
An intervention of occupational therapy in parasports using the matching person and technology model: A case study
Abstract
BACKGROUND:
The practice of occupational therapy in parasports aims to improve participation in sports as an occupation, reducing barriers stemming from the environmental factors.
OBJECTIVE:
To analyze the process of choice, prescription and follow-up of assistive technology (AT) in competitive adolescent parasports using the theoretical model Matching Person and Technology.
METHODS:
Case study with 3 adolescents from 12 to 18 years old in Bocce and Para-badminton modalities was performed. Characterization Questionnaire; Quebec User Evaluation of Satisfaction with assistive Technology (B-Quest); Assistive Technology Device - Predisposition Assessment (ATD PA-Br); Brazil Criteria and Intervention Report were used.
RESULTS:
Level of income was intermediate and low. The AT used were handcrafted by family and coaches. The Psychosocial factors detected were low privacy, autonomy, discomfort and device appearance. Pre-intervention there was dissatisfaction with AT related to the device and the context. Post-intervention, satisfaction scores increased.
CONCLUSIONS:
The model was a positive guide regarding the intervention of technology in the parasport, directing the participation of the specialist with the parathletes, their family and coaches, in the continuous monitoring of its use. This was key for the satisfaction in using the AT in sports, besides contributing to their occupational performance and maintaining people with disability in parasports, increasing the possibility of adolescents becoming professional para-athletes. Further studies in this area are suggested.
1Introduction
Developing the abilities of children and adolescents with disabilities is crucial for a high quality of life and social interaction [1].
Disability has been defined as functional or structural impairment of the body, resulting from the relationship between the individual and the environment, and evidenced by the limitations in participation and functions [2, 3].
Data from the World Health Organization, United Nations and UNICEF show that one in 10 children have a disability and about 10% of the world’s population live with some type of disability. This number is increasing due to population growth, advances in medicine, and the aging process. It has also been reported that 80% of people with disabilities live in developing countries, according to the United Nations Development Program (PNUD) [3, 4].
Accompanying the growth in population, the demand for various activities, among them sports, has grown accordingly. Often initiated in the early phases of physical rehabilitation, sports have become highly preferable to those with physical disabilities, providing sensations and movements that are unusual due to the limitations of their physical condition [5]. Thus, it was suggested that the potentials of children and adolescents with disabilities should be supported to improve social inclusion in adult life and to reduce the paradigm that focuses first on a disability rather than on the person [1].
Physical rehabilitation tailored to sports began after World War II with the need to rehabilitate war veterans in England. [5]. The adapted sport was focused on human development and its adaptive capacities involving functional, physical, psychic, educational, social and professional aspects. Focusing on the physical aspect, the goal was to increase participation in social settings and independence in daily living activities [6]. The pioneering sport in the area of rehabilitation in 1957 was wheelchair basketball, which fostered social integration and independence in meaningful activities [5].
This process resulted in adaptive sports, also known as disability sports or parasports, which aimed to introduce people with physical disabilities into the world of sports by adapting them to promote social inclusion and personal growth [7]. By surpassing its initial role of rehabilitation, sports have become a factor of improvement in the lives of athletes and their families. Sports can also lead them to a transition, from an informal sports situation to a formal sports (professional) situation, where they need to commit to competitive activities, thus reaping personal benefits and improving skills [8].
Paralympic sports, according to the Brazilian Paralympic Committee, came from the Greek word “para” which means “side, parallel”, and the word “Olympic”. It emerged after World War II when it was used in England as a rehabilitator of war veterans with spinal cord injury. Shaped upon the Olympic Games, the Paralympic Games were created to meet the needs of people with disabilities and thus became a high-performance event in the world [7].
Researchers pointed out that sports can result in significant improvements in the abilities of children and adolescents with cerebral palsy, for example, including benefits to their biopsychosocial profiles [9].
In this way, sports for the disabled also began to play a significant role beyond rehabilitation, namely in work and leisure.
The Model of Human Occupation comprises the contextual interaction between the occupations of individuals and their environments under conditions of occupational apartheid: a concept that involves the restriction of engagement in occupations due to social injustice. Thus, it can be considered that adolescents with disabilities in developing countries may be deprived of their occupations (sports and leisure) and the possibility of engagement and training to pursue a future profession, in this case, parasports [10].
However, for the process of inclusion of disabled persons into sports to occur, it is necessary to take into account the particularities of each sport, taking into account the principle use of the functional classification, since each athlete will present different functional potentials [11].
In the political arena, especially in developing countries, assistive technology (AT) has gained some ground through collective actions that guarantee that disabled persons have access to an AT that favors autonomy, mobility, and quality of life. Regarding labor laws, disabled persons have been guaranteed their freedom of choice in an accessible environment and the participation and accessibility of leisure for people with disabilities [12].
However, researchers have affirmed that little is known about the effects of assistive technology on the physically disabled population compared to the size of the intervention possibilities that are available [13].
Different professionals have contributed to the placement of people with disabilities into sports as rehabilitation, work or leisure. Therefore, the practice of occupational therapy in sports and parasports involves methods of intervention, prevention, promotion, protection and education with the aim to improve the occupation of sports as a profession as well as athletic performance. Recently, sports have come to represent the work of people with disabilities, and thus an occupational therapist could also perform interventions in relation to the barriers stemming from environmental factors [8, 10, 14].
Thus, professionals that perform follow-up visits with a para-athlete should seek to understand the games and its rules, while carefully considering the opinion and interest of the para-athlete and their need to use the AT within the context and rules of the sport.
Considering the prescription and use of AT in sports, the method of evaluation becomes paramount. Each AT device must be comfortably adapted to the individuals’ needs and their sporting modality, because even with similar rules and identical diagnoses, the needs of each para-athlete may differ in relation to AT use.
This discussion presupposes that adolescents with disabilities could be involved in competitive parasports as engagement in an occupation and, furthermore, that engagement in parasports could lead to a job in future. For this to happen, it is believed that the use of AT could enhance these possibilities.
Therefore, this research aimed to present the process of prescription, choice and follow-up of AT in competitive sports as practiced by adolescents with disabilities using a theoretical model of AT validated in the literature. As specific objectives, this article intends to characterize the practice of sports, the adolescent para-athlete who practices the sport, and their AT.
2Methods
This descriptive case-intervention study aimed to perform participatory research [16]. In this type of research, there is the interaction between the researchers and the participants, working to clarify the main collective problems in order to provide solutions. This research used the quantitative approach [17] and follow-up with the cooperation and participation of the researcher with the participants [16].
The research was conducted at the Special Physical Education Training Center (CETEFE). Since 1990, CETEFE has been a non-profit social assistance association and a national benchmark located in Brazil’s capital. It provides free services for people with disabilities and their families at social, public and private institutions. It covers social programs including sports activity, where participants arrive by walk-ins or referrals. It has about 270 people registered with disabilities and offers 12 sport and Paralympic modalities such as: wheelchair tennis, sitting volleyball, wheelchair rugby, archery, weightlifting, bocce ball, swimming, wheelchair basketball, para-badminton, athletics, para-canoeing (adapted sail), goalball and 7-a-side soccer [17]. For the choice of participants, the criteria used were adolescents with a physical disability, ages 12 to 18 years old, involved in competition, who did not initiate any intervention during the research, had regular attendance in training and during the intervention period and had authorization from their guardian. All sport modalities were visited by the researchers and all athletes were invited. Considering the collection period from October to November 2017, the final sample size included three adolescents playing competition games in school sports. The adults responsible for the adolescents were invited to be present in case the athletes needed their help in responding to the instruments and to the interventions.
It was later established as inclusion criteria that the athletes were registered at CETEFE, regularly attending the training sessions, and competing in school sports. Adolescents who did not use AT devices were excluded.
2.1Instruments
Three evaluation instruments were applied, which were directed to the adolescents themselves or their responsible adults when necessary. Prior to the implementation of the instruments, the team clarified those terms that the participants found difficult to understand.
2.1.1Questionnaire characterizing adolescents practicing sports and their family context
The main objective was identifying the age and diagnosis of the para-athlete, the sports practiced, the AT device necessary for practice in the sport, the device used by the adolescent as well as the access and acquisition of the device.
2.1.2Quebec User Evaluation of Satisfaction with assistive Technology (B-Quest) [19]
This was used to investigate the level of satisfaction the para-athlete had in relation to the assistive technology device and the services provided. The questionnaire consists of 12 satisfaction items which are scored on the scale of 1 to 5 (1 for dissatisfied and 5 for completely satisfied). The psychometric properties were tested to assure the validity of items and the reliability and stability of the scale for use in Brazil [19]. At the end, each participant was asked to choose 3 of the 12 items that were considered most important, using the sum of the answers divided by the number of items to obtain the result.
2.1.3Assistive Technology Devise Predisposition Assessment (ATD PA-Br) [20, 21]
This was applied for investigation into personal factors (section C), and for investigation into facilitators and barriers arising from the environment surrounding the physically handicapped. This questionnaire is divided into topics from A to D, where: A contains items 1 through 9, scored 1 for “bad” and 5 for “excellent” regarding the participant’s abilities; B contains items 10 through 21, scored 1 for “not satisfied” and 5 for “very satisfied”, in relation to their level of satisfaction in general areas; C contains items 22 through 54, scored “frequently” or “often”, related to questions that apply to psychosocial factors. The evaluation form also has a section examining the expectations regarding the use of the AT device in daily situations, scored on a scale of 1–5, where 1 is “never” and 5 is “all the time”, for items A to L, prioritizing at the end those 3 items that participants considered most important to them. The psychometric properties were tested to assure the validity of items and the reliability and stability of the scale for use in Brazil [20, 21].
2.1.4Application of the Brazilian criteria [22]
This aimed to classify the socioeconomic conditions of the adolescents’ families. The assessment is divided into two parts where the first evaluates the possession of consumer items in the residence and the second solicits the highest level of education achieved by the head of the family. A score is given for the quantity of items. According to the sum of points, the family income is classified as A1, A2, B1, B2, C1, C2, D or E, where A1 is the highest socioeconomic group and E is the lowest.
2.1.5Report for follow-up of the intervention
The researchers designed this instrument based on the theoretical model called Matching Person and Technology (MPT). Its accompanying assessment process includes forms for different types of technology (assistive, educational, workplace and health care). The assistive technology form was used in this study. The model states that three areas should be investigated and followed-up, referring to the process of recommending and using the device. The psychosocial factors that are related to the personal and social factors of the person involving the use of AT as social support, self-image and coping; the factors of the device, related to the dimensions of the device such as size and weight; and the context of the AT user which is related to the interrelations of situations centered on the person and the use of AT [21]. This instrument was answered by the adolescent, or through the tutor when necessary. It was used in the interventions and monitoring of the use of AT, considering questions that favor and disfavor the use of AT by adolescents. The report followed the premises of the MPT and contained questions that included: participation in choice of AT, weight, pain, size, adjustments, motivation for AT use, appearance of AT, independence with device use, discomfort, usefulness in sports, family, friends and coach support. It uses qualifiers such as: “good, fair and poor” and possible comments that the participants may want to add.
2.2Selection of participants
In order to select the participants, a survey of po-tential participants was initially performed using the general register and the coordinator of CETEFE. According to data from CETEFE, among the total number of people with disabilities, 22 adolescents aged 12 to 18 years were registered in the competition modalities. Among the 22 high-performing adolescents, 14 were either contacted during practice or by telephone during data collection, and of these 14 adolescents, 3 fulfilled the inclusion criteria.
Some of the difficulties encountered by the res-earchers in the recruitment of the participants were: outdated contact information, withdrawal and lack of training during the collection period, undefined training schedules and the fact that most of the registered adolescents were out of town for competitions. Even the research participants presented difficulties attending the research sessions, which were postponed a few times due to health or other reasons.
2.3Data collection
At the beginning of the data collection, the res-earchers sought knowledge on these parasports by participating in the context of each adolescent through visits to training sessions and consultations with the Paralympic Committee. Training session visits were performed to create a relaxed atmosphere between researchers and athletes (regardless of whether or not they participated in the research), to avoid any potential discomfort felt by athletes in future training sessions, and in order to understand the dynamics of each sport and the device needs of athletes in each modality. Later, the researchers performed the selection and invitation of athletes.
Firstly, the adolescents and responsible adults at the training sessions were invited to participate in the research, and the collection procedures were explained. All those in charge were present and received the consent form so that they could understand and authorize the participation of the adolescents.
For those who agreed to participate, evaluations and interventions were scheduled on days and times adjacent to their sports training sessions, or on other days and times that were suitable for the participants.
Regarding the interventions, due to the difficulties of some adolescents and adults responsible for them in attending the meetings, some planning and choices of materials were conducted either by phone or messaging applications in accordance with their initiative.
The intervention was divided into 3 sessions. For the first session, follow-up was performed by the researcher during the sports training session to understand the demands by the para-athletes; an evaluation with the instruments, and prescription and planning of the AT were performed by the researchers. For the second session, assembly of the assistive technology (if necessary) was performed and device adjustments were made together with the adolescents, families and coaches; Initial tests at sports training sessions and completion of the follow-up report was performed alongside participants. For the third session, device adjustments were performed jointly with the adolescents, families and coaches. Testing was conducted during the sports training session with participants and revaluation with the instruments was performed.
A group of undergraduate and postgraduate student researchers from the occupational therapy course at CETEFE performed the longitudinal follow-up.
Data analysis procedures and ethical procedures
The quantitative data were treated by descriptive statistical analysis by frequency and percentages [23] and presented in tables.
This research is part of the study “Health Status and Risk of Injury in Parasports”. The project was approved by the Research Ethics Committee of the Faculty of Health of the University of Brazil, under recommendation no. 1.713.534.
This project is in accordance with the resolution 466/2012, referring to ethics in research with human beings, submitted to and accepted by the committee.
3Results
Of the 3 evaluated participants, all had their tutors accompanying the evaluations and interventions, assisting the adolescents in the responses, in the development of AT or offering information on allergies to materials or previous failed attempts of equipment.
The findings of this study are presented below.
As can be observed in Fig. 1, P1 played bocce ball for more than 7 months with a BC3 classification. In this classification, according to the Brazilian Paralympic Committee (CPB), the athlete can use auxiliary instruments and receive help from third parties because of severe disability. In this instance, the athlete makes use of a headband to replace the function of hands to throw the balls on the court. However, for P1 the device was customized by the family with a cycling helmet, padded with rubberized paper and a bathroom towel rod, which fell over the eyes of the para-athlete during the game. Additionally, the towel rod rotated, making plays more difficult in higher moves.
Fig. 1
Characterization of juvenile parathletes. 1Brazil Criterion Instrument.
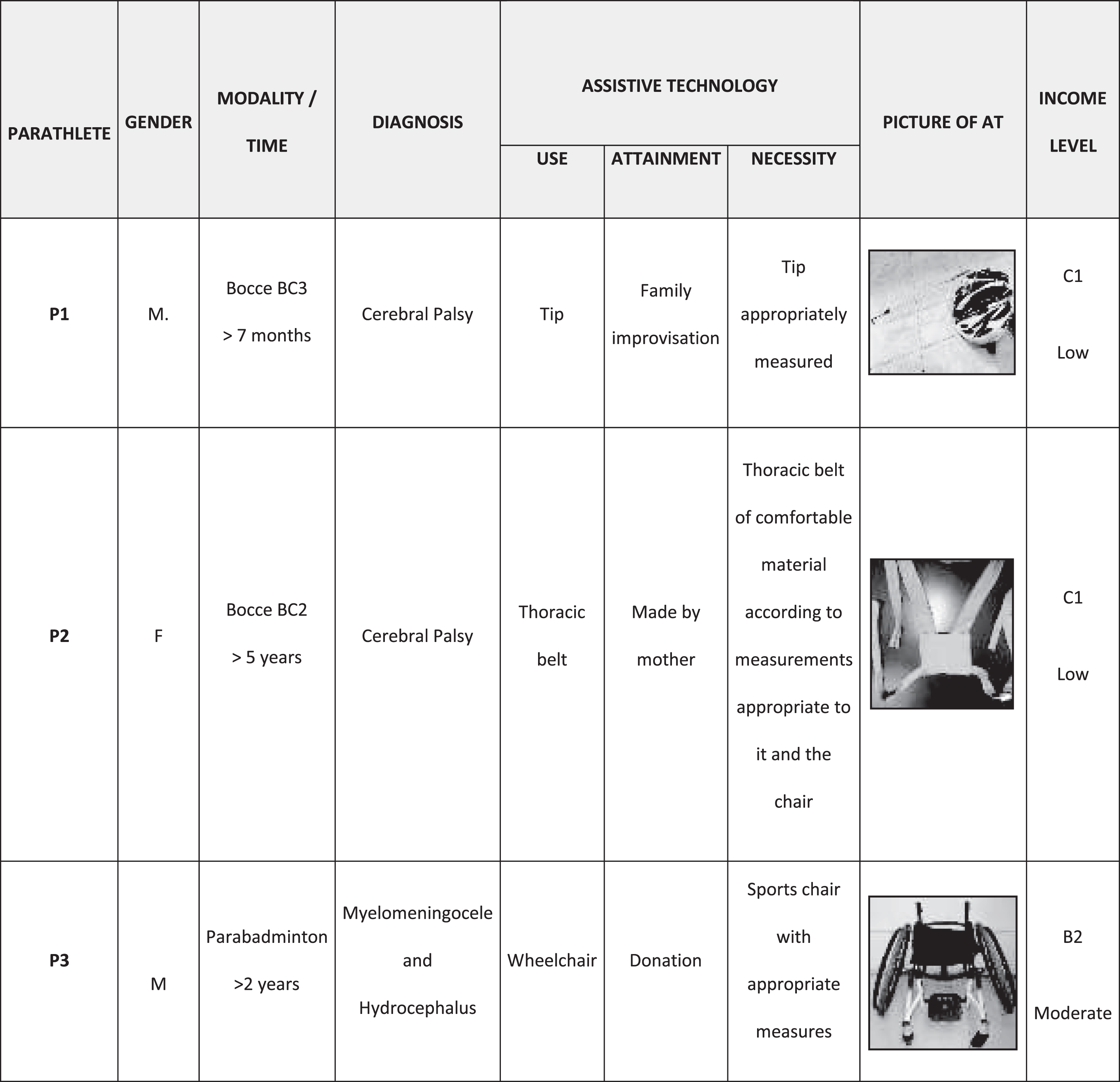
P2 has been playing bocce ball for over 5 years in the BC2 classification. According to CPB, the athlete cannot receive assistance during the game in this classification. P2 makes use of a thoracic belt due to the gradual forward displacement of her trunk in response to the force of throwing of the ball, and the difficulty that P2 experiences with keeping her trunk erect, as it should be during the game. P2’s mother made a belt that ties her to an iron barrel located at the back of the chair, but the belt’s knot gradually loosens itself during training due to the teenager’s power while performing moves, and the belt consequently places a lot of pressure on the shoulders and the adolescent’s breasts.
P3 practiced the modality para-badminton for more than 2 years and utilized a daily use chair with adaptations. However, the chair hinders the performance in sports because it is heavy and has small wheels. P3 received a sports wheelchair that was unsuitable for her anatomy, as it needed adjustments to the seat, backrest and chest belt.
In relation to public policies, only P1 received financial aid that is used in support of the sport, the so-called Continuous Stipend Benefit (BPC), and only two of them knew of a free AT distributor (the Sarah Hospital in Brazil).
Researchers noted that the use of AT devices was infrequent. Among those evaluated, all used more than two AT devices, excluding those that were produced in this study. All of them reported that they did not know about AT public service delivery, as their AT devices were improvised by users or received from donations.
Regarding the evaluation data from this study, Table 1 (below) shows the results of the evaluation Quest (2.0) in relation to satisfaction with the assistive technology device. A maximum score of 5 points is given when the user is considered totally satisfied.
Table 1
Satisfaction with device/service used before intervention
| Parathlete | Satisfaction 0-5 | |||||
| Before intervention | After intervention | |||||
| Device | Service | Total | Device | Service | Total | |
| P1 | 4,12 | 4,75 | 4,33 | 5 | 5 | 5 |
| P2 | 4,5 | 3,5 | 4,16 | 4,87 | 4,5 | 4,75 |
| P3 | 4,12 | 3 | 3,37 | 4,87 | 4,75 | 4,83 |
According to Quest (2.0), on average, adolescent satisfaction with AT scored a high, satisfactory score, but most of the athletes scored the lowest level of satisfaction in servicing AT. When the intervention report was applied, in which the adolescents judge their AT according to the demands observed in the first session, they pointed out questions that act as factors for dissatisfaction and abandonment of AT, (Fig. 3).
Fig. 3
Assessment of AT aspects throughout interventions.
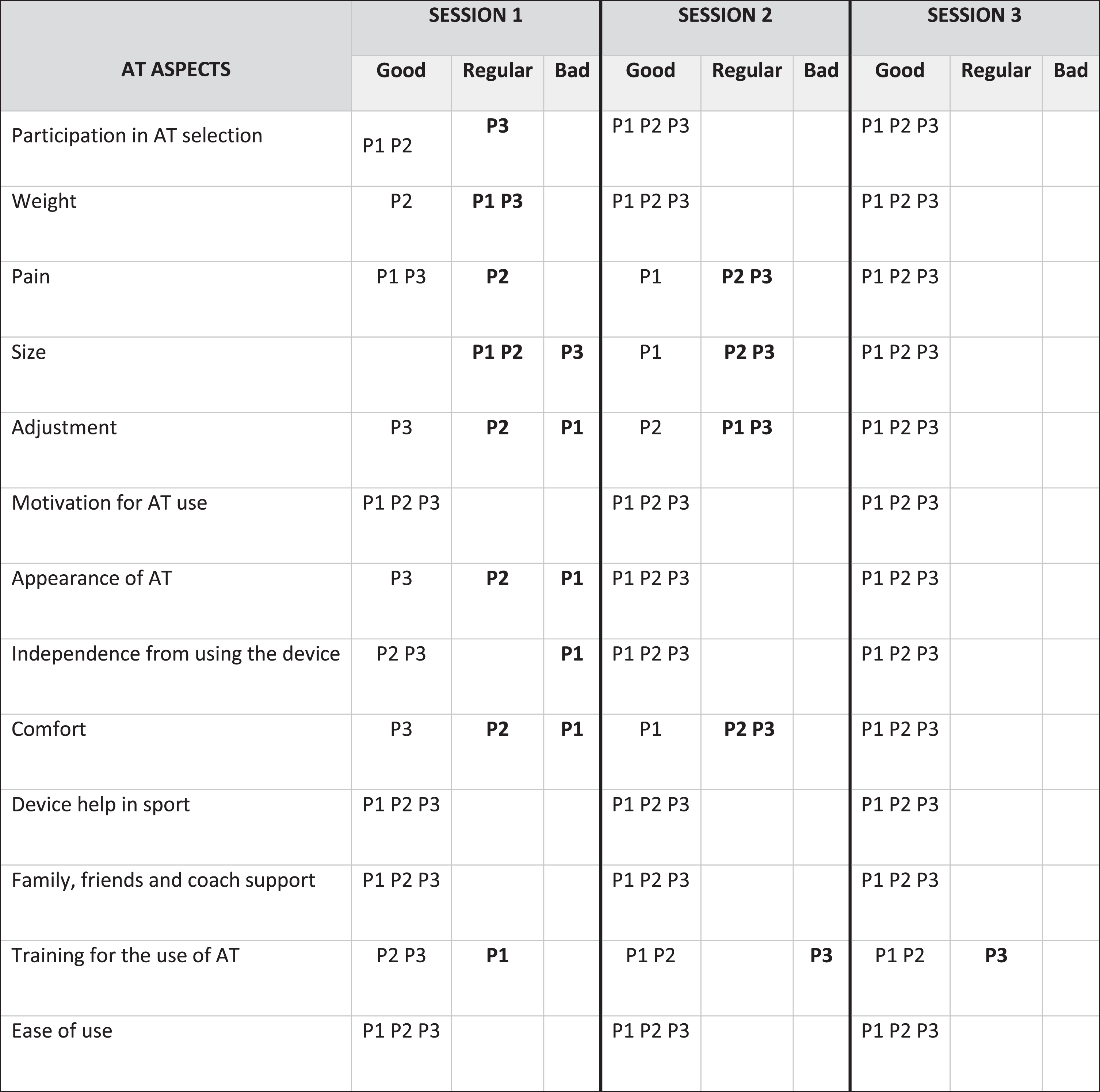
Figure 2 shows the results of the ATD PA-BR evaluation regarding satisfaction with daily items and personal factors. We used the B and C sections of the evaluation form, in which the most cited satisfaction was presented in the first columns, with a maximum score of 5 (totally satisfied), and in the last columns, the most cited points as positive or negative by adolescents.
Fig. 2
Satisfaction with day-to-day aspects and personal factors (ATD PA-Br).
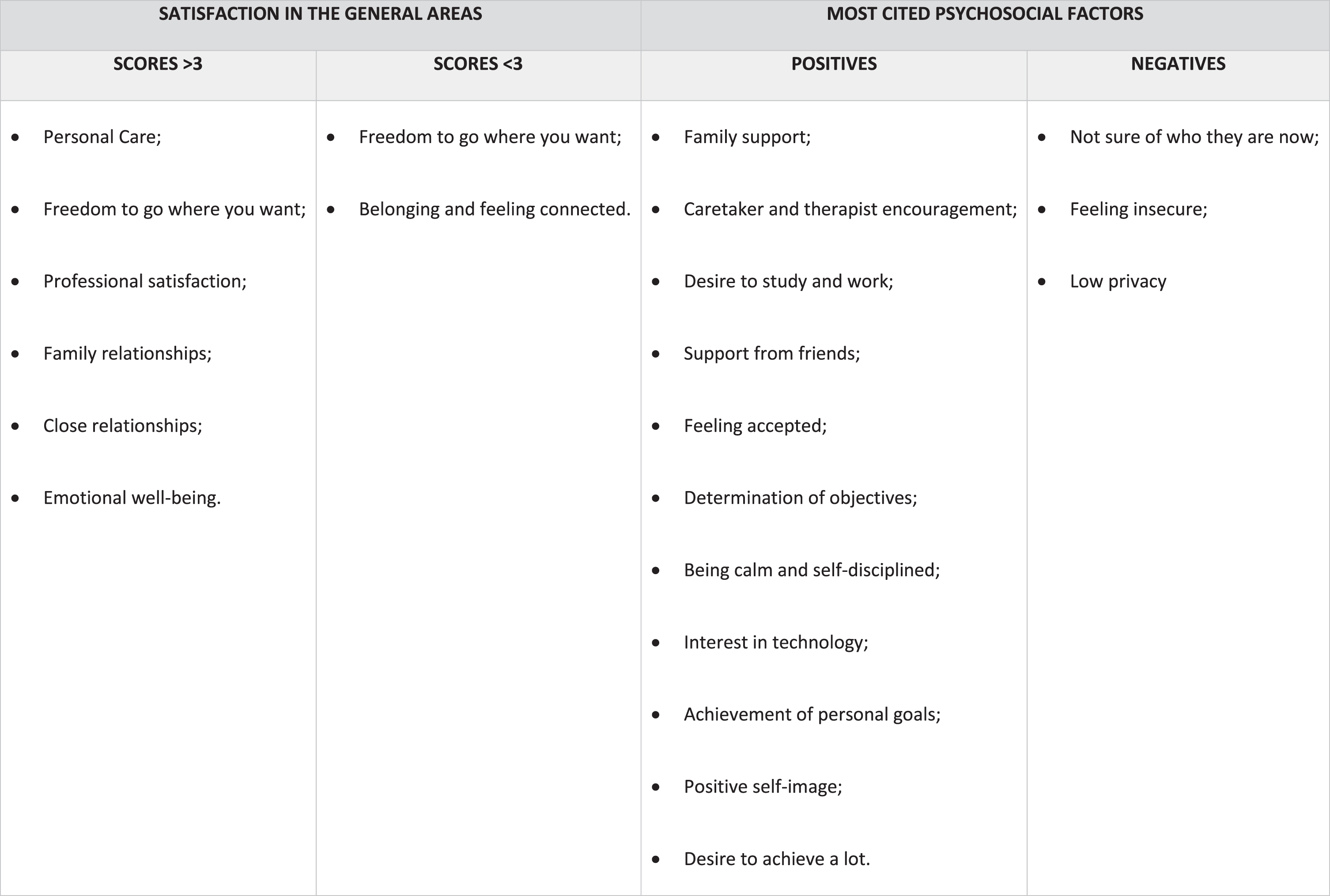
According to the ATD PA-Br, they are often motivated by the AT, offering the support they needed due to their physical condition; also, the joint effect of family, trainers/therapists and AT made them feel encouraged and accepted. However, other issues were listed as unsatisfying, such as wanting more independence, more freedom to go where they want, and desire of belonging/feeling connected with others.
3.1Intervention
The intervention was divided in 3 sessions of 4 hours each.
3.1.1Session 1
It was observed that the relatives and coaches of the adolescents who needed adaptations where the ones who improvised and crafted AT. Thus, the participants already started the interviews saying that they had already solved the problem. However, in the follow-up during training sessions, the adolescents themselves demonstrated demands, such as adjustments to devices already used. Thus, the researcher, together with the trainer, the adolescent and the responsible, listed the complaints to be worked out during the interventions.
After all the demands were listed, the AT prescriptions were made. Subsequently, the intervention report was completed individually to visualize the negative aspects that were most often identified by the adolescents, as observed in Fig. 3.
3.1.2Session 2
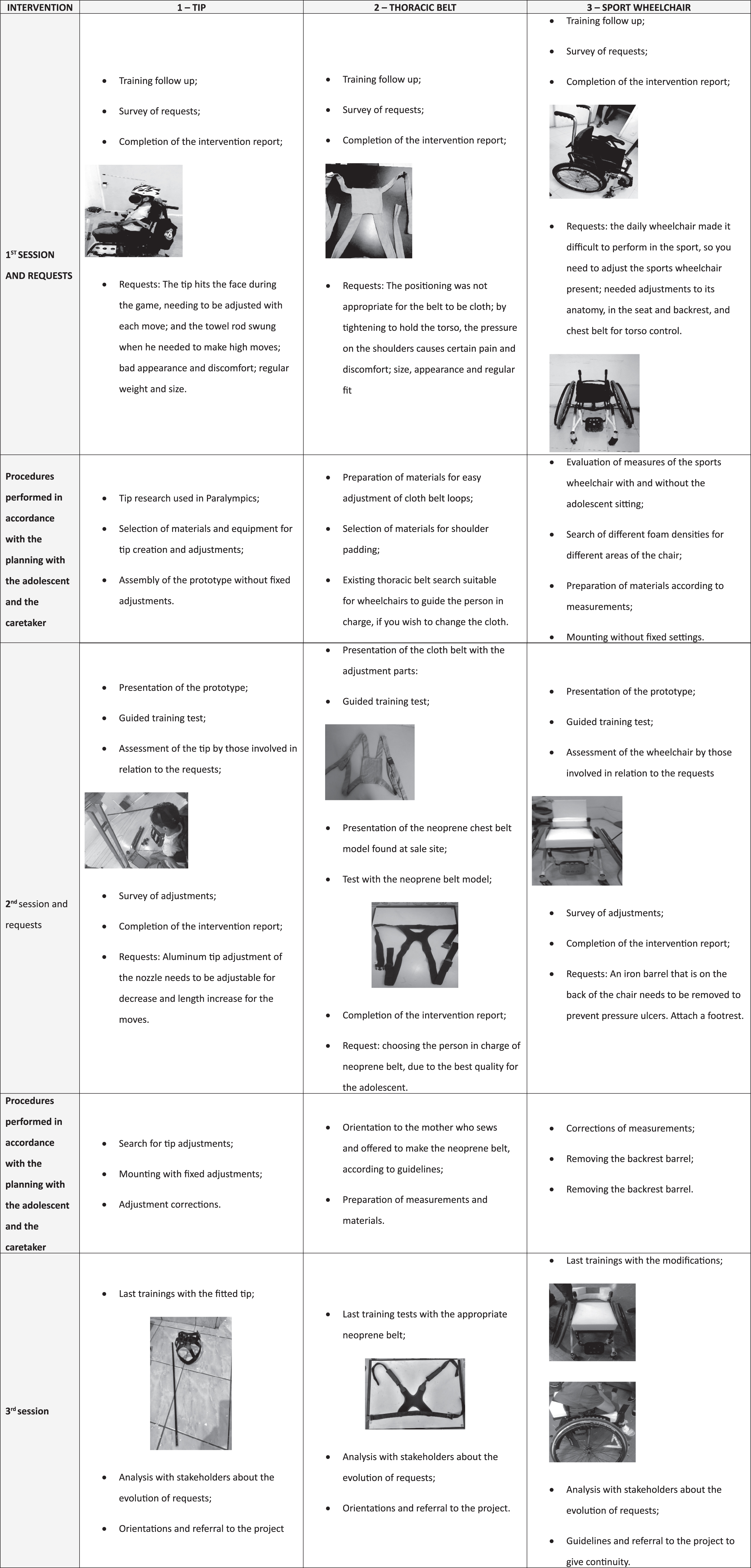
In the second session, the prototypes were presented to the para-athletes and family members to evaluate whether the measures were adequate, so that later adjustments could be made and tested in training. Thus, at this stage adjustments were made, materials were exchanged, and the coaches, the adolescents and those responsible for them were oriented, as detailed in Fig. 4.
Fig. 4
Step-by-step of the interventions according to the sessions.
After the training tests, the adjustments and the completion of the intervention report (Fig. 3) were listed, to verify whether the demands by the adolescents were being met.
3.1.3Session 3
During session 3, the demands from the first session, as seen in Fig. 3, were analyzed in order to see whether they were being met and were referred to the longitudinal care within the local project of assistive technology of the occupational therapy service. After this session, the final intervention report was completed.
Final tests in training were also performed by searching for new adjustments, advice was given to the family, the coaches and the adolescents, and referrals to the project were made.
It was possible to observe in Fig. 3 that the satisfaction of the use of the devices was gradually modified, and fundamental questions on the proper use of the AT devices were answered. The input of the adolescents, the coaches and the family members were considered throughout the process so that performance in each parasport and the overall level of satisfaction with the AT devices were improved.
We can observe that the items most cited as deficient were adjustments, size, appearance, independence with use and comfort; items rated as fair were participation in choice, device weight, pain, AT size and training for its use. It was also possible to observe the individuality of each para-athlete for each AT.
For better detailing of the interventions, Fig. 4 presents the trajectory of the interventions.
From Fig. 4, we can see that the follow-up created possibilities of adapting the AT devices to the context and the specific demands of the adolescents, thus reducing the dissatisfaction with AT. It was also reported a lack of expert professional assistance in AT in each sport.
4Discussion
Due to unforeseen health issues of the athletes, lack of training, or absenteeism due to competitions in other states, three follow-up sessions were held, associated with continuous social network contact with para-athletes and family members, who were able to illuminate important elements of this research.
The results demonstrate the complete process of prescription, choice and follow-up of AT for adolescents training for competition, and the importance of follow-up for the participation of the disabled person.
The entire process followed the tenets of the MPT model, thus considering factors beyond the devices, and psychosocial factors including motivation, expectations and availability for use. For this to occur, according to authors, it was important that the intervention was monitored, since this leads to better results in user empowerment, identification of their capabilities, and participation in the desired activities with AT [21].
The sample was characterized by 2 male adolescents and 1 female, with congenital or childhood deficiencies, ages 13 to 16 years, in the modalities of bocce ball and para-badminton.
According to the Brazilian Law for disabilities [24], assistive technology is guaranteed to people with disabilities to improve autonomy, quality of life and personal mobility. However, as seen in the results, due to a lack of knowledge and applicability of public policies, the devices were improvised and crafted by families and coaches in order to meet the needs of the athletes in training, without monitoring or guidance of qualified professionals in the area of assistive technology.
The lack of access and applicability of the disability inclusion law, in effect since 2017 in Brazil, is also under discussion, with a focus on the promotion of accessibility to sporting events, incentives for training and adequate devices, access to aid scholarships, and other factors that may influence the improvement of these athletes for training and competitions [25].
The lack of qualified professionals for the prescription, choice of TA and follow-up, together with the trainers and family members should be addressed. It is known that the occupational therapist, as part of the interdisciplinary team, must carry out this monitoring because, according to literature this professional is able to conceptualize the context, the individual, the activity performed, and the assistive technology [11]. Thus, the occupational therapist can use the analysis of the activity to choose the appropriate device and follow-up of those involved. It is well known that the shortage of these professionals for prescription of AT in sports and for the support of adults and adolescents with disabilities in Brazil because, as seen in the results, none were monitored, and all presented specific complains.
Regarding the satisfaction with the device and AT use by the participants, we can observe in the results of the B-QUEST evaluation that, although satisfied with the devices in the training sessions, the satisfaction scores with the servicing of such devices were low, because of the scarcity of services and the applicability of public policies and the lack of professionals who can maintain them.
Just as the sport can offer sensations and unusual movements to the person who has physical limitations [2, 5] and can be one of the factors that provides improvement of the social inclusion [1], there are still issues that have gone unrecognized and need to receive attention because they can influence participation in sports. Furthermore, participation in recreational activities is a critical component of the career development process, providing opportunities for individuals to explore interests and could develops work-related skills. But is knew that people with disabilities are often excluded from this kind of participation, which can act as barrier to knowledge about new possibilities and of a future career. So, the authors recommended the importance of recreational planning as part of a vocational rehabilitation process [28].
In this way, the intervention report created by the researchers to evaluate AT during follow-up was based on the theoretical model of MPT assistive technology. Thus, as we observed in the results, lack of training, discomfort, needed adjustments and other factors were cited as poor or fair regarding the satisfaction with the AT device used by the para-athletes. This data concurs with a review study [26], that reported the most relevant factors to the abandonment of AT such as: difficulty in use, dissatisfaction and discomfort.
As seen in the results of the ATD PA-Br evaluation, personal factors such as low freedom, a lack of belonging to the group, feeling unsafe, and lack of privacy were signaled among the para-athletes, and those factors can also lead to the abandonment of the AT and even the parasport itself.
In this study, it was seen that for the prescription of AT, it was necessary to understand the factors that cause the abandonment of the AT, and for this the participants were constantly involved in the prescription and selection of the device. Thus, this highlights the importance of the participation by the coach, family members and para-athletes during the AT prescription process.
Finally, AT can not only facilitate everyday actions, but the engagement in an occupation and in a job in future, while on the other hand, their absence can favor social inequality [13].
In this sense, researchers in study with 149 working-age persons with disabilities, presented moderate correlations between social participation and personal factors, such as self-efficacy and attitudes towards disability. Considering the employed, the scored higher in satisfaction with life, more positive attitudes toward disabilities and higher self-efficacy than the ones who are retired or unemployed. Also, persons who were involved in wheelchair selection scored higher in social participation, performance at work, and quality of life [29].
About the professionals, was confirmed [29] that they should have knowledge and understanding of the multiple factors that influence persons with disabilities’ participation at work and the programs should provide appropriate wheelchairs, skills training, empowerment and problem-solving strategies in labor activities and occupational environment to promote employment of working-age persons with disabilities [29]. These scored confirmed the need of early actions about the inclusion of adolescents in a potential work in the future, to contribute to increase of the variable of the participation, satisfaction and quality of life.
As seen in the results, it is necessary that follow-up be performed by a qualified professional in the area so that the evolving needs of the user of AT in the parasport are fulfilled and that AT plays a role as facilitator.
Based on the validity of the practice of occupational therapy in sports and parasports in Brazil as established in resolution 495 [15], it is expected that these professionals will be able to expand their work in this area and to foster the participation of persons with disabilities in social, leisure or work environments.
5Conclusions
This participatory research with the 3 adolescent para-athletes demonstrates that in order to achieve satisfaction with their AT device and, consequently for to it contribute to the performance in teenage parasports, it is necessary to perform assiduous and individualized follow-up of the para-athlete jointly with the people involved in the sport activity.
The Matching Person and Technology model and the AT instruments used contributed to the intervention process in the area of AT in parasports, including the understanding of the context and psychosocial factors of the para-athletes that use the devices.
Furthermore, the lack of accessibility for individuals with disabilities and their caregivers in relation to the knowledge and applicability of their rights to guaranteed benefits may be a barrier to the practice of parasports in the present, and thus its maintenance in the future.
As a limitation of the study, we can point to the small sample size of this study, which resulted from the established criteria. The main obstacle was the need for frequent attendance of adolescents in training prior to a period of competition. Thus, it is understood that there is a need for a larger sample so that the results can be analyzed more comprehensively to the context of AT in juvenile sports.
Conflict of interest
The authors have no conflicts of interest to declare.
Acknowledgments
We thank the University of Brasília - Ceilândia; the team, the juvenile parathletes of the Training Center of Special Physical Education - CETEFE; the research group Nucleus of Assistive Technology and Innovation of the Center West - NTAAI and the financial support of the Foundation of Support and Research of the Federal District - FAP. DF.
References
[1] | Azevedo ABL . et al. Manual de Orientação Departamento Científico de Adolescência: Atualização sobre Inclusão de Crianças e Adolescentes com Deficiência. Sociedade Brasileira de Pediatria. (2017) ;3: :6–13. |
[2] | Pavani R , Pavani S , Silva RP . Design em Tecnologia Assistiva: esgrima paraolímpica. Revista de Design, Tecnologia e Sociedade, Brasília. (2017) ;4: (1):53–79. |
[3] | Centro Regional das Nações Unidas. Alguns Factos e Números sobre as Pessoas com Deficiência [internet]. UNRIC. Available from: https://www.unric.org/pt/pessoas-com-deficiencia/5459. |
[4] | United Nations Children’s Fund - UNICEF, World Health Organization. Assistive Technology for Children with Dis-abilities: Creating Opportunities for Education, Inclusion and Participation A discussion paper. 2015 Available from: https://www.unicef.org/disabilities/files/Assistive-Tech-Web.pdf. |
[5] | Labronici RHDD , Cunha MCB , Oliveira ASB , Gabbai AA . Sport as integration factor of the physically handicapped in our society. Arquivo Neuropsiquiatra. (2000) ;58: (4):1094–9. |
[6] | Cardoso VD . The rehabilitation of persons with disabilities through adapted sport. Revista Brasileira de Ciências do Esporte. (2011) ;33: (2):529–239. |
[7] | Marques RFR , Duarte E , Gutierrez GL , Almeida JJG , Miranda TJ . Olympic and Paralympic sports: coincidences, divergences and specifies under a contemporary perspective. Rev. bras. educ. fís. Esporte. (2009) ;23: (4):365–77. |
[8] | Hiaiachi MC , Cardoso VD , Filho ARR , Gaya ACA . Reflections on the career of Brazilian Paralympic athletes. Ciência e saúde coletiva. (2016) ;21: (10):2999–3006. |
[9] | Feitosa LC , Muzzolon SRB , et al. The Effect Of Adapted Sports In Quality Of Life And Biopsychosocial Profile Of Children And Adolescents With Cerebral Palsy. Rev Paul Pediatr. (2017) ;35: (4):429–35. |
[10] | Cruz DMC . Models of practice in occupational therapy and possibilities for clinical practice and research in Brazil. Rev Interinst Bras Ter Ocup. (2018) ;2: (3):504–17. |
[11] | Costa e Silva AA , MarqueS RFR , Pena LGS , Molchansky S , Borges M , et al. Sport for persons with a disability: approach about the factors that influence the practice of team wheelchair sports. Rev Bras Educ Fís Esporte. (2013) ;27: (4):679–87. |
[12] | International Standard. International Standard. Assistive products for persons with disability –Classification and terminology, ISO 9999:2016. 6a Edição,, 2016. Available from: https://www.sis.se/api/document/preview/920988/. |
[13] | Bonilha FFG . Lei brasileira da pessoa com deficiência comentada: da tecnologia assistiva In. SETUBAL JM, FAYAN RAC. Mobilização Para Autonomia. (2017) ;1: (12):207–14. |
[14] | Silva LC . O design de equipamentos de tecnologia assistiva como auxílio no desempenho das atividades de vida diária de idosos e pessoas com deficiência, socialmente institucionalizados. Universidade Federal do Rio Grande do Sul. UFRGS LUME –Repositório Digital. 2011. |
[15] | Conselho federal de fisioterapia e terapia ocupacional - coffito. Resoluções: Resolução n° 495 de 18 de dezembro de 2017- Disciplina a Atuação Profissional da Terapia Ocupacional no Desporto e Paradesporto e dá outras previdências, 2018 [internet]. Available from: https://www.coffito.gov.br/nsite/?p=8781. |
[16] | Martins GA . Estudo de caso: uma reflexão sobre an aplicabilidade em pesquisas no Brasil. Revista de Contabilidade e Organizações. (2008) ;2: (2):9–18. |
[17] | Creswell JW . Projeto de Pesquisa: métodos qualitativo, quantitativo e misto. Artmed. (2010) ;3: :161–224. |
[18] | Centro de treinamento de educação física especial –CETEFE [internet]. Acesso a informações 2017. Available from: www.cetefe.org/?page_id=1044. |
[19] | Carvalho Kec , Junior MBG , Sá KN . Translation and validation of the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0) into Portuguese. Rev Bras Reumatol. (2014) ;54: (4):260–7. |
[20] | Alves ACJ , Martins EF . Reliability of assistive technology device –predisposition assessment (ATD PA Br) in Brazilian Portuguese. Reliability of assistive technology device. Rev Ter Ocup Univ São Paulo. (2018) ;29: (2):144–54. |
[21] | ALVES ACJ . Avaliação de tecnologia assistiva predis-posição ao uso: ATD PA Br: versão brasileira. Brasília: Editora Universidade de Brasília. 2017. |
[22] | Associação brasileira de empresas de pesquisa - ABEP. Critério de Classificação Econômica Brasil. 2015. |
[23] | Marconi MA , Lakatos EM . Fundamentos de Metodologia Científica. Atlas. 2010. |
[24] | Senado Federal. Estatuto da pessoa com deficiência. Secre- taria de Editoração e Publicações Coordenação de Edições Técnicas. Brasília, 2015. |
[25] | Gouveia R . Projeto de Lei N.º 6.860, DE 2017. Câmara dos deputados 2017. |
[26] | Costa RC , Ferreira FMRM , Bortolusb MV , Carvalho MGR . Dispositivos de tecnologia assistiva: fatores relacionados ao abandono. Cad. Ter. Ocup.UFSCar. (2015) ;23: (3):611–24. |
[27] | Comitê Paraolímpico Brasileiro –CBP [internet]. Available from: http://www.cpb.org.br. |
[28] | Devine MA , Koch LC . Recreational Planning: An Important Component of Career Counseling for People with Disabilities. WorK. (2003) ;1: :83–8. |
[29] | Martins AC . Using the International Classification of Functioning, Disability and Health (ICF) to address facilitators and barriers to participation at work. Work. (2015) ;50: (4):585–93. |

