
Relationship between duration of sick leave and time variation of words used in return-to-work programs for depression
Abstract
BACKGROUND:
Return-to-work (RTW) programs are provided as rehabilitation for people who have taken sick leave from work because of mental health problems. However, methods to present this information to workplaces objectively remain limited.
OBJECTIVE:
This study aimed to conduct an exploratory investigation of the relationship between duration of sick leave and time variation of words used in RTW programs for depression from textual data collected from electronic medical records as a new evaluation indicator.
METHODS:
The study subjects were those who had taken sick leave because of major depressive or adjustment disorder and had participated in an RTW program. The study data comprised demographic characteristics and texts. Textual data were collected from electronic medical records and classified based on the SOAP note. Thereafter, the textual data were quantified into category scores based on a standard text analysis dictionary. A generalized linear mixed model was used for the statistical analysis, with the score for each category (emotional, social, cognitive, perceptual, biological, motivational, relativity, and informal) as the dependent variable and the duration of sick leave, time, and interaction between the duration of sick leave and time as the independent variables. The level of statistical significance was set at 0.05.
RESULTS:
In total, 42 participants were included in the analysis. The results revealed a significant interaction between the social (p = 0.001) and emotional (p = 0.002) categories.
CONCLUSION:
The findings suggest a relationship between word changes in electronic medical records and the duration of sick leave.
1Introduction
1.1Mental health among workers
Work significantly impacts the mental health of employees, with one in six individuals experiencing mild-to-moderate depression or anxiety [1]. In Japan, the number of work-related accidents associated with mental health has been continuously increasing since 2012 [2], leading to approximately four out of every 1000 workers taking sick leave [3]. Moreover, economic losses due to depression and suicide are estimated at approximately 2.7 trillion yen per year [4]. Therefore, work-related mental health problems have become a substantial social issue. Various measures have been implemented in different fields to address the mental health of workers. The Japanese government has mandated companies with 50 or more employees to conduct “occupational stress checks” to enhance workplace environments [5]. Guidelines for “supporting the workplace return of employees who took sick leave because of mental health issues” have also been developed to assist employees on sick leave in their return-to-work (RTW) [6]. Companies are taking various initiatives to address mental health issues, with about 60% of Japanese companies providing education, training, and information on mental health to their employees [1]. Additionally, some companies have their own programs to support the RTW of employees on sick leave [1]. In the medical field, RTW programs are being implemented for employees on sick leave, and previous studies in Japan have found that these programs reduce the rate of recurrent sick leave [7]. A systematic review on the predictive factors for RTW suggests that older age, higher severity of depression, and comorbid mental or physical disorders may delay RTW [8]. In a meta-analysis of qualitative studies on the RTW of workers with common mental disorders, participants reported experiencing benefits from psychotherapy and rehabilitation, but found it difficult to determine the timing of their RTW [9]. Furthermore, a qualitative study that investigated the expectations of various stakeholders (e.g., workers, colleagues, supervisors, occupational physicians, health-care professionals) regarding RTW reported that smooth communication was an important common challenge [10].
There are several methods used by health-care professionals to communicate the conditions of their patients to other stakeholders from a medical perspective. For example, one method involves observing and documenting a patient’s behavior during participation in an RTW program, while another involves administering a self-report questionnaire to the patient and reporting the results [11, 12]. The former method can convey some of the health-care professional’s thoughts, but unlike numerical data, these thoughts are difficult to visualize and may not be a good indicator of the timing of the patient’s RTW. The latter method is useful in that it evaluates the patient’s subjective experience and can be quantified. Although this method is widely used, it is considered insufficient for use as a numerical goal for RTW.
1.2Natural language processing (NLP) for medical electronic records
In this study, we focused on NLP, which involves using computers to analyze the language used by humans in everyday life for such purposes as machine translation and summarizing textual data. Regarding the analysis of language by computers, Pennebaker [13] noted that it is based on the hypothesis that beyond their literal meaning, the words used by human beings convey information independent of the semantic context, and as such, human beings typically find it difficult to recognize words independent of their semantic context. Due to these benefits, several studies have used NLP methods and reported useful findings in the field of psychiatry. For instance, several studies have reported the characteristics of linguistic behavior in patients with schizophrenia [14], eating disorders [15], and borderline personality disorder [16]. Studies on depression show that higher depression severity is related to the increased use of negative emotional words [17], first-person singular pronouns [18], the past tense [19], absolutist words [20], tautologies, emphases [21], and fillers [22], and to the decreased use of positive emotional words, optimistic words [23], and the future tense [24].
There have been several reports of NLP studies targeting workers. For example, a study investigating work-related tweets using Twitter reported that tweets containing words such as “life” and “need” were included regardless of the emotion expressed in the tweet [25]. Another study that used NLP to investigate work-related suicides in the National Violent Death Reporting System database identified factors such as mental health issues and conflicts in relationships as preceding factors of suicide [26].
In the present study, we used electronic medical records as textual data for NLP. Electronic medical records contain longitudinal transcripts over the entire period for which the patient is undergoing treatment [27]. In addition, because of the various situations in which the subject is observed and evaluated, electronic medical records provide evaluation data that are more similar to the patient’s workplace and daily living environment, in contrast to evaluations such as examinations and measurements [27]. Additionally, no new data have to be obtained from the patients because large amounts of textual data about their conditions, which is regarded as important by medical staff through daily clinical practice, have already been accumulated [27]. The results of our previous study suggested that the frequency of positive words in electronic medical records is related to a shorter duration of sick leave [28]. Therefore, the indicators obtained from quantifying the textual data in electronic medical records might be related to the duration of sick leave. However, our previous study used a uniform set of all textual data collected during the entire period of program use, and did not consider therapeutic changes over time. In the present study, we investigated the time variation of words in textual data to identify the characteristics of subjects who were unable to avoid long-term sick leave, which might provide important insights into the development of interventions suited to individual patients.
1.3Objective
The objective of this study was to conduct an exploratory investigation of the relationship between duration of sick leave and time variation of words from textual data collected from electronic medical records during RTW programs for depression.
2Methods
2.1Overview of data
The present study was conducted using secondary data from Kutsuna et al. [28]. The following section explains the details of the data and procedures used in this study.
2.1.1Sample
The participants in the report by Kutsuna et al. [28] were selected based on the following inclusion criteria: patients at a mental health clinic in Japan who had been 1) diagnosed with depression or adjustment disorder according to the International Classification of Diseases and Related Health Problems, 10th Revision, or the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, and 2) had participated in an RTW program for at least 1 month because of sick leave and returned to work within 1 month after their last program session. The exclusion criteria were: 1) diagnosed with schizophrenia, schizoaffective disorder, bipolar disorder, personality disorder, or developmental disorder, and 2) had lost or changed their job during sick leave. All procedures were approved by the Research Ethics Committee of the Graduate School of Medicine, Nagoya University, Japan in 2018 (No. 2018-0149), and all participants provided informed written consent.
2.1.2RTW program
The RTW program at the clinic in question consists of two sessions per day, 5 days a week, with each session lasting approximately 90 minutes. Therefore, some subjects receive up to 15 session-hours per week. All sessions are conducted in a group setting and consist of cognitive behavioral therapy (CBT), meta-cognitive training for depression (D-MCT), psychoeducation, group discussions, aerobic exercise, sports, relaxation, and individual tasks. Some of the psychoeducation is work-focused, while other interventions focus on both work and daily life; on average, the subjects attend 22 sessions of CBT and MCT. However, the program aims to not only promote participation in each session, but also regulate the rhythm of life and provide opportunities for interactions with others. Therefore, participation in itself, regardless of the content of the sessions, is considered to have a therapeutic effect. The program staff consists of psychiatrists, nurses, clinical psychologists, and occupational therapists. The psychiatrist and nurse have more than 20 years of experience, and the clinical psychologist and occupational therapist have more than 5 years of experience. The subjects were outpatients who were referred to the program by their occupational physicians, supervisors at the workplace, or primary care physicians. The criteria for participation in the program were ultimately determined by program management staff based on the potential benefits from such a program, the unlikelihood of having a significant negative impact on the population, and the targeting of primarily depression. In addition, in consultation with the staff, the subjects determined the type of program they would participate in, the frequency of participation, and the duration of program use.
This RTW program is conducted as a medical practice, and its costs are covered as medical fees. In Japan, due to the existence of a public health insurance system, there are official prices set for these medical fees. As a principle, 70% of the medical fees are paid by the insurer, which is the government. Furthermore, some local governments have systems in place to reduce the patient’s own burden to 10% as well as systems to set a cap on monthly out-of-pocket expenses.
2.1.3Data contents
Demographic and medical data: The demographic data comprised the participants’ age, sex, diagnosis, somatic disease, education level, length of employment, occupation, and position. These were used as of the start date of the program.
Regarding the duration of sick leave and RTW program usage, the following formulas were used during sick leave and throughout the duration of program usage: Duration of sick leave = RTW date –Start date of sick leave, and Duration of program usage = Last date of program use –Start date of program use. Note, however, that RTW was defined as the date when the first full-time work was resumed, and duration of sick leave was defined as the period from the day off until the day full-time work was resumed. In this study, we distinguished between these two periods because generally in Japan, it is rare for employees on sick leave to start program usage on the same date as the start date of sick leave. Sick leave starts when a medical certificate from the physician is submitted to the company manager. By contrast, RTW programs are generally started at a stage equivalent to the recovery phase, after symptoms have been reduced and motivation has been restored.
Depression severity was evaluated using the Beck Depression Inventory-II (BDI-II) [29] every month from the start date of the program. The BDI-II is a self-rating scale calculated as a continuous variable. The reliability and validity of the Japanese version have been confirmed [30]. All participants completed the BDI-II in the clinic during the time between sessions.
Textual data:We used all textual data collected from the participants in the primary study. The data in the electronic medical records were described by the staff members during program use. The textual data included items such as statements and descriptions by the program participants, observations by medical staff, medical examination records, records of regular interviews with program staff, and conference records. Program names, headings, and other descriptions common to all program users were excluded.
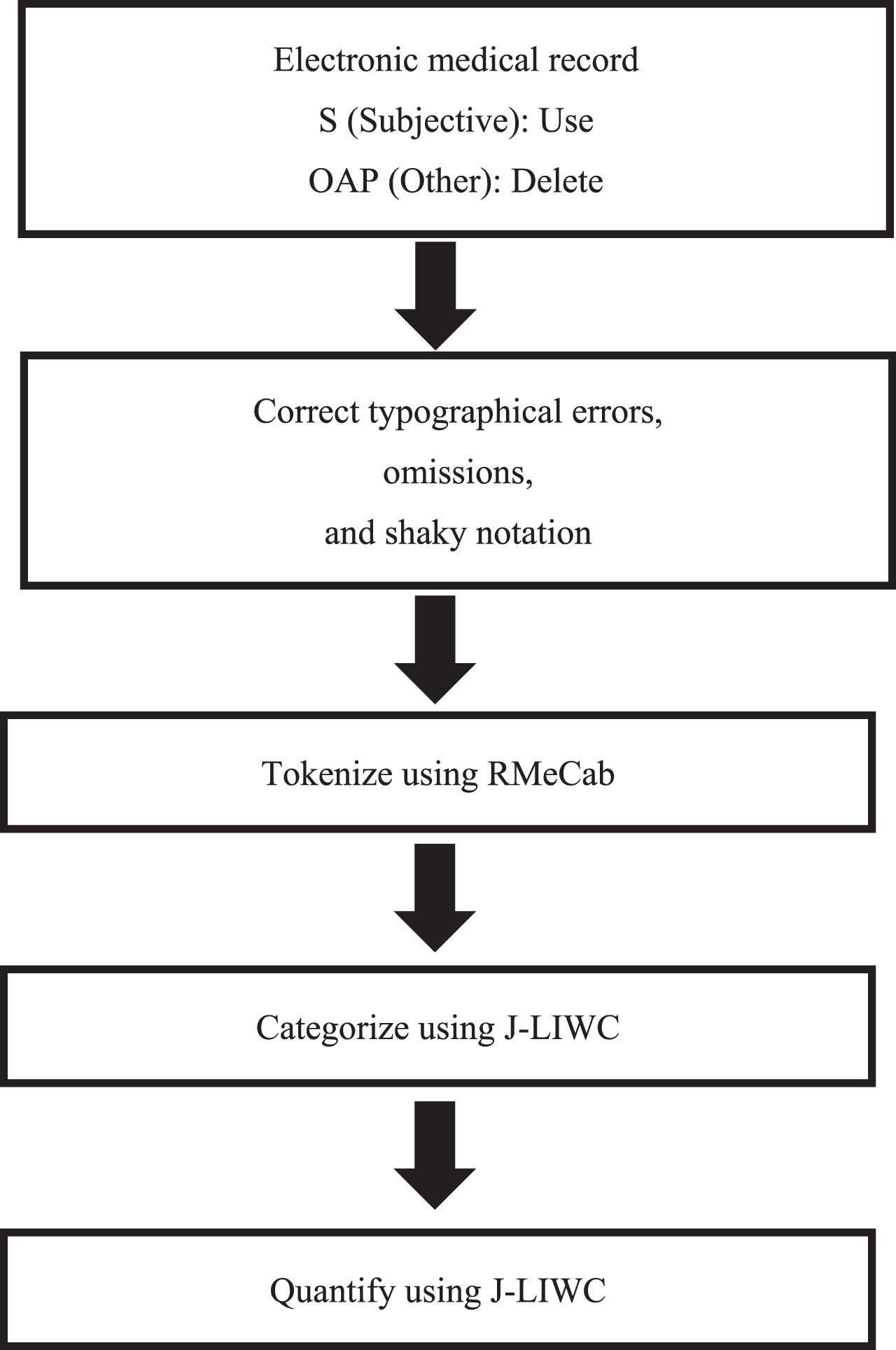
The textual data in the electronic medical records were in free format. Therefore, based on the subjective, objective, assessment, and plan (SOAP) note [31], a problem-oriented documentation method for patient medical charts, we classified the text as subjective (S) and other (OAP). Thereafter, we extracted only the S parts—the subjective part that includes the statements and descriptions of the patients themselves—for each participant and used these for the subsequent procedures. The S part differs from the objective part in that it describes the observations of health-care providers.
Textual data were analyzed after preparation in the primary study as outlined below. Namely, for the quantification of textual data, we conducted text normalization and tokenization.
Text normalization consisted of unifying the differences in notations. As Japanese contains multiple notations (e.g., writing systems, loan words) that express a single word, these were standardized by the three researchers (see [28]) according to specific rules for unifying the differences in notations. Tokenization consisted of dividing sentences into words and transforming them into fundamental forms. Because Japanese is written in “continuous writing,” meaning that the words join each other, it is essential to split the text into words as a preprocessing step for text analysis. Tokenization was conducted using RMeCab [32], a tokenization engine for Japanese.
2.2Data analysis
To quantify the textual data in the primary data and elucidate their relationship with the duration of sick leave through statistical analysis, the following processing and analysis methods were used. Figure 1 shows an overview.
Fig. 1
Overview of the NLP flow.
2.2.1Quantification of textual data
To quantify the textual data, we used the Linguistic Inquiry and Word Count Dictionary (LIWC) [13]. The LIWC is a de facto standard dictionary in the psychological field that is also widely used in the psychiatry field (e.g., [14, 18]). Additionally, the LIWC has been translated into more than 10 languages, and in 2021, a Japanese version (J-LIWC) was also developed [33]. The J-LIWC consists of 69 categories, including unique categories in Japanese, and contains approximately 11,600 words. Using the J-LIWC enabled us to calculate the features of the textual data as linguistic scores. For example, from 21 words in the Japanese fairy tale Momotaro (The Peach Boy), “He got treasures, such as gold and silver. Thus, he went home to his grandparents, where they lived happily ever after”, two words, “treasure” and “happy”, were classified in the emotional category, and one, “live”, was classified in the biological category. Hence, the emotional score was calculated as 0.095 (2/21) and the biological score as 0.048 (1/21). In this study, we divided the textual data of each participant into segments every 2 weeks from the start of the RTW program and treated them as a single document to investigate changes in linguistic scores over time. Then, a linguistic score was calculated for each document.
The J-LIWC has 69 categories, among which, nine are superordinate categories that can be aggregated: language dimension, emotional, social, cognitive, perceptual, biological, motivational, relativity, and informal. The language dimension category is an aggregated category of the grammatical aspects of words, with subcategories such as pronouns, conjunctions, and interrogatives. As the authors of the target text in this study are health-care providers rather than patients, we excluded the language dimension category; the remaining eight categories were used in the analysis. See Table 1 for the details of each category.
Table 1
Details of the J-LIWC categories
| Category | Subcategory | |||||
| Emotional | Posemo | Negemo | Anx | Anger | Sad | |
| Social | Family | Friend | Female | Male | ||
| Cognitive | Insight | Cause | Discrep | Tentat | Certain | Differ |
| Perceptual | See | Hear | Feel | |||
| Biological | Body | Health | Sexual | Ingest | ||
| Motivational | Affiliation | Achieve | Power | Reward | Risk | |
| Relativity | Motion | Space | Time | |||
2.2.2Statistical analysis
We conducted multiple regression analyses using generalized linear mixed models. First, we examined the variation in the BDI-II over time and its relationship with the duration of sick leave. The dependent variable was the BDI-II and the independent variables were time (changes in the BDI-II per month), duration of sick leave, and the interaction between time and duration of sick leave. In this study, we defined “time” as the time from the start of program use to the end of the program. The intercept assumed a random effect for each participant. Due to the lower limit of the BDI-II (0 points), the variance of the data was expressed using a Poisson distribution. Second, we examined variation over time in the textual data in the electronic medical records and its relationship with the duration of sick leave.
The dependent variable was the linguistic score for each of the eight categories (emotional, social, cognitive, perceptual, biological, motivational, relativity, and informal), and the independent variables were time (word changes in electronic medical records per 2 weeks, which was the same duration of depression as indicated by the collected BDI-II), duration of sick leave, and the interaction between time and duration of sick leave. The intercept was assumed to be a random effect for each participant. Because we considered that there were individual differences in the words used by the participants regardless of the duration of the sick leave, the data measured over time was also considered to reflect individual factors. In this analysis, the variance of the data was expressed using a Gaussian distribution. We also formulated regression equations with age, sex, education level, and BDI-II score at the start of program usage. The level of statistical significance was set at 0.05 for all analyses.
3Results
3.1Demographic and medical data
In total, 42 participants were included in this study. The following section presents the details of the participants and the textual data. The mean duration of sick leave before the start of full-time work was 393.71 days (standard deviation [SD] = 205.8 days), and the mean duration of program usage was 167.2 days (SD = 89.2 days). More complete details are shown in Table 2.
Table 2
Characteristics of the participants (n = 42)
| Age (years), mean (SD) | 39.9 (9.6) |
| Sex, n (%) | |
| Male / Female | 39 (92.9%) / 3 (7.1%) |
| Diagnosis, n (%) | |
| Depression / Adjusted disorder | 27 (64.3%) / 15 (35.7%) |
| Somatic disease, n (%) | |
| Yes / No | 14 (33.3%) / 28 (66.7%) |
| Duration of education (years), mean (SD) | 14.6 (2.4) |
| Length of employment (years), mean (SD) | 16.6 (9.9) |
| Occupation, n (%) | |
| Sales work | 2 (4.8%) |
| Clerical work | 11 (26.2%) |
| Engineering or technical work | 27 (64.3%) |
| Public official | 2 (4.8%) |
| Position, n (%) | |
| Higher than manager | 20 (47.6%) |
| General employee | 22 (52.4%) |
| Number of times sick leave was taken to date, n (%) | |
| 1 | 25 (59.5%) |
| 2 | 6 (14.3%) |
| 3 | 7 (16.7%) |
| 4 | 4 (9.5%) |
| Duration of program usage (days), mean (SD) | 167.2 (89.2) |
| Duration of sick leave (days), mean (SD) | 393.7 (205.8) |
| Initial BDI-II (points), mean (SD) | 18.8 (7.6) |
| Final BDI-II (points), mean (SD) | 8.0 (6.7) |
BDI-II = Beck Depression Inventory-II, SD = standard deviation.
3.2Depression severity
The mean BDI-II score at the start of program usage was 18.8 (SD = 7.6). No significant interaction between time and duration of sick leave was found in the BDI-II score based on the results of regression analysis with a generalized linear mixed model (p = 0.270). Table 3 shows the regression coefficient and p-value for different durations of sick leave, time, and their interaction.
Table 3
Results of regression analysis using generalized linear mixed models
| Outcome | Interaction between duration | Main effect of | Main effect of | |||
| Outcome | of sick leave and time | duration of sick leave | time | |||
| β | p | β | p | β | p | |
| BDI-II | 0.02 | 0.270 | –0.05 | 0.746 | –0.12 | 0.000* |
| Emotional | –0.14 | 0.018* | –0.14 | 0.017* | –0.06 | 0.205 |
| Social | –0.15 | 0.009* | –0.17 | 0.011* | 0.13 | 0.014* |
| Cognitive | –0.06 | 0.276 | –0.06 | 0.352 | –0.06 | 0.219 |
| Perceptual | 0.11 | 0.066 | 0.05 | 0.331 | 0.01 | 0.919 |
| Biological | 0.10 | 0.102 | 0.07 | 0.390 | –0.11 | 0.039* |
| Motivational | 0.01 | 0.815 | –0.05 | 0.471 | –0.08 | 0.129 |
| Relativity | 0.03 | 0.649 | 0.05 | 0.466 | 0.18 | 0.000* |
| Informal | –0.11 | 0.071 | –0.12 | 0.067 | 0.17 | 0.001* |
BDI-II = Beck Depression Inventory-II. β: coefficients, p: p-value, *: p < 0.05.
3.3Textual data
3.3.1Number of documents and words
The total number of documents among the 42 participants was 529. The number of words excluding symbols was 465,140 (500.2 words per document, SD = 336.2).
3.3.2Regression analysis
The categories that showed a significant interaction between duration of sick leave and time were social (p = 0.001) and emotional (p = 0.002). Table 3 shows the regression coefficient and p-value for different durations of sick leave, time, and their interaction. Both social and emotional categories increased in proportion over time, with a shorter duration of sick leave showing a greater rate of increase. These results were similar after adjustment for age, sex, education level, and BDI-II score at the start of program usage (See Table 4).
Table 4
Results of regression analysis using generalized linear mixed models adjusted for age, gender, education level, and BDI-II score at the start of program usage
| Outcome | Interaction | Main effect of | Main effect of | Age | Sex | Education | BDI-II score | |||||||
| between duration | duration of | time | level | at the start of | ||||||||||
| of sick leave and time | sick leave | program usage | ||||||||||||
| β | p | β | p | β | p | β | p | β | p | β | p | β | p | |
| Emotional | –0.13 | 0.023* | –0.16 | 0.009* | –0.06 | 0.236 | 0.01 | 0.880 | –0.01 | 0.850 | –0.12 | 0.044* | 0.09 | 0.118 |
| Social | –0.16 | 0.007* | –0.16 | 0.022* | 0.12 | 0.018* | –0.02 | 0.775 | 0.07 | 0.301 | 0.02 | 0.728 | 0.10 | 0.131 |
| Cognitive | –0.06 | 0.300 | –0.05 | 0.424 | –0.06 | 0.228 | 0.03 | 0.583 | 0.03 | 0.597 | –0.03 | 0.673 | –0.02 | 0.780 |
| Perceptual | 0.101 | 0.063 | 0.04 | 0.495 | 0.01 | 0.816 | –0.08 | 0.127 | –0.05 | 0.271 | –0.03 | 0.594 | –0.12 | 0.016* |
| Biological | 0.10 | 0.096 | 0.06 | 0.474 | –0.10 | 0.042 | –0.04 | 0.649 | –0.10 | 0.234 | 0.06 | 0.50 | –0.16 | 0.051 |
| Motivational | 0.01 | 0.8030 | –0.04 | 0.550 | –0.08 | 0.122 | 0.05 | 0.511 | 0.02 | 0.712 | 0.00 | 0.971 | 0.07 | 0.287 |
| Relativity | 0.03 | 0.600 | 0.38 | 0.616 | 0.18 | 0.000* | 0.05 | 0.516 | –0.07 | 0.311 | –0.44 | 0.580 | –0.07 | 0.364 |
| Informal | –0.11 | 0.069 | –0.11 | 0.120 | 0.17 | 0.001* | 0.11 | 0.112 | 0.03 | 0.613 | 0.06 | 0.374 | –0.04 | 0.493 |
BDI-II=Beck Depression Inventory-II. β: coefficients, p: p-value, *: p < 0.05.
4Discussion
The textual data revealed significant interactions between the duration of sick leave and time in the social and emotional categories. On the other hand, the BDI-II scores showed no significant interaction between the duration of sick leave and time.
4.1Social category
The appearance of words belonging to the social category in the S section of the electronic medical records indicates that the participant made statements about others or social interactions in the RTW program. Therefore, the results of this study suggest that as the RTW date approaches, statements related to social interactions increase, and that the rate of increase is greater for those with shorter sick leave periods.
Previous studies have reported that patients with depression have low social skills, including cognitive impairments, as well as difficulties building and maintaining relationships or engaging in conversations [34, 35]. On the other hand, it is also known that treatment with antidepressants and other therapies can improve social skills [36]. Therefore, it is considered that as the RTW program or treatment progresses, contact with others increases and is reflected in the electronic medical records. Additionally, the Japanese government recommends that employees on sick leave have a meeting with their supervisor and attempt a work trial as the RTW date approaches [6]. Work trials in Japan involve spending a short amount of time in the workplace without being given any tasks, or starting with simple tasks for a short period of time. Thus, it is speculated that participants inevitably increase their social contacts just before RTW, and that this is reflected in the results [6].
Furthermore, it is believed that participants with shorter sick leave periods had a faster progression rate until RTW, resulting in a greater increase in social statements.
4.2Emotional category
The occurrence of words belonging to the emotion category of the S of SOAP in the electronic medical records means that the participants made statements in the RTW program that were considered emotionally charged. In other words, the results of this study suggest that the number of emotionally charged statements increases as the RTW date approaches, and that the rate of increase is greater for those who have been on sick leave for a shorter period of time.
Previous studies have reported that patients with depression suppress emotions such as anger [37] and have impaired verbal skills for expressing emotions [38]. On the other hand, it has been reported that treatments such as CBT increase the degree to which emotions are experienced as the patient progresses [39], and that (mainly positive) emotional expression increases with recovery [40]. Therefore, it is likely that as RTW programs and treatment progressed, emotional and verbal expression increased, and this was reflected in the electronic medical records.
In addition, those who had been on sick leave for a shorter period of time may have progressed more quickly to RTW and thus had a greater rate of increase in the amount of social speech.
4.3Depression severity
The results of this study suggest that the RTW program was effective for reducing depression independent of the length of time to RTW, and that there is a weak relationship between recovery from depression and the length of time to RTW. In previous studies, a Cochrane review of interventions for people on sick leave due to depression suggested that interventions for reducing the duration of sick leave differ from those for reducing the severity of depression [41]. In addition, Arima et al. [42] considered RTW readiness, which is the next stage of disease recovery, including interpersonal interaction, task performance, and stress tolerance, to be important for RTW. Based on these findings, we consider it reasonable that no relationship was found between improvement in depression and length of time to RTW in this study.
4.4Clinical implications
As the RTW date approaches, there is an increase in social interaction-related and emotional statements in the S part of the electronic medical record SOAP notes, particularly among those with shorter sick leave periods. This finding is consistent with clinical depression and suggests that the commonly used electronic medical records can be useful in monitoring changes in RTW program users.
One advantage of classifying electronic medical records into SOAP categories is that it allows for the separation of the subjective parts of the patient and the objective parts of the medical staff. In this study, we used SOAP notes to perform NLP only on the subjective parts of the patient in the electronic medical records containing various types of information. By doing so, we were able to show the results in a more easily interpretable form.
In the future, it is expected that more detailed NLP can be implemented by using SOAP note classifications to classify events that occur in the medical field. Additionally, not only electronic medical records, but also NLP for themes presented by the subject in each session of structured interviews or CBT can be conducted to capture the temporal changes in word meanings more clearly. We believe that this study is the first step in demonstrating the potential use of these methods in the RTW field.
4.5Limitations
This study has several limitations. First, the sample size was small and all participants were recruited from a single mental health clinic. Although the clinic belonged to the Japanese Association of RTW for Depression, the results might have been influenced by the characteristics of the facilities and surrounding companies. For instance, the facilities involved in this study are in areas surrounded by many manufacturing companies, which is reflected in the fact that about 65% of the study’s participants are engineering or technical workers. Consequently, the results of this study may differ if conducted in places where sales and clerical workers are prevalent, such as in more urban areas. Furthermore, males made up most of the participants in this study, which suggests that they were influenced by the environment surrounding the clinic. Future studies should increase the number of eligible facilities and aim to eliminate regional influences such as gender differences and occupational variations.
Second, we conducted tokenization to analyze the textual data. Hence, we ignored all contextuality of the textual data. Future studies should also consider contextuality using n-grams or other methods of analysis.
Third, we used only time variation in depression severity, textual data, age, sex, and education level to examine the relationship between changes over time and the duration of sick leave. Previous studies have reported that other factors (e.g., comorbidities, income) are also related to RTW [8]. In future studies, we expect to analyze our results together with other factors related to RTW to elucidate more multifaceted aspects of the prolonged duration of sick leave.
Fourth, the factor involving staff who write the electronic medical records should be noted. Electronic medical records are not written by the participants themselves, but rather, by members of the medical staff who manage the program. Therefore, we suspect that variations due to the specialties and skills of the medical staff also influenced the results. In the future, it will be necessary to consider how to eliminate factors depending on the medical staff who describe the electronic medical records. Future studies should take these findings into account and investigate them in more detail.
5Conclusion
The results of this study indicate that words in the social and emotional categories increased over time in the S portion of the electronic medical records in an RTW program for depression. These factors may affect the duration of sick leave. Nevertheless, based on the results of this study, further research is necessary because of the various factors affecting sick leave and RTW.
Acknowledgments
The authors are grateful to all participants who provided data for this study. They are also grateful to the clinical staff and students of the Department of Integrated Health Science, Graduate School of Medicine, Nagoya University for supporting this research.
Ethical Approval
All procedures were approved by the Research Ethics Committee of the Graduate School of Medicine, Nagoya University, Japan in 2018 (No. 2018-0149).
Informed Consent
All participants provided written informed consent.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
This work was supported by JST SPRING and JSPS KAKENHI (Grant No. JP18K17716).
References
[1] | Lelliott P , Boardman J , Harvey S , Henderson M , Knapp M , Tulloch S Mental Health and Work: A Report for the National Director forWork and Health.Working for Health. London: Royal College of Psychiatrists. 2008. |
[2] | Heisei30nendo“karoushinadonorousaihosyoujyoukyou” [Internet]. Ministry of Health, Labor and Welfare. 2019 [cited 2021 Jul 31]. Available from: https://www.mhlw.go.jp/stf/newpage_05400.html |
[3] | Reiwa2nenroudouannzeneiseityosa (jittaityosa) [Internet]. Ministry of Health, Labour and Welfare. 2020 [cited 2021 Jul 31]. Available from: https://www.mhlw.go.jp/toukei/list/r02-46-50b.html |
[4] | Jisatsu/Utsutaisakunokeizaitekibeneki (jisatsuyautsuniyo rushakaitekisonshitsu) [Internet]. Ministry of Health, Labor and Welfare. 2010 [cited 2021 Jul 31]. Available from: https://www.mhlw.go.jp/stf/houdou/2r9852000000qvsy.html |
[5] | Stress check nadonosyokubaniokeru mental health taisaku/ kajyurodotaisakunado [Internet]. Ministry of Health, Labor and Welfare. Available from: https://www.mhlw.go.jp/bunya/roudoukijun/anzeneisei12/index.html |
[6] | Kokoronokenkomondainiyorikyugyositarodosyanosyokub ahukkishiennotebiki [Internet]. Ministry of Health, Labour and Welfare. 2019 [cited 2021 Jul 31]. Available from: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000055195_00005.html |
[7] | Igarashi Y , Ooki Y Rework program riyoshatohiriyosh anosyuroyogonikansuruhikakukokakenkyu. MHLW GRA NTS Syst. 2012; |
[8] | Ervasti J , Joensuu M , Pentti J , Oksanen T , Ahola K , Vahtera J , et al. Prognostic factors for return to work after depression-related work disability: A systematic review and meta-analysis. J Psychiatr Res. (2017) ;95: :28–36. |
[9] | Attribution CC , License I , Issn P , Issn E . Meta-synthesis of qualitative research on return to work among employees with common mental disorders (2022) ;38: (2):93–104. |
[10] | Scharf J , Angerer P , Müting G , Loerbroks A Return to Work after Common Mental Disorders: A Qualitative Study Exploring the Expectations of the Involved Stakeholders. 2020; |
[11] | Zung WWK . A Self-Rating Depression Scale. Arch Gen Psychiatry. (1965) ;12: (Jan):63–70. |
[12] | Kessler RC , Barber C , Beck A , Berglund P , Cleary PD , McKenas D , et al. The World Health Organization Health and Work Performance Questionnaire (HPQ). J Occup Environ Med. (2003) ;45: (2):156–74. |
[13] | Pennebaker JW , Mehl MR , Niederhoffer KG . Psychological Aspects of Natural Language Use: Our Words, Our Selves. Annu Rev Psychol. (2003) ;54: :547–77. |
[14] | Buck B , Penn DL . Lexical Characteristics of Emotional Narratives in Schizophrenia. J Nerv Ment Dis. (2015) ;203: (9):702–8. |
[15] | Brockmeyer T , Zimmermann J , Kulessa D , Hautzinger M , Bents H , Friederich HC , et al. Me, myself, and I: Self-referent word use as an indicator of self-focused attention in relation to depression and anxiety. Front Psychol. (2015) ;6: (OCT):1–10. |
[16] | Rosenbach C , Renneberg B . Remembering rejection: Specificity and linguistic styles of autobiographical memories in borderline personality disorder and depression. J Behav Ther Exp Psychiatry [Internet]. (2015) ;46: :85–92. Available from: https://doi.org/10.1016/j.jbte2014.09.002 |
[17] | Dirkse D , Hadjistavropoulos HD , Hesser H , Barak A . Linguistic analysis of communication in therapist-assisted internet-delivered cognitive behavior therapy for generalized anxiety disorder. Cogn Behav Ther. (2015) ;44: (1):21–32. |
[18] | Zimmermann J , Brockmeyer T , Hunn M , Schauenburg H , Wolf M . First-person Pronoun Use in Spoken Language as a Predictor of Future Depressive Symptoms: Preliminary Evidence from a Clinical Sample of Depressed Patients. Clin Psychol Psychother. (2017) ;24: :384–91. |
[19] | Smirnova D , Cumming P , Sloeva E , Kuvshinova N , Romanov D , Nosachev G Language patterns discriminate mild depression from normal sadness and euthymic state. Front Psychiatry. 2018;9(APR). |
[20] | Al-Mosaiwi M , Johnstone T . In an absolute state: elevated use of absolutist words is a marker specific to anxiety, depression, and suicidal ideation. Clin Psychol Sci. (2018) ;6: (4):529–42. |
[21] | Trifu RN , Nemeş B , Bodea-Haţegan C , Cozman D Linguistic indicators of langjage in major depressive disorder (MDD) an evidence based research. J Evidence-Based Psychother. (2017) ;17: (1):105–28. |
[22] | Alpert M , Pouget ER , Silva RR . Reflections of depression in acoustic measures of the patient’s speech. J Affect Disord. (2001) ;66: :59–69. |
[23] | Rude SS , Gortner EM , Pennebaker JW . Language use of depressed and depression-vulnerable college students. Cogn Emot. (2004) ;18: (8):1121–33. |
[24] | Sloan DM . It’s all about me: Self-focused attention and depressed mood. Cognit Ther Res. (2005) ;29: (3):279–88. |
[25] | Tania MH , Hossain R , Jahanara N , Andreev I , Clifton DA Thinking Aloud or Screaming Inside: Exploratory Study of Sentiment Around Work Corresponding Author: 2022;6. |
[26] | Kristen Kim , Gordon Y , Angela Maria Haddad , Nicholas Kos , Sidney Zisook JED . Thematic analysis and natural language processing of job-related problems prior to psysician suicide in -Suicide Life-Threatening Behav (2022) ;52: (5):1002–11. |
[27] | Lee S , Kim H , Kim H . Prospect of Artificial Intelligence Based on Electronic Medical Record (2021) ;10: (3):282–90. |
[28] | Kutsuna I , Hoshino A , Morisugi A , Mori Y , Shirato A , Takeda M , et al. Relationship between emotional words in electronic medical records and leave periods of users of a return-to-work program with depression. Br J Occup Ther. 2022; |
[29] | Beck AT , Steer RA , Brown GK Manual for the Beck Depression Inventory-2. San Antonio, Texas: Psychological Corporation; 1996. |
[30] | Kojima M , Furukawa TA , Takahashi H , Kawai M , Nagaya T , Tokudome S . Cross-cultural validation of the Beck Depression Inventory-II in Japan. Psychiatry Res. (2002) ;110: :291–9. |
[31] | Joseph DP . SOAP is good for medical record. Arch Intern Med. (1992) ;152: (12):2511. |
[32] | Ishida M RMeCab: interface to MeCab. 2019 p. R package version 1.04. |
[33] | Igarashi T , Okuda S , Sasahara K Development of the Japanese Version of the Linguistic Inquiry andWord Count Dictionary 2015. Front Psychol. 2022;13(March). |
[34] | Tse WS , Bond AJ . The Impact of Depression on Social Skills: A Review. J Nerv Ment Dis. (2004) ;192: (4):260–8. |
[35] | Chris S . Social Skills Deficits Associated With Depression. Clin Psychol Rev [Internet]. (2000) ;20: (3):379–403. Available from: https://ac.els-cdn.com/S0272735898001044/1-s2.0-S0272735898001044-main.pdf?_tid=d466bf01-3cbb-48c8-b40f-350850f73847&acdnat=1537793245_49d804949779424140dd8ce969b5ab58 |
[36] | Weissman MM . Social Functioning and the Treatment of Depression r py ig a du s (2000) ;61: (suppl 1):33–8. |
[37] | Luutonen S . Anger and depression - Theoretical and clinical considerations. Nord J Psychiatry. (2007) ;61: (4):246–51. |
[38] | Pietrzak T , Lohr C , Jahn B , Hauke G . Embodied cognition and the direct induction of affect as a compliment to cognitive behavioural therapy. Behav Sci (Basel). (2018) ;8: (3) |
[39] | Mackay HC , Barkhama M , Stiles WB , Goldfriedc MR . Patterns of client emotion in helpful sessions of cognitive-behavioral and psychodynamic-interpersonal therapy. J Couns Psychol. (2002) ;49: (3):376–80. |
[40] | Boumparis N , Karyotaki E , Kleiboer A , Hofmann SG , Cuijpers P . The effect of psychotherapeutic interventions on positive and negative affect in depression: A systematic review and meta-analysis. J Affect Disord [Internet]. (2016) ;202: :153–62. Available from: https://doi.org/10.1016/j.jad.2016.05.019 |
[41] | Nieuwenhuijsen K , Faber B , Verbeek J , Neumeyer-Gromen A , Hees H , Verhoeven A , et al. Interventions to improve return to work in depressed people. Cochrane Database Syst Rev. (2014) ;(12). |
[42] | Arima H , Akiyama T , de Moura PA , Bernick P , Sakai Y , Ozaki Y , et al. Resilience building for mood disorders: Theoretical introduction and the achievements of the Re-Work program in Japan. Asian J Psychiatr [Internet]. (2021) ;58: :102580. Available from: https://doi.org/10.1016/j.ajp.2021.102580 |


