
COVID-19 anxiety and hygiene status in vocational schools of health services students in Turkey: A multicenter study
Abstract
BACKGROUND:
While the coronavirus (COVID-19) pandemic creates fear and anxiety on the students’ academic achievement, the risk of an infectious disease may negatively affect education by reducing the concentration ability of students. Thus, it is essential to evaluate the knowledge, behaviors, anxiety levels, and hygiene status of students.
OBJECTIVE:
This study aimed to investigate the knowledge, behavior change, anxiety, and hygiene status of university students about COVID-19.
METHODS:
The investigation was conducted with students of three vocational schools of health services located in different provinces of Turkey (n = 1055). Data collected by an online survey consisted of knowledge questions about COVID-19, items about behavior change, the hygiene behavior scale (HBS), and the Generalized Anxiety Disorder 7 (GAD-7) scale.
RESULTS:
The knowledge scores of women were significantly higher than the scores of men. Of the students, 59.6%showed positive hygiene behaviors, and 31.5%had anxiety. Female students’ total HDC scale score was significantly lower than that of men, and the total HDC scale score of those who received hand hygiene education was significantly lower than that of participants who did not receive training, which shows a positive hygiene behavior. The total GAD-7 scale score of women was significantly higher than that of men. More than half of the students showed positive hygiene behaviors, and about a third had anxiety.
CONCLUSIONS:
Based on the study’s results, psychological support and training should be provided to students.
1Introduction
One of the most important problems concerning public health was infectious diseases that caused millions of deaths in the past. Coronavirus (COVID-19), a recent infectious disease, has caused a pandemic in a short time, which could be overcome with simple hygiene measures [1]. This disease is transmitted mainly through droplets caused by coughs and sneezes of infected people. After people get in contact with these droplets with their hands, they touch their mouth, nose, or eye mucosa. Common symptoms of infection are respiratory symptoms, fever, cough, and dyspnea. Pneumonia, severe acute respiratory infection, kidney failure, and even death may occur in more serious cases [2].
The risk of health care workers being infected with COVID-19 is very high due to the way it is transmitted. In addition to long working hours, physical and psychological stress, burnout, and fatigue, infectious diseases are an additional danger for health care professionals [3]. In international classifications, it has been revealed in various national records and researches that the health sector, which is in the service sector, is a risky business line [4]. For this reason, COVID-19 is thought to cause uneasiness in health care professionals. This situation causes individuals to drift into anxiety and panic. The pandemic can affect university students physically, academically, financially, and psychologically [5]. The rapid spread of COVID-19 and implemented quarantine measures are expected to worsen mental health by causing anxiety among university students. It has been stated that 24.9%of university students in China were worried about the COVID-19 outbreak, and 87.7%of students in Bangladesh had symptoms of anxiety [6, 7]. Intense anxiety, fear, and uncertainty experienced by individuals can lead to different reactions and poor life quality. Simple measures are very effective in preventing infectious diseases. It has been reported that the failure to provide hand hygiene, which is the first step of personnel hygiene, is the most important risk in the emergence of diseases that occur in different working groups and cause problems that threaten public health [8].
One of the crucial precautions to be taken against the risks that health care professionals are exposed to at work is hand hygiene. Hand washing is also the most important step in preventing hospital infections. In this respect, it contributes significantly to reduce infection risks of health workers [9]. Taking pre-determined precautionary measures (i.e., hand hygiene, wearing a mask) to prevent the spread of COVID-19 can reduce negative psychological effects by providing a sense of security [5]. The infection rate and death statistics of COVID-19 make us think that this situation will spring an unease among students of the vocational school of health services, and this unease will have a positive effect on the hygiene behaviors of the students.
This study aimed to investigate the knowledge status, behavioral change, hygiene, and anxiety levels of university students who will become health technicians against COVID-19.
The following hypotheses have been determined for the research:
H0: There is no difference between students’ state of knowledge about COVID-19, anxiety, and hygiene behavior.
H1: There is a difference between students’ state of knowledge about COVID-19, anxiety, and hygiene behavior.
2Materials and methods
The population of this descriptive and cross-sectional study consisted of students studying in the vocational school of health services at three different universities in Turkey. The total number of students attending the Vocational School of Health Services in Diyarbakır Dicle University (n = 850), Elazig Firat University (n = 780), and Bingol University (n = 760) were 2390. One of every two students was included in the study with a systematic sampling method. Out of 1195 students, 1055 were reached (Response rate 88.3%). Volunteering was taken into account in participation in the study, and non-volunteers were asked not to fill in the questionnaire and ignore the incoming message. The field study of the research was carried out with an online survey method after obtaining the ethics committee (Fırat University Non-invasive Clinical Research Ethics Committee, Number: 390555, Date: 28/04/2020) approval and institutional permission.
2.1Data collection tools
The questionnaire consisted of 5 sections: demographic questions, knowledge questions about COVID-19, questions about behavior change, the hygiene behavior scale, and the Generalized Anxiety Disorder 7 (GAD-7) scale. There were demographic questions in the first part of the questionnaire. In the second part of the questionnaire, the participants were asked questions about the protective practices related to COVID-19 prepared by the researchers using the questions frequently asked on the websites of the World Health Organization and the Turkish Ministry of Health, and by performing a literature search [10–13]. One point was given for each correctly answered question. The score that could be obtained from the knowledge section varied between 0 and 6. In the third part of the questionnaire, questions were about students’ perception of behavior change in their personal hygiene and social habits after COVID-19. The answers to these questions were scored as 0 points for ‘I don’t know,’ 1 point for ‘unchanged,’ 2 points for ‘slightly changed,’ 3 points for ‘moderately changed,’ and 4 points for ‘changed a lot.’ Scores in this section could vary between 0 and 24.
2.2Generalized Anxiety Disorder 7-item (GAD-7) scale
GAD-7 scale is a seven-item scale developed by Spitzer et al. in 2006 according to DSM-IV-TR criteria [14]. Its validity and reliability in the Turkish population were done by Konkan et al. [15]. Studies had reported that GAD-7 had good psychometric characteristics [16, 17]. The GAD-7 scale measures generalized anxiety levels according to DSM IV-TR criteria. GAD-7 is a self-assessment-type scale. A Likert-type scale (0 for none, 1 for some days, 2 for more than half of the number of days, 3 for almost every day) is used in the 7-items of GAD-7. The score that can be obtained from the scale can vary between 0 and 21. The total scores of 5, 10, and 15 obtained from the scale were cut points for mild, moderate, and severe anxiety, respectively.
2.3Hygiene behavior scale
This scale was developed in 2015 by Coban and Bilgin and tested for validity and reliability. The Cronbach alpha internal consistency coefficient of the scale was calculated as 0.90. Therefore, this scale was sufficient in terms of psychometric characteristics. The hygiene behavior scale consists of 25 questions in total and has three sub-dimensions. There were thirteen questions about personal hygiene, six questions about handwashing, and six questions about food hygiene. The scoring of the scale was as follows: 1 point for ‘always,’ 2 points for ‘sometimes,’ 3 points for ‘rare,’ and 4 points for ‘never.’ As the scale score increases, the positive hygiene behavior decreases. The lowest total score that can be obtained from the scale was 25, and the highest score was 100. Those who scored 38 points or above were classified as having a negative hygiene behavior [18].
2.4Statistical analysis
The SPSS version 22.0 statistical packaged software was used for data analysis. Descriptive values were indicated by numbers, percentages, means, and standard deviations. Normality analysis of the numerical data was performed using the Kolmogorov-Smirnov Test. The Student t-test was used to compare binary groups, and the one-way ANOVA test was used in the comparison of more than two groups. Post-hoc analysis was used to find out where the difference originated in triple groups. Pearson correlation analysis was used to compare quantitative data with each other, and p < 0.05 was considered statistically significant in all analyses.
3Results
A total of 1055 students (73.5%women) participated in the study. The mean age of the students was 21.01±2.54 years (min = 18, max = 49). Of students, 37.0%were studying at Dicle University, 33.2%at Firat University, and 29.9%at Bingol University. On the other hand, 59.1%were first grade, and 40.9%were second grade. 56.5%of the students received infectious diseases lectures, and 66.0%had hand hygiene training. COVID-19 positivity was found only in the first- and second-degree relatives of 4.9%of the students (Table 1).
Table 1
Sociodemographic characteristics of the participants
| Number | % | ||
| Age | ≤20 age | 574 | 54.4 |
| >20 age | 481 | 45.6 | |
| Gender | Female | 775 | 73.5 |
| Male | 280 | 26.5 | |
| Years at university | First grade | 624 | 59.1 |
| Second grade | 431 | 40.9 | |
| University | Dicle University | 390 | 37.0 |
| Firat University | 350 | 33.2 | |
| Bingol University | 315 | 29.9 | |
| Marital status | Married | 28 | 2.7 |
| Single | 1027 | 97.3 | |
| Place of residence where he/she lived longest | City | 665 | 63.0 |
| District | 209 | 19.8 | |
| Rural | 181 | 17.2 | |
| Economic status of the family | High | 58 | 5.5 |
| Medium | 806 | 76.4 | |
| Low | 191 | 18.1 |
Of the students, 77.9%believed that the experts’ statements about COVID-19 are true, while 83.8%believed that science and technology would solve the COVID-19 problem. Only 11.2%of the participants thought of quitting school after the COVID-19 outbreak because of the possibility of exposure to this kind of infection at work.
While students gave the most correct answers to the question ‘Avoiding hand, eye, and mouth contact with the hand prevents virus infection and protects against COVID-19,’the question ‘Getting infected will protect against COVID-19’ had the lowest correct answers. The students’ mean score of knowledge was 5.34±1.09. The proportions of correct answers to the knowledge questions are shown in Table 2.
Table 2
Students’ knowledge about COVID-19 [n (%)]
| Question (correct answer) | Correct answer |
| n (%) | |
| COVID-19 is a serious risk that threatens people’s lives (yes) | 910 (86.3) |
| Covering mouth and nose during sneezing prevents virus infection and protects against COVID-19 (yes) | 923 (87.5) |
| Washing hands with soap and water prevents virus infection and protects against COVID-19 (yes) | 992 (94.0) |
| Avoiding hand contact with the eye, mouth, and nose protects against COVID-19 by preventing virus infection (yes) | 1004 (95.2) |
| Eating healthy foods and having a healthy lifestyle protects against COVID-19 (yes) | 923 (87.5) |
| Gaining immunity by getting infected by virus protects against COVID-19 (yes) | 879 (83.3) |
| COVID-19 knowledge score (mean±SD) | 5.34±1.09 |
The answers given by students to the behavioral questions related to COVID-19 are shown in Table 3. Students’ behaviors of avoiding handshakes and getting in touch with people, who have symptoms, have changed, and the mean of their total score was found to be 17.30±5.83.
Table 3
COVID-19 behavior questions
| Questions | I don’t know | Unchanged | Slightly changed | Moderately changed | Changed a lot |
| n (%) | n (%) | n (%) | n (%) | n (%) | |
| Hand washing behavior | 33 (3.1) | 275 (26.1) | 209 (19.8) | 209 (19.8) | 329 (31.2) |
| Buying disinfectants | 56 (5.3) | 208 (19.7) | 243 (23.0) | 197 (18.7) | 351 (33.3) |
| Avoiding contact with people who have symptoms | 54 (5.1) | 63 (6.0) | 97 (9.1) | 123 (11.7) | 718 (68.1) |
| Avoiding social meetings | 87 (8.2) | 94 (8.9) | 127 (12.0) | 165 (15.6) | 582 (55.3) |
| Avoiding handshakes | 41 (3.9) | 78 (7.4) | 111 (10.5) | 131 (12.4) | 694 (65.8) |
| Avoiding public services | 110 (10.4) | 148 (14.0) | 173 (16.4) | 205 (19.4) | 419 (39.8) |
COVID-19 behavior score (mean±SD) = 17.30±5.83.
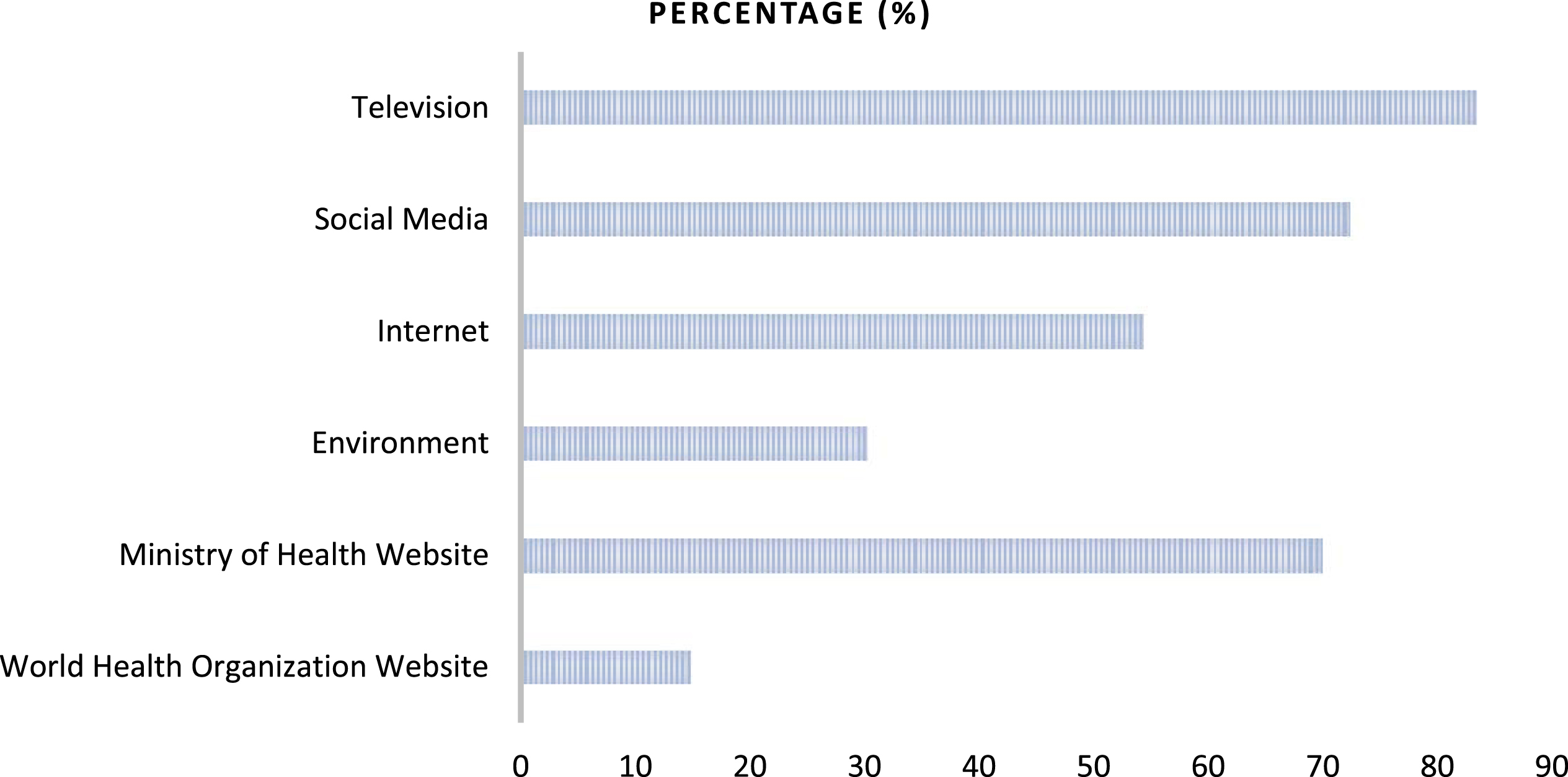
Students mostly used television as a source of information about COVID-19, followed by information from social media, the Ministry of Health website, the internet, the environment, and the World Health Organization website (Fig. 1).
Fig. 1
COVID-19 information sources of students.
Anxiety was observed in 31.5%of the students. Furthermore, 59.6%showed positive hygiene behaviors, 42.7%of the sub-dimensions of hygiene behaviors showed positive personal hygiene behaviors, 61.2%showed positive hand hygiene behaviors, and 73.7%displayed positive food hygiene behaviors (Table 4).
Table 4
Distribution of the students according to their anxiety status and total hygiene behavior and sub-dimensions of hygiene behavior
| GAD-7 scale | n | % |
| Has anxiety | 332 | 31.5 |
| No anxiety | 723 | 68.5 |
| Hygiene behavior scale and sub-dimensions | ||
| Personal hygiene | ||
| Positive hygiene behavior | 450 | 42.7 |
| Negative hygiene behavior | 605 | 57.3 |
| Hand hygiene | ||
| Positive hygiene behavior | 646 | 61.2 |
| Negative hygiene behavior | 409 | 38.8 |
| Food hygiene | ||
| Positive hygiene behavior | 778 | 73.7 |
| Negative hygiene behavior | 277 | 26.3 |
| Total hygiene behavior | ||
| Positive hygiene behavior | 629 | 59.6 |
| Negative hygiene behavior | 426 | 40.4 |
Knowledge scores of women were significantly higher than that of men, scores of the second graders were higher than that of the first graders, and scores of those who received hand hygiene training were higher than those who did not (p < 0.05). Also, a significant difference has been found in terms of the knowledge score relationship with the university where the education was provided. This difference was caused by Dicle University and Firat University and the difference between Dicle and Bingol Universities (p = 0.001). Behavioral scores of women were significantly higher than that of men (p = 0.002). The mean total generalized anxiety disorder score was 7.55±5.98, and the mean total hygiene behavior scale score was 37.57±8.98.
The total HBS score of female students was significantly lower than that of men, and the HBS scale score of students aged 20 years and less was substantially lower than that of those over 20 years. Also, the score of those who received hand hygiene education was lower than those who did not (p < 0.05). A significant difference was found regarding the total HBS score and the university where the education was provided. This difference originated between Firat University and Dicle University (p = 0.003). The total GAD-7 scale score of women was significantly higher than that of the men, while the total GAD-7 scale of students in the second grade was substantially higher than that of students in the first grade (p < 0.05). Additionally, a significant difference was found between the level of perception of the family’s economic status and the total GAD-7 scale, which was caused by the difference between those who gave their answer as ‘high’ and those as ‘medium’ (p = 0.022) (Table 5).
Table 5
Comparing students’ behavior, knowledge, and scale scores according to various variables
| Knowledge score | Behavior score | GAD-7 | HBS | |||||||
| n | Mean±SD | Test | Mean±SD | Test | Mean±SD | Test | Mean±SD | Test | ||
| Age* | 20 years and under | 574 | 5.34±1.09 | t = 0.24, p = 0.808 | 17.39±5.66 | t = 0.58, p = 0.562 | 7.81±6.11 | t = 1.55, p = 0.120 | 37.05±8.31 | t = –2.03, p = 0.042 |
| Over 20 years old | 481 | 5.33±1.11 | 17.18±6.02 | 7.23±5.81 | 38.20±9.71 | |||||
| Gender* | Female | 775 | 5.46±0.97 | t = 5.17, p < 0.001 | 17.64±5.72 | t = 3.17, p = 0.002 | 7.85±5.99 | t = 2.70, p = 0.007 | 36.45±8.50 | t = –6.88, p < 0.001 |
| Male | 280 | 5.01±1.33 | 16.35±6.02 | 6.72±5.90 | 40.68±9.58 | |||||
| Years at university* | First grade | 624 | 5.30±1.10 | t = –1.23, p = 0.044 | 17.04±6.00 | t = –1.71, p = 0.087 | 7.22±6.05 | t = –2.11, p = 0.034 | 37.18±8.54 | t = –1.72, p = 0.085 |
| Second grade | 431 | 5.39±1.09 | 17.66±5.55 | 8.02±5.86 | 38.15±9.59 | |||||
| University** | Dicle Univ. | 390 | 5.18±1.27a,b | F = 6.63, p = 0.001 | 16.84±5.89 | F = 1.89, p = 0.150 | 7.54±5.80 | F = 1.24, p = 0.287 | 38.75±10.41a | F = 5.69, p = 0.003 |
| Firat Univ. | 350 | 5.45±0.97a | 17.58±5.72 | 7.20±6.01 | 36.61±7.82a | |||||
| Bingol Univ. | 315 | 5.41±0.97b | 17.54±5.85 | 7.94±6.16 | 37.19±8.12 | |||||
| Marital status* | Married | 28 | 5.36±0.99 | t = 0.09, p = 0.923 | 16.79±6.43 | t = –0.47, p = 0.638 | 6.00±5.35 | t = –1.38, p = 0.165 | 41.21±11.58 | t = 1.69, p = 0.101 |
| Single | 1027 | 5.34±1.10 | 17.31±5.81 | 7.59±5.99 | 37.48±8.89 | |||||
| Place of residence where he/she lived longest** | City | 665 | 5.30±1.09 | F = 1.09, p = 0.335 | 17.50±5.82 | F = 1.63, p = 0.195 | 7.69±6.01 | F = 0.67, p = 0.509 | 37.55±9.34 | F = 0.12, p = 0.887 |
| District | 209 | 5.41±1.07 | 17.24±5.82 | 7.48±5.92 | 37.42±8.40 | |||||
| Rural | 181 | 5.40±1.15 | 16.62±5.84 | 7.11±5.96 | 37.85±8.33 | |||||
| Economic status of the family** | High | 58 | 5.33±1.25 | F = 0.20, p = 0.819 | 16.40±6.67 | F = 0.78, p = 0.457 | 8.97±6.32a | F = 3.81, p = 0.022 | 38.50±11.03 | F = 1.99, p = 0.137 |
| Medium | 806 | 5.35±1.07 | 17.32±5.78 | 7.28±5.85a | 37.27±8.73 | |||||
| Low | 191 | 5.29±1.16 | 17.47±5.78 | 8.26±6.33 | 38.59±9.34 | |||||
| Received infectious diseases training* | Yes | 596 | 5.38±1.04 | t = 1.35, p = 0.176 | 17.34±5.82 | t = 0.30, p = 0.764 | 7.68±6.06 | t = 0.81, p = 0.415 | 37.36±8.64 | t = –0.87, p = 0.383 |
| No | 459 | 5.29±1.16 | 17.24±5.84 | 7.38±5.88 | 37.85±9.43 | |||||
| Received hand hygiene training* | Yes | 696 | 5.39±1.01 | t = 2.18, p = 0.029 | 17.45±5.70 | t = 1.17, p = 0.240 | 7.73±6.02 | t = 1.41, p = 0.159 | 37.19±8.49 | t = –1.95, p = 0.042 |
| No | 359 | 5.23±1.24 | 17.00±6.06 | 7.19±5.89 | 38.33±9.85 | |||||
| COVID-19 positivity in relatives* | Yes | 52 | 4.94±1.59 | t = –1.86, p = 0.068 | 17.08±5.79 | t = –0.27, p = 0.780 | 8.81±6.49 | t = 1.55, p = 0.119 | 38.98±12.19 | t = 1.15, p = 0.247 |
| No | 1003 | 5.36±1.06 | 17.31±5.83 | 7.48±5.95 | 37.50±8.79 | |||||
GAD-7: Generalized Anxiety Disorder 7-item scale, HBS: Hygiene behavior scale. *Student t-test, **One-way ANOVA test. a,bEach superscript letter denotes a subset of categories whose means do not differ significantly from each other at the 0.05 level.
A positive relationship was found between mean age and total HBS scores, while a negative relationship was observed between age and GAD-7 scale scores. A significant positive correlation was found between the total HBS and GAD-7 scores and a negative correlation between total HBS scores and knowledge and behavior scores. Besides, a positive relationship was seen between the knowledge and behavior scores (Table 6).
Table 6
Correlation between scale and knowledge scores
| Age | HBS total | GAD-7 | Knowledge score | ||
| HBS total | r | 0.086 | |||
| p | 0.005 | ||||
| GAD-7 | r | –0.061 | 0.077 | ||
| p | 0.049 | 0.012 | |||
| Knowledge score | r | –0.005 | –0.273 | –0.036 | |
| p | 0.877 | 0.000 | 0.244 | ||
| Behavior score | r | 0.005 | –0.144 | 0.036 | 0.166 |
| p | 0.874 | < 0.001 | 0.247 | < 0.001 |
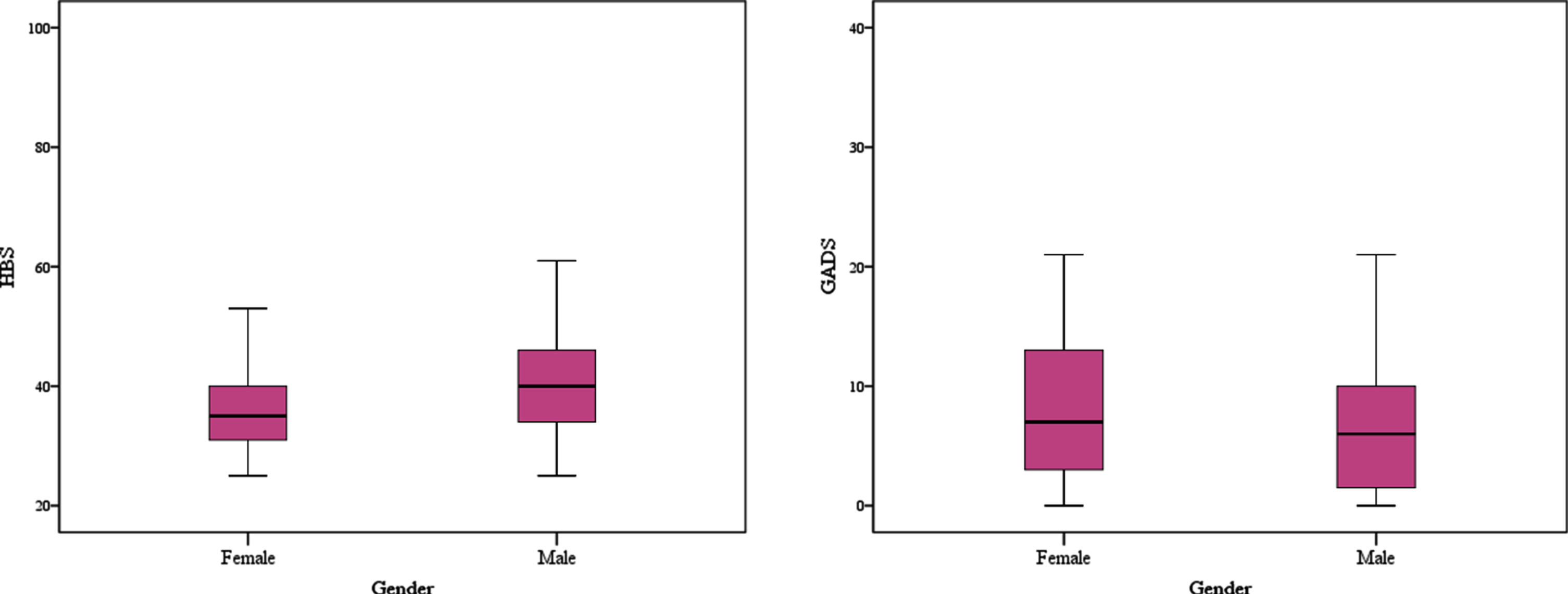
The distribution of students’ HBS and GAD-7 scores by gender is indicated in Fig. 2.
Fig. 2
The distribution of HBS and GAD-7 scores by gender.
4Discussion
There was a difference in the knowledge, anxiety, and hygiene behaviors about COVID-19 among the participating students. Hence, the H0 hypothesis was rejected, and the H1 hypothesis was accepted. Contrary to our expectations, the knowledge and behavior change scores of the students about COVID-19 were high. It was revealed that the disease causes anxiety in students. It has been demonstrated that more than half of the students also showed positive hygiene behaviors in the face of this situation.
The mean knowledge score of the students was 5.34±1.09 from a maximum of six points. Our results showed high knowledge levels and positive behaviors against the COVID-19 outbreak among the students. It has been reported that Iranian medical students had a high level of relevant knowledge and high performance in COVID-19 preventive behaviors [19]. It is important to have a good knowledge of the COVID-19 clinical picture, recognize the disease, and obtain appropriate measurements to save lives. Among students’ responses to behavioral questions related to COVID-19, the behaviors of avoiding people with disease symptoms and avoiding handshake had changed the most. Students’ taking the subject seriously as a vulnerable group had an impact on their behavioral practices. It is essential to follow preventive measures, including handwashing, as well as avoiding handshaking and sneezing to prevent infection [13].
For proper information management, disease control authorities should develop effective channels to receive and share disease-related information. Our study determined that students preferred television in the first place, social media in the second place, and the Ministry of Health website in the third place to obtain information about COVID-19. Similar to our findings, it was reported that the participants generally received information about infectious diseases from television and the internet [13, 20]. In Turkey, the Ministry of Health strives to educate people about COVID-19 on television and social media through scientists.
Anxiety was found in approximately one-third of the students. In China, 24.9%of university students experienced anxiety due to the COVID-19 outbreak, 0.9%had severe anxiety, and 21.3%had mild anxiety [6]. In a similar study conducted in Bangladesh, it was stated that 87.7%of the students had mild to severe anxiety symptoms [7]. While there were regional differences in anxiety rates, students not knowing the effects of the virus and being at risk of infectious diseases may have an increase in anxiety.
According to the total hygiene behavior of the students, the rate of showing positive hygiene behavior was determined as 59.6%. Of the university students in China, 84.04%think that they comply with their personal hygiene behaviors and believe that they contribute to the government’s health policies [21]. Numerous reports from different countries have shown that the hand hygiene compliance rate was estimated at around 40%, while the compliance rate in critical care units was only 46.25%[22, 23]. The current pandemic has made handwashing a focus of attention. Now we have to keep this focus going.
Both the knowledge and behavioral change scores of women about COVID-19 were significantly higher than that of men. In a study on the SARS outbreak in Hong Kong by Leung et al., it was reported that men are less likely to engage in self-defense behaviors than women [24]. Zandian et al. mentioned in their study with university students that the knowledge of women was higher than that of men [25]. Women demonstrated good practices in general attitudes and behavior towards disease prevention measures and responses in the event of infection. The more sensitive character of women also manifests itself in pandemics that may be associated with COVID-19. The knowledge score of second graders was significantly higher than the score of first graders (p < 0.05). In the study conducted by Peng et al. with undergraduate students, it was observed that the COVID-19 knowledge was better in women and individuals in higher grades [26]. In a study conducted in Jordan, postgraduate students had significantly higher knowledge scores compared to undergraduate ones [27]. In line with the literature, our findings showed that the higher the education level, the higher the knowledge scores.
In our study, the total score of women on the GAD-7 scale was significantly higher than that of men (p < 0.05). Similar to our findings, female students were shown to have more fear and anxiety about the disease [28, 29]. Wang et al. reported that the COVID-19 outbreak had a greater psychological effect on women and had higher levels of stress, anxiety, and depression [5]. Biological gender differences, culture, diet, hormonal changes, and educational status of women were some factors contributing to higher anxiety and depression rates [30]. Outbreaks were expected to cause anxiety in individuals. It is stated that students working in the emergency unit may be affected by many psychological conditions that can be expressed as fear and anxiety [31]. It was important to know the factors related to anxiety and help people by intervening and reducing their anxiety levels. Anxiety levels also increased in those who perceived the family’s economic status as high. Liu et al. stated that increasing psychological and financial pressure due to stagnation in family income during the COVID-19 crisis was an important factor in students’ anxiety [32]. Because of the pandemic, some families will lose their income sources, so students may get worried about paying tuition fees [33]. While COVID-19 causes fear and anxiety over the academic achievement of university students, it can negatively affect their education by causing students to avoid their learning activities and by reducing their concentration.
The total HBS score of female students was significantly lower than that of men, and the HBS scale score of students aged 20 years and under was markedly lower than that of those who were over 20 years old, and the HBS score of those who did receive hand hygiene education was lower than that of those who did not (p < 0.05). This indicated positive hygiene behavior. In a study conducted among students studying in medical and non-medical departments in the United Arab Emirates, it was reported that most of the students had an increase in hand hygiene (85%) and the use of hand sanitizer (85.5%) and that medical students performed better hand hygiene practices [34]. In the research conducted by Kwok et al. in Hong Kong, the most effective method of preventing the COVID-19 epidemic was seen as increasing personal hygiene practices [35]. In another study, although personal hygiene was emphasized very much, it was reported that there was a small proportion (14.89%) of students who perceived not paying more attention to personal hygiene than before [21]. For the current COVID-19 outbreak, training and information were provided on hygiene behaviors for both health care professionals and the public. Health care professionals must follow the 5 recommendations made by WHO for hand hygiene: They must wash their hands before touching a patient, before clean or aseptic procedures, after exposure to body fluids, after touching a patient, or touching the patient’s environment [36].
In our study, a significant negative correlation was found between the total HBS score and the knowledge and behavior scores. This showed that as the knowledge score increases, there was an increase in positive hygiene behaviors. In a study conducted in Nigeria, higher COVID-19 knowledge was associated with higher precautionary behaviors (handwashing habits, social distance, etc.) [37]. From this perspective, our findings were compatible with the literature.
4.1Limitations
Since this was a cross-sectional study, a causal relationship could not be established between dependent and independent variables. Although the survey was multi-centered, the fact that it does not cover all health services vocational schools in Turkey could be considered another limitation.
5Conclusions
In conclusion, students’ knowledge and behavior change scores regarding COVID-19 were high. Approximately one-third of the students had anxiety, and more than half showed positive hygiene behaviors. Women’s knowledge and behavior scores were higher, and they were more sensitive about their hygiene behaviors and anxiety perceptions. In line with these results, psychological support programs can be created for health care students during the infectious disease outbreak. In these challenging times, students will also be able to exercise at home, work at home, read books, listen to music, etc. They can manage their own psychological processes with these activities and by communicating with their friends and family. In addition, training should be carried out on this subject by paying more attention to positive hygiene behaviors.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
References
[1] | World Health Organization (WHO) Director-General&s opening remarks at the media briefing on COVID-19- 11 March 2020. Available from:https://www.who.int/dg/speeches/detail/who-directorgeneral-s-opening-remarks-at-the-media-briefing-oncovid-19—11-/ |
[2] | World Health Organization (WHO), Coronavirus. 2020. Available from: https://www.who.int/healthtopics/coronavirus/ |
[3] | Langade D , Modi PD , Sidhwa YF , Hishikar NA , Gharpure AS , Wankhade K , et al. Burnout syndrome among medical practitioners across India: a questionnaire-based survey. Cureus. (2016) ;8: (9):771. |
[4] | International Standard Industrial Classification of All Economic Activities. United Nations; 2002. Available from:https://unstats.un.org/unsd/publication/seriesM/seriesm_4rev4e.pdf/ |
[5] | Wang C , Pan R , Wan X , Tan Y , Xu L , Ho CS , et al. Immediate psychological responses and associated factors during the initial stage of the coronavirus disease (COVID-19) epidemic among the general population in China. International Journal of Environmental Research and Public Health. (2020) ;17: (5):1729. |
[6] | Cao W , Fang Z , Hou G , Han M , Xu X , Dong J , et al. The psychologicalimpact of the COVID-19 epidemic on college students in China. Psychiatry Research. (2020) ;(287):112934. |
[7] | Islam MA , Barna SD , Raihan H , Khan MNA , Hossain MT . Depression and anxiety among university students during the COVID-19 pandemic in Bangladesh: A web-based cross-sectional survey. PloS one. (2020) ;15: (8). |
[8] | Dokuzoguz B . Hand hygiene. Microbiology –Infection Journal. (2003) ;2: (2). |
[9] | Arefi MF , Poursadeqiyan M . A review of studies on the epidemic crisis of COVID-19 diseasewith a preventive approach. Work. 2020;717–729. |
[10] | World Health Organization (WHO), Coronavirus disease (COVID-19). Available from: https://www.who.int/news-room/q-a-detail/coronavirus-disease-covid-19/. |
[11] | Republic ofTurkey Ministry of Health,COVID-19 Information Page.Available from: https://covid19.saglik.gov.tr/TR-66125/sikca-sorulan-sorular-halka-yonelik.html. |
[12] | Maheshwari S , Gupta PK , Sinha R , Rawat P . Knowledge, attitude, andpractice towards coronavirus disease (COVID-19) among medicalstudents: a cross-sectional study. Journal of Acute Disease. (2020) ;9: (3):100. |
[13] | Alzoubi H , Alnawaiseh N , Al-Mnayyis A , Abu-Lubada M , Aqel A , Al-Shagahin H . COVID-19 - Knowledge, Attitude and Practice among Medical and Non-Medical University Students in Jordan. J Pure Appl Microbiol. (2020) ;14: (1):17–24. |
[14] | Spitzer RL , Kroenke K , Williams JB , Löwe B . A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) ;166: :1092–97. |
[15] | Konkan R , Senormancı O , Guclu O , Aydın E , Sungur MZ . Validityand reliability study for the Turkish adaptation of the GeneralizedAnxiety Disorder-7 (GAD-7) scale. Archives of Neuropsychiatry. (2013) ;50: :53–8. |
[16] | Löwe B , Decker O , Müller S , Brähler E , Schellberg D , Herzog W , et al. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med Care. (2008) ;46: :266–74. |
[17] | Dear BF , Titov N , Sunderland M , McMillan D , Anderson T , Lorian C , et al. Psychometric Comparison of the Generalized Anxiety Disorder Scale-7 and the Penn State Worry Questionnaire for Measuring Response during Treatment of Generalised Anxiety Disorder. Cogn Behav Ther. (2011) ;40: :216–27. |
[18] | Coban GI , Bilgin S . Development of the scale of hygiene behaviors for nursing students. BMC Medical Research Methodology. (2015) ;15: (69):2–6. |
[19] | Taghrir MH , Borazjani R , Shiraly R . COVID-19 and Iranian medical students; a survey on their related-knowledge. Preventive Behaviors and Risk Perception. Archives of Iranian Medicine. (2020) ;23: (4):249–54. |
[20] | Tork HM , Mersal FA . Middle East Respiratory Syndrome-Corona virus: Knowledge and attitude of Qassim University students. KSA. Global Adv Res J Med Med Sci. (2018) ;7: (4):90–7. |
[21] | Haimin P . A glimpse of university students’ family life amidst the COVID-19 virus. Journal of Loss and Trauma. 2020;1–4. |
[22] | Erasmus V , Daha TJ , Brug H , Richardus JH , Behrendt MD , Vos MC , et al. Systematic review of studies on compliance with hand hygiene guidelines in hospital care. Infection Control & Hospital Epidemiology. (2010) ;31: :283–94. |
[23] | Bezerra TB , Valim MD , Bortolini J , Ribeiro RP , Marcon SR , Moura MEB . Adherence to hand hygiene in critical sectors: Can we go on like this?. Journal of Clinical Nursing. 2020. |
[24] | Leung GM , Ho LM , Chan SK , Ho SY , Bacon-Shone J , Choy RY , et. al. Longitudinal assessment of community psycho behavioral responses during and after the 2003 outbreak of Severe Acute Respiratory Syndrome in Hong Kong. Clinical Infectious Diseases. (2005) ;40: (12):1713–20. |
[25] | Zandian H , Sarailoo M , Dargahi S , Gholizadeh H , Vosoughi M , Dargahi A . Evaluation of knowledge and health behavior of university of medical sciences students about the prevention of COVID-19. Work. 2021;1–7. |
[26] | Peng Y , Pei C , Zheng Y , Wang J , Zhang K , Zheng Z , et al. A cross-sectional survey of knowledge, attitude and practice associated with COVID-19 among undergraduate students in China. BMC Public Health. (2020) ;20: (1):1–8. |
[27] | Olaimat AN , Aolymat I , Shahbaz HM , Holley RA . Knowledge and information sources about COVID-19 among university students in Jordan: a cross-sectional study. Frontiers in Public Health. (2020) ;8: :254. |
[28] | Liu X , Liu J , Zhong X . Psychological State of College Students During COVID-19 Epidemic. The Lancet Global Health. 2020. |
[29] | Al-Rabiaah A , Temsah MH , Al-Eyadhy , Hasan GM , Al-Zamil F , Al-Subaie S , et al. Middle East Respiratory Syndrome-Corona Virus (MERS-CoV) associated stress among medical students at a university teaching hospital in Saudi Arabia. J Infect Public Health. (2020) ;13: (5):687–91. |
[30] | Albert PR . Why is depression more prevalent in women? Journal of Psychiatry & Neuroscience. (2015) ;40: (4):219–21. |
[31] | Mei SL , Yu JX , He BW , Li JY . Psychological investigation of university students in a university in Jilin province. Med Soc (Berkeley). (2011) ;24: (05):84–6. |
[32] | Liu ZF . A Study On the Relationship Between Adverse Family Experiences in Childhood and Emotional and Anxiety Disorders. Dalian medical university. (2013) . |
[33] | Peng L , Zhang J , Li M , Li P , Zhang Y , Zuo X , et al. Negative life events and mental health of Chinese medical students: the effect of resilience, personality and social support. Psychiatry Res. (2012) ;196: (1):138–41. |
[34] | Saddik B , Hussein A , Sharif-Askari FS , Kheder W , Temsah MH , Koutaich RA , et al. Increased levels of anxiety among medical and non-medical university students during the COVID-19 pandemic in the United Arab Emirates. Risk Management and Health care Policy. (2020) ;13: :2395. |
[35] | Kwok KO , Li KK , Chan HHH , Yi YY , Tang A , Wei WI , et al. Community responses during the early phase of the COVID-19 epidemic in Hong Kong. Emerg Infect Dis. (2020) ;16;26: (7). |
[36] | World Health Organization. Guidelines on hand hygiene in health care. First global patient safety challenge clean care is safer care. Available from:https://apps.who.int/iris/bitstream/handle/5/2/6_eng.pdf?sequence=1./ |
[37] | Iorfa SK , Ottu IF , Oguntayo R , Ayandele O , Kolawole SO , Gandi JC , et al. COVID-19 Knowledge, Risk Perception, and Precautionary Behavior Among Nigerians: A Moderated Mediation Approach. Frontiers in Psychology. (2020) ;11: . |


