
Collaboration in the context of supporting people with mental health and addiction issues into employment: A scoping review
Abstract
BACKGROUND:
People with mental health and addiction issues have significantly lower levels of labor force participation than the general population. How organizations collaborate, particularly employment and health services, influence this disparity. Whilst collaboration has been examined, investigation of the role of collaboration context is limited.
OBJECTIVE:
To identify what affects collaboration to support people with mental health and addiction issues into employment.
METHODS:
A review and synthesis of the collaborative healthcare literature identified important a priori factors at macro, meso, and micro levels. A targeted scoping review of vocational rehabilitation literature identified the collaboration factors most relevant to supporting people with mental health and addiction issues into employment.
RESULTS:
Twenty articles met the inclusion criteria for the scoping review. Whilst some factors affecting collaboration aligned across these different contexts, there were notable differences. The vocational rehabilitation literature emphasized roles and responsibilities, contracting, training and technical assistance, sharing information, relationship continuity and practitioner value alignment. There was less emphasis in the vocational rehabilitation literature on practitioners’ beliefs about collaboration, how agencies work together around the person, and on infrastructure support.
CONCLUSIONS:
Collaboration in the context of supporting people with mental health and addiction issues into employment needs planning and support. Whilst many factors known to enable collaboration remain important, the collaboration context matters.
1Introduction
People of working-age living with mental health and addiction issues have significantly reduced labor force participation when compared to the general population (Jonsdottir & Waghorn, 2015). This disparity is greatest for people with diagnoses including schizophrenia, bi-polar disorder, clinical depression, and substance use disorders. There are also greater economic inequities for indigenous people and people from ethnic minority groups who have mental health and addiction issues (Jonsdottir & Waghorn, 2015; Priest & Lockett., 2020; Prinz, Lockett, Arends, & Stermsek, 2018).
At both policy and practice levels the importance of collaboration, particularly across health, welfare and employment services, has been identified as crucial to improving the labor force status of people with mental health and addiction issues (Organisation for Economic Co-operation and Development (OECD), 2015a). Integrated welfare, education, health and workplace systems and policy are recommended (OECD), 2015b). This is because no one agency or organization can address these disparities in isolation – actions in one part of the system are interrelated and interdependent on other parts of the system (Arends, Baer, Miranda, Prinz, & Singh, 2014). For example, people who are unemployed with symptoms of depression may need mental health or addiction treatment at the same time as receiving help to look for and secure employment. Similarly, the way the workplace responds to employees with mental distress influences the person’s likelihood of staying at work and maintaining good mental health whilst working. Yet, despite the knowledge of the importance of integrated health and employment policy and services, integrated services are not routinely available (Bond, Lockett, & van Weeghel, 2020; Cram et al., 2020) and collaborative policymaking across health, employment and welfare agencies remains the exception rather than business as usual (OECD, 2021).
Collaboration as a mechanism to support policy and service integration has been reasonably well explored in the delivery of health treatment services, particularly models of collaborative care (D’Amour, Ferrada-Videla, San Martin Rodriguez, & Beaulieu, 2005; Mulvale, Embrett, & Razavi, 2016; Overbeck, Davidsen, & Kousgaard, 2016). However, collaborative healthcare usually involves practitioners with the closely aligned objective of improving patient clinical symptoms and with health practitioners frequently coming from within a single organization (D’Amour et al., 2005).
When the context, that is the setting and the focus, is different and is concerned with supporting people with mental health and addiction issues to secure and maintain competitive employment, there is frequently a fundamental disconnect between the primary aims of health services and those of employment support and welfare services (Lockett & Bensemann, 2013). “Medical services aim to treat people and improve symptoms and daily life functioning, with very limited attention to employment and workplace issues. Employment services aim to reintegrate people into work through activation and training but do not address frequently occurring health issues of clients or wait until ‘cured’ clients return from treatment” (Arends et al., 2014, p. 5).
Furthermore, the funding and delivery of health services and employment services usually falls across two or more government agencies, which in the absence of integrated policymaking reinforces the separate delivery of health and employment services (Bond et al., 2020; Drake, Bond, Goldman, Hogan, & Karakus, 2016; Lockett, Waghorn, & Kydd, 2018, OECD, 2021).
Whilst collaboration in healthcare settings has been examined, investigation of the role of collaboration context is limited, and particularly as this relates to who needs to collaborate and how this is best achieved to support people with mental health and addiction issues into employment. The aim of this scoping review was therefore to address this knowledge gap. The research questions that guided the review were:
RQ1. For people experiencing mental health and addiction issues, what are the factors affecting collaboration in the context of supporting people to get and sustain employment?
RQ2. To what extent are these factors distinct or different from collaboration in health settings more generally?
2Methods
This scoping review is part of a wider research program. The scoping review was undertaken to inform the method for an empirical investigation on how to implement effective collaboration to improve employment outcomes for people with mental health and addiction issues. The ultimate aim of the wider research program, and therefore also of this scoping review, is to provide evidence to inform practice. Others have argued that informing practice, as distinct from addressing effectiveness, is one of the main reasons that a scoping review would be chosen as a method instead of a systematic review (Munn et al., 2018). Other reasons for a scoping review, again consistent with the overall aim of the research, are to identify: 1) key characteristics or factors related to a concept, and; 2) the types of evidence in a given field (Peters et al., 2015). It is for these reasons that a scoping review was chosen.
There were two distinct reviews undertaken as part of the methods for scoping review, which were conducted in parallel by the research team. The review of the vocational rehabilitation literature to identify papers meeting the inclusion criteria, and the review of systematic reviews in the collaborative healthcare literature to develop the a priori coding structure used subsequently for extracting data.
2.1Data collection – review of the vocational rehabilitation literature
The protocol for the scoping review was developed using the guidelines provided by the Joanna Briggs Institute Reviewer’s Manual (Peters et al., 2015). To be included in the review the papers needed to focus on a population with mental health and addiction issues, report results related to some type of collaborative endeavor (collaboration, coordinated care, integrated services), and report on initiatives explicitly aimed to improve employment outcomes. Papers were included if they were published since 1996. This year was chosen because the first randomized controlled trial of integrated employment support in mental health and addiction services was published (Drake & Bond, 2017). Papers were also included if they were written in the English language and were conducted in an OECD country. OECD countries have relatively comparable policy and funding environments and a shared commitment to build integrated systems for health, work and skills (OECD, 2015). Given the aims of the scoping review, to map out the available types of evidence a range of study designs were included.
The following bibliographic databases were searched for relevant papers published from 1996 to August 2019: MEDLINE, EMBASE, CINAHL, PsychInfo, and the OECD library. The search strategy was developed by the research team, with the final search results exported into RefWorks. The electronic database search was supplemented by hand searching relevant key journals, including International Journal of Integrated Care, Psychiatric Rehabilitation Journal, Health and Social Work, and Journal of Vocational Rehabilitation.
The initial search was conducted by the first author [MKW], and peer reviewed by the research team. The search terms were (mental health OR mental illness OR substance use OR addiction OR drug dependence OR alcohol dependence) AND (employment OR employment support*) AND (case management OR coordination OR collaboration OR integration). In accordance with the inclusion and exclusion criteria, the search was limited to papers published in the English language and published between 1996 and August 2019.
To increase the reliability of the search two researchers conducted the title check and abstract scan of all papers that resulted from the initial search. To aid this checking process, and ensure interrater consistency, the whole study team took the same five papers to determine if they met the inclusion criteria. This process was used to refine the abstract screening phase. Papers that passed the abstract screen then proceeded to a full paper to be read and assessed against the inclusion criteria.
2.2Developing the coding structure
To capture and code the findings on factors affecting collaboration from the vocational rehabilitation scoping review papers a coding structure was developed a priori. This structure was developed through a review of systematic reviews of collaboration, specifically within the collaborative healthcare literature. Collaborative healthcare was chosen because it is an area that has received significant attention over the last 20 years (Davy et al., 2015). It looks at collaboration both with the individual patient and collaboration within healthcare organisations (Körner et al., 2016).
To identify these reviews of collaborative healthcare CINAHL was used, searching for systematic reviews that had the terms ‘collaborative care’ or ‘integrated care’ in the title. The abstracts in the returned papers that included a discussion on factors affecting collaboration were reviewed. Each paper was read by research team member [GH] to capture the factors affecting collaboration for delivering models of collaborative healthcare.
The review of papers stopped once saturation of the themes reported in the papers was reached. This resulted in seven papers guiding the coding structure (D’Amour et al., 2005; Karam, Brault, Van Durme, & Macq, 2018; Morgan, Pullon, & McKinlay, 2015; Mulvale et al., 2016; Overbeck et al., 2016; San Martín-Rodríguez, Beaulieu, D’Amour, & Ferrada-Videla, 2005; Wood, Ohlsen, & Ricketts, 2017).
Next each of the seven review studies was re-read to build a conceptual explanation for each factor. For example, the theme of physical space was identified and conceptually defined as ‘sufficient physical space to work together formally, and or informally which supports communication and relationship building’. (For the coding structure refer to the Appendix). To help organize the themes, three categories were used based on the level the factors were operating - macro, meso or micro (Bronfenbrenner, 1979; Durlak & DuPre, 2008). Macro level factors impact externally on organisations and affect governance arrangements and resourcing such as funding, policy, and legislation. Meso factors were within organisations, for example management and leadership, inter-agency agreements, organizational policies and procedures, workforce development. Micro factors were those primarily impacting at the practitioner level, including individual values, beliefs, attitudes, and experiences.
2.3Data extraction and analysis
To guide the extraction of data from the included papers from the vocational rehabilitation literature, a one-page template was developed. The template included details on the research questions, method, participants, outcomes, and factors affecting collaboration. The final set of included papers was divided up amongst the five members of the research team. Each team member wrote a one-page summary for the papers they were allocated and then met to discuss and resolve any differences by discussion. The bias of any individual study was not assessed because the aim was to map the evidence, rather than to inform clinical practice (Peters et al., 2015).
For the next stage of the data analysis, the Excel spreadsheet was populated by each team member as each of the included articles was re-reviewed. Each included study formed a row, with the a priori coding structure of macro, meso and micro factors forming the columns. This assisted each team member to extract data at the factor level from the included paper. As team members identified any factors that were not in the a priori coding structure, these were added as factors in new columns.
Once this process was completed for all the included papers the factors that emerged were consolidated and the key factors affecting collaboration in vocational rehabilitation were identified. Next these factors were compared and contrasted with factors that emerged as important in the collaborative healthcare literature, to identify areas of alignment and difference.
3Results
3.1Literature search
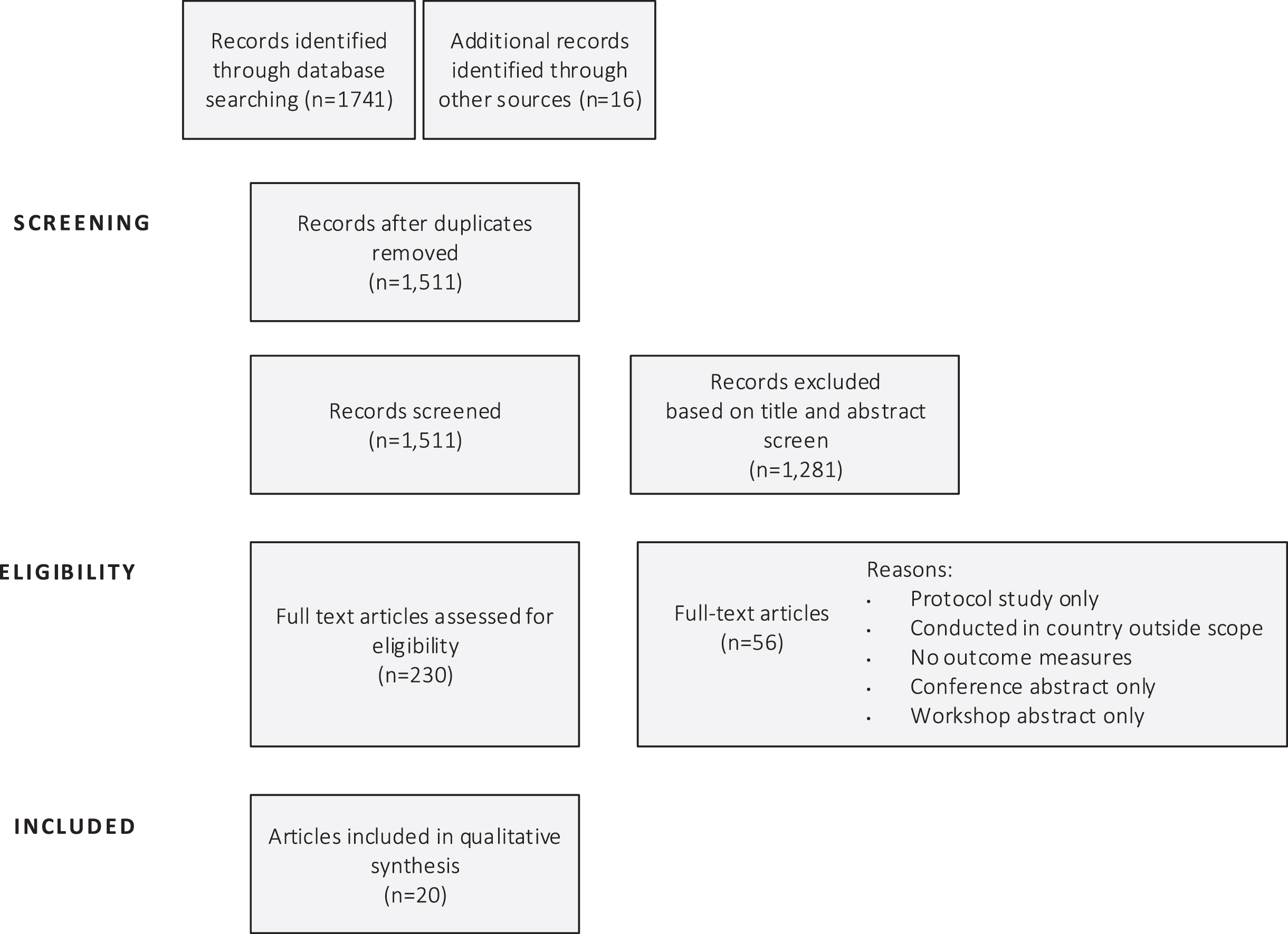
A total of 1,511 titles and abstracts and 230 full-text articles were assessed for eligibility. From this, 20 studies were finally included, with reasons for excluding full-text articles provided (see Fig. 1).
Fig. 1
PRISMA diagram for the scoping review.
3.2Characteristics of the included studies
The 20 included studies came from seven countries. Most were from the USA (n = 7), four each from Sweden and New Zealand, two from Australia and The Netherlands (2), and one conducted in the UK. The majority of the studies had a qualitative design (interview-based or case study). Only one study was a controlled trial design. In terms of participants in the collaboration, all included papers were investigating the collaboration between health practitioners, vocational rehabilitation specialists (working in government and non-government employment services), and government welfare agencies (i.e., social security or social insurance agencies). Of the included studies, only two had a specific focus on people with addiction, and one focused on people with a dual diagnosis of mental health and addiction issues.
Whilst all included studies had an explicit focus on supporting people into employment, only four reported employment outcomes. All studies reported on other outcomes from collaboration related to service delivery and staff and participant engagement. For example, improved information sharing and referral pathways, or a greater commitment across agencies to improve employment outcomes. There was also evidence of collaboration leading to health practitioners seeing the value of employment, and a shift in attitudes across health, welfare and employment services staff. A description of the included studies is presented in Table 1.
Table 1
Factors affecting collaboration and the outcomes from collaboration: Summary of included studies in the review of vocational rehabilitation literature (n = 20)
| First author, date | Study title | Country | Study design | Factors affecting collaboration | The outcomes from collaboration |
| Becker, 2007 | Critical strategies for implementing supported employment. | USA (seven States) | Case study | •MoU between VR and MH to delineate roles and responsibilities in relation to employment. | •Streamlined the referral pathways between agencies. |
| •Blended financing structure and tied to outcomes-based contracts. •Regular leadership team meetings to oversee delivery and re-align policy. | •Improved the commitment across agencies to improve employment outcomes | ||||
| •On-site training and technical assistance •Leaders modelled flexibility and commitment. | |||||
| •Leaders modelled flexibility and commitment. | |||||
| Becker, 2005 | Supported employment for people with co-occurring mental health and addiction issues. | USA | Qualitative study | •The team consider the individual carefully in terms of interests, skills, work history, coping strategies. | •A team approach helps mitigate the impact of addiction and MH issues on employment outcomes. E.g., members of the treatment team collaborate to identify the individual’s strengths, skills, coping mechanisms and triggers to identify jobs, work settings and supports that promote abstinence and recovery. |
| •In the engagement phase of treatment team forms a collaborative relationship around the person. | •Better sharing of information to promote timely, coordinated, holistic support and better understanding of the person to help with job search process. | ||||
| •Regular team meetings | •Whole team supports the individual through all phases of their employment journey. | ||||
| •Shared vocational plan between the agencies | |||||
| Bejerholm, 2011 | Individual placement and support illustrated in the Swedish welfare system: A case study. | Sweden | Case study | •Welfare regulations and policy meant people were required to do some pre-vocational training before accessing open employment and also that ES were not allowed to provide continuous support to people once in employment. | •Person dropped out of support/lost hope. |
| •Regular meetings between agencies were held, but lack of local autonomy to implement rules meant meetings focused mainly on information sharing rather than problem solving. | •ES stopped working with public employment service and welfare agency. | ||||
| •Different understanding and definition of work capacity between agencies | •Lower level of fidelity to evidence-based practices in supported employment | ||||
| •Practitioners worked to the regulations even if these contradicted the person/clients’ interests and support needs. | |||||
| •Power in balance, government agency rules dominated | |||||
| Browne, 2009 | Developing high performing employment services for people with mental illness. | New Zealand | Qualitative | •Funding and contracting systems impeded collaboration | •Influences who the employment service can work with |
| Drake, 2003 | A process analysis of integrated and non-integrated approaches to supported employment. | USA | Qualitative and quantitative | •Clear identification of cross government responsibilities and contracting. | •Increased information sharing, increased learning across disciplines |
| •Effective leadership at all levels | •Changed the culture of mental health services, clinicians changed the value they saw on work | ||||
| •Shared commitment ES and MH practitioners | |||||
| •Regular sharing of information into same support plan | |||||
| •Change in attitudes of clinicians, seeing value of employment | |||||
| Germundsson, 2012 | Vocational rehabilitation, interagency collaboration, and social representations. | Sweden | Qualitative | •Work demands impacts on ability to collaborate. | •Increased knowledge about the role of each agency increased collaboration |
| •Continuity of relationships and workers | •Improves the efficiency of each agency. | ||||
| •Builds trust, shared decision-making. | |||||
| •Absence of an ‘important actor’ | |||||
| Germundsson, 2011 | Interagency collaboration in vocational rehabilitation for persons with mental health problems: the perspective of the service users and the professionals. | Sweden | Qualitative | •Availability of resources | •Collaboration enhanced their mutual understanding of each other’s activities. |
| •How the collaboration is organized and managed | •Recognized the legitimacy of others’ knowledge. | ||||
| •The recognition that other agencies have something to contribute. | |||||
| •Mutual trust and respect | |||||
| •Time constraints and management inflexibility impact on collaboration | |||||
| Glenn, 2008 | Building collaboration in substance use treatment and vocational rehabilitation. | USA | Qualitative | •Cross-training of staff and on-site technical assistance | •Changing staff attitudes towards peoples’ employability |
| •Regular joint meetings to problem solve. | |||||
| •Having dedicated time for collaboration | |||||
| Gordon, 2001 | Developing services for people with mental health problems in the New Deal for Disabled People personal advisor pilots. | UK | Case study | •Expectations of involvement and clear requirements of each role in the program. | •Improved the performance of the public employment services, by increasing the number of people with MH issues participating and number gaining employment or entering vocational training |
| •Joint steering group and cross-agency secondment of staff | |||||
| •Directions from management regarding the coaches and therapists’ respective areas of responsibility. | |||||
| •Peer support | |||||
| •Training employment staff in mental health | |||||
| •Time. Collaboration between organizations were considered time consuming, developed a framework for collaboration. | |||||
| Hanrahan, 2006 | Limitations of system integration in providing employment services for persons with mental illness. | USA | Survey | •Mental health and vocational rehabilitation specialists found that differences in philosophies, goals, mandates, and expectations of services were identified as creating problems between and among agencies. | •More frequent meetings and regular follow up associated with successful employment outcomes. |
| •Staff training in supported employment has often been utilized to facilitate collaboration. | •Found an association between staff attending interagency training and meetings and the employment outcomes of that agency. | ||||
| •Quality of relationships between staff in the agencies, more than actual collaborative activities, which predicts success in employment outcomes. | |||||
| Holwerda, 2016 | Collaboration between mental health and employment services to support employment of individuals with mental disorders. | The Netherlands | Survey | •A national formal agreement between MH and welfare services | •Increased knowledge of the people in collaborating agencies, sharing of client information. |
| •Putting a structure around collaboration, rather than ad hoc. | •Collaboration with other agencies also improved. | ||||
| •Shared positive views on the importance of teamwork. | •All agencies considered collaboration helped them support their clients. | ||||
| •Knowledge of each other’s organizations. | |||||
| Kemp, 2004 | Developing Employment Services for Criminal Justice Clients Enrolled in Drug User Treatment Programs. | USA | Trial | •Openness re: needs, resources, mutual trust, | •Coordination of information and developed linkages to employers. |
| •Joint policy development and decision making. | •Fifty-four percent obtained employment. | ||||
| •Monthly meetings to problem solve. | |||||
| •Communication negotiation between agencies where original goals were complicated. Philosophies of change need to be congruent and compatible. Philosophies are the same at client level. | |||||
| •Practical solutions, flexibility, transparency. | |||||
| King, 2006 | Enhancing employment services for people with severe mental illness: The challenge of the Australian service environment. | Australia | Qualitative | •National and state policy | •Clinicians and ES coordinate their work with clients. Clinicians consider vocational goals when implementing treatment and care plans. |
| •VR bought under the responsibility of one federal agency, previously split across several agencies. | •Formal communication structures and protocols established between agencies, supported by regular meetings and cross-training | ||||
| Marrone, 2014 | Vocational rehabilitation and mental health employment services: True love or marriage of convenience? | USA | Case study | •Formal system partnership between VR and MH | •Shared belief that target population can work. |
| •Interagency agreements and joint funding responsibilities | •Clear and mandated referral pathways. | ||||
| •Cross-agency steering group and training. | •The establishment of a technical assistance center to support VR and MH agencies to collaborate. | ||||
| •Shared measures of success and outcome measures. | |||||
| •Aligned contracts and staff performance measures. | |||||
| •Senior MH leader who placed employment core to MH services. | |||||
| •Clear and consistent messaging across all agencies | |||||
| Nepe, 2011 | Enhancing mental health services through joint delivery with employment and other essential community services: early lessons from an innovative New Zealand program. | New Zealand | Case study | •Equitable and joint governance structure | •Improved outcomes for clients. |
| •Communications strategies and discussion forums | •Changes in staff attitudes. | ||||
| •On-site leadership | |||||
| •Lack of clarity on organizational boundaries | |||||
| •Sharing of information | |||||
| •Organizational culture | |||||
| •Inter-agency competition | |||||
| Porteous, 2007 | Implementing evidence-based employment services in New Zealand for young adults with psychosis: progress during the first five years. | New Zealand | Case study | •Sharing data increases cross agency engagement, a common outcome measurement | •Improved outcomes for clients. |
| •49% achieved vocational outcomes in year 1 and 59% in year 2. | |||||
| •Staff attitudes changed. | |||||
| Porter, 2018 | Critical factors for the return-to-work process among people with affective disorders: Voices from two vocational approaches. | Sweden | Qualitative | •Bureaucratic structures and regulatory and budgetary processes | •Clients experience hope, power, and support from MH and VR professionals |
| •Clients did not like it when MH treatment was separate from the employment support service. | |||||
| •Continuity of support for the individual | |||||
| •Individuals needs lead the process. | |||||
| •Genuine interest and engagement from all those who provide support. | |||||
| •Whether the family is part of the process or not | |||||
| Vukadin, 2018 | Experiences with the implementation of Individual Placement and Support for people with severe mental illness: A qualitative study among stakeholders. | The Netherlands | Qualitative | •Regular meetings of managers and practitioners, Policy and funding supporting collaboration. | •Stakeholders viewed the collaboration as successful. |
| •Belief in and ownership of the innovation | •Improved the communication across agencies and practitioners. | ||||
| •Communication and regular meetings | •Built shared belief/values between ES and MH practitioners | ||||
| •Staff attitudes and beliefs | •Increased trust and respect in partners’ judgements and expertise | ||||
| •Legislation | |||||
| •Joint agency financial strategy | |||||
| •Duration of funding | |||||
| •Mandate from decision makers | |||||
| •Formal agreement clarifying roles and responsibilities. | |||||
| Waghorn, 2011 | The importance of service integration in developing effective employment services for people with severe mental health conditions. | New Zealand | Observational | •Funding and contracting terms and conditions | •Referral pathways / service access |
| •Seventy-four percent achieved employment outcomes | |||||
| Waghorn, 2007 | Challenges to implementing evidence-based supported employment in Australia. | Australia | Multi-site case study | •Funding and contracting terms and conditions | •Improves employment outcomes. |
| •Funding the time it takes to collaborate | |||||
| •Confidentiality, insurance, and related legal issues | |||||
| •Resources (e.g., car, mobile phone) Training on collaboration and cross-training | |||||
| •Have a set of EBPs against which to assess levels of collaboration. | |||||
| •Organizational cultures | |||||
| •MoU between agencies |
Notes. N = number of included studies. ES = Employment Specialist. MH = mental health. VR = vocational rehabilitation. SI = social insurance. MoU = Memorandum of Understanding.
3.3Factors affecting collaboration in vocational rehabilitation
The core question for this scoping review was to understand the factors affecting collaboration in the context of supporting people with mental health and addiction issues to get and keep employment. In reporting the results of this review, the authors drew on the framing that structured factors into macro, meso and micro levels (Durlak & DuPre, 2008). Table 2 presents these results, comparing factors found in this vocational rehabilitation scoping review to those found in the review of systematic reviews of collaborative healthcare. Notably, there were sixteen factors which were found in both the collaborative healthcare literature and vocational rehabilitation literature, six factors in the vocational rehabilitation literature that were not present in the collaborative healthcare literature, and four factors in the collaborative healthcare literature that were not found in the scoping review.
Table 2
Factors affecting collaboration in vocational rehabilitation: A comparison with the collaborative healthcare literature
| Factors affecting collaboration | Count of studies identifying factor in the collaborative healthcare literature | Factor also identified as important in vocational rehabilitation literature |
| Macro level | ||
| Funding, financing and resourcing | 3 | Y |
| Contracting | 01 | Y |
| Government policies and planning | 2 | Y |
| Legislation and regulatory frameworks | 2 | Y |
| Meso level | ||
| Formalization of processes | 4 | Y |
| Shared vision and objectives | 4 | Y |
| Shared organizational values | 3 | Y |
| Management and leadership | 4 | Y |
| Systems for frequent and clear communication | 6 | Y |
| Clarification of roles and responsibilities | 3 | Y |
| Creating physical space | 4 | Y |
| Shared client focus | 3 | N |
| Client participates in the collaboration | 2 | N |
| Appropriate administrative and IT support | 4 | N |
| Training and technical assistance | 0 | A2 |
| Support for innovation, adaptable | 3 | Y |
| Mechanisms to feedback information and outcomes | 0 | A |
| Shared referral systems | 0 | A |
| Micro level | ||
| Mutual trust and respect | 3 | Y |
| Shared knowledge and responsibilities | 5 | Y |
| Shared power | 2 | Y |
| Role clarity | 4 | Y |
| Belief in collaboration | 2 | N |
| Willingness to collaborate | 4 | Y |
| Alignment of values | 0 | A |
| Continuity of relationships | 0 | A |
Notes. Y = Yes. N = No. A = Additional. 1. Contracting was conceptualized as part of funding and resources. 2. Factors was identified as important to collaboration in the vocational rehabilitation literature but not in the collaborative healthcare literature.
3.3.1Macro factors
The findings from the vocational rehabilitation literature review were generally consistent with the findings from the generic literature on collaboration in healthcare. The three macro factors: (1) funding, financing and resourcing, (2) government policies and planning, and; (3) legislation and regulatory frameworks, were all identified as important enablers and barriers to collaboration. The vocational rehabilitation literature highlighted the importance of joint government and cross-agency funding mechanisms (Marrone, Burns, & Taylor, 2014; Vukadin, Schaafsma, Westerman, Michon, & Anema, 2018), re-organization of funds (Becker et al., 2007; Kemp, Savitz, Thompson, & Zanis, 2004), and a lead agency for funding (Drake, Becker, Bond, & Mueser, 2003; King et al., 2006). Having formal agreements for the provision of joint services was also identified as important (Becker et al., 2007; Holwerda, Fokkens, Engbers, & Brouwer, 2016), with examples of government agencies acting separately considered as a major barrier to collaboration between mental health and vocational rehabilitation agencies (Hanrahan, Heiser, Cooper, Oulvey, & Luchins, 2006). The studies also emphasized the importance of the right legislative framework. For example, in one Swedish study, national welfare legislation led to organizational rules overshadowing individual aspirations. This resulted in participants dropping out of employment support services and a lack of co-operation between the vocational rehabilitation provider and the welfare agency (Bejerholm, Larsson, & Hofgren, 2011).
In terms of any differences in the macro factors, the vocational rehabilitation literature gave a greater and a specific emphasis on the role of contracting in enabling or inhibiting collaboration between agencies. Examples included contracts that limited how long agencies could keep supporting individuals once working (Germundsson et al., 2011), contracting specifically to deliver employment outcomes (Browne et al., 2009), and contracting to encourage fidelity to evidence-based practices (Hanrahan et al., 2006). This contrasted with the collaborative healthcare literature where contracting was not specifically highlighted but rather incorporated into financing and resourcing.
3.3.2Meso factors
Eight of the eleven meso factors identified as important in the review of the vocational rehabilitation literature aligned with those from the collaborative healthcare literature. These were: (1) formalization of processes for collaboration; (2) shared vision and objectives; (3) shared organizational values; (4) management and leadership; (5) systems for frequent and clear communication; (6) clarification of roles and responsibilities; (7) creating physical space, and; (8) a culture within the organization which promotes adaptability and a willing to take on new things (Becker et al., 2007; Bejerholm et al., 2011, Germundsson et al., 2012; Glenn & Moore 2008, Gordon & Mills, 2001). Formalization of processes for collaboration included examples of protocols and memorandums of understanding (MoUs) which allowed staff to spend time on collaboration, and dedicated regular meetings for the transfer of knowledge and to problem solve (Becker et al., 2007; Holwerda et al., 2016; Marrone et al., 2014; Porter et al., 2018). Terms of reference assisted with clarifying things such as group membership, meeting regularity, the roles and responsibilities of each organization. These structural arrangements aided communication and built a joint commitment to the goals of improved mental health and employment outcomes, and if missing, inhibited collaboration (Vukadin et al., 2018). Studies gave examples of where organisations altered their philosophies, for example mental health agencies gave a greater focus on employment and employment agencies took a greater focus on mental health (Becker et al., 2007; Marrone et al., 2014). In contrast, a lack of buy-in and role-modelling from senior mental health or vocational rehabilitation leaders was identified as inhibiting collaboration (Germundsson et al., 2012).
Whilst there was generally alignment across the two bodies of literature, there was also some notable differences. The vocational rehabilitation literature had a stronger emphasis on the importance of training, particularly cross-agency training and on access to technical assistance (Hanrahan et al., 2006), shared referral systems, and on the development of mechanisms to feedback information and outcomes (Becker, Drake, & Naughton, 2005; Drake et al., 2003), than the collaborative healthcare literature.
There were also meso factors important in the collaborative healthcare literature but not emphasized in the vocational rehabilitation examined. These were: (1) shared client focus including shared plans and joint monitoring and systematic feedback to the client (D’Amour et al., 2005; Overbeck et al., 2016; Wood et al., 2017); (2) client participation and awareness, particularly client participation in decision-making and the client’s awareness of the collaboration (D’Amour et al., 2005; Karam et al., 2018), and; (3) sufficient administration, human resources, and information technology especially integrated information systems for information sharing (Karam et al., 2018; Mulvale et al., 2016; Overbeck et al., 2016; San Martin-Rodriguez et al., 2005).
3.3.3Micro factors
The review of the collaborative healthcare literature identified six micro factors. Five of these were also found in the vocational rehabilitation literature, these were: (1) mutual trust and respect; (2) shared knowledge and responsibilities; (3) shared power (e.g., consensus in decision making and peer workers); (4) practitioners’ role clarity and understanding of the role of their team and team members, and; (5) willing to collaborate and be flexible (Germundsson et al., 2012; Gordon & Mills., 2001; Hanrahan et al., 2006). As one study stated, “although professionals of mental health services and social security insurance only recently started working together, they seem to have a strong awareness of needing each other in the process of helping clients to improve work outcomes” (Holwerda et al., 2016, p. 1254).
There were two factors identified as important in the vocational rehabilitation not highlighted in the collaborative healthcare literature. These were: (1) alignment of values, and; (2) continuity of relationships. Alignment of values at the practitioner level was particularly important where staff were coming from different professional backgrounds and training (Bejerholm et al., 2011). The literature also highlighted the importance of a shared belief that the person can work, and the importance of maintaining optimism and hope. “Staff must instill hope and a belief that people can recover and work, even when they have given up on themselves” (Becker et al., 2005, p. 333).
4Discussion
This paper responds to an international call to better support collaboration between mental health, welfare, and employment support services to improve the labor force participation of working-age people living with mental health and addition issues (OECD, 2015; 2018). This scoping review brings together the emerging evidence on the factors supporting and inhibiting collaboration within this policy, funding and delivery context.
Whilst overall there was alignment in terms of the factors important to supporting or inhibiting collaboration there were some interesting differences. These differences indicate that some areas need particular attention to enable effective collaboration to support people with mental health and addiction issues into employment.
The first area relates to contracting. Evidence identified the importance of a contract that explicitly outlines the roles and responsibilities of the respective organisations. The contract typically outlines a shared governance arrangement and is supported with a clear MoU. The importance of contracting is likely to be a more important factor where there are different agencies trying to coordinate support around an individual and particularly where the respective organizations have different worldviews and organizational systems. A clear contract can help to make the importance of collaboration more explicit for each party.
The second area of notable difference in vocational rehabilitation is the importance of cross agency training and the provision of technical assistance. Training and technical assistance were found to be important to help build a common understanding across the parties and help to build mutual understanding and trust. Again, given the different primary focus of organizations, it is likely that these intentional implementation strategies are critical to supporting practitioners across different organizations to help familiarize themselves with each other and support working together.
Also identified as important at a meso level in vocational rehabilitation but not in the collaborative healthcare literature, is the need for shared referral systems and feedback mechanisms. These both relate to the infrastructure needed to communicate across organizations and systems that previously had little need to interact. The evidence indicates that a clear and shared system for referrals is needed as people pass through different organizational administrative systems, to support client engagement (Becker et al., 2007). Equally important is a mechanism to feedback to the referring agency, thereby closing the communication loop, both in terms of feeding back on client progress and outcomes.
At a micro-level the alignment of practitioner values and the importance of continuity of relationships were highlighted as important to collaboration in vocational rehabilitation. Collaboration is more likely to be successful when people in the selected partner agencies have previously worked with each other. Continuity of relationships was also identified as important from the perspective of clients. For both clients and practitioners, continuity of relationships likely aids the growth of familiarity, trust building, and the provision of consistency of support.
There were also factors identified as important in the collaborative healthcare literature but not highlighted as important in the vocational rehabilitation literature. Most notably was an absence of evidence of the role of the client – either the client as a shared focus in the collaboration, or the client as part of the collaboration. This finding was surprising given the importance of person-centered practice in vocational rehabilitation (Drake, 2020). The pathway to collaboration emphasized in the vocational rehabilitation examined in this review had a much greater focus on the structural mechanisms of contracts, funding, MoU, and joint governance.
The evidence presented in this review has several implications for policy and practice. Of most relevance is that collaboration does not just happen. Collaboration needs to be well planned and supported. If the policy call to increase collaboration across agencies working in vocational rehabilitation is to be realized, then policy needs to be complemented with clear guidelines. These guidelines would helpfully include advice of how to develop contracts for collaboration, strategies to support the alignment of values, and training on effective collaboration. In addition, funding from central agencies to support this collaboration should consider such things as additional funding for secondments, training and technical assistance, investment to support shared referral systems, and longer-term funding to support the continuity of relationships.
This scoping review is an early effort to bring together the evidence on collaboration in vocational rehabilitation. There were limitations in conducting a scoping review rather than a systematic review, and therefore it is possible that not all the available evidence were identified. Furthermore, the quality of the papers was not assessed, and papers were included whether or not they reported employment outcomes. As such, while the review outlines factors that studies report affect collaboration, it is unclear the extent to which these factors are fundamental to achieving employment outcomes for people with mental health and addiction issues. Given there were only four studies in the included papers that reported on employment outcomes, it is likely that this is an area that would merit further research.
5Conclusion
Despite the limitations this scoping review has drawn together evidence which could guide the intentional design of collaboration across agencies to support people with mental health and addiction issues into employment. The review highlights several important and distinctive factors. These distinctive factors appear due to the fact that in vocational rehabilitation two or more agencies are providing support to an individual, rather than a single healthcare provider. In vocational rehabilitation, the agencies and practitioners involved are also frequently coming from very different priorities and worldviews. For example, in the case of employment support practitioners and organizations, the value of employment to recovery and wellbeing is central, for health services symptom reduction is often paramount, and for welfare agencies the principal aim is usually reducing a person’s reliance on welfare payments. Given these competing demands, an explicitly designed process and set of support for collaboration is key.
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
Funding for this study was received from the Health Research Council of New Zealand (reference 18/821).
Ethical approval
This study, as a scoping review, was exempt from Institutional Review Board approval.
Informed consent
This study, as a scoping review, did not interview participants.
References
1 | Arends, I. , Baer, N. , Miranda, V. , Prinz, C. & Singh, S. ((2014) ). Mental health and work: Achieving well-integrated policies and service delivery. (No. 161). Paris France: OECD Publishing. |
2 | *Becker, D. R. , Baker, S. R. , Carlson, L. , Flint, L. , Howell, R. , Lindsay, S. , . . . & Drake, R. E. ((2007) ). Critical strategies for implementing supported employment. Journal of Vocational Rehabilitation, 27: (1), 13–20. |
3 | *Becker, D. R. , Drake, R. E. & Naughton W. J. Jr ((2005) ). Supported employment for people with co-occurring disorders. Psychiatric Rehabilitation Journal, 28: (4), 332. |
4 | *Bejerholm, U. , Larsson, L. & Hofgren, C. ((2011) ). Individual placement and support illustrated in the Swedish welfare system: A case study. Journal of Vocational Rehabilitation, 35: (1), 59–72. |
5 | Bond, G. R. , Lockett, H. & van Weeghel, J. ((2020) ). International growth of individual placement and support. Epidemiology and Psychiatric Sciences, 29: (e183), 1–3. |
6 | Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. London, England: Harvard University Press. |
7 | *Browne, D. J. , Wright, J. , Waghorn, G. & Stephenson, A. ((2009) ). Developing high performing employment services for people with mental illness. International Journal of Therapy and Rehabilitation, 16: (9), 502–511. doi: 10.12968/ijtr.2009.16.9.43769. |
8 | Cram, F. , Jury, S. , Kokaua, J. , Ku, B. , Lockett, H. & Wilson, M. (2020). Individual Placement and Support (IPS) in Aoteaora New Zealand – New insights from Linked Administrative Data. Wellington, New Zealand: Ministry of Social Development |
9 | D’Amour, D. , Ferrada-Videla, M. , San Martin Rodriguez, L. & Beaulieu, M. ((2005) ). The conceptual basis for interprofessional collaboration: Core concepts and theoretical frameworks. Journal of Interprofessional Care, 19: (sup1), 116–131. |
10 | Davy, C. , Bleasel, J. , Liu, H. , Tchan, M. , Ponniah, S. & Brown, A. ((2015) ). Effectiveness of chronic care models: Opportunities for improving healthcare practice and health outcomes: A systematic review. BMC Health Services Research, 15: (1), 1–11. |
11 | Drake, R. E. ((2020) ). Introduction to the special issue on Individual Placement and Support (IPS) International. Psychiatric Rehabilitation Journal, 43: (1), 1. |
12 | Drake, R. E. & Bond, G. R. ((2017) ). Individual placement and support: Penetration and new populations. Administration and Policy in Mental Health and Mental Health Services Research, 44: (3), 309–310. |
13 | *Drake, R. E. , Becker, D. R. , Bond, G. R. & Mueser, K. T. ((2003) ). A process analysis of integrated and non-integrated approaches to supported employment. Journal of Vocational Rehabilitation, 18: (1), 51–58. |
14 | Drake, R. E. , Bond, G. R. , Goldman, H. H. , Hogan, M. F. & Karakus, M. ((2016) ). Individual placement and support services boost employment for people with serious mental illnesses, but funding is lacking. Health Affairs, 35: (6), 1098–1105. doi: 10.1377/hlthaff.2016.0001. |
15 | Durlak, J. A. & DuPre, E. P. ((2008) ). Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation. American Journal of Community Psychology, 41: (3), 327–350. |
16 | *Germundsson, P. & Danermark, B. ((2012) ). Vocational rehabilitation, interagency collaboration and social representations. Work, 42: (4), 507–517. |
17 | *Germundsson, P. , Hillborg, H. & Danermark, B. ((2011) ). Interagency collaboration in vocational rehabilitation for persons with mental health problems: The perspective of the service users and the professionals. Disability & Society, 26: (6), 699–713. |
18 | *Glenn, M. K. & Moore, L. C. ((2008) ). Building collaboration in substance abuse treatment and vocational rehabilitation. Journal of Teaching in the Addictions, 7: (2), 97–108. |
19 | *Gordon, J. & Mills, B. ((2001) ). Developing services for people with mental health problems in the New Deal for Disabled People personal adviser pilots. A Life in the Day, 5: (3), 9–15. |
20 | *Hanrahan, P. , Heiser, W. , Cooper, A. E. , Oulvey, G. & Luchins, D. J. ((2006) ). Limitations of system integration in providing employment services for persons with mental illness. Administration and Policy in Mental Health and Mental Health Services Research, 33: (2), 244–252. |
21 | *Holwerda, A. , Fokkens, A. S. , Engbers, C. & Brouwer, S. ((2016) ). Collaboration between mental health and employment services to support employment of individuals with mental disorders. Disability and Rehabilitation, 38: (13), 1250–1256. |
22 | Jonsdottir, A. & Waghorn, G. ((2015) ). Psychiatric disorders and labour force activity. Mental Health Review Journal, 20: (1), 13–27. |
23 | Karam, M. , Brault, I. , Van Durme, T. & Macq, J. ((2018) ). Comparing interprofessional and interorganizational collaboration in healthcare: A systematic review of the qualitative research. International Journal of Nursing Studies, 79: , 70–83. |
24 | *Kemp, K. , Savitz, B. , Thompson, W. & Zanis, D. A. ((2004) ). Developing employment services for criminal justice clients enrolled in drug user treatment programs. Substance use and Misuse, 39: (13–14), 2491–2511. |
25 | *King, R. , Waghorn, G. , Lloyd, C. , McLeod, P. , McMah, T. & Leong, C. ((2006) ). Enhancing employment services for people with severe mental illness: The challenge of the Australian service environment. Australian and New Zealand Journal of Psychiatry, 40: (5), 471–477. |
26 | Körner, M. , Bütof, S. , Müller, C. , Zimmermann, L. , Becker, S. & Bengel, J. ((2016) ). Interprofessional teamwork and team interventions in chronic care: A systematic review. Journal of Interprofessional Care, 30: (1), 15–28. |
27 | Lockett, H. & Bensemann, C. ((2013) ). Employment as a health intervention: The role of psychiatry in bridging the evidence to practice ga. Australian & New Zealand Journal of Psychiatry, 47: (5), 417–420. |
28 | Lockett, H. , Waghorn, G. & Kydd, R. ((2018) b). Policy barriers to evidence-based practices in vocational rehabilitation for people with psychiatric disabilities in New Zealand. WORK, A Journal of Prevention, Assessment & Rehabilitation, 60: (3), 421–435. |
29 | *Marrone, J. , Burns, R. & Taylor, S. ((2014) ). Vocational rehabilitation and mental health employment services: True love or marriage of convenience? Journal of Vocational Rehabilitation, 40: (2), 149–154. |
30 | Morgan, S. , Pullon, S. & McKinlay, E. ((2015) ). Observation of interprofessional collaborative practice in primary care teams: An integrative literature review. International Journal of Nursing Studies, 52: (7), 1217–1230. |
31 | Mulvale, G. , Embrett, M. & Razavi, S. D. ((2016) ). Gearing up to improve interprofessional collaboration in primary care: A systematic review and conceptual framework. BMC Family Practice, 17: (1), 1–13. |
32 | Munn, Z. , Peters, M. D. , Stern, C. , Tufanaru, C. , McArthur, A. & Aromataris, E. ((2018) ). Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Medical Research Methodology, 18: (1), 1–7. |
33 | *Nepe, M. , Pini, T. & Waghorn, G. ((2011) ). Enhancing mental health services through joint delivery with employment and other essential community services: Early lessons from an innovative New Zealand program. Mental Health Review Journal, 16: (2), 64–75. |
34 | Organisation for Economic Co-operation and Development OECD. ((2021) ). Fitter Minds, Fitter Jobs: From awareness to change in integrated mental health, skills and work policies, Mental Health and Work. Paris, France: OECD Publishing. |
35 | Organisation for Economic Co-operation and Development OECD. ((2015) a). Mental Health and Work Fit Mind, Fit Job: From Evidence to Practice in Mental Health and Work. Paris, France: OECD Publishing. |
36 | Organisation for Economic Co-operation and Development OECD. (2015b). Recommendation of the Council on integrated mental health, skills and work policy. Retrieved June 15, 2016 from https://legalinstruments.oecd.org/en/instruments/334. |
37 | Overbeck, G. , Davidsen, A. S. & Kousgaard, M. B. ((2016) ). Enablers and barriers to implementing collaborative care for anxiety and depression: A systematic qualitative review. Implementation Science, 11: (1), 165. |
38 | Peters, M. D. , Godfrey, C. M. , Khalil, H. , McInerney, P. , Parker, D. & Soares, C. B. ((2015) ). Guidance for conducting systematic scoping reviews. International Journal of Evidence-Based Healthcare, 13: (3), 141–146. |
39 | *Porteous, N. & Waghorn, G. ((2007) ). Implementing evidence-based employment services in New Zealand for young adults with psychosis: Progress during the first five years. The British Journal of Occupational Therapy, 70: (12), 521–526. |
40 | *Porter, S. , Lexén, A. , Johanson, S. & Bejerholm, U. ((2018) ). Critical factors for the return-to-work process among people with affective disorders: Voices from two vocational approaches. Work, 60: (2), 221–234. |
41 | Priest, B. & Lockett, H. ((2020) ). Working at the interface between science and culture: The enablers and barriers to individual placement and support implementation in Aotearoa/New Zealand. Psychiatric Rehabilitation Journal, 43: (1), 40–52. |
42 | Prinz, C. , Lockett, H. & Stermsek, M, Arends, I. ((2018) ). Mental health and work: Aotearoa New Zealand. Paris, France: OECD Publishing. |
43 | San Martín-Rodríguez, L. , Beaulieu, M. , D’Amour, D. & Ferrada-Videla, M. ((2005) ). The determinants of successful collaboration: A review of theoretical and empirical studies. Journal of Interprofessional Care, 19: (sup1), 132–147. |
44 | *Vukadin, M. , Schaafsma, F. G. , Westerman, M. J. , Michon, H. W. & Anema, J. R. ((2018) ). Experiences with the implementation of individual placement and support for people with severe mental illness: A qualitative study among stakeholders. BMC Psychiatry, 18: (1), 145. |
45 | *Waghorn, G. , Collister, L. , Killackey, E. & Sherring, J. ((2007) ). Challenges to implementing evidence-based supported employment in australia. Journal of Vocational Rehabilitation, 27: (1), 29–37. |
46 | *Waghorn, G. , Stephenson, A. & Browne, D. ((2011) b).The importance of service integration in developing effective employment services for people with severe mental health conditions. The British Journal of Occupational Therapy, 74: (7), 339–347. |
47 | Wood, E. , Ohlsen, S. & Ricketts, T. ((2017) ). What are the barriers and facilitators to implementing collaborative care for depression? A systematic review. Journal of Affective Disorders, 214: , 26–43. |
Appendices
Appendix
Coding structure developed from the review of the collaborative healthcare literature
| Macro | ||
| Factor | Description | Papers |
| Funding, financing and resourcing | Funding models based on fee for service and not objectives do not support collaboration. Funding needs to be sustainable and there needs to be sufficient resource for organisations to be able to collaborate and not just compete. Funding models should allow for collaboration to be seen as revenue neutral or revenue enhancing. | 2, 6,7 |
| Government policies and planning | Regional planning and sector policies can encourage or discourage collaboration between organisations. | 2, 6 |
| Legislation and regulatory frameworks | Professional scope of practice and organizational functions may limit the opportunity to collaborate if not aligned. | 2, 6 |
| Formalization of processes | Formal processes around meetings and written documents help to establish collaborative structure and allow time for teamwork and clarification of roles and responsibilities. | 2,3,4,6 |
| Management structures should be explicitly collaborative no matter the size to support the rest of the team. | ||
| Shared vision and objectives | Collaborators should have clear, common and realistic objectives focusing on the client and the team, and expectations from the collaboration. Collaborators should believe in the benefits of collaboration. | 1,2,4,6 |
| Philosophy/atmosphere | Shared organizational philosophies and values support collaboration. Open philosophies and positive atmospheres also support collaboration. | 1,4,6 |
| Management and leadership | Management and leadership teams need to support collaboration and create organizational buy in for collaboration. They should be committed to collaboration, share decision making, support team development and processes, and provide regular feedback on team performance. | 2, 3,6,7 |
| Communication | Formal and informal communication channels are crucial for collaboration and shared decision making, especially relationship building. | 2,3,4,5,6,7 |
| Meetings to support group discussions are important, along with having the space and time for informal communication. | ||
| All team members need access to essential information/data when they need it and ability to exchange information easily is important whether asynchronous or synchronous. | ||
| Warm handovers support communication between professionals. | ||
| Clarification of roles and responsibilities of each partner | All team members and partners should have their roles and responsibilities defined to support shared understanding of the team, especially their contribution and the strengths of other professionals. It will also reduce duplication of tasks, especially where there is scope overlap. | 1, 2, 3 |
| Physical space | Sufficient physical space to work together formally, and/or informally gather supports communication and relationship building. | 2,3,6,7 |
| Client focus | Shared focus on the client fosters collaboration. This includes shared plans, interventions, monitoring and systematic feedback from the patient. | 1,5,7 |
| Client participation and awareness | Client participation in the decision-making/collaborative process improves positive health outcomes. Minimizes professional paternalism. | 1,2 |
| Client awareness of the collaboration is also important, as the team may be invisible to the client. Clients can see team as a source of division and a barrier between them and a specific professional. | ||
| Administrative, Human Resources and Information Technology resources. | Sufficient administrative, HR and technical support is needed to foster collaboration. | 2, 4, 5,6 |
| Integrated information systems are important for information sharing. | ||
| Training | Training of professionals in collaboration supports shared understanding of collaboration, roles and helps to create buy in. | 6 |
| Quality/audit/accreditation process | Availability of joint written documents including standards, protocols, policies, unified and standardized documentation support shared understanding and collaboration. Joint accreditation and quality processes and also foster collaboration. | 4 |
| Support for innovation | Organisations where there is an ability to innovate are more likely to collaborate. Ability to innovate is influenced by their historical experiences and in turn influences readiness for change. | 2,4,7 |
| Term used for the team | While definitions are not consistent, labelling of team type (multi-, inter-, trans-agency) can indicate level of collaboration. | 1 |
| Task scope, complexity, and uncertainty | Level of collaboration varies between task complexities. Periods of crisis with urgent, complex tasks can encourage collaboration. | 2 |
| Interpersonal communication | Active and open, efficient, vehicle for other determinants of collaboration | 3, 4,5,6 |
| Trust and respect | Members of the team need to trust and respect each other. This helps relationship building, communication and to address power dynamics between professionals and organisations. | 1,2,6 |
| Shared knowledge and responsibilities | Each partner must be a ‘reflective practitioner’ and be aware of and value the contributions and perspectives of the other professionals. | 1,2, 3, 6, 7 |
| Power | Shared among team members, recognized by all. Supported by horizontal organizational structure, not hierarchal. | 1,6 |
| Partnership | Collaborative partnerships should be authentic, constructive, and have open and honest communication, mutual trust and respect. | 1 |
| Understanding of role in team | Team members should understand how their work contributes to outcomes and to team objectives to feel part of the team. Accept grey zones of overlap with other professionals’ scope. | 1,2, 4, 6 |
| Belief in collaboration | Individuals need to believe in the benefits of collaboration, which is impacted by previous experience with collaboration and leadership. | 4,6 |
| Willingness to collaborate | Individuals’ flexibility in way of working and readiness for change support them to collaborate. | 2,4, 6,7 |
Notes. Papers included in the review (n = 7): 1. D’Amour, D., Ferrada-Videla, M., San Martin Rodriguez, L., & Beaulieu, M.-D. (2005). The conceptual basis for interprofessional collaboration: core concepts and theoretical frameworks. Journal of Interprofessional Care Supplement 1, 116–131. 2. Karam, M., Brault, I., Van Durme, T., & Macq, J. (2018). Comparing interprofessional and interorganisational collaboration in healthcare: a systematic review of the qualitative research. International Journal of Nursing Studies 79, 70–83. 3. Morgan, S., Pullon, S., & McKinlay, E. (2015). Observation of interprofessional collaborative practice in primary care teams: An integrative literature review. International Journal of Nursing Studies 52, 1217–1230. 4. Mulvale, G., Embrett, M., & Razavi, S. D. (2016). ‘Gearing Up’ to improve interprofessional collaboration in primary care: a systematic review and conceptual framework. BMC Family Practice 17:83. 5. Overbeck, G., Davidsen, A. S., & Kousgaard, M. B. (2016). Enablers and barriers to implementing collaborative care for anxiety and depression: a systematic qualitative review. Implementation Science 11:165. 6. San Martin-Rodriguez, L., Beaulieu, M.-D., D’amour, D., & Ferrada-Videla, M. (2005). The determinants of successful collaboration: A review of theoretical and empirical studies. Journal of interprofessional care Supplement 1, 132–147. 7. Wood, E., Ohlsen, S., & Ricketts, T. (2017). What are the barriers and facilitators to implementing Collaborative Care for depression? A systematic review. Journal of Affective Disorders 214, 26–43.


