
Prevalence of impaired upper extremity neural mobility among smart device users during the COVID-19 pandemic
Abstract
BACKGROUND:
Both the development of various countries and people’s health were impacted by the unforeseen global COVID-19 outbreak. Many countries prefer to do their daily business online. Although it was incredibly useful at the time, it still had a problem that was not properly addressed, especially among the student population.
OBJECTIVE:
The objective of this study was to examine the prevalence of upper extremity neural mobility among students who were using smart devices during the COVID-19 pandemic.
METHODS:
458 students who had previously taken home-based online classes during the COVID-19 pandemic and used a smart device for more than six hours were included in this study. The study was conducted in three phases. After being examined in the first two stages of the study, a total of 72 people were chosen for the final phase. Peripheral nerve mobility tests were performed on these 72 subjects.
RESULTS:
This study observed that 15.72% of smart device users have been affected by forward neck posture and impaired peripheral nerve mobility in the cervical spine.
CONCLUSION:
The study concludes that forward neck posture is associated with impaired peripheral nerve mobility among smart device users who were in home-based online classes during the COVID-19 pandemic lockdown. Hence, we suggest an appropriate treatment strategy focusing on preventing the forward neck posture through timely analysis and self-care therapies.
1Introduction
SARS-CoV-2 (COVID-19) originated in December 2019 and caused a pandemic that affected the entire world. The initial discovery was made in Wuhan, China. The World Health Organization (WHO) classified the virus as a global pandemic in March 2020 as a result of its widespread spread across many countries [1]. As of March 2023, over 761 billion COVID-19 cases have been documented worldwide. In India, there have been approximately 10,000,000 confirmed cases and over 150,000 deaths [2]. Social isolation measures were proposed to prevent and manage the spread of COVID-19 infection. As a result, the WHO advised all governments around the world to impose a curfew in order to combat the pandemic [2, 3]. The curfew imposed during COVID-19 had an impact on the country’s and the public’s health and prosperity and many countries saw significant drops in their gross domestic product as well. As a result, the government was forced to seek an alternative solution in areas such as banking, commerce, and education [2]. In addition to preventing the spread of the disease, the curfew allowed educational institutions, governments and private organisations to implement a work-from-home policy, which was shown to be economically beneficial by lowering infrastructure maintenance costs [2, 4–6].
According to the literature, implementing a work-from-home policy was both beneficial and detrimental because it caused issues with software professionals’ mental health. In contrast, incorporating an online platform for educational institutions had its own set of benefits and drawbacks because it caused problems for both teachers and students, as shown by a study done during the pandemic which found that the online platform had a negative impact on physical and mental well-being [5, 7, 8]. According to the literature, the pandemic caused some musculoskeletal difficulties for teachers as a result of switching to a digital platform for teaching, in addition to their acute anxiety and stress [6, 9]. Additionally, the online learning environment has led to some student behavioural aberrations and has been a silent contributing factor to a variety of musculoskeletal dysfunctions, which received the least attention during the pandemic [10, 11].
Therefore, the current research aims to address the ignored element of the musculoskeletal dysfunctions that the students experienced throughout the pandemic because the pandemic forced the students to spend more time with digital devices, like laptops and cell phones [12]. Due to this, it was difficult to maintain a suitable ergonomic position, which raised the likelihood of neck, shoulder, and back pain [13]. The majority of the students suffered from non-specific neck pain as a result, which caused them to slouch their necks forward and have limited neural mobility [14, 15]. The forward-neck posture is considered to be the most emerging cause of mechanical and neurogenic pain over the upper limb and neck [16]. Forward neck posture is prevalent in 66% of the population who present with thoraco-cervical-shoulder postural abnormalities (forward neck posture). An increase in angulations places the peripheral nerves under increased mechanical stress, resulting in upper limb neurogenic pain [17–19]. The common diagnostic procedures used to examine the forward neck posture are done through physical assessment and X-ray [20]. Since exposing an individual to X-rays may result in unwanted radiation exposure, physical evaluation is regarded as a non-invasive, cost-effective approach, and we have included the photogrammetric method via Kinovean software to measure forward neck posture, which is regarded as the uniqueness of our work. This study also examined the neural mobility of the peripheral nerve via the upper limb tension test (ULTT) rather than the standard ultrasonography and MRI procedures, which are thought to be more expensive than the ULTT.
The purpose of this study is to assess the prevalence of forward neck posture and impaired peripheral nerve mobility of the medial, radial, and ulnar nerves, which are correlated to neck pain, among students using smart devices during the COVID-19 pandemic.
2Methods
2.1Study design and study setting
The study was approved by the Institutional Scientific Review Board before recruitment of the first participant (01/011/2021/ISRB/PGSR/SCPT). This cross-sectional study was done among students from a deemed university after obtaining their willingness and informed consent.
2.2Study participants
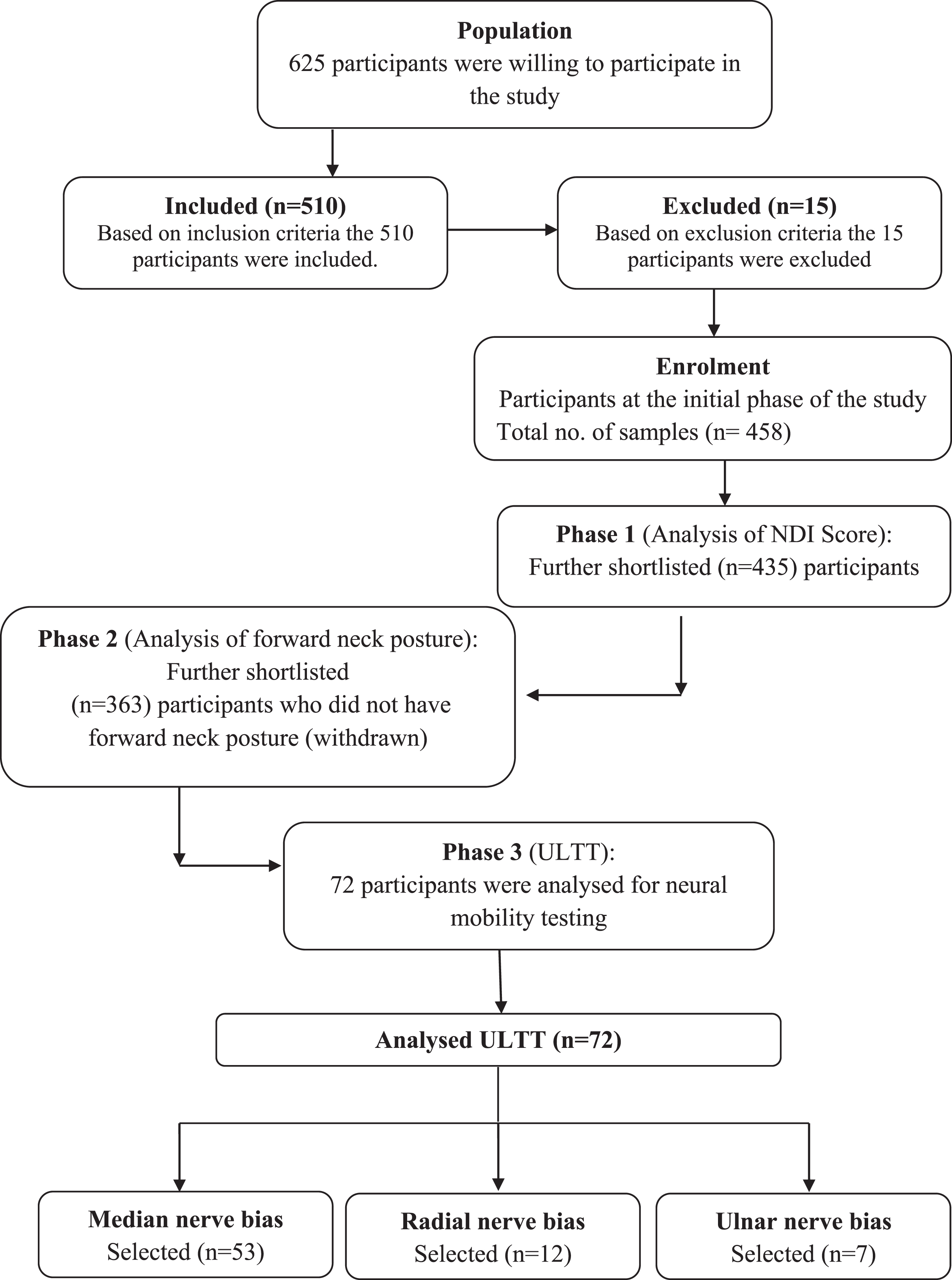
Students from a private university were invited to take part in this study by the researcher. The invitation was personally conveyed to them via email and WhatsApp and put on the notice board of their respective departments. 625 people expressed a desire to take part in the survey. Participants were included in the study once they met the inclusion criteria, which included being between the ages of 18 and 30, of both genders, using a smart device for more than 6 hours, and scoring between 3 and 6 on the Numerical Pain Rating scale. 510 participants were shortlisted for the study at this level. Participants with cervical spondylolisthesis, acute inflammatory lesions, recent trauma to the cervical spine, and space-occupying lesions were excluded from the study in accordance with the exclusion criteria. Thus, 458 participants were enrolled in the study. After thoroughly explaining the study’s methodology to each participant, formal informed consent was obtained. The first phase of the study continued with these 458 student participants to assess the neck disability index rating. The participants in the mild and moderate disability categories were selected and taken for phase 2 analysis (n = 435). In phase 2, the forward neck posture was analysed using Kinovean software, hence the participants who did not have a forward neck posture were relieved from the study (n = 363). Finally, a total of 72 subjects were selected for the third phase of the study, during which their neural mobility was assessed. The details of each phase and its procedure were then explained.
2.3Data collecting procedure
This study was divided into three phases, as outlined below.
2.3.1Phase 1: Survey
A Google Form was created and distributed to the 495 participants. The form was divided into three sections. Section 1 contains personal dates and Section 2 contains information on the type of smart device, the duration of smart device usage, the position they adopt with smart device, and the purpose of smart device usage [21]. Section 3 contains NDI ranging from no disability, defined as 0–4 points (0–8%); mild disability, defined as 5–14 points (10–28%); moderate disability, defined as 15–24 points (30–48%); severe disability, defined as 25–34 points (50–64%); and total impairment, defined as 35–50 points (70–100%). The Google Form responses were obtained.
2.3.2Phase 2: Analysis of forward neck posture
Kinovean software was used in Phase 2 to calculate the cranio-vertebral (CV) angle, which was used to measure forward neck posture [22]. For the subjects in their normal standing position, a digital lateral-view photograph was taken. The 7th cervical vertebra, the tragus, and the acromion were all marked. The subject was asked to stand 104 inches away from the camera, which was placed 33 inches above ground level. The subjects were instructed to stand and stretch their heads three times as far as they could before looking in the front mirror at their eyes. A snapshot was taken and calibrated through Kinovean software. To prevent the subjects from deliberately altering their neck posture, they were blinded to the study. A photograph was taken from the side with a digital camera. The following approach was used to determine the CV angle: The anteriorly running C7 spinous process was marked with a horizontal line, and another line was drawn from the C7 spinous process to the tragus, the pointed part of the earhole. The CV angle is produced when these two lines meet at the C7 vertebra [24]. In those with neck discomfort, a lower craniovertebral angle was linked to a more forward head position. An angle between the skull and the vertebrae (CVA) that is too small represents a forward neck posture. CVA is below 48–50, which was defined as forward neck posture [24].
2.3.3Phase 3: Neural mobility test
In phase 3, the study addresses the upper limb tension tests (ULTTs) for the radial, medial, and ulnar nerves. In ULTTs, it was used to determine whether forward neck posture was inducing peripheral nerve compression, which comes from the cervical spine to the extremity. During this technique, the therapist talked to the patient about what would happen and got their permission.
Procedure for ULTT:
ULTT-Radial nerve bias: The shoulder girdle is depressed, the shoulder abduction is 20°–30°, the whole arm is medially rotated, forearm pronation, the wrist, fingers, and thumb are flexed, and the elbow is extended. ULTT-Median nerve bias: The shoulder girdle is depressed, the shoulder abduction is 100°, the whole arm is rotated, forearm supination, the wrist, fingers, and thumb are extended, and the elbow is extended. ULTT-Ulna nerve bias: The shoulder girdle is depressed, abducted, and externally rotated, forearm pronation, the wrist and fingers are extended, and finally, the elbow is flexed.
Each test was first done on the normal/asymptomatic side. The testing motion was repeated 3 times, holding position for 10 sec until the symptom was elicited. The test would have been considered positive if the patient presented with complaints of tingling, pinpricking, and pulling types of pain sensations.
2.4Data analyses
In this procedure, the subjects (n = 458) were participants in the study. In the study, 72 individuals were selected for phase 3 of ULTT’s analysis after completing phases 1 and 2 and a significant impairment of peripheral nerve mobility was found. There were 53 individuals with a positive signal in the median nerve bias, 12 individuals with a positive signal in the radial nerve bias, and 7 individuals with a positive signal in the ulnar nerve bias (Fig. 1).
Fig. 1
Methodology of the study.
3Results
Sample characteristics of 458 participants were analysed from 625 smart device users during COVID-19. Forward neck posture in smart device users was significantly increased and associated with the COVID-19 pandemic. Descriptive analysis and the chi-square test were employed in the statistical analysis. The validity of the three-structure of the peripheral nerve mobility was confirmed. ULTTs for the median, radial, and ulnar nerves could be partially differentiated in 72 individuals. 73. 61% had a median nerve bias, 16. 67% had a radial nerve bias, and 9. 42% had an ulnar nerve bias (Fig. 2). 72% of smart device users were affected out of 458 participants during the COVID-19 pandemic.
Fig. 2
Prevalence of impaired upper extremity neural mobility using upper limb tension test.
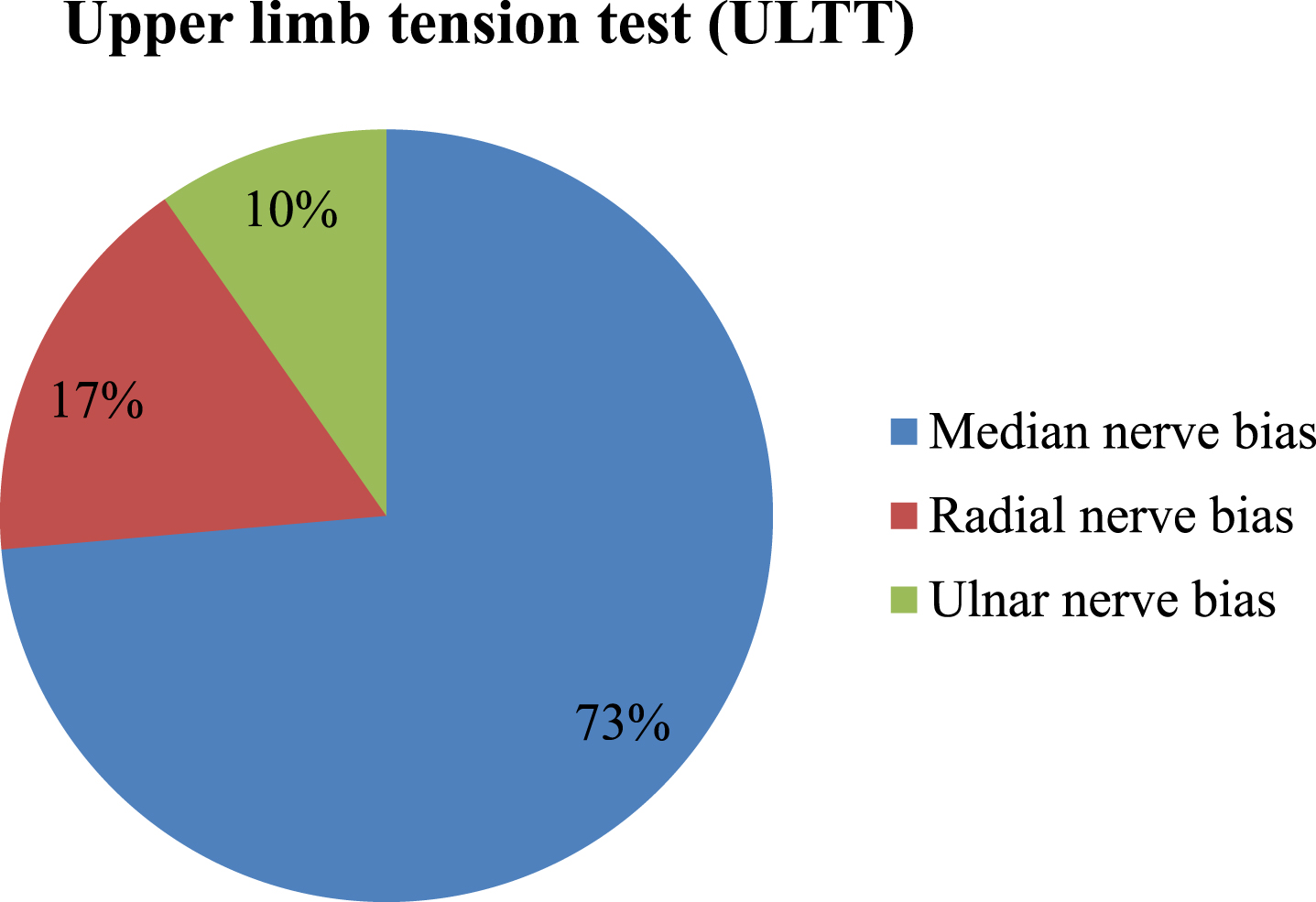
Table 1
Demographic data
| Age | 16–20 | 21–25 | 26–30 | Total | Mean | SD | % | |
| Gender | Male | 54 | 80 | 13 | 147 | 22.03 | 2.94 | 32% |
| Female | 92 | 172 | 47 | 311 | 22.09 | 3.19 | 68% | |
| Total population | 146 | 252 | 60 | 458 | 22.07 | 3.11 | 100% | |
Table 2
Peripheral nerve bias
| ULTT | Population (n = 72) | Percentage % |
| Median nerve bias | 53 | 73% |
| Radial nerve bias | 12 | 17% |
| Ulna nerve bias | 7 | 10% |
4Discussion
A developing country like India requires instruction in low-cost technology (desktops/laptops/wi-fi routers), broadband internet services, and online education will be a huge success thanks to SAT technology, according to this survey. Despite some drawbacks, students liked online learning environments and favoured creative or tech-based teaching methods. It was advised to engage students by combining modern teaching techniques with an ideal class design (40 minutes in each class, a minimum 10-minute break between classes, and a maximum of 2–4 hours of classes). Additionally, it lowers the chance of boredom and health issues [21].
According to the review of the literature by Ramane et al., the internet app has serious physical health issues such as computer eye syndrome and headaches. The pain in the neck, shoulders, and back was significant. The students also reported feeling uncomfortable, irritable, tired, and sleeping poorly at the same time. Therefore, health-related concerns with loneliness linked to online learning may aid in the learner’s overall growth. Increased physical and psychological stress might likely seriously impair the health of future learners if this trend persists for an extended period of time [22].
Studies have shown neck discomfort connected with smart device users in class settings [23] and concluded that technology advancement has disturbed education institutions, particularly e-learning platforms where lessons are done online. In this research, the smart phone was a key instrument for attending online courses in Arab countries, according to the findings. Sharing class notes and having online access to eBooks required the use of modern technology. As a result, the importance of smart devices in our daily lives increased. The user would also have acute neck pain and muscle discomfort as a result of the smart device.
According to Tang et al., wearing prism glasses while using a smart phone in stationary situations was studied for biomechanical effectiveness, discomfort effects, usability, desirability, and performance results. The prism perspective was reported to lower neck muscular activation, provide more neutral postures, and minimise neck discomfort in symptomatic individuals; biomechanics was also improved in those who did not have pain. Typing speed was much slower while using the prism glasses than when utilising the direct view, although accuracy was not impaired [24].
Although many studies have been conducted on smart devices through the worker population, this study was conducted on the student population. The purpose of this research was to observe the forward neck posture among smart device users and those who were studying from home during COVID-19. They were given some questionnaires based on neck pain with radiating pain and asked to take an upper limb tension test to find out the nerve involvement for radiating pain or pulling type pain. Statistically, descriptive analysis and chi-square were used. Our findings showed that 30.29% of smart device users had neck pain from radiating pain. Further analysis of the results shows that 73.61% of the participants with impairments in peripheral nerve mobility had a positive sign in median nerve bias, 16.67% of the participants had a positive sign in radial nerve bias, and 9.72% of the participants had a positive sign in ulnar nerve bias. In addition, the user would face major discomforts while using the smart devices, like neck pain, soreness in the muscles, and neck postural deformities like a forward neck posture. Therefore, students have to maintain good health throughout the COVID-19 pandemic in order to complete their coursework effectively. It should be emphasised, however, that the factors included in this research did not demonstrate any correlation. The independent factors and the peripheral nerve mobility bias were both negligible. The analysis did not show a proper connection among variables that determined that the data collected would affect results purely based on the students’ consciousness. One of the limitations of the study was the small sample.
5Conclusion
According to the findings of the current study, the median nerve exhibited a bias towards poorer peripheral nerve mobility when compared to the radial and ulnar nerves. It was made abundantly evident that extended use of smart gadgets by the students in poor ergonomic positions will modify neck posture, placing an undue strain on the cervical spine, which leads to entrapment of the peripheral nerve. This could be an important risk factor for early degenerative changes in the cervical spine, which in turn can lead to disc herniation and cervical radiculopathy. Thus, impaired peripheral nerve mobility can be avoided through attaining ergonomically non-vulnerable postures while using smart devices. Our research has shed light on the musculoskeletal issues faced by the students during COVID-19 due to the poor ergonomic posture adaptation while attending the online-based education platform.
Funding
None to report.
Conflict of interest
The authors have no conflicts of interest to report.
Acknowledgments
The authors would like to thank all participants who were involved in this study. Also, they would like to thank the software developers of the Kinovean software.
References
[1] | Milić S , Marić N Concerns and mental health of teachers from digitally underdeveloped countriesregarding the reopening of schools after the first wave of the COVID-19 pandemic. Work. (2022) ;71: (1):53–64. |
[2] | Banur RA Challenges faced during COVID-19 pandemic. IP International Journal of Medical Microbiology and Tropical Diseases. (2021) ;7: (1):1–2. |
[3] | Atalan A Is the lockdown important to prevent the COVID-19 pandemic? Effects on psychology, environment and economy-perspective. Annals of Medicine and Surgery ((2020) ) 56: , 38–42. |
[4] | Jena PK Online learning during lockdown period for COVID-19 in India. International Journal of Multidisciplinary Educational Research (IJMER). (2020) ;9. |
[5] | Ipsen C , van Veldhoven M , Kirchner K , Hansen JP Six key advantages and disadvantages of working from home in Europe during COVID-19. International Journal of Environmental Research and Public Health. (2021) ;18: (4):1826. |
[6] | Chuenyindee T , Montenegro LD , Ong AK , Prasetyo YT , Nadlifatin R , Ayuwati ID , Sittiwatethanasiri T , Robas KP The perceived usability of the learning management system during the COVID-19 pandemic: Integrating system usability scale, technology acceptance model, and task-technology fit. Work. (Preprint):1–8. |
[7] | Kumaresan A , Suganthirababu P , Srinivasan V , Chandhini VY , Divyalaxmi P , Alagesan J , Vishnuram S , Ramana K , Prathap L Prevalence of burnout syndrome among Work-From-Home IT professionals during the COVID-19 pandemic. Work. (2022) (Preprint):1–5. |
[8] | Xiao Y , Becerik-Gerber B , Lucas G , Roll SC Impacts of working from home during COVID-19 pandemic on physical and mental well-being of office workstation users. Journal of Occupational and Environmental Medicine. (2021) ;63: (3):181. |
[9] | Ma K , Liang L , Chutiyami M , Nicoll S , Khaerudin T , Van Ha X COVID-19 pandemic-related anxiety, stress, and depression among teachers: A systematic review and meta-analysis. Work. (2022) (Preprint):1–25. |
[10] | Srinivasan V , Vishnuram S , Suganthirababu P , Kumaresan A , Divyalaxmi P , Saranya Devi M , Alagesan J Impact of COVID-19 online classes on morningness-eveningness personality among adult college students: A survey study. Work. (2021) (Preprint):1–6. |
[11] | Almhdawi KA , Alazrai A , Obeidat D , Altarifi AA , Oteir AO , Aljammal AH , Arabiat AA , Alrabbaie H , Jaber H , Almousa KM Healthcare students’ mental and physical well-being during the COVID-19 lockdown and distance learning. Work. (2021) (Preprint):1–8. |
[12] | Firth J , Torous J , Stubbs B , Firth JA , Steiner GZ , Smith L , Alvarez-Jimenez M , Gleeson J , Vancampfort D , Armitage CJ , Sarris J The “online brain”: How the Internet may be changing our cognition. World Psychiatry. (2019) ;18: (2):119–29. |
[13] | Jahanimoghadam F , Abdolalizadeh M Ergonomics, musculoskeletal disorders, and computer work. Journal of Health and Biomedical Informatics. (2016) ;3: (2):145–54. |
[14] | Bhagawati D , Gwilym S. Neck pain with radiculopathy. BMJ Clinical Evidence. (2015) ;2015:1103 |
[15] | Sheikhhoseini R , Shahrbanian S , Sayyadi P , O’Sullivan K Effectiveness of therapeutic exercise on forward neck posture: A systematic review and meta-analysis. Journal of Manipulative and Physiological Therapeutics. (2018) ;41: (6):530–9. |
[16] | Kim MS Influence of neck pain on cervical movement in the sagittal plane during smartphone use. Journal of Physical Therapy Science. (2015) ;27: (1):15–7. |
[17] | OzudogruCelik T , DuyurCakit B , Nacir B , Genc H , Cakit MO , Karagoz A Neurodynamic evaluation and nerve conduction studies in patients with forward neck posture. Acta NeurologicaBelgica. (2020) ;120: (3):621–8. |
[18] | Butler D A concept of adverse mechanical tension in the nervous system-application to repetitive strain injury. In Proceedings of the 5th Biennial MTAA Conference Melbourne. (1987) ;247–270. |
[19] | Yılmaz S , Taş S , Yılmaz ÖT Comparison of median nerve mechanosensitivity and pressure painthreshold in patients with nonspecific neck pain and asymptomatic individuals. Journal of Manipulative and Physiological Therapeutics. (2018) ;41: (3):227–33. |
[20] | Câmara-Souza MB , Figueredo OM , Maia PR , Dantas ID , Barbosa GA Cervical posture analysis in dental studentsand its correlation with temporomandibular disorder. CRANIO®. (2018) ;36: (2):85–90. |
[21] | Singh HK , Joshi A , Malepati RN , Najeeb S , Balakrishna P , Pannerselvam NK , Singh YK , Ganne P A survey of E-learning methods in nursing and medical education during COVID-19 pandemic in India. Nurse Education Today ((2021) ) 99: , 104796. |
[22] | Ramane DV , Devare UA , Kapatkar MV The impact of online learning on learners’ education and health. The Online Journal of Distance Education and E-Learning. (2021) ;9: (2):303–9. |
[23] | Mustafa GR The use of smartphones in distance learning/e-learning/online classes and its impact to neck pain in the light of the Covid-19 pandemic. Psychology and Education. (2020) ;57: (9):1988–99. |
[24] | Tang M , Sommerich CM , Lavender SA An investigation of an ergonomics intervention to affect neck biomechanics and pain associated with smartphone use. Work. (2021) ;69: (1):127–39. |


