
Efficacy of occupational rehabilitation in return to work for back pain: A systematic literature review
Abstract
BACKGROUND:
Currently, there is no standard procedure for a return to work (RTW) rehabilitation program used by practitioners.
OBJECTIVE:
The aim is to investigate the efficacy of occupational rehabilitation programs for workers with back pain.
METHODS:
Two independent reviewers screened abstracts and full-text articles in a systematic literature search in three databases conducted in 2023. Subsequently, they extracted data according to the PRISMA Statement.
RESULTS:
Among the 4,010 articles retrieved, 20 met the inclusion criteria. Data from accepted studies were abstracted into tables relating to the RTW, improvement of pain intensity, quality of life (QOL), and degree of disability in persons with back pain. The risk of bias was assessed using the (SIGN)-criteria. Significant improvements in RTW were shown by a workplace intervention with a physical approach and a multidisciplinary intervention but with a wide range of effect sizes. Five studies showed significant improvements in pain intensity and QOL, six studies observed significant improvements in disability.
CONCLUSION:
The studies that stated positive effects on work-related data differed between intervention programs and traditional care. A combination of activity, maintenance therapy, stretching, and manual therapy showed promising results in improving RTW. In addition, the relationship and mediation between employer/workplace and employee seems to be an important aspect of RTW. However, pain intensity, disability, and QOL were enhanced with interventions that included a high proportion of physical activity. However, the intervention programs differed widely, leading to the assumption that the treatment effect of the intervention programs is not established, yet.
1Introduction
Chronic and/or acute back pain has become one of the most common orthopedic complaints in industrial countries. At least 80–90% of the people in the western hemisphere suffer from acute back pain [1]. According to a Systematic Review from 2019, 15% of US citizens claimed to have neck pain in the past three months, as well as 33.9% suffered from back pain [2]. An Austrian study from 2016 reported dramatically increased numbers of back pain [3]. Most of the time back pain lasts for only 4–6 weeks; however, it seems difficult to recover fully from chronic back pain [4, 5]. In 2008, Germany’s healthcare spent about eight billion Euros addressing people with back pain [6] due to the use of healthcare, disability pensions, and sickness absence [7]. This shows the immense difficulties in the employee’s ability to work and demonstrates the demand for interventional therapy to insure the job market as well as to prevent a lack of sickness absence.
This systematic literature review informs rehabilitation concerning return to work (RTW) ability. When addressing rehabilitation, we focused on occupational rehabilitation/therapy which specializes in work-related strategies. In Germany, occupational rehabilitation is established as an insurance-supported rehabilitation program. Moreover, occupational rehabilitation incorporated a multidisciplinary approach toward rehabilitation curing work-related diseases. This supports the suggestion of Pransky et al., by implementing an interdisciplinary approach for improving RTW [8].
To improve the ability to work and enhance the RTW capacity, the current medical advice for people with chronic and/or acute back pain is a multidisciplinary rehabilitation next to a bio-psychological approach [7, 9]. There are two different medical procedures to ensure RTW abilities [10]. According to the “supported employments” approach –a term used in the health care system for teaching work-related basic skills for job placement [11] –people need to get accustomed to an immediate integration within their profession, and therefore, a work-related rehabilitation program. However, work-related –occupational –rehabilitation appears to be internationally different. In Germany, work-related medical rehabilitation (Work MR) is a multimodal interdisciplinary approach that aims to reduce a skill mismatch to increase occupational participation for disabled employees. In general, this program refers to people with long-term unemployment, inability to work, low work expectancy, and/or socio-medically necessary change of work. Work MR appears to be an occupational program [12], which refers to the occupational situation in terms of stress, necessary psychological and physiological abilities, and qualifications. Furthermore, patients will get RTW training oriented to their specific work barriers. Consequently, they are going to be trained at their place of work to get used to the general work requirement, which has shown to have a significantly higher chance of occupational reintegration [13–16]. These clinical diagnostics lead to an intervention of social and occupational counseling; however, no specific profession is appointed to oversee treatment plans. One such product of this ambiguity is evident as there appears to be an educational program in the US for occupational therapists accessing different treatment options. This profession is not internationally standardized, thus creating different treatment approaches to cure work disabilities. Ambulant-treated occupational rehabilitation is leading to help people depending on their place of residence or educational possibilities in cooperation with employers to get constant occupational (re-)integration at their workplace [17]. A Danish study investigated occupational therapy (OT) which mostly referred to self-perception in everyday living and how the participants are satisfied with these activities. A Finnish randomized controlled trial (RCT) tested an occupational health care system on people with an elevated risk of sickness absence [18] where they used occupational physicians and nurses to propose a health program for the participants. This seems unlike the German system where there is no commonly known profession of an occupational physician. A comparable approach to the German Work MR program, called MBOR, is the Norwegian I-MORE program, which includes solving work-related problems, physical exercise, and treatment plans for work-specific belongings [9].
As described, the various rehabilitation programs are diverse and difficult to compare with each other. There seems to be an empirical absence of analyses of the individual treatments and their indications. The high number of diseases, each treated differently, makes the comparison even more complex. However, a structured procedure of how-to-treat-whom would be a massive alleviation for general practitioners and patients. Because of the high heterogeneity of studies that approached specific occupational rehabilitation, we conducted a systematic literature review (SLR) to compare international RCTs, trying to address treatment within the constellation of occupational rehabilitation.
The present SLR evaluates the different therapy options and treatment procedures for patients with acute and/or chronic (non-specific) back pain and investigates the outcomes of the rehabilitation programs, trying to increase workability.
2Methods
An SLR was performed following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines [19, 20]. The review protocol was registered with the International Prospective Register of Systematic Reviews (CRD42023431299).
2.1Eligibility criteria
Studies fulfilling the following inclusion criteria were included:
1 Study Design. Studies with an RCT design were included. The exclusion criteria were duplicate records, study protocols, literature reviews, meta-analysis, abstracts published in conference proceedings, and articles without a full text available and/or not written in English language. Specific exclusion criteria were studies with medical rehabilitation only, without occupational rehabilitation or workplace interventions, and without RTW relation.
2 Participants. Studies were eligible if the participants were aged 18 years or older. No restrictions on gender or ethnicity were applied. The subjects suffered from acute and chronic (non-specific) back pain and they received an occupational rehabilitation intervention or a job-related intervention. To ensure the significance of the informative value of this SLR, studies with less than 100 subjects were dismissed.
3 Outcome Measures. The primary objective of this study was to assess the efficacy of occupational rehabilitation and workplace interventions, using the variables of RTW, pain intensity, Quality of Life (QOL), and disability.
2.2Search methods for identification of studies
Relevant studies were identified by electronic literature research in MEDLINE via PubMed, PEDro, and OTseeker published before July 2023. Search keywords included OT/rehabilitation/RTW and back pain. The terms were carefully selected by identifying which terms have previously been used in related studies.
The precise search strategy for the databases was: (occupational therapy) OR (occupational rehabilitation) OR (return to work) AND (back pain).
2.3Study selection
Studies were selected independently by two reviewers (LK and LV). All potentially eligible studies were considered. Initially, the titles and abstracts were screened and full reports from potentially relevant studies were retrieved. The authors used EndNote 20.5 to assess and document the full reports regarding their inclusion or exclusion according to the predefined selection criteria. Disagreements were resolved by discussion, and when an agreement could not be reached, third and fourth reviewers were consulted (SH and BW).
2.4Data collection and extraction
Data extraction was performed by LK and LV and checked by SH and BW. Both independent raters reviewed full-text versions of the articles and articles were retained if they met inclusion criteria. The agreement on inclusion and exclusion assignment was unanimous. Data extracted from the studies included the following information: lead author, location of data collection, number and age of subjects, results and outcome related to RTW, pain intensity and QOL, and interventions. All data, required to answer the research questions were published within the papers, so no contact with authors was necessary. These results were recorded in Tables 1 and 2.
Table 1
Characteristics of included studies
| Study | Country | Sample | Age of | Outcome/Results | Rating | |||
| Size (n=) | Subjects (years) | RTW/Workability | Pain Intensity | Quality of Life | Disability | (SIGN Checklist) | ||
| Anema et al. (2007) | Netherlands | 196 | 18–65 | workplace intervention effective, graded activity negative effect, combined intervention no effect | improvement at workplace intervention but no significant difference | significant improvement for no graded activity vs. graded activity | ++ | |
| Bogefeldt et al. (2008) | Sweden | 160 | 20–55 | positive effect of RTW and sick leave due manual therapy | ++ | |||
| Dufour et al. (2010) | Denmark | 286 | 18–60 | positive effect of both interventions with no statistical significance | questionnaire showed significant improvement in both groups | improvement | significant improvement in both groups | + |
| Fisker et al. (2022) | Denmark | 770 | 18–65 | improvement in both groups regarding sick leave but no statistical significances/ differences between groups | improvement in both groups but no statistical significances/ differences between groups | improvement in both groups, but no statistical significances/ differences between groups | improvement in both groups but no statistical significances/ differences between groups | ++ |
| Hagen et al. (2010) | Denmark | 457 | 18–60 | no significant differences between groups | significant improvement in both groups | improvement of FABQ | no improvement in both groups | + |
| Henchoz et al. (2010) | Switzerland | 109 | 18–60 | significant improvement at multidisciplinary rehabilitation with significant difference | no significant difference | significant improvement at multidisciplinary intervention | + | |
| Heymans et al. (2006) | Netherlands | 299 | 18–65 | low-intensity with positive effect but no significant effect between the groups | low-intensity with positive effect but no significant effect | low-intensity with higher functional status | low-intensity significant to usual care | ++ |
| Jensen et al. (2012) | Denmark | 351 | 16–60 | no significant difference between the groups | + | |||
| Kääpä et al. (2006) | Finland | 120 | 22–57 | no significant difference | no significant difference | no significant difference | no significant differences | + |
| Lambeek et al. (2010) | Netherlands | 134 | 18–65 | RTW improvement in favor of integrated care | improvement in both groups without significance | significant improvement in favor of the integrated group | ++ | |
| Langagergaard et al. (2021) | Denmark | 476 | 18–60 | brief intervention with higher rates for employees with strong job relations | no significant difference | improvement at brief intervention with strong job relations | no significant difference | – |
| Lindell et al. (2008) | Sweden | 125 | 18–59 | no significant differences between the groups | ++ | |||
| Marchand et al. (2015) | Norway | 413 | 18–60 | RTW related to fear-avoidance-belief | decreased in both groups but no significant effect | no significant difference between groups | ++ | |
| Myhre et al. (2014) | Norway | 405 | 18–60 | no significant effect | + | |||
| Pedersen et al. (2018) | Denmark | 535 | 16–60 | no significant effect | – | |||
| Rantonen et al. (2018) | Finland | 126 | ≤56 | no effects on sick leave | both interventions reduced pain | interventions increased QOL | disability decreased in both active groups | + |
| Roche-Leboucher et al. (2001) | France | 132 | 18–50 | significantly reduce of sick-leave days in the FRP | significant improvement in both groups | significant improvement in both groups | significant improvement in both groups | + |
| Ronzi et al. (2017) | France | 159 | 18–55 | significant reduce of sick leave in all groups | improvement in FRP and mixed group | no significant difference between groups | no significant difference between groups | + |
| Stapelfeldt et al. (2011) | Denmark | 351 | 16–60 | multidisciplinary intervention with positive effect | no difference | + | ||
| Steenstra et al. (2006) | Netherlands | 112 | 18–65 | combined interventions negative effect in RTW | significant difference in favor of usual care group | no significant difference | no significant improvement | ++ |
Abbreviations: FRP Functional Restoration Program, QOL Quality of life, RTW Return to Work, FABQ Fear Avoidance Belief Questionnaire, MBR Multidisciplinary Biopsychosocial Rehabilitation. Rating scale: ++ High quality, + Acceptable, –Low quality, 0 Unacceptable –reject.
Table 2
Overview of interventions
| Method | Intervention 1 | Intervention 2 | Intervention 3 | Intervention 4 | Duration | |
| Anema et al. (2007) | workplace intervention vs. usual/graded activity | usual physical and/or behavioral graded exercises guided by PT | workplace assessment i.e. obstacle-solutions | 2–6 weeks or 8 weeks of sick leave for an unknown time | ||
| Bogefeldt et al. (2008) | standardized care vs. comprehensive program | standardized stay active therapy | standardized stay active therapy plus stretching | comprehensive stay active, stretching plus manual therapy | comprehensive stay active, stretching, manual therapy plus steroid injection | 10 weeks |
| Dufour et al. (2010) | group-based rehabilitation vs. individual therapist-assisted exercise | group-based physical exercise, education therapy | individual back muscle exercise via personal training | 12 weeks | ||
| Fisker et al. (2022) | usual care vs multidisciplinary rehabilitation | functional treatment by PT or a chiropractor in cooperation with a rheumatologist and a social worker | functional treatment as in Intervention 1 in addition of ‘return to work coordinator’, psychologist, ergonomist, occupational physician, and case manager | 12 weeks | ||
| Hagen et al. (2010) | brief intervention vs. standardized physical exercise program | brief intervention by physician and PT | brief intervention plus standardized physical exercise program | 8 weeks | ||
| Henchoz et al. (2010) | functional multidisciplinary rehabilitation vs. outpatient physiotherapy | multidisciplinary treatment by physical and ergonomic training, pain management, back school | active outpatient physiotherapy | 3 weeks vs. 9 weeks | ||
| Heymans et al. (2006) | high-intensity back school vs. low-intensity back school vs. usual care | usual activities plus intervention such as back school after sick leave | low-intensity back school and workplace intervention | high-intensity back school and workplace interventions | 4–12 weeks (depending on intervention) | |
| Jensen et al. (2012) | multidisciplinary vs. brief intervention | brief intervention by general practitioner | multidisciplinary treatment by PT, rheumatologist, specialist of social medicine, social worker, occupational therapist and workplace initiative | not described | ||
| K ääpä et al. (2006) | multidisciplinary rehabilitation vs. physiotherapy | workplace intervention, behavioral and physical training | physical exercise administered from PT | 8 weeks | ||
| Lambeek et al. (2010) | usual care vs. integrated care | usual care treatment by medical specialist, occupational physician, general practitioner and/or allied health professional | Integrated care treatment by clinical occupational physician, workplace intervention, graded activity on cognitive behavioral principle | not described | ||
| Langagergaard et al. (2021) | multidisciplinary vs. brief intervention | MRI, brief exercise training by PT, pain medication, diary | brief intervention plus case manager | individually with maximum at 3 months | ||
| Lindell et al. (2008) | cognitive behavioral vs. primary care | treatment from physician, PT, psychologist or social worker and health care adviser | multidisciplinary rehabilitation | 2–8 month | ||
| Marchand et al. (2015) | brief/multidisciplinary vs. workplace intervention | medical training by PT or physical and behavioral training | RTW focus and trained by case manager | 3 weeks | ||
| Myhre et al. (2014) | work-focused vs. controlled intervention | physical and behavioral training | RTW focus and trained by case manager | 3 weeks | ||
| Pedersen et al. (2018) | brief vs. multidisciplinary intervention | clinical examination by PT and usual treatment with general practitioner | RTW focus and trained by case manager, PT and social worker | case was closed when patient resumed work or if this was deemed impossible | ||
| Rantonen et al. (2018) | physical unit vs. specific exercise vs. advised self-care vs. no exercise | physical exercise program | physical (back) exercise with a PT | advised Self-care by a physician via Back Book® booklet | no such invited exercise program, only questionnaire after 2 years | 6–12 weeks (depending on intervention) |
| Roche-Leboucher et al. (2001) | FRP vs. AIT | FRP by occupational therapist and psychologist | AIT by PT | 5 weeks | ||
| Ronzi et al. (2017) | FRP vs. AIP vs. mixed strategy | FRP | AIP | AIP plus behavioral therapy | 5 weeks | |
| Stapelfeldt et al. (2011) | brief vs. multidisciplinary intervention | clinical examination by PT and usual treatment with general practitioner | RTW focus and trained by case manager, PT and social worker | 12 months | ||
| Steenstra et al. (2006) | usual dare vs. graded activity | sick leave guidance | workplace and behavioral intervention guided by PT | maximum 13 weeks |
Abbreviations: AIP Ambulatory Individual Physiotherapy, AIT Active Individual Treatment, FRP Functional Restoration Program, MRI Magnetic Resonance Imaging, PT Physiotherapist, RTW Return to Work.
2.5Methodological assessment of studies and risk of bias
The methodological quality and risk of bias were assessed using the Scottish Intercollegiate Guidelines Network (SIGN)-criteria, Methodology Checklist 2 for RCTs (SIGN; http://www.sign.ac.uk/). SIGN criteria include internal validity for a focused question, randomization, blinding of subjects and investigators, similarities and differences between groups, outcome measurement as well as the level of dropout, and an overall criterion for rating study quality. Eventually, the bias was concluded regarding the former assessments of the study. Three reviewers (LK, LV, and SH) independently assessed all points on the methodology checklist 2 for RCTs. When the reviewers agreed on a point, this assessment was considered eventually. Discrepancies between authors were resolved by discussion until reaching a consensus.
2.6Ethics and data analysis
The study did not involve contact with humans, so the need for ethical approval was waived. A meta-analysis was considered inappropriate due to the high heterogeneity in intervention and treatments between the studies. Accordingly, a narrative synthesis of studies was conducted.
3Results
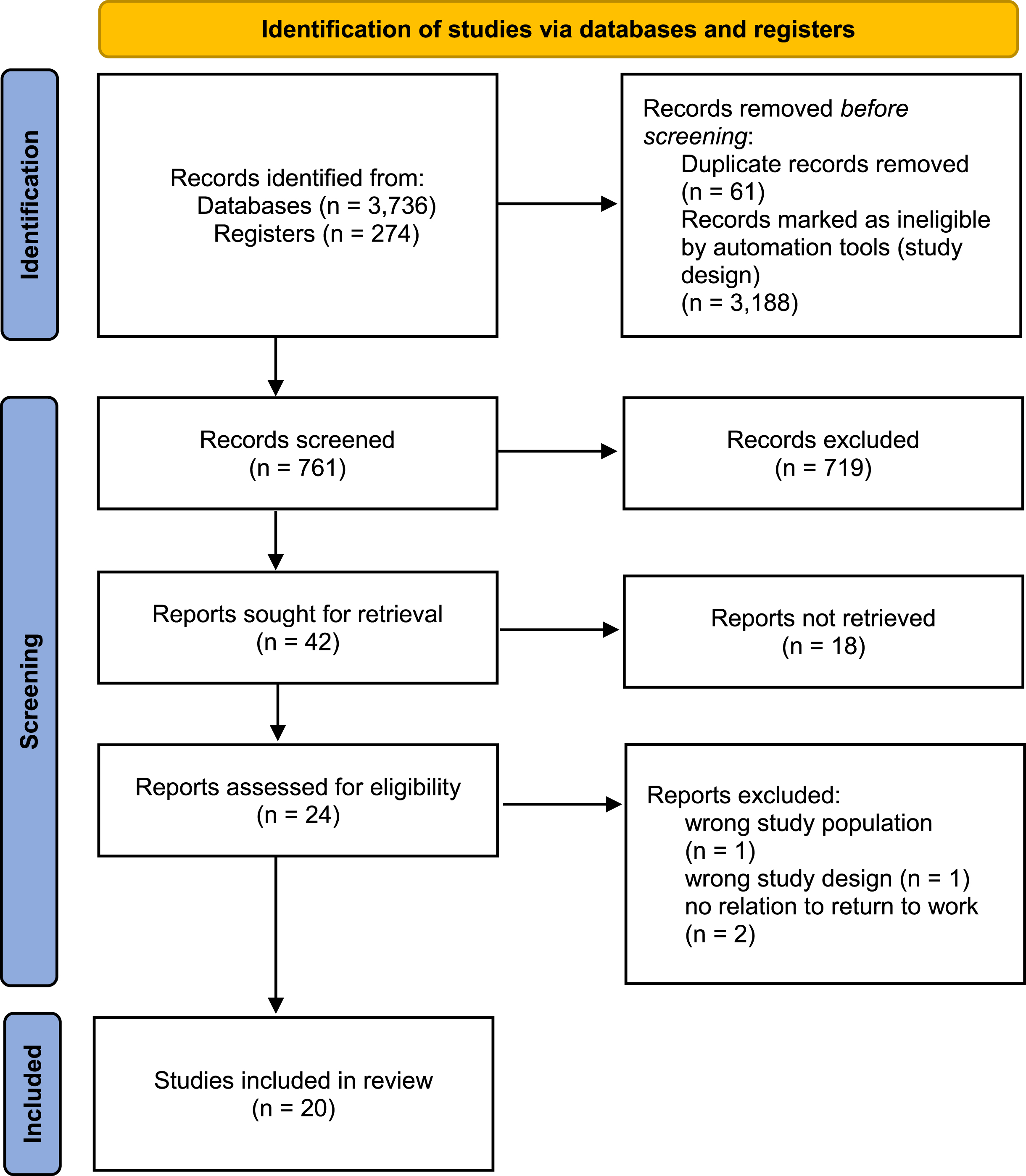
The literature search resulted in a total number of 4,010 hits. After marking records as ineligible by automation tools and duplicate removal, 761 hits were screened on the title and abstract. This resulted in 42 full-text articles that were assessed for eligibility, of which 18 articles did not meet the inclusion criteria (e.g., no occupational rehabilitation for back pain with a focus on RTW). Of the remaining 24 articles, 4 articles were eliminated, leaving 20 studies that met the inclusion criteria (Fig. 1).
Fig. 1
PRISMA diagram showing a selection of studies for systematic review.
3.1Characteristics of included studies
The characteristics of the included studies are presented in Table 1. Twenty studies were assessed. There are four studies from the Netherlands [21–24], seven Danish RCTs [25–31], two from Sweden [32, 33], two from Norway [34, 35], two Finnish studies [36, 37], two RCT from France [38, 39], and one from Switzerland [40]. The sample sizes of the studies differ from a minimum of 109 to 535 subjects. All studies addressed work-related rehabilitation or intervention programs with a focus on RTW for back pain. The various interventions differed in their treatments.
To collect data concerning work-specific models and/or interventions, the included studies investigated sick leave, ability to work, healthcare consumption, or employment status as the primary outcome of RTW, e.g. using register-based data on sick leave. The main secondary outcomes were pain intensity, QOL, and disability. Pain intensity was measured with the Visual Analogue Scale (VAS) [21–25, 27, 33, 36–39], Dallas Pain Questionnaire (DPQ) [39] the Low Back Pain Rating Scale (LPB-NRS) [26, 28, 29] or the Numeric Rating Scale [34, 35]. Disability was measured with the Roland-Morris disability questionnaire (RMDQ) [21–29, 37], Oswestry Disability Index (ODI) [24, 34, 35, 37, 40], or Short Form 36 questionnaire (SF-36) or Neck Disability Index (NDI) [34, 35]. A few studies also collected data for mental health-related QOL measured with the SF-36 [25, 39, 41], and 15 D QOL score [37]. The Symptom Checklist-90 (SCL-90), Fear-Avoidance Belief Questionnaire (FABQ) [27, 34, 35, 37, 39, 41]–including the FABQ-work scale (FABQ-W) and the FABQ- physical activity (FABQ-P) [26, 27, 35, 37], the Hopkins Symptoms Checklist [35], Orebro Musculoskeletal Pain Questionnaire (about FABQ-P) [29] or an index value by Danish country-specific values [29].
3.2Inclusion and exclusion criteria for participants
All studies included participants of working age suffering from acute and/or chronic (non-specific) back pain. Back pain was described as acute, subacute, or chronic and with or without pain radiating into the legs such as sciatica or radiculopathy. Most of the studies included subjects who were on sick leave for a certain time due to back pain. The sick leave time varied between two weeks to twelve months. The exclusion criteria were defined very differently in the included articles. The main exclusion criteria were as follows: Non-working age, back pain due to specific causes, the need for surgical treatment, pregnancy, and coexisting cardiovascular and psychiatric contraindications.
3.3Quality assessment and risk of bias
A summary of the quality assessment using the SIGN checklist is shown in Table 1. In summary, eight studies were evaluated at a general high-quality level. They fulfilled all criteria according to the SIGN checklist, which overall led to the final assessment and therefore a low risk of bias. Ten studies were rated at an acceptable quality due to the non-existing blinding, inadequate description of randomization, or missing level of dropout. Two studies were rated with low quality because of their missing empirical questioning, randomization, blinding, level of dropout, or different treatments for the participants at baseline.
The percentage agreement between reviewers (LK, LV, and SH) was at 96% agreement.
3.4Interventions
The included articles were studies comparing an intervention group compared with one or more control groups. Ten studies [21, 23, 27–29, 30, 31, 34–36] compared workplace interventions or Multidisciplinary Interventions (MDI) with a non-interventional group. Two of them had a second control group consisting of a graded activity group [21, 34], or an MDI if the first intervention group received a workplace intervention [35]. Eight studies [22, 24, 25, 32, 33, 37–39] compared interventions with a physical therapy approach including sessions with a physiotherapist (PT) with either a non-intervention group and/or another intervention group. Four studies compared an MDI to usual care including physiotherapy [26, 31, 36, 40]. Most of these studies had more than one control group. One of them included a psychotherapy-based treatment [26]. Detailed information about the interventions is presented in Table 2.
3.5Effects on return to work
Results are presented in Table 1. The level of significance was set to 5% in all studies.
All of the studies included in the SLR investigated the effect of different occupational therapies on RTW. When investigating the first five-week period without work absence, Marchand et al. [34] estimated an odds ratio (OR) of 0.97 (95% -confidence interval (CI): 0.47, 1.99) for the work intervention within 12 months. Myhre et al. [35] investigated the effect of the intervention group compared to the control group on the time to RTW estimating a hazard ratio (HR) of 0.76 (95% -CI: 0.556, 1.04) for the first center and an HR of 1.15 (95% -CI: 0.84, 1.57) for the second center.
When investigating the first four weeks without work absence, the adjusted HR at the intention-to-treat analysis of the intervention group at Steenstra et al. [24] was 0.66 (95% -CI: 0.40,1.10). The HR for people with high job satisfaction was 0.72 (95% -CI: 0.38, 1.38) and the HR for people with low job satisfaction was 1.41 (95% -CI: 0.77, 2.57), in favor of the MDI. Lambeek et al. [23] estimated an HR of 1.90 (95% -CI: 1.18, 2.76). In comparison to this, Langagergaard et al. [29] detected an HR of 1.07 (95% -CI: 0.77, 1.49) in favor of MDI at weak job relations and an HR of 0.73 (95% -CI: 0.55, 0.96) for strong job relation, in favor of BI. Comparing the low-intensity back school with the high-intensity back school at Heymans et al. [22], the HR was 1.3 (95% -CI: 1.0, 1.8). Anema et al. [21] estimated an HR of 1.7 (95% -CI: 1.2,2.3) for the first time to RTW compared with the workplace intervention with control, though the HR of 0.4 (95% -CI: 0.3,0.6) in favor of no graded activity, as well an HR of 0.7 (95% -CI: 0.3,1.2) in favor of no combined intervention. Jensen et al. [28] investigated an HR of 0.82 (95% -CI: 0.62, 1.08) when comparing MDI with BI.
Rantonen et al. [37] estimated a mean difference of accumulated sickness absence days in 4 years of –5 (95% -CI: –34,24) between the rehab group and the control group, a difference of 1 (95% -CI: –29,31) between the physio and the control group and a difference of 11 (95% -CI: –22,44) between the advice and the control group. Dufour et al. [25] reported an improvement in workability from 29% up to 40% in group A and 36% at the beginning and 38% after treatment in group B. Bogefeldt et al. [32] calculated an HR of 1.62 (95% -CI: 1.006,2.60) regarding the RTW for at least one week, in favor of the manual therapy group. Pedersen et al. [30] reported a total of 41% of patients in the MDI received a “work participation score” above 75%, in comparison to 51% of patients in the brief intervention (BI). At Roche-Leboucher [38] the mean change reduction of the number of sick-leave days (post-treatment year-pretreatment year) at the functional restoration from the baseline to 12-month follow-up was –101.2 (SD = 126.5). At the active individual therapy, the mean change was –79 (SD = 143.9).
Regarding the RTW chance –the workability over 18 months independently by the duration of the achievement –, Lindell et al. [33] estimated an HR of 1.6 (95% -CI: 0.7, 3.6) in favor of the rehabilitation group. In Henchoz et al. [40], work status, quantified by the percentage of professional activity reported by patients, was unemployment in 6 patients (43%) at 12 months by the 14 patients in functional multidisciplinary rehabilitation. Regarding the 10 participants off-work at the outpatient physiotherapy intervention, one (10%) was at work after 12 months.
3.6Effects on pain intensity
When investigating the pain via VAS (0–100 mm), the HR of the intervention group was 0.43 (95% -CI: 0.31, 1.16) at 12 weeks and 1.03 (95% -CI: 0.05, 2.01) at 26 weeks for the study by Seenstra et al. [24]. Rantonen et al. [37] calculated a mean difference between the rehabilitation and control group of –13 (95% -CI: –24,–1) and a mean difference between the physio and control group of –13 (95% -CI: –29,2). The mean difference between advice and control was –10 (95% CI –0.03, 0.08). Dufour et al. [25] showed improvement regarding the mean of pain from 3 months (group A mean = 16.5, (SD = 2.50), group B mean = 11.2, (SD = 23.8) to 6 months (group A mean = 12.6, SD = (24.7), group B mean = 9.0, SD = (24.2). Anema et al. [21] reported a coefficient of the longitudinal regression of –0.20 (95% -CI: –0.75, 0.35) in favor of no workplace intervention, an effect of 0.67 (95% -CI: –0.05,1.38) in favor of no graded activity and 0.47 (95% -CI: –0.42,1.35) in favor of no combined intervention. Lambeek et al. [23] calculated a between-group difference at 12-month follow-up at 2.1 (95% CI: –8,12) (integrated care: 16.4 (SD = 3.5); usual care: 18.5 (SD = 3.6). Roche-Leboucher et al. [38] investigated a mean change at the functional restoration of –17 (SD = 26) and a mean change at the active individual therapy of –10 (SD = 23).
Marchand et al. [34] estimated an OR of 1.04 (95% -CI: 0.54, 2.00) in the intervention group via the NRS (0–10). When investigating the LBP-NRS (0–60) at Langergaard et al. [29], people with weak job relations, showed a mean change in the score from baseline to follow-up of –10.1 (95% -CI: –13.4, –6.7) for the MDI and a mean difference of –12.7 (95% -CI: –16.7, 8.7) for the BI. Strong job relations revealed a mean change of –10.5 (95% -CI: –13.3, –7.7) at the MDI and a mean change of –13.6 (95% -CI: –16.6, –10.6) for the BI. Hagen et al. [27] showed a mean change at the NRS of –0.58 (95% - CI: –0.78, –0.28) at the 2-year follow-up in both groups.
3.7Effects on disability
Marchand et al. [34] estimated an OR of 0.86 (95% -CI: 0.38, 1.96) in the work-focused intervention for the ODI (0–50), applying a cut-off point of 12 for the change between baseline and 12 months after the intervention. For the same questionnaire, Rantonen et al. [37] calculated a mean difference between rehab (8 points) and control group (14 points) of –6 (95% -CI: –10, –2) and a mean difference of –5 (95% -CI: –9, 0) between the physio (9 points) and the control group (14 points). The mean difference between advice (12 points) and the control group (14 points) was –2 (95% -CI: –6, 2). Henchoz et al. [40] investigated at their ODI (a 10-item scale ranging from 0 to 100%) a decrease at the functional multidisciplinary rehabilitation of 37.6 (15.8) at baseline down to 26.2 (18.0) in 12-month follow-up. The outpatient therapy registered a decrease of 39.1 (14.7) at baseline down to 38.0 (18.4) at 12-month follow-up.
Langagergaard et al. [29] estimated, for people with weak job relations, a mean change from baseline to follow-up of –5.1 (95% -CI: –6.6,–3.6) points on the RMDQ scale (0–24) for the MDI and a mean change of –6.4 (95% -CI: –7.9,–4.9) RMDQ for the BI. Regarding strong job relations, the mean change was –6.6 (95% -CI: –7.8,–5.3) RMDQ for the MDI and –7.7 (95% -CI: –9.1,–6.4) RMDQ for the BI. Dufour et al. [25] showed an improvement of 3.0 points for the multidisciplinary biopsychosocial intervention in comparison to the Assisted Back Muscle Strengthening Group with 1.5 points. Anema et al. [21] estimated a longitudinal regression coefficient of –0.25 (95% -CI: –1.57,1.06) in favor of workers who did not receive workplace intervention, as well as a regression coefficient of 1.74 (95% -CI: 0.07,3.42) in favor of the graded activity and a regression coefficient of 1.49 (95% -CI: –0.33,3.31) in favor of the combined intervention. Hagen et al. [27] showed a mean change of –1.65 points (95% -CI: –2.46, –0.83) in both groups at the 2-year follow-up. Lambeek et al. [23] estimated a between-group difference at 12-month follow-up of –2.86 (95% -CI: –4.9,–0.9) (integrated care: 7.16 (SD = 0.71); usual care: 4.43 (SD = 0.72).
3.8Effects on quality of life
Langagergaard et al. [29] showed a mean change from baseline to follow-up of 1 (95% - CI: 0.1, 0.2) of the Danish country-specific value for MDI and a mean change of 0.1 (95% -CI: 0.1, 0.2) to the BI in the subpopulation of people with weak job relations. People with strong job relations resulted in a mean change of 0.1 (95% -CI: 0.1, 0.2) Danish country-specific value for MDI and 0.2 (95% -CI: 0.2, 0.3) for the BI. Rantonen et al. [37] (QOL, range 0–1) calculated a mean difference between the rehabilitation and control group of 0.06 (95% -CI: 0.00, 0.12) and a mean difference of 0.07 (95% -CI: 0.01, 0.13) between the physio and control group. The mean difference between the advice and control group was 0.02 (95% -CI: –0.03, 0.08). Hagen et al. [27] calculated at the FABQ (0–96) a mean change of –0.11 points (95% -CI: –0.18, –0.04) at both groups at the 2-year follow-up.
4Discussion
This SLR aims to establish the current state of the applied therapeutic methods of occupational rehabilitation for people with back pain and to define an appropriate therapy that improves or restores workability.
In terms of improving pain intensity, disability, and QOL, interventions with a physical therapy approach, adding a high proportion of exercise under the guidance of trained coaches, appear to be clinically appropriate.
Three of the high-quality assessed studies detected a significant difference between the groups in RTW due to their rehabilitation programs, which reveals to be clinically relevant [21, 23, 32]. Concerning the positive results of the manual therapy program, the program contained a ‘black-box’ approach. Thus, therapists can use the most appropriate treatment modalities for a specific patient from a specific list, such as the approach used in clinical practice [32]. The positive effect of an exercise program is no novel knowledge. However, the ‘black-box’ approach, in the context of intervention programs, significantly improves RTW. Hence, the importance of an incorporation of the therapist, whilst determining a suitable rehabilitation program seems to be of value. Furthermore, the benefit due to a possible individual intervention within the ‘black-box’ approach may be promising, hence advising more room for physical therapists in clinical practice.
The workplace intervention of Anema et al. [21] contained a workplace assessment with work adjustments by an ergonomist to brainstorm and discuss workable solutions. The research group [21] suspected that the effects of workplace interventions are not only based on simply reducing physical and mental workload. They assumed other mechanisms of importance for the success of workplace interventions in terms of working capabilities and workplace opportunities. This may underline RTW failure, caused by a collapsed social transaction, rather than a worker’s medical condition [42–44].
Stapelfeldt et al. [31] also presented significant differences in RTW in a subgroup of subjects with low job satisfaction for the multidisciplinary group. Further, they detected two more significant effects on variables if claimants were excluded. Claimants were described as sick-listed employees who have claimed economic compensation for their disease or injury. If these participants were excluded, significant interaction for the variables ‘influence on work planning’ and ‘feeling at risk of losing one’s job due to the present sick leave’ were found. Participants with low job satisfaction, no influence on work, no interest in returning to the same job, and at risk of losing their job returned earlier to work if they obtained the MDI. If receiving a BI, participants without the formerly described attributes had a faster rate of RTW. An independent second study by the research group, [31], confirmed these findings. However, it must be examined, whether the correlations are plausible. It might be suspected that those who feel at risk of losing their job have benefited the most from the cooperation between vocational, and social professionals, and the employer. This suggests the confidence of employees with no concern of losing their job when reaching an agreement with their employer about a job change. Furthermore, it may accompany the dependency on a worker’s initial situation. A rehabilitation program in an occupational setting seems to be promising to improve RTW, pain, disability, and QOL (Table 1) but also depends on the worker’s attitudes themselves. Hence, we recommend a detailed clinical and anamnestic investigation regarding a worker’s occupational perspective. Thus leading to more standardized trials to assess the most reasonable patient for an OT. Underlined by a statement by Lambeek et al. [23] as well, who ascribe the occupational therapist as the best-equipped “manager” of a patient in the use of OT. Thus, supporting a more internationally standardized profession in this field, and opening more possibilities for RCTs. Furthermore, a more specialized treatment setting and surrounding could simplify the how-to-treat-whom question.
Ronzi et al. [39] suggested the similar effectiveness of different treatments for chronic LBP due to the same changes in beliefs, attitudes, and coping mechanisms. The coordination between medical and occupational issues is key to successful RTW for patients with chronic LBP [39] and a beneficial economical use of OT.
Concerning pain intensity and disability, seven of twelve studies [23, 25, 27, 36, 38–40] detected significant improvements after the follow-up period with clinical relevance. The commonality of these interventions is their inclusion of physical exercises with a therapist.
This indicates the necessity of a high percentage of physical exercise with a special therapist for improvements in back pain intensity and disability in clinical settings. In terms of QOL, treatments with physical exercise can achieve improvements.
When adding a psychological component, improvements in all variables were found but without any significant differences from the usual care group, Fisker et al. [26]. Hence, when addressing sick leave, RTW, pain, disability, or QOL, clinically no further additional treatment due to psychologists might be necessarily recommended, though still needs to be discussed due to the missing significance and conflict by Lambeek et al. [23], who state back pain as not only a clinical problem but also as a psychosocial concern.
Comprehensive therapy could certainly be beneficial for the individual outside of the parameters measured (e.g., pain and QOL). Regarding the interrelation between back pain and OT, the results of the studies should be proportionated by the consideration of treatment success for back pain in general. As already described in the introduction, back pain treatment reveals to be difficult [4, 5], thus leading to a contorted conception of the OT. Therefore, we would recommend more studies investigating the efficacy of OT in correlation with other diseases, which may be more precise in terms of treatment options and success rate.
In the evaluation of the studies and their results, it must be noted that some of the studies were downgraded in the SIGN checklist due to their missing blinding process. However, it seems impossible to proceed with blinding in some cases [45] because otherwise, the therapists would not know about the treatment. Moreover, some studies did not describe their drop-out quote whereas correspondingly smaller sample sizes lead to larger effect sizes [45] regarding the difference inside the cohort and higher risk of type 2 errors.
4.1Study strengths
The present SLR for testing the efficacy of OT for people with back pain brings a (socio) medical value to occupational rehabilitation programs. This might help practitioners and medical administrations to improve their treatment protocols.
Moreover, the SLR was structured by the PRISMA diagram to ensure the empirical standardization of the study and therefore fulfill the three scientific quality criteria. In addition to that, a validated Risk of Bias Tool was used to compare the RCTs and, therefore, their strengths and limitations.
4.2Limitations
There were some limitations. The reviewers only included RCTs for the best available evidence, but this means some occupational therapy and intervention approaches have been excluded because no trials have existed. The studies, evaluated in the SLR, only integrated 20 studies, which could falsify the concluded results. Based on our selected search terms and inclusion and exclusion criteria, only European studies remained for our analysis, especially many Scandinavian studies, which was not an inclusion criterion. One reason could be that the healthcare system and pension systems are very different worldwide. In the Scandinavian region in particular, many studies are conducted in the area of rehabilitation, as researchers can more easily incorporate register or secondary data into their analysis. Therefore, non-European predictions are difficult to determine. One possibility for future work would be to expand the search terms to include the parameters ‘Pain Intensity’, ‘Disability’, and ‘QOL’. The findings must be interpreted within the context of our study’s limitations.
5Conclusion
Some of the included studies in this SLR established positive effects concerning work-related data, especially regarding RTW [21, 23, 25, 26, 31, 32, 38–40]. However, the intervention programs and the usual care/control groups differed highly, which leads to the assumption of inconclusive evidence regarding the treatment effect of the intervention programs. The results of this SLR suggest that a manual therapy program, including stay-active therapy, stretching, and manual therapy, could positively reduce RTW [31]. Because of the ‘black box’ approach of the manual therapy in this study, it was impossible to identify exactly, which variables were most effective in reducing RTW. Therefore, more research and standardization are needed to determine the effectiveness of different forms of manual treatment in reducing sick leave. Further research should focus on the contributions of various treatment modalities as well as the importance of the therapist’s influence and/or value, which may have potential clinical input.
Moreover, the social transaction between the workplace and employees appears to be an important key to work-related outcomes [21]. Therefore, evaluated mediation between employees and employers is beneficial, as supposed in former publications [8].
Considering these results, it is useful to check these variables among the workers to include this information in a planned rehabilitation. The included studies in the present SLR showed exclusively positive effects for interventions with a high percentage of physical exercise regarding the improvement of pain intensity, disability, and QOL [21, 22, 24]. This is why intervention programs with a high percentage of physical exercise, led by a professional therapist for back pain, are appropriate to improve these variables and should be revised in clinical settings. However, more research is needed to evaluate which specific physical exercise best improves pain intensity. In addition, further investigations about pain intensity are needed, to be able to assess individual suffering and compare it with a sample. Hence, it is highly recommended to create more uniformity in design and methodology in future studies of OT. There is a need for more high-quality studies on this topic [8]. Furthermore, OT should be revised in more RCT in the context of other diseases for wider empirical proof of its efficacy.
Author contributions
LK: study conception and design. LK and LV: selected the studies for inclusion and abstracted data. LK: wrote the first draft and conducted the analyses. LV and SH: wrote the manuscript and conducted the analyses. BW: critically revised the paper for important intellectual content. All authors read and agreed to the published version of the manuscript.
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical approval
Not applicable.
Acknowledgments
None to report.
Funding
None to report.
Supplementary material
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/WOR-230277.
References
[1] | Brötz D , Weller M . Diagnostik und Therapie bei Bandscheibenschäden: Thieme; 2017. |
[2] | Lo J , Chan L , Flynn S . A systematic review of the incidence, prevalence, costs, and activity and work limitations of amputation, osteoarthritis, rheumatoid arthritis, back pain, multiple sclerosis, spinal cord injury, stroke, and traumatic brain injury in the united states: A update. Arch Phys Med Rehabil. (2021) ;102: (1):115–31. |
[3] | Großschädl F , Stolz E , Mayerl H , Rásky É , Freidl W , Stronegger WJ . Rising prevalence of back pain in Austria: Considering regional disparities. Wien Klin Wochenschr. (2016) ;128: (1-2):6–13. |
[4] | Pena Junior PM , de Sá Ferreira A , Telles G , Lemos T , Calazans Nogueira LA . Concurrent validation of the centre of pressure displacement analyzed by baropodometry in patients with chronic non-specific low back pain during functional tasks. J Bodyw Mov Ther. (2021) ;28: :489–95. |
[5] | Maher C , Underwood M , Buchbinder R . Non-specific low back pain. Lancet. 3890). (2017) ;389: :(10070):736–47. |
[6] | Hamel M , Heinrich M , Niemier K , Marnitz U . Rückenschmerzen therapieren: Von der multimodalen Idee zur interdisziplinären Lösung: De Gruyter; 2018, p. 299. |
[7] | Fauser D , Zimmer JM , Golla A , Schmitt N , Mau W , Bethge M . Self-reported prognosis of employability as an indicator of need for rehabilitation: A cohort study in people with back pain. Rehabilitation (Stuttg). (2022) ;61: (2):88–96. |
[8] | Pransky G , Gatchel R , Linton SJ , Loisel P . Improving return to work research. J Occup Rehabil. (2005) ;15: (4):453–7. |
[9] | Gismervik S , Aasdahl L , Vasseljen O , Fors EA , Rise MB , Johnsen R , et al.Inpatient multimodal occupational rehabilitation reduces sickness absence among individuals with musculoskeletal and common mental health disorders: A randomized clinical trial. Scand J Work Environ Health. (2020) ;46: (4):364–72. |
[10] | Eichert HC . Ambulante berufliche Rehabilitation psychisch erkrankter Menschen. Rehabilitation (Stuttg). (2012) ;51: (03):181–8. |
[11] | Beyer S , Kilsby M . Supported employment in britain. Tizard Learning Disability Review. (1997) ;2: (2):6–14. |
[12] | Fauser D , Vogel M , Bethge M . Medizinisch-beruflich orientierte Rehabilitation bei Rehabilitanden mit muskuloskelettalen Erkrankungen: Eine Propensity-Score-Analyse. Rehabilitation (Stuttg). (2020) ;59: (06):332–40. |
[13] | Bethge M , Herbold D , Trowitzsch L , Jacobi C . Work status and health-related quality of life following multimodal work hardening: A cluster randomised trial. J Back Musculoskelet Rehabil. (2011) ;24: (3):161–72. |
[14] | Bethge M , Neuderth S . Medizinisch-berufliche Maßnahmen - Psychologie in der medizinischen Rehabilitation: Ein Lehr- und Praxishandbuch. Heidelberg: Springer; 2016. |
[15] | Kleist B , Alliger K , Winter S , Beyer W . Work Hardening bei chronischen unspezifischen Rückenschmerzen in der stationären Rehabilitation. Praxis Klin Verhaltensmed Rehab. (2001) ;14: :145–50. |
[16] | Streibelt M , Bethge M . Effects of intensified work-related multidisciplinary rehabilitation on occupational participation: A randomized-controlled trial in patients with chronic musculoskeletal disorders. Int J Rehabil Res. (2014) ;37: (1):61–6. |
[17] | Hansen A , Pedersen CB , Jarden JO , Beier D , Minet LR , Søgaard K . Effectiveness of physical therapy- and occupational therapy-based rehabilitation in people who have glioma and are undergoing active anticancer treatment: Single-blind, randomized controlled trial. Phys Ther. (2020) ;100: (3):564–74. |
[18] | Taimela S , Aronen P , Malmivaara A , Sintonen H , Tiekso J , Aro T . Effectiveness of a targeted occupational health intervention in workers with high risk of sickness absence: Baseline characteristics and adherence as effect modifying factors in a randomized controlled trial. J Occup Rehabil. (2010) ;20: (1):14–20. |
[19] | Liberati A , Altman DG , Tetzlaff J , Mulrow C , Gøtzsche PC , Ioannidis JP , et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. (2009) ;6: (7):e1000100. |
[20] | Page MJ , McKenzie JE , Bossuyt PM , Boutron I , Hoffmann TC , Mulrow CD , et al. The PRISMA statement: An updated guideline for reporting systematic reviews. PLOS Medicine. (2021) ;18: (3):e1003583. |
[21] | Anema JR , Steenstra IA , Bongers PM , de Vet HC , Knol DL , Loisel P , et al. Multidisciplinary rehabilitation for subacute low back pain: Graded activity or workplace intervention or both? A randomized controlled trial. Spine (Phila Pa 1976). (2007) ;32: (3):291–8; discussion 9-300. |
[22] | Heymans MW , de Vet HC , Bongers PM , Knol DL , Koes BW , van Mechelen W . The effectiveness of high-intensity versus low-intensity back schools in an occupational setting: A pragmatic randomized controlled trial. Spine (Phila Pa. (2006) ;31: (10):1075–82. |
[23] | Lambeek LC , van Mechelen W , Knol DL , Loisel P , Anema JR . Randomised controlled trial of integrated care to reduce disability from chronic low back pain in working and private life. Bmj. (2010) ;340: :c1035. |
[24] | Steenstra IA , Anema JR , Bongers PM , de Vet HC , Knol DL , van Mechelen W . The effectiveness of graded activity for low back pain in occupational healthcare. Occup Environ Med. (2006) ;63: (11):718–25. |
[25] | Dufour N , Thamsborg G , Oefeldt A , Lundsgaard C , Stender S . Treatment of chronic low back pain: A random- ized, clinical trial comparing group-based multidisciplinary biopsychosocial rehabilitation and intensive individual therapist-assisted back muscle strengthening exercises. Spine (Phila Pa 1976). (2010) ;35: (5):469–76. |
[26] | Fisker A , Langberg H , Petersen T , Mortensen OS . Effects of an early multidisciplinary intervention on sickness absence in patients with persistent low back pain-a randomized controlled trial. BMC Musculoskelet Disord. (2022) ;23: (1):854. |
[27] | Hagen EM , Ødelien KH , Lie SA , Eriksen HR . Adding a physical exercise programme to brief intervention for low back pain patients did not increase return to work. Scand J Public Health. (2010) ;38: (7):731–8. |
[28] | Jensen C , Jensen OK , Nielsen CV . Sustainability of return to work in sick-listed employees with low-back pain. Two-year follow-up in a randomized clinical trial comparing multidisciplinary and brief intervention. BMC Musculoskelet Disord. (2012) ;13: :156. |
[29] | Langagergaard V , Jensen OK , Nielsen CV , Jensen C , Labriola M , Sørensen VN , et al. The comparative effects of brief or multidisciplinary intervention on return to work at 1 year in employees on sick leave due to low back pain: A randomized controlled trial. Clin Rehabil. (2021) ;35: (9):1290–304. |
[30] | Pedersen P , Nielsen CV , Jensen OK , Jensen C , Labriola M . Employment status five years after a randomised controlled trial comparing multidisciplinary and brief intervention in employees on sick leave due to low back pain. Scand J Public Health. (2018) ;46: (3):383–8. |
[31] | Stapelfeldt CM , Christiansen DH , Jensen OK , Nielsen CV , Petersen KD , Jensen C . Subgroup analyses on return to work in sick-listed employees with low back pain in a randomised trial comparing brief and multidisciplinary intervention. BMC Musculoskelet Disord. (2011) ;12: :112. |
[32] | Bogefeldt J , Grunnesjo MI , Svardsudd K , Blomberg S . Sick leave reductions from a comprehensive manual therapy programme for low back pain: The Gotland Low Back Pain Study [with consumer summary]. Clinical Rehabilitation. (2008) ;22: (6):529–41. |
[33] | Lindell O , Johansson SE , Strender LE . Subacute and chronic, non-specific back and neck pain: Cognitive behavioural rehabilitation versus primary care. A randomized controlled trial. BMC Musculoskelet Disord. (2008) ;9: :172. |
[34] | Marchand GH , Myhre K , Leivseth G , Sandvik L , Lau B , Bautz-Holter E , et al. Change in pain, disability and influence of fear-avoidance in a work-focused intervention on neck and back pain: A randomized controlled trial. BMC Musculoskelet Disord. (2015) ;16: :94. |
[35] | Myhre K , Marchand GH , Leivseth G , Keller A , Bautz-Holter E , Sandvik L , et al. The effect of work-focused rehabilitation among patients with neck and back pain: A randomized controlled trial. Spine (Phila Pa 1976). (2014) ;39: (24):1999–2006. |
[36] | Kaapa KF E , Sarna S , Malmivaara A . Multidisciplinary group rehabilitation versus individual physiotherapy for chronic nonspecific low back pain: A randomized trial. Spine. (2006) ;31: (4):371–6. |
[37] | Rantonen J , Karppinen J , Vehtari A , Luoto S , Viikari-Juntura E , Hupli M , et al. Effectiveness of three interventions for secondary prevention of low back pain in the occupational health setting - a randomised controlled trial with a natural course control. BMC Public Health. (2018) ;18: (1):598. |
[38] | Roche-Leboucher G , Petit-Lemanac’h A , Bontoux L , Dubus-Bausière V , Parot-Shinkel E , Fanello S , et al. Multidisciplinary intensive functional restoration versus outpatient active physiotherapy in chronic low back pain: A randomized controlled trial. Spine (Phila Pa 1976). (2011) ;36: (26):2235–42. |
[39] | Ronzi Y , Roche-Leboucher G , Bègue C , Dubus V , Bontoux L , Roquelaure Y , et al. Efficiency of three treatment strategies on occupational and quality of life impairments for chronic low back pain patients: Is the multidisciplinary approach the key feature to success? Clin Rehabil. (2017) ;31: (10):1364–73. |
[40] | Henchoz Y , Goumëens P , So AK , Paillex R . Functional multidisciplinary rehabilitation versus outpatient physio- therapy for non specific low back pain: Randomized controlled trial. Swiss Med Wkly. (2010) ;140: :13133. |
[41] | Hoff A , Poulsen RM , Fisker J , Hjorthøj C , Rosenberg N , Nordentoft M , et al. Integrating vocational rehabilitation and mental healthcare to improve the return-to-work process for people on sick leave with depression or anxiety: Results from a three-arm, parallel randomised trial. Occup Environ Med. (2022) ;79: (2):134–42. |
[42] | Shaw WS , Pransky G , Fitzgerald TE . Early prognosis for low back disability: Intervention strategies for health care providers. Disabil Rehabil. (2001) ;23: (18):815–28. |
[43] | Waddell G , Burton AK . Occupational health guidelines for the management of low back pain at work: Evidence review. Occup Med (Lond). (2001) ;51: (2):124–35. |
[44] | Frank J , Sinclair S , Hogg-Johnson S , Shannon H , Bombardier C , Beaton D , et al. Preventing disability from work-related low-back pain. New evidence gives new hope–if we can just get all the players onside. Cmaj. (1998) ;158: (12):1625–31. |
[45] | Namnaqani FI , Mashabi AS , Yaseen KM , Alshehri MA . The effectiveness ofMcKenzie method compared to manual therapy for treating chronic low back pain: A system- atic review. J Musculoskelet Neuronal Interact. (2019) ;19: (4):492–9. |


