a pilot study. Journal of Psychosocial Nursing and Mental Health Services. (2017) ;55: (10):39–44. |
[11] | Anderson L , FitzGerald M , Luck L . An integrative literature review of interventions to reduce violence against emergency department nurses. Journal of Clinical Nursing. (2010) ;19: (17-18):2520–30. |
[12] | Beech B , Leather P . Workplace violence in the health care sector: A review of staff training and integration of training evaluation models. Aggression and Violent Behavior. (2006) ;11: (1):27–43. |
[13] | Martinez AJ . Managing workplace violence with evidence-based interventions: a literature review. Journal of Psychosocial Nursing and Mental Health Services. (2016) ;54: (9):31–6. |
[14] | Raveel A , Schoenmakers B . Interventions to prevent aggression against doctors: a systematic review. BMJ Open. (2019) ;9: (9):e028465. |
[15] | Liberati A , Altman DG , Tetzlaff J , Mulrow C , Gotzsches PC , Ioannidis JPA , et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. (2009) ;339: :b2700. |
[16] | Tufanaru C , Munn Z , Aromataris E , Campbell J , Hopp L . Chapter 3: Systematic Reviews of Effectiveness. In: Aromataris E, Munn Z, eds. JBI Manual for Evidence Synthesis. JBI 2020. |
[17] | ReviewManager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre. |
[18] | Hsieh HF , Huang I , Liu Y , Chen WL , Lee YW , Hsu HT . The effects of biofeedback training and smartphone-delivered biofeedback training on resilience, occupational stress, and depressive symptoms among abused psychiatric nurses. International Journal of Environmental Research and Public Health. (2020) ;17: (8):2905. |
[19] | Ming JL , Huang HM , Hung SP , Chang CI , Hsu YS , Tzeng YM , Huang HY , Hsu TF . Using simulation training to promote nurses’ effective handling of workplace violence: A quasi-experimental study. International Journal of Environmental Research and Public Health. (2019) ;16: (19):3648. |
[20] | de la Fuente M , Schoenfisch A , Wadsworth B , Foresman-Capuzzi J . Impact of behavior management training on nurses’ confidence in managing patient aggression. JONA: The Journal of Nursing Administration.. (2019) ;49: (2):73–8. |
[21] | Coneo AM , Thompson AR , Parker K , Harrison G . The outcome of a training programme (RESPECT) on staff’s attitudes towards causes and management of aggression in a Regional Referral Hospital of northern Uganda. Journal of Psychiatric and Mental Health Nursing. (2020) ;27: (1):25–40. |
[22] | Layne DM , Nemeth LS , Mueller M , Schaffner MJ , Stanley KM , Martin MM , Wallston KA . Negative behaviours in health care: Prevalence and strategies. Journal of Nursing Management. (2019) ;27: (1):154–60. |
[23] | Baby M , Gale C , Swain N . A communication skills intervention to minimise patient perpetrated aggression for healthcare support workers in New Zealand: A cluster randomised controlled trial. Health Soc Care Community. (2019) ;27: (1):170–81. |
[24] | Hemati-Esmaeili M , Heshmati-Nabavi F , Pouresmail Z , Mazlom SR , Reihani H . Educational and Managerial Policy Making to Reduce Workplace Violence Against Nurses: An Action Research Study. Iran J Nurs Midwifery Res. (2018) ;23: :478–85. |
[25] | Sanner-Stiehr E . Responding to disruptive behaviors in nursing: A longitudinal, quasi-experimental investigation of training for nursing students. Nurse Education Today. (2018) ;68: :105–11. |
[26] | Arnetz JE , Hamblin L , Russell J , Upfal MJ , Luborsky M , Janisse J , Essenmacher L . Preventing patient-to-worker violence in hospitals: outcome of a randomized controlled intervention. Journal of Occupational and Environmental Medicine. (2017) ;59: (1):18. |
[27] | Kang J , Kim JI , Yun S . Effects of a cognitive rehearsal program on interpersonal relationships, workplace bullying, symptom experience, and turnover intention among nurses: A randomized controlled trial. Journal of Korean Academy of Nursing. (2017) ;47: (5):689–99. |
[28] | Al-Ali NM , Al Faouri I , Al-Niarat TF . The impact of training program on nurses’ attitudes toward workplace violence in Jordan. Applied Nursing Research. (2016) ;30: :83–9. |
[29] | Wong AH , Wing L , Weiss B , Gang M . Coordinating a team response to behavioral emergencies in the emergency department: a simulation-enhanced interprofessional curriculum. Western Journal of Emergency Medicine. . (2015) ;16: (6):859. |
[30] | Björkdahl A , Palmstierna T , Hansebo G . The bulldozer and the ballet dancer: aspects of nurses’ caring approaches in acute psychiatric intensive care. Journal of Psychiatric and Mental Health Nursing. (2010) ;17: (6):510–8. |
[31] | Inoue M , Kaneko F , Okamura H . Evaluation of the effectiveness of a group intervention approach for nurses exposed to violent speech or violence caused by patients: a randomized controlled trial. International Scholarly Research Notices. 2011;2011. |
[32] | Luck L , Jackson D , Usher K . Innocent or culpable? Meanings that emergency department nurses ascribe to individual acts of violence. Journal of Clinical Nursing. (2008) ;17: (8):1071–8. |
[33] | Escribano RB , Beneit J , Garcia JL . Violence in the workplace: some critical issues looking at the health sector. Heliyon. (2019) ;5: (3):e01283. |
[34] | World Health Organization (WHO) WHO; Geenva: 2002. World Report on Violence and Health. |
[35] | Liu J , Gan Y , Jiang H , Li L , Dwyer R , Lu K , Yan S , Sampson O , Xu H , Wang C , Zhu Y . Prevalence of workplace violence against healthcare workers: a systematic review and meta-analysis. Occupational and Environmental Medicine. (2019) ;76: (12):927–37. |
[36] | Fafliora E , Bampalis VG , Zarlas G , Sturaitis P , Lianas D , Mantzouranis G . Workplace violence against nurses in three different Greek healthcare settings. Work. (2016) ;53: (3):551–60. |
[37] | Kvas A , Seljak J . Sources of workplace violence against nurses. Work. (2015) ;52: (1):177–84. |
[38] | Nikathil S , Olaussen A , Gocentas RA , Symons E , Mitra B . Workplace violence in the emergency department: A systematic review and meta analysis. Emergency Medicine Australasia. (2017) ;29: (3):265–75. |
[39] | Camerino D , Estryn-Behar M , Conway PM , van Der BI , Hasselhorn HM . Work-related factors and violence among nursing staff in the European NEXT study: a longitudinal cohort study. International Journal of Nursing Studies. (2008) ;45: (1):35–50. |
[40] | Bresler S , Gaskell MB . Risk assessment for patient perpetrated violence: analysis of three assaults against healthcare workers. Work. (2015) ;51: (1):73–7. |
[41] | Forté L , Lanctôt N , Geoffrion S , Marchand A , Guay S . Experiencing violence in a psychiatric setting: Generalized hypervigilance and the influence of caring in the fear experienced. Work. (2017) ;57: (1):55–67. |
[42] | Hahn S , Zeller A , Needham I , Kok G , Dassen T , Halfens RJ . Patient and visitor violence in general hospitals: a systematic review of the literature. Aggression and Violent Behavior. (2008) ;13: (6):431–41. |
[43] | Martinez-Ferran M , de la Guía-Galipienso F , Sanchis-Gomar F , Pareja-Galeano H . Metabolic impacts of confinement during the COVID-19 pandemic due to modified diet and physical activity habits. Nutrients. (2020) ;12: (6):1549. |
[44] | Dean M , Oetzel JG . Physicians’ perspectives of managing tensions around dimensions of effective communication in the emergency department. Health Communication. . (2014) ;29: (3):257–66. |
[45] | Hallett N , Dickens GL . De-escalation of aggressive behaviour in healthcare settings: Concept analysis. International Journal of Nursing Studies. (2017) ;75: :10–20. |
[46] | Renker P , Scribner SA , Huff P . Staff perspectives of violence in the emergency department: appeals for consequences, collaboration, and consistency. Work. (2015) ;51: (1):5–18. |
[47] | Baitha U , Ranjan P , Sarkar S , Arora C , Kumari A , Dwivedi SN , Patil A , Jamshed N . Development of a self-assessment tool for resident doctors’ communication skills in India. Journal of Educational Evaluation for Health Professions. 2019;16. |
[48] | Gillespie GL , Gates DM , Fisher BS . Individual, relationship, workplace, and societal recommendations for addressing healthcare workplace violence. Work. (2015) ;51: (1):67–71. |


