
Clinically significant effects of gait modification on knee pain: A systematic review and meta-analysis
Abstract
BACKGROUND:
Knee pain is the main symptom of knee osteoarthritis. Walking is effective against knee pain, and some studies have shown that gait modification can also relieve this condition. However, the quality of evidence for the clinically significant effects of gait modification on knee pain has not been examined.
OBJECTIVE:
This systematic review and meta-analysis aimed to evaluate the level of evidence for the clinically significant effects of gait modification on knee pain and determine if the effects are greater than the minimal clinically important difference (MCID).
METHODS:
We comprehensively searched electronic databases such as MEDLINE, Cochrane Central Register of Controlled Trials, Physiotherapy Evidence Database, and Cumulative Index to Nursing and Allied Health Literature. Intervention studies with experimental groups who received gait modification and control groups who did not were evaluated. The Grading of Recommendations Assessment, Development and Evaluation system was used to assess the level of evidence.
RESULTS:
Nine studies met the inclusion criteria. All were included in the systematic review and two in the meta-analysis. Results showed that gait modification have significant effects (
CONCLUSIONS:
We concluded that there is a lack of high-quality evidence that supports the general efficacy of gait modification. Although based on low-quality evidence, when applied to the foot, it may have clinically significant effects.
1.Introduction
Knee osteoarthritis (OA) affects about one in five adults aged over 45 years [1], and it is a leading cause of chronic physical disability. Moreover, this condition is characterized by pain and commonly affects the medial aspect of the knee [2, 3]. In knee OA, excessive mechanical stress in the joint is a major contributor to knee pain [4]. Worsening knee pain can lead to higher medical costs and a lower quality of life [5]. To prevent these issues, early treatment for knee pain relief must be provided.
Land-based exercise is one of the most effective therapies for knee pain relief [6, 7, 8] and walking is one of land-based exercises. As excessive loading on the medial aspect of the knee contributes to knee OA progression [9, 10, 11], performing walking exercises in a manner that reduces the medial knee loading is reasonable. Different types of gait modifications for reducing medial load have been proposed. Mechanical stress on the knee changes with the type of gait [12]. Multiple gait modification methods and their effects on mechanical stress on the knee and knee pain have been investigated [12, 13, 14]. Results showed that gait modification can alleviate knee pain.
Although several types of gait modifications are effective, the level of evidence for their efficacy is unknown. Moreover, even if knee pain relief after gait modification is statistically significant, whether its effect is clinically significant is unknown. Hence, this notion should be investigated to improve the evidence-based practice of walking instructors who use methods for alleviating knee pain.
Therefore, the current study aimed to assess the level of evidence for the efficacy of gait modification against knee pain. Moreover, whether its effect is clinically significant was investigated using the minimum clinical important difference (MCID), which is a criterion to evaluate the significance of an effect from a patient perspective rather than from a statistical perspective. To the best of our knowledge, this is the only study that evaluated the clinical significance of gait modification based on a high level of evidence and the perspective of patients.
2.Materials and methods
A systematic literature review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocol guidelines [15] and registered with UMIN. Because this was a systematic review, approval by the ethics committee was not required.
2.1Data sources and search strategy for identification of studies
Electronic databases such as MEDLINE, Cochrane Central Register of Controlled Trials (CENTRAL), Physiotherapy Evidence Database (PEDro), and Cumulative Index to Nursing and Allied Health Literature (CINAHL) were comprehensively searched on September 19, 2022. Search terms including “patient,” “intervention,” and “outcome” were combined with the “AND” operator. Patient was defined as individuals with knee OA. The intervention was gait modification, and the study outcome was pain. Medical Subject Headings terms and synonyms were combined using the “OR” operator for each concept. There were no limits on the dates.
2.2Eligibility criteria
The inclusion criteria were as follows: (1) studies with patients with knee OA, (2) those that used gait modification, (3) those that assessed knee pain, (4) interventional research, and (5) those written in English.
The exclusion criteria were as follows: (1) studies of patients with rheumatoid arthritis; (2) those that included patients who had a surgical history; (3) those with interventions including drug, exercise, manual, cognitive behavioral, and insole therapy, Kinesio
2.3Article screening and selection
The articles identified via the database search were summarized in spreadsheets created using Microsoft Excel 2019. After the exclusion of duplicates, two reviewers (HT and KH) independently screened each article based on the titles and abstracts using the predetermined eligibility criteria for determining relevant manuscripts that could undergo full-text review. Subsequently, the full-text copies of articles that were not excluded based on the titles or abstracts were retrieved, and the inclusion and exclusion criteria were reapplied to these studies to identify their suitability for the final inclusion. Any disagreements in article screening and selection process were resolved via a discussion, and a consensus decision was made by a third party (RT).
2.4Data collection process
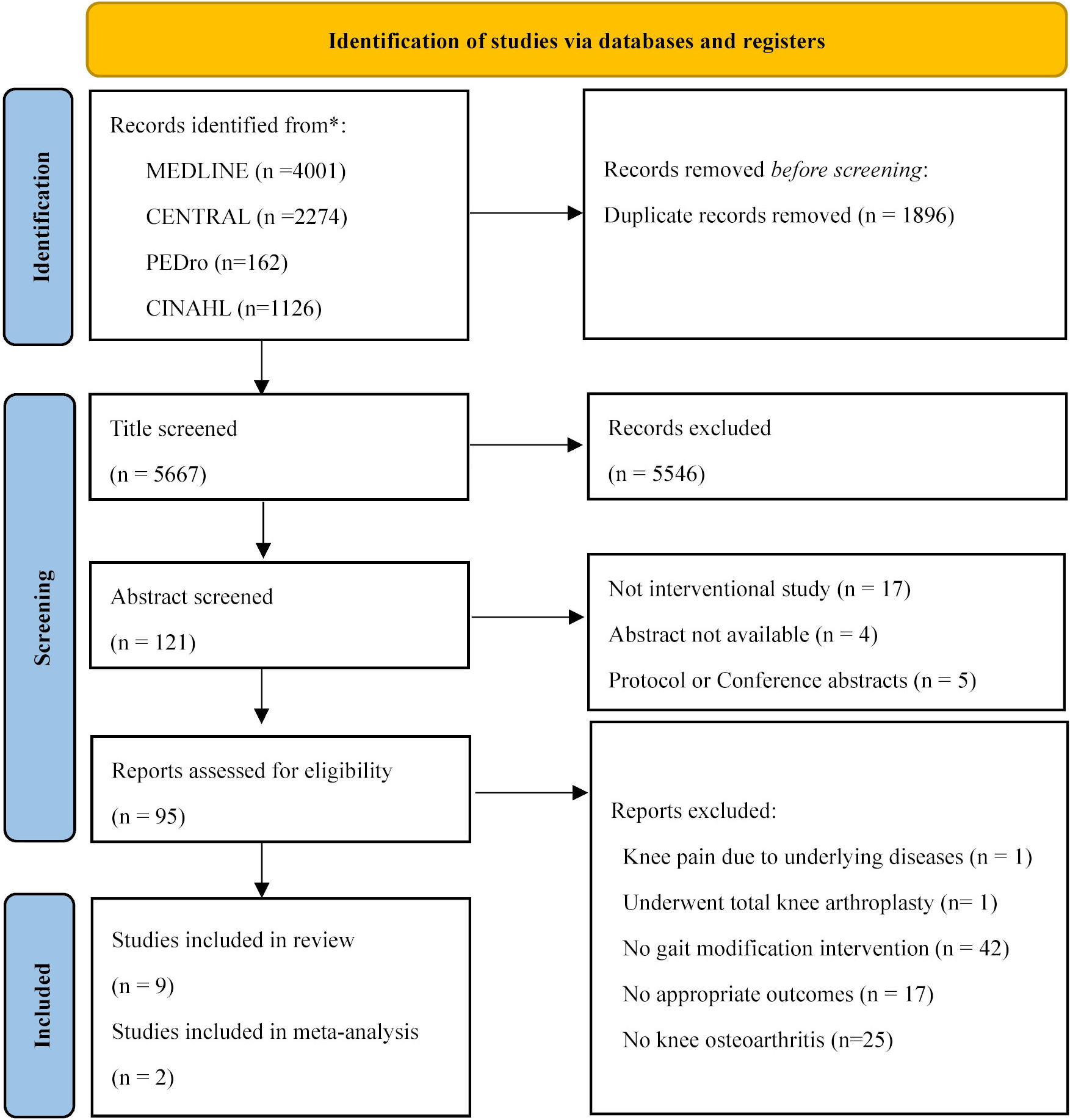
Figure 1.
Flow diagram of the study selection process. CENTRAL; Cochrane Central Register of Controlled Trials, PEDro; Physiotherapy Evidence Database, CINAHL; Cumulative Index to Nursing and Allied Health Literature.
To extract data about, simple predesigned spreadsheets created using Microsoft Excel 2019 were prepared and used to extract data on participants, interventions, outcome measurements, and results. Two authors (HT and KH) discussed and decided whether gait modification was used and whether the outcome was pain.
2.5Data items
We chose the following outcome measures to perform our meta-analysis: (1) Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), which is used to assesses pain, stiffness, and function in patients with hip or knee OA; (2) Knee Injury and Osteoarthritis Outcome Score (KOOS), which is utilized to evaluate pain and other symptoms, function in daily living and in sport and recreation, and knee-related quality of life; (3) Numerical Rating Scale (NRS), which is used to evaluate the subjective intensity of pain; and (4) Visual Analog Scale (VAS), which is utilized to investigate pain intensity.
2.6Assessment of the methodological quality in individual studies
For the assessment of the methodological quality in individual studies, two researchers (TM and HT) independently applied the PEDro scale [16]. Any differences in items were resolved with the help of a third party (RT). Studies with a PEDro score of
2.7Statistical analysis
If the unit of measurements for continuous outcomes was consistent across trials, the results were presented as weighted mean difference (MD) with 95% confidence intervals (95% CIs). However, if the same units were not used in the outcomes across studies, the standardized mean difference (SMD), rather than the MD, was utilized.
All statistical comparisons were performed using Review Manager version 5.4. Only RCTs were included in our meta-analysis. Data from trials with experimental group who received gait modification and control groups who did not were synthesized. If there was more than two value, the value measured at the earliest time point in the study or at a similar time point across RCTs was used in the meta-analysis. This meta-analysis used the mean and standard deviation of the difference between pre- and post-interventions. In addition, the code of the values was unified to express pain relief as a negative value in the meta-analysis. We did not include studies that did not specify pain values before and after the intervention in the meta-analysis.
2.8Certainty assessment
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) system was used for assessing the quality of evidence for each evaluation parameter [17]. GRADE was used if at least two applicable outcomes had been used. The quality of evidence was assessed as very low, low, moderate, or high based on the criteria. Factors downgrading the quality (risk of bias, inconsistency, indirectness, impression, and publication bias) or upgrading the quality (large effect, plausible confounding, and dose-response) were evaluated [18].
3.Results
3.1Study selection
In total, 7563 trials were identified via the combined database search (Fig. 1). After adjusting for duplicates, 5667 trials were included in the analyses, of which 5546 did not meet the selection criteria for reviewing the article titles and abstracts. A detailed examination of the complete texts of the remaining 95 studies was performed. 86 studies did not meet the inclusion criteria, and finally, nine studies met the inclusion criteria. All were included in the systematic review [19, 20, 21, 22, 23, 24, 25, 26, 27] and two [19, 23] were included in the meta-analysis.
3.2Study characteristics
Table 1
Patient characteristics
| Authors | Design | Populations | Size | Age (SD) | Female (%) | Height (SD) | Body mass (SD) | BMI (SD) | K/L 1 (%) | K/L 2 (%) | K/L 3 (%) | K/L 4 (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hunt et al. [19] | RCT | Radiographic | EG: 40 | EG: 64.6 (7.6) | EG: 27 (67.5) | EG: 1.64 (0.10) | EG: 73.6 (13.2) | EG: 27.3 (3.5) | EG: 19 (48) | EG: 17 (42) | EG: 4 (10) | |
| KOA | CG: 39 | CG: 65.4 (9.6) | CG: 28 (71.8) | CG: 1.66 (0.09) | CG: 75.6 (13.2) | CG: 27.4 (3.5) | CG: 18 (46) | CG: 14 (36) | CG: 7 (18) | |||
| Hunt et al. [20] | Non-RCT | Radiographic | 16 | 64.8 (5.2) | 9 (56.2) | Not recorded | Not recorded | 29.9 (3.4) | 4 (25) | 9 (56) | 3 (19) | |
| KOA | ||||||||||||
| Richards et al. [21] | Non-RCT | Radiographic | 21 | 61.3 (5.73) | 15 (71.4) | 1.72 (0.08) | 75.9 (11.0) | 25.4 (2.6) | 12 (63) | 2 (10.5) | 4 (21.1) | 1 (5.2) |
| KOA | ||||||||||||
| Cheung et al. [22] | RCT | Radiographic | EG: 10 | EG: 60.8 (6.4) | EG: 5 (50) | EG: 1.62 (0.09) | EG: 64.3 (7.1) | EG: 24.5 (2.4) | EG: 2 (10) | EG: 8 (40) | ||
| KOA | CG: 10 | CG: 63.1 (5.9) | CG: 5 (50) | CG: 1.64 (0.10) | CG: 67.4 (6.1) | CG: 25.2 (1.1) | CG: 3 (15) | CG: 7 (35) | ||||
| Segal et al. [23] | RCT | Symptomatic | EG: 29 | EG: 69.1 (3.7) | EG: 22 (75.9) | Not recorded | Not recorded | Not recorded | EG: 5 (18) | EG: 13 (47) | EG: 10 (36) | |
| KOA | CG: 19 | CG: 69.6 (3.2) | CG: 10 (52.6) | CG: 5 (26) | CG: 9 (47) | CG: 5 (26) | ||||||
| Takacs et al. [24] | Non-RCT | Radiographic | 12 | 64.1 (9.1) | 7 (58.3) | Not recorded | Not recorded | 28.3 (4.9) | 5 (42) | 5 (41.6) | 2 (18) | |
| medial KOA | ||||||||||||
| Shull et al. [25] | Non-RCT | Radiographic | 10 | 60 (13) | 4 (40) | 171 (9) | 79 (20) | 26.6 (4.7) | 3 (30) | 6 (60) | 1 (10) | |
| medial KOA | ||||||||||||
| Simic et al. [26] | Non-RCT | Radiographic | 22 | 68.4 (5.1) | 13 (59) | 1.67 (0.05) | 78.3 (8.1) | 27.9 (2.4) | 9 (41) | 9 (41) | 4 (18) | |
| medial KOA | ||||||||||||
| Wang et al. [27] | RCT | Radiographic | EG: 31 | EG: 59.1 (7.2) | EG: 16 (51.6) | EG: 1.65 (0.09) | EG: 62.0 (11.0) | EG: 1.65 (0.09) | EG: 15 (48) | EG: 16 (51) | ||
| medial KOA | CG: 31 | CG: 61.7 (6.8) | CG: 17 (54.8) | CG: 1.65 (0.08) | CG: 64.2 (10.6) | CG: 1.65 (0.08) | CG: 16 (51) | CG: 15 (48) |
Table 2
The content of gait modification
| Authors | Type of gait modification | Biofeedback | Number of training sessions | Training period |
|---|---|---|---|---|
| Hunt et al. [19] | Toe-out gait | Mirror-guided biofeedback | 8 (1, 2, 4, 6, 8, 10, 12, 15 weeks) | 4 months |
| Hunt et al. [20] | Toe-out gait | Real-time biofeedback of performance | 6 (1, 2, 3, 5, 7, 9 weeks) | 10 weeks |
| Richards et al. [21] | Toe-in gait | Visual feedback | 6 (1, 2, 3, 4, 5, 6 weeks) | 6 weeks |
| Cheung et al. [22] | Toe-out gait | Visual feedback | 6 (1, 2, 3, 4, 5, 6 weeks) | 6 weeks |
| Segal et al. [23] | Gait aimed to move toward symmetrical and typical displacements of the trunk and pelvis about neutral frontal and transverse axes | Visual 3D | 24 (biweeks) | 12 months |
| Takacs et al. [24] | Trunk lean gait | Visual feedback | 1 | Immediate |
| Shull et al. [25] | Toe-in gait | Visual feedback | 6 (1, 2, 3, 4, 5, 6 weeks) | 6 weeks |
| Simic et al. [26] | Trunk lean gait | Real-time movement biofeedback system | 1 | Immediate |
| Wang et al. [27] | Toe-in gait | Visual feedback | 6 (1, 2, 3, 4, 5, 6 weeks) | 6 weeks |
Table 2 shows the population characteristics of the studies included in this review. Four RCTs [19, 22, 23, 27] and five non-RCTs [20, 21, 24, 25, 26] were analyzed. The sample sizes ranged from 10 to 79, and the participants were classified under the experimental and control groups. The average age of the participants in the nine studies ranged from 59.1 to 69.6 years.
Table 2 shows the content of gait modification performed in the studies. The gait modification methods were toe-out gait [19, 20, 22], toe-in gait [21, 25, 27], trunk lean gait [24, 26], and move toward symmetrical and typical displacements of the trunk and pelvis about neutral frontal and transverse axes [23]. Chueng et al. [22], Shull et al. [25], and Wang et al. [27] did not indicate a specific gait modification method, but all subjects walked with toe-out gait or toe-in gait. All gait modification methods were visual feedback using mirrors and biofeedback.
Table 3
Outcome data
| Authors | Outcome scale | Evaluate point | Baseline (SD), [IQR] | Post-intervention (SD), [IQR] | Mean difference (SD) | |||
|---|---|---|---|---|---|---|---|---|
| EG | CG | EG | CG | EG | CG | |||
| Hunt et al. [19] | WOMAC P, WOMAC F, NRS | 4, 5 months | WOMAC P: 7.6 (0.5) WOMAC F: 28.1 (1.9) NRS: 4.7 (0.4) | WOMAC P: 6.4 (0.4) WOMAC F: 21.4 (1.5) NRS: 3.7 (0.3) | WOMAC P: 4.2 (0.5) WOMAC F: 13.0 (1.6) NRS: 2.0 (0.3) 4 months | WOMAC P: 5.4 (0.5) WOMAC F: 16.7 (1.6) NRS: 2.3 (0.3) 4 months | WOMAC P: | WOMAC P: |
| Hunt et al. [20] | WOMAC P, WOMAC T, NRS | 11 weeks | WOMAC P: 7.4 (3.4) WOMAC T: 36.9 (14.8) NRS: 4.5 (1.7) | Not application | WOMAC P: 5.3 (2.9) WOMAC T: 26.4 (13.5) NRS: 2.6 (1.8) | Not application | WOMAC P: | Not application |
| Richards et al. [21] | WOMAC P, WOMAC F, NRS | 6 weeks, 3, 6 months | WOMAC P: 10.5 [9] WOMAC F: 14.5 [16] NRS: 1.5 [2] | Not application | WOMAC P: 7 [6] WOMAC F: 6.5 [10] NRS: 1 [2] 6 weeks | Not application | Not recorded | Not application |
| Cheung et al. [22] | WOMAC P, WOMAC F | 6 weeks 6 months | WOMAC P: 30.0 (12.5) (%) WOMAC F: 29.3 (7.2) (%) | WOMAC P: 22.5 (12.3) (%) WOMAC F: 24.7 (7.2) (%) | Not recorded | Not recorded | Not recorded | Not recorded |
| Segal et al. [23] | KOOS | 3, 6, 12 months | 62.7 (10.8) | 59.8 (13.1) | Not recorded | Not recorded | 8.2 (14.0) | 1.1 (13.7) |
| Takacs et al. [24] | NRS | Immediate | 1.8 (1.8) | Not application | 2.2 (2.1) | Not application | 0.3 (0.9) | Not application |
| Shull et al. [25] | WOMAC P, WOMAC F, VAS | 6, 10 weeks | Not recorded | Not application | Not recorded | Not application | Not recorded | Not application |
| Simic et al. [26] | WOMAC P, WOMAC F, NRS | Immediate | WOMAC P: 5 (3) WOMAC F: 19 (11) NRS: 2.2(2.0) | Not application | NRS: 2.3 (2.9) | Not application | Not recorded | Not application |
| Wang et al. [27] | KOOS, VAS | 6 weeks | KOOS: 73.1 (7.9) VAS: 4.3 (2.2) | KOOS: 72.5 (12.1) VAS: 4.5 (2.0) | Not recorded | Not recorded | KOOS: 6.4 (8.8) | KOOS: Not recorded VAS: Not recorded |
VAS: Visual Analog Scale, WOMAC P: Western Ontario and McMaster Universities Osteoarthritis pain, WOMAC F: Western Ontario and McMaster Universities Osteoarthritis function, WOMAC T: Western Ontario and McMaster Universities Osteoarthritis total, IQR: Interquartile range, KOOS: Knee injury and Osteoarthritis Outcome Score, NRS: Numerical Rating Scale, EG: experimental group, CG: control group.
Table 4
GRADE summary of findings
| Certainty assessment | No. of patients | Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Outcome | No. of studies | Study design | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | EG | CG | ||
| Pain | 2 | RCT | Very serious | Not serious | Not serious | Serious | None | 65 | 22 |
| Important |
| Very low | |||||||||||
GRADE; Grading of Recommendations Assessment, Development and Evaluation, RCT; randomized controlled trial, EG; experimental group, CG; control group. Explanations:
Figure 2.
Forest plot of the standardized mean differences (SMD) between gait modification and non-gait modification.

Table 3 shows the outcome data of the studies. Six studies used the WOMAC [19, 20, 21, 22, 25, 26]; two, the KOOS [23, 27]; two, the VAS [25, 27]; and five, the NRS [19, 20, 21, 24, 26]. Hunt et al. [19] revealed that the mean deference in the WOMAC pain subscale score between baseline and post-intervention was 2.7 in the experimental group. Cheung et al. [22] found that the rate of change in knee pain in the experimental group was 49% based on the WOMAC. Wang et al. [27] showed that the percentage of change in the VAS score was 35.5%. Three non-RCTs used toe-in or toe-out gait. In the research of Hunt et al. [20], the WOMAC score changed by 2.1 and the NRS score by 1.9. Meanwhile, Richards et al. [21] revealed that the WOMAC score changed from 10.5 at baseline to 7 at post-intervention. The percentage of change in the WOMAC score was 29% and the decrease in VAS was 2 points on the study of Shull et al. [25].
3.3Results of individual studies and syntheses
Figure 2 shows the forest plots of the meta-analysis. Two studies [19, 23] integrated their data. In total, 122 participants were included in these studies. One RCT [22] was not included in the meta-analysis due to lack of required data. Results showed that the SMD was
3.4Certainty of evidence
Table 4 shows the GRADE summary of findings. The quality of evidence was very low, with a risk of bias and impression as factors that reduced quality.
4.Discussion
Nine interventional studies were included in the systematic review and two RCTs in the meta-analysis. Moreover, the GRADE system was used to determine the level of evidence. Results showed that the quality of evidence for the efficacy of gait modification against knee pain was very low. However, several studies have revealed that gait modification effects were greater than the MCID. That is, some types of gait modifications can alleviate knee pain, thereby providing patient satisfaction.
The level of evidence supporting the effect of gait modification on knee pain is a novel finding. The conventional practical guidelines for knee OA recommends land-based exercises [6, 7]. However, to the best of our knowledge, there are no guidelines on the characteristics of walking (e.g., foot direction and stride length). Our review, which evaluated the level of evidence for gait modification methods, can contribute in updating guidelines that recommend walking.
Our study was conducted specifically on individuals with knee OA. In a previous systematic review, the target population comprised healthy individuals and those with knee OA, and it focused mainly on knee adduction moment [12, 13, 14]. In contrast, our study performed a systematic review and meta-analysis focusing on pain in people with knee OA alone. Our findings are valuable for clinicians who want to provide satisfactory care to people with knee OA.
Gait modification, which can significantly alleviate knee pain, focuses on the feet. The results of the GRADE system did not provide a high level of evidence for the efficacy of gait modification against knee pain. This indicates that the effect size is likely to change in future studies. However, changing foot orientation is a common denominator among gait modifications with statistical significance in RCTs [19, 22] with a low risk of bias (PEDro score of
Although the effect size cannot be guaranteed, foot-focused interventions can have effects that are beyond patient satisfaction. According to Pham et al. [28], the MCID of the WOMAC improved by pain
Pain relief through gait modification that focuses on the foot can be effective for physical function. According to Newberry et al. [31], the MCID of the WOMAC function is 9.1 on a scale of 0 to 100 [32]. Of the studies included in our review, there were five studies [19, 21, 22, 25, 26] that used the scale of the WOMAC function. Four of them [19, 21, 22, 25] had a gait modification focused on the foot, all of which significantly improved the scores and three of them [19, 22, 25] exceeded the MCID. One study [21] did not report the amount of change, so it could not be determined if the change exceeded the MCID. Simic et al. [26], who focused on trunk lean, did not report the amount of change, so it could not be determined whether the effect exceeded the MCID. Thus, gait modification focused on the foot may be clinically effective not only in reducing pain but also in improving physical function.
This study showed the characteristics of individuals with knee OA who can benefit from the procedure beyond the MCID. Five studies, which showed that the effect of toe-in or toe-out gait was beyond the MCID, included overweight women aged over 60 years. Based on the OARSI guideline [6, 7], a common core intervention is recommended for all patients. Additionally, patients are sub-grouped, and different interventions are recommended for each subgroup. The two criteria for subgrouping are OA other than in the knee and presence of complications. Nevertheless, age, sex, and body composition are not considered. To make walking more effective than gait modification, a subgroup of older and overweight women should be targeted.
The current study had several limitations. First, there were only four RCTs in the systemic review, and only two RCTs specified the extent of change between the experimental and control groups. Therefore, no reliable conclusions about the effect size could be drawn. Nevertheless, more high-quality studies should be performed to provide stronger evidence about the effect size of gait modification. Second, only few studies used similar gait modification methods. The data of multiple RCTs could not be integrated using similar gait modification methods, and a reliable effect size was not achieved. Since effect sizes between methods could not be compared, we cannot confirm which gait modification method is the most effective. Because the effect size of gait modification focused on the toe-in and/or toe-out exceeded the MCID, more RCTs confirming this effect size are warranted. Despite these limitations, to the best of our knowledge, there are currently no systematic reviews that determined the level of evidence for the efficacy of gait modification. Our review can help clinicians in the decision-making process regarding the use of gait modification and can facilitate designing future studies.
5.Conclusion
The level of evidence for the efficacy of gait modification against knee pain in people with knee OA is very low. However, toe-in or toe-out gait is effective in relieving knee pain in RCTs, and several studies revealed that it is more effective than MCID. These reports included overweight women aged over 60 years old.
Ethical approval
This study has been registered with UMIN (registration number: 000045647).
Informed consent
Not applicable.
Funding
This work was supported by the Grants-in-Aid for Scientific Research of Japan Society for the Promotion of Science (Grant Number JP20K11230).
Author contributions
Protocol stage: All authors drafted the protocol.
Review stage: KH and HT selected which reviews to include.
Review stage: HT, KH and KH extracted data from reviews.
Review stage: HT entered data into RevMan.
Review stage: HT carried out the analysis.
Review stage: All authors interpreted the analysis.
Review stage: All authors drafted the final review.
Update stage: All authors updated the review.
Acknowledgments
None to report.
Conflict of interest
The authors declare that they have no conflict of interest.
References
[1] | Lawrence RC, Felson DT, Helmick CG, Arnold LM, Choi H, Deyo RA, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum. (2008) Jan; 58: (1): 26-35. |
[2] | Thomas RH, Resnick D, Alazraki NP, Daniel D, Greenfield R. Compartmental evaluation of osteoarthritis of the knee. A comparative study of available diagnostic modalities. Radiology. (1975) Sep; 116: (3): 585-94. |
[3] | Jinks C, Jordan K, Ong BN, Croft P. A brief screening tool for knee pain in primary care (KNEST)+ 2+ Results from a survey in the general population aged 50 and over. Rheumatology (Oxford). (2004) Jan; 43: (1): 55-61. |
[4] | Thorp LE, Sumner DR, Wimmer MA, Block JA. Relationship between pain and medial knee joint loading in mild radiographic knee osteoarthritis. Arthritis Rheum. (2007) Oct 15; 57: (7): 1254-60. |
[5] | March LM, Bachmeier CJ. Economics of osteoarthritis: a global perspective. Baillieres Clin Rheumatol. (1997) Nov; 11: (4): 817-34. |
[6] | Bannuru RR, Osani MC, Vaysbrot EE, Arden NK, Bennell K, Bierma-Zeinstra SMA, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. (2019) Nov; 27: (11): 1578-89. |
[7] | McAlindon TE, Bannuru RR, Sullivan MC, Arden NK, Berenbaum F, Bierma-Zeinstra SM, et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis Cartilage. (2014) Mar; 22: (3): 363-88. |
[8] | Fransen M, McConnell S, Harmer AR, Van der Esch M, Simic M, Bennell KL. Exercise for osteoarthritis of the knee: a Cochrane systematic review. Br J Sports Med. (2015) Dec; 49: (24): 1554-7. |
[9] | Andriacchi TP, Mundermann A. The role of ambulatory mechanics in the initiation and progression of knee osteoarthritis. Curr Opin Rheumatol. (2006) Sep; 18: (5): 514-8. |
[10] | Vincent KR, Conrad BP, Fregly BJ, Vincent HK. The pathophysiology of osteoarthritis: a mechanical perspective on the knee joint. PM R. (2012) May; 4: (5 Suppl): S3-9. |
[11] | Block JA, Shakoor N. Lower limb osteoarthritis: biomechanical alterations and implications for therapy. Curr Opin Rheumatol. (2010) Sep; 22: (5): 544-50. |
[12] | Simic M, Hinman RS, Wrigley TV, Bennell KL, Hunt MA. Gait modification strategies for altering medial knee joint load: a systematic review. Arthritis Care Res (Hoboken). (2011) Mar; 63: (3): 405-26. |
[13] | Bowd J, Biggs P, Holt C, Whatling G. Does Gait Retraining Have the Potential to Reduce Medial Compartmental Loading in Individuals With Knee Osteoarthritis While Not Adversely Affecting the Other Lower Limb Joints? A Systematic Review. Arch Rehabil Res Clin Transl. (2019) Dec; 1: (3-4): 100022. |
[14] | Richards R, van den Noort JC, Dekker J, Harlaar J. Gait Retraining With Real-Time Biofeedback to Reduce Knee Adduction Moment: Systematic Review of Effects and Methods Used. Arch Phys Med Rehabil. (2017) Jan; 98: (1): 137-50. |
[15] | Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) Mar 29; 372: : n71. |
[16] | de Morton NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Aust J Physiother. (2009) ; 55: (2): 129-33. |
[17] | Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. (2011) Apr; 64: (4): 383-94. |
[18] | Yamakawa K, Aihara M, Ogura H, Yuhara H, Hamasaki T, Shimazu T. Recombinant human soluble thrombomodulin in severe sepsis: a systematic review and meta-analysis. J Thromb Haemost. (2015) Apr; 13: (4): 508-19. |
[19] | Hunt MA, Charlton JM, Krowchuk NM, Tse CTF, Hatfield GL. Clinical and biomechanical changes following a 4-month toe-out gait modification program for people with medial knee osteoarthritis: a randomized controlled trial. Osteoarthritis Cartilage. (2018) Jul; 26: (7): 903-11. |
[20] | Hunt MA, Takacs J. Effects of a 10-week toe-out gait modification intervention in people with medial knee osteoarthritis: a pilot, feasibility study. Osteoarthritis Cartilage. (2014) Jul; 22: (7): 904-11. |
[21] | Richards R, van den Noort JC, van der Esch M, Booij MJ, Harlaar J. Gait retraining using real-time feedback in patients with medial knee osteoarthritis: Feasibility and effects of a six-week gait training program. Knee. (2018) Oct; 25: (5): 814-24. |
[22] | Cheung RTH, Ho KKW, Au IPH, An WW, Zhang JHW, Chan ZYS, et al. Immediate and short-term effects of gait retraining on the knee joint moments and symptoms in patients with early tibiofemoral joint osteoarthritis: a randomized controlled trial. Osteoarthritis Cartilage. (2018) Nov; 26: (11): 1479-86. |
[23] | Segal NA, Glass NA, Teran-Yengle P, Singh B, Wallace RB, Yack HJ. Intensive Gait Training for Older Adults with Symptomatic Knee Osteoarthritis. Am J Phys Med Rehabil. (2015) Oct; 94: (10 Suppl 1): 848-58. |
[24] | Takacs J, Kirkham AA, Perry F, Brown J, Marriott E, Monkman D, et al. Lateral trunk lean gait modification increases the energy cost of treadmill walking in those with knee osteoarthritis. Osteoarthritis Cartilage. (2014) Feb; 22: (2): 203-9. |
[25] | Shull PB, Silder A, Shultz R, Dragoo JL, Besier TF, Delp SL, et al. Six-week gait retraining program reduces knee adduction moment, reduces pain, and improves function for individuals with medial compartment knee osteoarthritis. J Orthop Res. (2013) Jul; 31: (7): 1020-5. |
[26] | Simic M, Hunt MA, Bennell KL, Hinman RS, Wrigley TV. Trunk lean gait modification and knee joint load in people with medial knee osteoarthritis: the effect of varying trunk lean angles. Arthritis Care Res (Hoboken). (2012) Oct; 64: (10): 1545-53. |
[27] | Wang S, Chan PPK, Lam BMF, Chan ZYS, Zhang JHW, Lam WK, et al. Sensor-Based Gait Retraining Lowers Knee Adduction Moment and Improves Symptoms in Patients with Knee Osteoarthritis: A Randomized Controlled Trial. Sensors (Basel). (2021) Aug 19; 21: (16): 5596. |
[28] | Pham T, Van Der Heijde D, Lassere M, Altman RD, Anderson JJ, Bellamy N, et al. Outcome variables for osteoarthritis clinical trials: The OMERACT-OARSI set of responder criteria. J Rheumatol. (2003) Jul; 30: (7): 1648-54. |
[29] | Salaffi F, Stancati A, Silvestri CA, Ciapetti A, Grassi W. Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur J Pain. (2004) Aug; 8: (4): 283-91. |
[30] | Wandel S, Juni P, Tendal B, Nuesch E, Villiger PM, Welton NJ, et al. Effects of glucosamine, chondroitin, or placebo in patients with osteoarthritis of hip or knee: network meta-analysis. BMJ. (2010) Sep 16; 341: : c4675. |
[31] | Newberry SJ, FitzGerald J, SooHoo NF, Booth M, Marks J, Motala A, et al. Treatment of Osteoarthritis of the Knee: An Update Review. Rockville (MD): Agency for Healthcare Research and Quality (US); (2017) May. Report No.: 17-EHC011-EF. |
[32] | Tubach F, Ravaud P, Baron G, Falissard B, I Logeart I, Bellamy N, et al. Evaluation of clinically relevant changes in patient reported outcomes in knee and hip osteoarthritis: the minimal clinically important improvement. Ann Rheum Dis. (2005) May 9; 64: : 29-33. |


