
A scoping review of the different types of exercise programs proposed for the improvement of postural balance in adolescents with idiopathic scoliosis
Abstract
BACKGROUND:
Adolescent idiopathic scoliosis (AIS), which is the most common type of scoliosis, is a progressive disease that occurs in children aged 10–16 years. Abnormal curvature in AIS provokes spinal asymmetry of the upper body alignment and might deteriorate postural balancing and control ability.
OBJECTIVE:
To evaluate the effect of exercise interventions on balance and postural stability in patients with adolescent idiopathic scoliosis.
METHODS:
Embase, Scopus, Pubmed (Medline) and Web of Science databases were searched using the terms idiopathic scoliosis, physiotherapy, and balance. The articles selected were published in English in peer-reviewed journals from 2012 to July 2022.
RESULTS:
Ten studies met the inclusion criteria. The PEDro scale values ranged from 2 to 6 (mean, 3.6), indicating a low level of scientific rigor. In the sample studies, spinal stabilization exercises were most often trialed (
CONCLUSIONS:
Physical therapists will be able to apply hippotherapy, Schroth exercise, physiotherapy scoliosis-specific exercise, trunk stabilization, proprioceptive neuromuscular facilitation exercise, spinal stabilization exercise, core stabilization exercise, and body awareness therapy to manage balance impairments in patients with adolescent idiopathic scoliosis, and further studies are needed to provide stronger evidence.
1.Introduction
Scoliosis is a type of structural three-dimensional spinal deformity accompanied by lateral deviation and abnormal sagittal curvature of the spine with a Cobb angle
However, the etiology of AIS remains unclear [3]. Genetic issues such as heredity, as well as endocrine, body mass, practice of high risk sports, and postural problems have been considered possible causes of AIS [3, 6, 7, 8]. Nutrients such as vitamin D, calcium, and melatonin had also been reported to occur and progress the symptom of AIS [9]. Furthermore, according to the neuro-osseous timing of maturation concept of Burwell et al., AIS patients have several abnormal growth factors [10]. AIS is usually regarded as pain-free; however, previous studies have revealed that AIS can produce negative effects on muscle imbalance, back pain, breathing dysfunction, and morphological problems [11, 12, 13, 14, 15]. In addition, the development of spinal deformities may lead to functional impairments and balance disorders [16, 17].
Abnormal curvature in AIS provokes spinal asymmetry of the upper body alignment and might deteriorate postural balancing and control ability [3]. Morphological deformity is closely related to the central nervous system, causing impairment of the sensory integrator process and a balance disorder of static stability [16]. However, some studies have shown that AIS patients do not have impaired postural balance when compared to healthy controls [18, 19], while several others have found an effect of AIS on postural balance [20, 21, 22]. Nault et al. reported that AIS patients showed increased sway area measured by enhanced anteroposterior center of pressure (COP) and center of mass compared with controls [23].
Scoliosis treatment options can be divided into surgical or conservative treatments, with the choice depending on the patient’s age, risk of disease progression, type of deformity, and quality of life [11, 24]. Among, conservative therapies, interventions such as brace, casting, specific scoliosis exercise, and core stabilization exercises have been used to alleviate pain, prevent curvature progression in AIS, and improve quality of life [2, 11]. In particular, therapeutic and specific exercises for scoliosis, such as Schroth exercise, pilates, and tai chi, could assist in the stabilization of curves, correct spinal alignment, and increase muscle strength and endurance [2, 25, 26, 27]. Exercises are commonly used alone or incorporated with a brace that facilitates self-correction of posture and improves self-awareness of general body alignment [1, 28, 29].
Exercise approaches have also been used to improve postural balance and stability in AIS patients. A previous study by Radwan et al. demonstrated that scoliosis exercise improved postural stability and Cobb angle in the AIS group compared with the control group [2]. AIS patients who are known to have a posteriorly shifted COP position on the sagittal plane, also have a greater postural instability than typically developed adolescents [30]. However, the currently available studies that investigated the effects of exercise on balance in AIS are inconsistent, and there is limited evidence on whether exercise treatments are effective in improving postural balance and stability [31, 32]. This scoping review aimed to evaluate the effects of exercise interventions on balance and postural stability in patients with AIS.
2.Methods
2.1Search strategy
Figure 1.
Flowchart of the study selection process based on PRISMA guidelines.
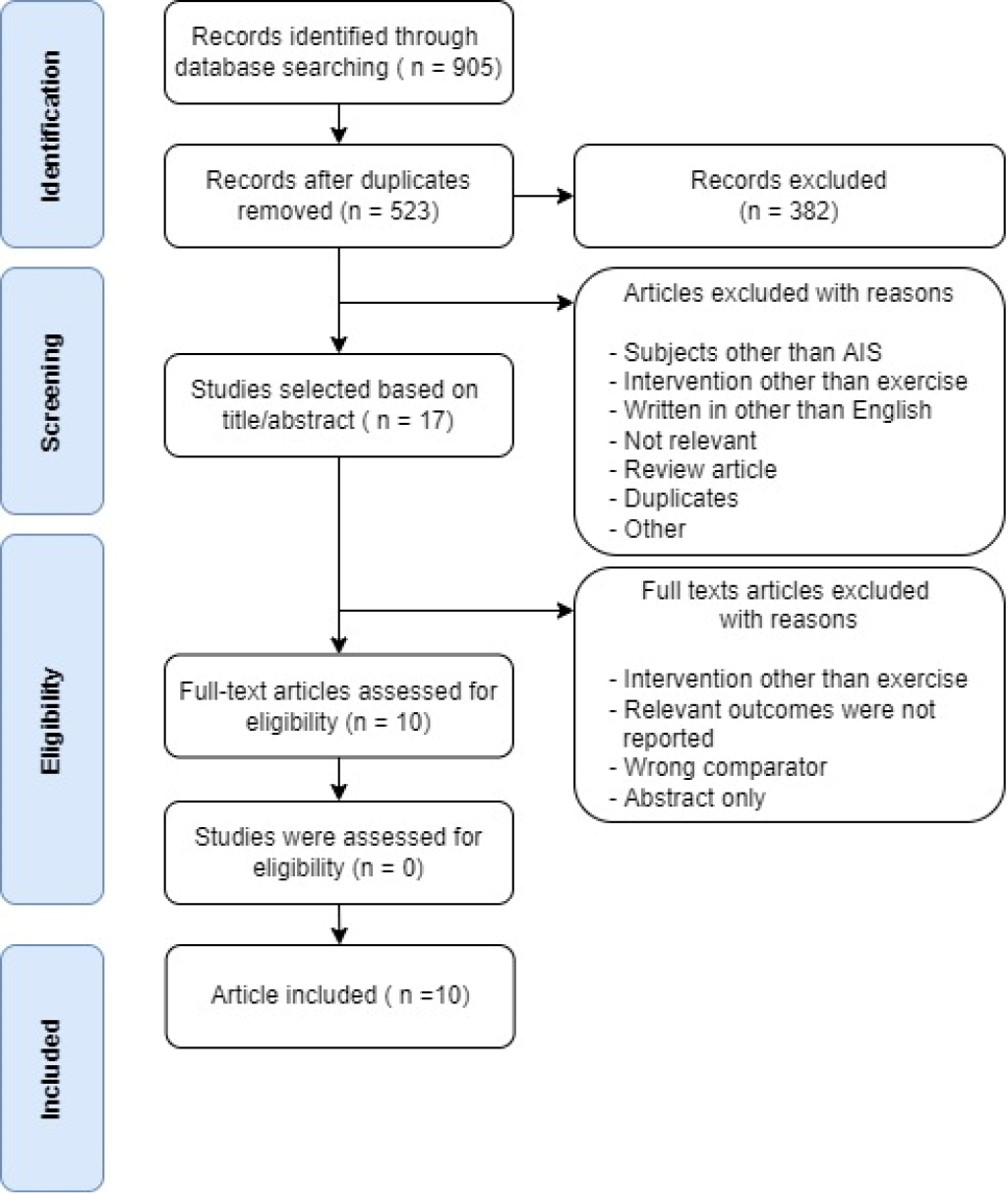
In this review, we utilized the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to describe the study selection procedure in the following four databases: Embase, Scopus, PubMed (Medline), and Web of Science. The keywords used were idiopathic scoliosis; AND one of the following: exercise, physiotherapy, physical therapy, rehabilitation, exercise therapy, therapeutic exercise, yoga, Pilates, or tai chi; AND one of the following: kinetic, kinematic, balance, stability, or postural control. The selected studies from each database were cross-checked by two researchers (SMB and SHK). Potentially relevant studies that included the above keywords in the title were screened according to inclusion criteria, and the final selection was validated by investigating relevant abstracts based on the inclusion criteria. Full-text articles from the selected studies were obtained and assessed for eligibility. The risk of bias was minimized by reviewing the titles, abstracts, and full-text articles independently by the two authors. If there was any disagreement on the selection of studies, the two researchers reached a consensus through discussion and third researcher (JHL) also participated in final decision (Fig. 1).
2.2Study selection
2.2.1Inclusion criteria
The PICOS principle was used to establish inclu-sion criteria as follows: P (population), subjects with adolescent idiopathic scoliosis; I (intervention), exercise in either experimental or control group; C (comparison), compared with non-scoliosis-specific exercise, conventional exercise or treatment, or no treatment (observation only); O (outcome), balance parameters such as center of pressure variance in antero-posterior and medio-lateral directions, COP sway area and velocity, body alignment and maximal tilt angle, foot pressure, and subjective postural perception; and S (study design); due to the limited number of available randomized controlled trial (RCT) studies, clinical, cross-sectional study, multi-group pre-test-posttest design, one-group pretest-posttest design, and single subject design were also included. Only studies written and published in English have been included.
2.2.2Exclusion criteria
(1) animal studies; (2) improper statistical methods or descriptions; (3) duplicate publications or incomplete data; (4) systematic reviews; (5) reviews; and (6) meta-analysis.
2.2.3Data extraction and evaluation of methodological quality
The titles and abstracts of the potentially relevant studies were screened. Two researchers extracted specific data, such as author and date of publication, characteristics of participants, study design, types of interventions, primary and secondary outcome measures, and key results from each selected study. All studies were assessed based on the inclusion criteria, and methodological quality was evaluated. The methodological quality of the selected studies was measured using the PEDro scale. The PEDro scale has verified the validity and reliability of assessing the methodological quality of clinical trials. The PEDro scale consists of 10 items: 1) random allocation of subjects; 2) concealed allocation; 3) similar prognosis at baseline; 4) blind subjects; 5) blind therapists; 6) blind assessors; 7) more than 85% follow-up; 8) intention-to-treat analysis; 9) between-group statistical analysis; and 10) point of variability. PEDro scores of 0–3 are regarded as poor, 4–5 as fair, 6–8 – regarded as good and 9–10 are regarded as excellent [33]. Studies with the above information in the title or abstract were eligible for inclusion. Only studies written and published in English were included (Table 1).
The investigation was reviewed by the Institutional Review Board of Baekseok University, Republic of Korea (BUIRB-202210HR-027) and deemed exempt from ethical approval.
Table 1
Level and methodological quality of the evidence at PEDro scale
| Author and year | Level of evidence | Eligibility criterion | Random allocation of subjects | Concealed allocation | Similar prognosis at Baseline | Blinded subjects | Blinded therapists | Blind assessor | More than 85% follow-up | Intention to-treat analysis | Between group statistical analysis | Point of variability | Total score |
| Abdel-aziem et al. [31] | Good | Yes | Yes | No | No | No | No | Yes | Yes | No | Yes | Yes | 6 |
| Levi et al. [34] | Fair | Yes | Yes | No | No | No | No | No | Yes | No | Yes | Yes | 5 |
| Radwan, Ibrahim, and Mahmoud [2] | Fair | Yes | No | No | No | No | No | No | Yes | No | Yes | Yes | 4 |
| Marin et al. [35] | Poor | No | No | No | No | No | No | No | Yes | No | No | Yes | 2 |
| Bidari et al. [32] | Fair | Yes | No | No | No | No | No | No | Yes | No | Yes | Yes | 4 |
| Selthafner et al. [37] | Poor | Yes | No | No | No | No | No | Yes | Yes | No | No | Yes | 3 |
| Shin, Lee, and Song [4] | Poor | yes | No | No | No | No | No | No | Yes | No | No | Yes | 2 |
| Lee [38] | Poor | No | No | No | No | No | No | No | Yes | No | No | Yes | 2 |
| Lee and Shim [39] | Poor | Yes | No | No | No | No | No | No | Yes | No | No | Yes | 2 |
| Yagci, Yakut, and Simsek [40] | Good | Yes | Yes | No | Yes | Yes | No | No | yes | no | yes | Yes | 6 |
Table 2
Studies that investigating the effects of exercise on balance parameter
| Author and year | Study design | Number and age of experimental group | Number and age of control group | Cobb’s angle of experimental group | Cobb’s angle of control group | Intervention vs control | Outcome measures | Results |
|---|---|---|---|---|---|---|---|---|
| Abdel-aziem et al. [31] | RCT (longitudinal) | 27 (19 girls), mean age 14.74 | 25 (18 girls), mean age 15.04 | 18.59 | 19.32 |
| OSI, APSI, and MLSI | Both group showed significantly improved balancing ability (OSI, APSI, and MLSI), but more effectively in experimental group. |
| Levi et al. [34] | RCT (crossover) | 18 girls, age between 10–18 years. | Same as experimental group | 20–50 | Same as experimental group |
| Measuring changes of head, upper trunk, lower trunk, and pelvic angle during maintaining posture exercise | Stretching exercise prior to performing posture maintaining exercise reduced the ability to maintain the trunk postural alignment. |
| Radwan, Ibrahim and Mahmoud [2] | Pretest-posttest controlled (longitudinal) | 20 girls, mean age 13.86 | 20 girls, mean age 14.34 | 24.13 | Not measured (healthy girls) |
| OSI, APSI, and MLSI | Schroth exercises under a specialist’s supervision had positive effects on improving postural stability indices (OSI, APSI, and MLSI). |
| Marin et al. [35] | Cross-sectional | 10 girls, mean age 13.8 | None | 14.1 | None |
| Sway-X, Sway-Y, Sway Area, Speed Sway | Sway parameter of the COP in standing position and during the performance of self-elongation had no significant differences. |
| Bidari et al. [32] | Cross-sectional | 17 (12 girls), mean age 15 | None | Mean 23.3 | None | None | COP-AP and COP-ML standing on solid or foam surface with and without brace | No significant differences in all balance parameters among the three groups; Patients were allocated into three groups (good, ordinary and weak) according to the quality and amount of exercise performed. |
| Selthafner et al. [37] | One-group pretest-posttest design (longitudinal) | 6 girls, age between 10–18 years. | None | Mean 26 | None |
| COP-AP, COP-ML, COP-OS, and max pressure at the forefoot, midfoot and hindfoot | PSSE intended to improve dynamic posture allows the patient’s trunk to lean forward and have less sway in the coronal plane. |
| Shin, Lee and Song [4] | One-group pretest-posttest design (longitudinal) | 18 (15 girls), mean age 14 | None | 31.4 | None |
| Mean balance, AP sway angle, ML sway angle, sway area, sway path, maximum velocity with EO or EC | AP sway angle, sway area and sway path during with EO or EC were significantly decreased and ML sway angle with EC was also significantly decreased. |
|
Table 2, continued | ||||||||
|---|---|---|---|---|---|---|---|---|
| Author and year | Study design | Number and age of experimental group | Number and age of control group | Cobb’s angle of experimental group | Cobb’s angle of control group | Intervention vs control | Outcome measures | Results |
| Lee [38] | Single-subject design | Single female subject, age 21 years. | None | None | None |
| COP-TL, C90A, and sum of maximum tilt angles in four directions | Balancing abilities after 6-week PNF exercise program were improved compared to the baseline values. |
| Lee and Shim [39] | One-group pretest-posttest design (longitudinal) | 10 (5 girls), mean age 10.2 | None | 14.5 | None |
| Plantar pressure of eight plantar areas during walking with a bag load of 0% or 15% of their body weight | Plantar pressure of fifth metatarsal head and lateral heel during walking with the bag load of 15% of their body weight were significantly decreased after spinal stabilization exercise. |
| Yagci, Yakut and Simsek [40] | Multi-group pretest-posttest design (longitudinal) | 32 girls, age between 10–16 years. | None | Thoracic Cobb angle of 32.29 | None |
| Subjective postural perception | Subjective postural vertical perception and the total SPP score improved in the CSE and the BBAT groups, although there was no change in the TE group. There was no difference between the CSE and BBAT groups. For SPP parameters of 60 |
Abbreviation: RCT, randomized controlled trial; OSI, overall stability index; APSI, anteroposterior stability index; MLSI, mediolateral stability index; COP, center of pressure; COP-AP, anteriorposterior center of pressure; COP-ML, mediolateral center of pressure; COP-OS, center of pressure oscillation; PSSE, physiotherapy scoliosis-specific exercise; AP, anteroposterior; ML, mediolateral; EO, eyes opened; EC, eyes closed; PNF, proprioceptive neuromuscular facilitation; COP-TL, center of pressure trace length; C90A, center of pressure 90%-confidence-level ellipse area; BBAT, basic body awareness therapy; CSE, core stabilization exercise; TE, traditional exercise; SPP, subjective postural perception.
3.Results
The results of the final 10 articles are summarized in Table 2.
3.1Hippotherapy and Schroth’s exercise
Abdel-aziem et al. reported that the overall stability index (OSI), anteroposterior stability index (APSI), and mediolateral stability index (MLSI) significantly decreased after Schroth’s exercise alone or with hippotherapy in patients with AIS [31]. Post-intervention, the Schroth’s exercise with hippotherapy group showed significantly lower OSI, APSI, and MLSI than the group with Schroth’s exercise alone.
Radwan, Ibrahim, and Mahmoud also demonstrated the effects of Schroth’s exercise for three months on OSI, APSI, and MLSI in patients with AIS [2]. The OSI decreased significantly with each measurement (baseline, one-month and three-months post-intervention). The APSI score significantly decreased from baseline to one-month or three-month post-intervention. One month post-intervention, MLSI was significantly decreased compared to baseline, and three-month post-intervention was significantly decreased compared to one-month post-intervention.
3.2Stretching exercise
Radwan et al. measured the head, upper trunk, lower trunk, and pelvic angles during postural exercise to quantify the ability to maintain postural body alignment in patients with AIS [34]. The head and pelvic angles during postural exercise showed no significant differences before and after the stretching exercises. However, the upper and lower trunk angles were significantly increased after stretching exercise.
3.3Self-elongation exercise
Marin et al. measured the displacement of the COP during self-elongation (SE) exercises in patients with AIS [35]. However, the maximum display of the COP along the medio-lateral or anteroposterior direction, the total sway area, and the speed of the COP displacement showed no significant difference between the standing position and the performance of SE.
3.4Exercise protocol of Blount and Moe
Bidari et al. demonstrated the effect of exercise based on the Blount and Moe protocol [36] on static balance in patients with AIS [32]. Patients were allocated into three groups (good, ordinary, and weak) according to the quality and amount of exercise performed, and there were no significant differences in all balance parameters (anterior-posterior or medio-lateral COP displacement on firm or foam surface, with or without brace) among the three groups.
3.5Physiotherapeutic scoliosis-specific exercise
Selthafner et al. demonstrated the effects of physiotherapy scoliosis-specific exercise (PSSE) on postural sway in AIS [37]. Although not statistically analyzed, COP displacement in the anterior-posterior direction increased by 15% and COP displacement in the mediolateral direction decreased by 25%. The COP oscillation effectively moved away from the midline by approximately 16% on the left. The oscillation of the entire body from the midline became more symmetrical after PSSE. For the maximum pressure of the foot, improvements were observed in the forefoot at the left fifth metatarsal (
3.6Lumbar stabilization exercise
Shin, Lee, and Song reported that lumbar stabilization exercise (LSE) effectively improved sitting balance of AIS [4]. With the eyes open, there were significant decreases in the anteroposterior sway angle, sway area, and sway path after LSE. However, sitting balance parameters such as mean balance, right-left sway angle, and maximum velocity were not significantly different. With the eyes closed, the anterior-posterior sway angle, right-left sway angle, sway area, and sway path significantly decreased after LSE. There were no significant differences in the mean balance and maximum velocity.
3.7Proprioceptive neuromuscular facilitation exercise
A single case study by Lee revealed the effects of proprioceptive neuromuscular facilitation (PNF) exercise programs on balancing abilities in female patients with AIS [38]. For the static balance test, sway of the posture on the COP measured by the trace length and COP confidence ellipse area decreased after the 6-week PNF exercise program. Furthermore, the weight distribution between the two feet was even. For the dynamic balance test, dynamic balancing ability symmetry expressed by the maximum leaning angle showed a maintained balance after the PNF exercise programs.
3.8Spinal stabilization exercise
Spinal stabilization exercises (SSE) also affected the dynamic foot pressure of AIS in a study by Lee and Shim [39]. Although plantar pressure measurements of the bag load of 0% of the subjects’ body weight before and after the SSE showed no significant difference, the two areas of the fifth metatarsal and lateral heel had significantly lower plantar pressure with a bag load of 15% of the subjects’ body weight after the SSE.
3.9Core stabilization exercise and basic body awareness therapy
Yagci, Yakut and Simsek investigated the effects of core stabilization exercise (CSE) and basic body awareness therapy (BBAT) on perception of verticality in AIS [40]. Subjective postural vertical perception and total subjective postural perception (SPP) score significantly increased after CSE and BBAT, but there was no significant difference after traditional exercise (TE). However, no significant difference was observed between the CSE and BBAT groups. For SPP parameters at 60
4.Discussion
The purpose of this scoping review was to evaluate the effects of exercise interventions on balance and postural stability in patients with AIS. According to the results from 10 articles that investigated the effects of exercise programs, several exercises improved the balance parameters such as OSI, APSI, and MLSI.
During hippotherapy, precise, rhythmic, and repetitive patterns of movement that mimic human gait are given to riders, and riders activate stabilizing muscles as a reaction [31, 41, 42]. This riding intervention provides vestibular stimulation, and riders who adapt to the movements of horses change muscle utilization by developing neuromuscular coordination [31, 43, 44]. Therefore, it seems that the activation of the trunk core muscles caused by horse riding contributes to improving OSI, APSI, and MLSI in patients with AIS.
Similarly, the Schroth exercise is also core muscle training and consists of three-dimensional self-correction and stabilization of the corrected posture, as well as patient education [45, 46]. This individualized, corrective breathing exercise causes the contraction of convex areas of the trunk; thus, lengthening and mobilization of soft tissues are provoked in concave areas by directing the inspired air [2, 47]. Thus, improvements in trunk symmetry, weight distribution, and neuromuscular control following corrective exercise can trigger improvements in stability indices, such as OSI, APSI, and MLSI [2].
However, stretching exercises appear to have a negative effect on balance in AIS [34]. Nelson, Kokkonen, and Arnall reported that the stretching technique converts motor units into a fatigue-like state, which decreases the pool of motor units available for activation [48]. This loss of motor units eventually leads to a decrease in performance [48]. Furthermore, static stretching also decreases the viscosity of tendon structures, which results in a reduction in the ability to produce force [34, 49]. For these reasons, stretching prior to tasks negatively affects motor learning [34]. In addition, despite of characteristics of scoliosis as an asymmetric and three-dimensional deformity, it seems there is a lack of studies applied stretching exercises to every muscle involved. Nevertheless, the application of stretching exercise should be considered carefully, since a recent study reported the asymmetry of erector spinae tone in the thoracic or lumbar region in children aged 7–8 with scoliosis [50].
The SE and Blount and Moe exercise protocols had no effect on the dynamic or static balance in AIS [32, 35]. SE involves a variation of the spine that depends on a linear combination of the positions in the pelvis, thoracic spine, lumbar spine, and sacral spine [35]. The Blount and Moe exercise protocol also focuses on the orientation of body segments and curve correction [32]. However, balance impairments in patients with AIS are under the control of the central processing of balance, and it seems that SE or Blount and Moe exercise protocols may have no direct effect on the central nervous system that processes balance control [32].
PSSE decreased COP sway in the coronal plane and pressure of the forefoot and medial hind foot, indicating a procedure for creating proper equilibrium, leading to improved symmetry [37]. When comparing PSSE with the Schroth method, which incorporates sensorimotor, postural, and breathing exercises, and spine stabilization exercises, PSSE has both characteristics. PSSE has been utilized to improve postural static and dynamic balance and correct postural alignment during functional activities [51, 52]. In a study by Selthafner et al., PSSE altered postural control patterns and weight distribution in subjects with AIS [37].
Webber et al. demonstrated that trunk stabilization decreased peak lumbar acceleration during the motion of the upper and lower extremities [53]. Shin, Lee, and Song demonstrated that LSE provided trunk stability for static postural control, and thus reduced sway angle, area, and path, suggesting improved postural balance [4]. In addition, LSE with the eyes closed changed mediolateral sway compared to open eyes because individuals with AIS depend more on proprioception than visual input to maintain balance [22].
Lee demonstrated that a 6-week PNF exercise program increased static and dynamic balance compared to baseline by reducing trace length and sway area and increasing the leaning angle in balance test [38]. The PNF program has been proven effective in correcting spine alignment and enhancing static and dynamic balance [54]. Lee utilized the PNF technique to stabilize the lumbopelvic system during bridge exercises by manual resistance, which progressively narrowed the supporting plane [38]. This PNF technique and instruction decreased spinal deformity and increased the strength of the abdominal muscles, which are associated with balancing ability [38].
Lee and Shim found that spinal stabilization exercises improved balancing ability by effectively spreading the distribution of plantar pressure when a load was applied [39]. In the standing position, the foot is the first body region that contacts the external surface, and plantar pressure is used to diagnose foot problems [56]. To maintain body balance, sensory input is critical for generating normal spinal and pelvic alignment, physical balance, and stability during walking [57, 58, 59]. Park et al. demonstrated that the movement patterns of plantar pressure in both feet were correlated with the magnitude of scoliosis, which affects foot balance [60]. Spinal stabilization exercise may be an effective exercise to prevent morphological changes and improve neuromotor control and physical balance stability.
Yagci, Yakut and Simsek showed that SPP was improved in BBAT and CSE [40]. These results may be associated with improved motor coordination and an upright body orientation. In particular, BBAT educates deep spinal muscles, thereby facilitating postural awareness, dynamic balancing ability, and coordination [61]. CSE stimulates the proprioceptive facilitation effect for correcting contraction of the stabilizer by providing feedback about trunk position, as well as enhanced endurance of core muscles that are essential for maintaining dynamic stability of the spine [62]. Both BBAT and CSE restored the capacity for body awareness and remained upright; thus, they may have a better SPP [63].
AIS patients have fear and dissatisfaction with the abnormal growth and appearance of their bodies [64]. Applying exercise to AIS patients with incorrect perceptions of their spine would help overcome physical and psychological discomfort [65]. In addition, the postural control ability obtained through exercise would help improve self-proprioception through the promotion of spin alignment, resulting in an improvement in response to the rehabilitation process [66]. Thus, the results of the present study can be useful in prescribing exercise therapy for patients with AIS.
This study has several limitations. First, the 10 studies included in this review had a poor to good level of evidence derived from the PEDro scale. Furthermore, only three studies had a control group design. Second, patient characteristics such as Cobb angle, curve type, and type of intervention were heterogeneous. Third, several studies omitted the statistical analysis or failed to demonstrate a significant difference between the groups. Therefore, further studies including high-quality RCT or applying a blinding design, with the qualification of heterogeneity of patients, are needed.
5.Conclusion
Our results revealed that the effects of different types of exercise on balance in AIS remain controversial. Emerging evidence has shown that interventions stimulating the postural system such as hippotherapy, Schroth exercise, PSSE, trunk stabilization, PNF exercise, spinal stabilization exercise, BBAT, and CSE improve postural balance, but geometric and mechanical detorsion such as stretching and self-elongation exercises do not affect postural balance in patients with AIS. Therefore, physical therapists will need to apply exercise therapy carefully to manage balance impairments in patients with AIS, and further studies are needed to provide stronger evidence.
Ethical approval
The investigation was reviewed by the Institutional Review Board of Baekseok University, Republic of Korea (BUIRB-202210HR-027) and deemed exempt from ethical approval.
Funding
This research was funded by the Ministry of Education (NRF-2021R1G1A1093552).
Informed consent
Not applicable.
Author contributions
All authors contributed to the concept, design, data collection, and analysis of this study.
Acknowledgments
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF).
Conflict of interest
The authors declare that they have no conflict of interest.
References
[1] | Fan Y, Ren Q, To MKT, Cheung JPY. Effectiveness of scoliosis-specific exercises for alleviating adolescent idiopathic scoliosis: a systematic review. BMC Musculoskelet Disord. (2020) ; 21: : 495. doi: 10.1186/s12891-020-03517-6. |
[2] | Radwan NL, Ibrahim MM, Mahmoud WS. Comparison of two periods of Schroth exercises for improving postural stability indices and Cobb angle in adolescent idiopathic scoliosis. J Back Musculoskelet Rehabil. (2021) ; doi: 10.3233/BMR-200342. |
[3] | Schimmel JJ, Groen BE, Weerdesteyn V, de Kleuver M. Adolescent idiopathic scoliosis and spinal fusion do not substantially impact on postural balance. Scoliosis. (2015) ; 10: : 1-8. |
[4] | Shin SS, Lee YW, Song CH. Effects of lumbar stabilization exercise on postural sway of patients with adolescent idiopathic scoliosis during quiet sitting. Journal of Physical Therapy Science. (2012) ; 24: : 211-215. |
[5] | Kuznia AL, Hernandez AK, Lee LU. Adolescent idiopathic scoliosis: common questions and answers. Am Fam Physician. (2020) ; 101: : 19-23. |
[6] | Kinikli GI, Yüksel, İ, Yakut Y, Alanay A, Yazici M. Alterations of postural sway in adolescent idiopathic scoliosis. Fizyoterapi Rehabilitasyon. (2011) ; 22: : 17-22. |
[7] | Scaturro D, Balbo A, Vitagliani F, Stramazzo L, Camarda L, Letizia Mauro G. Is There a Relationship between Idiopathic Scoliosis and Body Mass? A Scoping Review. Nutrients. (2022) ; 14: : 4011. doi: 10.3390/nu14194011. |
[8] | Scaturro D, Costantino C, Terrana P, Vitagliani F, Falco V, Cuntrera D, Emilia Sannasardo C, Vitale F, Letizia Mauro G. Risk Factors, Lifestyle and Prevention among Adolescents with Idiopathic Juvenile Scoliosis: A Cross Sectional Study in Eleven First-Grade Secondary Schools of Palermo Province, Italy. Int J Environ Health Res. (2021) ; 18: : 12335. doi: 10.3390/ijerph182312335. |
[9] | Herdea A, Dragomirescu MC, Ulici A, Lungu CN, Charkaoui A. Controlling the progression of curvature in children and adolescent idiopathic scoliosis following the administration of Melatonin, Calcium, and Vitamin D. Children. (2022) ; 9: : 758. doi: 10.3390/children9050758. |
[10] | Burwell RG, Dangerfield PH, Freeman BJC. Etiologic theories of idiopathic scoliosis. Somatic nervous system and the NOTOM escalator concept as one component in the pathogenesis of adolescent idiopathic scoliosis. Research into Spinal Deformities 6th; edition. IOS Press, (2008) . |
[11] | Veis Karami M, Aboutorabi A, Ebrahimzadeh K, Arazpour M, Asare E. The effect of orthotic interventions on balance performance in adolescent idiopathic scoliosis: A systematic literature review. Assist Technol. (2020) ; 32: : 260-267. doi: 10.1080/10400435.2018.1539419. |
[12] | Agabegi SS, Kazemi N, Sturm PF, Mehlman CT. Natural History of Adolescent Idiopathic Scoliosis in Skeletally Mature Patients: A Critical Review. J Am Acad Orthop Surg. (2015) ; 23: : 714-723. doi: 10.5435/JAAOS-D-14-00037. |
[13] | Bettany-Saltikov J, Parent E, Romano M, Villagrasa M, Negrini S. Physiotherapeutic scoliosis-specific exercises for adolescents with idiopathic scoliosis. Eur J Phys Rehabil Med. (2014) ; 50: : 111-121. |
[14] | Fortin C, Pialasse JP, Knoth IS, Lippe S, Duclos C, Simoneau M. Cortical dynamics of sensorimotor information processing associated with balance control in adolescents with and without idiopathic scoliosis. Clin Neurophysiol. (2019) ; 130: : 1752-1761. doi: 10.1016/j.clinph.2019.07.005. |
[15] | Ramirez N, Johnston CE, Browne RH. The prevalence of back pain in children who have idiopathic scoliosis. J Bone Joint Surg Am. (1997) ; 79: : 364-368. doi: 10.2106/00004623-199703000-00007. |
[16] | Guo X, Chau WW, Hui-Chan CW, Cheung CS, Tsang WW, Cheng JC. Balance control in adolescents with idiopathic scoliosis and disturbed somatosensory function. Spine (Phila Pa 1976). (2006) ; 31: : E437-440. doi: 10.1097/01.brs.0000222048.47010.bf. |
[17] | Leteneur S, Simoneau-Buessinger E, Barbier F, Rivard CH, Allard P. Effect of natural sagittal trunk lean on standing balance in untreated scoliotic girls. Clin Biomech (Bristol, Avon). (2017) ; 49: : 107-112. doi: 10.1016/j.clinbiomech.2017.09.004. |
[18] | Driscoll DM, Newton RA, Lamb RL, Nogi J. A study of postural equilibrium in idiopathic scoliosis. J Pediatr Orthop. (1984) ; 4: : 677-681. doi: 10.1097/01241398-198411000-00004. |
[19] | Kuo FC, Wang NH, Hong CZ. Impact of visual and somatosensory deprivation on dynamic balance in adolescent idiopathic scoliosis. Spine (Phila Pa 1976). (2010) ; 35: : 2084-2090. doi: 10.1097/BRS.0b013e3181cc8108. |
[20] | Beaulieu M, Toulotte C, Gatto L, Rivard CH, Teasdale N, Simoneau M, Allard P. Postural imbalance in non-treated adolescent idiopathic scoliosis at different periods of progression. Eur Spine J. (2009) ; 18: : 38-44. doi: 10.1007/s00586-008-0831-6. |
[21] | Simoneau M, Mercier P, Blouin J, Allard P, Teasdale N. Altered sensory-weighting mechanisms is observed in adolescents with idiopathic scoliosis. BMC Neuroscience. (2006) ; 7: : 1-9. |
[22] | Simoneau M, Richer N, Mercier P, Allard P, Teasdale N. Sensory deprivation and balance control in idiopathic scoliosis adolescent. Exp Brain Res. (2006) ; 170: : 576-582. doi: 10.1007/s00221-005-0246-0. |
[23] | Nault M-L, Allard P, Hinse S, Le Blanc R, Caron O, Labelle, H, Sadeghi H. Relations between standing stability and body posture parameters in adolescent idiopathic scoliosis. Spine. (2002) ; 27: : 1911-1917. |
[24] | Herdea A, Stancu TA, Ulici A, Lungu CN, Dragomirescu MC, Charkaoui A. Quality of life evaluation using SRS-30 score for operated children and adolescent idiopathic scoliosis. Medicina. (2022) ; 58: : 674. doi: 10.3390/medicina58050674. |
[25] | Blum CL. Chiropractic and pilates therapy for the treatment of adult scoliosis. J Manipulative Physiol Ther. (2002) ; 25: : E3. doi: 10.1067/mmt.2002.123336. |
[26] | Lewis C. A review of non-invasive treatment interventions for spinal deformities. Physical Therapy Perspectives in the 21st; Century – Challenges and Possibilities. (2012) ; 3: : 67-88. |
[27] | Romano M, Minozzi S, Zaina F, Saltikov JB, Chockalingam N, Kotwicki T, Hennes AM, Negrini, S. Exercises for adolescent idiopathic scoliosis: a Cochrane systematic review. Spine (Phila Pa 1976). (2013) ; 38: : E883-893. doi: 10.1097/BRS.0b013e31829459f8. |
[28] | Day JM, Fletcher J, Coghlan M, Ravine T. Review of scoliosis-specific exercise methods used to correct adolescent idiopathic scoliosis. Archives of Physiotherapy. (2019) ; 9: : 1-11. |
[29] | Szczygiel E, Gigon A, Chudyba IC, Joanna G, Edward G. Evaluation attempt of own body sensing amongst persons with and without scoliosis. J Back Musculoskelet Rehabil. (2021) ; 34: : 425-430. doi: 10.3233/BMR-191761. |
[30] | Dufvenberg M, Adeyemi F, Rajendran I, Öberg B, Abbott A. Does postural stability differ between adolescents with idiopathic scoliosis and typically developed? A systematic literature review and meta-analysis. Scoliosis and Spinal Disorders. (2018) ; 13: : 1-18. |
[31] | Abdel-Aziem AA, Abdelraouf OR, Ghally SA, Dahlawi HA, Radwan RE. A 10-Week Program of Combined Hippotherapy and Scroth’s Exercises Improves Balance and Postural Asymmetries in Adolescence Idiopathic Scoliosis: A Randomized Controlled Study. Children (Basel). (2021) ; 9. doi: 10.3390/children9010023. |
[32] | Bidari S, Kamyab M, Ahmadi A, Ganjavian MS. Effect of exercise on static balance and Cobb angle during the weaning phase of brace management in idiopathic scoliosis and hyperkyphosis: A preliminary study. J Back Musculoskelet Rehabil. (2019) ; 32: : 639-646. doi: 10.3233/BMR-181128. |
[33] | Cashin AG, McAuley JH. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J Physiother. (2020) ; 66: : 59. doi: 10.1016/j.jphys.2019.08.005. |
[34] | Levi D, Springer S, Parmet Y, Ovadia D, Ben-Sira D. Acute muscle stretching and the ability to maintain posture in females with adolescent idiopathic scoliosis. J Back Musculoskelet Rehabil. (2019) ; 32: : 655-662. doi: 10.3233/BMR-181175. |
[35] | Marin L, Kawczynski A, Carnevale Pellino V, Febbi M, Silvestri D, Pedrotti L, Lovecchio N, Vandoni M. Displacement of Centre of Pressure during Rehabilitation Exercise in Adolescent Idiopathic Scoliosis Patients. J Clin Med. (2021) ; 10. doi: 10.3390/jcm10132837. |
[36] | Richards BS, Bernstein RM, D’Amato CR, Thompson GH. Standardization of criteria for adolescent idiopathic scoliosis brace studies: SRS Committee on Bracing and Nonoperative Management. Spine (Phila Pa 1976). (2005) ; 30: : 2068-2075; discussion 2076-2067, doi: 10.1097/01.brs.0000178819.90239.d0. |
[37] | Selthafner M, Liu X, Ellis F, Tassone C, Thometz J, Escott B. Effect of PSSE on postural sway in AIS using center of pressure. Studies in Health Technology and Informatics. (2021) ; 280: : 121-125. |
[38] | Lee B-K. Influence of the proprioceptive neuromuscular facilitation exercise programs on idiopathic scoliosis patient in the early 20s in terms of curves and balancing abilities: single case study. Journal of Exercise Rehabilitation. (2016) ; 12: : 567. |
[39] | Lee S, Shim J. The effects of backpack loads and spinal stabilization exercises on the dynamic foot pressure of elementary school children with idiopathic scoliosis. J Phys Ther Sci. (2015) ; 27: : 2257-2260. doi: 10.1589/jpts.27.2257. |
[40] | Yagci G, Yakut Y, Simsek E. The effects of exercise on perception of verticality in adolescent idiopathic scoliosis. Physiother Theory Pract. (2018) ; 34: : 579-588. doi: 10.1080/09593985.2017.1423429. |
[41] | Benda W, McGibbon NH, Grant KL. Improvements in muscle symmetry in children with cerebral palsy after equine-assisted therapy (hippotherapy). J Altern Complement Med. (2003) ; 9: : 817-825. doi: 10.1089/107555303771952163. |
[42] | Goldmann T, Vilimek M. Kinematics of human spine during hippotherapy. Comput Methods Biomech Biomed Engin. (2012) ; 15: (Suppl 1), 203-205. doi: 10.1080/10255842.2012.713619. |
[43] | Funakoshi R, Masuda K, Uchiyama H, Ohta M. A possible mechanism of horseback riding on dynamic trunk alignment. Heliyon. (2018) ; 4: : e00777. doi: 10.1016/j.heliyon.2018.e00777. |
[44] | Biery MJ, Kauffman N. The effects of therapeutic horseback riding on balance. Adapted Physical Activity Quarterly. (1989) ; 6: : 221-229. |
[45] | Park JH, Jeon HS, Park HW. Effects of the Schroth exercise on idiopathic scoliosis: a meta-analysis. Eur J Phys Rehabil Med. (2018) ; 54: : 440-449. doi: 10.23736/S1973-9087.17.04461-6. |
[46] | Liang J, Zhou X, Chen N, Li X, Yu H, Yang Y, Song Y, Du Q. Efficacy of three-dimensionally integrated exercise for scoliosis in patients with adolescent idiopathic scoliosis: study protocol for a randomized controlled trial. Trials. (2018) ; 19: : 485. doi: 10.1186/s13063-018-2834-x. |
[47] | Otman S, Kose N, Yakut Y. The efficacy of Schroth’s 3-dimensional exercise therapy in the treatment of adolescent idiopathic scoliosis in Turkey. Neurosciences Journal. (2005) ; 10: : 277-283. |
[48] | Nelson AG, Kokkonen J, Arnall DA. Acute muscle stretching inhibits muscle strength endurance performance. J Strength Cond Res. (2005) ; 19: : 338-343. doi: 10.1519/R-15894.1. |
[49] | Kubo K, Kanehisa H, Kawakami Y, Fukunaga T. Influence of static stretching on viscoelastic properties of human tendon structures in vivo. J Appl Physiol 1985. (2001) ; 90: : 520-527. doi: 10.1152/jappl.2001.90.2.520. |
[50] | Wilczyński J. Relationship between muscle tone of the erector spinae and the concave and convex sides of spinal curvature in low-grade scoliosis among children. Children. (2021) ; 8: : 1168. doi: 10.3390/children8121168. |
[51] | Gur G, Ayhan C, Yakut Y. The effectiveness of core stabilization exercise in adolescent idiopathic scoliosis: A randomized controlled trial. Prosthet Orthot Int. (2017) ; 41: : 303-310. doi: 10.1177/0309364616664151. |
[52] | Schreiber S, Parent EC, Khodayari Moez E, Hedden DM, Hill DL, Moreau M, Lou E, Watkins EM, Southon SC. Schroth Physiotherapeutic Scoliosis-Specific Exercises Added to the Standard of Care Lead to Better Cobb Angle Outcomes in Adolescents with Idiopathic Scoliosis – an Assessor and Statistician Blinded Randomized Controlled Trial. PLoS One. (2016) ; 11: : e0168746. doi: 10.1371/journal.pone.0168746. |
[53] | Webber SC, Kriellaars DJ. The effect of stabilization instruction on lumbar acceleration. Clin Biomech (Bristol, Avon). (2004) ; 19: : 777-783. doi: 10.1016/j.clinbiomech.2004.05.014. |
[54] | Zarzycka M, Rozek K, Zarzycki M. Alternative methods of conservative treatment of idiopathic scoliosis. Ortop Traumatol Rehabil. (2009) ; 11: : 396-412. |
[55] | Lee JH, Cynn HS, Yoon TL et al. The effect of scapular posterior tilt exercise, pectoralis minor stretching, and shoulder brace on scapular alignment and muscles activity in subjects with round-shoulder posture. Journal of Electromyography and Kinesiology. (2015) ; 25: : 107-114. |
[56] | Nurse MA, Nigg BM. The effect of changes in foot sensation on plantar pressure and muscle activity. Clin Biomech (Bristol, Avon). (2001) ; 16: : 719-727. doi: 10.1016/s0268-0033(01)00090-0. |
[57] | Giacomozzi C. Appropriateness of plantar pressure measurement devices: a comparative technical assessment. Gait Posture. (2010) ; 32: : 141-144. doi: 10.1016/j.gaitpost.2010.03.014. |
[58] | De Blasiis P, Fullin A, Sansone M, Perna A, Caravelli S, Mosca M, De Luca A, Lucariello A. Kinematic evaluation of the sagittal posture during walking in healthy subjects by 3D motion analysis using DB-Total protocol. J Funct Morphol Kinesiol. (2022) ; 7: : 57. doi: 10.3390/jfmk7030057. |
[59] | Mosca M, Caravelli S, Massimi S, Fuiano M, Catanese G, Barone G, Bragonzoni L, Benedetti MG. Evaluation of proprioception and postural control at a minimum 1 year follow-up after ankle capsuloligamentous lateralplasty with Brostrom technique: A cohort study. Medicine. (2020) ; 99: : e19862. doi: 10.1097/MD.0000000000019862. |
[60] | Park JY, Park GD, Lee SG, Lee JC. The effect of scoliosis angle on center of gravity sway. J Phys Ther Sci. (2013) ; 25: : 1629-1631. doi: 10.1589/jpts.25.1629. |
[61] | Gyllensten AL, Hansson L, Ekdahl C. Outcome of basic body awareness therapy. A randomized controlled study of patients in psychiatric outpatient care. Advances in Physiotherapy. (2003) ; 5: : 179-190. |
[62] | Akuthota V, Nadler SF. Core strengthening. Arch Phys Med Rehabil. (2004) ; 85: : S86-92. doi: 10.1053/j.apmr.2003.12.005. |
[63] | Michaelson P, Michaelson M, Jaric S, Latash ML, Sjölander P, Djupsjöbacka M. Vertical posture and head stability in patients with chronic neck pain. J Rehabil Med. (2003) ; 35: : 229-235. doi: 10.1080/16501970306093. |
[64] | Payne WK, III., Ogilvie JW, Resnick MD, Kane RL, Transfeldt EE, Blum RW. Does scoliosis have a psychological impact and does gender make a difference? Spine. (1997) ; 22: : 1380-1384. doi: 10.1097/00007632-199706150-00017. |
[65] | Notarnicola A, Fari G, Maccagnano G, Riondino A, Covelli I, Bianchi FP, Tafuri S, Piazzolla A, Moretti B. Teenagers’ perceptions of their scoliotic curves. An observational study of comparison between sports people and non-sports people. Muscles Ligaments Tendons J. (2019) ; 9: : 225-235. doi: 10.32098/mltj02,2019,11. |
[66] | Marin L, Lovecchio N, Pedrotti L, Manzoni F, Febbi M, Albanese I, Patane P, Pellino VC, Vandoni M. Acute effects of self-correction on spine deviation and balance in adolescent girls with idiopathic scoliosis. Sensors. (2022) ; 22: : 1883. doi: 10.3390/s22051883. |


