
Changes in memory and attention during and after occupational rehabilitation: A longitudinal study
Abstract
BACKGROUND:
There is need for more knowledge about the relationship between work and cognitive functioning in sick-listed individuals.
OBJECTIVE:
This study investigated whether the degree of work participation is relevant for recovery of cognitive functioning in sick-listed individuals.
METHODS:
177 occupational rehabilitation participants and 70 controls participated in a non-randomised, longitudinal study. Participants completed computerised cognitive tests targeting sustained attention and working memory at start and end of rehabilitation and 3 and 12 months after rehabilitation. The change score performance in attention and memory between start and end, start and 3 months and 12 months was compared in individuals on sick leave 100–75%, 74–40% and 39–0% (three sick leave groups) of the time in the year after rehabilitation, and a control group not being on sick leave. Fixed effect analysis of covariance adjusting for education and work ability was used.
RESULTS:
The sick leave group 100–75% had significantly lower score on work ability compared to the other groups at baseline. The main findings indicated that the sick leave group 39–0% improved significantly more in sustained attention compared to the sick leave group 100–75% between start and end of rehabilitation and from start of rehabilitation to 3 and 12 months after.
CONCLUSION:
The degree of work participation seems relevant to recovery of the cognitive function sustained attention in sick-listed individuals. These findings encourage work rehabilitation clinicians, work consultants and employers to develop RTW plans which take into account that graded employment influence cognitive functioning.
1Introduction
There is need for more knowledge about the relationship between work and cognitive functioning in sick-listed individuals and especially for how to preserve good cognitive health. Mental demands at work, also named cognitive job complexity, stimulate the brain [1, 2] and contribute to staying mentally healthy by engaging cognitive functions [3]. Stimulating cognitive functions is argued to build up a cognitive reserve that acts as a buffer against premature cognitive decline [4]. Both mental and physical work demands, as well as stimulating cognitive effort during daily life activities, may boost the reserve [1–3]. Cognitive health in old age is partly dependent upon being engaged in intellectually and complex work tasks and activities that are demanding [1]. This empirical knowledge emphasises that the nature of the work tasks, that is, the degree of cognitive job complexity afforded by the job role, positively affects cognition.
Another way of investigating whether work positively affects cognition is to assess whether the amount of time spent in work plays a role. Research has to a large extent focused on the relationship between retirement and cognitive aging [5], while the degree of work participation and its impact on cognitive functioning has received less attention [6, 7]. One way of investigating how the degree of work participation could influence cognitive functioning is to compare whether different degrees of work participation in sick-listed individuals could influence memory and attention after occupational rehabilitation. This assumption has implications for individuals on sick leave where the aim is return to work (RTW) because sick-listed individuals show impairments in both cognitive (sustained attention, spatial awareness, psychomotor speed) and executive functions (inhibition, working memory, cognitive flexibility), also compared to working individuals, not on sick leave [8–12]. Inpatient and outpatient occupational rehabilitation are forms of work-related rehabilitation and psychological treatment, where referred individuals commonly report musculoskeletal pain and common mental health complaints such as anxiety and depression [13]. Enhancing the knowledge about the cognitive performance and changes in sick-listed individuals could result in the application of more efficacious cognitive treatment components in rehabilitation programmes [9] and clinical practice [14]. The result being that individuals are better equipped to handle cognitively complex work tasks [5] and better cope with mental demands at work [1, 15].
The focus of this study is to explore the degree to which the amount of time spent at work positively influences memory and attention. These two domains were selected because it has been shown that attention and memory functions improve more than executive function and emotion regulation in occupational rehabilitation patients [9, 10] as well as being associated with RTW [16]. Sustained attention and working memory were specifically selected as the cognitive constructs in the current study. Sustained attention helps us to hold focus and engagement on a task over time and is most commonly related to monotonous activities [17]. Working memory is a limited and short-term capacity store for holding information and for engaging the information of this store [18]. Improvements in sustained attention and higher scores in working memory are also associated with reduced sick leave rates in the year following rehabilitation [16]. The opposite has also been documented, that impairments in working memory is associated with a higher chance of being unemployed or full-time sickness absent [14]. These findings suggest that certain cognitive functions are implicated in the RTW process.
In the current study, cognitive functioning at start and end of rehabilitation and at three and 12 months after start was measured. The rehabilitation sample was divided into three sick leave groups based on how much each individual was on sick leave in the year after rehabilitation: 100–75%, 74–40% and 39–0%. The individuals belonging to these categories and a control group were compared in order to investigate whether there were differences in improvements in sustained attention and working memory both during and after rehabilitation, thus extending previous findings [9, 10, 16]. It was hypothesised that the degree of work participation is relevant to recovery of cognitive functioning in sick-listed individuals after occupational rehabilitation, where higher work participation would result in larger improvement in sustained attention and working memory. Cognitive functioning was also assessed at the end of rehabilitation before returning to work to explore whether changes during rehabilitation differed from changes after.
2Methods
2.1Design
A non-randomised longitudinal cohort design was used where computerised cognitive tests targeting sustained attention and working memory and questionnaires about work and health, were administered at start of rehabilitation (T1), end of rehabilitation (T2), 3 (T3) and 12 (T4) months after start of rehabilitation. The outcome measures for the cognitive tests were change scores between T1-T2, T1-T3 and T1-T4. The data collection for the control group was conducted at the same intervals as the rehabilitation group. This study used objective register data on health-related benefits, here named sick leave days, from the Norwegian Labour and Welfare Organization. This register provides accurate data on graded sick leave from 0-100% because all individual benefits with start and end dates are registered by general practitioners, physicians, or jobcentres (also named social security offices which are run by the Norwegian Labour and Welfare Organization) in the health-related benefit system. If someone is registered with no sick leave, it is assumed that the person is working. The following procedure was used to define the degree of sick leave: First, the total number of sick leave days in the year after rehabilitation (T2-T4) was counted and converted to whole days for each participant if sick leave was graded. That is, days on health-related benefits were adjusted for graded sick leave according to employment fraction. Second, the total number of sick leave days was divided by the total number of days between measurement point T2 and T4 to calculate the percentage of days each participant was on sick leave (the number of days between each measurement point varied between participants). Based on this percentage, three groups were created: 100–75%, 74–40% and 39–0% sick leave in the year after rehabilitation. The cognitive performance in the three sick leave groups and a control group was compared on sustained attention and working memory.
2.2Participants
177 study participants were recruited from four occupational rehabilitation clinics. The participants were diagnosed by their general practitioner according to ICD-10, mainly in category M, diseases of the musculoskeletal system and connective tissue (50%) and category F, mental and behavioural disorders (35%). The inclusion criteria were participation in occupational rehabilitation at one of the four clinics and completing the rehabilitation programme. Participants reporting a history of head injury were excluded from the study because it could impair cognitive functioning [5]. Those having applied for full disability pension either prior to or during rehabilitation were also excluded. The control group was the same as in Johansen et al. [9] and were individuals from the wider community and employees from three rehabilitation clinics. The 70 healthy controls were all working full time of their weekly contracted hours. This was obtained through self-report and the controls were therefore not on sick leave or attended rehabilitation during the study period.
2.3Intervention and health-related benefit system
Inpatient and outpatient occupational rehabilitation is one of several work-related interventions offered by the specialist health care system and by the Norwegian Labour and Welfare Organization in Norway. Most referrals come from general practitioners and the decision is taken in collaboration with the patient. Individuals referred for occupational rehabilitation represent workers in education and schooling, health care and marketing, sales and service and physical and manual workers [19, 20]. The main reasons for referrals are long term sick leave and motivation to RTW and are thus independent of medical diagnosis. Sick leave could be either work-related, non-work related and/or in combination with health-related issues. The main aim at all four clinics was RTW and included an assessment of work ability and physical fitness at arrival. An interdisciplinary team is responsible for the patient activities and consultations during rehabilitation and consist of a physician, physiotherapist, psychologist, work consultant/coach, nurse/psychiatric nurse and sports pedagogue. The rehabilitation programme starts with an assessment of work-related and health-related barriers and facilitators. Based on this assessment, both individual and group activities are individually tailored during rehabilitation of which the key interventions are adapted physical activity such as supervised exercise adjusted to the person’s needs and physical capacity (e.g. indoor cycling, outdoor walking, resistance exercise, endurance exercise) and cognitive behaviour treatment components based on a cognitive approach focusing on work and health [21]. “The cognitive approach utilise principles based on work-focused cognitive behaviour therapy, acceptance and commitment therapy and psychoeducation for anxiety, depression, pain; adapted physical activity and the effects on body and mind; behavioural activation relevant for depression; skills training in problem solving; mindfulness; pain education; fear avoidance beliefs and exposure principles at work and during physical activity” [9].
On a general note, the content of rehabilitation was the same for all participants, although, and naturally, there exist some programme differences between the clinics. The length of the rehabilitation programme offered at the four clinics varied from 3 to 12 weeks. Other main differences concerned the types and frequency of specific physical activities offered, such as cycling, walking, swimming, running, rowing, the usage of outdoor versus indoor facilities, the number of RTW consultations with the personnel in the interdisciplinary team, the extent to which the employer, workplace, general practitioner and jobcentre were involved during rehabilitation and types of mindfulness and meditation exercises.
The Norwegian sickness insurance scheme cover all individuals on sick leave. Full wage compensation is provided by the tax-paid national insurance system up to one year of which the employer covers the first 16 days of sick leave. Further compensation is granted if the individual is not able to RTW after one year, with benefits reduced to two thirds of full wages. The benefits are adjusted accordingly if partial sick leave is chosen.
2.4Cognitive and questionnaire assessment
Assessment of cognitive function was undertaken in a quiet room by trained administrators using validated computerised tests from the Cambridge Neuropsychological Test Automated Battery (CANTAB) [22]. At www.camcog.com more information is provided about the tests as well as access to other studies having applied CANTAB in different target groups. The cognitive tasks have been standardised in a large group of normal subjects [23]. The standardised test procedure makes CANTAB applicable and feasible to use in everyday clinical settings, comparing test results against healthy controls and across different population groups [24, 25]. Also, each test has several difficulty levels limiting performances in the floor and ceiling ends. The performance from two tests measuring sustained attention and working memory was analysed. These two tests were part of a battery of eight tests targeting the domains attention, memory, executive function and emotion recognition. At each time point (T1-T4) the testing took approximately one hour to complete. The tests were administered and counterbalanced in two prearranged orders to ensure that tests targeting the same cognitive functions did not appear after each other. The participants completed a motor screening task before completing the eight tests to reduce any worry related to testing and familiarise themselves with the touch screen. The choice of tests selected in the current study have solid psychometric properties [25, 26] and have been extensively used in populations reporting anxiety [27], depression [28] and pain [29]. It is argued however that traditional cognitive and neuropsychological tests could have limited ecological validity [30].
The task information given to the participants is standardised and outlined in CANTAB manuals [22]: 1. Sustained attention: On the rapid visual information processing task, the participants have to detect and respond by pressing a button on a press pad to target sequences 3-5-7, 2-4-6, and 4-6-8, from digits between 2 and 9 appearing one at a time in a pseudo-random order, at the rate of 100 digits per minute, lasting four minutes. The dependent variables were calculated as the mean correct response latency and probability of hit; 2. Working memory: The spatial working memory task is self-ordered and requires participants to search for yellow tokens hidden inside an array of boxes. The participants select the box they want to open and once a token is found, they place it in a column area called ‘home’ on the right-hand side of the screen. Then a new token is hidden in a different box because a token never appears in the same box twice during the same search sequence and the number of tokens to be found corresponds to the number of boxes on the screen. The trial is completed when a token has been found in each box. Four practice trials are given, each with three boxes. The assessed trials included two blocks of four, six, and eight boxes. The dependent variable was calculated as the mean total number of between-search errors (returning to a box where a token has already been found during the same trial).
The following self-reported questionnaires were administered and took approximately 30 minutes to complete at each time point: Work ability was assessed using one item from the work ability index [31] “comparing current work ability with the lifetime best” ranging from 0 = completely unable to work to 10 = lifetime best [32]. The work ability index has been found to be a valid and reliable measure of work ability [31] and the one item work ability correlates strongly with the total work ability score from the index [32]. Subjective health complaints (SHC) were measured with the SHC Inventory [33], a 29-item questionnaire targeting common health complaints during the last month, rated on a 4-point scale. The questionnaire has satisfactory validity and reliability [33]. Fear avoidance beliefs was assessed with the Fear Avoidance Beliefs Questionnaire (FABQ) [34] targeting fear avoidance for work (four items on a 7-point scale) and physical activity (seven items on a 7-point scale). Acceptable reliability and construct validity have been confirmed in the Norwegian version [35]. Anxiety and depressions symptoms were captured with the Hospital Anxiety and Depression Scale (HADS) [36] and rated on a 4-point scale (seven items each for anxiety and depression). The Norwegian version has been found to have adequate reliability and validity [37].
2.5Statistical analysis
Demographic, work and health characteristics at baseline were compared between the three sick leave groups using univariate analysis of variance (ANOVA) and chi-square tests and presented as means and standard deviation or numbers and percentages. The three sick leave groups and the control group were also compared on the same variables. Change scores from T1-T2, T1-T3 and T1-T4 for sustained attention and working memory were calculated and compared between patients in the three sick leave groups 100–75%, 74–40% and 39–0% and the control group. The four groups were matched for age and sex. Data were analysed using fixed effects analysis of covariance (ANCOVA) with change scores in sustained attention and working memory performance as the dependent variable, group as fixed factor, and one item work ability and education as covariates. If the overall ANCOVA was significant, post hoc least significant difference tests were conducted to compare the four groups in a pairwise fashion. Both mean and estimated marginal mean were calculated. Corrections for multiple post hoc comparisons were carried out by accepting statistical significance at a two-tailed p-value of 0.025 for sustained attention since two dependent variables were used in the analysis (latency and hit). For working memory, a p-value of 0.05 was used because one dependent variable was used in the analysis (between-search errors). Partial eta-squared (η2p) was used as the effect size measure adhering to the suggested values [38]: below 0.06 small, 0.06–0.14 moderate and above 0.14 large. Data were analysed using SPSS version 28.
3Results
The demographic, work, health and cognitive characteristics at baseline in the three sick leave groups are presented in Table 1. The groups differed in self-reported work ability where the sick leave group 100–75% had significantly lower score compared to the 74–40% and 39–0% groups.
Table 1
Demographic, work, health and cognitive characteristics at baseline for the three sick leave groups [X2 = chi-square statistic; F = univariate analysis of variance (ANOVA); SD = standard deviation; # Note that degrees of freedom differ between measures as participants were not mandated to answer all questions, since some questions could be found to be of sensitive nature and not all participants were able to complete the rapid visual information processing task due to its demanding procedure]
| Sick leave | Sick leave | Sick leave | Statistics | |||||
| 100–75% | 74–40% | 39–0% | ||||||
| (n = 56) | (n = 32) | (n = 89) | ||||||
| Variable | Mean | SD | Mean | SD | Mean | SD | F (df)# | p-value |
| Age | 46.6 | 8.6 | 48.5 | 8.7 | 45.2 | 9.6 | 1.61 (2,174) | 0.203 |
| Work ability (0–10; 10 = best work ability) | 2.5 | 2.0 | 3.3 | 1.8 | 4.6 | 2.4 | 16.57 (2,174) | <0.001 |
| Subjective Health Complaints Inventory (SHC) | ||||||||
| Pseudoneurology (0–21; 21 = most complaints) | 8.0 | 4.1 | 7.4 | 4.4 | 6.8 | 3.7 | 1.48 (2,168) | 0.231 |
| Musculoskeletal pain (0–24; 24 = most complaints) | 9.5 | 5.2 | 10.7 | 4.4 | 9.1 | 5.1 | 1.07 (2,168) | 0.346 |
| Fear Avoidance Beliefs Questionnaire (FABQ) | ||||||||
| Work (0–42; 0 = no fear avoidance) | 21.7 | 11.4 | 19.8 | 11.0 | 18.6 | 10.9 | 1.17 (2,155) | 0.314 |
| Physical activity (0–24; 0 = no fear avoidance) | 9.7 | 5.6 | 9.1 | 5.3 | 8.4 | 5.9 | 0.80 (2,158) | 0.450 |
| Hospital Anxiety and Depression Scale (HADS) | ||||||||
| Anxiety (0–21; 0 = no anxiety) | 8.8 | 4.5 | 8.0 | 3.4 | 8.2 | 4.7 | 0.34 (2,167) | 0.713 |
| Depression (0–21; 0 = no depression) | 6.9 | 4.1 | 6.2 | 3.8 | 6.0 | 4.1 | 0.90 (2,167) | 0.408 |
| Rapid Visual Information Processing (response latency milliseconds) | 391.2 | 81.1 | 399.6 | 77.1 | 411.5 | 93.3 | 0.92 (2,168) | 0.402 |
| Rapid Visual Information Processing (probability of hit) | 0.61 | 0.22 | 0.64 | 0.19 | 0.63 | 0.15 | 0.25 (2,169) | 0.776 |
| Spatial Working Memory (total between errors) | 12.9 | 10.3 | 12.9 | 10.0 | 11.9 | 9.7 | 0.23 (2,174) | 0.796 |
| Variable | n | % | n | % | n | % | X2 (df) | p-value |
| Gender | ||||||||
| Female | 40 | 71 | 25 | 78 | 57 | 64 | 2.42 (2) | 0.298 |
| Male | 16 | 29 | 7 | 22 | 32 | 36 | ||
| Education | ||||||||
| Elementary | 12 | 21 | 1 | 3 | 9 | 10 | 7.83 (4) | 0.098 |
| Secondary | 20 | 36 | 17 | 53 | 41 | 46 | ||
| Higher | 24 | 43 | 14 | 44 | 39 | 44 | ||
| Diagnostic codes from the ICD-10 | ||||||||
| Diseases of the musculoskeletal system and connective tissue | 24 | 43 | 14 | 44 | 51 | 57 | 4.18 (4) | 0.383 |
| Mental and behavioral disorders | 22 | 39 | 14 | 44 | 26 | 29 | ||
| Other diagnostic codes | 10 | 18 | 4 | 12 | 12 | 14 | ||
The three sick leave groups were also compared to the control group (results not shown), and it was found that the groups did not differ in age and gender. Level of education was found to differ, with a larger percentage of individuals in the control group (43%) completing higher education compared to the three sick leave groups (18% in the group 100–75%, 10% in 74–40% and 29% in 39–0%). As expected, the control group reported significantly higher work ability at baseline and significantly lower scores on the SHC factors pseudoneurology and musculoskeletal pain, lower fear avoidance for work and physical activity and less anxiety and depression symptoms. In cognitive functioning, the control group had significantly higher probability of hit on the rapid visual information processing task (0.70) compared to the sick leave groups 100–75% (0.61) and 39–0% (0.63).
3.1Changes in sustained attention during rehabilitation
Figure 1 and Table 2 display change scores in sustained attention and working memory for the time periods T1-T2. Differences between the four groups were found for sustained attention on the variable response latency. Pairwise comparisons revealed that the sick leave groups 74–40% and 39–0% improved significantly more in sustained attention compared to the sick leave group 100–75% (p = 0.020 and 0.001 respectively).
Fig. 1
Change scores from T1-T2 (top), T1-T3 (middle) and T1-T4 (bottom) for response latency on the rapid visual information processing task displayed as estimated marginal means with error bars showing 95% confidence intervals and the covariates education and one item work ability appearing in the model for the sick leave groups 100–75%, 74–40%, 39–0% and control group.
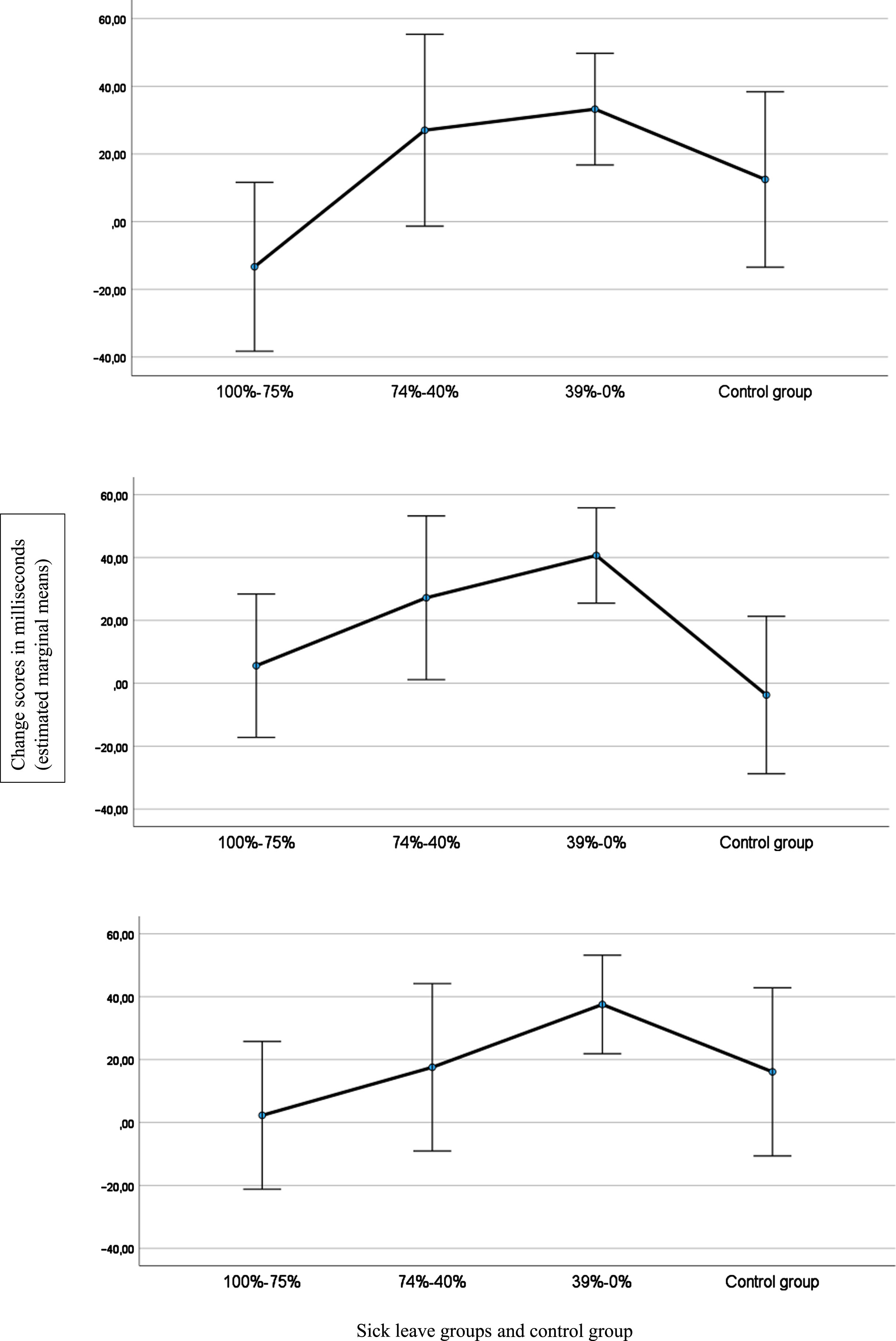
Table 2
Comparison of change scores in sustained attention and working memory for the time periods T1-T2, T1-T3 and T1-T4 between individuals in the sick leave categories 100–75%, 74–40%, 39–0% and control group in 12 months follow up period. [df = degrees of freedom; EMM = estimated marginal means evaluated with covariates education and one item work ability in the model; η2p = partial eta squared; SD = standard deviation]; # Degrees of freedom differ between measures as some participants were not able to attend the T3 and T4 testing sessions]
| Sick leave | Sick leave | Sick leave | Control group | Statistics | ||||||||||||
| 100–75% | 74–40% | 39–0% | (n = 70) | |||||||||||||
| (n = 56) | (n = 32) | (n = 89) | ||||||||||||||
| Variables | Time period | Change score | SD | EMM | Change score | SD | EMM | Change Score | SD | EMM | Change score | SD | EMM | F (df)# | p-value | η2p |
| Rapid Visual Information Processing | ||||||||||||||||
| Response latency (milliseconds) | T1-T2 | –9.9 | 85.6 | –13.4 | 29.5 | 61.0 | 27.0 | 34.1 | 78.6 | 33.2 | 7.8 | 71.4 | 12.5 | 4.243 (3, 235) | 0.006 | 0.05 |
| T1-T3 | 1.9 | 75.9 | 5.6 | 24.9 | 62.7 | 27.2 | 39.7 | 66.8 | 40.6 | 1.7 | 73.7 | –3.7 | 4.884 (3, 228) | 0.003 | 0.06 | |
| T1-T4 | 4.7 | 67.2 | 2.3 | 20.5 | 68.0 | 17.6 | 37.2 | 76.3 | 37.5 | 12.8 | 72.6 | 16.1 | 2.682 (3, 218) | 0.048 | 0.04 | |
| Probability of hit | T1-T2 | –0.09 | 0.13 | –0.08 | –0.11 | 0.15 | –0.11 | –0.10 | 0.15 | –0.10 | –0.05 | 0.15 | –0.05 | 0.978 (3, 236) | 0.404 | 0.01 |
| T1-T3 | –0.10 | 0.14 | –0.09 | –0.12 | 0.16 | –0.12 | –0.13 | 0.17 | –0.13 | –0.11 | 0.13 | –0.11 | 0.746 (3, 229) | 0.526 | 0.01 | |
| T1-T4 | –0.14 | 0.17 | –0.14 | –0.12 | 0.16 | –0.12 | –0.16 | 0.14 | –0.16 | –0.10 | 0.15 | –0.11 | 0.992 (3, 218) | 0.397 | 0.01 | |
| Spatial Working Memory | ||||||||||||||||
| Total between errors | T1-T2 | 1.5 | 8.0 | 1.7 | 2.7 | 7.8 | 2.7 | 1.2 | 7.5 | 1.3 | 1.1 | 9.0 | 0.8 | 0.256 (3, 241) | 0.857 | 0.01 |
| T1-T3 | 2.5 | 8.0 | 2.5 | 0.8 | 9.4 | 0.7 | 2.3 | 7.9 | 2.4 | 2.3 | 8.8 | 2.2 | 0.353 (3, 234) | 0.787 | 0.01 | |
| T1-T4 | 2.3 | 6.7 | 2.3 | 4.6 | 10.0 | 4.5 | 2.5 | 8.1 | 2.5 | 1.3 | 8.5 | 1.3 | 0.765 (3, 223) | 0.515 | 0.01 | |
3.2Changes in sustained attention after rehabilitation
Change scores in sustained attention and working memory for the time periods T1-T3 and T1-T4 indicated differences in sustained attention on the variable response latency between T1-T3 and T1-T4. Pairwise comparisons revealed that the sick leave group 39–0% improved significantly more in sustained attention compared to the sick leave group 100–75% between T1-T3 (p = 0.009) and T1-T4 (p = 0.011), and compared to the control group between T1-T3 (p = 0.005). Change scores are shown in Fig. 1 for the four groups as estimated marginal means for the variable response latency.
4Discussion
This study explored the assumption that exposure to work produces improvements in cognitive functioning in people whose abilities may have deteriorated due to absence from the workforce. It was hypothesised that higher work participation is associated with larger amounts of improvement in sustained attention and working memory. Results seem to support the hypothesis regarding sustained attention but not for working memory. The results showed significantly more improvement in sustained attention in the group with the lowest sick leave following rehabilitation (39–0%) compared to the group with the highest sick leave following rehabilitation (100–75%) between T1-T2 (low effect size), T1-T3 (moderate effect size) and T1-T4 (low effect size). Compared to the control group, the group with the lowest sick leave following rehabilitation (39–0%) improved more in sustained attention between T1-T3 (low effect size). The findings indicate that higher work participation could be associated with larger amounts of improvement in sustained attention. The present results support the assumption that being in graded employment from 39–0% contributed to more positive changes in sustained attention. Cognitive function was also assessed at the end of the rehabilitation programme to explore whether changes during rehabilitation differed from changes after. The patterns observed seemed to support a stable trajectory during the three time periods for the three sick leave groups and the control group. Rehabilitants, reporting symptoms of anxiety, depression and musculoskeletal pain, returned to work at a higher cognitive capacity, in particular the 39% –0 and 74–40% sick leave groups. This differential change in capacity between the groups remained stable in the year after rehabilitation.
Although impairments in working memory is associated with unemployment and long term sick leave [14], the differential findings between sustained attention and working memory in the present study could be due to that engaging in mentally stimulating work activities may also buffer against attentional bias. That is, excessive processing of negative and adverse events which contribute to maintaining and developing anxiety, depression and pain, and consequently depleting attentional resources [39]. This type of attentional bias is detrimental to attention resources, because anxious and depressive mood, such as worry and rumination, depletes attention [39] and working memory [40]. Attention directed towards symptoms and complaints deplete cognitive resources more than positive and salutogenic stimuli in the surroundings [41]. Also, improved attentional resources support coping at work despite experiencing health complaints [42]. The ability to shift focus away from oneself to the surroundings has been shown to be associated with a reduction in social anxiety symptoms [43]. This ability is also transferable to the work context, where attentional resources directed at work activities and tasks, diverts attention away from thoughts and symptoms and could contribute to improvement and replenishment of attentional resources. Such an interpretation could be in accordance with current results where the levels of sustained attention increased as the number of sick leave days decreased. Work could therefore have a therapeutic effect on anxiety, depression and pain [44].
A large amount of time is spent at work compared to other daily life activities. At work, workers are engaged in complex tasks that require focus and expertise. Falling out of the labour market and going on sick leave affects cognitive functioning [9, 45]. However, cognition can be recovered as the present results show cognitive benefits could be derived from employment. The brain is subjected to neuroplastic change throughout life, and a deterioration in cognitive functioning is inevitable [46]. On the positive side, being in work can potentially postpone the onset of dementia as preserving cognitive abilities can be achieved at work [47]. Work encourages us directly and indirectly to stay focused and concentrated. After a period of short- or long-term sick leave, cognitive capacity is reduced compared to working individuals not on sick leave [9]. Sustained attention helps us both at work and during daily life to maintain goals in working memory, resist or suppress distracting information and keep track of thought processes [18]. Attention and working memory are in this way interdependable. The ability to control and direct attention at work by avoiding the processing of irrelevant, distracting or even threatening stimuli, reduce interference and result in better work performance and productivity [48]. This type of controlled attention does not seem to be task dependent [49] and could operate across different work activities and contexts. Attentional processes can aid individuals in performing work tasks in two ways because attention is proposed to be operating both as a cognitive resource and as a selection mechanism [18]. Resource is related to the capacity limitation of the cognitive system, which means attentional resources can both be depleted and replenished, whereas attentional selection, a cognitive asset, is capable of prioritising which information to focus on and is consequently held in working memory. It is not known whether the improvements in the group with the lowest sick leave following rehabilitation (39–0%) is due to greater levels of attentional resources or being more efficient in selecting the most appropriate information to focus on. Nevertheless, being in work could replenish attentional resources, more so in the group with the lowest sick leave compared to the group with the highest sick leave because these individuals were exposed to a higher amount of work.
4.1Clinical implications
Sustained attention compared to working memory seem to be influenced more by the degree of work participation in sick-listed individuals returning to work. This is dependent upon the usage of graded sick leave, where clinicians are encouraged to assess and gauge more precisely the extent and appropriateness of the employment grading for each individual [50] in order to develop better RTW plans. Clinicians should also be aware of the fact that cognitive functioning might be related to the nature of the condition amongst the sick leave groups, for example, musculoskeletal pain, anxiety and depression. These conditions could affect cognition, and consequently attention, differently. For example, computerised cognitive training has been shown to improve cognition in chronic pain [51] whereas attention bias modification training reduces symptoms related to depression [52].
Based on the knowledge that the degree of work participation could affect sustained attention, it seems fruitful to develop and enhance work-related interventions during rehabilitation and psychological treatment as well as during workplace interventions [53]. One option is to have a greater focus on attention-related activities at work during work-focused cognitive behavioural therapy [54]. It has been shown that mindfulness training at work improves attentional focus [55] and could be considered as a work-related intervention for various groups either on sick leave or those struggling to remain in work. Another avenue is to integrate attention and memory activities related to work using virtual reality training, which has been shown to improve sustained attention and cognitive functions [56]. Developing a work-related version of the attention bias modification training task is another avenue to pursue [57]. Furthermore, physical exercise improves cognition and prevent early cognitive decline [58]. Combining a mental (cognitive) and a physical (motor) task, so called dual-task exercise [59], is therefore recommended. This double exposure through the combination of mental and physical exercise seems to drive even more improvements in cognition [60], and in particular if physical exercises are performed multimodally [61]. The multimodal perspective is commonly applied in occupational rehabilitation, while the dual-task approach could be developed in terms of gradually increasing the task complexity during rehabilitation to make sure all patients cope and experience self-efficacy.
4.2Improving limitations for future research
The issue of causality cannot be solved by the present research design and future studies should improve by conducting cognitive testing immediately before each individual is partly or fully back at work, and retest the same individuals after a short, medium or long stay in work. In this way, more precise changes in cognitive functioning are assessed after the start and end of rehabilitation, since the cognitive tests cannot fully inform real work engagement in daily life. Also, it cannot be ruled out that those individuals recovering more cognitive functioning during rehabilitation, returned to work at a larger cognitive capacity rather than the other way around. Future studies are encouraged to investigate this further by applying different designs to fully capture and elucidate how work influences cognitive functioning. This study targeted sustained attention and working memory [9, 16], however, it cannot be ruled out that executive functions such as attentional set-shifting, inhibition and updating, are influenced by the degree of work participation during the RTW process. It is therefore premature to rule out how work participation may influence executive functions in the present target group. The clinical meaningfulness and utility of the rehabilitation intervention under study should be interpreted with caution due to the low effect sizes established with regards to improvements in sustained attention. The groups were not homogeneous because education differed between the sick leave groups and the control group, however, level of education was controlled for during the analyses. Although the self-report of health complaints and the referral diagnoses did not differ between the groups, the comorbid nature of complaints and the specific diagnoses could affect cognition differently in the three sick leave groups. During repeated testing of cognitive function, a degree of learning effect is present because the amount of learning between individuals varies and cannot be completely disregarded. The application of a control group did however show that there are factors other than the learning effect alone that resulted in larger amounts of improvement in sustained attention in the group with the lowest sick leave following rehabilitation (39–0%). Differences in occupations were not accounted for in the sample and assessing the degree to which work was low, moderate, or high in cognitive job complexity was not possible. The target group should be kept in mind when generalising the findings as self-reported symptoms of anxiety, depression, and musculoskeletal pain were from low to moderate, acknowledging that the burden of symptoms could influence the degree to which attentional resources replenish or improve as a result of being in work.
5Conclusion
Work participation may be relevant to the recovery of cognitive functioning in sick-listed individuals. Higher work participation seems to be associated with improvements in sustained attention and not working memory in the year following occupational rehabilitation. This indicates that the degree of work participation could have differential and therapeutic effects on the cognitive function sustained attention in individuals on long term sick leave returning to work. A tentative conclusion is proposed, stating that the level of sustained attentional resources vary as a function of the level of graded work participation. These findings encourage work rehabilitation clinicians, work consultants and employers to develop RTW plans which take into account that graded employment influence cognitive functioning.
Ethical approval
The study was approved by the South-East Regional Committee for Medical and Health Research Ethics, Norway (2013/1559).
Informed consent
Written informed consent was given by all participants, and all procedures followed the 1975 Declaration of Helsinki, as revised in 2000.
Conflict of interest
The authors declare that they have no competing interests.
Acknowledgments
Gratitude goes to all who participated in the study. A special thank you to Erik Storli at CatoSenteret Rehabilitation Center, Son, Norway, Ann Marit Flokenes at Valnesfjord Health Sports Center, Valnesfjord, Norway and Olav Hahn at the Norwegian National Advisory Unit on Occupational Rehabilitation, Rauland, Norway, for the data collection. We also thank Heidi Bjorå Arset and Lena Klasson, Idrettens Helsesenter, Oslo, Norway and Anders Sandvik and Tone Hild Sørland Lyslid at Vinje Municipality, Vinje, Norway for the support.
Funding
This study was funded by the Norwegian Labour and Welfare Administration and the Northern Norway Regional Health Authority (SFP1173-14).
References
[1] | Rodriguez FS , Hussenoeder FS , Spilski J , Conrad I , Riedel-Heller SG Evaluation of a multidisciplinary concept of mental demands at work on cognitive functioning in old age. Aging Ment Health. 2020:1-10. |
[2] | Fisher GG , Stachowski A , Infurna FJ , Faul JD , Grosch J , Tetrick LE . Mental work demands, retirement, and longitudinal trajectories of cognitive functioning. J Occup Health Psychol. (2014) ;19: (2):231–42. |
[3] | Fisher GG , Chaffee DS , Tetrick LE , Davalos DB , Potter GG . Cognitive functioning, aging, and work: A review and recommendations for research and practice. J Occup Health Psychol. (2017) ;22: (3):314–36. |
[4] | Stern Y . What is cognitive reserve? Theory and research application of the reserve concept. J Int Neuropsychol Soc. (2002) ;8: (3):448–60. |
[5] | Fisher GG , Chacon M , Chaffee DS Theories of Cognitive Aging and Work. In: Baltes BB, Rudolph CW, Zacher H, editors. Work Across the Lifespan: Academic Press; 2019. pp. 17-45. |
[6] | Kajitani S , McKenzie C , Sakata K Use it too much and lose it? The effect of working hours on cognitive ability. Melbourne Institute Working Paper. 2016;7/16. |
[7] | Pihlajamäki M , Arola H , Ahveninen H , Ollikainen J , Korhonen M , Nummi T , et al. Subjective cognitive complaints and permanent work disability: a prospective cohort study. Int Arch Occup Environ Health. 2021;94(5):901-10. |
[8] | Eskildsen A , Andersen LP , Pedersen AD , Vandborg SK , Andersen JH . Work-related stress is associated with impaired neuropsychological test performance: a clinical cross-sectional study. Stress. (2015) ;18: (2):198–207. |
[9] | Johansen T , Jensen C , Eriksen HR , Lyby PS , Dittrich WH , Holsen IN , et al. Occupational Rehabilitation Is Associated With Improvements in Cognitive Functioning. Front Psychol. (2019) ;10: :2233. |
[10] | Johansen T , Skjerve A , Jensen C , Dittrich WH , Øyeflaten I . Changes in cognitive functioning in sick-listed participants in occupational rehabilitation: A feasibility study. Scand J Occup Ther. (2016) ;23: (6):437–45. |
[11] | Jonsdottir IH , Nordlund A , Ellbin S , Ljung T , Glise K , Wahrborg P , et al. Cognitive impairment in patients with stress-related exhaustion. Stress. (2013) ;16: (2):181–90. |
[12] | Oosterholt BG , Van der Linden D , Maes JH , Verbraak MJ , Kompier MA . Burned out cognition–cognitive functioning of burnout patients before and after a period with psychological treatment. Scand J Work Environ Health. (2012) ;38: (4):358–69. |
[13] | Eftedal M , Tveito TH , Gensby U , Islam MK , Lie SA , Aasland G , et al. Comparing two interdisciplinary occupational rehabilitation programs for employees on sick leave: a mixed-method design study protocol. BMC Musculoskelet Disord. (2021) ;22: (1):158. |
[14] | Worm MS , Miskowiak KW , Purdon SE , Flachs EM , Thomsen JF , Eller NH , et al. Do objective and subjective measures of cognitive impairment predict occupational status in patients with work-related stress? A clinical follow-up study. International Archives of Occupational and Environmental Health. 2023;96(1):121-30. |
[15] | Bosma H , van Boxtel MP , Ponds RW , Houx PJ , Burdorf A , Jolles J . Mental work demands protect against cognitive impairment: MAAS prospective cohort study. Exp Aging Res. (2003) ;29: (1):33–45. |
[16] | Johansen T , Oyeflaten I , Eriksen HR , Lyby PS , Dittrich WH , Holsen I , et al. Sustained Attention and Working Memory Predict the Number of Days on Health-Related Benefits in the Year Following Occupational Rehabilitation. J Occup Rehabil. 2021;31(3):592-603. |
[17] | Unsworth N , Robison MK . Working memory capacity and sustained attention: A cognitive-energetic perspective. J Exp Psychol Learn Mem Cogn. (2020) ;46: (1):77–103. |
[18] | Oberauer K . Working Memory and Attention - A Conceptual Analysis and Review. J Cogn. (2019) ;2: (1):36. |
[19] | Braathen TN , Brage S , Tellnes G , Eftedal M . Psychometric properties of the readiness for return to work scale in inpatient occupational rehabilitation in Norway. J Occup Rehabil. (2013) ;23: (3):371–80. |
[20] | Øyeflaten I , Hysing M , Eriksen HR . Prognostic factors associated with return to work following multidisciplinary vocational rehabilitation. J Rehabil Med. (2008) ;40: (7):548–54. |
[21] | Gismervik SO , Aasdahl L , Vasseljen O , Fors EA , Rise MB , Johnsen R , et al. Inpatient multimodal occupational rehabilitation reduces sickness absence among individuals with musculoskeletal and common mental health disorders: a randomized clinical trial. Scand J Work Environ Health. 2020;46(4):364-72. |
[22] | Cambridge Cognition Limited. CANTAB Connect Research: Test Administration User Guide. Cambridge: Cambridge Cognition Limited; 2022. |
[23] | Robbins TW , James M , Owen AM , Sahakian BJ , McInnes L , Rabbitt P . Cambridge Neuropsychological Test Automated Battery (CANTAB): a factor analytic study of a large sample of normal elderly volunteers. Dementia. (1994) ;5: (5):266–81. |
[24] | Chamberlain SR , Sahakian BJ . The neuropsychology of mood disorders. Curr Psychiatry Re. (2006) ;8: (6):458–63. |
[25] | Sahakian BJ , Owen AM . Computerized assessment in neuropsychiatry using CANTAB: discussion paper. J R Soc Med. (1992) ;85: (7):399–402. |
[26] | Karlsen RH , Karr JE , Saksvik SB , Lundervold AJ , Hjemdal O , Olsen A , et al. Examining 3-month test-retest reliability and reliable change using the Cambridge Neuropsychological Test Automated Battery. Applied Neuropsychology: Adult. (2022) ;29: (2):146–54. |
[27] | Owens M , Stevenson J , Hadwin JA , Norgate R . When does anxiety help or hinder cognitive test performance? The role of working memory capacity. Br J Psychol. (2014) ;105: (1):92–101. |
[28] | Taivalantti M , Barnett JH , Halt A-H , Koskela J , Auvinen J , Timonen M , et al. Depressive symptoms as predictors of visual memory deficits in middle-age. Journal of Affective Disorders. (2020) ;264: :29–34. |
[29] | Corti EJ , Gasson N , Loftus AM . Cognitive profile and mild cognitive impairment in people with chronic lower back pain. Brain and Cognition. (2021) ;151: :105737. |
[30] | Spooner DM , Pachana NA . Ecological validity in neuropsychological assessment: A case for greater consideration in research with neurologically intact populations. Archives of Clinical Neuropsychology. (2006) ;21: (4):327–37. |
[31] | Ilmarinen J . The Work Ability Index (WAI). Occupational Medicine. (2007) ;57: (2):160. |
[32] | Ahlstrom L , Grimby-Ekman A , Hagberg M , Dellve L . The work ability index and single-item question: associations with sick leave, symptoms, and health–a prospective study of women on long-term sick leave. Scand J Work Environ Health. (2010) ;36: (5):404–12. |
[33] | Eriksen HR , Ihlebæk C , Ursin H . A scoring system for subjective health complaints (SHC). Scandinavian Journal of Public Health. (1999) ;27: (1):63–72. |
[34] | Waddell G , Newton M , Henderson I , Somerville D , Main CJ . A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. (1993) ;52: (2):157–68. |
[35] | Grotle M , Brox JI , Vøllestad NK . Reliability, validity and responsiveness of the fear-avoidance beliefs questionnaire: methodological aspects of the Norwegian version. J Rehabil Med. (2006) ;38: (6):346–53. |
[36] | Zigmond AS , Snaith RP . The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) ;67: (6):361–70. |
[37] | Leiknes KA , Dalsbø TK , Siqveland J Måleegenskaper ved den norske versjonen av Hospital Anxiety and Depression Scale (HADS): Psykometrisk vurdering. [Psychometric assessment of the Norwegian version of the Hospital Anxiety and Depression Scale (HADS)]. Oslo: Folkehelseinstituttet. 2016. |
[38] | Cohen J Statistical power analysis for the behavioral sciences, 2nd ed. Hillsdale, N.J.: Lawrence Erlbaum Associates; 1988. |
[39] | Yiend J . The effects of emotion on attention: A review of attentional processing of emotional information. Cognition & Emotion. (2010) ;24: (1):3–47. |
[40] | Grant DM , White EJ Influence of Anxiety on Cognitive Control Processes. In: Oxford Research Encyclopedia of Psychology. 2016. |
[41] | Pashler H . The Psychology of Attention. Cambridge: The MIT Press. 1999. |
[42] | Ursin H , Eriksen HR . Cognitive activation theory of stress (CATS). Neurosci Biobehav Rev. (2010) ;34: (6):877–81. |
[43] | Mortberg E , Hoffart A , Boecking B , Clark DM . Shifting the focus of one’s attention mediates improvement in cognitive therapy for social anxiety disorder. Behav Cogn Psychother. (2015) ;43: (1):63–73. |
[44] | Waddell G , Burton AK Is work good for your health and well-being? London, UK: The Stationary Office; 2006. |
[45] | Eskildsen A , Andersen LP , Pedersen AD , Andersen JH . Cognitive impairments in former patients with work-related stress complaints - one year later. Stress. (2016) ;19: (6):559–66. |
[46] | Fjell AM , Walhovd KB . Structural brain changes in aging: courses, causes and cognitive consequences. Rev Neurosci. (2010) ;21: (3):187–221. |
[47] | Then FS , Luppa M , Schroeter ML , Konig HH , Angermeyer MC , Riedel-Heller SG . Enriched environment at work and the incidence of dementia: results of the Leipzig longitudinal study of the aged (LEILA 75+). PLoS One. (2013) ;8: (7):e70906. |
[48] | Clark M , DiBenedetti D , Perez V . Cognitive dysfunction and work productivity in major depressive disorder. Expert Rev Pharmacoecon Outcomes Res. (2016) ;16: (4):455–63. |
[49] | Engle RW , Tuholski SW , Laughlin JE , Conway ARA . Working memory, short-term memory, and general fluid intelligence: A latent-variable approach. Journal of Experimental Psychology: General. (1999) ;128: (3):309–31. |
[50] | Bethge M . Effects of graded return-to-work: a propensity-score-matched analysis. Scand J Work Environ Health. (2016) ;42: (4):273–9. |
[51] | Baker KS , Georgiou-Karistianis N , Lampit A , Valenzuela M , Gibson SJ , Giummarra MJ . Computerised training improves cognitive performance in chronic pain: a participant-blinded randomised active-controlled trial with remote supervision. Pain. (2018) ;159: (4):644–55. |
[52] | Bo R , Kraft B , Jonassen R , Harmer CJ , Hilland E , Stiles TC , et al. Symptom severity moderates the outcome of attention bias modification for depression: An exploratory study. J Psychiatr Res. (2021) ;138: :528–34. |
[53] | Salomonsson S , Hedman-Lagerlof E , Ost LG . Sickness absence: a systematic review and meta-analysis of psychological treatments for individuals on sick leave due to common mental disorders. Psychol Med. (2018) ;48: (12):1954–65. |
[54] | Gjengedal RGH , Reme SE , Osnes K , Lagerfeld SE , Blonk RWB , Sandin K , et al. Work-focused therapy for common mental disorders: A naturalistic study comparing an intervention group with a waitlist control group. Work. 2020;66(3):657-67. |
[55] | Slutsky J , Chin B , Raye J , Creswell JD . Mindfulness training improves employee well-being: A randomized controlled trial. Journal of Occupational Health Psychology. (2019) ;24: (1):139–49. |
[56] | Jha AP , Krompinger J , Baime MJ . Mindfulness training modifies subsystems of attention. Cognitive, Affective, & Behavioral Neuroscience. (2007) ;7: (2):109–19. |
[57] | Kraft B , Jonassen R , Heeren A , Harmer C , Stiles T , Landrø NI . Attention Bias Modification in Remitted Depression Is Associated With Increased Interest and Leads to Reduced Adverse Impact of Anxiety Symptoms and Negative Cognition. Clinical Psychological Science. (2019) ;7: (3):530–44. |
[58] | Stillman CM , Esteban-Cornejo I , Brown B , Bender CM , Erickson KI . Effects of Exercise on Brain and Cognition Across Age Groups and Health States. Trends Neurosci. (2020) ;43: (7):533–43. |
[59] | Jardim NYV , Bento-Torres NVO , Costa VO , Carvalho JPR , Pontes HTS , Tomás AM , et al. Dual-Task Exercise to Improve Cognition and Functional Capacity of Healthy Older Adults. Frontiers in Aging Neuroscience. 2021;13. |
[60] | Gheysen F , Poppe L , DeSmet A , Swinnen S , Cardon G , De Bourdeaudhuij I , et al. Physical activity to improve cognition in older adults: can physical activity programs enriched with cognitive challenges enhance the effects? A systematic review and meta-analysis. Int J Behav Nutr Phys Act. (2018) ;15: (1):63. |
[61] | Northey JM , Cherbuin N , Pumpa KL , Smee DJ , Rattray B . Exercise interventions for cognitive function in adults older than a systematic review with meta-analysis. Br J Sports Med. (2018) ;52: (3):154–60. |


