
Work readiness and barriers to employment during COVID-19 for individuals with Neurofibromatosis Type 1 (NF1)
Abstract
BACKGROUND:
The global COVID-19 pandemic has directly impacted individuals with rare diseases who are attempting to maintain or obtain employment. Individuals with Neurofibromatosis Type 1 are especially at risk due to their disease.
OBJECTIVE:
The current study compared the impact that generalized anxiety and quality of life had on work readiness and potential barriers that individuals with NF1 had in gaining and maintaining employment during the COVID-19 pandemic to a sample of healthy individuals using a moderating mediation analysis.
METHODS:
A total of 213 individuals (105 NF1; 108 Healthy individuals) were recruited to complete a cross-sectional study in which a series of work-related assessments were completed.
RESULTS:
Generalized anxiety had an indirect effect on work readiness, fully mediated by barriers, with higher anxiety associated with more barriers, in turn negatively correlating with work readiness; quality of life partially mediated the effect of barriers on work readiness and was negatively associated with the former and positively with the latter.
CONCLUSION:
Quality of life was a mediator of the relationship between perceived employment barriers and work readiness for the healthy individuals group only. The results imply that anxiety and quality of life are significant mediators and require consideration in terms of evaluation and facilitation of employment maintenance and acquisition.
1Introduction
The coronavirus disease (COVID-19) has dramatically impacted the United States (U.S.) and international workforce [1] since its inception at the end of 2019, with an estimated 2.4 million women [2] and 1.8 million men exiting the labor force between February 2020– 2021. Due to the increase in cumulative COVID-19 hospitalization rates reaching 207.4/100,000 (18–49-year-olds) and 505.7/100,000 (50–64-year-olds) in the U.S., restrictive measures were put in place to mitigate transmission of COVID-19 and had an immediate and unprecedented impact on people’s psychological health and well-being, especially as it relates to incidences and severity of depression and anxiety [3, 4]. Furthermore, concerns regarding job loss among individuals with chronic conditions and disabilities [5–7] and isolation due to lack of employment has had a negative impact on health and psychological well-being [8].
1.1Neurofibromatosis Type 1
For individuals with rare diseases and/or disabilities such as Neurofibromatosis Type 1 (NF1), COVID-19 presents with new issues in resuming work during an outbreak, dealing with lockdowns, and taking special account of workers with vulnerabilities as the pandemic wanes [2–4, 9–11]. Neurofibromatosis Type 1 (NF1) is an autosomal dominant disorder characterized as a neurocutaneous disease that can impact all regions of the body (e.g., nervous system, bone, skin) and affects 1 in 2500 individuals worldwide [12–14]. Previous research has shown that lack of employment has a significant effect on depression and anxiety within individuals with NF1 [15] and is associated with negative emotions of oneself which contributes to reduced psychological wellbeing [16, 17]. Work-related issues for individuals with NF1 have been an under-explored focus of research. Although studies have found evidence of significant employment-related challenges for individuals with NF1 [15, 18], the impact that COVID-19 [19] has had on employment barriers has yet to be explored.
The medical complications associated with NF1 have been well-documented in the literature, with typical presentations including a plexiform neurofibromas, Lisch nodules, optic pathway gliomas, and/or caféau lait patches. Additionally, other physical manifestations of NF1 (e.g., pseudarthrosis, scoliosis, osteoporosis), along with cognitive impairments (e.g., dyslexia, lower IQ scores, attentional deficit hyperactivity disorder (ADHD)) can impact an individual’s quality of life, and ability to obtain and maintain gainful employment [20–23]. There is much research that has shown that physical disfigurement, cognitive impairments, and ADHD can create challenges with job obtainment and retention within other populations [24–27]. The focus of the current study was to evaluate how generalized anxiety and quality of life (QOL) influence work readiness and perceived barriers, while examining the role that these factors have in obtaining and maintaining gainful employment during the COVID-19 pandemic.
1.2Work readiness and perceived employment barriers
Work readiness and employment barriers are two factors that can influence one’s ability to obtain work [28, 29]. Often these barriers are addressed in pre-employment training that focuses on specific job skills training and identification of employment barriers (e.g., transportation, chronic pain, child-care, interviewing skills, growth mindset). These job skills often need to be addressed to prepare individuals to enter the workforce [30]. Despite literature showing that these factors have been explored for diverse disability groups [15], there is a scarcity of research further examining these variables for the NF1 population.
1.3Vocational rehabilitation as an intervention
The most recent publication has shown that individuals with NF1 have the same levels of self-motivation when it comes to employment hope (e.g., positive emotional state directed at work, limited feelings of hopelessness towards obtaining employment) and are equally goal-oriented when compared to the general population [15]. Yet, feeling psychologically empowered and understanding how to use one’s skills have been shown to be more significant employment barriers for individuals with NF1 [15]. The impact of COVID-19 on job obtainment and retention has been a focus of research as of late. Significant job loss among individuals with chronic conditions and disabilities during the pandemic has been shown in recent literature [31, 32], with research showing a negative impact on health and psychological well-being of people with disabilities due to isolation based on lack of employment [33]. Study findings showed significant direct effects of anxiety, perceived barriers to employment on work readiness of individuals with NF1 (compared to the control group), and while quality of life were significant indirect effects. Vocational rehabilitation (VR) that addresses the employment barriers faced by individuals with NF1 can serve to improve their employability, QOL, and mental well-being.
The current study hypothesized that due to constraints put on employees on account of COVID-19 protocols, individuals with NF1 would have more difficulties in adapting and being successful in their work readiness. More specifically, anxiety, and barriers on one hand and quality of life on the other hand, have opposing influence on work readiness and ask whether their influences and dynamic relationships differ for those with NF1 vs healthy individuals.
2Methods
2.1Participants
Two groups of participants were recruited between May through August 2021. Group 1 consisted of individuals with NF1. They were recruited through a secure mass email sent out to two of the largest NF advocacy’s listservs (NF Network and NF Northeast), after acquiring approval from both executive directors. The NF1 group consisted of 140 individuals of which 105 completed the assessments, 29 did not complete the assessments, and 6 were excluded for not having a documented case of NF1. The second group consisted of 119 healthy individuals recruited via Qualtrics recruitment services, of which 108 successfully completed the assessment.
The inclusion criterion for the study were as follows: 1) at least 18 years of age, 2) a current documented case of NF1, and 3) no documented case of NF1 (healthy individuals). The exclusion criterion were the following: 1) unable to read through and consent to the study, 2) no access to internet via computer, tablet, or smart phone, 3) diagnosis of NF2, Schwannomatosis, or undiagnosed NF symptoms, 4) no prior medical diseases (healthy individuals), as defined within the last 5 years. It should be noted that each group was balanced on sample size but was not matched on the age. This will be discussed in the limitations section.
2.2Assessments
The Work Readiness Inventory (WRI) is a 36-item self-report scale intended to help identify specific challenges facing consumers when they are making career choices. Participants report on a 5-point scale (5 = Very Concerned, 1 = Not Concerned) across six subscales: Responsibility, Flexibility, Skills, Communication, Self-View, and Health/Safety. Scores are summed into five groupings (Very Concerned = 25–30 to Not Concerned = 6). Reliability of the WRI has demonstrated a Cronbach’s alpha ranging from .74 to .94.
The Barriers to Employment Success Inventory (BESI), Fifth Edition, is a scale designed to identify and explore potential barriers to securing employment, enjoying employment success, and career advancement. The scale consists of 50 items; for each item participants select an answer from four options (1 = no concern, 4 = greatest concern). Five barrier categories are assessed: Personal and Financial, Emotional and Physical, Career Decision-Making and Planning, Job-Seeking Knowledge, and Education and Training. The subfactors of the measure have good to excellent reliability with Cronbach’s alphas ranging between .87 and .95.
The Short-form Questionnaire of Medical Outcomes (SF-12) [34] is a quality of life questionnaire that focuses on health-related concepts. The 12-item measure assesses both functioning (physical, social and role) and well-being (mental health, health perception and pain). The SF-12 yields six sub scores that are then aggregated into a parameter (0–100), with higher scores indicating better functioning or well-being. The reliability of the SF-12 is .7 with a Mosier’s alpha [35].
The Generalized Anxiety Disorder Scale-7 (GAD-7) [36] is a self-reported screening tool and severity indicator for generalized anxiety disorder (GAD) that was developed in alignment with the Diagnostic and Statistical Manual-5th Edition (DSM-5). The scale consists of 7 items, for which respondents select a response from a 4-point scale (1 = not at all, 2 = several days, 3 = over half days, 4 = nearly every day). Once a total score is obtained, it is categorized into four levels of anxiety: minimal (1–4); mild (5–9); moderate (10–14); and severe (15–21). The GAD-7 has excellent reliability, demonstrated by a Cronbach’s alpha of 0.92 (α=0.92).
2.3Procedure
Prior to any data collection, approval from the Human Subjects Committee (HSC) at the primary author’s institution (Research ID# 2000026514) was received. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all participants for being included in the study.
The current study was a cross-sectional design quantitative method that followed the methodology of Buono et al. [15], in which participants matched across both groups: gender (at minimum 45% were female) and age. Utilizing an NF1 advocacy listserv, individuals with NF1 were contacted via email to participate in the study. If interested, participants clicked a link at the bottom of the email that led them to a protected survey on Qualtrics. Participants were then presented with an informed consent form that described the study and data management procedures. If they agreed, participants electronically signed the form and began the survey. Data was then anonymized by the first author (FB) and stored on a secure server hosted by the first author’s institution. Per participants’ requests, a copy of the informed consent could be either mailed or securely emailed. Participants were debriefed about the study with a standardized script after completing the assessments. Participants were randomly selected to win four $50 USD Amazon gift cards based on the completion of the study.
2.4Data analysis
To explore the relative effects of anxiety on work readiness and investigate potential mediating relationships among the variables identified as significant correlates through bivariate testing, while also accounting for moderating impact of NF (NF vs healthy individuals), we performed a multi-group path analysis [37] with anxiety as exogenous variables, perceived barriers and quality of life as mediators, and work readiness as an endogenous variable. We controlled for age, gender, and education level, and estimated indirect effects via bootstrapping procedures, while stepwise eliminating insignificant paths and “hanging” variables.
Path models provide a more complete theoretical testing, specification, and understanding relative to traditional regression analyses [38]. Path models allow one to examine direct, indirect, and total effects simultaneously in one model, as well as to apply some of the bootstrap resampling techniques, which appropriately correct for missing data problems and non-normality in the data [39]. Performing multi-group path analysis is similar to running multiple regressions with interaction terms simultaneously; therefore, the results presented here are likely to hold with less sophisticated and more common techniques. The structural equation modeling program IBM SPSS AMOS.27 was utilized to perform a multi-group path analysis. To calculate indirect effects and investigate potential mediating relationships among the variables in the model, we used the AMOS bootstrapping procedure with a bias-corrected accelerated confidence intervals, a recommended analytic strategy for avoiding measurement error and underestimation of the mediation significance [40]. After removing insignificant paths and omitting “hanging” variables, we obtained the final structural model that is presented in Fig. 1 and is described below. The decomposition of direct and indirect effects among the variables in the model is presented in Table 1.
Fig. 1
Multi-group model. Note > Multi-group results for mediation analysis. Indirect effects were tested via AMOS bootstrapping procedure with 4000 bootstrap samples and bias-corrected accelerated confidence intervals. Control variables (covariates) are not shown in the figure for ease of presentation. Group moderated the relationship among all variables in the model (z > 2.38, p < .01 in all cases). Overall model fit: X2 = 3.69, p = 0.45; Root Mean Square Error of Approximation (RMSEA)=0.00, PCLOSE=0.68; Comparative Fit Index (CFI)=1.00; Goodness of Fit Index (GFI)=0.99. Multi-group results in figure correspond to Table 1x. The dashed paths for quality of life represent its significance for control group only.
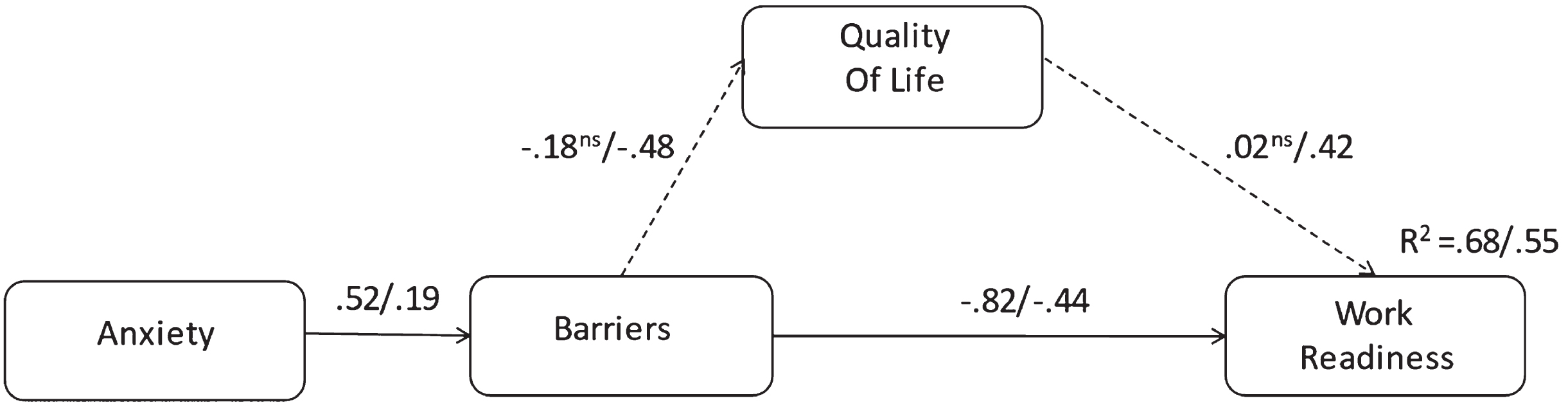
Table 1
Direct, indirect and total effects among the variables in the model
| Variables | Direct Effects Beta (SE) | Indirect Effects Beta (SE) | Total Effects Beta (SE) | ||||
| Predictor | Criterion Group | NF | Control a | NF | Control | NF | Control |
| Anxiety | Barriers | .519a (.075) | .187 (.090) | – | – | .519a (.075) | .187 (.090) |
| Quality of Life | – | – | –.096 (.053) | –.090 (.048) | –.096 (.053) | –.090 (.048) | |
| Work Readiness | – | – | –.428a (.068) | –.120 (.060) | –.428a (.068) | –.120 (.060) | |
| Barriers | Quality of Life | –.185 (.094) | –.484 (.093) | – | – | –.185 (.094) | –.484 (.093) |
| Work Readiness | –.821a (.036) | –.443 (.102) | –.003 (.011) | –.201 (.052) | –.824a (.036) | –.645 (.082) | |
| Quality of Life | Work Readiness | .017 (.054) | .416 (.100) | – | – | .017 (.054) | .416 (.100) |
aDirect, indirect, and total effects are significant at p < .05. All effects in the control group were significant.
3Results
3.1Participant characteristics
The NF1 group (N = 105) was comprised of 66% (n = 69) female, 33% (n = 34) male, and 1% (n = 1) defined as other, while the healthy individuals’ group (N = 108) was 56% (n = 60) female, 42% (n = 45) male, 2% (n = 2) transgender, and 2%, (n = 2) defined as other. The average age differed between groups with the NF1 group being M = 43.6, SD = 12.5, while the healthy individuals was M = 30.1; SD = 10.2. As noted, there was a significant difference in age discrepancy between the groups, this was largely due to inability to retain younger individuals with NF1, as discussed in the limitations. There was a relatively even split difference across groups when it came to marital status, where 43% (n = 46) in the NF1 group and 50%, (n = 56) in the healthy individuals’ group were single, and 41% (n = 43) NF1 and 39% (n = 42) were married. Respectively, both groups had a preponderance of the sample that were actively employed NF1 65% (n = 70) and healthy individuals 62% (n = 67). Only a minority of the participants in either group were unemployed 11% of (n = 12) NF1 and 16% (n = 17) of healthy individuals; or receiving social security income/disability 11% (n = 12) NF1 and 6% of (n = 6) healthy individuals.
3.2Moderating mediation analysis
Optimal model fit [41] was achieved (X2 = 9.43, p = 0.15; GFI = 0.99; CFI = 0.99; RMSEA = 0.05; PCLOSE = 0.41) when anxiety had an indirect effect on work readiness, fully mediated by barriers, with higher anxiety associated with more barriers, in turn negatively correlating with work readiness; quality of life partially mediated the effect of barriers on work readiness and was negatively associated with the former and positively with the later. There were two significant covariates in the model (Table 2). This aggregate model explained 61 % of the variance in the outcome variable work readiness. The multi-group model with an identical path structure was a good fit to the data as well (X2 = 3.69, p = 0.45; GFI = 0.99; CFI = 1.00; RMSEA = 0.00; PCLOSE = 0.68). The final multi-group model is presented in Fig. 1, and the multi-group moderated mediation results with indirect, direct and total effects for both groups presented in Table 1.
Table 2
Significant covariates in the final path modela
| Control variable | Criterion variable | B (SE) | C.R. | Beta |
| Age | Barriers | –.491 (.450) | 4.42 | –.171 |
| Gender | Quality of Life | 1.75 (.619) | 2.83 | .175 |
aEffects are significant at p < .01.
4Discussion
The current study measured the impact that generalized anxiety and quality of life have on work readiness and barriers to employment across individuals with NF1 as compared to that of the healthy individuals population using moderating mediating analysis. We found that quality of life serves as a buffer against barriers to employment, only for the healthy individuals’ population. For both groups, perceived employment barriers fully mediated the effect of anxiety on work readiness, whereby anxiety was positively associated with perceived employment barriers that in turn was negatively associated with work readiness (consistent with Buono et al. [15]). Both associations among these variables, as well as the indirect effect of anxiety on work readiness, were higher for the NF1 group.
Prior research has indicated that employment has a positive effect on psychological well-being [17, 18], and given that majority of participants were employed, we expected to observe lower anxiety rates and higher work readiness scores. However, the uncertainty surrounding the impact of the COVID-19 pandemic may have heightened perceived employment barriers and decreased work readiness despite the employment status of study participants. Recent research has indicated that increased workplace stress and anxiety were noted in returning to workplace environments [42], signaling vulnerable populations could have increased risk in sustainability, and barriers of employment [43]. Quality of life was a significant partial mediator of the relationship between perceived employment barriers and work readiness for the healthy individuals group only. The model explained 68% of the variance in the outcome among NF1 and 55% among healthy participants. The results further clarify the hypothesized relationship among these important constructs and demonstrate the usefulness of conducting moderated mediation analyses.
In interpreting the results there are several significant outcomes. Quality of life was a significant indicator for perceived employment barriers for the healthy individuals’ population but not for individuals with NF1. An explanation of these findings may be that individuals with NF1 already suffer from an array of different symptoms that are indirectly or caused by NF1 such as chronic pain [44, 45], tumors [46], leg stenosis [14, 47]; thus, due to this have habituated to reduced quality of life. Moreover, it was expected that a negative relationship would exist between perceived employment barriers and work readiness, as the more employment barriers one has, the less likely they are to enter the workforce. One explanation is that the individuals with NF1 have either accepted or forgone the potential reductions of quality of life due to inabilities to obtain or maintain jobs, as they understand the implications of the disease. A recently published article [48], indicated that 50% of individuals with disabilities during COVID-19 met the criterion for a generalized anxiety. Wolter et al. [19] reported that individuals with NF1 had moderate-to-high levels of stress, with a majority of these stressors coming directly from the pandemic due to either unemployment or loss of significant income. Future understanding of the prolonged impact of generalized anxiety and its disruption of employment opportunities following the pandemic should be evaluated within individuals with other diseases and disabilities.
4.1Vocational rehabilitation
VR is one such intervention that could mitigate the impact that the pandemic has had on people with NF1. VR focuses on assisting people with disabilities in obtaining and maintaining employment that is compatible with their knowledge, skills, interests, and functional abilities [49]. Employment placement and retention are accomplished by reducing the impact of employment related barriers and developing individualized employment plans that are customized to the individual’s vocational, psychological, social, and medical needs [50, 51]. VR professionals identify the aforementioned barriers for individuals with NF1 and facilitate/coordinate services to improving their needs and remove employment-related obstacles, as well as engage in advocacy, assist in the request of reasonable accommodations, and recommend workplace modifications [49, 52, 53]. Accommodations that individuals with NF1 may need have yet to be fully explored, but given that NF1 is associated with chronic pain [54], the following accommodations may be useful in improving work readiness and decrease employment related barriers due to disability, including decreasing or reallocating lifting/reaching/pushing/pulling requirements (Job Accommodations Network, 2022) and flexible work hours, working at home, and job/workplace modifications [55]. In determining disability rights for people with NF1 and other disabilities, resources such as employer assistance programs [56], accommodation problems and solutions with telework or reopening, and laws such as the Equal Employment Opportunity Commission, ADA, and Rehabilitation Act [52] can assist in preparing appropriate accommodation requests consistent with legislation.
4.2Limitations of study
The current study is not without limitations. As noted, there is a difference in the age groups of the healthy individuals and the individuals with NF1. Given the rarity of the NF1, and inclusion criterion that were preestablished based on previous works [19], it was notably difficult to obtain equally balanced groups in terms of age. Specifically, we did have difficulty finding younger employed adults with NF1. The notable age difference could partially explain the differences in the results between the groups. However, as noted in a previous study [19], adults between 18 to 81 years of age with NF1 had consistent anxious feelings and reduced quality of life when it came to COVID-19. The current study extended these findings specifically to barriers to employment and work readiness, indicating the impact that barriers to employment and work readiness can have on quality of life and anxiety. Future studies should evaluate the within and between differences across age groups (e.g., 18–34, 35–50, 51–66).
A second limitation is that the current study employed a cross-sectional approach and that all participants lived in the U.S. Given that evaluation was a singular recording period and that participants only came from a limited population, the likelihood for generalization across cultures and reliability of the information is reduced. Future impact of the COVID-19 pandemic has yet to be discussed within the employment for individuals with rare diseases, but the anticipated greater effects of the COVID-19 pandemic will be extending well past the deflation of the number of outbreaks. Lastly, despite the result’s implications, additional factors (e.g., family relationships, chronic pain) can impede the likelihood of successful work placement or continuance of work and the current study did not thoroughly evaluate these additional variables. More research is needed to provide a complete understanding of the impact that a rare disease has on work related success and its impact on the work-place environment.
5Conclusion
The current study attempted to explain how work readiness and barriers to employment within individuals with NF1 compared to healthy individuals during the COVID-19 pandemic. The results imply that anxiety and quality of life are significant mediators and require consideration in terms of evaluation and facilitation of employment maintenance and acquisition for individuals with NF1.
Ethics approval
Prior to any data collection, approval from the Human Subjects Committee (HSC) at the Yale University’s Institutional Review Board (Research ID# 2000026514) was received. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000.
Informed consent
Informed consent was obtained from all participants before being included in the study.
Conflicts of interest
The authors declare that they have no conflict of interest.
Acknowledgments
The authors have no acknowledgements.
Funding
The authors report no funding.
References
[1] | Hwang H , Hur WM , Shin Y . Emotional exhaustion among the South Korean workforce before and after COVID-19. Psychol Psychother. (2021) ;94: (2):371–81. |
[2] | Kochhar R , Bennett J . U.S. labor market inches back from the COVID-19 shock, but recovery is far from complete. 2021. |
[3] | Kujawa A , et al. Exposure to COVID-19 pandemic stress: Associations with depression and anxiety in emerging adults in the United States. Depress Anxiety. (2020) ;37: (12):1280–8. |
[4] | Liu CH , et al. Evidence for elevated psychiatric distress, poor sleep, and quality of life concerns during the COVID-19 pandemic among U.S. young adults with suspected and reported psychiatric diagnoses. Psychiatry Res. (2020) ;292: :113345. |
[5] | Rumrill PD , et al. Differences in employment concerns between Hispanic and Caucasian persons with multiple sclerosis: A propensity score matching analysis. Journal of Vocational Rehabilitation. (2021) ;54: :33–42. |
[6] | Umucu E . Functional limitations and worrying to lose employment among individuals with chronic conditions and disabilities during COVID- A hierarchical logistic regression model. Journal of Vocational Rehabilitation. (2021) ;54: :25–32. |
[7] | Fuentes K , Lindsay S . Workplace accommodations during the COVID-19 pandemic: A scoping review of the impacts and implications for people with disabilities. Work. 2022. |
[8] | Sani G , et al. Mental health during and after the COVID-19 emergency in Italy. Psychiatry Clin Neurosci. (2020) ;74: (6):372. |
[9] | Shaw WS , et al. Opening the Workplace After COVID- What Lessons Can be Learned from Return-to-Work Research? Journal of Occupational Rehabilitation. (2020) ;30: (3):299–302. |
[10] | Taylor T , et al. Safely Returning America to Work: Part I: General Guidance for Employers. J Occup Environ Med. (2020) ;62: (9):771–9. |
[11] | Wong J , et al. Employment Consequences of COVID-19 for People with Disabilities and Employers. Journal of Occupational Rehabilitation. (2022) :1–9. |
[12] | Anderson JL , Gutmann DH . Neurofibromatosis type 1. Handb Clin Neurol. (2015) ;132: :75–86. |
[13] | Kodra Y , et al. Health-related quality of life in patients with neurofibromatosis type 1. A survey of 129 Italian patients. Dermatology. (2009) ;218: (3):215–20. |
[14] | Tonsgard JH . Clinical manifestations and management of neurofibromatosis type 1. Semin Pediatr Neurol. (2006) ;13: (1):2–7. |
[15] | Buono FD , et al. The mediating effects of quality of life, depression, and generalized anxiety on perceived barriers to employment success for people diagnosed with Neurofibromatosis Type 1. Orphanet J Rare Dis. (2021) ;16: (1):234. |
[16] | Krueger AB , et al. Job search, emotional well-being, and job finding in a period of mass unemployment: Evidence from high frequency longitudinal data. Brookings apers on Economic Activity 2011. |
[17] | Rocha C , Crowell JH , McCarter AK . The Effects of Prolonged Job Insecurity on the Psychological Well-Being of Workers. Journal of Sociology and Social Welfare. (2006) ;33: (3):9–28. |
[18] | Fjermestad KW . Health complaints and work experiences among adults with neurofibromatosis 1. Occup Med (Lond). (2019) ;69: (7):504–10. |
[19] | Wolters PL , et al. Impact of the coronavirus pandemic on mental health and health care in adults with neurofibromatosis: Patient perspectives from an online survey. Am J Med Genet A. (2022) ;188: (1):71–82. |
[20] | Ferner RE . Psychological Impact of the Neurofibromatoses, in Neurofibromatoses in Clinical Practice. Springer London: London. (2011) ;129–140. |
[21] | Ferner RE , et al. Evaluation of quality of life in adults with neurofibromatosis 1 (NF1) using the Impact of NF1 on Quality Of Life (INF1-QOL) questionnaire. Health Qual Life Outcomes. (2017) ;15: (1):34. |
[22] | Page PZ , et al. Impact of neurofibromatosis 1 on Quality of Life: a cross-sectional study of 176 American cases. Am J Med Genet A. (2006) ;140: (18):1893–8. |
[23] | Pasini A , et al. Detecting anxiety symptoms in children and youths with neurofibromatosis type I. Am J Med Genet B Neuropsychiatr Genet. (2012) ;159B: (7):869–73. |
[24] | Adamou M , et al. Occupational issues of adults with ADHD. BMC Psychiatry. (2013) ;13: :59. |
[25] | Jacobs M , Hart EP , Roos RAC . Cognitive Performance and Apathy Predict Unemployment in Huntington’s Disease Mutation Carriers. J Neuropsychiatry Clin Neurosci. (2018) ;30: (3):188–93. |
[26] | Reis BB , et al. Quality of life, work ability, and facial deformities. Rev Bras Med Trab. (2018) ;16: (3):318–26. |
[27] | Vélez-Coto M , et al. Unemployment and general cognitive ability: A review and meta-analysis. Journal of Economic Psychology. (2021) ;87: :102430. |
[28] | Herbert IP , et al. Graduate employability, employment prospects and work-readiness in the changing field of professional work. The International Journal of Management Education. (2020) ;18: (2):100378. |
[29] | Lau PL , Wilkins-Yel KG , Wong YJ . Examining the Indirect Effects of Self-Concept on Work Readiness Through Resilience and Career Calling. Journal of Career Development. (2019) ;47: (5):551–64. |
[30] | Cmar JL , McDonnall MC . Short-Term Effectiveness of Job Search Skills Training: Comparisons by Summer Work Experience Participation. Rehabilitation Counseling Bulletin. (2020) ;64: (2):86–96. |
[31] | Rumrill PD , et al. Differences in employment concerns between Hispanic and Caucasian persons with multiple sclerosis: A propensity score matching analysis. Journal of Vocational Rehabilitation. (2021) ;54: (1):33–42. |
[32] | Umucu E . Functional limitations and worrying to lose employment among individuals with chronic conditions and disabilities during COVID- A hierarchical logistic regression model. Journal of Vocational Rehabilitation. (2021) ;54: (1):25–32. |
[33] | Jesus TS , Landry MD , Jacobs K . A ‘new normal’ following COVID-19 and the economic crisis: Using systems thinking to identify challenges and opportunities in disability, telework, and rehabilitation. Work. (2020) ;67: (1):37–46. |
[34] | Ware JK, Kosinski M, Keller SD. SF-12: How to score the SF-12 physical and mental health summary scales. 1995, Lincoln, RI: QualityMetric Incorporated. |
[35] | Huo T , et al. Assessing the reliability of the short form 12 (SF-12) health survey in adults with mental health conditions: a report from the wellness incentive and navigation (WIN) study. Health and Quality of Life Outcomes. (2018) ;16: (1):34. |
[36] | Spitzer RL , et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) ;166: (10):1092–7. |
[37] | Preacher KJ , Rucker DD , Hayes AF . Addressing moderated mediation hypotheses: Theory, methods, and prescriptions. Multivariate Behavioral Research. (2007) (42):185–227. |
[38] | Kline RB . Principles and practice of structural equation modeling. (2011) : Guilford press. |
[39] | Bollen KA , Stine RA .Bootstrapping Goodness-of-Fit Measures in Structural Equation Models. Sociological Methods & Research. (1992) ;21: (2):205–29. |
[40] | Hoyle RH . Path analysis and structural equation modeling with latent variables. (2012) ;333–67. |
[41] | Bentler PM . Comparative fit indexes in structural models. Psychological Bulletin. (1990) ;107: (2):238. |
[42] | Liu X , et al. Fears of COVID-19 and cancer recurrence related to work sustainability among male cancer survivors. JOMH. (2021) ;17: (2):49–54. |
[43] | Yuan Z , Ye Z , Zhong M . Plug back into work, safely: Job reattachment, leader safety commitment, and job engagement in the COVID-19 pandemic. J Appl Psychol. (2021) ;106: (1):62–70. |
[44] | Buono FD , et al. Pain symptomology, functional impact, and treatment of people with Neurofibromatosis type 1. J Pain Res. (2019) ;12: :2555–61. |
[45] | Wolkenstein P , et al. Quality-of-life impairment in neurofibromatosis type a cross-sectional study of 128 cases. Arch Dermatol. (2001) ;137: (11):1421–5. |
[46] | Jett K , Friedman JM . Clinical and genetic aspects of neurofibromatosis 1. Genet Med. (2010) ;12: (1):1–11. |
[47] | Suratwala SJ , et al. Malignant peripheral nerve sheath tumor of the sciatic nerve presenting with leg pain in the setting of lumbar scoliosis and spinal stenosis. Spine Deform. (2020) ;8: (2):333–8. |
[48] | Wang K , et al. Predicting depression and anxiety among adults with disabilities during the COVID-19 pandemic. Rehabil Psychol. 2022. |
[49] | Sprong ME , et al.. The role of disability in the hiring process: Does knowledge of the Americans with Disabilities Act Matter? Journal of Rehabilitation. (2019) ;4: :42–0. |
[50] | Austin B , et al. Utilization of interviewing as an assessment tool to enhance vocational rehabilitation service delivery: Fostering the therapeutic alliance and professionals’ judgment accuracy. Vocational Evaluation and Work Adjustment Association Journal and Vocational Evaluation and Career Assessment Journal. (2015) ;37–51. |
[51] | Moreno-Tucker V , McCarthy AK , Sprong ME . Unrecognized potential: The value of the rehabilitation professional in the transition process. Vocational Evaluation and Work Adjustment Association Journal. (2017) ;41: (2):66–77. |
[52] | Commission, U.S.E.E.O., The Rehabilitation Act of 1973 1973: Washington DC. |
[53] | Bonaccio S , et al. The Participation of People with Disabilities in the Workplace Across the Employment Cycle: Employer Concerns and Research Evidence. J Bus Psychol. (2020) ;35: (2):135–58. |
[54] | Allen TM , et al. The Relationship Between Heart Rate Variability, Psychological Flexibility, and Pain in Neurofibromatosis Type 1. Pain Practice. (2018) ;18: (8):969–78. |
[55] | Imahashi K , et al. Perceptions regarding a range of work-related issues and corresponding support needs of individuals with an intractable disease. Intractable Rare Dis Res. (2016) ;5: (3):202–6. |
[56] | Inclusion EAaRNoD. COVID-19 and Job Applicants and Employees with Disabiliites: Emerging Practices to Employ and Protect Workers, U.D.o. Labor, Editor. 2020: Washington DC. |


