
3D reconstruction computed tomography scan in diagnosis of bilateral wilm’s tumor with its embolus in right atrium
Wilms’ tumor, a rare kidney cancer, mostly affects children. It usually occurs in the first five years of life. In most cases, Wilms’ tumor affects just one kidney, though it can sometimes be simultaneously found in both kidneys. In the United States, about 500 children are diagnosed with a Wilms’ tumor each year [1]. This tumor is histologically divided into two types: favorable types of Wilms’ tumor with a better outcome that requires less aggressive treatment, anaplastic histology of Wilms’ Tumor that needs more aggressive chemotherapy and higher doses of radiation therapy. In spite of the more aggressive therapies, survival rate is generally poorer. Wilms’ tumors may grow larger without causing any pain or other symptoms. Various image technologies are used in the diagnosis of this kidney lesion or metastasized tumors, such as ultrasound [2], CT scan or enhanced CT with contrast urography [3], MRI scan, chest x-ray for detecting the spread of cancer to the lungs, and bone scan for monitoring the spread to the bones. Tissue biopsy often is taken when the affected kidney is removed during surgery, not before surgery.
CT imaging is most commonly used in the diagnosis of renal tumors, including Wilm’s Tumor [4–6] among above image diagnosis technologies. However, in clinic setting, traditional CT images are consisted of multiple images of the target tissue or organ, which is time consuming for physicians to review in more details for making precision surgery treatment strategy, especially for invasive and metastatic tumors. We here reported that a single rotated image of three-dimensional (3D) CT, instead of many 2D images in diagnosis of a case of giant Wilm’s Tumor alone with its embolus involved with the inferior vena cava and the atrium of heart.
A 3-year-old girl was referred to this hospital because of a massive tumor in abdomen. She had no hypertension and other significant medical history, and no the family history. Physical examination indicated a large solid mass in right abdomen. Laboratory tests, including blood cell count, renal function and electrolytes, were in the normal range. Serum alpha fetoprotein (AFP) and urine vanillyl mandelic acid (VMA) were negative. Ultrasonic examination (SIEMENS Sequoia512) indicated a big solid tumor in right kidney (13.0 cm×11.2 cm×9.6 cm), a solid tumor within left kidney (3.0 cm×2.5 cm×2.5 cm), a long tumor embolus (8.3 cm×2.0 cm) extended from right renal vein through inferior vena cava to right atrium. Bilateral Wilm’s tumors with embolus were diagnosed. Preoperative chemotherapy was administrated with antidrugs, i.e. vincristine, dactinomycin and adriamycin for 6 weeks (one course). Ultrasonic examination revealed that the volume of mass was reduced in left kidney, but no obvious changes on the large tumor in right kidney and the tumor embolus. To develop surgical strategy, CT scan (GE light Speed VCT 64 Slice) was performed. CT images displayed bilateral Wilm’s tumor with embolus in the intravenous and right atrium at Stage III, (Figs. 1 and 2) based on the the Children’s Oncology Group staging system in the United States [7]. Surgical procedure for removal of complex renal tumors was performed, including radical resection of tumor in right kidney, nephron-sparing surgery on left kidney tumor, plus embolectomy under cardiopulmonary bypass. The extracorporeal circulation time was 60 min and left kidney artery interruption time was 25 min. Acute renal insufficiency was occurred post-operation and recovered gradually after one course of hemodialysis. Histopathological examination of the surgical samples confirmed the favorable type of Wilm’s tumor. Eight courses of anti-cancer chemotherapy administrated with vincristine, cyclophosphamide, carboplatin / cisplatine, and adriamycin / Etoposide. The patient is in good condition now 8 months after surgery, no tumor relapse, with the renal function in normal range.
Conservative renal surgery is most commonly selected treatment option for Wilm’s tumor in children. Therefore, the precise edge detection is an important prerequisite for the open surgery. The 3D reconstructed CT used in this patient gave detailed and accurate anatomical information, and facilitated the assessment of tumor resectability, which provides a detailed road map for preoperative decision-making and predicted the postoperative management [8, 9]. Compared the observations of surgical specimen as the gold standard, 3D reconstruction image is close to the tumor specimen. Thus 3D visualization technology provides preoperative assessment and allows individualized surgical planning [10], which could be widely used in diagnosis of Wilm’s tumor, especially for the tumors at Stage III and higher stage. Although CT 3D reconstruction imaging can exhibit the entirety morphology of mass, surgeons and oncologists still need to refer to 2D CT section imaging for detail information of consistency, blood supply, margin, relationship with surrounding organs and tissues [6].
In summary, in this report, a rare case of bilateral Wilm’s tumors with embolus involved in the inferior vena cava and right atrium was diagnosed with CT 3D reconstruction. This 3D reconstructed CT exhibits accurate anatomical information in the diagnosis, which plays an important role in determining the prognosis of renal tumors, specifically for Wilm’s tumor.
Acknowledgments
Supported by the National key Clinical Specialist Construction Programs of China (No. (2013) 544).
References
[1] | |
[2] | Gao Y. , Xu M. , Xu Z.F. , Liu D.W. , Tu X.A. , Zheng Y.L. , Wang D.H. , Sun X.Z. , Zheng F.F. , Qiu S.P. , Lu M.D. , Zhang Y.Y. , Xie X.Y. and Deng C.H. , Percutaneous ultrasound-guided radiofrequency ablation treatment and genetic testing for renal cell carcinoma with Von Hippel-Lindau disease, Journal of X-ray Science and Technology 20: ((2012) ), 121–129. |
[3] | Lu X. , Wu R. , Huang X. and Zhang Y. , Noncontrast multidetector-row computed tomography scanning for detection of radiolucent calculi in acute renal insufficiency caused by bilateral ureteral obstruction of ceftriaxone crystals, Journal of X-ray Science and Technology 20: ((2012) ), 11–16. |
[4] | Khanna G. , Naranjo A. , Hoffer F. , Mullen E. , Geller J. , Gratias E.J. , Ehrlich P.F. , Perlman E.J. , Rosen N. , Grundy P. and Dome J.S. , Detection of preoperative wilms tumor rupture with CT: A report from the Children’s Oncology Group, Radiology 266: ((2013) ), 610–617. |
[5] | Pshak T.J. , Cho D.S. , Hayes K.L. and Vemulakonda V.M. , Correlation between CT-estimated tumor volume, pathologic tumor volume, and final pathologic specimen weight in children with Wilms’ tumor, Journal of Pediatric Urology 10: ((2014) ), 148–154. |
[6] | McDonald K. , Duffy P. , Chowdhury T. and McHugh K. , Added value of abdominal cross-sectional imaging (CT or MRI) in staging of Wilms’ tumours, Clinical Radiology 68: ((2013) ), 16–20. |
[7] | Kieran K and Ehrlich PF, Current surgical standards of care in Wilms tumor, Urologic Oncology 34: ((2016) ), 13–23. |
[8] | Wen J. , Hou X. , Chu X. , Xue X. and Xue Z. , Application of three dimensional reconstruction technique in selection of incision of thoracic surgical operation with robot, International Journal of Clinical and Experimental Medicine 8: ((2015) ), 17818–17823. |
[9] | Ji D. , Hu C. and Yang H. , Image reconstruction algorithm for in-line phase contrast imaging computed tomography with an improved anisotropic diffusion model, Journal of X-ray Science and Technology 23: ((2015) ), 311–320. |
[10] | Su L. , Dong Q. , Zhang H. , Zhou X. , Chen Y. , Hao X. and Li X. , Clinical application of a three-dimensional imaging technique in infants and young children with complex liver tumors, Pediatric surgery international. 2016. |
Figures and Tables
Fig.1
Surgical samples and CT images of Wilm’s tumor, intravenous and right atrium embolus. Surgical samples of the renal mass in right kidney (A), and embolus from the right aterium (B). CT image of the renal mass and embolus: cross section (C) and coronal (D) (★: Wilm’s tumor in right kidney; Φ: embolus in right atrium; *: heart; #: liver; §: residual kidney; Arrow: press mark of diaphragm surround the embolus).
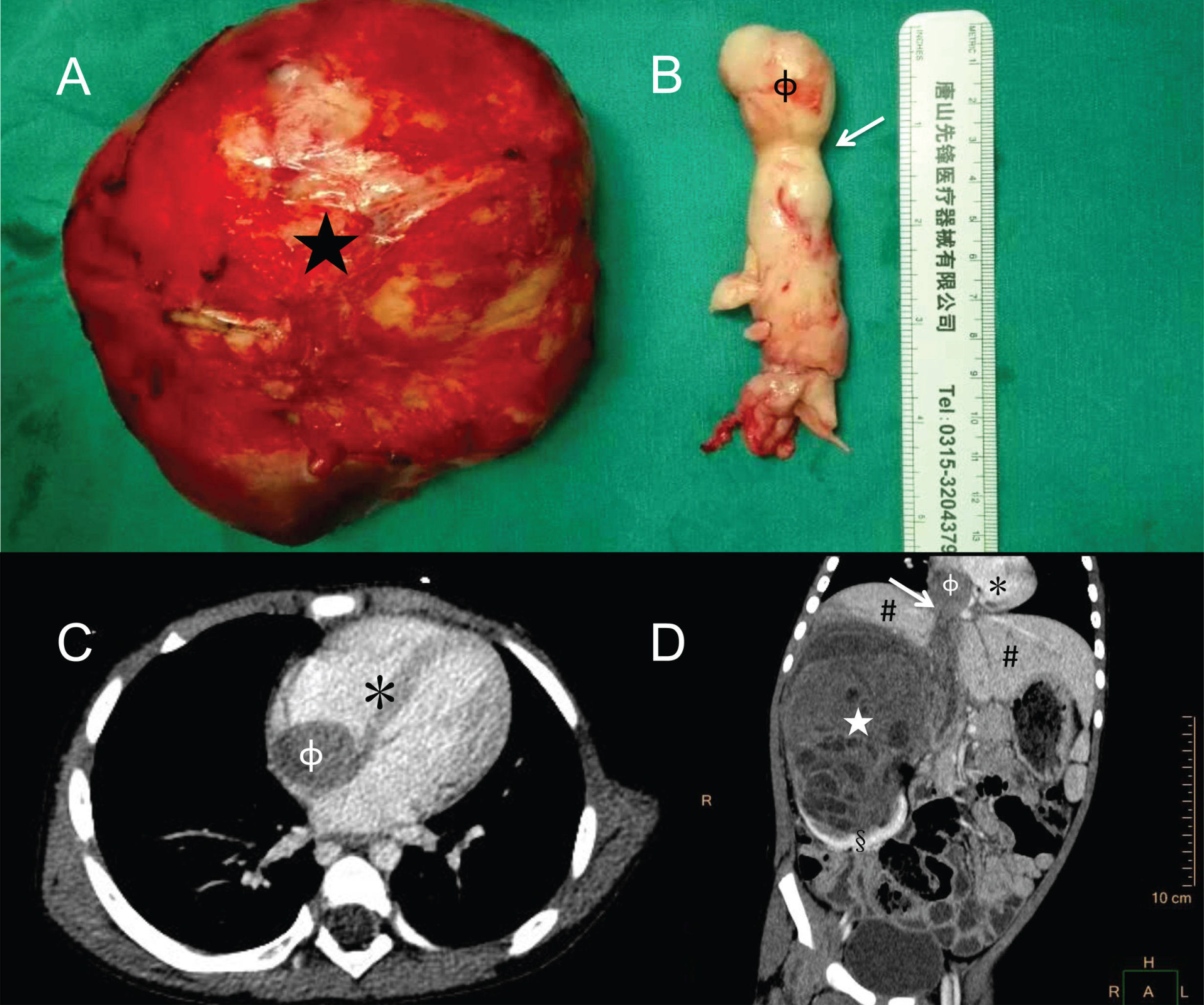
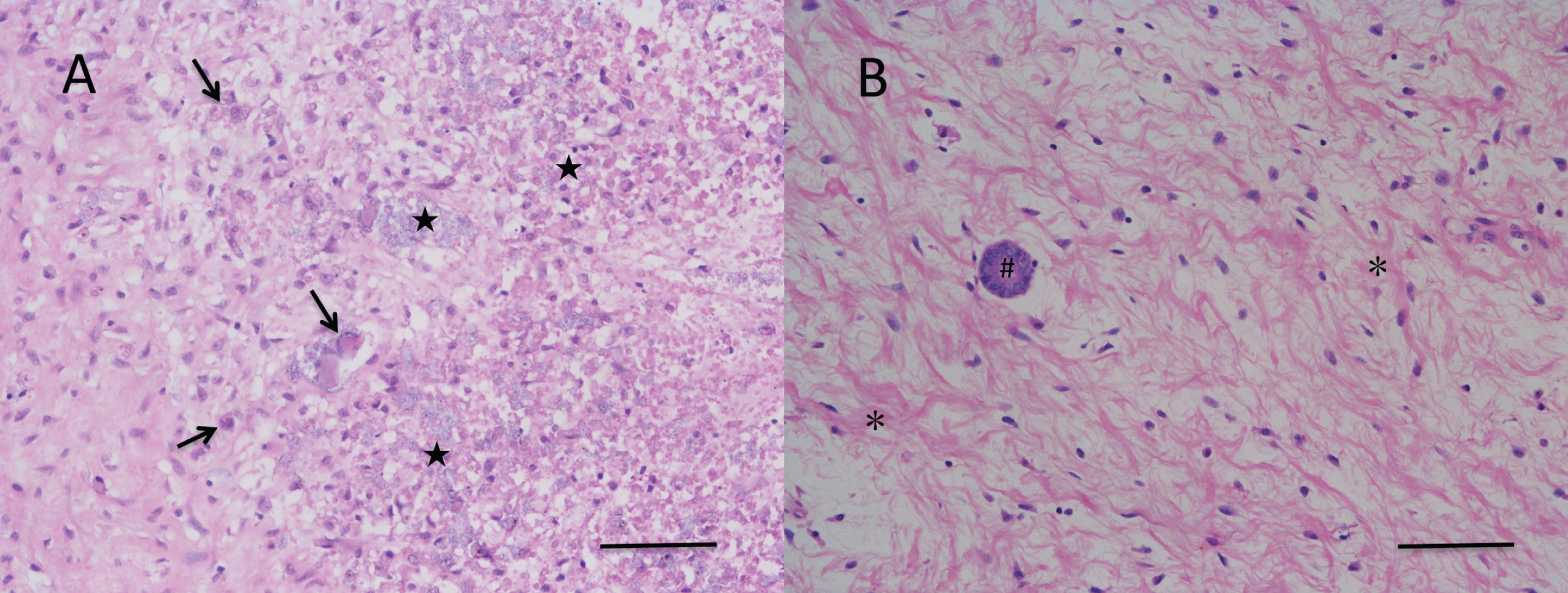
Fig.2
Histopathology of the tumor in right kidney, intravenous and right atrium embolus. (A), Patchy necrosis (★) and atypical tumor cells (arrow) were observed in intravenous and right atrium tumor embolus; (B) Kidney tubules (#), hyperplasia of spindle cell (*) but no anaplasia was found in kidney post-chemotherapy. (HE stain, bar = 100 μm).
3D Reconstruction computed tomography scan of bilateral giant Wilm’s tumor.


