
Harmful or safe? Exposure and pain provocation during physiotherapy of complex regional pain syndrome I: a narrative review
Abstract
BACKGROUND:
Complex regional pain syndrome (CRPS) is a clinical diagnosis and an umbrella term for a heterogeneous group of states associated with pain disproportionate to any inciting event, together with a number of signs and symptoms that are manifested mainly in the limbs. There are often concerns among clinicians and patients about the potential harms caused by pain provocation during physiotherapy of CRPS, even though clinical guidelines de-emphasize pain-contingency.
OBJECTIVE:
The objective of this narrative review is to summarize current evidence regarding potential harms due to pain provocation during so-called exposure-based therapies in individuals with CRPS.
METHODS:
Six studies evaluating exposure-based approach were included (
RESULTS:
Although only one included study focused primarily on safety and in the rest of the included studies the reporting of harms was insufficient and therefore our certainty in evidence is very low, taken together with outcome measures, available data does not point to any long-term deterioration in symptoms or function, or any major harms associated with pain provocation during physiotherapy of CRPS.
CONCLUSION:
There is a great need for higher-quality studies to determine which therapeutic approach is the most appropriate for whom and to evaluate the risks and benefits of different approaches in more detail.
1.Introduction
Table 1
Budapest criteria
| Conditions | Continuing pain which is disproportionate to any inciting event | The patient has at least one sign in two or more of the categories | The patient reports at least one sign in three or more of the categories | No other diagnosis can better explain the signs and symptoms |
|---|---|---|---|---|
| Categories | Sensory: hyperalgesia and/or allodynia | Vasomotor: temperature asymmetry and/or skin colour changes and/or skin colour asymmetry | Sudomotor/oedema: oedema and/or sweating changes and/or sweating asymmetry | Motor/trophic: decreased range of motion and/or motor dysfunction (weakness, tremor, dystonia) and/or trophic changes (hair, nail, skin) |
Complex regional pain syndrome (CRPS) is a pain syndrome that can develop after trauma, surgery, immobilization, minimal injuries and possibly even spontaneously [1, 2, 3]. CRPS has also been associated with soft-tissue injuries to the shoulder after a stroke [4]. A typical feature of CRPS is pain disproportionate to any inciting event and that CRPS primarily affects the limbs. Further, although the pain is often described with characteristics typical of neuropathic pain, peripheral nerve lesions have typically not been proven in type I CRPS [1, 2, 3, 4]. CRPS is a clinical diagnosis with a controversial history that covers a relatively heterogeneous group of clinical manifestations with not fully explained etiopathogenesis [5, 6]. CRPS is now predominately being associated with functional and structural changes in the neurological and immune systems, however, the results of different authors are often contradictory [7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18]. Currently, the Budapest Criteria are used in the diagnosis of CRPS [1], which are described in Table 1. Differential diagnosis is paramount since CRPS is a diagnosis based on exclusion [1, 19]. For this reason, additional assessment methods facilitating diagnosis and treatment incl. diagnostic imaging should be used in selected patients [1, 5, 7]. Regarding prognosis, recent prospective study shows that only 5.5% of individuals with CRPS are asymptomatic 12 months after the onset even with treatment, although the majority showed significant improvements in pain (average decrease of 50%) and disability (average decrease of 60%) [20]. Unfortunately, it seems that in a minority of individuals with CRPS symptoms persist or even worsen and progress over time [21].
There is generally a lack of robust evidence for the use of any physiotherapy management approach and for this reason, existing management strategies are mostly based only on insufficient evidence or expert opinions while the mechanism of action is not fully understood [22, 23, 24, 25]. According to clinical practice guidelines [1, 19, 26, 27], early diagnosis and timely treatment are paramount and patients must have access to rehabilitation treatment as soon as possible. There is also consensus that physiotherapy should be goal-oriented and focus should be placed on restoration or preservation of function as well as on pain management. Earlier guidelines promote pain-contingency [26] while more recent guidelines de-emphasize a pain-contingent approach and point out that therapy should be graded and function-oriented while an optimal balance between “doing too much” or “doing too little” must be sought [1, 19, 27]. There is an ongoing debate whether a reduction in pain facilitates an increase in function or an increase in a function facilitates pain reduction or when one is more important than the other. Because of this, there is a spectrum of opinions regarding the balance between these seemingly contradictory approaches [28]. Unfortunately, there is huge uncertainty involved as there is no evidence to guide us in the exact dosing, intensity, order or a suitable combination of approaches, nor to tell us who will respond better to which regimen. In summary, it can be recommended that “(1) no single-treatment approach should be preferred for management of this client group and (2) therapists should not blindly apply all treatment approaches” [29].
1.1Pain provocation during exposure-based therapies
Exposure-based approaches were developed due to the perceived insufficient effects of the commonly used interventions for some individuals with CRPS. It is hypothesized that too much emphasis on pain control could adversely affect the quality of life, disability and paradoxically also pain through intertwined psychological (e.g. pain-related fears), behavioural (e.g. avoidance) and physiological factors (changes in peripheral tissues as well as functional and structural changes of the neuro-immune system) [30, 31]. The goal of exposure-based approaches is primarily to reduce avoidance behaviours and increase function to which pain is secondary. There is some evidence that the perceived harmfulness of activities mediates disability in chronic CRPS [32] but kinesiophobia, fear-avoidance and pain catastrophizing are not mediators for disability or pain when measured via questionnaire [32, 33]. Thus, reducing the avoidance and perceived harmfulness of activities would seem to be potential treatment goals. These approaches have in common a thorough individualized education and motivation of individuals with CRPS and the creation of appropriate conditions to increase the levels of activity – especially towards pre-defined and individually valuable and meaningful activities. Exposure outside the therapy is also encouraged and independence from the therapist is gradually promoted. Parallels with exposure-based approaches, e.g. graded activity and graded exposure in vivo, in chronic low back pain patients are apparent [34, 35].
Graded Exposure in vivo (GEXP) in the context of CRPS treatment was first described by de Jong et al. [30] and was created especially for individuals with increased fear of movement and re/injury. Education in GEXP focuses on the hypothesized vicious circle of pain
Other approaches additionally include exposure. Graded Motor Imagery (GMI) is basically graded exposure and incorporates some elements of the aforementioned approaches, but is based on a somewhat different rationale and has some important specifics incl. limitation of pain increases during exposure with the goal of “disassociating movement and pain” [38]. Thus, GMI will not be the main focus of this narrative review. In the past so-called “stress-loading” was developed by Watson and Carlson [39]. This consists of exposure to active traction and compression exercises that provide stressful stimuli to the extremity without joint motion. Because their study was aimed at individuals with “reflex sympathetic dystrophy” and the current CRPS diagnostic criteria were not used at that time, stress-loading will not be evaluated further in this review.
2.Objectives
Even though clinical practice guidelines de-emphasize pain contingency [1, 19, 27] and there is some evidence that exposure-based approaches and desensitization are being implemented in clinical practice [40, 41, 42, 43], pain aggravation during physiotherapy of individuals with CRPS is commonly perceived as dangerous by clinicians [43] and patients. This could be problematic because it is hypothesized that increased pain-related fear resulting in excessive focus on pain control and any associated avoidance of activity perpetuates a vicious cycle leading to more disability and pain [33, 37]. Since pain provocation during movement or exercise is standardized in the form of exposure to valued but painful activities in the so-called exposure-based approaches, results of studies regarding exposure-based approaches could be used as a proxy for evaluation, whether or not pain provocation during movement is harmful for individuals living with CRPS. Thus, the main objective of this narrative review is to answer the following PICO question [44]: Are exposure-based approaches associated with any harms in adult individuals diagnosed with CRPS? A related secondary goal was to also evaluate to what extent and quality are harms reported in studies regarding exposure-based therapies.
3.Methods
This narrative review was conducted in accordance with a Scale for the Quality Assessment of Narrative Review Articles (SANRA) [45] and secondarily with the PRISMA harms checklist [46] since its focus is on harms. This study, as a literature review, is exempt from Institutional Review Board approval. The main author identified articles using keyword database searches and then by a manual search through reference lists of identified eligible studies. Eligibility criteria were based on a PICO(S) format suggested by PRISMA statements [44]:
• Population: adult individuals diagnosed with CRPS
• Intervention: exposure-based approach as a primary intervention
• Outcomes: adverse events reports and/or outcome data for disability and/or pain
• Study type: any prospective interventional study design with any length of follow-up
Table 2
Search strategy
| PubMed: (("CRPS"[All Fields] OR ("complex regional pain syndromes"[MeSH Terms] OR ("complex"[All Fields] AND "regional"[All Fields] AND "pain"[All Fields] AND "syndromes"[All Fields]) OR "complex regional pain syndromes"[All Fields] OR ("complex"[All Fields] AND "regional"[All Fields] AND "pain"[All Fields] AND "syndrome"[All Fields]) OR "complex regional pain syndrome"[All Fields])) AND ("exposure"[All Fields] OR "exposure s"[All Fields] OR "exposured"[All Fields] OR "exposures"[All Fields] OR "exposuring"[All Fields])) AND ((casereports[Filter] OR clinicalstudy[Filter] OR clinicaltrial[Filter] OR controlledclinicaltrial[Filter] OR multicenterstudy[Filter] OR observationalstudy[Filter] OR pragmaticclinicaltrial[Filter] OR randomizedcontrolledtrial[Filter]) AND (humans[Filter]) AND (english[Filter])) |
| Cochrane Library: (complex regional pain syndrome): ti, ab, kw AND (exposure): ti, ab, kw |
| PEDro: Abstract & Title field: complex (AND) regional (AND) pain (AND) syndrome (AND) exposure |
| Web of Science: complex regional pain syndrome (Abstract) and exposure (Abstract) |
Further, only studies written in English were eligible and this review searched only for published data. Exposure-based approaches were defined as any approach where a) exposure to painful activities or exercises is explicitly implemented and promoted, b) pain-contingency is de-emphasized and c) where pain provocation or aggravation is not a signal to cease the intervention. For this review, we followed the definition of harms by CONSORT extension [47] defining harms as “the totality of possible adverse consequences of an intervention or therapy”. Specifically, this review was focused on a) any reported adverse events, b) any reported deterioration in functional state and c) any reported long-term increase in pain intensity (
PubMed, Cochrane Library, PEDro and Web of Science databases were searched using the terms ‘complex regional pain syndrome’ and ‘exposure’ from inception to January 2022. The last search was performed in July 2022. The search strategy is described in Table 2. The records located were screened for relevance by title. Duplicates and not relevant records were removed. After that, the identified reports were retrieved and assessed for eligibility. Further, reference lists of these reports were screened for additional studies. The main author extracted the following relevant data from each eligible study: first author and year of publication, study design and setting, intervention description, characteristics of participants, duration of follow-up, outcome measures (pain, disability, quality of life), medication use, drop-outs and adverse events reports. Since the aim of this narrative review was not to evaluate the effectiveness of exposure-based approaches over other therapies but only associated harms and their safety, an extension of the CONSORT statement for reporting harms [47] was used for all included studies. Even though CONSORT harms extension was developed for evaluation of randomized clinical trials, it was also used for any prospective interventional study included in this review, as it was used by some authors for evaluation of observational studies previously [50, 51]. Further, to summarize to what extent the harms are reported overall in the studies regarding exposure-based approaches, CONSORT harms extension [47] was used also for studies primarily investigating efficacy, despite of being intended for studies primarily investigating harms. Both these discrepancies will be distinguished in the results section.
4.Results
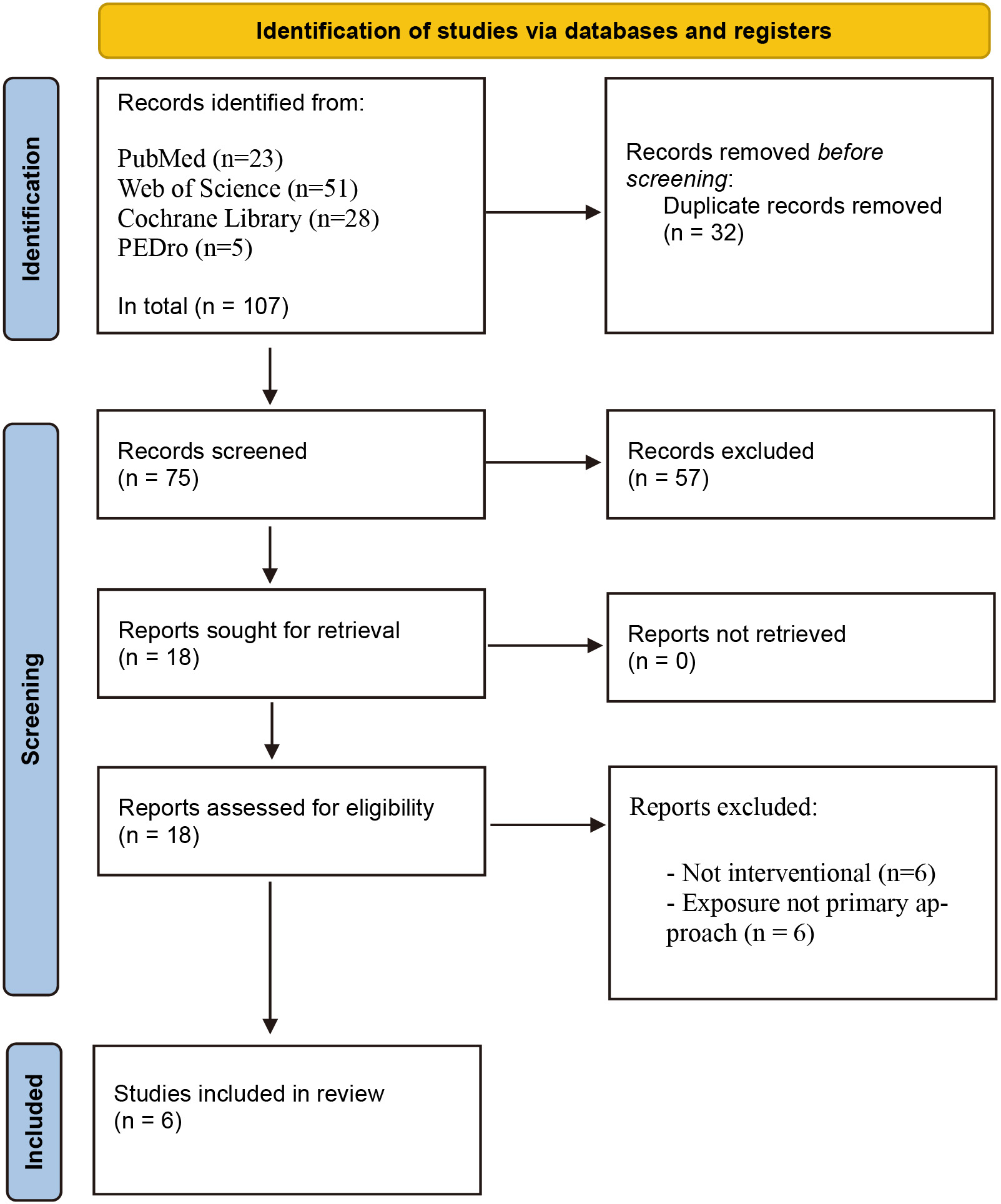
A total of 107 records were identified through the search. Duplicates (
Figure 1.
Flow diagram.
Only one study reported “safety” as a primary goal [37] and one study reported “efficacy and safety” as a primary goals but focused on efficacy only [31]. Only two identified studies were randomized controlled trials [36, 52]. Regarding adverse events associated with PEPT and its safety, van de Meent et al. [37] actively collected data about the severity of predefined CRPS signs and symptoms as well as functioning and disability 3–4 times per treatment phase and specified that a 30% change was determined as a minimal clinically important change (MCID), but no grading was implemented. Even though described, fluctuations in symptoms on an individual level were unfortunately not numerically presented and only some measurement methods were previously validated. Further, Barnhoorn et al. [52] stated that serious adverse events during PEPT treatment were collected through the use of a standardized form, but without sufficient details – in the trial protocol [54] it was found that exacerbations of signs and symptoms leading to medical consultation were monitored with this form but it was not clear whether an active or passive approach was implemented. Two other studies mentioned the absence of adverse events or harms but did not specify anything about their collection or interpretation [31, 36]. It can be speculated that in these studies the absence of adverse events or safety was referring to disability and pain outcomes but this was not explicitly specified and necessary details were lacking. Further, in two studies adverse events or harms were not mentioned at all [30, 53]. No study specified how severity or seriousness was measured nor whether and how causality was assessed or determined. On the other hand, all the included studies provided sufficient descriptions of withdrawals that were due to harm and the experience of the allocated treatment. Although drop-out rates were significant (25 out of 201, i.e. 12%), most of them occurred prior to the treatment or after education about the treatment (
Follow-ups in the included studies ranged between 2–9 months and the mode was 6 months. Although fluctuation of symptoms during the intervention phase as well as a temporary increase in pain and other symptoms during and after physiotherapy sessions were common, this was expected and explained to patients. No study reported any long-lasting increase in symptoms or deterioration of function at follow-up. It is of interest, that all the included studies that presented numerical data for pain intensity (sample means) [31, 36, 37, 52] reported a decrease in pain at follow-up which was clinically significant, despite the fact that pain reduction was not the main aim of these approaches. Of interest is also the
Table 3
Extended CONSORT criteria – quality of reporting of harms [47]
| van de Meent et al. [37] (†) | Barnhoorn et al. [52] (*‡) | Ek et al. [31] (‡) | den Hollander et al. [36] (*‡) | de Jong et al. [30] (§) | den Hollander et al. [53] (§) | ||
|---|---|---|---|---|---|---|---|
| 1. If the study collected data on harms and benefits, the title or abstract should so state. |
|
|
|
| / | / | 2/6 |
| 2. If the trial addresses both harms and benefits, the introduction should so state. |
|
|
|
| / | / | 2/6 |
| 3. List addressed adverse events with definitions for each. |
|
|
|
| / | / | 1/6 |
| 4. Clarify how harms-related outcomes were collected. |
|
|
|
| / | / | 2/6 |
| 5. Describe plans for presenting and analyzing information on harms. |
|
|
|
| / | / | 1/6 |
| 6. Describe for each treatment arm the participant withdrawals that are due to harms and the experience with the allocated treatment. |
|
|
|
|
|
| 6/6 |
| 7. Provide the denominators for analyses on harm. |
|
|
|
| / | / | 1/6 |
| 8. Present the absolute risk of each adverse event and present appropriate metrics for recurrent events, continuous variables and scale variables, whenever pertinent. |
|
|
|
| / | / | 1/6 |
| 9. Describe any subgroup analyses and exploratory analyses for harms. |
|
|
|
| / | / | 0/6 |
| 10. Provide a balanced discussion of benefits and harms with emphasis on study limitations, generalizability, and other sources of information. |
|
|
|
| / | / | 3/6 |
| 9/10 | 3/10 | 4/10 | 1/10 | 1/10 | 1/10 |
*Randomized controlled trial, † “safety” as primary goal, ‡ adverse events as secondary findings, § adverse events/harms not mentioned. “
Table 4
Summary of Pain Exposure Physical Therapy (PEPT) studies
| Authors | Study design and setting | Intervention | Sample characteristics | Outcomes | Drop-outs | Deterioration/adverse events |
|---|---|---|---|---|---|---|
| Ek et al. [31] | Prospective description of a case series Setting: not-specified outpatient clinic |
| (
|
|
|
|
| Van de Meent et al. [37] | Multiple single-case design Setting: rehabilitation department with CRPS specialization, delivered by two therapists |
| (
|
|
|
|
| Barnhoorn et al. [52] | Randomized controlled trial Setting: rehabilitation department with CRPS specialization, delivered by two physical therapists trained by a psychologist |
| (
|
|
|
|
CONT – control group; ISS-RV – Impairment level Sum Score-Restricted Version; MCID – Minimal Clinically Important Change; PDI – Pain Disability Index; PEPT – Pain Exposure Physical Therapy; RST-lim – Radboud Skills Test limitation score; SF-36-PHC – 36-Item Short Form Survey-physical health component; VAS – Visual Analogue Scale.
Table 5
Summary of Graded Exposure in vivo (GEXP) studies
| Authors | Study design and setting | Intervention | Sample characteristics | Outcomes | Drop-outs | Deterioration/adverse events |
|---|---|---|---|---|---|---|
| de Jong et al. [32] | Single-case experimental design Setting: secondary care; experienced behavioural therapist, supervised by a rehabilitation specialist |
| (
|
|
|
|
| den Hollander et al. [36] | Randomized controlled trial Setting: tertiary care centre, experienced GEXP therapists |
| (
|
|
|
|
| den Hollander et al. [53] | Replicated single-case experimental design Setting: outpatient rehabilitation department, behavioural therapist and an occupational therapist experienced in the cognitive behavioural rehabilitation |
| (
|
|
|
|
CONT – control group; GEXP – Graded Exposure in vivo (m-multiple, r-repeated); NPS – Neuropathic Pain Scale; PCS – Pain Catastrophizing Scale; QRS – Questionnaire Rising and Sitting down; RASQ – Radbound Skills Questionnaire; SF-36-PC – 36-Item Short Form Survey-Physical Component; TSK – Tampa Scale of Kinesiophobia; TENS – Transcutaneous Electric Neural Stimulation; VAS – Visual Analogue Scale; WAQ – Walking Ability Questionnaire; WSQ – Walking Stairs Questionnaire.
observation that positive change in symptoms and function is more pronounced with longer follow-up after the treatment phase [30, 36, 37, 52] which indicates that the effects of exposure-based therapies seem rather to increase over time and that early short-term increases in symptoms can precede improvement in some patients. It should be noted, however, that in both included RCTs medication was used together with the exposure-based approach in some patients (36% in PEPT [52] and 65% in GEXP [36]). In the other two included PEPT studies no report on adherence with medication cessation was present and in the other two included GEXP studies no mention of medication use was found.
Taken together, no adverse events were reported outside temporary fluctuations in CRPS-related symptoms but which were regarded as expected non-harmful side-effects. No withdrawals due to pain increase were reported during the treatment for GEXP and only 2% for PEPT. Summary of extracted data can be found in Tables 4 and 5.
5.Discussion
Even though only one included study evaluated “safety” as its primary goal and the reporting of harms in the rest of the included studies was of insufficient quality or absent, taken together with outcome measures, the available data does not point to any major adverse reactions by way of pain provocation during physiotherapy of individuals with CRPS outside of temporary increases in CRPS-related symptoms during the treatment period. But it has to be emphasized that absence of evidence should not be interpreted as evidence of absence, since only very few relevant studies were identified and only one focused primarily on safety. This insufficiency in harms reporting is surprising since these exposure-based approaches are not widely accepted [43]. But the included studies are not an exception, since a recent Cochrane review [22] reports that most studies regarding physiotherapy for CRPS did not report on adverse events and generally we are uncertain if any of the physiotherapy treatments investigated in the Cochrane review of RCTs (including PEPT [52] a GEXP [36]) caused any unwanted side effects [22]. For this reason, comparison with other approaches is not possible. But inadequate reporting of harms is generally problematic across clinical areas and types of interventions [55, 56].
It should be emphasized that the results of this review must not be generalized to any pain provocation in CRPS patients. For example, even though based mainly on expert opinion for lack of robust evidence, elective surgery is recommended to be performed no less than 12 months after symptoms have settled or at least after the symptoms are well controlled because of the expected risk of exacerbation or recurrence of CRPS [57, 58, 59]. In cases when surgery is indicated, careful patient selection and appropriate pre-, peri- and post-operative management may lower this risk, but a number of the presented studies used older diagnostic criteria or combined CRPS types I and II [60, 61, 62, 63].
What needs consideration is that drop-out rates indicate that
For future research, it should be recommended that reporting of harms and data about symptom fluctuation should be of higher quality and detail. Open or semi-structured questions may provide additional information about both expected and unexpected adverse events and harms. Also, reporting of psychological impact outside pain-related fears might be valuable as well (distress, anxiety, depression, etc.). Even though not based on any evidence, some authors argue that only activities in the full control of CRPS patients should be implemented because of the potential for psychologically traumatizing events due to insensitive handling or interventions against the will of the individual with CRPS [65]. Higher quality of harm reporting should lead to more realistic expectations and set boundaries about what is a common and normal reaction to these approaches and how to prevent any unintended harms. In terms of treatment effectiveness, comparison is also not possible since only two of the involved studies were RCTs and there are some methodological concerns in both of them [66]. Generally, there is a lack of higher-quality evidence to inform clinical decision-making [22, 29].
6.Limitations
The main limitation of this narrative review is that available evidence is sparse and generally of low quality – only one identified study evaluated “safety” as the primary goal. Further, in almost all the included studies the treatment was delivered in a CRPS-specialized setting and/or by specifically trained therapist, which decreases any external validity for common practice. A significant risk for bias is that evaluation based on extended CONSORT criteria for reporting of harms [47] was performed by only one author. This is of importance because the subjective nature of assessment of harms reporting (e.g. multiple components in only one item) probably causes inconsistencies in assessments across assessors and reviews [55, 56]. Further, even though the Scale for the Quality Assessment of Narrative Review Articles (SANRA) [45] was followed, narrative reviews are generally more prone to bias than systematic reviews, but for which significant resources are necessary.
7.Conclusion
Even though only very few relevant studies were identified and the reporting of harms in the included studies was generally of insufficient quality and therefore our confidence in the evidence is very low, taken together with outcome measures, available data does not point to any major harms associated with exposure-based approaches and related pain provocation during physiotherapy of CRPS. No deterioration in symptoms or function was reported at follow-ups and the majority of patients motivated enough to initiate participation in these pain-provoking treatments were able to perform the proposed exercises despite temporary fluctuations in CRPS-related symptoms. Comparison with other approaches is not possible since harms reporting is generally lacking and therefore should be a priority in future research.
Funding
The author reports no funding.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Acknowledgments
The author has no acknowledgments.
Conflict of interest
The author declares that there are no conflicts of interest.
References
[1] | Goebel A, Barker C, Birklein F, Brunner F, Casale R, Eccleston C, et al. Standards for the diagnosis and management of complex regional pain syndrome: Results of a European Pain Federation task force. Eur J Pain. (2019) ; 23: : 641–51. doi: 10.1002/ejp.1362. |
[2] | Stanton-Hicks M. CRPS: what’s in a name? Taxonomy, epidemiology, neurologic, immune and autoimmune considerations. Reg Anesth Pain Med. (2019) ; 44: : 376–87. doi: 10.1136/rapm-2018-100064. |
[3] | Ott S, Maihöfner C. Signs and symptoms in 1,043 patients with complex regional pain syndrome. J Pain. (2018) ; 19: : 599–611. doi: 10.1016/j.jpain.2018.01.004. |
[4] | Altas EU, Onat ŞŞ, Konak HE, Polat CS. Post-stroke complex regional pain syndrome and related factors: Experiences from a tertiary rehabilitation center. J Stroke Cerebrovasc Dis. (2020) ; 29: : 104995. doi: 10.1016/j.jstrokecerebrovasdis.2020.104995. |
[5] | Iolascon G, de Sire A, Moretti A, Gimigliano F. Complex regional pain syndrome (CRPS) type I: Historical perspective and critical issues. Clin Cases Miner Bone Metab. (2015) ; 12: : 4–10. doi: 10.11138/ccmbm/2015.12.3s.004. |
[6] | Bharwani KD, Kersten AB, Stone AL, Birklein F, Bruehl S, Dirckx M, et al. Denying the truth does not change the facts: A systematic analysis of pseudoscientific denial of complex regional pain syndrome. J Pain Res. (2021) ; 14: : 3359–76. doi: 10.2147/JPR.S326638. |
[7] | de Sire A, Paoletta M, Moretti A, Brandi ML, Iolascon G. Complex regional pain syndrome: Facts on causes, diagnosis and therapy. Clinical Cases in Mineral and Bone Metabolism. (2018) ; 15: : 166–72. doi: 10.11138/ccmbm/2018.15.2.166. |
[8] | Knudsen LF, Terkelsen AJ, Drummond PD, Birklein F. Complex regional pain syndrome: A focus on the autonomic nervous system. Clin Auton Res. (2019) ; 29: : 457–67. doi: 10.1007/s10286-019-00612-0. |
[9] | Cooper MS, Clark VP. Neuroinflammation, neuroautoimmunity, and the co-morbidities of complex regional pain syndrome. J Neuroimmune Pharmacol. (2013) ; 8: : 452–69. doi: 10.1007/s11481-012-9392-x. |
[10] | Oaklander AL, Rissmiller JG, Gelman LB, Zheng L, Chang Y, Gott R. Evidence of focal small-fiber axonal degeneration in complex regional pain syndrome-I (reflex sympathetic dystrophy). Pain. (2006) ; 120: : 235–43. doi: 10.1016/j.pain.2005.09.036. |
[11] | Velzen G, Rombouts S, Buchem M, Barthel J, Hilten J. Is the brain of complex regional pain syndrome patients truly different? Eur J Pain. (2016) ; 20: : 1622–33. doi: 10.1002/ejp.882. |
[12] | Prasad MA, Chakravarthy MK. Review of complex regional pain syndrome and the role of the neuroimmune axis. Mol Pain. (2021) ; 17: : 17448069211006616. doi: 10.1177/1744806. |
[13] | Andronic D, Andronic O, Juengel A, Berli MC, Distler O, Brunner F. Skin biomarkers associated with complex regional pain syndrome (CRPS) type I: A systematic review. Rheumatol Int. (2022) ; 42: : 937–47. doi: 10.1007/s00296-021-05061-5. |
[14] | Bilgili A, Çakır T, Doğan ŞK, Erçalık T, Filiz MB, Toraman F. The effectiveness of transcutaneous electrical nerve stimulation in the management of patients with complex regional pain syndrome: A randomized, double-blinded, placebo-controlled prospective study. J Back Musculoskelet Rehabil. (2016) ; 29: : 661–71. doi: 10.3233/BMR-160667. |
[15] | Zangrandi A, Allen Demers F, Schneider C. Complex regional pain syndrome. A comprehensive review on neuroplastic changes supporting the use of non-invasive neurostimulation in clinical settings. Front Pain Res (Lausanne). (2021) ; 2: : 732343. doi: 10.3389/fpain.2021.732343. |
[16] | Littlejohn G. Therapy: Bisphosphonates for early complex regional pain syndrome. Nat Rev Rheumatol. (2013) ; 9: : 199–200. doi: 10.1038/nrrheum.2013.6. |
[17] | Varenna M, Braga V, Gatti D, Iolascon G, Frediani B, Zucchi F, et al. Intramuscular neridronate for the treatment of complex regional pain syndrome type 1: A randomized, double-blind, placebo-controlled study. Therapeutic Advances in Musculoskeletal. (2021) ; 13: : 1759720X2110140. doi: 10.1177/1759720X211014020. |
[18] | Varenna M, Adami S, Rossini M, Gatti D, Idolazzi L, Zucchi F, et al. Treatment of complex regional pain syndrome type I with neridronate: A randomized, double-blind, placebo-controlled study. Rheumatology. (2013) ; 52: : 534–42. doi: 10.1093/rheumatology/kes312. |
[19] | Goebel A, Turner-Stokes LF. Complex regional pain syndrome in adults (2nd edition): UK guidelines for diagnosis, referral and management in primary and secondary care. 2nd ed. London: Royal College of Physicians of London; (2018) . |
[20] | Bean DJ, Johnson MH, Heiss-Dunlop W, Kydd RR. Extent of recovery in the first 12 months of complex regional pain syndrome type-1: A prospective study. Eur J Pain. (2016) ; 20: : 884–94. doi: 10.1002/ejp.813. |
[21] | Bean DJ, Johnson MH, Kydd RR. The outcome of complex regional pain syndrome type 1: A systematic review. The Journal of Pain. (2014) ; 15: : 677–90. doi: 10.1016/j.jpain.2014.01.500. |
[22] | Smart KM, Ferraro MC, Wand BM, O’Connell NE. Physiotherapy for pain and disability in adults with complex regional pain syndrome (CRPS) types I and II [Systematic Review]. Cochrane Database of Systematic Reviews 2022 2022. |
[23] | Duong S, Bravo D, Todd KJ, Finlayson RJ, Tran DQ. Treatment of complex regional pain syndrome: An updated systematic review and narrative synthesis. Can J Anaesth. (2018) ; 65: : 658–84. doi: 10.1007/s12630-018-1091-5. |
[24] | Żyluk A, Puchalski P. Effectiveness of complex regional pain syndrome treatment: A systematic review. K Neurochir Pol. (2018) ; 52: : 326–33. doi: 10.1016/j.pjnns.2018.03.001. |
[25] | Méndez-Rebolledo G, Gatica-Rojas V, Torres-Cueco R, Albornoz-Verdugo M, Guzmán-Muñoz E. Update on the effects of graded motor imagery and mirror therapy on complex regional pain syndrome type 1: A systematic review. J Back Musculoskelet Rehabil. (2017) ; 30: : 441–9. doi: 10.3233/BMR-150500. |
[26] | Perez RS, Zollinger PE, Dijkstra PU, Thomassen-Hilgersom IL, Zuurmond WW, Rosenbrand KC, et al. Evidence based guidelines for complex regional pain syndrome type 1. BMC Neurol. (2010) ; 10: : 20. doi: 10.1186/1471-2377-10-20. |
[27] | Harden RN, McCabe CS, Goebel A, Massey M, Suvar T, Grieve S, et al. Complex regional pain syndrome: Practical diagnostic and treatment guidelines, 5th edition. Pain Med. (2022) ; 23: : S1–53. doi: 10.1093/pm/pnac046. |
[28] | Pons T, Shipton EA, Williman J, Mulder RT. A proposed clinical conceptual model for the physiotherapy management of Complex Regional Pain Syndrome (CRPS). Musculoskeletal Science & Practice. (2018) ; 38: : 15–22. doi: 10.1016/j.msksp.2018.08.001. |
[29] | Packham T, Holly J. Mechanism-specific rehabilitation management of complex regional pain syndrome: Proposed recommendations from evidence synthesis. J Hand Ther. (2018) ; 31: : 238–49. doi: 10.1016/j.jht.2018.01.007. |
[30] | Jong JR, Vlaeyen JWS, Onghena P, Cuypers C, Hollander M, Ruijgrok J. Reduction of pain-related fear in complex regional pain syndrome type I: The application of graded exposure in vivo. Pain. (2005) ; 116: : 264–75. doi: 10.1016/j.pain.2005.04.019. |
[31] | Ek J-W, Gijn JC, Samwel H, Egmond J, Klomp FPAJ, Dongen RTM. Pain exposure physical therapy may be a safe and effective treatment for longstanding complex regional pain syndrome type 1: A case series. Clin Rehabil. (2009) ; 23: : 1059–66. doi: 10.1177/0269215509339875. |
[32] | Jong JR, Vlaeyen JWS, Gelder JM, Patijn J. Pain-related fear, perceived harmfulness of activities, and functional limitations in complex regional pain syndrome type I. J Pain. (2011) ; 12: : 1209–18. doi: 10.1016/j.jpain.2011.06.010. |
[33] | Barnhoorn KJ, Staal JB, Dongen RTM, Frölke JPM, Klomp FP, Meent H, et al. Are pain-related fears mediators for reducing disability and pain in patients with complex regional pain syndrome type 1? An explorative analysis on pain exposure physical therapy. PLoS One. (2014) ; 10: : e0123008. doi: 10.1371/journal.pone.0123008. |
[34] | López-de-Uralde-Villanueva I, Muñoz-García D, Gil-Martínez A, Pardo-Montero J, Muñoz-Plata R, Angulo-Díaz-Parreño S, et al. A systematic review and meta-analysis on the effectiveness of graded activity and graded exposure for chronic nonspecific low back pain. Pain Med. (2016) ; 17: : 172–88. doi: 10.1111/pme.12882. |
[35] | Vlaeyen JWS, Crombez G, Linton SJ. The fear-avoidance model of pain. Pain. (2016) ; 157: : 1588–9. doi: 10.1097/j.pain.0000000000000574. |
[36] | Hollander M, Goossens M, Jong J, Ruijgrok J, Oosterhof J, Onghena P, et al. Expose or protect? A randomized controlled trial of exposure in vivo vs pain-contingent treatment as usual in patients with complex regional pain syndrome type 1. Pain. (2016) ; 157: : 2318–29. doi: 10.1097/j.pain.0000000000000651. |
[37] | Meent H, Oerlemans M, Bruggeman A, Klomp F, Dongen R, Oostendorp R, et al. Safety of “pain exposure” physical therapy in patients with complex regional pain syndrome type 1. Pain. (2011) ; 152: : 1431–8. doi: 10.1016/j.pain.2011.02.032. |
[38] | Moseley GL, Butler SD, Beames BT, Giles TJ. The Graded Motor Imagery Handbook. Noigroup publications; (2012) . |
[39] | Watson HK, Carlson L. Treatment of reflex sympathetic dystrophy of the hand with an active “stress loading” program. J Hand Surg Am. (1987) ; 12: : 779–85. doi: 10.1016/s0363-5023(87)80069-2. |
[40] | Anandkumar S, Manivasagam M. Multimodal physical therapy management of a 48-year-old female with post-stroke complex regional pain syndrome. Physiother Theory Pract. (2014) ; 30: : 38–48. doi: 10.3109/09593985.2013.814186. |
[41] | Fisher-Pipher S, Kenyon LK. Management of bilateral complex regional pain syndrome in a pediatric patient. Pediatric Physical Therapy. (2015) ; 27: : 443–51. doi: 10.1097/PEP.0000000000000175. |
[42] | Grieve S, Llewellyn A, Jones L, Manns S, Glanville V, McCabe CS. Complex regional pain syndrome: An international survey of clinical practice. Eur J Pain. (2019) ; 23: : 1890–903. doi: 10.1002/ejp.1463. |
[43] | Miller C, Williams M, Heine P, Williamson E, O’connell N. Current practice in the rehabilitation of complex regional pain syndrome: A survey of practitioners. Disability and Rehabilitation. (2019) ; 41: : 847–53. doi: 10.1080/09638288.2017.1407968. |
[44] | Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ. (2021) ; 372: : n160. doi: 10.1136/bmj.n160. |
[45] | Baethge C, Goldbeck-Wood S, Mertens S. SANRA – a scale for the quality assessment of narrative review articles. Research Integrity and Peer Review. (2019) ; 4: : 5. doi: 10.1186/s41073-019-0064-8. |
[46] | Zorzela L, Loke YK, Ioannidis JP, Golder S, Santaguida P, Altman DG, et al. PRISMA harms checklist: Improving harms reporting in systematic reviews. BMJ. (2016) ; 352: : i157. doi: 10.1136/bmj.i157. |
[47] | Ioannidis JPA, Evans SJW, Gøtzsche PC, O’Neill RT, Altman DG, Schulz K, et al. Better reporting of harms in randomized trials: An extension of the CONSORT statement. Ann Intern Med. (2004) ; 141: : 781–8. doi: 10.7326/0003-4819-141-10-200411160-00009. |
[48] | Forouzanfar T, Weber WEJ, Kemler M, van Kleef M. What is a meaningful pain reduction in patients with complex regional pain syndrome type 1? Clin J Pain. (2003) ; 19: : 281–5. doi: 10.1097/00002508-200309000-00001. |
[49] | Bahreini M, Safaie A, Mirfazaelian H, Jalili M. How much change in pain score does really matter to patients? Am J Emerg Med. (2020) ; 38: : 1641–6. doi: 10.1016/j.ajem.2019.158489. |
[50] | Carlesso LC, Gross AR, Santaguida PL, Burnie S, Voth S, Sadi J. Adverse events associated with the use of cervical manipulation and mobilization for the treatment of neck pain in adults: A systematic review. Man Ther. (2010) ; 15: : 434–44. doi: 10.1016/j.math.2010.02.006. |
[51] | Carlesso LC, Macdermid JC, Santaguida LP. Standardization of adverse event terminology and reporting in orthopaedic physical therapy: Application to the cervical spine. J Orthop Sports Phys Ther. (2010) ; 40: : 455–63. doi: 10.2519/jospt.2010.3229. |
[52] | Barnhoorn KJ, Meent H, Dongen RTM, Klomp FP, Groenewoud H, Samwel H, et al. Pain exposure physical therapy (PEPT) compared to conventional treatment in complex regional pain syndrome type 1: A randomised controlled trial. BMJ Open. (2015) ; 5: : e008283. doi: 10.1136/bmjopen-2015-008283. |
[53] | Hollander M, Jong J, Onghena P, Vlaeyen JWS. Generalization of exposure in vivo in Complex Regional Pain Syndrome type I. Behav Res Ther. (2020) ; 124: : 103511. doi: 10.1016/j.brat.2019.103511. |
[54] | Barnhoorn KJ, Oostendorp RAB, Dongen RTM, Klomp FP, Samwel H, Wilt GJ, et al. The effectiveness and cost evaluation of pain exposure physical therapy and conventional therapy in patients with complex regional pain syndrome type 1. Rationale and design of a randomized controlled trial. BMC Musculoskelet Disord. (2012) ; 13: : 58. doi: 10.1186/1471-2474-13-58. |
[55] | Hodkinson A, Kirkham JJ, Tudur-Smith C, Gamble C. Reporting of harms data in RCTs: A systematic review of empirical assessments against the CONSORT harms extension. BMJ Open. (2013) ; 3: : e003436. doi: 10.1136/bmjopen-2013-003436. |
[56] | Junqueira DR, Phillips R, Zorzela L, Golder S, Loke Y, Moher D, et al. Time to improve the reporting of harms in randomized controlled trials. Journal of Clinical Epidemiology. (2021) ; 136: : 216–20. doi: 10.1016/j.jclinepi.2021.04.020. |
[57] | Henderson J. Updated guidelines on complex regional pain syndrome in adults. J Plast Reconstr Aesthet Surg. (2019) ; 72: : 1–3. doi: 10.1016/j.bjps.2018.08.017. |
[58] | Katz MM, Hungerford DS. Reflex sympathetic dystrophy affecting the knee. J Bone Joint Surg Br. (1987) ; 69: : 797–803. doi: 10.1302/0301-620X.69B5.3680346. |
[59] | Lunden LK, Kleggetveit IP, Jørum E. Delayed diagnosis and worsening of pain following orthopedic surgery in patients with complex regional pain syndrome (CRPS). Scand J Pain. (2016) ; 11: : 27–33. doi: 10.1016/j.sjpain.2015.11.004. |
[60] | Marx C, Wiedersheim P, Michel BA, Stucki G. Preventing recurrence of reflex sympathetic dystrophy in patients requiring an operative intervention at the site of dystrophy after surgery. Clin Rheumatol. (2001) ; 20: : 114–8. doi: 10.1007/s100670170080. |
[61] | Veldman PH, Goris RJ. Surgery on extremities with reflex sympathetic dystrophy. Unfallchirurg. (1995) ; 98: : 45–8. |
[62] | Kissling RO, Bloesch AC, Sager M, Dambacher MA, Schreiber A. Prevention of recurrence of Sudeck’s disease with calcitonin. Rev Chir Orthop Reparatrice Appar Mot. (1991) ; 77: : 562–7. |
[63] | Dellon AL, Andonian E, Rosson GD. CRPS of the upper or lower extremity: Surgical treatment outcomes. J Brachial Plex Peripher Nerve Inj. (2009) ; 4: : 1. doi: 10.1186/1749-7221-4-1. |
[64] | Glombiewski JA, Holzapfel S, Riecke J, Vlaeyen JWS, Jong J, Lemmer G, et al. Exposure and CBT for chronic back pain: An RCT on differential efficacy and optimal length of treatment. J Consult Clin Psychol. (2018) ; 86: : 533–45. doi: 10.1037/ccp0000298. |
[65] | Birklein F, O’Neill D, Schlereth T. Complex regional pain syndrome: An optimistic perspective. Neurology. (2015) ; 84: : 89–96. doi: 10.1212/WNL.0000000000001095. |
[66] | Moseley GL. More than “just do it” – fear-based exposure for complex regional pain syndrome. Pain. (2016) ; 157: : 2145–7. doi: 10.1097/j.pain.0000000000000667. |


