
The design and evaluation of an ergonomic valve-wrench
Abstract
BACKGROUND:
The torque required to manually turn a handwheel-valve typically exceeds operators’ capabilities, requiring them to use a valve-wrench. Although valve-wrenches are commonly used, an ergonomic wrench has not yet been developed.
OBJECTIVE:
To introduce an ergonomically designed valve-wrench and evaluate it with respect to conventional valve opening methods.
METHODS:
Four methods were compared including: bare hands, restricted conventional wrench (assumes presence of obstructions), unrestricted conventional wrench, and ergonomically-modified wrench. Each method was performed at two torque settings, 15 Nm and 30 Nm. Electromyography activities were measured from eight trunk and shoulder muscles. The time to fully open the valve and Borg-ratings were recorded for each method.
RESULTS:
The modified wrench resulted in the lowest average time and Borg-rating; however, these averages were not significantly different from the averages of the unrestricted conventional wrench. The method that was associated with the lowest overall electromyography activities was restricted conventional wrench, followed subsequently by bare hands, modified wrench, and unrestricted conventional wrench.
CONCLUSIONS:
Although the ergonomically-modified wrench was associated with relatively high electromyography activities, it was the most time-efficient method, allowing the muscles to sustain physical loads for shorter periods of time. Overall, participants rated this method as the least physically demanding.
1.Introduction
Manual cracking, opening, and closing of valves are common tasks in various industries. Some of the different workplaces that utilize handwheels to control valves are the power generation, water supply, petrochemical, railways, and waste management industries [1]. Handwheel actuation is primarily used to regulate the flow of material within a valve system, such as steam, oil, refrigerant, and fly ash. Handwheels can also be used to regulate the movement of rail cars as it is done in the railway industry.
In a typical plant that generates power or processes materials, there are thousands of handwheels that are either motor operated or manually operated [2]. Typically, the torque required to manually actuate a handwheel exceeds operators’ capabilities. Parks and Schulze [3] investigated 336 valves of various handwheel diameters and heights at a large petroleum refinery and found that the cracking torque to open a handwheel ranged from 100 Nm to as high as 225 Nm; the ‘cracking torque’ is defined as the torque required to start the initial movement of the handwheel from a locked position to an unlocked position [1]. Also, Jackson et al. [4] measured the cracking torque of 217 valves in a chemical plant and found that 93% of the valves required torques of over 400 Nm. A gross discrepancy results when comparing these torque values with operators’ strengths. Several studies measured maximum torque production capabilities of operators using handwheels of different sizes, heights, angles, and distances from operators [5, 6, 7]. The average maximum torque produced by the operators in these studies was approximately 62 Nm, which is significantly less than the torque demands in the field.
The disparity between the torque demands in the field and operators’ capabilities poses a risk of injuries to the operators. Parks and Schulze [3] conducted data searches for five downstream facilities of the Phillips Petroleum Company to determine the type and number of injuries experienced by operators over a three-year period. Results showed that 57% of back injuries and 75% of head, neck, and face injuries were associated with valve operations. Furthermore, valve operations have been described as the most physically demanding task by plant operators [4].
Due to the high torque demands in the field, valve operators are forced to use wrenches for turning handwheels. The use of wrenches is prevalent in valve operations; and therefore, it is vital to develop an ergonomic valve-wrench through systematic research to reduce the risk of injury and improve efficiency. In this study an ergonomic valve-wrench was designed using past research, ergonomic principles, and user feedback, and its efficacy was tested in valve operation experiments. Specifically, the objectives of this research were to: (1) compare the ergonomically modified valve-wrench to conventional valve opening methods, in terms of efficiency (time to open valve), perceived physical exertion (Borg-scale), and muscle loading of shoulder and trunk muscles; and (2) determine whether the torque setting (15 Nm and 30 Nm) of the valve affects the preferred valve opening method. This research hypothesized that the modified wrench will be the least physically demanding and most efficient method in opening a valve regardless of torque level.
2.Methods
2.1Participants
Fifteen healthy university-aged male participants were recruited for this study. The experimental procedures and the demands of the testing were explained to the participants and their signatures were obtained on informed consent forms approved by the institutional review board (IRB). The Physical Activity Readiness Questionnaire (PAR-Q, British Columbia Ministry of Health) was used to screen participants for cardiac and other health problems, such as dizziness, chest pain, or heart trouble [8]. Any participant who answered yes to any of the questions on the PAR-Q was excluded from the study. The average (SD) age, height, and weight of the participants were 23.4 (3.1) years, 179.8 (5.1) cm and 81.1 (12.1) kg, respectively.
2.2Tools and equipment
2.2.1Handwheel-valve system
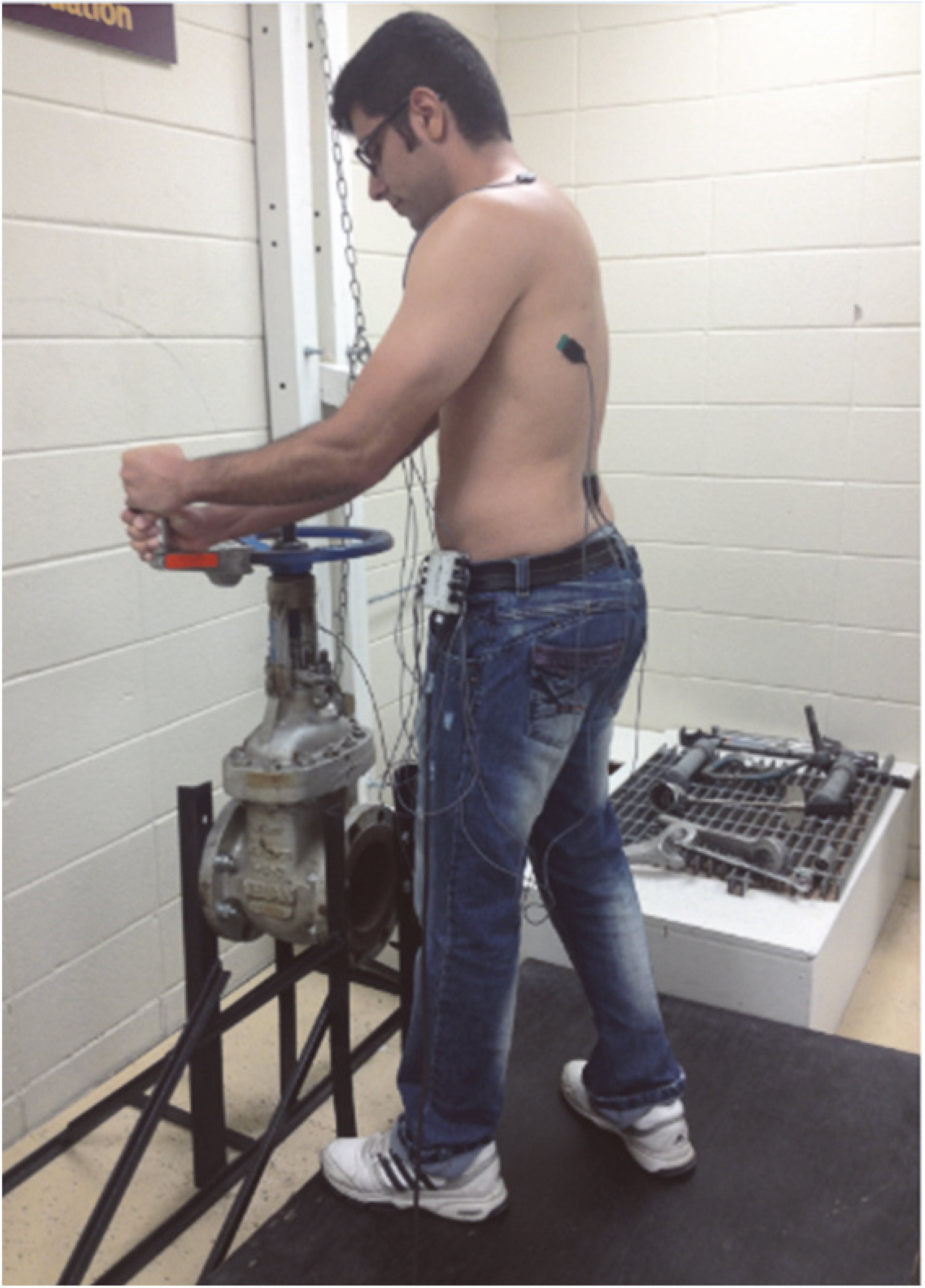
A handwheel-valve system was used for this study (Fig. 1). The handwheel-valve system consists of a standard 15 cm (inside diameter) manual gate valve and a 36 cm diameter handwheel. The handwheel is horizontally-oriented at a height of about 100 cm from the grade. To fully open this valve system from a closed position, it requires approximately 18 counterclockwise handwheel revolutions.
Figure 1.
A 15 cm manual gate valve with a 36 cm diameter handwheel.
2.2.2Valve-wrenches
Two types of wrenches for handwheel actuation were used in this study: (1) a conventional wrench available in the market and (2) an ergonomically-designed wrench. The conventional wrench is a forged aluminum ‘crow’s foot’ valve-wrench (Fig. 2a). Its handle is approximately 28 cm in length. The redesigned wrench was similar in design, except that the handle was modified to be adjustable between 0 and 180 degrees (Fig. 2b). This was done by fabricating a hinge in the handle 17 cm from the crow’s foot. Since the modified wrench has a shorter handle than the conventional wrench, obstructions (i.e. pipes, tanks, walls, etc.) during handwheel actuation is limited. It allows the operator to turn a handwheel continuously without having to unhook the wrench from the handwheel. On the other hand, the conventional wrench typically requires unhooking and reattaching it to the handwheel, due to its longer handle confronting obstructions. The handle diameter and length of the redesigned wrench were also modified to meet ergonomic designs. Kong and Lowe [9] evaluated the relationships between the diameter of cylindrical aluminum handles and perceived comfort. They found that the optimal handle diameter in maximizing subjective comfort was 19.7% of the user’s hand length. Based on the results, they recommended a handle diameter of approximately 3.76 cm. Hence, a handle diameter of 3.76 cm was selected for this study. Also, the handle for the modified wrench was designed to be larger than the hand breadth of the 95
Figure 2.
(a) Conventional valve-wrench; and (b) Ergonomically modified valve-wrench.

2.2.3Electromyography (EMG)
This study used an eight channel wireless EMG system to measure the electrical activity of shoulder and trunk muscles (Delsys Inc., Boston, USA). The EMG system consists of a Myomonitor IV, an input module, eight surface electrodes, and one reference electrode. The surface electrodes that were used for EMG signal acquisition were parallel bar active surface electrodes (DE-2.3 EMG Sensors, Delsys Inc., Boston, USA).
2.3Experimental task
Participants were asked to fully open a valve from the closed position, using four different methods. All methods were performed at two different torque settings, 15 Nm (11.06 ft-lb) and 30 Nm (22.13 ft-lb). The four valve opening methods were:
1) Bare hands (BH): This method required participants to repetitively turn the handwheel, using their bare hands. Each actuation began with the right hand supine at approximately the 6 o’clock position and the left hand prone at approximately the 12 o’clock position. The maximal length of each actuation was limited to half a revolution.
2) Conventional wrench unrestricted (CW-U): In this method, the conventional wrench was used to actuate the handwheel. Participants were asked to keep both hands at the end of the wrench, as they continuously turned the handwheel all the way around. This method simulated a handwheel-valve system that has no obstructions that would limit movement during handwheel actuation.
3) Conventional wrench restricted (CW-R): This method used the conventional wrench to turn the handwheel, but it assumed the presence of obstructions getting in the way of actuation and limiting the amount of turning. Hence, the maximal length of each actuation was limited to 2/3
4) Modified wrench (MW): This method used the ergonomically-modified wrench to actuate the handwheel. Participants were required to keep both hands on the handle of the wrench, as they continuously turned the handwheel all the way around.
2.4Experimental design
A two factor split-plot experimental design was used. Participants served as blocks within which experimental conditions were randomized. The independent variables were method (BH, CW-R, CW-U, and MW) and torque setting (15 Nm and 30 Nm). Each participant performed a total of 8 (4 methods
2.5Data collection and processing
2.5.1Orientation
Each participant was given an orientation, introducing them to the equipment, data collection procedures, and specifics of the experimental tasks. The demographic information (age, height, weight, and gender) of the participants were recorded. Then the participants underwent a five-minute warm-up session on a treadmill. The speed of the treadmill was adjusted by the participants to their comfortable walking speed (
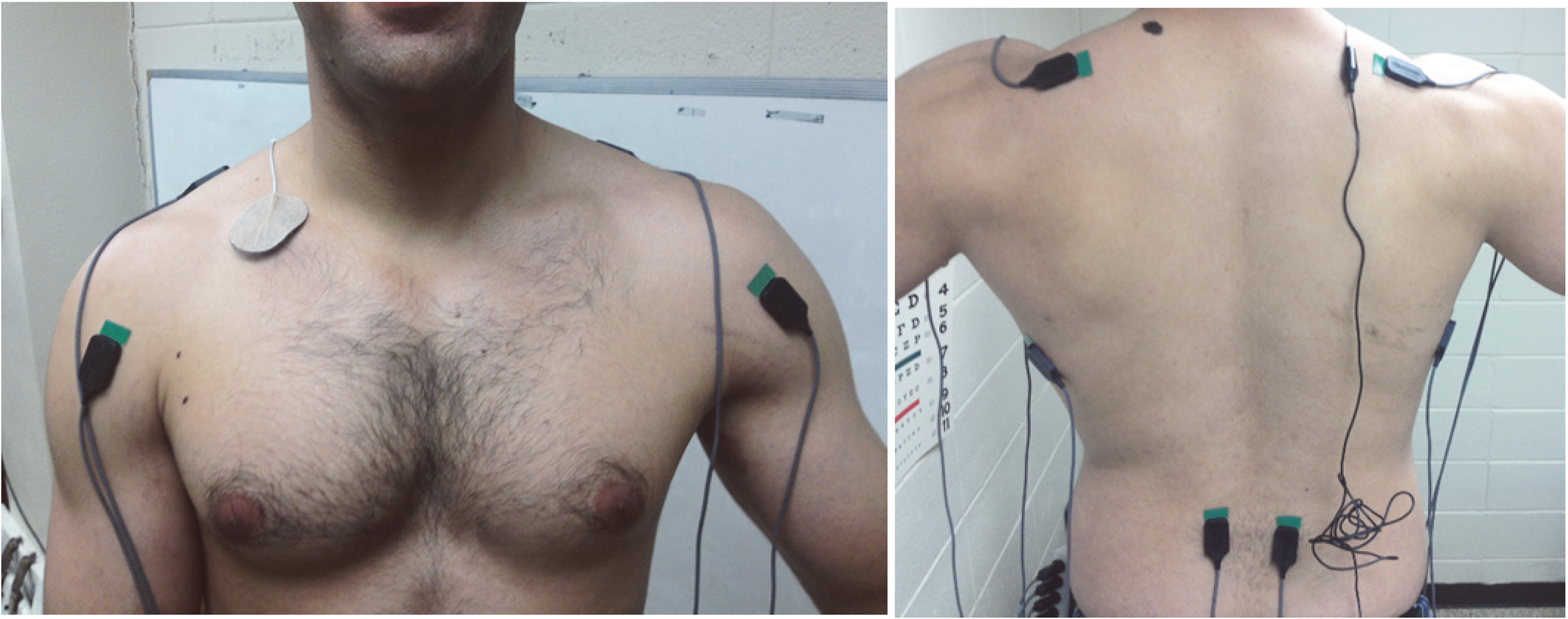
Figure 3.
The exact location and positioning of each electrode for the anterior deltoid, trapezius, latissimus dorsi, and erector spinae (Konrad, 2005).
2.5.2EMG preparation
Subsequent to the warm-up session, preparations were made to prepare the participants for EMG data acquisition. Any hair on the skin was removed at the right and left anterior deltoids, right and left trapezius, right and left latissimus dorsi, and right and left erector spinae muscles. Also, the same areas were cleaned with alcohol to remove dead skin cells, dirt, and sweat. After cleaning the skin, the EMG surface electrodes were attached to the muscles of interest parallel to the muscle fibers (Fig. 3). This study used the same electrode locations as recommended or used by: Perotto et al. [11] for the anterior deltoids and latissimus dorsi, Farina et al. [12] for the trapezii, McGill [13] for the erector spinae, and Soderberg and Knutson [14] for the ground electrode.
2.5.3RC exertions
Comparison of EMG between and within participants required normalizing the EMG data. To do this, participants first performed a series of reference contraction (RC) exertions, also known as maximum voluntary contractions (MVC). The RC exertions were performed for each investigated muscle separately. Each RC exertion sought to isolate its corresponding muscle in a maximum isometric exertion against a static resistance. The maximum EMG activities in the RC exertions were used for normalizing the EMG data collected in the experimental trials. This study used the same RC exertions recommended or used by: Al-Qaisi and Aghazadeh [15] for the anterior deltoids and trapezii, Hintermeister et al. [16] for the latissimus dorsi, and Kendall et al. [17] for the erector spinae.
For the RC exertions, participants were asked to gradually exert to their maximum effort in 3 to 5 seconds, hold it for 3 seconds, and gradually decrease the force in 3 seconds [18]. Each RC exertion was repeated three times. To avoid muscular fatigue, repetitions were separated with 30 to 60 seconds of rest [18] and RC sets were separated with 2 minutes of rest [19]. The maximum EMG activity of the three repetitions was used for normalizing the EMG data. During RC exertions, EMG data was collected for a period of 15 seconds, giving participants enough time to reach their maximum exertion.
2.5.4Experimental trials
After the RC exertions, the participants actuated a handwheel-valve system from fully closed to fully open (counterclockwise). Since this research is concerned with continuous handwheel actuation and not the initial cracking force, the handwheel was cracked open 1/3
Before each trial, participants were trained and given time to practice the valve opening methods (i.e. BH, CW-R, CW-U, MW) until they felt comfortable with the procedure. They were instructed to use only their upper body in actuating the handwheel. Feet were kept firm on the ground at approximately shoulder length apart. They were asked to stand at a distance from the handwheel that they felt was most comfortable. However, once they determined their comfortable distance, they had to maintain that position and limit their foot movement as much as possible. All the methods were performed as fast as possible to simulate ‘real world’ conditions where valves must be opened and/or closed quickly. Such situations occur during emergency conditions and in starting up and shutting down of a unit.
The EMG data acquisition started approximately 3 seconds into each trial and lasted for 20 seconds. The raw EMG activity from each electrode location was demeaned first and then full-wave rectified. The full wave rectified EMG activity was then low pass filtered at 4 Hz, using a fourth-order dual pass Butterworth digital filter, to form a linear envelope [21]. The peak activation of each muscle in each trial was normalized with respect to the maximum EMG activity of its corresponding RC exertion. Thus, results for each muscle were reported as a percentage of the muscle’s RC (%RC).
The task of fully opening the valve system from the closed position was timed for each trial using a stopwatch. The time measurements were used to compare the efficiency of the different valve opening methods.
Immediately after each trial, participants were required to rate their perceived physical exertion on a Borg CR-10 scale [22, 23]. All the participants were given a brief introduction on the Borg scale and an explanation on how to use it.
2.6Statistical analysis
A two factor split-plot analysis of variance (ANOVA) was used to assess the effects of the different valve opening methods and torque-settings on the normalized EMG activities, Borg-ratings, and times. A post hoc analysis, in the form of Tukey-Kramer multiple pairwise comparisons (referred to as the Tukey test in the remainder of the manuscript), was performed. A significance level (
Table 1
The p-values associated with each dependent variable and effect
| Effects | Time | Borg | R Del | L Del | R Trap | L Trap | R Lat | L Lat | R ES | L ES | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| rating | ||||||||||||||||||||
| Method (M) | .0001 | .0001 | 0 | .0029 | .0001 | .0001 | .0001 | 0 | .1419 | .0001 | .0001 | 0 | .0352 | |||||||
| Torque (T) | 0 | .0042 | .0001 | 0 | .0059 | 0 | .0132 | 0 | .5413 | 0 | .0365 | 0 | .5269 | .0001 | 0 | .4784 | 0 | .1136 | ||
| T | 0 | .6954 | 0 | .4501 | 0 | .4245 | 0 | .9043 | 0 | .3953 | 0 | .6424 | 0 | .2758 | 0 | .1869 | 0 | .6328 | 0 | .4456 |
Values with asterisks (*) represent significant p-values. Note: R
3.Results
This research compared four different valve opening methods at two torque levels in terms of efficiency (time to open valve), perceived physical exertion (Borg-ratings), and peak EMG activities of shoulder and trunk muscles. Table 1 summarizes the p-values from the ANOVA output associated with each effect (i.e. method main effect, torque main effect, and torque-method interaction effect) for each dependent variable investigated. Values with asterisks in the table represent significant p-values. The torque-method (T*M) interaction effect was not significant for any of the dependent variables, indicating that the effects of torque and method were independent of each other for all the dependent variables. Therefore, the following sections will compare: methods averaged over both torques; and torques averaged over all methods.
Table 2
The maximum EMG activities (%RC) associated with each valve opening method
| Maximum EMG activities (%RC) | ||||||||
| Method | R Del | L Del | R Trap | L Trap | R Lat | L Lat | R ES | L ES |
| BH | 70.4 | 21.5 | 37.6 | 25.9 | 38.8 | 73.5 | 42.4 | 52.2 |
| CW-R | 69.9 | 63.1 | 27.8 | 28.2 | 33.6 | 40.0 | 46.1 | 50.3 |
| CW-U | 86.4 | 64.8 | 56.8 | 55.1 | 44.6 | 55.8 | 62.9 | 63.2 |
| MW | 81.2 | 63.2 | 52.4 | 70.2 | 44.9 | 57.2 | 56.9 | 58.4 |
Note: R
3.1Comparison of valve opening methods
Table 2 summarizes the average peak EMG activities associated with each valve opening method. The Tukey results are also presented in Table 2, where methods are grouped into different letter groups. Within each dependent variable (or column), methods that are in the same letter group indicate that no significant difference exist between their EMG activities (i.e.
• High EMG activity group: includes the highest EMG activity in a column (muscle) and EMG activities that were not significantly different from it;
• Low EMG activity group: includes the lowest EMG activity in a column and EMG activities that were not significantly different from it;
• High & low EMG activity group: includes EMG activities that were not significantly different from the highest and lowest EMG activities;
• Medium EMG activity group: includes EMG activities that were significantly different from both the highest and lowest EMG activities.
The aim was to identify the method associated with relatively low loading across most of the muscles or, in other words, the method that had the most muscles in the low EMG activity group. On the other hand, a method with many muscles in the high EMG activity group indicates a relatively high loading on the corresponding muscles. In terms of EMG activities, the CW-R appears to be the best method. All of the muscles with the exception of the left anterior deltoid were in the low EMG group. The left anterior deltoid was in the high EMG group with an EMG activity of 63.1%RC. This EMG activity was not significantly different from the highest EMG activity for that muscle, which was 64.8%RC for the CW-U. Overall, the CW-R appears to have the lowest EMG activities.
Figure 4.
The average times (and standard deviations) associated with each valve opening method averaged over 15 Nm and 30 Nm.
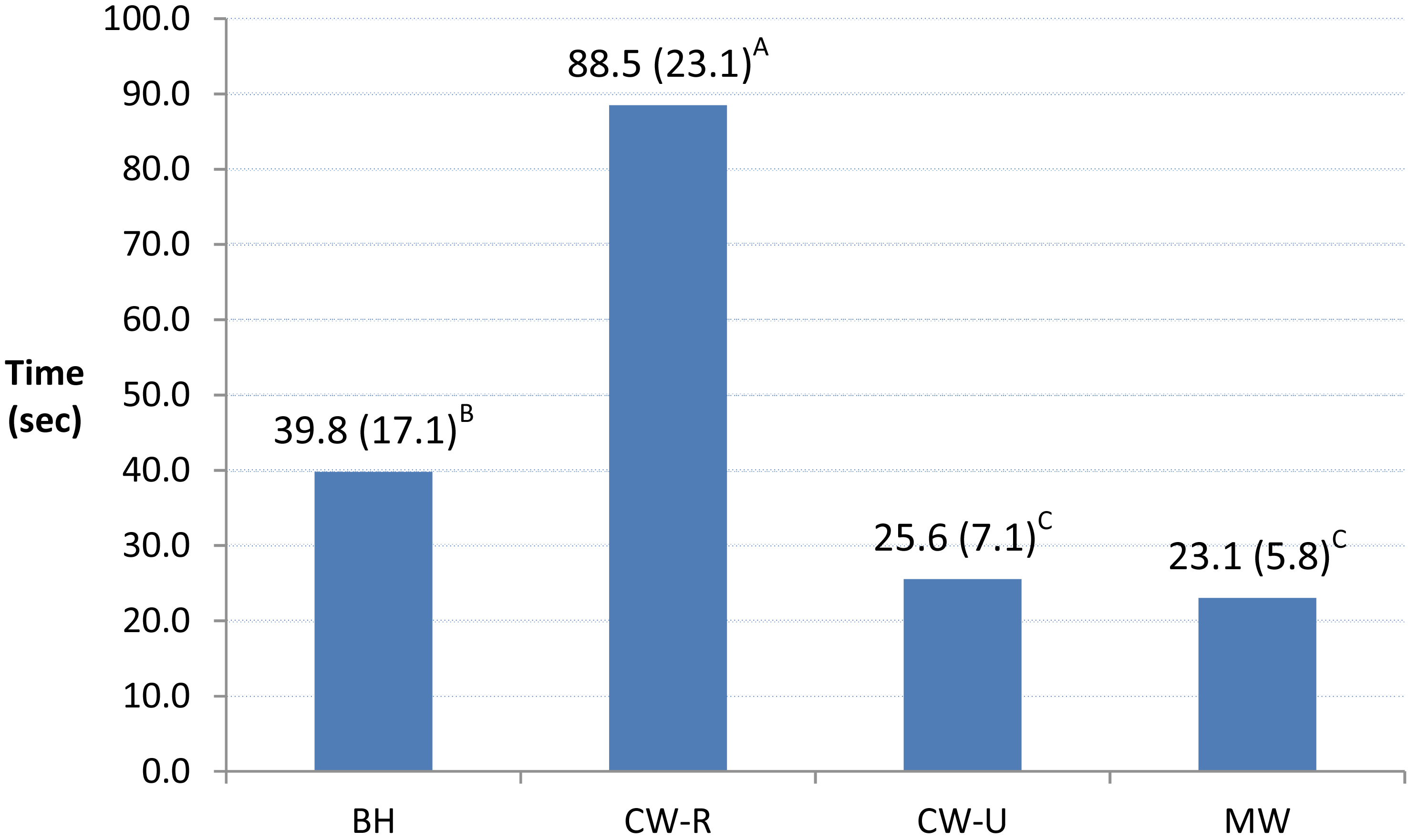
However, a downside to the CW-R method is that it was the least efficient method. Figure 4 shows a bar graph of the average times (and standard deviations) it took to fully open the valve using the different methods. The Tukey results of the time variable are also presented in Fig. 4. Methods are grouped into different letter groups according to the statistical results of the pairwise comparisons. CW-R required an average of 88.5 s to fully open the valve, which was significantly greater than the average times of the other methods. Although this method required low muscle activations, it required the most time to fully open the valve.
Figure 5.
The average Borg-ratings (and standard deviations) associated with each valve opening method averaged over 15 Nm and 30 Nm.
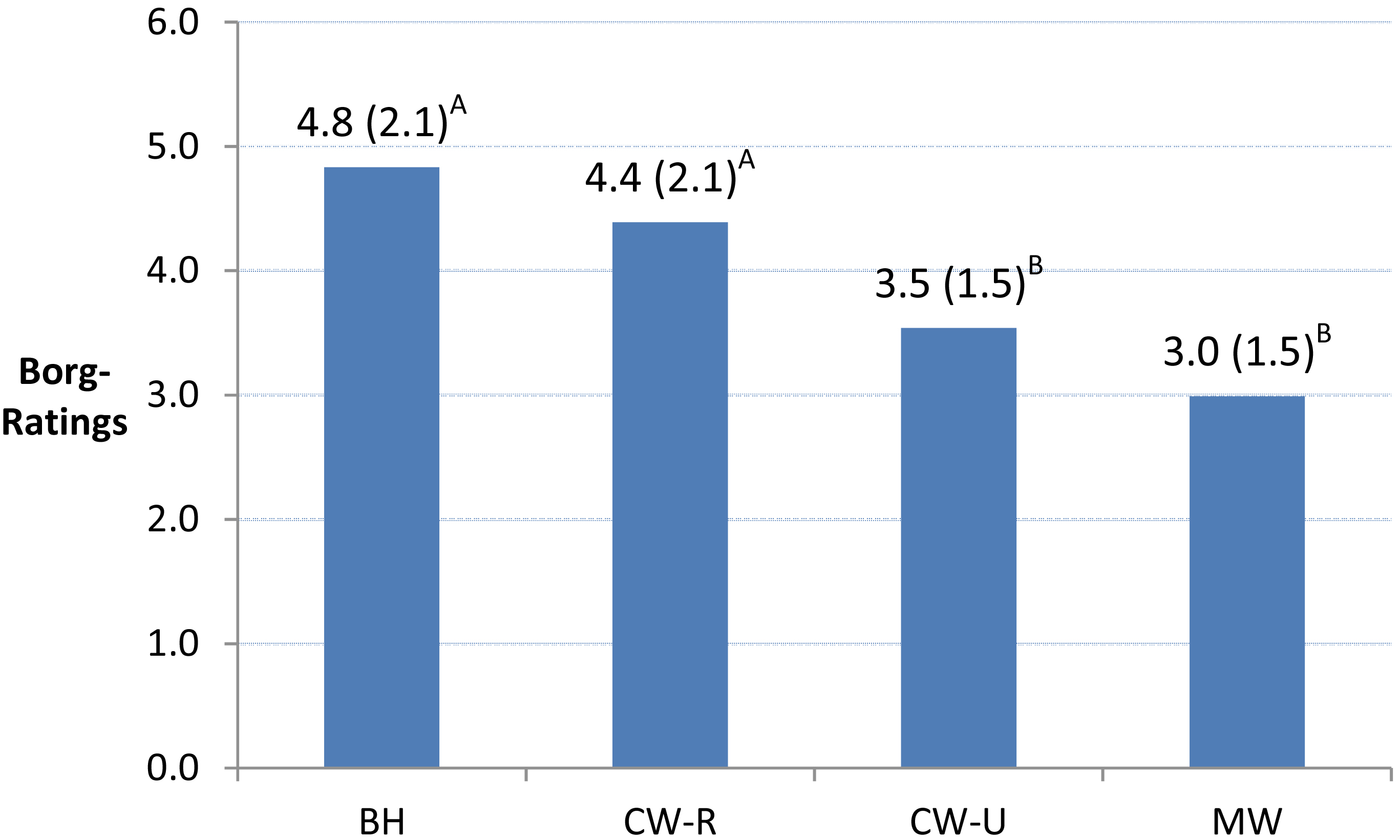
In contrast to the EMG output, participants perceived CW-R to be one of the more strenuous methods. Figure 5 shows a bar graph of the average Borg-rating (and standard deviation) associated with each method. The Tukey results are also presented in Fig. 5 grouping methods into different letter groups. CW-R received an average Borg-rating of 4.4, which was not significantly different than the highest average Borg-rating of 4.8 for BH. In the Borg-scale, a 4.4 corresponds to a physical task that falls between ‘somewhat difficult’ (4) and ‘difficult’ (5). A possible explanation as to why this method received a high Borg-rating is that it involved forceful exertions for longer periods of time (Fig. 4).
Another method that was associated with low EMG activities was the BH method (Table 2). All the muscles, except for the left latissimus dorsi and left erector spinae, were in the low EMG group. The left latissimus dorsi was associated with significantly higher EMG activity (62.2%RC) in this method than all the other methods. The left erector spinae on the other hand was not significantly different from both the lowest and highest EMG activities (50.3%RC and 63.2%RC, respectively). However, its EMG activity (52.2%RC) was closer to the lowest EMG activity than the highest EMG activity. Apart from the left latissimus dorsi, all the muscles in this method had relatively low EMG activities.
The BH method was associated with significantly lower times than the CW-R; yet, participants perceived BH to be one of the more strenuous methods. It had an average Borg-rating of 4.8, which was the highest average of all the methods. All the methods except for BH involved the use of a valve-wrench, which permits the generation of greater torques with less force. This lack of leverage may explain why BH was associated with the highest average Borg-rating.
The CW-U method appears to have the greatest loading on the trunk muscles than all the other methods. Five of the eight muscles were in the high EMG group using this method, including the right anterior deltoid (86.4%RC), the left anterior deltoid (64.8%RC), right trapezius (56.8%RC), right erector spinae (62.9%RC), and left erector spinae (63.2%RC). The advantage of this method, however, is that it required significantly less time to fully open the valve than BH and CW-R. It required an average of only 25.6 s to fully open the valve. Another advantage of this method is that participants perceived it to be significantly less strenuous than BH and CW-R. The average Borg-rating of the CW-U method was 2.6. Although the overall EMG activities were highest using CW-U, it was perceived to be less strenuous than BH and CW-R. This method may, in fact, be less physically demanding since the high muscle activities were sustained for a relatively short period of time.
In using the MW, four of the eight muscles were in the high EMG group, including the left anterior deltoid (63.2%RC), right trapezius (52.4%RC), left trapezius (70.2%RC), and right erector spinae (56.9%RC). Only one muscle was in the low EMG group, which was the right latissimus dorsi (44.9%RC).
Although the muscle activities were relatively high in the MW method, it was associated with the lowest average Borg-rating (3.0) and time (23.1 s). Both of these measures for the MW did not differ significantly from the CW-U mean Borg-rating and time, respectively. In other words, participants perceived this method to require a relatively low physical exertion, and it was relatively more efficient in opening the valve. Since the high EMG activities were endured for shorter times in this method, participants may have perceived it to be less strenuous.
Table 3
The EMG, Borg-rating, and time results for 15 Nm and 30 Nm
| Maximum EMG activities (%RC) | ||||||||||
| Torque | R Del | L Del | R Trap | L Trap | R Lat | L Lat | R ES | L ES | Borg-rating | Time (s) |
| 30 Nm | 84.6 | 57.8 | 44.8 | 48.4 | 42.5 | 65.2 | 53.0 | 58.8 | 4.9 | 47.5 |
| 15 Nm | 69.3 | 48.4 | 42.5 | 41.3 | 38.5 | 48.0 | 51.1 | 53.3 | 3.0 | 40.9 |
| Difference | 15.3 | 9.4 | 2.3 | 7.1 | 4.0 | 17.2 | 1.9 | 5.5 | 1.9 | 6.6 |
Note: R
3.2Comparison of torque settings
One of the objectives of this research was to determine how the torque level (15 Nm and 30 Nm) affects the values of the dependent variables among the different valve opening methods. For all the dependent variables, the interactions between the torque and method effects were not statistically significant (Table 1). However, the torque main effect was statistically significant for the majority of the dependent variables. Table 3 presents the averages of the dependent variables at each torque. For all the dependent variables, the means at 30 Nm were either greater than or equal to the means at 15 Nm and never lower.
4.Discussion
Most ergonomic research concerned with handwheel-valve operations investigated the design of the handwheel, including handwheel height, orientation, diameter, and grip design [2, 5, 6, 7, 24, 25]. The current research, on the other hand, was concerned with the design of the valve-wrench used to facilitate handwheel actuation. Ergonomic modifications were introduced into the design of the valve-wrench, and the new wrench was compared to conventional valve opening methods. No past research was found in the literature investigating ergonomic valve-wrenches.
At both 15 Nm and 30 Nm, the MW was one of the most efficient and least physically demanding methods in opening a valve. The only concern with the new design is that it was generally associated with higher maximum EMG activities than the conventional valve opening methods. However, these EMG activities were endured for relatively shorter time periods, possibly explaining why it was perceived to be the least physically demanding.
During the experiments, several participants commented that the joint or hinge in the MW was unstable. Participants found it difficult to maintain a 90
5.Research limitations
Several limitations were recognized in this study, which included the following:
• Participants were recruited from a student population. Many of the student participants did not have previous experience in handwheel actuation; however, they were trained and allowed to practice the techniques of handwheel actuation before the experimental trials. The benefit of using inexperienced participants may inform about the effectiveness of the MW among novice valve operators.
• The findings of this study are limited to one handwheel height (100 cm from the floor) and angle (0
• To minimize risk of injury, this study considered relatively low torque values compared to those found in practice. Higher torques might have led to different results.
6.Conclusions
The aim of this research was to compare the usability of an ergonomic valve-wrench (MW) to three conventional valve opening methods (BH, CW-R, and CW-U). The ergonomic wrench was designed to include the following features: a joint in the handle that permits angular adjustment; a handle diameter that was proven to maximize comfort; a handle length that accommodates the populations’ hand breadths; and a sleeve around the handle for minimizing friction between the hand and the wrench during handwheel actuation. Also, this study recommended incorporating a locking joint for additional stability in the handle.
The method that was associated with the least overall EMG activity of the shoulder and trunk muscles was CW-R, followed by BH, MW, and finally CW-U. However, the methods that were perceived to be the least physically demanding were MW (Borg rating
In conclusion, this study would recommend the MW for valve operation. Although it was associated with relatively high EMG activities, the EMG activities were sustained for shorter periods of time. Participants perceived it to be overall the least strenuous method.
All the valve opening methods in this study were performed at two different torque levels, 15 Nm and 30 Nm. The mean values of the times, Borg-ratings, and EMG results were significantly higher at 30 Nm than at 15 Nm. The MW was the overall preferred method at both torque levels.
7.Future research
The following research are recommended for future work:
• Test the MW among experienced valve operators and in the field, where torque requirements are much greater than those in a controlled lab study. Administer usability questionnaires to the valve operators to evaluate the design of the MW.
• Replicate the study at other handwheel heights (e.g. knee, elbow, shoulder, and overhead levels) and angles (e.g. vertical, horizontal, and slanted orientations). This research will determine the overall best valve opening method considering several handwheel positions. It can also identify the best handwheel position for cases where valve-wrenches are used.
• Consider other measures in the analysis, such as subjective discomfort ratings, oxygen consumption, and heart rate. By using additional measures more accurate conclusions can be made about the valve opening methods.
Conflict of interest
None to report.
References
[1] | Amell TK, Kumar S. Industrial handwheel actuation and the human operator: a review. International Journal of Industrial Ergonomics. (2001) ; 28: : 291-302. |
[2] | Wieszczyk SM, Marklin RW, Sanchez HJ. Height of industrial hand wheel valves affects torque exertion. Human Factors: The Journal of the Human Factors and Ergonomics Society. (2009) ; 51: (4): 487-496. |
[3] | Parks SC, Schulze LJH. The effects of valve wheel size, operation position and in-line pressures on required torque for gate valves. Process Safety Progress. (1998) ; 17: (4): 263-271. |
[4] | Jackson AS, Osburn HG, Laughery KR, Vaubel KP. Validity of isometric strength tests for predicting the capacity to crack, open, and close industrial valves. Proceedings of the Human Factors Society 36th Annual Meeting. (1992) , 688-691. |
[5] | Schulze LJH, Goldstein D, Patel A, Stanton E, Woods J. Torque production using handwheels of different size during a simulated valve operation task. International Journal of Occupational Safety and Ergonomics. (1997) ; 3: (3): 109-118. |
[6] | Wood KK, Schulze LJH, Chen J, Cleveland TG. The effects of handwheel position on torque production capability of operators. Occupational Ergonomics. (1999) /2000; 2: (1): 53-65. |
[7] | Al-Qaisi S, Aghazadeh F, Ikuma L. Effect of handwheel height and angle on operators’ torque production capabilities. IIE Transactions on Occupational Ergonomics and Human Factors. (2015) ; 3: (2): 139-149. |
[8] | Hafen BQ, Hoeger WWK. Wellness; guidelines for a healthy lifestyle. Englewood, Colorado: Morton Publishing Company; (1994) . |
[9] | Kong Y, Lowe BD. Optimal cylindrical handle diameter for grip force tasks. International Journal of Industrial Ergonomics. (2005) ; 35: : 495-507. |
[10] | NASA. Anthropometric source book, Vol. I: anthropometry for designers. Yellow Springs, Ohio: NASA Scientific Technical Information Service; (1978) . |
[11] | Perotto AO, Delagi EF, Iazzetti J, Morrison D. Anatomical guide for the electromyographer. 3 |
[12] | Farina D, Madeleine P, Graven-Nielsen T, Merletti R, Arendt-Nielsen L. Standardising surface electromyogram recordings for assessment of activity and fatigue in the human upper trapezius muscle. European Journal of Applied Physiology. (2002) ; 86: (6): 469-478. |
[13] | McGill SM. A myoelectrically based dynamic three-dimensional model to predict loads on lumbar spine tissues during lateral bending. Journal of Biomechanics. (1992) ; 25: (4): 395-414. |
[14] | Soderberg GL, Knutson LM. A guide for use and interpretation of kinesiologic electromyographic data. Physical Therapy. (2000) ; 80: (5): 485-497. |
[15] | Al-Qaisi S, Aghazadeh F. Electromyography analysis: comparison of maximum voluntary contraction methods for anterior deltoid and trapezius muscles. Procedia Manufacturing. (2015) ; 3: : 4578-4583. |
[16] | Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ. Electromyographic activity and applied load during shoulder rehabilitation exercises using elastic resistance. The American Journal of Sports Medicine. (1998) ; 26: (2): 210-220. |
[17] | Kendall FP, McCreary EK, Provance PG, Rodgers MM, Romani WA. Muscles: testing and function with posture and pain. Baltimore, Maryland: Lippencott, Williams, & Wilkins; (2005) . |
[18] | Konrad P. The ABC of EMG: a practical introduction to kinesiological electromyography. USA: Noraxon Inc; (2005) . |
[19] | Caldwell LS, Chaffin DB, Dukes-Dobos FN, Kroemer K, Laubach LL, Snook SH, Wasserman DE. A proposed standard procedure for static muscle strength testing. American Industrial Hygiene Association Journal. (1974) ; 35: (4): 201-206. |
[20] | De Salles BF, Simao R, Miranda F, Da Silva Novaes J, Lemos A, Willardson JM. Rest interval between sets in strength training. Sports Medicine. (2009) ; 39: (9): 765-777. |
[21] | Burnett A, Green J, Netto K, Rodrigues J. Examination of emg normalization methods for the study of the posterior and posterolateral neck muscles in healthy controls. Journal of Electromyography and Kinesiology. (2007) ; 17: (5): 635-641. |
[22] | Borg G. Perceived exertion as an indicator of somatic stress. Scandinavian Journal of Rehabilitation Medicine. (1970) ; 2: (2): 92-98. |
[23] | Borg G. Psychophysical bases of perceived exertion. Medicine and Science in Sports and Exercise. (1982) ; 14: (5): 377-81. |
[24] | Woldstad JC, McMulkin ML, Bussi CA. Forces applied to large hand wheels. Applied Ergonomics. (1995) ; 26: (1): 55-60. |
[25] | Meyer JP, Lodde B, Didry G, Horwat F. Cardiorespiratory and subjective strains during actuation of large hand wheels. International Journal of Industrial Ergonomics. (2000) ; 26: : 47-56. |
[26] | Wieszczyk SM, Marklin RW, Sanchez HJ. Industrial hand wheel valves: effects of height and torque direction on maximum torque and muscle activity. Human Factors and Ergonomics Society Annual Meeting Proceedings. (2008) ; 52: (15): 1020-1025. |


