
The Illinois Work and Well-Being Model: An intervention framework to improve employment and health outcomes for stroke survivors
Abstract
OBJECTIVE:
This article describes the Illinois Work and Well-Being Model as a framework that can be applied to facilitate the career development of people who have sustained strokes. The model depicts the interaction of contextual and career development domains to improve participation in the areas of work, society, community, and home.
CONCLUSION:
A discussion of the model’s implications regarding vocational rehabilitation research, service, and policy is presented, with the overall aim of establishing career development as the foundation of vocational rehabilitation services for stroke survivors.
1Introduction
Researchers continually report that participating in meaningful work-related activities is imperative to the physical health, psychological well-being, and quality of life of people with and without disabilities, including people with chronic health conditions such as strokes (de Boer, 2005; Dutta, Gervey, Chan, Chou, & Ditchman, 2008; Shaw et al., 2016). There is no doubt that paid employment is an important factor in providing avenues for economic security and access to health insurance, in facilitating social participation, and in improving health and quality of life (Bishop & Chiu, 2011). In keeping with the notion that work is important to well-being, work is considered a fundamental human right of people with disabilities and the primary focus of vocational rehabilitation services (Chan et al., 1997; Strauser, 2013). Therefore, using scientifically validated interventions based on theoretical models to enhance employment has been an important focus of governmental policy and programs. Despite this focus, there is a significant disparity in the access to vocational rehabilitation services, level of employment, and labor market participation for individuals with chronic health conditions and disability (Institute on Disability, 2018).
1.1Stroke
Stroke, also known as cerebrovascular accident (CVA), is a term that refers to a group of conditions characterized by neurological deficits due to an interruption in cerebral blood flow (Zhang, Chapman, Plested, Jackson, & Purroy, 2012). Residual effects of stroke span a wide range, depending on the person’s pre-stroke health status, the area of the brain that is affected, and the amount of cerebrovascular damage that has occurred (National Stroke Association, 2016). Every year, approximately 800,000 Americans sustain a new or recurrent stroke, and there are more than 7 million (2.5%) people living in the US who have survived a stroke (Zhang et al., 2012; Wang, Kapellusch, & Garg, 2014; American Stroke Association, 2016). Stroke is the fifth leading cause of death in the United States, accounting for 129,000 deaths annually (American Stroke Association, 2016). The risk of stroke is nearly doubled for African Americans in comparison to people of European descent, and stroke risk increases as a linear function of age with two-thirds of strokes occurring in individuals aged 65 years or older (CDC, 2015). The total annualized cost of stroke in the United States is estimated to be $34 billion in health care consumption, medication, and lost productivity (CDC, 2015).
Frequently reported symptoms of stroke include hemiparesis (weakness on one side of the body), hemiplegia (paralysis on one side of the body), dys-arthria (difficulty speaking or slurred speech), dysphagia (trouble swallowing), fatigue, loss of emotional control and changes in mood, memory loss, poor judgment, issues with problem-solving, personality changes, inappropriate language or actions, decreased field of vision, and difficulties with visual perception (American Stroke Association, 2016). Most complications of stroke are specific to the side of the brain that is affected; as an example, aphasia (difficulty in speaking or comprehending spoken language) and behavior becoming more cautious are common accompaniments of a left-brain injury, whereas one-sided neglect (lack of awareness of the left side of the body), trouble understanding facial expressions and tone of voice, and behavior becoming more impulsive are typical of right-brain injuries. Owing to the brain’s contralateral functionality, the physical effects of any brain injury manifest on the side of the body opposite to the injury. Many individuals who sustain strokes also experience neuropsychiatric complications such as apathy, depression, anxiety, post-traumatic stress disorder, irritability, pseudobulbar affect (e.g. uncontrolled laughing or crying), and denial (American Stroke Association, 2016).
Although the number of individuals sustaining strokes each year has decreased slightly over the past decade (American Stroke Association, 2016), the proportion and total number of people who survive strokes have drastically increased. Preventative measures and medical advances have resulted in the prevalence of stroke in the United States remaining relatively stable over time and the mortality rate decreasing significantly. Moreover, as the US adult population continues to “gray,” the numbers of people who will be seeking medical, psychosocial, and vocational rehabilitation services for this age-related condition will continue to increase for decades to come (Gatchel, Choi, & Hanna, 2018).
Given the wide range of functional limitations caused by stroke, and the deleterious impact that this condition has on survivors’ psychosocial functioning and quality of life, it is not surprising that stroke survivors report significant changes in everyday functioning. These changes include the loss of valued roles, difficulty leaving the house, lack of participation in leisure activities, difficulty with communication and memory, and deterioration of important relationships (Schouten, Murray, Boshoff, Sherman, & Patterson, 2011; Thompson & Ryan, 2009). Community involvement and quality of life are most prominently affected among stroke survivors who experience the highest number of stroke related deficits, particularly depression and the most common stroke complication, hemiplegia. Hemiplegia creates problems with mobility, produces pain and discomfort, and can hinder independence in the performance of activities of daily living (Min & Min, 2015).
1.1.1Stroke and employment
Stroke is one of the most common causes of work disability worldwide, and it is the leading cause of adult disability in the United States (National Stroke Association, 2016). As many as 70% of working-age stroke survivors have some type of impairment to their work capacity; only about 40% of individuals employed at the time of stroke are able to successfully return to work (Conroy, Milani, Levine, & Stein, 2009), and only 19% are able to successfully sustain that employment and remain in the workforce after 5 years (Wang et al., 2014).
According to Conroy and colleagues (2009), key issues associated with return to work likelihood include age, severity of stroke, and nature of residual impairments, psychological factors, socioeconomic status, financial and family obligations, education level, and pre-stroke occupational type. Research reveals a higher probability of return to work for stroke survivors with shorter lengths of stay in the hospital, with less severe strokes, with an absence of severe physical and cognitive impairments, with high ability to perform activities of daily living, with more supportive work environments, and with more flexible professional level jobs (Wang et al., 2014).
For older individuals, experiencing a stroke may be the impetus for the decision to retire. Given that the incidence of stroke increases with age, it is not surprising that many individuals who have the financial means to stop working do so following a stroke, especially if they were planning to retire in the near future before the stroke occurred (Saeki, 2000; Conroy et al., 2009). However, leaving the workforce prematurely may negatively affect the person’s sense of self-worth; retirees who sustained strokes shortly before exiting the workforce frequently report feeling that they are a burden on their families, that their lives lack a strong purpose and direction, and that they are not contributing fully to society (Conroy et al., 2009).
1.1.2Stroke and vocational intervention
For those stroke survivors who choose to return to employment, early intervention and management of workplace barriers is crucial. Slowly reintegrating individuals into the workplace after stroke is important because of the extended recovery period associated with post-stroke treatment (Saeki, 2000; Conroy et al., 2009). Domains of functioning including cognition, affect, language, communication, physical strength and coordination, and perceptual abilities require varying degrees of time for recovery, often making immediate return to full-time employment a difficult proposition (Conroy et al., 2009). When cognitive and motor functions are significantly impacted, there can be a shift from the notion of return to work to a return to productivity, with an increased emphasis on the use of supported employment strategies (Brede et al., 2016).
There is no clear-cut successful formula for helping stroke survivors return to work, but, just as the complications of stroke are highly individualized, there is a need to individualize rehabilitation plans, especially as they relate to an individual’s limitations, accommodation needs, and rehabilitation goals. In general, employers who are supportive and willing to modify the work environment contribute to increased success in return to work plans (Saeki, 2000; Kwan & Schultz, 2016). Taking advantage of volunteer and part-time work opportunities and gradually transitioning to full-time work can be a helpful strategy, and the benefits of long-term part-time work or even volunteer activities should not be overlooked in helping people re-establish a sense of purpose and psychosocial well-being (Conroy et al., 2009). Developing and implementing creative job accommodation strategies or changing positions to less labor-intensive roles (e.g., transitioning from performing carpentry work to teaching carpentry in a classroom) may be particularly relevant for individuals who occupied physically demanding positions prior to their stroke. Given the high incidence of fatigue post-stroke, accommodations such as increased breaks, flexible scheduling, ergonomic assessment of the work station, and mobility aids should be considered as part of the return-to-work plan. Finally, because stroke often compromises one’s ability to drive, transportation to and from work and for required on-the-job travel is often an important return-to-work issue.
1.2The centrality of work to health and well-being for people with stroke
Because work is closely tied to meeting basic needs and increased physical and psychological well-being, and because competitive paid employment is an expected outcome of the vocational rehabilitation process, gaining an understanding of the factors that impact an individual’s career development is not only important for vocational rehabilitation, but also has important physical and psychological health implications. Career development describes a complex, multifaceted, lifelong process of an individual’s efforts to develop and maintain connection with productive activities such as education, paid work, and providing care to important family members and others of significance (Strauser, 2013). It encompasses both structure and long-term changes in behavior (Herr & Cramer, 1992) and is directly applicable to individuals with stroke (Koch & Rumrill, 2017; Strauser et al., 2014).
Specifically, career development can be conceptualized as an interaction of individual behavioral, affective, and cognitive processes that are influenced by contextual variables (e.g., family, socioeconomic status [SES], gender) and consists of the following three phases: 1) awareness (making sure the environment fits with the individual’s values, skills, etc.), 2) acquisition (job seeking and placement), and 3) maintenance (what it takes to keep a job; Peterson, Sampson, & Reardon, 1991; Sampson, 2004; Saunders, Peterson, Sampson, & Reardon, 2000; Strauser, 2013). Unfortunately, many vocational rehabilitation counselors view the career development process as a linear sequence of activities and experiences, which can negatively impact employment outcomes and the development and utilization of effective vocational interventions. This may be especially problematic for individuals with strokes, as they are typically diagnosed in late career; therefore, vocational rehabilitation interventions with this population will likely focus on return to work strategies (i.e., re-acquisition) following the initial stroke and subsequently on maintaining the person’s career as long as he or she wishes to do so as opposed to awareness and acquisition strategies.
Because employment is sometimes a cyclical developmental process that is affected by a variety of individual, systemic, and environmental factors, it is important to have an operational Model for conceptualizing the career development process for individuals with stroke. In this article, we present the Illinois Work and Well-Being Model (IW2M) as a conceptual framework that can be used to guide career development services and research related to individuals with stroke. The IW2M is designed to be parsimonious in nature to facilitate broad application, yet refined enough to promote in-depth research related to each of the domains and factors that compose the model. After a presentation of the IW2M, there will be a brief discussion of the Model’s implications for services and research related to individuals with stroke.
2The Illinois Work and Well-Being Model
The IW2M is comprised of the Contextual, Career Development, and Participation domains that interact to provide a structure for understanding the career development of people with strokes. The Career Interventions component is purposefully situated between the Contextual and Career Development domains. As a result, the IW2M model implies that career interventions directly and indirectly influence both the Contextual and Career Development domains and have an indirect effect on the Participation domain. Each domain is made up of factors, which facilitates analysis at both individual domain and factor levels. As a result, domains and factors can be conceptualized as both independent and interdependent in nature. All arrows between domains and factors are bi-directional, indicating a reciprocal effect between the model’s components. Relationships between domains, factors, and interventions can be positive, negative, or neutral, implying that the value of the directional impact is determined by the situation-specific activities, expressions, and reactions to both specific and broad stimuli. Each domain is briefly described below and outlined in Table 1. Detailed discussions regarding the IW2M can be found in Strauser, Greco, and O’Sullivan (2018) and Strauser, O’Sullivan, and Wong (2018).
Table 1
Domains, factors and components of the Illinois Work and Well-Being Model
| Domain | Factors | Components |
| Contextual | Personal | Personality, interests, values, gender, age, ethnicity, aptitude, SES, education attainment, identity, past personal experiences, temperament |
| Environmental •Individual level: individual systems of support; support network •Services level: services and resources available •Cultural/legal systems levels: societal and cultural attitudes; political and legal factors (Falvo, 2014; Peterson & Rosenthal, 2005) | Culture, society, economic physical environment, quality of education, discrimination, services available, political systems, transportation, technology, climate, social attitudes, | |
| Functional/Limitations •Capacity: actual ability □ Maximum function-greatest degreeof function possible •Performance: actually does □ Optimal functioning-subjective viewpoint of the individual and derivedfrom individual goals and experience | Physical Communication (expression &reception) Emotional Cognitive, Executive functioning | |
| Career | Awareness | Vocational identity, career awareness, vocational maturity, work personality |
| Acquisition | Job seeking skills, impression management, Resume Development | |
| Maintenance | Carry out required job tasks, meet production demands, complete normal work day, Engage co-workers | |
| Participation | Home | Independent living, Self-care at home (bath, cook) Maintain house (clean), Wash cloths, choose or create contexts suitable to meet personal needs and values, manage every day affairs |
| Society/Social | Appropriate social relationships, meaningful and trusting intimate relationships, understands give and take of human relationships | |
| Community | Concerned about the welfare of others, engages in appropriate community activities, Access and use appropriate transportation, engage in appropriate civic activities | |
| Work | Maintain steady employment, meet the demands of work, engage in career development, earn appropriate wages |
2.1IW2M domains
The Contextual domain applies the ICF framework as a guide to operationalize how personal and environmental factors interact with stroke and treatment related limitations and restrictions. The bi-directional arrows between the domain factors imply a reciprocal relationship whereby growth or change in one factor can directly or indirectly impact the growth or change in the other factors. The solid bi-directional arrow between the Contextual and Career Development domains indicates a direct reciprocal connection between these two major domains independent of any intervention, implying a mutually interdependent developmental process. The solid bi-directional arrow along the bottom of the model between the Contextual and Participation domains implies a reciprocal relationship independent of the Career Development domain and any career interventions.
The Career Development domain is based on career and employment research related to individuals with disabilities (Strauser, 2013). The domain consists of the following three factors: Individual Awareness, Educational and Employment Acquisition, and Educational and Employment Maintenance. Specifically, Awareness is developmentally mediated with the individual becoming aware of how he or she relates to the world and in which activities he or she may choose to participate. The individual awareness factor theoretically provides the foundation for the acquisition and maintenance factors, although, as implied by the bi-directional arrows, all factors have a reciprocal impact influencing each factor’s continual development. The Education and Employment Acquisition factor addresses the process by which individuals go about acquiring access to educational and employment related activities. From an educational perspective, acquisition includes, but is not limited to, the process and activities associated with applying for appropriate educationally related activities including trade, two-year, and four-year training programs. The Employment and Educational Acquisition factor provides the foundation for the Maintenance Factor related activities and has a reciprocal impact on individual awareness. The Educational and Employment Maintenance factor addresses the activities and behaviors associated with maintaining engagement and participation in educational and occupationally related activities. Although Maintenance occurs after Acquisition and is typically conceptualized as an outcome, it too has a reciprocal effect on the preceding factors.
The Participation Domain utilizes the ICF framework as a guide to identify meaningful and broad-based participation in major life areas. In this conceptual model the life areas of home, society, community, and work have been identified and can serve as outcomes of interest. Although the work area may seem an obvious focal area for those working to improve career development and employment outcomes for individuals with strokes, the model stresses the interconnectivity of all participation areas. A fundamental tenet guiding the model is that increased positive participation will lead to an overall increase in individual’s well-being and overall quality of life.
According to the conceptual model, the Intervention Component is situated between the Contextual and Career Development Domains. This placement suggests that the primary goal of career preparatory, educational, and employment interventions is to facilitate and maximize the direct interaction between the Contextual and Career domains, which will, in turn, indirectly impact the Participation Domain. By placing the intervention component outside of the Career Development Domain and situating it between the Contextual and Career Development Domain, the model implies that interventions should focus on the correspondence between the two respective domains. Effective interventions should focus on maximizing the personal, environmental, and stroke related limitations to impact the Career Development Domain and specific Career Development Domain factors.
3Implications for stroke survivors
Applying the Illinois model to increase the community and employment participation of individuals who have survived strokes has a number of important implications. The IW2M was developed to guide researchers in examining the domains, factors, and participation outcomes related to career development and employment of individuals with disabilities. The model presents researchers with both within-and across-domain analyses and examination at the factorial level. The model also provides a structure for practitioners and psychosocial service providers to operationalize the factors and domains that may be contributing to decreased labor market participation for individuals who have survived strokes. Practitioners can use the framework to gain an understanding of service delivery strengths and potential areas of need. Below, specific implications for services and research are briefly discussed.
3.1Case conceptualization and services
The IW2M has potential implications for the provision of career and vocational services for individuals with strokes at both the individual and program levels. At the individual level, practitioners can apply the model to conceptualize cases to identify specific needs and to develop services that address specific factors of need across and within domains. Specifically, the IW2M allows practitioners to undertake a multilevel analysis of the individual through the identification of primary, secondary, and tertiary associations and effects between factors and domains. Across domains, the model allows practitioners to identify the individual’s personal, environmental, and functional contextual factors and examine if they are acting as facilitators or barriers in the career development domain. Based on the multilevel analysis, specific interventions and services can be targeted that reduce the negative effect of specific contextual factors while leveraging the impact of other positive factors.
The multilevel analysis is also dynamic in nature, allowing for continual between and within factor analysis as the individual’s needs, facilitators, and barriers evolve and change in response to the impact of the specific services and interventions provided. For example, initial interventions and services may be directed at facilitating and helping the individual gain a better understanding of his or her emotional functioning (Contextual Domain) that strengthens a stroke survivor’s vocational identity and awareness (Career Domain). Presuming that the services and interventions provided are effective in helping the individual gain an increased understanding of his or her emotional functioning, which in turn increases vocational identity and awareness, the practitioner can build on the success to determine across domain and within domain impact and develop relevant clinical hypotheses and questions that will guide additional interventions, services, and supports. For example, in the Career Domain, does the individual’s increased vocational identity and awareness allow the individual to advocate for job modifications that can facilitate job maintenance (Within Domain)? Does increased clarity regarding emotional functioning and increased career awareness increase an individual’s level of participation in social and community factors (Across Domain)? In the following paragraphs, we provide an illustrative example of how the IW2M can be used in a multilevel analysis to facilitate effective service delivery to individuals with strokes.
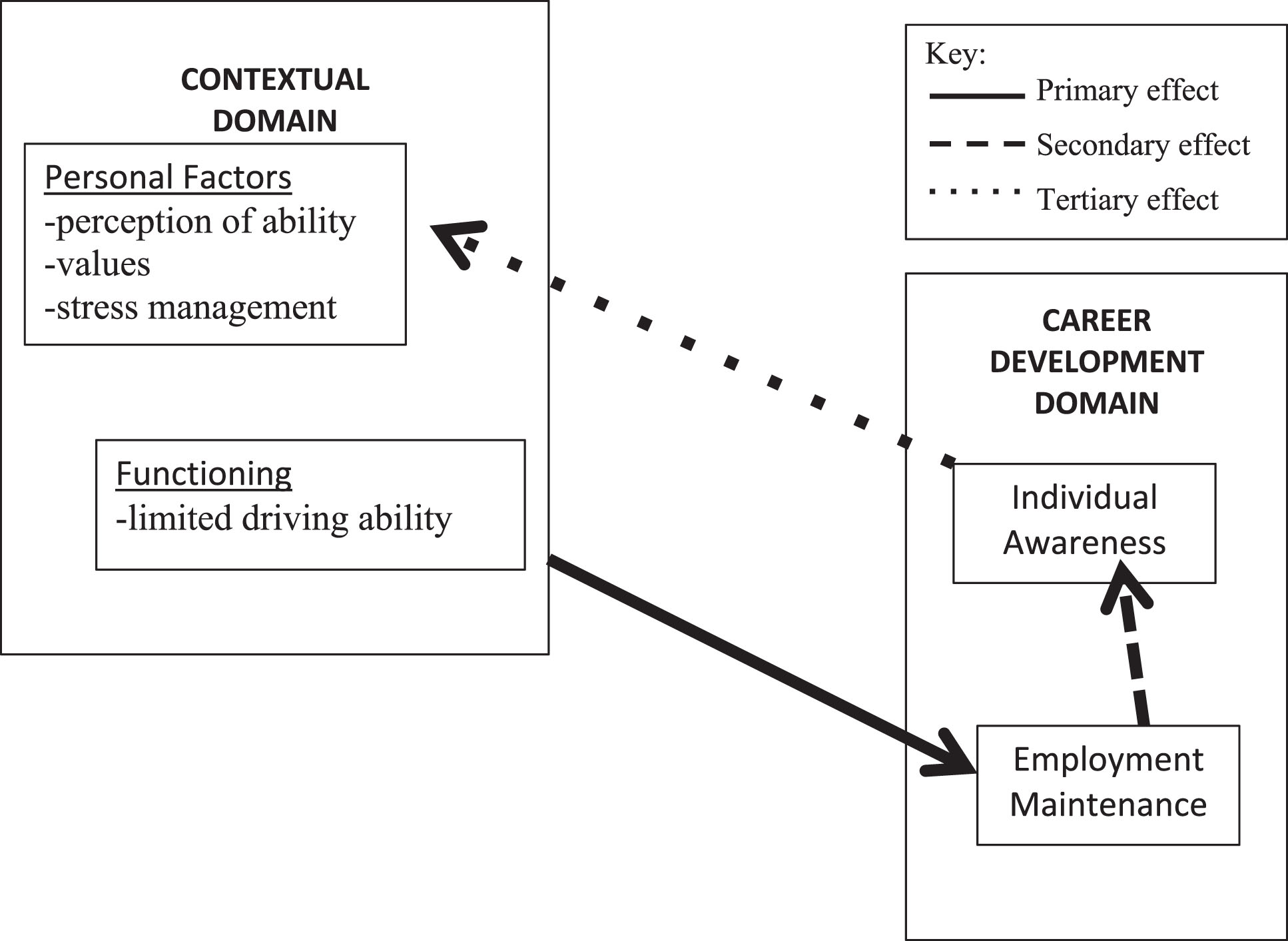
A 64-year-old woman who is working as an elementary teacher sustained a stroke at age 62. Hemiparesis related to her stroke makes it difficult for her to walk steadily, especially with her fatigue. She is also noticing that her memory often fails her, especially her short-term memory. She is currently able to perform the necessary functions of her job but is becoming increasingly concerned and stressed about her ability to maintain her teaching position for the next five years. Prior to her stroke, this person had planned to continue working until age 69.
This person’s internalized concern that she may need to retire prematurely has created significant uncertainty regarding her future financial security and has created self-doubt regarding her vocational identity. She is unsure about workplace accommodation strategies, such as cognitive support technology to accommodate her memory impairment, that might allow her to extend her career. She is also unaware of what options she might have for employment in another capacity should she decide to leave the teaching profession.
This person’s situation can be conceptualized as a primary across domain effect, with her perception of her physical and cognitive functioning (Contextual Domain) potentially impacting her job maintenance (Career Domain). The impact of her across-domain concern regarding functioning and job maintenance is contributing to a secondary within-domain effect; her concerns regarding her ability to keep her job (Job Maintenance) is creating doubts regarding her vocational identity (Awareness). Finally, because of her decreased vocational identity, she is starting to question personal factors such as her physical and emotional abilities, her individual and career values, and her ability to manage stress. Therefore, her decreased level of vocational identity is contributing to her decreased emotional functioning, which would be considered a tertiary across-domain effect (see Fig. 2.).
Fig. 1
The Illinois career development framework.
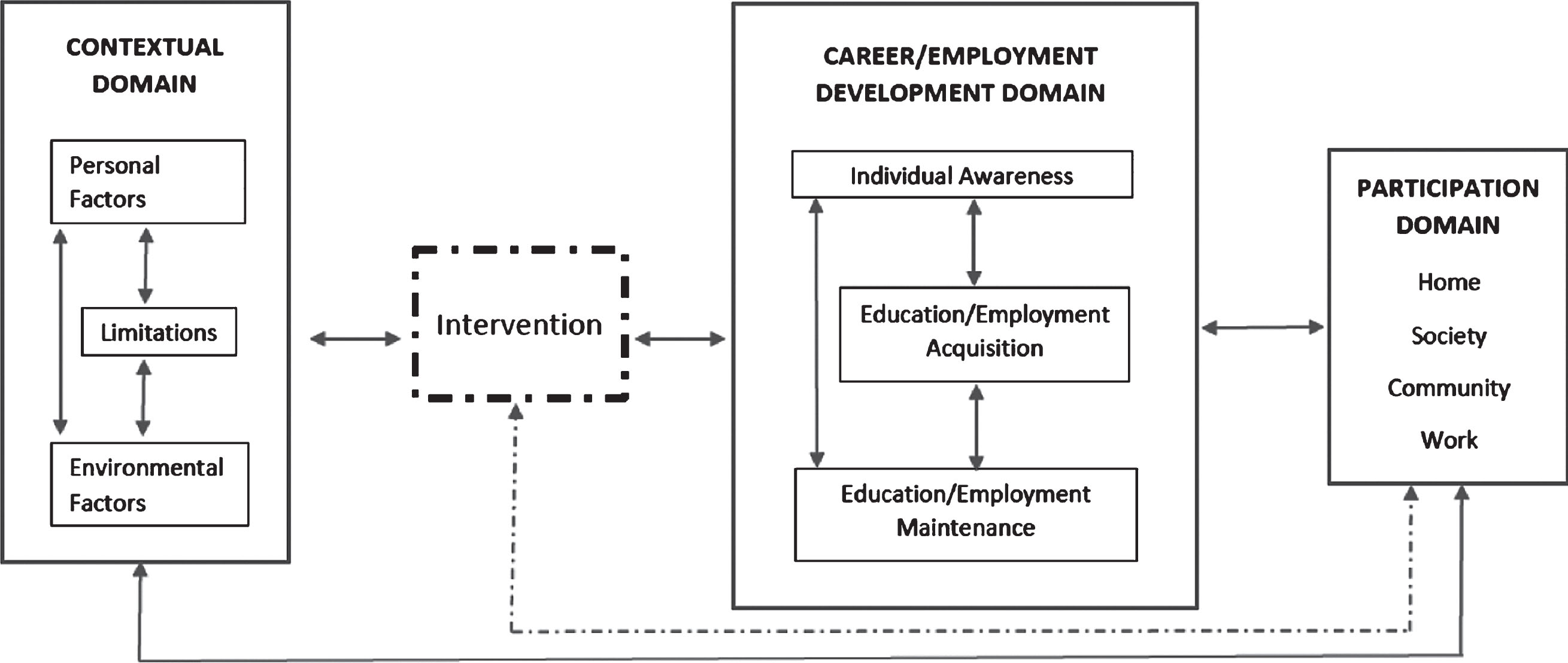
Fig. 2
Primary, secondary and tertiary effect using the illinois work and well-being model.
Engaging in across and within domain level analysis may allow the practitioner to conceptualize the types of direct and indirect services and interventions that can be employed to maximize career and vocational outcomes. Using the example above to address the primary impact of the individuals perceived functioning on job maintenance, the practitioner may choose to examine potential job modifications with a primary emphasis on mobility aids, memory enhancement applications or ‘apps’ for the teacher’s smart phone, and energy conservation strategies to reduce fatigue. Indirectly, the practitioner may recommend that the individual identify and participate in health promotion activities offered through a local community organization or health care facility that will provide benefits to both her physical and mental health and overall well-being.
In addressing secondary and tertiary influences, the practitioner may choose to implement a combination of direct and indirect services. Directly, the practitioner may work with the individual to develop self-advocacy skills that allow the individual to engage her principal in a dialogue regarding her ability to meet the demands of her job as a teacher. In addition, the practitioner may also provide direct service vocational counseling focused on helping the individual develop knowledge regarding additional job accommodation strategies that could be utilized to promote vocational identity, and/or focused on other employment options that she might wish to consider. These measures would allow the individual to examine how the accommodations could be used to help her meet the demands of her current position, or how her experience as a teacher could transfer into other jobs, thereby preserving or reinforcing her level of vocational identity. Indirectly, the practitioner may recommend that the individual seek personal adjustment counseling to help manage the stress and uncertainty regarding her employment and financial situations. A referral might also be made to a financial planner to help the person understand the retirement and disability benefits she is eligible for through the school district. The key to being successful is that practitioners use the model to leverage both direct and indirect services to provide a continuum of support across domains and levels (primary, secondary, tertiary) so that services become fully integrated and not fragmented.
4Organization-level implications
At the organizational level, the model can be applied to guide a multi-level and between and within domain program evaluation to identify potential areas of program strength and need. By applying the model in the program evaluation process, an organization may find that vocational services are isolated and only focus on one particular domain or factor, potentially limiting the services’ reach and effectiveness. Applying the model in the program evaluation process may also allow an organization, agency, or company to examine resource allocation and the potential need to shift or re-allocate resources to maximize program effectiveness. Program evaluation should also consider the depth and breadth of direct services offered and allow the organization to map indirect services to specific domains and factors to ensure comprehensive coverage of clients’ potential needs. Finally, application of the conceptual model at the organizational level reinforces the view that the ultimate outcome of rehabilitation services is an increase in all four participation domain factors, which allows organizations to consider their services and supports in a holistic context.
5Implications for research
Given the specific and often complicated career and employment needs of individuals who have sustained strokes, research must endeavor to gain an understanding of the factors that determine outcomes for this emerging rehabilitation clientele (Koch & Rumrill, 2017). The IW2M can be used to develop a comprehensive research strategy to address the career and employment needs of individuals with stroke. First, the model can be used to identify specific areas that are in need of research development. With a few exceptions (e.g., supported employment, outcomes of the state-federal VR system), vocational rehabilitation research has been limited in scope and has focused primarily on issues related to the awareness factor, which may not be as applicable to the career and employment needs of adults with stroke. By employing this conceptual model, it becomes very clear that there are many other areas that need to be examined to gain a basic understanding of the career development process as it relates to adults with stroke.
Second, the conceptual model places an emphasis on broader societal participation as the overall goal of the career development process, which is consistent with the ICF. The majority of VR research has exclusively focused on the career development domain factors and constructs, such as career readiness and vocational identity, with minimal focus on the overall goal of how and why these factors and constructs relate to improving societal participation and overall well-being (Strauser et al, 2014). Future research should focus on gaining an understanding of the interaction between the career and contextual domains that contribute to employment and participation and developing interventions that facilitate this process for individuals with stroke.
Third, by incorporating a contextual domain into the career development process, this model acknowledges and places an emphasis on addressing the chronic health factors as they relate to and impact the career development process. The acknowledgement of disability related factors has been emphasized in VR research, but to date it has had limited application to empirical career development research. Encouragingly, the study of return to work as a multi-systemic intervention is being undertaken through the development of state model demonstration grants for those experiencing illness or injury while in the workforce (US Department of Labor, 2018). Addressing the interaction between medical and career related factors is important and should be the foundation for career development research with adults with stroke (Koch & Rumrill, 2017).
Fourth, this model expands the traditional focus of career development research from the within-domain to the across-domain level. This is an important expansion because it enlarges the scope of the research focus and places an emphasis on more complex questions related to the interactions among career development, health, and treatment related factors. For example, the development of research questions that address the interaction between residual post-treatment health and functioning and the multiple factors within the career development domain would be important to address, and this would require advanced analysis to examine the multi-level and mediator and moderator effects between factors and domains.
Finally, this model provides an impetus for conducting research focused on developing interventions that emphasize effective interaction among multiple domains and between domain factors, because it takes into account direct and indirect effects. For example, an intervention directed at job maintenance should not exclusively address factors within the career development domain, but should also take into account factors from the contextual domain such as personal, environmental, and functional limitations. In addition, by examining direct and indirect effects, research can conceptualize and analyze the primary, secondary, and tertiary impact of interventions and conduct analyses using mediator and moderator variables to gain a full understanding of an interventions impact on the individual’s participation and overall physical and psychological well-being.
6Conclusion
In this article, we presented the IW2M as a multi-domain conceptual model designed to guide career development and employment research and services for individuals with stroke. The model’s domains and associated factors were explained, and participation in the areas of work, society, community, and home were conceptualized as outcomes of interest. Brief discussions of potential implications were presented at the service and research levels. It is our hope that the model will serve as a framework for broadening the scope and analysis of career and employment development services and research related to adults with stroke.
Author Note
Preparation of this article was partly funded by the United States Department of Labor, Office of Disability Employment Policy in the amount of $2.5 million under Cooperative Agreement No. OD-32548-18-75-4-21. This document does not necessarily reflect the views or policies of the U.S. Department of Labor, nor does mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government.
Conflict of interest
None to report.
References
1 | American Stroke Association. (2016). Impact of stroke. http://www.strokeassociation.org/STROKEORG/AboutStroke/Impact-of-Stroke-Stroke-statistics_UCM_310728_Article.jsp#.Vvh_yPkrJhE |
2 | Bishop, M , Chiu, C. ((2011) ). Epilepsy and employment. In PinikahanaJ. & WalkerC. (Eds.), Neurology – Laboratory and clinical research developments: Society, behaviour and epilepsy (pp. 93-114). Nova Biomedical Books. |
3 | Brede, E , Ikram, F , Howard, K , Asih, S. R , Knauf, M. T , Polatin, P. B. ((2016) ). Measurement of return to work and stay at work outcomes. In I. Z. Schultz, & R. J. Gatchel (Eds.), Handbook of return to work: From research to practice (pp. 181-206). Springer. |
4 | Centers for Disease Control and Prevention. (2015). Stroke. http://www.cdc.gov/stroke |
5 | Chan, F , Reid, C , Mathias Kaskel, L , Roldan, G , Rahimi, M , Mpofu, E. ((1997) ). Vocational assessment and evaluation of people with disabilities. Physical Medicine and Rehabilitation Clinics of North America, 2: (2), 311–325. 10.1016/S1047-9651(18)30328-0 |
6 | Conroy, B. E , Milani, F , Levine, M , Stein, J. ((2009) ). Vocational rehabilitation after stroke. In R. L. Harvey, R. F. Macko, J. Stein, C. Winstein, & R. D. Zarowitz (Eds.), Stroke recovery and rehabilitation (2nd ed., pp. 735-746). Demos Medical. |
7 | de Boer, H. M. ((2005) ). Overview and perspectives of employment in people with epilepsy. Epilepsia, 46: (s1)., 52–4. doi: 10.1111/j.0013-9580.2005.461016.x |
8 | Dutta, A , Gervey, R , Chan, F , Chou, C , Ditchman, N. ((2008) ). Vocational rehabilitation services and employment outcomes for people with disabilities: A United States study. Journal of Occupational Rehabilitation, 18: (4), 326–334. doi: 10.1007/s10926-008-9154-z |
9 | Falvo, D. R. ((2014) ). Medical and psychosocial aspects of chronic illness and disability (5th ed.). Jones & Bartlett Learning. |
10 | Gatchel, R. J , Choi, J. Y , Hanna, M. ((2018) ). Epidemiology of chronic illnesses: Associations with the aging population and future socioeconomic implications. In R. J. Gatchel, I. Z. Schultz, & C. T. Ray (Eds.), Handbook of rehabilitation in older adults (pp. 3-19). Springer. |
11 | Herr, E. L , Cramer, S. H. ((1992) ). Career guidance and counseling through the lifespan: Systematic approaches (4th ed.). Harper Collins. |
12 | Institute on Disability. ((2018) ). Annual disability statistics compendium: 2017 Disability statistics & demographics (2018). Institute on Disability: University of New Hampshire. https://disabilitycompendium.org/sites/default/files/user-uploads/Compendium_2017_Final.pdf |
13 | Koch, L , Rumrill, P. ((2017) ). Emerging disabilities in rehabilitation counseling. Springer. |
14 | Kwan, H.C. , & Schultz, I.Z. , Work accommodations: A social perspective. In In R. J. Gatchel, I. Z. Schultz, & C. T. Ray (Eds.), Handbook of rehabilitation in older adults (pp. 271-288). Springer. |
15 | Min, K , Min, J. ((2015) ). Health-related quality of life is associated with stroke deficits in older adults. Age and Ageing, 44: (4), 700–704. doi: 10.1093/ageing/afv060 |
16 | National Stroke Association. (2016). What is stroke? http://www.stroke.org/understand-stroke/what-stroke |
17 | Peterson, D. B , Rosenthal, D. A. ((2005) ). The international classification of functioning, disability and health (ICF): A primer for rehabilitation educators, Rehabilitation Education 19: (2-3), 81–94. |
18 | Peterson, G. W , Sampson Jr, J. P , Reardon, R. C. ((1991) ). Career development and services: A cognitive approach. Thomson Brooks/Cole Publishing Co. |
19 | Saeki, S. ((2000) ). Disability management after stroke: Its medical aspects for workplace accommodation. Disability & Rehabilitation, 22: (13), 578–582. doi: 10.1080/09638280050138241 |
20 | Sampson, J. P. ((2004) ). Career counseling and services: A cognitive information processing approach. Thomson/Brooks/Cole. |
21 | Saunders, D. E , Peterson, G. W , Sampson, J. P , Reardon, R. C. ((2000) ). Relation of depression and dysfunctional career thinking to career in decision. Journal of Vocational Behavior, 56: , 288–298. doi: 10.1006/jvbe.1999.1715 |
22 | Schouten, L , Murray, C , Boshoff, K , Sherman, K , Patterson, S. ((2011) ). Overcoming the long-term effects of stroke: Qualitative perceptions of involvement in a group rehabilitation programme. International Journal of Therapy & Rehabilitation 18: (4), 198–208. |
23 | Shaw, W. S , Main, C. J , Pransky, G , Nicholas, M. K , Anema, J. R , Linton, S. J. ((2016) ). Employer policies and practices to manage and prevent disability: Foreward to the special issue, Journal of Occupational Medicine, 26: (4), 394–398. |
24 | Strauser, D. R. ((2013) ). Introduction to the centrality of work for individuals with disabilities. In D. R. Strauser (Ed.), Career development, employment and disability in rehabilitation: From theory to practice. (pp. 1-11). Springer Publishing Company. |
25 | Strauser, D. R , Greco, C , O’Sullivan, D. ((2018) ). Career and lifestyle planning in vocational rehabilitation settings. In D. Capuzzi & M. D. Stauffer (Eds.), Career Counseling: Foundations, Perspectives, and Applications (3rd ed.; pp. 375-406). Routledge. |
26 | Strauser, D , Klosky, J. L , Brinkman, T. M , Wong, A. W , Chan, F , Lanctot, J , Ness, K. K. ((2014) ). Career readiness in adult survivors of childhood cancer: a report from the St. Jude Lifetime Cohort Study, Journal of Cancer Survivorship,, 8: (1), 1–10. |
27 | Strauser, D. R , O’Sullivan, D , Wong, A. W. ((2018) ). Career development and employment of people with disabilities. In V. M. Tarvydas & M. T. Hartley (Eds.), The Professional practice of rehabilitation counseling (pp. 273-296). Springer. |
28 | Thompson, H. S , Ryan, A. ((2009) ). The impact of stroke consequences on spousal relationships from the perspective of the person with stroke, Journal of Clinical Nursing 18: (12), 1803–1811. doi: 10.1111/j.1365-2702.2008.02694.x. |
29 | USDepartment of Labor. (2018). Office on Disability Employment Policy. https://www.dol.gov/odep/topics/SAW-RTW/how-to-apply.htm |
30 | Wang, Y , Kapellusch, J , Garg, A. ((2014) ). Important factors influencing the return to work after stroke. Work: Journal of Prevention, Assessment & Rehabilitation 47: (4), 553–559. |
31 | Zhang, Y , Chapman, A , Plested, M , Jackson, D , Purroy, F. ((2012) ). The incidence, prevalence, and mortality of stroke in France, Germany, Italy, Spain, the UK, and the US: A literature review. Stroke Research & Treatment, 1–11. doi: 10.1155/2012/436125 |


