
Exploring the frontiers of vestibular migraine: A case series
Abstract
INTRODUCTION:
Patients with episodic vestibular syndrome (EVS) whose symptoms resemble those of vestibular migraine (VM) but who do not meet the criteria for it are common.
OBJECTIVE:
To describe those patients suffering from EVS in whom defined etiologies have been ruled out in order to determine if their symptoms can be linked to VM.
MATERIAL AND METHODS:
Prospective multicenter study. The medical records of patients with VM and patients with EVS suggestive of VM but not meeting the criteria for it were examined. The characteristics of headache, the number and the length of attacks, the association of vestibular symptoms and headache, the intensity of symptoms and the response to treatment were recorded.
RESULTS:
58 patients met the criteria for VM or probable VM; 30 did not. All of the symptoms improved significantly in the treated patients with VM or probable VM; in the rest of the treated patients, only the vestibular symptoms improved.
CONCLUSION:
A subgroup of patients that cannot be attributed to any known vestibulopathy according to present day VM criteria profited from migraine treatment, suggesting that their vestibular symptoms belong to the migraine spectrum; whereas some do not, yet our analysis could not identify distinctive features that allowed subgroup attribution.
1Introduction
Vestibular migraine (VM) is a cause of episodic vestibular syndrome (EVS), which was defined in 2012 according to the criteria of the Bárány Society (cf. Table 1) [11]. Although the link between head-ache and vestibular symptoms (VS) was described in the late nineteenth century, it was not until the publication of these diagnostic criteria for VM that systematic studies could be performed using common inclusion criteria for patients. Since then, many studies have been published in an attempt to determine the physiopathology of VM [8, 10] and the most effective treatment for it [1, 7, 12–14].
Table 1
Diagnostic criteria for vestibular migraine [11]
| 1. Vestibular migraine |
| A. At least 5 episodes with vestibular symptoms of moderate or severe intensity, lasting between 5 minutes and 72 hours. |
| B. A current or previous history of migraine with or without aura according to the International Classification of Headache Disorders (ICHD). |
| C. One or more migraine features with at least 50%of the vestibular episodes: |
| •headache with at least two of the following characteristics: one-sided location, pulsating quality, moderate or severe pain intensity, aggravation by routine physical activity. |
| •photophobia and phonophobia. |
| •visual aura. |
| D. Not better accounted for by another vestibular or ICHD diagnosis. |
| 2. Probable vestibular migraine |
| A. At least 5 episodes with vestibular symptoms of moderate or severe intensity, lasting between 5 minutes and 72 hours. |
| B. Only one of the criteria B and C for vestibular migraine is met (migraine history or migraine features during the episode). |
| C. Not better accounted for by another vestibular or ICHD diagnosis. |
However, in the daily praxis, it is not hard to find patients presenting with EVS whose symptoms do not correspond to any known pathology but seem somehow suggestive of VM. This group includes patients who feel head pressure rather than headache, patients whose vertigo attacks are too short or too long to be classified as VM attacks, patients with too few attacks to be diagnosed as suffering from VM and patients who suffer from many attacks of non-migraine headache that is not associated with their VSs.
Three years ago, our group started a research project to find out what was the most effective prophylactic treatment for VM. This study had very strict inclusion criteria and the clinical researchers were shocked by the large number of patients with EVS in which VM was the main suspected diagnosis but the criteria for it were not met and other causes of EVS had been ruled out. These patients presented a clinical challenge for two reasons. Firstly, they could not be diagnosed, thus causing diagnostic uncertainty for both the clinicians and the patients themselves. Secondly, with no diagnosis, professionals were unsure as to what the most appropriate treatment would be. On the one hand, these patients would only be candidates for a generic symptomatic treatment; on the other hand, some authors, based on their clinical experience, have suggested trying a prophylactic treatment for VM despite the lack of a definitive diagnosis [4].
This is the reason for publishing this case series, which aims to quantify and describe the characteristics of patients suffering from EVS in which all known defined etiologies have been ruled out in order to determine if their clinical cases are linked in some way to VM.
2Material and methods
2.1Selection and grouping of the patients
This study is an analysis of a group of patients who were excluded from an earlier prospective multicenter study into the effectiveness of prophylactic treatment of VM as they did not meet the criteria for VM, as well as its comparison with those patients diagnosed of VM.
Firstly, all patients over the age of 14 who presented with a suspected diagnosis of VM at any of the Otoneurology Units of the seven participating hospitals between 2017 and 2018 were initially recruited. The candidates were then sorted according to the exclusion criteria in Table 2.
Table 2
Exclusion criteria for participation in this study
| Previous intake of any drug commonly used for migraine prophylaxis, regardless of the reason for having taken it. |
| Definite or probable Ménière’s disease according to the criteria of the Bárány Society [13]. |
| Vestibular paroxysmia according to the criteria of the Bárány Society [17]. |
| Acute vestibular syndrome in the past suggesting vestibular neuritis. |
| Any of the forms of benign paroxysmal positional vertigo, as defined by the criteria of the Bárány Society [3], in the last 180 days, except “probable BPPV, spontaneously resolved”. |
| Third window syndromes (excluded by using the Vasalva maneuver as the trigger of the vestibular symptoms). |
| Bilateral vestibulopathy (excluded by conducting tests of vestibular function on all patients). |
| Selective serotonin reuptake inhibitor (SSRI) withdrawal syndrome. |
| Any of the following focal neurologic deficits related to the vestibular crisis: impairment of ocular motricity, facial paralysis, sudden hearing loss, dysphagia, dysphonia, impaired lingual motricity, cerebellar symptoms such as dysmetria or ataxia, or deficits in corporal motricity or sensitivity. |
After this, the patients underwent a structured anamnesis that covered different items related to their history and the quantitative and qualitative characteristics of their symptoms. The intensity of headache and vertigo was recorded using a visual analogue scale (VAS) numbered from 0 to 100 and the number of monthly attacks was also recorded. Next, all of the patients were submitted to a systematic neurotological exploration that included an instrumental study of nystagmus, saccades, smooth pursuit and diagnostic positional maneuvers for benign paroxysmal positional vertigo (BPPV). Patients diagnosed as having concomitant BPPV according to any of the Bárány Society criteria [3] were excluded from the study. A magnetic resonance imaging (MRI) scan was carried out on all patients and patients with MRI scan results that could indicate other causes of episodic vestibular syndrome were excluded from the study. Patients who did not consent to participate in the study were also excluded.
Then, all of their medical records were studied in order to note the presence and the characteristics of headache, photophobia, photophobia, visual auras, the number of attacks experienced by each patient, the association of VSs and headache, and the length of the attacks. These variables were used to place patients in three groups. The two first groups were made up of patients who met the criteria for “vestibular migraine” and “probable vestibular migraine” according to the Bárány Society [11]. All patients who suffered from three or more attacks a month and where the intensity of said attacks had an impact on their daily lives were considered as candidates for receiving VM prophylaxis (acetazolamide, amitriptyline, flunarizine, propranolol or topiramate, depending on their clinical characteristics and according to an automatized algorithm that chose the best therapeutic option [6]). The rest of the patients were placed in a third heterogeneous group. Some of the patients in this third group were also considered as candidates for prophylactic treatment on an individual basis, depending on the impact that symptoms had on their daily lives.
Regardless of the group a patient was placed in, they were called back for a follow-up visit 5 weeks later if a prescription had been made. In this follow-up visit, patients were asked about their compliance with the treatment and the evolution of their symptoms (headache, VSs and number of attacks). If they had taken medication on 80%of the days or more, they were selected and their response to the treatment was evaluated.
2.2Analysis of data
First, a descriptive analysis was done in order to quantify the number of patients that made up each group. Then, the patients in the VM and probable VM groups were studied using paired data tests to see if their symptoms improved. Afterwards, both groups were compared with each other to see if they could be treated as one group.
After that, the third group of patients with EVS that did not meet the criteria for VM was analyzed to see the evolution of their symptoms. Later, the characteristics of the patients in all the groups were compared. Finally, this third group was divided into subgroups based on the presence or absence of headache, the absence or presence of migraine-like headache characteristics, the number of attacks, the association between headache and VSs, and the length of the attacks, and a descriptive analysis of these subgroups was performed.
2.3Ethical considerations
The informed consent of all of the patients was required for their inclusion in this study. The protocol of this research study was accepted by the ethics committee of the main participating hospital.
3Results
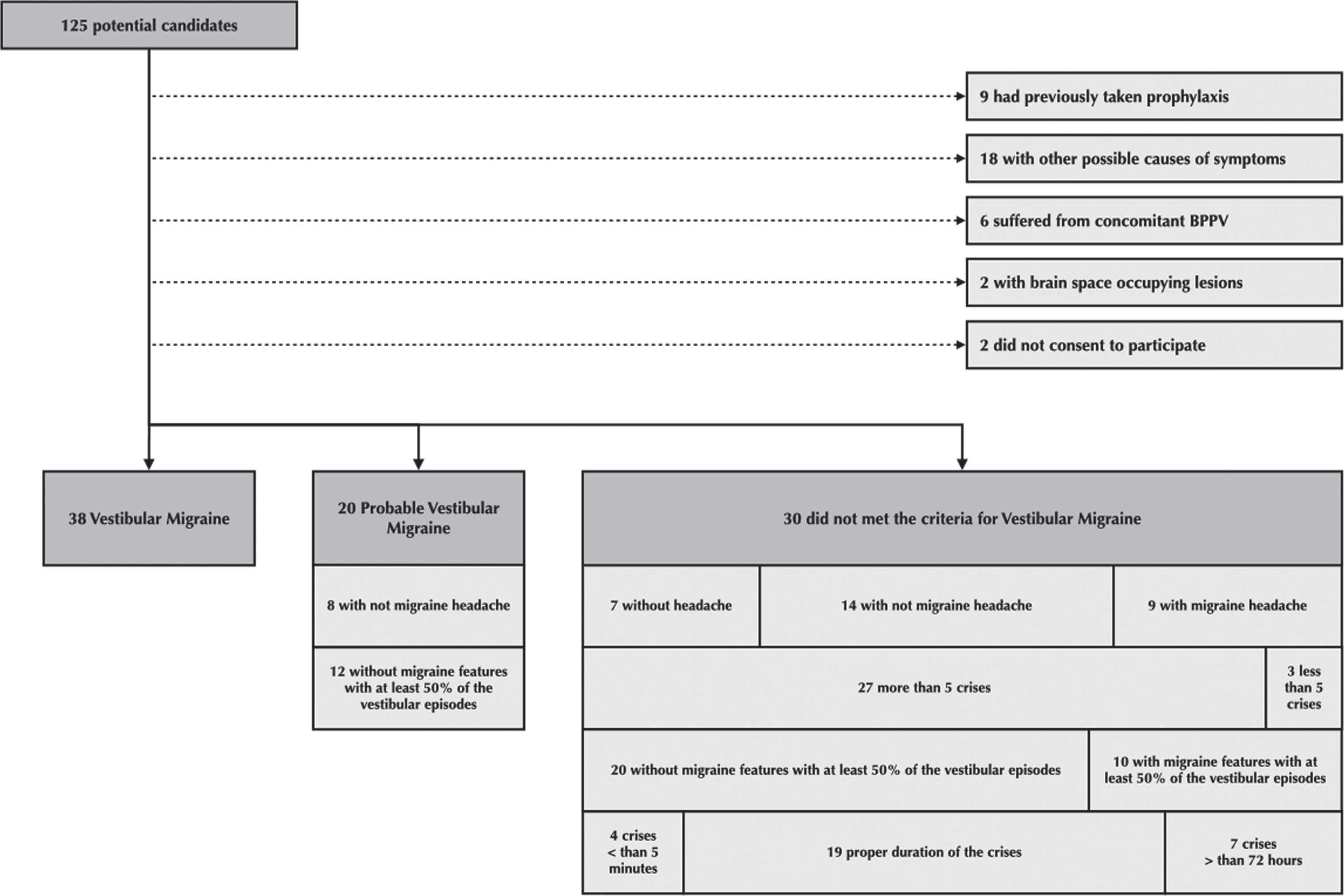
The initial sample of patients was made up of 125 patients. 9 of them had previously taken prophylaxis for migraine symptoms and they were thus excluded from the study. In 18 of the remaining patients, other causes of EVS could not be ruled out. These causes included situations such as having suffered from benign paroxysmal positional vertigo (BPPV) in the last six months, orthostatic hypotension, fluctuating hearing loss suggestive of Ménière’s disease and bilateral loss of vestibular function. 6 of the patients were suffering from BPPV at the time when they joined the study and they were also excluded. Brain space-occupying lesions were found in the MRI scans of 2 patients and therefore they were not taken into account for the analysis. Finally, 2 patients did not consent to participate in the study. Therefore, the final sample size was 88 patients. Figure 1 sketches the selection process.
Fig. 1
Screening of potential candidates to participate in the study and their division into three study groups.
The remaining patients were studied for three symptoms: headache intensity, intensity of VSs and the number of attacks. None of these were normally distributed according to the Kolmogorov-Smirnov test and thus non-parametric tests were used to perform the statistical comparisons.
When patients were assigned to groups, 38 patients met the criteria for VM, 20 patients met the criteria for probable VM (due to the fact that in 12 of them migraine symptoms did not accompany at least 50%of the vestibular episodes and in 8 of them the headache did not meet the criteria for migraine), and 30 were placed in the group of patients who did not fully meet one or more of the criteria for VM, hereafter known as the “borderline group”.
Firstly, the VM and probable VM groups were studied. Both groups showed a reduction in headache intensity (Wilcoxon signed-rank test p = 0.001 and p = 0.006 respectively), in the intensity of VSs (Wilcoxon signed-rank test p = 0.001 and p = 0.008 respectively) and in the number of attacks per month (Wilcoxon signed-rank test p = 0.049 and p = 0.008 respectively). Then, both groups were compared with each other. No significant difference was found in the percentage of females (78.9%vs. 75.0%; Fisher’s exact test p = 0.750), the median age (45 years in both; Mann-Whitney U-test p = 0.793), the distribution of the previous intensity of headache (Mann-Whitney U-test p = 0.206) or its differences (Mann-Whitney U-test p = 0.508), the distribution of the previous intensity of the VSs (Mann-Whitney U-test p = 0.363) or its differences (Mann-Whitney U-test p = 0.780), or the distribution of the monthly number of attacks (Mann-Whitney U-test p = 0.803) or its differences (Mann-Whitney U-test p = 0.079). In light of these results, the VM and probable VM groups were hereafter treated as one group known as the “unified group of VM” that included the VM and the probable VM patients. In this unified group of VM, 52 patients were given prophylaxis and 57.7%followed the course of treatment. All of the symptoms studied improved significantly in this group: headache, VSs and number of attacks (Wilcoxon signed-rank test p < 0.001, p = 0.001 and p = 0.002 respectively).
Next, the borderline group was analyzed. In this last group, 26 patients were given a prescription and 46.2%of them followed the course of treatment. When their symptoms were considered separately, only the VSs improved significantly (Wilcoxon signed-rank test p = 0.009), but headache intensity and the number of attacks did not ((Wilcoxon signed-rank test p = 0.139 and p = 0.534 respectively). The patients in the borderline group without headache were excluded before comparing headache intensity.
After this, the unified group of VM and the borderline group were compared. No significant difference was found in the percentage of females (77.6%vs 90.0%; Fisher’s exact test p = 0.126), the mean age (45.9 y. vs. 45.6 y.; Student’s t-test p = 0.922), the percentage of patients who had received treatment (89.7%vs 86.7%; Fisher’s exact test p = 0.729) or that of patients who had followed the course of treatment (57.7%vs 46.2%; Fisher’s exact test p = 0.349).
The borderline group was subsequently divided into subgroups. These subgroups were not mutually exclusive. Table 3 and Fig. 1 show the data for each of the groups and subgroups studied. A more detailed Table 3, called Table 4 can be consulted as a supplementary dataset. The results for each of the subgroups into which the 30 patients in the borderline group were placed are as follows:
a) 7 patients without headache: Firstly, the group with VSs but with no headache and that did not meet the criteria for probable VM was analyzed. They presented 85.7%of females and a mean age of 58.2 years. The median duration of the evolution of the symptoms was 0.7 years. Prophylactic treatment was prescribed for 4 of the 7 patients. The percentage of patients that met the criteria for prophylaxis was 57.1%; none of them followed the course of treatment. Despite this lack of compliance with the treatment, 3 out of 4 patients from this sub-subgroup were completely asymptomatic by the time of the follow-up visit. In relation to this fact, the percentage of patients in the unified VM group that had not taken their medication and were asymptomatic by the time of the follow-up visit was 40%.
b) 14 patients with non-migraine headache that did not meet the criteria for probable VM: Then, the subgroup that did not meet the criteria for the unified VM group and that suffered from headaches where these headaches did not meet the criteria for migraine was analyzed. 13 of them had had 5 or more episodes of vertigo, but headache was present in less than 50%of the vestibular episodes; in 2 of these 13 patients, the attack lasted over 72 hours and 12 of them received treatment. A fourteenth patient was included in this subgroup because they had had less than 5 episodes of VSs with headache in over 50%of them; they also received treatment. 61.5%of patients followed the course of treatment.
c) 3 patients attending a consultation in their first four attacks: The next subgroup analyzed was that made up of patients who were experiencing their first VS attacks. Two of them had migraine episodes, but this was not associated with the VSs in at least 50%of attacks because they suffered from continuous attacks lasting over 72 hours; the third patient, discussed in the previous section, suffered from non-migraine headache associated with attacks. A prophylactic treatment was prescribed for all patients and 2 of them followed the course of treatment, one from each sub-subgroup.
d) 20 patients with vestibular and migraine symptoms that were associated in less than 50%of the attacks: This subgroup was mainly made up of those with non-migraine headache with dissociated VSs (65%), but it also included those with migraine, dissociated VSs and atypical length of attacks (25%) and those with migraine and dissociated VSs in their first attacks (10%). 95%of those in this group were prescribed prophylaxis with a compliance rate of 52.6%of the cases.
e) 4 patients with attacks lasting under 5 minutes: These patients reported attacks that lasted between a few seconds and one minute. All of them had had more than 5 attacks and suffered from migraine, but the episodes were so short that it was impossible to associate migraine and VSs. All patients were prescribed prophylaxis and 50.0%of them followed the course of treatment.
f) 7 patients with attacks lasting over 72 hours: These patients reported attacks that lasted between 80 hours and 14 days. 71.4%of them suffered from migraine headache, 71.4%of them had had 5 or more attacks, and 28.6%of them had VSs associated with migraine in at least 50%of the cases. All of them were prescribed medication and 42.9%of them followed the course of treatment.
Table 3
Characteristics of the patients included in each of the groups. The difference between the intensity of the symptoms during the first visit and after treatment was calculated using only the data for patients who followed the course of treatment for 80%of the time or more
| Percentage of female | Median age | Patients with a prescription | Therapeutic compliance in the treated patients | Median of the differences of the intensity of headache before and after treatment | Median of the differences of the intensity of vestibular symptoms before and after treatment | Median of the differences of the numbers of attacks before and after treatment | |
| Vestibular migraine | 78.9% | 45.0 | 92.1% | 54.3% | 10.5 | 12.5 | 4.1 |
| Probable vestibular migraine | 75.0% | 45.0 | 85.0% | 64.7% | 23.0 | 24.0 | 18.3 |
| Total for the “unified VM group” | 77.6% | 45.0 | 89.7% | 57.7% | 9.5 | 10.5 | 8.1 |
| Patients without headache | 85.7% | 55.5 | 57.1% | 0% | - | - | - |
| Patients with non-migraine headache that did not meet the criteria for probable vestibular migraine | 92.9% | 41.5 | 92.9% | 72.7% | 18.0 | 46.5 | 1.2 |
| Patients with less than 5 attacks of VSs | 100% | 42.0 | 100% | 66.6% | 9.0 | 15.0 | 4.0 |
| Patients with migraine features in less than 50%of vestibular episodes | 95.0% | 42.0 | 95% | 52.6% | 28.0 | 46.5 | 2.1 |
| Patients with attacks lasting under 5 minutes | 100% | 46.5 | 100% | 50.0% | 36.5 | 46.0 | 7.7 |
| Patients with attacks lasting longer than 72 hours | 85.7% | 37.0 | 100% | 42.9% | 20.0 | 38.0 | 1.1 |
| Total for the “borderline group” | 90.0% | 47.0 | 86.7% | 46.2% | 10.5 | 41.5 | 0.7 |
Table 4
Characteristics of the patients included in each of the groups. The difference between the intensity of the symptoms during the first visit and after treatment was calculated using only the data for patients who followed the course of treatment for 80%of the time or more
| Percentage of female | Mean and median age | Patients with a treatment prescription | Therapeutic compliance in the treated patients | Mean and median intensity of headache | Mean and median intensity of vestibular symptoms | Mean and median number of crises | |||||||
| First visit | After treatment | Difference | First visit | After treatment | Difference | First visit | After treatment | Difference | |||||
| Vestibular migraine | 78.9% | 45.8 | 92.1% | 54.3% | 48.3 | 29.3 | 21.7 | 51.0 | 27.0 | 23.7 | 11.7 | 8.2 | 5.3 |
| 45.0 | 60.0 | 15.0 | 10.5 | 60.5 | 11.0 | 12.5 | 7.5 | 4.0 | 4.1 | ||||
| Probable vestibular migraine | 75.0% | 46.1 | 85.0% | 64.7% | 58.9 | 37.0 | 30.2 | 63.8 | 36.8 | 29.7 | 19.6 | 3.5 | 18.5 |
| 45.0 | 65.0 | 23.0 | 23.0 | 66.5 | 40.0 | 24.0 | 13.5 | 2.0 | 18.3 | ||||
| Total for the “unified VM group” | 77.6% | 45.9 | 89.7% | 57.7% | 52.0 | 31.7 | 20.9 | 55.4 | 33.0 | 20.1 | 14.4 | 5.8 | 9.1 |
| 45.0 | 64.0 | 21.5 | 9.5 | 65.5 | 20.0 | 10.5 | 8.0 | 2.6 | 8.1 | ||||
| Patients without headache | 85.7% | 58.2 | 57.1% | 0% | – | – | – | 52.7 | – | – | 18.6 | – | – |
| 55.5 | 60 | 4.0 | |||||||||||
| Patients with non-migraine headache that did not meet the criteria for probable vestibular migraine | 92.9% | 40.6 | 92.9% | 72.7% | 40.8 | 15.6 | 23.3 | 49.6 | 16.5 | 41.4 | 7.7 | 2.4 | 1.2 |
| 41.5 | 41.0 | 7.5 | 18.0 | 54.5 | 8.0 | 46.5 | 2.5 | 1.3 | 1.2 | ||||
| Patients with less than 5 crises of VSs | 100% | 44.0 | 100% | 66.6% | 61.7 | 38.5 | 9.0 | 54.7 | 36.5 | 15.0 | 1.0 | 13.7 | 6.2 |
| 42.0 | 90.0 | 38.5 | 9.0 | 61.0 | 36.5 | 15.0 | 1.0 | 13.7 | 4.0 | ||||
| Patients with migraine features in less than 50%of vestibular episodes | 95.0% | 42.2 | 95% | 52.6% | 56.0 | 20.5 | 28.2 | 59.4 | 20.4 | 45.3 | 10.1 | 5.2 | –0.8 |
| 42.0 | 67.5 | 8.5 | 28.0 | 60.0 | 8.5 | 46.5 | 4.5 | 2.6 | 2.1 | ||||
| Patients with crises lasting under 5 minutes | 100% | 47.7 | 100% | 50.0% | 68.7 | 8.5 | 36.5 | 62.2 | 8.5 | 46.0 | 20.0 | 4.3 | 7.7 |
| 46.5 | 82.5 | 8.5 | 36.5 | 70.0 | 8.5 | 46.0 | 21.0 | 4.3 | 7.7 | ||||
| Patients with crisis lasting longer than 72 hours | 85.7% | 37.3 | 100% | 42.9% | 51.3 | 48.7 | 2.0 | 66.4 | 42.0 | 53.7 | 4.7 | 9.7 | –4.7 |
| 37.0 | 50.0 | 70.0 | 20.0 | 93.0 | 55.0 | 38.0 | 2.0 | 2.6 | 1.1 | ||||
| Total for the “borderline group” | 90.0% | 45.6 | 86.7% | 46.2% | 49.9 | 23.9 | 18.1 | 55.7 | 22.3 | 40.9 | 11.2 | 4.5 | –0.7 |
| 47.0 | 50.0 | 8.5 | 10.5 | 60.0 | 9.5 | 41.5 | 4.0 | 1.7 | 0.7 | ||||
4Discussion
4.1Where are the outer limits of “vestibular migraine”?
The main conclusion that the authors want to highlight from the results of this study is that many patients that present with EVS with symptoms that are in some way suggestive of VM, and in which other causes of EVS have been ruled out, cannot currently be diagnosed with any known neurotologic disease. Such patients made up 34%of those that were finally selected, and this is a significant proportion of our sample.
VM, like other neurotologic entities, is diagnosed using criteria and these criteria constitute a diagnostic gold standard. This will continue to work like this until new diagnostic tests such as those using biomarkers [9] allow us to identify common physiopathological markers for these patients. Until such a time, criteria will be the only diagnostic tool available to us and hence they generate a compromise of sensitivity and specificity. In any case, the criteria should be specific enough to allow physicians to rely on them and sensitive enough to allow patients that could respond to medication to be treated.
The VM criteria of the Bárány Society state that “() a favorable response to anti-migraine drugs may support the suspicion of an underlying migraine mechanism. However, the apparent efficacy of a drug may be influenced by confounding factors (. . .)” [11]. According to this statement, we cannot use the response to treatment of patients in the borderline group to justify their inclusion in the group of patients with VM. Some of the patients of our borderline group improved, and this could lead us to think that the current criteria are not sensitive enough, but we could not prove that the positive response was due to the treatment or due to other factors such as spontaneous improvement or placebo response. In our opinion, when dealing with patients who suffer from VM, one has to keep in mind that the diagnosis is based on clinical criteria and that these criteria were defined to be specific. Therefore, some patients with EVS could not fulfill the VM criteria and still response to treatment as well as the patients who met criteria do, regardless of the reason for the improvement.
This fact should not be interpreted as a weakness of the criteria, but as a strength. When defining a new disease, it makes sense to prioritize specificity over sensitivity in order to study groups as homogeneous as possible. The aim of the new biomarkers will be to find out how far vestibular migraine goes and which of the current criteria are not necessary for diagnosis.
On the other hand, increasing sensitivity may lead to a loss of specificity. In this sense, we cannot rule out that some of these borderline group patients, or even all of them, suffer from diseases other than vestibular migraine, still unknown, but with common symptoms. This study is not intended to prove that all cases of episodic vestibular syndrome with headache can be considered vestibular migraine. Its objective is to describe what type of patients form the borderline group and how they respond to treatment. The study does not attempt to establish a pathophysiological relationship between patients with vestibular migraine and borderline patients by comparing their response to treatment.
However, from an empirical point of view, it is more interesting to identify those patients with a good response to treatment rather than finding out who suffers from a specific physiopathological disturbance. In this sense, the patients in the unified VM group showed significant improvements to all of the studied symptoms in the analysis of paired data; however, in the borderline group, only the VSs improved significantly. Therefore, further studies of the borderline group are needed in order to identify patients who could benefit from treatment.
4.2Is headache a necessary part of vestibular migraine?
8%of patients in the final selection had EVS without any kind of headache and their symptomatology improved spontaneously within 5 weeks in most cases. There were also patients who improved spontaneously in the unified VM group. These findings lead us to conclude that this group requires further attention in future research. Our data can neither confirm nor reject the idea that they suffer from a type of VM with a similar physiopathological substrate in which headache is not a symptom, but this means that we must evaluate whether it is necessary to prescribe treatment in these cases.
4.3Dissociated migraine or associated headache; what’s about dissociated not migraine headache?
According to the diagnostic criteria for VM [11], either criterion B. or C. must be present in order to make a diagnosis of probable VM. 13 out of 88 patients (14.8%) had headache and recurrent VSs, but none of the aforementioned criteria were met. These patients made up the majority of those included in sections b) and d) of the results section. This is a high percentage of the population with EVS suggestive of VM. Therefore, it is necessary to consider if the criteria for probable VM are too restrictive, as well as the possibility of creating new categories in the spectrum of VM, in order to identify groups of patients that could benefit from a treatment.
4.4Less than 5 attacks: current clues about these patients
Unfortunately, the group made up of patients that had had less than 5 attacks was small and was so heterogeneous that it was impossible to draw any strong conclusions. However, the existence of this group suggests that it is necessary to define what a VS attack is, to determine why some patients may experience continuous symptoms and to evaluate whether clinical trials are required in order to identify the best way of treating isolated attacks.
4.5Attacks shorter and longer than those in the VM criteria
According to the current criteria, the VM attacks have to last between 5 minutes and 72 hours; however, 12.2%of our patients reported attacks that were not included in this range. Shorter attacks need a differential diagnosis that includes vestibular paroxysmia [16], third-window syndromes, uncompensated vestibular hypofunction or SSRI withdrawal syndrome [2]. However, headache is not a characteristic part of any of them and thus, once these diagnoses have been ruled out, a VM prophylaxis may be attempted, although it is necessary to make a careful consideration of their risks and benefits due to the doubtful efficacy of the treatment. In the case of longer attacks, we believe that these may be caused by the persistence of mild symptoms between attacks of greater intensity. Bronstein et al. described this situation as “chronic vestibular migraine” and suggested treatment with migraine prophylaxis for these cases [5]. Based on our sample, we cannot systematically recommend treating these patients; however, this option must be considered. We are concerned that recently described persistent positional-perceptual dizziness [15] symptoms could interfere with the self-perception of the evolution of VM symptoms in this subgroup.
4.6When should I try migraine prophylaxis if the VM criteria are not met?
Never systematically. Based on our data, we recommend ruling out other causes when dealing with patients suffering from EVS (the exclusion criteria used for his study may be useful in this regard). Then, if the patient does not meet either of the VM criteria, one must judge whether the intensity of the symptoms impede or obstruct the patient’s daily life in such a way as to warrant treatment. In these cases, migraine prophylaxis should be tried, even though at present this treatment must be seen as compassionate. According to our series, some patients from the borderline group who followed their course of treatment saw improvements to their VSs, but we could not determine which of them did or if this improvement was caused by the prescribed treatment as no control group with a placebo treatment was included in the study.
5Conclusion
At present, a substantial percentage of patients suffering from episodic vestibular syndrome cannot be diagnosed, although some of them present with symptoms that seem somehow suggestive of vestibular migraine. Although the relationship between a prophylactic treatment for vestibular migraine and the improvement of symptoms remains doubtful to this day, a subgroup of patients that cannot be attributed to any known vestibulopathy according to present day VM criteria seemed to profit from migraine treatment, suggesting that their vestibular symptoms belong to the migraine spectrum; whereas some do not. Dissapointly, our analysis could not identify distinctive features that allowed subgroup attribution.
References
[1] | Bayer O. , Adrion C. , Al Tawil A. , Mansmann U. , Strupp M. , PROVEMIG investigators, Results and lessons learnt from a randomized controlled trial: prophylactic treatment of vestibular migraine with metoprolol (PROVEMIG), Trials 20: ((2019) ) , 813. |
[2] | Black K. , Shea C. , Dursun S. , Kutcher S. , Selective serotonin reuptake inhibitor discontinuation syndrome: proposed diagnostic criteria, J Psychiatry Neurosci JPN 25: ((2000) ) , 255–261. |
[3] | von Brevern M. , Bertholon P. , Brandt T. , Fife T. , Imai T. , Nuti D. , Newman-Toker D. , Benign paroxysmal positional vertigo: Diagnostic criteria, J Vestib Res Equilib Orientat 25: ((2015) ) , 105–117. |
[4] | Bronstein A. , Lempert T. , Recurrent vertigo and dizziness, in: Dizziness Pract. Approach Diagn. Manag., 1st ed., Cambridge University Press, (2009) , pp. 80–130. |
[5] | Bronstein A. , Lempert T. , Chronic dizziness and unsteadiness, in: Dizziness Pract. Approach Diagn. Manag., 2nd ed., Cambridge University Press, 2017, pp. 131–146. |
[6] | Domínguez-Durán E. , Baños-López P. , Martín-Castillo E. , Galera-Ruiz H. , Inter-rater agreement in the choice of prophylactic treatment for vestibular migraine and role of an assisted algorithm for this choice, Acta Otorrinolaringológica Esp 71: ((2020) ), 140–146. |
[7] | Domínguez-Durán E. , Montilla-Ibáñez M.A. , Álvarez-Morujo de Sande M.G. , Domènech-Vadillo E. , Bécares-Martínez C. , González-Aguado R. , Guerra-Jiménez G. , Analysis of the effectiveness of the prophylaxis of vestibular migraine depending on the diagnostic category and the prescribed drug, Eur. Arch. Oto-Rhino-Laryngol. Off. J. Eur. Fed. Oto-Rhino-Laryngol. Soc. EUFOS Affil. Ger. Soc. Oto-Rhino-Laryngol. - Head Neck Surg. (2020). |
[8] | Espinosa-Sanchez J.M. , Lopez-Escamez J.A. , New insights into pathophysiology of vestibular migraine, Front Neurol 6: ((2015) ), 12. |
[9] | Flook M. , Frejo L. , Gallego-Martinez A. , Martin-Sanz E. , Rossi-Izquierdo M. , Amor-Dorado J.C. , Soto-Varela A. , Santos-Perez S. , Batuecas-Caletrio A. , Espinosa-Sanchez J.M. , Pérez-Carpena P. , Martinez-Martinez M. , Aran I. , Lopez-Escamez J.A. , Differential Proinflammatory Signature in Vestibular Migraine and Meniere Disease, Front Immunol 10: ((2019) ). |
[10] | King S. , Priesol A.J. , Davidi S.E. , Merfeld D.M. , Ehtemam F. , Lewis R.F. , Self-motion perception is sensitized in vestibular migraine: pathophysiologic and clinical implications, Sci Rep 9: ((2019) ), 14323. |
[11] | Lempert T. , Olesen J. , Furman J. , Waterston J. , Seemungal B. , Carey J. , Bisdorff A. , Versino M. , Evers S. , Newman-Toker D. , Vestibular migraine: diagnostic criteria, J Vestib Res Equilib Orientat 22: ((2012) ), 167–172. |
[12] | Liu F. , Ma T. , Che X. , Wang Q. , Yu S. , The Efficacy of Venlafaxine, Flunarizine, and Valproic Acid in the Prophylaxis of Vestibular Migraine, Front Neurol 8: ((2017) ), 524. |
[13] | Salmito M.C. , Duarte J.A. , Morganti L.O.G. , Brandão P.V.C. , Nakao B.H. , Villa T.R. , Gananca F.F. , Prophy-lactic treatment of vestibular migraine, Braz J Otorhinolaryngol 83: ((2017) ), 404–410. |
[14] | Salviz M. , Yuce T. , Acar H. , Karatas A. , Acikalin R.M. , Propranolol and venlafaxine for vestibular migraine prophylaxis: A randomized controlled trial, The Laryngoscope 126: ((2016) ), 169–174. |
[15] | Staab J.P. , Eckhardt-Henn A. , Horii A. , Jacob R. , Strupp M. , Brandt T. , Bronstein A. , Diagnostic criteria for persistent postural-perceptual dizziness (PPPD): Consensus document of the committee for the Classification of Vestibular Disorders of the Bárány Society, Res Equilib Orientat 27: ((2017) ), 191–208. |
[16] | Strupp M. , Lopez-Escamez J.A. , Kim J.-S. , Straumann D. , Jen J.C. , Carey J. , Bisdorff A. , Brandt T. , Vestibular paroxysmia: Diagnostic criteria, J Vestib Res Equilib Orientat 26: ((2016) ), 409–415. |


