
Psychosocial work aspects, stress and musculoskeletal pain among musicians. A systematic review in search of correlates and predictors of playing-related pain
Abstract
BACKGROUND:
Musicians face numerous psychosocial and physical demands at work resulting in high prevalence of musculoskeletal problems. Unlike physical risks, little is known about psychosocial work factors influencing such health problems in this particular group.
OBJECTIVE:
The paper aimed to identify psychosocial work demands resulting in musculoskeletal problems among musicians.
METHODS:
A systematic review was undertaken to find data linking psychosocial work demands or stress with musculoskeletal disorders among musicians.
RESULTS:
The exploration of databases resulted in nine research studies linking psychosocial aspects of work or stress with musculoskeletal problems among musicians. The analyzed studies linked psychosocial aspects with musculoskeletal problems in three ways – showing proportions of people indicating particular causes of pain, indicating correlations between these variables or performing regression analysis showing psychosocial predictors of musculoskeletal pain.
CONCLUSIONS:
Only a few studies have undertaken the issue of psychosocial risk factors for musculoskeletal problems among musicians. The results revealed that some psychosocial aspects of work, e.g. long hours at work, work content, high job demands, low control/influence, lack of social support, were related to musculoskeletal pain, however, the methods and results were inconsistent. The extant studies employed variety of definitions of psychosocial aspects that hindered the possibility for consistent conclusions. Basing on those conclusions, future directions were offered.
1Introduction
Musicians experience specific work demands that result in a growing amount of occupational diseases [1]. Performing Arts Medicine specialists postulate that full understanding of work strain and health consequences among performers can succeed only when physical, personal and social contexts of their work are considered [1]. Why should researchers address this particular occupational group? Firstly, musicians confront high physical demands at work – repetitive movements, high arms abduction angles, forced, unnatural, asymmetrical body postures [2] etc. Secondly, they face numerous psychosocial demands that can possibly become sources of their stress – public exposure and the risk of being judged (resulting in performance anxiety), rivalry, mistakes impossible to correct when playing live, the need to practice systematically, remember the notes and concentrate for long hours, little influence on the general perception of the music played with the orchestra/band [3–5] Lastly, Playing-Related Musculoskeletal Disorders (PRMD) are exceedingly common among musicians. Because physical demands and their impact on musicians’ health have already been investigated [2, 6, 7], the following paper was aimed at identifying psychosocial work demands possibly resulting in or exacerbating PRMD symptoms among musicians. Understanding the psychosocial determinants of musicians’ musculoskeletal disorders could prevent them from pain and the decrease in working ability or premature end of their careers.
2Musicians’ work demands
Coordinating body work and bright mind constitutes a basic working tool for musicians. The job requires high physical demands coinciding with high psychological demands what exposes musicians to greater stress and increases the risk of musculoskeletal disorders. Moreover, unlike in most occupations, here the immediate symptoms of stress - trembling hands, lips or legs, excessive perspiration, hot flashes, shortness of breath, impaired concentration and memory – directly exacerbate the ability to perform their work what becomes a source of additional stress. Physical strain plays an inevitable role in the musicians’ work. Sometimes, introducing ergonomic improvements to the workplace protects workers against work-related pain, yet, considering musicians, it is usually impossible as this physical workload is what constitutes playing the instrument [2]. Even providing they might be changed, it could influence the technique and affect the quality of performance [1]. Thus, although musicians experience PRMD very often, its prevalence cannot be decreased with simple reducing the physical demands of their work. Moreover, musicians need to organize their work and learning process, remember and recall the notes (especially difficult under pressure), concentrate for long hours of rehearsals and concerts [8]. They are also constantly exposed to assessment, need to manage their emotions and deal with stress effectively [3]. They usually start their playing careers early in their childhood and until they commence their professional careers, they could have already played for years and starting that early, they learn the necessity to practice systematically, sometimes devoting their private lives to music [9]. Then, the potential need to change the job results in the lack of alternatives [9, 10]. Thus, also the risk of injury that could exacerbate their ability to play or even terminate their careers can be a source of stress.
3Playing-Related Musculoskeletal Problems
Playing-Related Musculoskeletal Disorders (PRMD) refer to ‘any pain, weakness, numbness, tingling or other symptoms that interfere with the ability to play your instrument at the level you are accustomed’ [11, p.93]. Musculoskeletal symptoms range from minor pain, burning or muscle tiredness up to serious disorders and chronic, severe pain debilitating the capability to play [10–12]. Such health problems are precariously common among musicians. Kaufman-Cohen and Ratzon [4] argue that the majority of musicians experience musculoskeletal problems at least once in their lives. Indeed, earlier studies indicate that musculoskeletal disorders occur among 38 up to 89% of musicians [4, 12–15].
Impact of physical demands on the development of musculoskeletal diseases has already been extensively investigated [16, 17]. Playing instruments involves repeating the same movements, bearing the instrument weight for long hours, remaining in asymmetrical body postures, dealing with technical demands of an instrument or a particular piece of music causing specific stress to hands and fingers [6, 7]. A constant spine pressure typical for musician’s body postures can be to five times higher than that of an average person [2]. Such postures are often forced and non-physiologic and they result in overloads of lumbar and cervical spine, possibly leading to degenerative-productive changes and severe pain [2].
However, musculoskeletal disorders can also result from or be exacerbated due to psychosocial burden and stress, what has already been documented by a lot of research conducted on various occupational groups [18–21]. Notably, musicians themselves consider their work as demanding and stressful. For instance, in a Danish study, the authors compared the perception of the work demands between musicians and the general work force in Denmark, using a database developed by means of the Copenhagen Psychosocial Questionnaire [3]. It occurred, that both female and male musicians assessed their own work as more emotionally and cognitively demanding than other workers assessed theirs[3].
4Psychosocial aspects, stress and musculoskeletal problems – theory
Extant literature provides a few explanatory models that justify searching for the relationships between psychosocial aspects of work or stress and musculoskeletal problems.
The model frequently referred to in studies on psychosocial determinants of musculoskeletal problems is Demand-Control model by Karasek. The author stated that high work demands combined with low decision possibility lead to negative health outcomes affecting either physical or psychological aspects [22]. The model has been recognized as explanatory as regards work-related musculoskeletal pain – in their systematic reviews, Bongers, Ijmker, van den Heuvel and Blatter [17] and Bongers, Kremer and ter Laak [23] revealed that most of the analyzed high-quality studies confirmed the relationship between high work demands and musculoskeletal disorders (as regards those concerning upper extremities). Also low control and low support influenced the occurrence of pain, however, those relationships were weaker [23]. Cross-sectional character of the analyzed studies constituted a limitation of the conclusions. However, in their second review [17] those authors reviewed twenty-four longitudinal researches and concluded that although there was an association between musculoskeletal pain and high work demands and/or low control, the effects were rather small. Some of the analyzed studies indicated work demands and some indicated decision latitude as a stronger predictor of neck and upper limb problems [17]. Such conclusions correspond to the findings of De Lange et al. [24] – basing on 19 studies they found only few researches to confirm the impact of that model variables on the health-related issues (stress, burnout, job/life satisfaction, physical illness). Bongers et al. [17] explain such results with the fact that the categories of demands-control-support variables studied so far are too broad and linked with each other what makes it difficult to verify their impact on health.
In the literature there are also a few other explanatory models for the relationship between psychosocial aspects or stress and musculoskeletal problems. Siegrist’s model indicates the discrepancy between the effort put in the work and the reward achieved as its result as a cause of work-related stress [25]. However, in their review, Koch, Schablon, Latza & Nienhaus [26] identified studies linking effort-reward imbalance model with musculoskeletal pain and provided only moderate support for the hypothesized relation between the studied variables. Armstrong et al. [27], in turn, assumed that musculoskeletal pain occurs when high work demands strain the organism causing physical or mental load what leads to certain physiological or psychological responses. When the strain exceeds the person’s capacity, then muscles, nerves or tendons may get injured what results in pain [27]. This model does not directly refer to psychosocial aspects of work - the author mentions them among external aspects of work constituting the worker’s exposure and suggests further research [27]. Yet, in her model, Roman-Liu [28] assumes that direct impact occurs when a person’s musculoskeletal system is exposed to physical demands of his or her work or psychosocial demands. Indirectly, the demands (doses) additionally burden the individual’s mental system what increases the musculoskeletal strain [28]. A similar distinction to direct and indirect impact of psychosocial aspects occurred in a model developed by Bongers et al. [16, 17, 23]. Unlike the previous models, this was designed on the basis of the systematic literature reviews including researches concerning this issue. On such grounds, those authors assumed that psychosocial aspects of work affect musculoskeletal pain - due to their impact on the body posture, or physical effort required to perform a task and on the other hand, due to a direct influence of work-related stress and physiological reactions being its result [23]. Moreover, due to stress, an individual may perceive his or her working environment (including its psychosocial aspects) and already experienced musculoskeletal as more troublesome and threatening [23]. Another model, called biopsychosocial, assumes that increased muscle tension or endocrine reactions may result from physical (biomechanical strain) and psychological stressors, considering not only a possible overload but also underload [29]. Workstyle construct developed by Feuerstein, Huang and Pransky [30], in turn, combines beliefs, behaviors and physiological reactions that emerge as a response to work demands – considered as psychosocial and physical risks. What distinguishes that model is the assumption that attempts to cope with high work demands may occur additionally demanding-an individual given too short deadline, works even longer, takes breaks less frequently and put more effort to perform the task [31]. Such approach may be of particular significance to understand the origins of musculoskeletal pain in musicians because playing and performing despite health problems is particularly common among them [13]. Each of these models could be used as a theoretical background also in the studies involving musicians. However, so far researchers have paid only little attention to the issue of the contribution of psychosocial aspects in the development of musculoskeletal disorders among musicians. Therefore, the following review was aimed at identifying research undertaking the issue of the relationships between psychosocial aspects of work, stress and musculoskeletal problems among musicians and summing up the achieved results and theoretical explanations. The primary goal was to assess the contribution of psychosocial aspects in the development of musculoskeletal problems among the representatives of this occupation.
5Method
A systematic review was undertaken to identify studies linking psychosocial aspects of work with the risk of musculoskeletal problems among musicians. The author explored EBSCO, Web of Science, PubMed and Scopus databases to find papers written in English and with no time limitations (additional criterion available only in EBSCO: articles published in peer-reviewed journals). Searched keywords included: musculoskeletal/pain/strain/upper extremity/shoulder AND psychosocial/stress/workplace AND musician in different combinations. The searched items were supposed to occur in abstracts (EBSCO, Scopus), in a topic (Web of Science, there is no option to search the abstracts) or in a title or abstract (PubMed). The exact duplicates were excluded from further analyses. Then the abstracts of the articles were screened in search for papers describing:
1. original quantitative studies;
2. studies involving psychosocial aspects of work/work-related stress or musculoskeletal problems,
3. studies on musicians.
Then, the full content of the papers was analyzed in search for articles describing studies linking both, any psychosocial aspects of work or stress with any musculoskeletal problems. All studies that revolved around the topic were included, without restrictions to any theoretical background, neither as regards psychosocial issues nor musculoskeletal problems. This was due to a small total amount of research undertaking that issue among musicians.
6Results
The exploration of the databases resulted in 361 records and having removed the exact duplicates and screened the abstracts, there were 39 records available for further reading (Fig. 1).
Full texts analysis resulted in nine papers linking psychosocial aspects or stress with musculoskeletal disorders among musicians. The results and conclusions are presented below.
All but one analyzed studies were cross-sectional. With such searching terms no longitudinal studies linking psychosocial aspects with musculoskeletal problems were found. The studies included from 20 to 281 musicians- professional musicians or university or high school music students. Usually the studies involved classical musicians, however one research aimed to diversify the sample and included also jazz, rock and other genres musicians [35]. All studies focused on instrumentalists as the most vulnerable to musculoskeletal problems, neither vocalists nor music theory specialists were included. The studies were conducted in Canada, Australia, Sweden, Brazil, the United Kingdom or Israel. All but one paper [11] provided information on the instruments played by the respondents: one study involved only flautists [32], in other studies string players usually comprised the biggest studied group (from 18 to 66% of the studied sample), followed by woodwind and brass players. Keyboard or percussion players were less common. This resulted from the similar distribution of players in music universities as well as in orchestras. Mean age of the studied musicians equaled from 23 to 44 years old. Three papers did not provide response rates [4, 32, 37], the other response rates equaled from 45 to 97%.
The only theoretical model explaining the influence of psychosocial aspects on musculoskeletal problems that researchers referred to was Karasek and Theorell including job demands, control and social control and it occurred in four out of nine analyzed studies [4, 12, 34, 37]. The analyzed studies investigated also generic stress or work and study stress [11, 36] as well as musicians-specific playing-related factors distinguished by the authors themselves such as travel strains, rivalry, lack of practice time, lack of creative satisfaction, job insecurity, performance anxiety, work content [12, 33, 35]. The variables were measured with a variety of methods including Karasek and Theorell questionnaire, Visual Analogue Scale for stress, Generic Job Stress Questionnaire or questionnaires developed by the authors, adapted to musicians’ work demands.
Musculoskeletal problems were generally referred to as pain, discomfort, tingling, swelling, weakness, loss of control, pins or needles or numbness in different body areas. The researchers usually asked for the PRMD occurrence within the 12 months preceding the study. Musculoskeletal problems were mainly measured with the use of Standardized Nordic Musculoskeletal Questionnaire, and with Visual Analogue Scale for pain, McGill Pain Questionnaire and sometimes with the questionnaires developed by the authors.
From 68 to 95% of the studied musicians suffered from pain or discomfort. The most affected body areas included upper back (41–42% of the studied musicians suffered from pain within this area), neck (13–56%), wrists, hands or fingers (8–65%), shoulders (7–65%), lumbar spine (7–56%) and thoracic spine (7–11%).
The analyzed studies linked psychosocial aspects with musculoskeletal problems in three ways – showing proportions of people indicating particular causes of pain, indicating correlations between these variables or performing regression analysis showing psychosocial predictors of musculoskeletal pain. Considering the perceived psychosocial causes of PRMD, the studied flautists (N = 20) indicated long hours spent at work (65%), performance anxiety (45%), travels (25%) or inadequate equipment (15–20%) [32]. Music students (N = 227) considered musical activity (49% males and 53% females) but also stress as the reasons for their pain (21% males and 47% females) [34]. Similarly, 59% of the studied musicians considered long hours spent at work and 35% of them stress as the reasons of their playing-related pain [35]. Also in a study by Kaneko et al. [36] 26% of the studied musicians indicated stress as the source of their musculoskeletal problems.
Considering different work-related variables investigated in the analyzed studies, pain correlated significantly with work content (r = –0.21, p < 0.01) and influence at work (r = –0.15, p < 0.05) [33], stress affecting performance quality (only p value provided, p = 0.01) [36] and psychosocial job stressors (job demands, control and social support counted together: r = 0.35, p < 0.01) [4].
Regression analyses revealed that work and study stress as well as generic life stress predicted the first incidence (OR = 1.66, 95% CI 1.15 to 2.40 and OR = 1.51, 95% CI 1.06 to 2.15 respectively) as well as recurrent PRMDs (OR = 1.41, 95% CI 1.10 to 1.81 and OR = 1.25, 95% CI 1.00 to 1.58 respectively) [11]. Also performance anxiety occurred a significant predictor, and it increased the probability of the recurrent PRMD only by 9% (95% CI 1.00 to 1.18) [11]. In another study playing-related stress resulting from performance anxiety, short deadlines, rivalry, lack of artistic satisfaction, job insecurity or touring and working late at night (counted together) correlated with pain or symptoms ever (β= 0.19, p = 0.04) and within the 12 months preceding the study (β= 0.20, p = 0.05). Also stress interaction with lack of warm-ups or breaks correlated significantly with pain severity (β= 0.27, p = 0.01) [35]. Only one study showed significant correlations in regression models for job demands, control and social support – low control correlated with neck pain among men (p < 0.05), low support related with neck pain among women (p < 0.05) and knee pain among men (p < 0.05), higher demands correlated with more body areas affected with musculoskeletal problems among men (p < 0.03, p values provided as cited by the authors) [34]. Two studies revealed no significant psychosocial predictors of pain [4, 12].
7Discussion
The above systematic review shows that there are only a few researches undertaking the issue of relationships between psychosocial work aspects, stress and musculoskeletal disorders among musicians. The variety of definitions and methods used to assess psychosocial aspects does not allow for direct comparison of the results. The variable consistently occurring as a significant correlate or predictor of pain was stress – either playing-related or general life stress. Yet, considering particular psychosocial aspects of work, mainly general work demands-control stressors correlated with or predicted PRMD. More diverse and job-specific causes of pain occurred when researchers directly asked musicians about their perception of reasons for pain (for example, they mentioned long hours at work, performance anxiety, inadequate equipment) but no further analyses were performed to confirm that result. Moreover, Demand-Control model was the only theoretical approach considered in the studies. The literature review of studies referring to the impact of high demands and low control on musculoskeletal problems among other occupational groups revealed that relationships between those variables were of weak to moderate strength and some studies indicated control and some - demands as more related to such health problems [23]. The authors of that review also pointed that demand-control categories were too broad to determine their impact on health precisely. The more, those categories might be insufficiently specific as regards musicians’ work. However, there are some studies identifying various other, far more precise, sources of stress in musicians’ work. In a Danish study [3] on 342 orchestral musicians, the researchers distinguished various psychosocial aspects of musicians’ work and identified those that were perceived as stressful. The authors found that the higher work demands (emotional demands or the need to manage emotions), worse work organization and its content (such as less possibilities to develop), poorer relationships and leadership (smaller sense of community) increased the intensity of all types of stress. There, stress was rated with the use of emotional, cognitive and somatic symptoms of stress providing comprehensive picture of psychosocial work aspects-stress relationships. Another study, on American orchestra musicians, revealed that musicians experienced two types of work-related stress resulting from different psychosocial demands – firstly, psychological distress resulting from lack of artistic integrity and difficult tasks undertaken at work and secondly, boredom stress resulting from “underload”, social tension but also lack of artistic integrity [5]. Thus, the future research on the impact of psychosocial risks should include the moderating power of stress, because the occurrence of psychosocial work demand does not necessarily mean that a person meeting such demand feels stressed or will experience any negative health consequences as its result. Defining psychosocial aspects as well as distinguishing those constituting sources of stress is of crucial importance. Unluckily, the categories of psychosocial aspects of work used in the above studies have not been used to investigate the relations between psychosocial work demands and musculoskeletal problems.
8Conclusion
The above considerations lead to a conclusion that musculoskeletal problems may result from a variety of work-related reasons, including psychosocial aspects of work and stress and the exposition of musicians to high physical and psychosocial demands makes them vulnerable to experience of pain. In the above paper, the author discussed psychosocial aspects of musicians’ work and their relations with musculoskeletal disorders. It occurred that there are only a few studies that have undertaken the issue of psychosocial risk factors for musculoskeletal problems among musicians.
The extant literature provides evidence that musicians suffer from work-related musculoskeletal problems, they experience high work demands involving physical and mental strain and those work demands result in stress. However, the research including psychosocial risks of musculoskeletal pain among musicians is still scarce and provides inconsistent results. Usually high psychosocial work aspects co-occurred with musculoskeletal problems, yet, they were not always identified as risk factors. What still needs to be investigated is the extent to which physical and psychosocial work demands contribute to the development of musculoskeletal problems. Especially longitudinal research could show what role they play in rehabilitation process. Such knowledge would be of value to design preventive programmes, particularly considering that large amount of physical demands can be hardly reduced as regards musicians’ work, for instance repetitive movements, prolonged remaining in one body posture, carrying the instrument could be hard or impossible tochange.
Moreover, further research should define psychosocial aspects of work more precisely, focusing on those that directly apply to musicians’ working reality. Referring to such broad categories as demand-control poses a question of their suitability for practical implications. Research by Parasuraman and Purohit [5] or Holst et al. [3] provided such work demands typically occurring in musicians’ work such as the need to manage emotions (hide stress symptoms but stay sensitive to music) [3], or sense of lack of artistic integrity [5]. The categories distinguished in those studies may serve as a starting point for further investigation of possible sources of playing-related stress. Furthermore, the extant research leaves much room for doubts whether musicians perceive their work as physically and psychologically demanding and stressful. It is possible that musicians perceive some work demands as an inevitable part of their work and because music is often assumed to be their passion, they do not find them stressful nor burdensome. Therefore, the perception of stress could mediate the relationship between work demands and musculoskeletal problems. Similarly, mental fatigue resulting from performing cognitively demanding tasks (such as the need for prolonged concentration or vigilance, typical for performing musicians) has already been confirmed to deteriorate the physical capacity and endurance [38]. Future studies should include such variable to verify whether high work demands themselves or the perception of them decide about negative health outcomes.
Previous literature offers a wide range of theoretical models explaining the relationships between psychosocial aspects of work or stress and health, or particularly – musculoskeletal problems. However, the analyzed studies referred only to Karasek’s model, still providing inconsistent results. Thus, future research might use other theoretical models as background to their study. What could particularly refer to musicians is the role of household demands [29] that could additionally burden their musculoskeletal and mental systems, especially given their non-stable working hours. Also the assumption that attempts to deal with high work demands may also constitute another source of strain may apply to musician’s situation. Literature provides evidence that musicians tend to work without breaks or despite feeling pain [13]. Moreover, the variety of definitions employed to explain psychosocial aspects of work in the analyzed studies and models do not allow for simple comparisons and unambiguous conclusions. The categories used to describe psychosocial issues seem to be too broad and not specific enough [31] to capture the unique characteristics of sources of strain at musicians’ work. For instance, increasing ‘control’ (as in demands-control model) as a mean to reduce e.g. orchestral musicians’ stress seems unrealistic – there is hardly a chance for musicians to decide about the repertoire, technique, interpretation, working hours or even co-workers. Moreover, following Bongers’s et al. suggestion, there is a need to investigate the interactions of the physical and psychosocial risks for musculoskeletal problems and the role of psychosocial aspects of work in maintenance and deterioration of musculoskeletal symptoms since those aspects have not been included neither in theoretical models nor empirical researches yet [17]. In musicians it may be of particular significance because even minor problems with health, let alone long-lasting health problems or rehabilitation process, may definitely terminate their careers. Above all, some of the models have not been empirically verified yet, so the relations are not clear even as regards general working population. What is also worth considering is the role of capacity (as mentioned by Armstrong et al. [27]) or coping with stress and demands in particular. Researchers undertaking the issue of musicians’ work demands underline the need to include coping into models explaining the reasons for musicians’ health problems [3, 5]. Previous research considering psychosocial risks of musculoskeletal problems did not include coping strategies and abilities. Situation-adjusted and effective coping repertoire can reduce stress and as a result, reduce the negative impact of work demands on health outcomes. Thus, coping strategies should also be included in the future studies undertaking the issue. Such knowledge would constitute a value for health specialists to understand the specific strain put on musicians and to find a suitable way of treatment that would not exclude musicians from playing. It would also sensitize musicians to the possible consequences of struggling with specific needs and demands of their work because as the previous analyses revealed they tend to avoid consulting physicians, ignore symptoms and play despite the ailments, or neglect the role of breaks and rest while practicing [13].
The above review has its limitation. All the terms were searched in English and also the analyzed papers were expected to be written in English. This was due to the assumption that English is the most universal language and such search would result in the greatest amount of records. Nevertheless, this might have resulted in omitting some valuable results published in other languages.
Summing up, the previous studies confirm the multifactorial origin of musculoskeletal disorders, and only a few researchers have undertaken this issue and investigated it among musicians. Such result is surprising considering the high prevalence rate of such health problems in this occupational group. Identifying those psychosocial work demands that increase the risk of PRMD – either directly or indirectly via stress mechanisms – may occur crucial to protect musicians’ health. It seems that correcting the psychosocial work context or developing the skills to cope with it would facilitate musicians’ workinglife.
Conflict of interest
None to declare.
Acknowledgments
Prepared within a statutory project of the Nofer Institute of Occupational Medicine, “Development of a tool to study psychosocial risks in musicians”, project no. IMP 21.8.
References
[1] | Branfonbrener AG . Performing arts medicine. Music Educ (1991) ;77: (5):37–41. |
[2] | Janiszewski M , Gałuszka G , Ochwanowska A , Gaciarz A , Hak A , Ochwanowski P , et al . Biomechanical analysis of dynamics and statics of the moving arm in musical instrumentalists. Med Pr (2005) ;56: (1):25–33. |
[3] | Holst GJ , Paarup HM , Baelum J . A cross-sectional study of psychosocial work environment and stress in the Danish symphony orchestras. Int Arch Occup Environ Health (2012) ;85: (6):639–49. |
[4] | Kaufman-Cohen Y , Ratzon NZ . Correlation between risk factors and musculoskeletal disorders among classical musicians. Occup Med (2011) ;61: (2):90–5. |
[5] | Parasuraman S , Purohit YS . Distress and boredom among orchestra musicians: the two faces of stress. J Occup Health Psychol (2000) ;5: (1):74–83. |
[6] | Chan C , Driscoll T , Ackermann B . Exercise DVD effect on musculoskeletal disorders in professional orchestral musicians. Occup Med (2014) ;64: (1):23–30. |
[7] | Price K , Watson AHD . Postural problems of the left shoulder in an orchestral trombonist. Work A J Prev Assess Rehabil (2011) ;40: (3):317–24. |
[8] | Ministerstwo Gospodarki, Polityki Społecznej i Pracy. Przewodnik po zawodach. 2003; |
[9] | Stern H . The musician’s perspective. In: Winspur I , Wynn Parry CB , editors. The Musician’s Hand: A Clinical Guide. London: Martin Dunitz Ltd; (1998) . |
[10] | Paarup HM , Baelum J , Holm JW , Manniche C , Wedderkopp N . Prevalence and consequences of musculoskeletal symptoms in symphony orchestra musicians vary by gender: A cross-sectional study. BMC Musculoskeletal Disorders (2011) ;12: (1):223. |
[11] | Zaza C , Farewell VT . Musicians’ playing-related musculoskeletal disorders: An examination of risk factors. Am J Ind Med (1997) ;32: (3):292–300. |
[12] | Leaver R , Harris EC , Palmer KT . Musculoskeletal pain in elite professional musicians from British symphony orchestras. Occup Med (2011) ;61: (8):549–55. |
[13] | Bruno S , Lorusso A , L’Abbate N . Playing-related disabling musculoskeletal disorders in young and adult classical piano students. Int Arch Occup Environ Health (2008) ;81: (7):855–60. |
[14] | Paarup HM , Baelum J , Manniche C , Holm JW , Wedderkopp N . Occurrence and co-existence of localized musculoskeletal symptoms and findings in work-attending orchestra musicians - an exploratory cross-sectional study. BMC Research Notes (2012) ;5: (1):541. |
[15] | Kok LM , Vlieland TPMV , Fiocco M , Nelissen RGHH . A comparative study on the prevalence of musculoskeletal complaints among musicians and non-musicians. BMC Musculoskelet Disord (2013) ;14: (1):9. |
[16] | Bongers PM , De Winter CR , Kompier MAJ , Hildebrandt VH . Psychosocial factors at work and musculoskeletal disease. Scandinavian Journal of Work, Environment and Health (1993) ;19: , 297–312. |
[17] | Bongers PM , Ijmker S , Van Den Heuvel S , Blatter BM . Epidemiology of work related neck and upper limb problems: Psychosocial and personal risk factors (Part I) and effective interventions from a bio behavioural perspective (Part II). Journal of Occupational Rehabilitation (2006) ;16: (3):272–95. |
[18] | Chen WQ , Yu IT , Wong TW . Impact of occupational stress and other psychosocial factors on musculoskeletal pain among Chinese offshore oil installation workers. Occup Environ Med (2005) ;62: (4):251–6. |
[19] | Ekpenyong CE , Nyebuk DE , Ekpe AO . Associations between academic stressors, reaction to stress, coping strategies and musculoskeletal disorders among college students. Ethiopian J Heal Sci (2013) ;23: (2):98–112. |
[20] | Larsman P , Kadefors R , Sandsjö L . Psychosocial work conditions, perceived stress, perceived muscular tension, and neck/shoulder symptoms among medical secretaries. Int Arch Occup Environ Health (2013) ;86: (1):57–63. |
[21] | Van den Heuvel SG , van der Beek AJ , Blatter BM , Hoogendoorn WE , Bongers PM . Psychosocial work characteristics in relation to neck and upper limb symptoms. Pain (2005) ;114: (1-2):47–53. |
[22] | Karasek RRA . Job demands, job decision latitude, and mental strain: Implications for job redesign. Adm Sci Q (1979) ;24: (2):285–308 . |
[23] | Bongers PM , Kremer AM , ter Laak J . Are psychosocial factors, risk factors for symptoms and signs of the shoulder, elbow, or hand/wrist?: A review of the epidemiological literature. Am J Ind Med (2002) ;41: (5):315–42. |
[24] | De Lange AH , Taris TW , Kompier MAJ , Houtman ILD , Bongers PM . “The very best of the millennium”: Longitudinal research and the demand-control-(support) model. J Occup Health Psychol (2003) ;8: (4):282–305. |
[25] | Siegrist J . Adverse health effects of high-effort/low-reward conditions. J Occup Health Psychol (1996) ;1: (1):27–41. |
[26] | Koch P , Schablon A , Latza U , Nienhaus A . Musculoskeletal pain and effort-reward imbalance–a systematic review. BMC Public Health (2014) ;14: , 37. |
[27] | Armstrong TJ , Buckle P , Fine JF , Hagberg M , Jonsson B , Kilbom A , et al . A conceptual model for work-related neck and upper-limb musculoskeletal disorders. Scandinavian Journal of Work, Environment and Health (1993) ;19: , 73–84. |
[28] | Roman-Liu D . External load and the reaction of the musculoskeletal system - A conceptual model of the interaction. Int J Ind Ergon (2013) ;43: (4):356–62. |
[29] | Lundberg U , Forsman M , Zachau G , Eklöf M , Palmerud G , Melin B , et al . Effects of experimentally induced mental and physical stress on motor unit recruitment in the trapezius muscle. Work & Stress (2002) ;16: (2):166–78. |
[30] | Feuerstein M , Huang GD , Pransky G . Workstyle and work-related upper extremity disorders. Psychosoc Factors Pain New York Guilford (1999) )175–92. |
[31] | Huang GD , Feuerstein M , Sauter SL . Occupational stress and work-related upper extremity disorders: Concepts and models. American Journal of Industrial Medicine (2002) ;298–314. |
[32] | Ackermann BJ , Kenny DT , Fortune J . Incidence of injury and attitudes to injury management in skilled flute players. Work A J Prev Assess Rehabil (2011) ;255–9. |
[33] | Johansson YL , Theorell T . Satisfaction with work task quality correlates with employee health a study of 12 professional orchestras. Med Probl Perform Artists (2003) ;18: (4):141–9. |
[34] | Zetterberg C , Backlund H , Karlsson J , Werner H , Olsson L . Musculoskeletal problems among male and female music students. Med Probl Perform Artists (1998) ;13: , 160–6. |
[35] | Davies J , Mangion S . Predictors of pain and other musculoskeletal symptoms among professional instrumental musicians: Elucidating specific effects. Med Probl Perform Artists (2002) ;17: (4):155–68. |
[36] | Kaneko Y , Lianza S , Dawson WJ . Pain as an incapacitating factor in symphony orchestra musicians in São Paulo, Brazil. Med Probl Perform Artists (2005) ;20: (4):168–74. |
[37] | Pereira EF , Kothe F , Bleyer FT , Teixeira CS . Work-related stress and musculoskeletal complaints of orchestra musicians. Rev Dor (2014) ;15: (2):112–6. |
[38] | Marcora SM , Staiano W , Manning V . Mental fatigue impairs physical performance in humans. J Appl Phys (2009) ;106: (3):857–64. |
Figures and Tables
Fig.1
Databases search results.
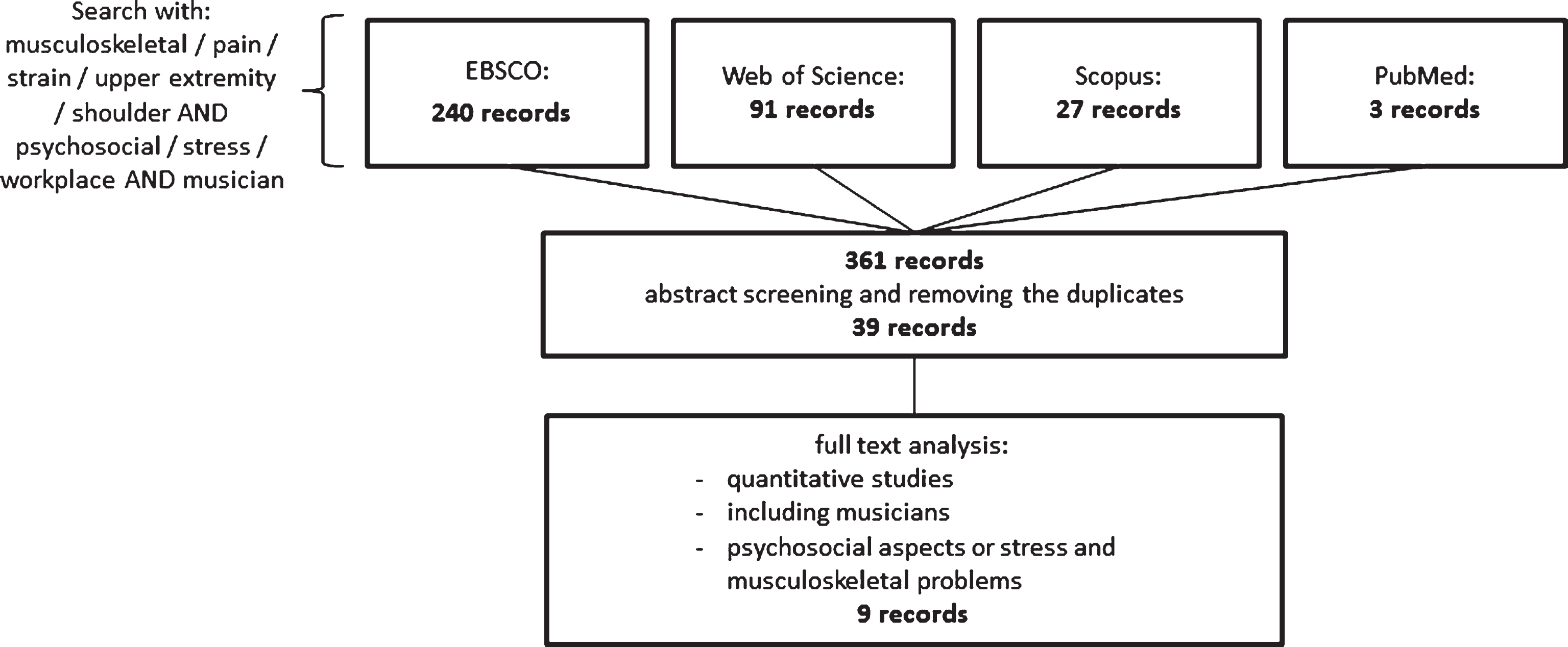
Table 1
Characteristics of the analyzed studies including study and sample characteristics, response rates, definitions and measurement methods for psychosocial aspects and musculoskeletal pain and analyses used to link these two types of variables
| Paper | Study design | Country | Sample characteristics | Instruments played | Response Rate | Psychosocial aspects (method) | Musculoskeletal aspects (method) | Analysis linking psychosocial work demands with musculoskeletal pain |
| Zaza &Farewell, 1997 [11] | case-control | Canada | 281 professional classical musicians and music university students (110 cases and 171 controls) (age M = 31, no SD provided; 45% males) | no information | 67% | questionnaire by Bartel &Thompson to study performance anxiety, 5-point Likert scale developed by the authors to study stress | PRMD defined as having any “playing-related musculoskeletal problem (i.e., any pain, weakness, numbness, tingling, or other symptoms that interfere with [the] ability to play [the] instrument at the level [one] is accustomed to)”, [11,p. 293] (one ‘yes/no’ self-reported question: “Currently, do you have a playing-related musculoskeletal problem ... ”) | logistic regression |
| Ackermann, Kenny, &Fortune, 2011 [32] | cross-sectional | Australia | 20 flute students (age M = 23+/–4; 15% males) | 100% flute | no information | perceived reasons of the injury (questionnaire developed by the authors) | location and intensity of any PRMDs experiences (health questionnaire about PRMDs among flautists developed by the authors) | frequencies |
| Johansson &Theorell, 2003 [33] | cross-sectional | Sweden | 250 professional orchestral musicians (age M = 39, no SD provided; 62% males) | 58% string, 19% brass, 18% woodwind and 4% other | 78% | quality of work: work content, management’s quality, trust in orchestra’s potential; psychosocial factors: influence, social support (questionnaire developed by the authors) | musculoskeletal symptoms and their location within the year preceding the study (questionnaire developed by the authors) | correlations, linear regression |
| Zetterberg, Backlund, Karlsson, Werner&Olsson, 1998 [34] | cross-sectional | Sweden | 227 music university students (age M females 24+/–3, males 24+/–4; 49% males) | 18% string, 25% woodwind and brass, 6% guitar, 22% keyboard, 4% percussion | 97% | stress resulting from job demands, control and social support (questionnaire by Karasek and Theorell) | musculoskeletal complaints (pain, discomfort, tingling or numbness) and their location over four weeks or 12 months preceding the study, type of problem and its relation to performing (Nordic Musculoskeletal Questionnaire, the von Korff pain and disability questionnaire) | frequencies, linear and logistic regression |
| Davies &Mangion, 2002 [35] | cross-sectional | Australia | 240 professional orchestral and non-orchestral instrumentalists (age M = 37+/–11; 56% males) | 42% strings, 18% wind, 16% brass, 7% percussion, 12% keyboard, 5% guitar | 45% | workplace factors including stress caused by playing-related stressors (performance anxiety, lack of practice time, rivalry, lack of creative satisfaction, insufficient work, job insecurity, touring and late night work) (one-question scale developed by the authors) | pain or symptoms (“pins or needles, swelling, weakness, loss of control”, p. 156) ever, pain or symptoms in the last 12 months, severity of pain (interference with the playing ability, persistence, causing non-playing activities difficult) (questionnaire developed by the authors) | frequencies and linear regression |
| Kaneko, Lianza &Dawson, 2005 [36] | cross-sectional | Brazil | 241 professional orchestral musicians, (age M = 32+/–11; 70% males) | 61% strings, 17% woodwinds, 2% brass, 8% percussion | 56% | generic stress (Visual Analogue Scale for stress) | pain - location and intensity (Visual Analagoue Scale for pain and McGill Pain Questionnaire) | Spearman’s rank correlations; logistics regression |
| Pereira, Kothe, Bleyer &Teixeira, 2014 [37] | cross-sectional | Brazil | 22 professional orchestral musicians (age M = 27+/–11; 77% males | strings, woods and metals instrumentalists (no information about the percentage of musicians playing each group of instruments) | 76% (not provided by the authors) | stress resulting from job demands, control and social support (Job Stress Scale) | musculoskeletal complaints (pain, discomfort, tingling or numbness) and their location in the seven days preceding the study (Standardized Nordic Questionnaire) | frequencies |
| Leaver, Harris &Palmer, 2011 [12] | cross-sectional | United Kingdom | 243 professional orchestral musicians (age M = 44+/–7; 56% males) | 62% strings, 36% wind, 16% brass and 7% other | 51% | stress resulting from job demands, control and social support; performance anxiety, job insecurity, (questionnaire ‘according to the Karasek model’ no further information) | musculoskeletal complaints (pain, discomfort, tingling or numbness) and their location over four weeks or 12 months preceding the study, disabling pain within 12 months preceding the study (Standardized Nordic Questionnaire) | logistic regression |
| Kaufman-Cohen &Ratzon, 2011 [4] | cross-sectional | Israel | 59 professional orchestral musicians (age M = 43+/–11; 49% males) | 66% string and 20% wind | no information | psychosocial job stressors: job control, job demands, workload (Generic Job Stress Questionnaire) | musculoskeletal complaints (pain, discomfort, tingling or numbness) and their location over four weeks or 12 months preceding the study (Standardized Nordic Questionnaire, the addition on upper extremities developed by the authors) | Pearson’s correlation, linear regression |


