
Neoadjuvant Cisplatin, Gemcitabine, and Docetaxel in Sarcomatoid Bladder Cancer: Clinical Activity and Whole Transcriptome Analysis
Abstract
BACKGROUND:
Sarcomatoid urothelial cancer of the bladder (SBC) is a rare, but aggressive histological subtype for which novel treatments are needed.
OBJECTIVE:
We evaluated the clinical activity and safety of neoadjuvant cisplatin plus gemcitabine plus docetaxel (CGD) in muscle-invasive patients with SBC and assessed SBC tumor biology by whole transcriptome RNA sequencing.
METHODS:
A single-institution, retrospective analysis of muscle-invasive SBC patients treated with neoadjuvant CGD with molecular analysis. Patients received cisplatin 35 mg/m2 + gemcitabine 800 mg/m2 + docetaxel 35 mg/m2 intravenously on days 1 and 8 + pegfilgrastim 6 mg subcutaneously on day 9 every 3 weeks for 4 cycles followed by cystectomy. The primary endpoint was pathologic complete response (ypCR) rate.
RESULTS:
Sixteen patients with SBC received neoadjuvant CGD with a ypCR rate of 38% and a < ypT2 rate of 50%. Grade 3 and 4 toxicity occurred in 80% and 40% of patients, but was manageable with 81% of patients completing > 3 CGD cycles. Whole transcriptome RNA sequencing demonstrates co-clustering of SBC with conventional urothelial tumors. SBC tumors are characterized by basal-squamous and stroma rich gene signatures with frequent increased expression of immune checkpoint (CD274 (PD-L1)), chemokine (CXCL9), and T-cell (CD8A) genes.
CONCLUSIONS:
SBC is a chemosensitive subtype, with ypCR rate similar to urothelial bladder cancer following CGD neoadjuvant therapy. Whole transcriptome tissue analyses demonstrate increased expression of immune checkpoint and T-cell genes with therapeutic implications.
INTRODUCTION
Sarcomatoid urothelial bladder cancer (SBC) is characterized by a bi-phasic histology composed of both epithelial and mesenchymal components. SBC is morphologically distinct and makes up less than 5% of all bladder cancers [1]. In retrospective investigations, SBC demonstrates an aggressive clinical course with reduced overall survival compared to conventional urothelial carcinoma (UC) [2–6]. Thus, novel treatment paradigms are essential to improve survival in this patient population.
The current standard treatment for muscle-invasive, surgically-resectable SBC is radical cystectomy (RC) [7]. Retrospective analyses suggest an improvement in overall survival (OS) in SBC patients treated with neoadjuvant chemotherapy (NAC) prior to RC compared to RC alone [8–13]. A meta-analysis has demonstrated a statistically significant 33% improvement in OS among patients with SBC who received NAC [14]. Similarly, a systemic review of NAC in patients with UC histological subtypes concluded that NAC may be beneficial to patients with SBC [15]. However, observed pathologic complete response rates (ypCR) of 9–20% in patients with SBC are lower than the 26–38% ypCR rates seen with NAC in muscle-invasive bladder cancer (MIBC) with conventional UC. [10, 11, 16–18]. Thus, the merit of NAC in patients with SBC remainsunresolved.
In 2014, an index patient at Johns Hopkins with bulky, locally-advanced, SBC of the prostatic urethra achieved a major radiographic partial response (PR) and a ypCR at cystectomy in response to combination neoadjuvant chemotherapy with cisplatin, gemcitabine, and docetaxel (CGD) (Supplementary Figure S1). The CGD regimen was chosen after consultation with our sarcoma program team. We aimed to utilize a multi-agent regimen with activity in urothelial carcinoma or soft tissue sarcomas and prior demonstration of safety [19–21]. Based on the favorable outcome of this index patient, we programmatically began offering the CGD NAC regimen to all surgically resectable SBC patients fit for such therapy. In this report, we detail clinical outcomes with this regimen and assess whole transcriptome gene expression in SBC patient tumors compared to conventional MIBC and leiomyosarcoma, a representative soft tissue sarcoma resected by our urologic surgeons. We hypothesized that CGD NAC would demonstrate a clinically meaningful pathologic CR rate in muscle invasive SBC, and that whole transcriptome analysis of SBC tumors would identify relevant SBC tumor biology insights.
MATERIALS (PATIENTS) AND METHODS
Study design
A retrospective cohort analysis of patients prospectively treated at Johns Hopkins Medical Institutions (JHMI) was conducted. Patients were not randomized in this study, and blinding was not performed. All patient clinical and tissue specimens were collected and analyzed under our IRB approved protocol (JHU IRB00176985) which was approved with a waiver of consent due to the retrospective and minimal patient risk nature. All protected health information (PHI) was removed to create an analytic dataset prior to analysis. All analyses were conducted in accord with the principles of the Helsinki Declaration [22].
Sarcomatoid bladder cancer neoadjuvant chemotherapy cohort
SBC NAC eligibility included: confirmed muscle-invasive (>T2) SBC, of any amount, by expert genitourinary pathology review on transurethral resection of bladder tumor (TURBT) specimen; no radiographic disease outside of the bladder and pelvis on pre-treatment CT scan and/or MRI imaging of the chest, abdomen, and pelvis; creatinine clearance > 50 ml/min, age > 18; ECOG performance status 0-1; and fit for curative intent cystectomy. Patients with resectable lymph node involvement were considered eligible.
Gene expression tissue analysis patients
Patients treated with curative intent cystectomy with archived formalin-fixed paraffin-embedded (FFPE) tissue available from three groups were eligible for comparative studies using RNA based gene expression tissue analyses: 1) Muscle-invasive SBC; 2) Muscle-invasive conventional UC with no SBC or other histologic subtypes present; and 3) leiomyosarcoma of the abdomen/pelvis. All diagnoses were confirmed by expert genitourinary pathology review. Use of neoadjuvant or adjuvant chemotherapy was permitted. Pre-treatment TURBT specimens were analyzed in SBC patients who received NAC. Cystectomy or surgical resection specimens were analyzed in all other groups.
Treatment
Patients with SBC eligible for cisplatin-based NAC received intravenous cisplatin 35 mg/m2, gemcitabine 800 mg/m2, and docetaxel 35 mg/m2 (CGD) on days 1 and 8 of a 21-day cycle for a maximum of 4 cycles [19]. All patients received pegfilgrastim 6 mg subcutaneous on day 9 of each cycle. Following NAC completion, a radical cystectomy with a standard pelvic lymph node dissection (LND) was performed. An extended pelvic LND was allowed at the discretion of the urologist. Similar surgical techniques were utilized in UC and leiomyosarcoma patients. All surgeries were performed at JHMI facilities.
Disease evaluations
Patients were clinically staged prior to NAC with CT or MRI imaging of the chest, abdomen, and pelvis. Restaging TURBT was not routinely performed. Complete blood count and comprehensive metabolic profile were performed prior to each NAC cycle. Treatment related toxicity events were graded according to Common Terminology Criteria for Adverse Events (CTCAE) version 5.0 [23]. Imaging was repeated prior to cystectomy to ensure no evidence of systemic progression. Pathologic staging was assessed according to the American Joint Committee on Cancer staging system [24]. Clinical and radiographic assessments after surgery followed National Comprehensive Cancer Network guidelines at the discretion of the treating physician [25]. Disease progression was assessed by RECIST criteria by the treating medical oncologist, and an independent RECIST read was not performed by the radiologist [26].
Pathologic complete response (ypCR) was defined by a ypT0, N0 stage at cystectomy. Pathologic downstaging (<ypT2) was defined by either ypT1, ypTa, or ypTis tumor stage at cystectomy with N0 nodal stage. Progression-free survival (PFS) and overall survival (OS) were defined as the time from start of treatment until radiographic progression or deathrespectively.
RNA sequencing analysis of tumor specimens
One-millimeter punch biopsy of tumor blocks or macrodissection of TURBT FFPE slides was performed in areas with greater than 75% tumor cells. Attempts were taken to focus on tumor regions enriched for SBC, however, complete restriction to pure SBC regions was not performed. RNA extraction was performed per manufacturer’s instructions (Roche High Pure miRNA, Rotkreuz, Switzerland). Library preparation and whole transcriptome RNA sequencing were performed utilizing the Ion Ampliseq™ Transcriptome Human Gene Expression kit and Ion S5™ XL sequencer platforms (Thermo Fisher Scientific, Waltham, MA). Gene expression analysis was performed using the AmpliSeqRNA analysis plugin in the Torrent Suite Software aligning the raw sequence reads to human reference genome (hg19 Ampliseq Transcriptome_ERCC_V1.fasta) using the Torrent Mapping Alignment Program (TMAP) [27].
Statistical considerations
The primary endpoint was ypCR in patients with SBC who were treated with the neoadjuvant CGD regimen. Secondary endpoints included < ypT2 rate, PFS, OS, toxicity rates, and gene expression analyses. ypCR,<ypT2, and toxicity rates are reported as percentages. PFS and OS were analyzed by Kaplan-Meier methods [28]. The gene expression data were analyzed with instruction from the R packages; “DESeq2” to normalize the sequencing data [29], “consensusMIBC” [30] to classify samples for Consensus_class, and “ComplexHeatmap” [31] and “circlize” [32] to generate heatmaps.
RESULTS
Patient demographics
Between August 2014 and July 2022, 16 patients with SBC were treated with neoadjuvant cisplatin, gemcitabine, and docetaxel. The data lock for this analysis occurred on May 17, 2023. The median age on C1D1 was 61; 6 patients were at least 69 years or older, and two patients were 80 or older. Most patients were male, Caucasian, former or current smokers, with primary tumors within the bladder. All patients had an Eastern Cooperative Group performance status of 0-1. Locally advanced disease was common with 9 patients (56%) having > T3 or node positive (N+) disease prior to treatment. Percentage of sarcomatoid subtype data was available in half of the SBC patients with 5 patients (31%) demonstrating 80% or greater sarcomatoid subtype present. Full demographics are summarized in Table 1.
Table 1
Patient Demographics (n = 16). (IQR = interquartile range; PS = performance status; UC = urothelial carcinoma; TURBT = transurethral resection of bladder tumor)
| Age, Median (IQR) | 61 (59 – 70) |
| Sex, n (%) | |
| Male | 10 (63) |
| Race, n (%) | |
| Caucasian | 12 (75) |
| African-American | 4 (25) |
| Smoking status, n (%) | |
| Current | 3 (19) |
| Former | 6 (38) |
| Never | 7 (44) |
| ECOG PS, n (%) | |
| 0 | 4 (25) |
| 1 | 12 (75) |
| Prior pelvic radiationa, n (%) | 2 (13) |
| Pre-treatment clinical stages, n (%) | |
| T2, N0 | 7 (44) |
| T3 or T4, N0 | 4 (25) |
| T3 N0 | 2 (13) |
| T4 N0 | 2 (13) |
| T any, N+ | 5 (31) |
| T2 N1 | 1 (6) |
| T3 N1 | 2 (13) |
| T3 N2 | 1 (6) |
| T4 N2 | 1 (6) |
| Primary site, n (%) | |
| Bladder | 15 (94) |
| Prostatic urethra | 1 (6) |
| Sarcomatoid TURBT percentage | |
| 80–100% | 5 (31) |
| <80% | 3 (19) |
| Not reported | 8 (50) |
aTwo male patients with clinically localized prostate cancer were treated with brachytherapy and brachytherapy plus external beam radiation 5 and 9 years respectively prior to their SBC diagnoses.
Clinical efficacy
Fifteen patients (94%) underwent cystectomy and were evaluable for pathologic response. One patient with a suspected solitary progressive lung metastasis did not proceed to cystectomy. This patient was later treated with radiation to the lung lesion, received pembrolizumab, developed pneumonitis, underwent biopsy of increasing mediastinal nodes which were found consistent with sarcoidosis with no malignancy. Cystoscopic surveillance of the bladder and serial CT imaging has shown no recurrence for two years off of all therapy. Six patients (38%) achieved a ypCR (Table 2). No association between sarcomatoid percentage and ypCR rate was observed with two ypCR responses in five (40%) patients with sarcomatoid percentage 80% or higher and four ypCR responses in 11 (36%) patients with less than 80% sarcomatoid percentage. Two additional patients (13%) had tumor downstaged to < ypT2 N0. Six patients (38%) had locally advanced ypT3/4 or N + disease.
Table 2
Pathologic responses (n = 16)
| Responders, n (%) | 8 (50) |
| Complete response | |
| ypT0 N0 | 6 (38) |
| Pathologic downstaging (<ypT2 N0) | 2 (13) |
| ypT1 N0 | 1 (6) |
| ypTa N0 | 1 (6) |
| Non-responders, n (%) | 8 (50) |
| Node-negative | 4 (25) |
| ypT2 N0 | 2 (13) |
| ypT4 N0 | 2 (13) |
| Node-positive or metastatic | 4 (25) |
| ypT0 N1 | 1 (6) |
| ypT2 N2 | 1 (6) |
| ypT3 N2 | 1 (6) |
| ypTx Nx M1a | 1 (6) |
aPatient developed a solitary clinical lung metastasis and did not undergo cystectomy. Biopsy of mediastinal node later showed caseating granulomas consistent with sarcoidosis.
With a median follow up of 23.1 months, the median PFS for all patients treated with CGD NAC was 21.9 months with a median OS that has not been reached (Fig. 2). Eleven patients (69%) were alive at time of data lock, and nine patients (56%) had no disease progression at time of data lock.
Fig. 1
Survival Analyses of Sarcomatoid Bladder Cancer Patients treated with Neoadjuvant Cisplatin+Gemcitabine+Docetaxel. A. Progression-Free Survival, B. Overall Survival.
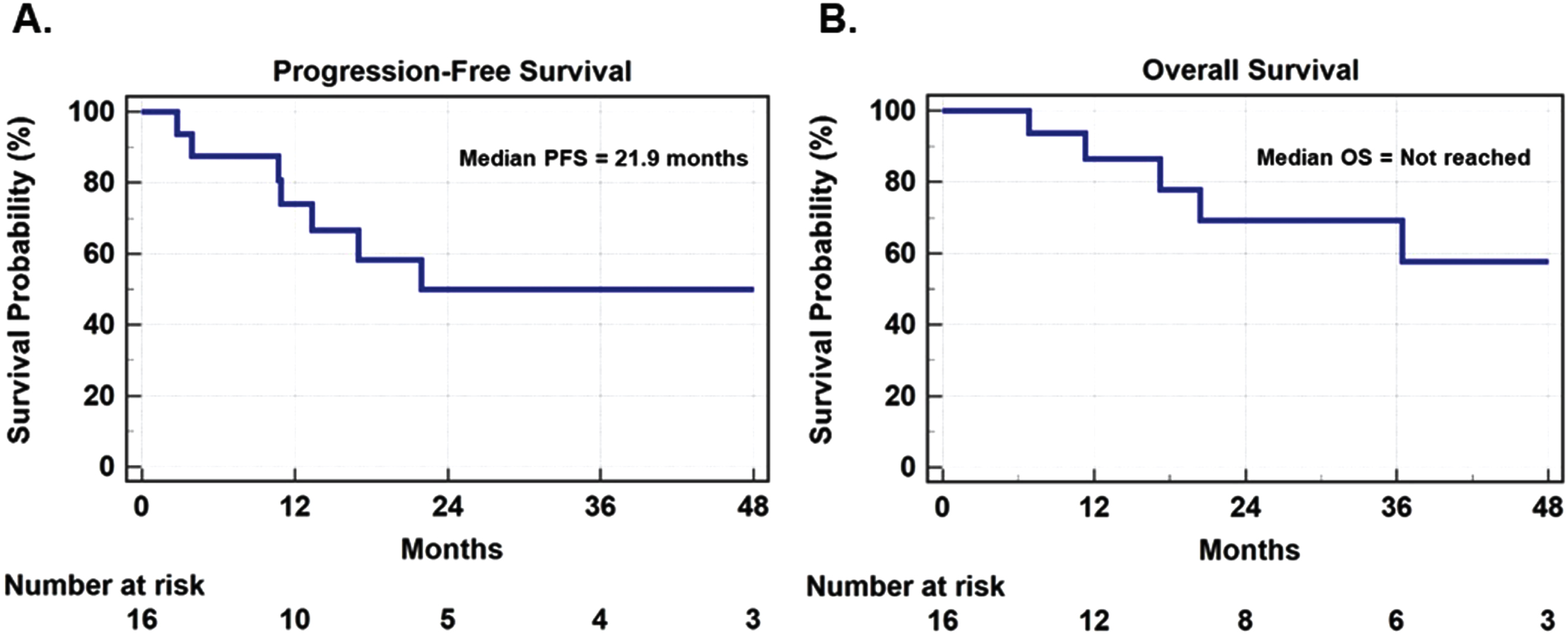
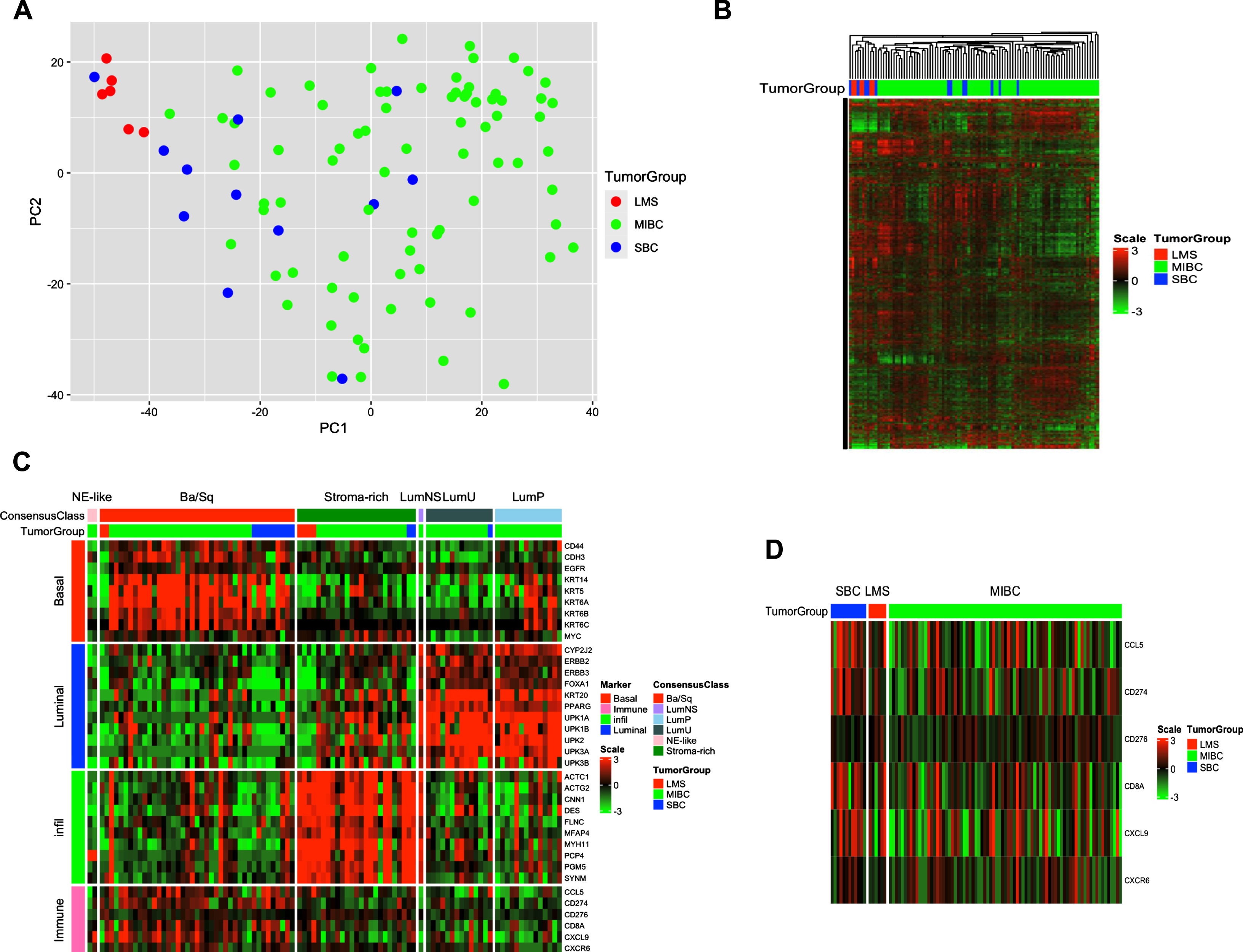
Fig. 2
Whole Transcriptome Analysis of SBC compared to MIBC and leiomyosarcoma. A. Principal component analysis of the SBC (n = 12), MIBC (n = 79), and leiomyosarcoma (n = 6) sample RNA sequencing data. Green = MIBC, Blue = SBC, Red = leiomyosarcoma. B. Unsupervised cluster analysis of gene expression among the top 5000 most variable genes of the samples in (A.). Green = MIBC, Blue = SBC, and Red = leiomyosarcoma. Red denotes higher expression, and green denotes lower expression. C. Application of The Consensus Molecular Classifier Gene Expression Signatures of Muscle-Invasive Bladder Cancer to SBC (n = 12), MIBC (n = 79), and leiomyosarcoma (n = 6) sample RNA sequencing data. Green = MIBC, Blue = SBC, Red = leiomyosarcoma. D. Gene Expression Signatures of Key Anti-tumor Immune Response, Inflammation, and T-cell Infiltration Genes in SBC (n = 12), MIBC (n = 79), and leiomyosarcoma (n = 6) sample RNA sequencing data. Green = MIBC, Blue = SBC, Red = leiomyosarcoma using the same color schema as in (B.). SBC = sarcomatoid bladder cancer; MIBC = muscle-invasive bladder cancer.
Toxicity and safety
Eight (50%) patients completed all four planned cycles of CGD NAC. Thirteen patients (81%) completed at least three cycles. Two of six patients 69 or older (33%) completed all four cycles, and four of six (67%) completed at least three cycles. Seven of sixteen patients (44%) required dose reductions, most commonly for myelosuppression or worsening renal function. Surgery was performed a median of 54 days (IQR 46 – 61) from the last day of chemotherapy administration.
Grade 3 toxicity events were observed in 12 (80%) patients and grade 4 toxicity events in 6 (40%) patients. Grade 3 events occurring in more than 10% of patients included: anemia (77%), thrombocytopenia (23%), fatigue (20%), hyponatremia (15%), and infection (13%). Grade 4 events included: thrombocytopenia (23%), pulmonary embolism (13%), and infection (7%). The full toxicity profile is shown in Table 3. Seven patients (44%) were admitted either during or just after NAC. Four admissions were due to infection, one due to clot associated urinary retention, one due to deep vein thrombosis, and one due to acute kidney injury. No surgeries were aborted due to on-treatment toxicity. No on-treatment or perioperative deaths were observed.
Table 3
All grade toxicity
| Grade 1-2 | Grade 3 | Grade 4 | |
| Hematologic and Laboratory (n = 13 evaluable), n (%) | |||
| Hematologic | |||
| Leukopenia | 5 (38) | 1 (8) | 1 (8) |
| Neutropenia | 4 (31) | 0 (0) | 1 (8) |
| Lymphopenia | 2 (15) | 1 (8) | 0 (0) |
| Anemia | 3 (23) | 9 (69) | 0 (4) |
| Thrombocytopenia | 3 (23) | 4 (31) | 3 (23) |
| Laboratory | |||
| Hyponatremia | 2 (15) | 3 (23) | 0 (0) |
| Hypomagnesemia | 4 (31) | 1 (8) | 0 (0) |
| Hypokalemia | 4 (31) | 0 (0) | 0 (0) |
| Hypocalcemia | 1 (8) | 1 (8) | 0 (0) |
| Hypophosphatemia | 0 (0) | 0 (0) | 1 (8) |
| Elevated creatinine | 5 (38) | 0 (0) | 0 (0) |
| Elevated alanine transferase | 5 (38) | 0 (0) | 0 (0) |
| Elevated aspartate transferase | 2 (15) | 0 (0) | 0 (0) |
| Elevated alkaline phosphatase | 4 (31) | 0 (0) | 0 (0) |
| Hyperbilirubinemia | 2 (15) | 0 (0) | 0 (0) |
| Non-hematologic (n = 15 evaluable), n (%) | |||
| Constitutional | |||
| Fatigue | 10 (67) | 3 (20) | 0 (0) |
| Pain | 2 (13) | 0 (0) | 0 (0) |
| Weight loss | 2 (13) | 0 (0) | 0 (0) |
| Infection | 3 (20) | 3(20) | 1 (7) |
| Neurologic | |||
| Headache | 2 (13) | 0 (0) | 0 (0) |
| Neuropathy | 5 (33) | 1 (7) | 0 (0) |
| Impaired hearing | 2 (13) | 0 (0) | 0 (0) |
| Pulmonary | |||
| Pulmonary embolism | 0 (0) | 0 (0) | 2 (13) |
| Dyspnea | 2 (13) | 0 (0) | 0 (0) |
| Cardiovascular | |||
| Leg swelling | 2 (13) | 0 (0) | 0 (0) |
| Deep vein thrombosis | 0 (0) | 1 (7) | 0 (0) |
| Gastrointestinal | |||
| Diarrhea | 4 (27) | 1 (7) | 0 (0) |
| Nausea | 8 (53) | 0 (0) | 0 (0) |
| Constipation | 3 (20) | 0 (0) | 0 (0) |
| Decreased appetite | 3 (20) | 0 (0) | 0 (0) |
| Taste disturbance | 3 (20) | 0 (0) | 0 (0) |
| Colitis | 0 (0) | 1 (7) | 0 (0) |
Whole transcriptome RNA sequencing analyses
Sufficient high-quality RNA for whole transcriptome RNA sequencing was available from 12 patients with SBC, 79 patients with conventional MIBC, and 6 patients with leiomyosarcoma (seminal vesicle, pelvic sidewall, pre-rectal space, kidney, uterus, and colon primary sites). Principal component analysis of RNA sequencing data from these samples demonstrated that leiomyosarcoma tumors cluster tightly, and separately from MIBC (Fig. 2A). In contrast, the majority of SBC tumors were interspersed among the MIBC tumors. Specifically, a distinct cluster of SBC tumors separate from MIBC tumors was not observed, nor did the majority of SBC tumors co-cluster tightly with the leiomyosarcoma tumors. Within the SBC tumors alone, we did not observe any transcriptomic signature differences according to older WHO sarcomatoid classification terminology in use at the time of patient diagnosis and treatment (e.g. carcinosarcoma vs UC with sarcomatoid features) (Suppl Fig S2).
In unsupervised hierarchical clustering analysis with the top 5000 most variable genes measured by median absolute deviation, leiomyosarcoma tumors again cluster tightly near each other and distinct from the MIBC tumors (Fig. 2B). The SBC tumors demonstrated prominent heterogeneity with individual SBC tumors found within both the MIBC and leiomyosarcoma tumor groups.
Upon application of the consensus molecular classifier of muscle-invasive bladder cancer gene expression signatures to each tumor specimen, most SBC tumors aligned with basal-squamous and stroma rich subtypes with only a singular tumor aligning with the luminal unstable subtype (Fig. 2C) [33]. Among the SBC basal-squamous tumors, increased expression of basal cytokeratins KRT5, KRT6A, and KRT14 were observed, whereas within the SBC stroma rich tumors, increases in the expression of mesenchymal/fibroblast genes ACTC1, DES, and MYH11 were noted. Increased expression of T-cell and inflammatory chemokine-associated genes CD274, CD8A, and CXCL9 were observed in both SBC basal-squamous and stroma-rich tumors. Among SBC tumors, nine (75%) aligned with the basal-squamous subtype, two (17%) with the stroma rich subtype and one (8%) with the luminal unstable subtype. Among SBC tumors across all subtypes, expression of inflammatory and T-cell genes was increased in the majority of tumors (Fig. 2D).
DISCUSSION
In this retrospective single-institution experience of a uniform cisplatin, gemcitabine, and docetaxel (CGD) regimen administered as neoadjuvant therapy (NAC) to patients with muscle-invasive SBC, we observed clinically relevant activity with pathologic complete response (ypCR) observed in 38% of patients. Our results compare favorably to prior reports of 9-20% pCR rates in patients with SBC when variable, non-standardized NAC regimens were utilized [10, 11, 18]. Moreover, our ypCR rates align with observed ypCR rates of 26-38% with cisplatin-based NAC regimens for conventional MIBC [16, 17, 34, 35]. Our data suggests muscle invasive SBC is chemotherapy-sensitive, and a uniform, higher-intensity regimen containing cisplatin, docetaxel, and gemcitabine may achieve superior pCR rates than previously used regimens in this disease.
While the benefit of NAC in SBC has been inconsistent in prior small, singular retrospective studies, a recent examination of SEER population-based data suggests patients with metastatic SBC who receive chemotherapy derive OS benefit [8–11, 36]. Furthermore, in a meta-analysis assessing the role of NAC or adjuvant chemotherapy in patients with bladder cancer with histologic subtypes, an OS benefit was observed in patients with SBC treated with NAC, but not adjuvant chemotherapy [14]. Similar to the patients with SBC treated with NAC in our cohort, the majority of patients in prior studies had clinical T2-T3 stage tumors [3, 4, 10]. In our study, we also noted responses in patients with clinical T4 and N + tumors. Therefore, a confounding effect of more favorable tumor stages on the higher pCR rate noted in our population is unlikely.
Treatment related toxicity was common with the higher-intensity CGD regimen with anemia, thrombocytopenia, infection, and worsening renal function as the most common grade 3 or 4 events leading to dose reductions or inability to complete all four intended treatment cycles. The grade 3 and grade 4 toxicity rates of 80% and 40% observed with the CGD regimen are higher than the 10-36% grade 3 and 8-9% grade 4 toxicity rates reported with the cisplatin and gemcitabine (CG), or the dose-dense methotrexate, vinblastine, doxorubicin, and cisplatin (ddMVAC) regimens in recent NAC investigations in conventional MIBC [16, 17, 34]. Although frequent, the CGD toxicity profile proved manageable for the majority of patients with 81% of patients able to receive at least three CGD treatment cycles. Among the six treated patients aged 69 or older, four were able to complete at least three cycles. Due to a high frequency of bulky, locally advanced bladder tumors with a tendency for accelerated hematuria due to treatment-related tumor necrosis, weekly complete blood count and comprehensive metabolic profile monitoring is recommended to rapidly detect and treat any significant treatment relatedtoxicities.
We sought to understand at a molecular level whether SBC more closely resembles conventional MIBC, a representative soft tissue sarcoma such as leiomyosarcoma, or represents its own distinct biological entity. Our analyses are primarily descriptive due to low number of SBC and leiomyosarcoma tumors analyzed. Given these limitations, our RNA sequencing analysis demonstrated that a subset of SBC clusters with conventional MIBC, which is consistent with our finding that SBC responds to CGD NAC. Our findings of increased KRT5, KRT6A, and KRT14 expression within some SBC tumors align with the work of others who have noted that such basal genes are upregulated in patients with SBC [37]. In conventional MIBC, increased expression of basal genes associates with favorable response to NAC [38].
When applying the consensus molecular classifier for MIBC to the SBC tumors, most SBC tumors aligned within either the basal-squamous or stroma rich classifications. Increased expression of genes with critical mediating functions of anti-tumor immune responses (CD274 (PD-L1)), inflammatory chemokines (CXCL9), or T-cell infiltration within the tumor microenvironment (CD8A) were observed in SBC specimens across all molecular subtypes. Our observation of frequent upregulation of CD274 (PD-L1) in SBC patient tumors agrees with similar findings from initial SBC tumor molecular characterization efforts by other groups [37]. This is especially relevant given that anti-PD-1 directed adjuvant therapy has demonstrated improved disease-free survival in patients with conventional MIBC, particularly in patients with PD-L1 positive tumors [39]. Moreover, two retrospective analyses of patients with advanced SBC treated with anti-PD-(L)1 therapy have demonstrated objective response rates of 37% and 38% respectively [40, 41]. Given this data, the PD-(L)1 pathway represents a promising therapeutic target in SBC that warrants evaluation in prospective clinical trials. Trials that are accruing will help answer this question including those examining neoadjuvant pembrolizumab combined with chemotherapy in the neoadjuvant treatment of MIBC with urothelial carcinoma histologic subtypes (including SBC) (NCT04383743) as well as combination treatment with enfortumab vedotin and pembrolizumab in patients with metastatic urothelial carcinoma histologic subtypes (including SBC) (NCT38446675), As nectin-4 expression in SBC is lower than conventional urothelial carcinoma and other histological subtypes including squamous cell carcinoma and adenocarcinoma, it remains to be seen whether this combination will be efficacious in advanced SBC [42–44].
The use of a uniform and consistent CGD dosing schedule in all patients treated represents a major strength of our study. To our knowledge, this is the first SBC data presented where a standardized chemotherapy regimen was employed. Past SBC reports of chemotherapy outcomes have relied on national registry or institutional databases to assess outcomes [8–11, 40, 41]. Therefore, evaluation of the merits of specific chemotherapy regimens was not possible. Our study establishes a preliminary benchmark for ypCR rate, PFS, and OS specific to the CGD regimen that can serve as the basis for future studies. Furthermore, our finding that the vast majority of SBC tumors demonstrate increased expression of immune checkpoint and T-cell genes confirms the initial work of other groups and has significant clinical relevance [37]. However, the small sample size of patients with SBC treated with NAC represents a limitation of the study. In addition, the single-institution nature of our study may introduce unaccounted biases with impact on clinical outcomes. Lastly, the inclusion of patients with any sarcomatoid component and the lack of variant percentage quantification in half of the SBC specimens within our SBC cohort introduces heterogeneity within the small SBC cohort that may have clinical and biologicalsignificance.
CONCLUSION
In this initial report of patients with SBC treated with a uniform cisplatin, gemcitabine, and docetaxel neoadjuvant chemotherapy regimen, we observed pathologic complete responses in 38% of patients with frequent, but manageable treatment related toxicity. Our results demonstrate that SBC is a chemosensitive malignancy and serve as a benchmark for future prospective clinical trials. Analysis of tumor RNA sequencing shows that increased expression of immune checkpoint and T-cell associated genes is frequent in SBC tumors, a finding of clinical relevance and with important implications for future SBC clinical trial considerations.
ACKNOWLEDGMENTS
We wish to thank the Bladder Cancer Advocacy Network (BCAN) for their continued support of investigations to improve the outcomes of all patients with bladder and upper tract cancers – including those with rare subtypes such as sarcomatoid urothelial carcinoma, through a series of discussions at BCAN-led Think Tank meetings on novel approaches to treat patients with histological subtypes. BCAN did not provide funding for any of the work presented in this manuscript.
FUNDING
This work was supported by grant funding from NCI Cancer Center Support grant funding (P30CA006973, B. Nelson, PI, salary support to B.A.J.), R01 grant funding (R01CA235681, to N.M.H.), and a Department of Defense Career Development Award (CA220769, to B.A.J.).
AUTHOR CONTRIBUTIONS
Conception: N.M.H.; Performance of Work: B.A.J., B.A.T., C.K., B.M., K.L., W.L., J.I.E., G.J.N., A.S.B., A.M., A.G., N.A., A.E.R., P.M.P., E.C., J.H-C., N.S., S.H.P., M.K., W.C., T.J.B., N.M.H.; Interpretation of Data: B.A.J., B.A.T., Y.J., D.J.M., W.C., N.M.H.; Writing the Article: B.A.J., N.M.H.
CONFLICT Of INTEREST
Noah Hahn discloses consulting compensation from AstraZeneca, Merck, BioGears, Seattle Genetics, Mirati, Incyte, RemGen, Janssen, Pfizer, EMD Serono, Verity Pharmaceuticals, Huron Consulting, Guidepoint, Natera, Protara Therapeutics, Astellas Pharma, Trya Biosciences; research support to the institution from HTG Molecular Diagnostics, AstraZeneca, Bristol Myers-Squibb, Genentech, Seattle Genetics, Pieris, Inovio, Principia Biopharm, Incyte, Loxo Oncology, and Ikena Oncology; speaking honorarium from Medscape. Max Kates discloses consulting compensation from Genesis Biotech, Janssen, Pacific Edge, and FerGene. Andres Matoso discloses consulting compensation from PathAI. Burles A. Johnson III discloses serving as an unpaid member of Seattle Genetics Emerging Thought Leaders Advisory Board. Burles A. Johnson III, Noah Hahn, Jean Hoffman-Censits, and David McConkey are co-authors on a provisional US patent for an immune-based biomarker to predict response to immunotherapy in patients with advanced bladder cancer.
T.J.B., J.H-C., N.M.H., and D.J.M. are on the Editorial Board of this journal, but these individuals were not involved in the peer-review process nor had access to any information regarding its peer-review.
DATA AVAILABILITY
The genomic data supporting this manuscript are currently available on request from the corresponding author, and we plan to upload these data into a publicly available database before publication.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/BLC-240008.
REFERENCES
[1] | Netto GJ , Amin MB , Berney DM , et al., The World HealthOrganization Classification of Tumors of the Urinary System and MaleGenital Organs & Part B: Prostate and Urinary Tract Tumors. European Urology. (2022) ;82: :469–482. |
[2] | Gu L , Ai Q , Cheng Q , et al., Sarcomatoid variant urothelial carcinoma of the bladder: a systematic review and meta-analysis of the clinicopathological features and survival outcomes. Cancer Cell Int. (2020) ;20: :550. |
[3] | Guo AT , Huang H , Wei LX . Clinicopathological characteristics and prognosis of Chinese patients with sarcomatoid carcinoma of the bladder. Histol Histopathol. (2013) ;28: :1167–74. |
[4] | Sanfrancesco J , McKenney JK , Leivo MZ , et al., Sarcomatoid Urothelial Carcinoma of the Bladder: Analysis of 28 Cases With Emphasis on Clinicopathologic Features and Markers of Epithelial-to-Mesenchymal Transition. Arch Pathol Lab Med. (2016) ;140: :543–51. |
[5] | Wang J , Wang FW , Lagrange CA , et al., Clinical features of sarcomatoid carcinoma (carcinosarcoma) of the urinary bladder: analysis of 221 cases. Sarcoma. (2010) , 2010. |
[6] | Wright JL , Black PC , Brown GA , et al., Differences in survival among patients with sarcomatoid carcinoma, carcinosarcoma and urothelial carcinoma of the bladder. J Urol. (2007) ;178: :2302-6; discussion 2307. |
[7] | Network NCC. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) Bladder Cancer Version 2.2023 – April 25, 2023, 2023. |
[8] | Chakiryan NH , Jiang DD , Gillis KA , et al., Pathological Downstaging and Survival Outcomes Associated with Neoadjuvant Chemotherapy for Variant Histology Muscle Invasive Bladder Cancer. J Urol. (2021) ;206: :924–932. |
[9] | Gelpi-Hammerschmidt F , Rodriguez D , Tinay I , et al. MP01-18 The potential impact of neoadjuvant chemotherapy on patients undergoing radical cystectomy for non-urothelial muscle invasive bladder cancer. The Journal of Urology. (2016) ;195: :e8. |
[10] | Sui W , Matulay JT , Onyeji IC , et al., Contemporary treatment patterns and outcomes of sarcomatoid bladder cancer. World J Urol. (2017) ;35: :1055–1061. |
[11] | Vetterlein MW , Wankowicz SAM , Seisen T , et al., Neoadjuvant chemotherapy prior to radical cystectomy for muscle-invasive bladder cancer with variant histology. Cancer. (2017) ;123: :4346–4355. |
[12] | Garje R , Ozair A , Manoharan M , et al., Survival outcomes of sarcomatoid versus classic urothelial carcinoma of bladder. Journal of Clinical Oncology. (2023) ;41: :4588–4588. |
[13] | Roy AM , Jatwani K , Kumarasamy VM , et al., Impact of neoadjuvant chemotherapy on pathological stage and survival in sarcomatoid bladder cancer. Journal of Clinical Oncology. (2023) ;41: :530–530. |
[14] | Zhu Z , Xiao Y , Hu S , et al., Neoadjuvant and Adjuvant Chemotherapy for Variant Histology Bladder Cancers: A Systematic Review and Meta-Analysis. Front Oncol. (2022) ;12: :907454. |
[15] | Veskimäe E , Espinos EL , Bruins HM , et al., What Is thePrognostic and Clinical Importance of Urothelial and NonurothelialHistological Variants of Bladder Cancer in Predicting OncologicalOutcomes in Patients with Muscle-invasive and Metastatic BladderCancer? A European Association of Urology Muscle Invasive andMetastatic Bladder Cancer Guidelines Panel Systematic Review. EurUrol Oncol. (2019) ;2: :625–642. |
[16] | Choueiri TK , Jacobus S , Bellmunt J , et al., Neoadjuvant dose-dense methotrexate, vinblastine, doxorubicin, and cisplatin with pegfilgrastim support in muscle-invasive urothelial cancer: pathologic, radiologic, and biomarker correlates. J Clin Oncol. (2014) ;32: :1889–94. |
[17] | Plimack ER , Hoffman-Censits JH , Viterbo R , et al., Accelerated methotrexate, vinblastine, doxorubicin, and cisplatin is safe, effective, and efficient neoadjuvant treatment for muscle-invasive bladder cancer: results of a multicenter phase II study with molecular correlates of response and toxicity. J Clin Oncol. (2014) ;32: :1895–901. |
[18] | Almassi N , Vertosick EA , Sjoberg DD , et al., Pathological and oncological outcomes in patients with sarcomatoid differentiation undergoing cystectomy. BJU International. (2022) ;129: :463–469. |
[19] | Pectasides D , Glotsos J , Bountouroglou N , et al., Weekly chemotherapy with docetaxel, gemcitabine and cisplatin in advanced transitional cell urothelial cancer: a phase II trial. Ann Oncol. (2002) ;13: :243–50. |
[20] | Bay JO , Ray-Coquard I , Fayette J , et al., Docetaxel and gemcitabine combination in 133 advanced soft-tissue sarcomas: a retrospective analysis. Int J Cancer. (2006) ;119: :706–11. |
[21] | Leu KM , Ostruszka LJ , Shewach D , et al., Laboratory and clinical evidence of synergistic cytotoxicity of sequential treatment with gemcitabine followed by docetaxel in the treatment of sarcoma. J Clin Oncol. (2004) ;22: :1706–12. |
[22] | Association WM . World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA. (2013) ;310: :2191–2194. |
[23] | Services UDoHaH: Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0, 2017. |
[24] | Amin MB , Greene FL , Edge SB , et al., The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. (2017) ;67: :93–99. |
[25] | Flaig TW , Spiess PE , Abern M , et al., NCCN Guidelines®Insights: Bladder Cancer, Version 2. Featured Updates to theNCCN Guidelines. Journal of the National Comprehensive CancerNetwork. (2022) ;20: :866–878. |
[26] | Eisenhauer EA , Therasse P , Bogaerts J , et al., New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. (2009) ;45: :228–47. |
[27] | Torrent Mapping Alignment Program. |
[28] | Kaplan EL , Meier P . Nonparametric Estimation from Incomplete Observations. Journal of the American Statistical Association. (1958) ;53: :457–481. |
[29] | Love MI , Huber W , Anders S . Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biology. (2014) ;15: :550. |
[30] | Kamoun A , de Reynies A , Allory Y , et al., A Consensus Molecular Classification of Muscle-invasive Bladder Cancer. Eur Urol. (2020) ;77: :420–433. |
[31] | Gu Z , Eils R , Schlesner M . Complex heatmaps reveal patterns and correlations in multidimensional genomic data. Bioinformatics. (2016) ;32: :2847–9. |
[32] | Gu Z , Gu L , Eils R , et al., circlize Implements and enhances circular visualization in R. Bioinformatics. (2014) ;30: :2811–2. |
[33] | Kamoun A , de Reyniès A , Allory Y , et al., A Consensus MolecularClassification of Muscle-invasive Bladder Cancer. Eur Urol. (2020) ;77: :420–433. |
[34] | Flaig TW , Tangen CM , Daneshmand S , et al., A Randomized Phase II Study of Coexpression Extrapolation (COXEN) with Neoadjuvant Chemotherapy for Bladder Cancer (SWOG S1314; NCT02177695). Clin Cancer Res. (2021) ;27: :2435–2441. |
[35] | Grossman HB , Natale RB , Tangen CM , et al., Neoadjuvant Chemotherapy plus Cystectomy Compared with Cystectomy Alone for Locally Advanced Bladder Cancer. New England Journal of Medicine. (2003) ;349: :859–866. |
[36] | Tappero S , Sorce G , Panunzio A , et al., Efficacy of chemotherapy on overall survival in metastatic sarcomatoid bladder cancer patients. Cent European J Urol. (2022) ;75: :352–356. |
[37] | Guo CC , Majewski T , Zhang L , et al., Dysregulation of EMT Drives the Progression to Clinically Aggressive Sarcomatoid Bladder Cancer. Cell Re-e. (1793) ;27: :4. |
[38] | Choi W , Porten S , Kim S , et al., Identification of distinct basal and luminal subtypes of muscle-invasive bladder cancer with different sensitivities to frontline chemotherapy. Cancer Cell. (2014) ;25: :152–65. |
[39] | Bajorin DF , Witjes JA , Gschwend JE , et al., Adjuvant Nivolumab versus Placebo in Muscle-Invasive Urothelial Carcinoma. New England Journal of Medicine. (2021) ;384: :2102–2114. |
[40] | Kobayashi M , Narita S , Matsui Y , et al., Impact of histological variants on outcomes in patients with urothelial carcinoma treated with pembrolizumab: a propensity score matching analysis. BJU Int. (2022) ;130: :226–234. |
[41] | Miller NJ , Khaki AR , Diamantopoulos LN , et al., Histological Subtypes and Response to PD-1/PD-L1 Blockade in Advanced Urothelial Cancer: A Retrospective Study. J Urol. (2020) ;204: :63–70. |
[42] | Hoffman-Censits J , Lombardo K , McConkey D , et al., New and topics: enfortumab vedotin mechanisms of response and resistance in urothelial cancer – What do we understand so far? Urol Oncol. (2021) ;39: :619–622. |
[43] | Hoffman-Censits JH , Lombardo KA , Parimi V , et al., Expression of Nectin-4 in Bladder Urothelial Carcinoma, in Morphologic Variants, and Nonurothelial Histotypes. Appl Immunohistochem Mol Morphol. (2021) ;29: :619–625. |
[44] | Rodler S , Eismann L , Schlenker B , et al., Expression of Nectin-4 in Variant Histologies of Bladder Cancer and Its Prognostic Value-Need for Biomarker Testing in High-Risk Patients? Cancers (Basel) 14 (2022) . |


