
Remote working during the COVID-19 pandemic: Computer-related musculoskeletal symptoms in university staff
Abstract
BACKGROUND:
The COVID-19 pandemic resulted in mandatory remote working for workers in many sectors, including education.
OBJECTIVE:
This study aimed to investigate the physical characteristics of workspaces, computer use, and prevalence, associated factors, and reported impact of computer-related musculoskeletal symptoms (MSS) among university staff during the COVID-19 pandemic.
METHODS:
A cross-sectional study of staff in a university in Ireland was conducted in March 2021. An anonymous online survey of computer use, work practices and 3-month prevalence and the reported impact of computer-related MSS (modified Nordic Musculoskeletal Questionnaire) was conducted. Data analysis involved descriptive statistics and relationships were tested using chi-squared analysis.
RESULTS:
The analysis included 1045 responses. The majority (63%) worked solely from home, used a laptop more frequently than a desktop computer, and worked a greater number of hours. Almost half (48%) did not have a dedicated home workspace. More respondents reported their university workspace (72%) was more comfortable than their home workspace (51.2%) (p < 0.0001). Prevalence of computer-related MSS was 83% : neck (62%), shoulder (57%), lower back (47%). Laptop-related MSS was reported more frequently (82%) than desktop-related MSS (65%) (p < 0.05). Computer-related MSS was associated with workspace, equipment at home, laptop use, female gender, and righthandedness (p < 0.05). A reduction in non-work-related activities (35%), work activities (18%) and seeking medical attention (24%) was reported.
CONCLUSION:
The prevalence of computer-related MSS was high and associated with remote working. Further studies that aim to mitigate the risks of computer-related MSS in those working remotely or in hybrid models are required.
1Introduction
The prevalence and associated risk factors of computer-related musculoskeletal symptoms (MSS) in the workforce have been widely researched [1–4]. The associations between computer-related MSS and female gender [5, 6], older age [7, 8], longer time spent working at a computer [6, 7], poor posture [9] and poor workstation design [10] have been documented in this population.
Some cross-sectional studies have investigated the 12-month prevalence of computer-related MSS among university employees, with prevalence rates of 94% [11], 85% [12], 78.7% [13] and 42.5% [14] reported. The discrepancy in prevalence may be partly explained by methodological differences, with some studies utilising interviews [11], while others used questionnaire surveys [12, 13]. Algarni et al. also used a questionnaire survey, but only included males in their study [14]. Studies also reported relationships between MSS and computer work exposures [11], workstation configuration, working posture and training [13, 14], and psychosocial risk exposures [12].
Due to regulations imposed during the COVID-19 pandemic, remote working was mandatory for workers in many sectors worldwide, including that of tertiary education. In the Republic of Ireland, the first case of COVID-19 was reported on February 29th, 2020 [15], and a stay-at-home order was issued on 27th March 2020 in response to the rising number of cases (n = 1639) [16]. Factors associated with remote working have not been previously addressed, despite the fact that many employees, including academics/university staff, have traditionally conducted at least some of their work away from the office environment [13, 17]. It has been suggested that remote working results in greater engagement in screen time [17] and stress [18] than working onsite. In the case of university staff during the pandemic, this was due to academics delivering lectures online and preparing additional supplemental online resources for students [18].
A recent questionnaire survey of employees from a wide range of industries and sectors in Ireland was conducted during one week in October 2020 to explore aspects concerning remote working during the COVID-19 pandemic [19]. ‘Physical workspace’ was one of the top three challenges for employees when working remotely, with 18% reporting that their physical workspace was a problem for them. However, the components of a physical workplace were not explored in the study. The working environment has been shown to influence the prevalence of MSS [3, 20, 21].
Mandatory remote working during the COVID-19 pandemic triggered some research focussing specifically on university employees. Gerding et al. [22] carried out a questionnaire survey of home office ergonomics and discomfort of 843 university employees in the US. The authors reported that laptops were widely used, and that respondents were working at sub-optimal workstations. Greater than 40% of the respondents had moderate to severe discomfort while working at home during the COVID-19 pandemic, compared to 21.5% prior to the pandemic when they were working on the university campus. Similarly, a study conducted among 220 staff in an Iranian university found a significant increase in the prevalence of self-reported musculoskeletal disorders among staff during COVID-19 compared to pre-COVID-19 [23]. Research is required to further investigate the issues around remote working for university staff. No such research has been carried out on university staff in Ireland to date.
The aim of the current study was to explore the prevalence of computer-related musculoskeletal symptoms in university staff during the COVID-19 pandemic. The study objectives were to: (i) investigate the pattern of computer use; (ii) investigate the computer-related workstations; (iii) establish the prevalence of computer-related symptoms; (iv) determine the relationship, if any, between computer use and musculoskeletal symptoms; (v) investigate the reported impact, if any, of computer-related musculoskeletal symptoms.
2Methods
2.1Participants
Current academic, administrative, library, laboratory, and research staff from a university in Ireland were included. All participants were at least 18 years old. Staff who did not use a computer for work purposes were excluded.
2.2Procedure
The Secretary’s Office at the university agreed to act as gatekeeper for the study and an invitation email including an anonymous online survey link (Qualtrics, Provo, UT) [24] and a participant information leaflet (PIL) were sent to all academic, administrative, library, laboratory and research staff on the staff mailing lists. Consent was assumed on completion and submission of the questionnaire. After seven days, a thank you/reminder email was sent to all staff.
2.3Study design
A cross-sectional online anonymous survey was conducted in March 2021 using a questionnaire related to computer use and musculoskeletal symptoms in the past 3 months.
2.4Questionnaire design
The questionnaire contained 39 questions with item responses being binary, multiple-choice options including ‘other’, or Likert-type scales. The questionnaire consisted of 4 sections: computer use; other activities; demographics; and musculoskeletal symptoms. Section 1 was based on questions used in previous studies [25–28] and enquired about the amount of time spent working at home and/or at the university workplace, the hours spent on average per day using a laptop or a desktop computer (<1 h;≥1 h-<2 h;≥2 h-<4 h;≥4 h-<6 h;≥6 h), the length of time usually spent on a laptop or desktop at any one time (<0.5 h;≥0.5 h-<1 h;≥1 h-<2 h;≥2 h-<4 h;≥4 h-<6 h;≥6 h), and if there were usually breaks taken during this time (yes; no). The questionnaire enquired about the use of equipment, such as an office chair, desk, monitor, keyboard, and mouse. The questionnaire also enquired about the perceived comfort of their university and/or home workstation(s) (comfortable place to work all of the time; most of the time; sometimes; rarely; never). Section 2 sought information about participation in sport [29] and playing a musical instrument [30, 31], as some are associated with musculoskeletal disorders. Section 3 sought demographic information related to age (20-29; 30-39; 40-49; 50-59; 60+), gender (male; female; non-binary; prefer not to say), handedness (left; right), faculty/administrative area (Arts; Engineering; Health Sciences; Administration) and job description (academic; administrative; clinical; demonstrator; researcher; technical officer; other). Section 4 was a Nordic Musculoskeletal Questionnaire [32], modified to enquire about musculoskeletal symptoms in the past 3 months and to include ‘pins and needles’ in the definition of musculoskeletal discomfort. For the purposes of this study a computer-related musculoskeletal symptom was defined as ‘any ache, pain, discomfort, pins and needles or numbness associated with your use of a laptop or desktop computer’. In keeping with the Occupational Safety and Health Administration (OSHA) definition of ‘work-related’ symptoms, the respondents were to report symptoms in any body part that were ‘caused by’ or ‘aggravated by’ laptop or desktop computer use [33]. The respondents were also asked if any musculoskeletal symptoms impacted their work (yes; no) or leisure activities (yes; no) [32] and if they sought medical treatment or advice (yes; no). The ‘skip logic’ function in Qualtrics was used to send respondents to the relevant questions based on a previous response to a question. The full questionnaire is available elsewhere in a report of the study [34].
2.5Data analysis
Data were transferred from Qualtrics to SPSS and screened and cleaned to ensure accuracy. Statistical analysis was completed using Statistical Package for Social Sciences (SPSS) version 27 for Windows (IBM Corp., Armonk, NY, USA). Data analysis and presentation predominantly involved descriptive statistics. Frequency and percentage were calculated for categorical variables. The participants were requested to complete the questionnaire once. In the questionnaire, they were asked about symptoms associated with laptop and desktop use separately. The participants could checkmark one or both as appropriate. The authors subsequently computed the data for the combined variable ‘laptop or desktop’. The associations between musculoskeletal symptoms and risk factors were explored using the chi-square test for independence, and comparison of means was performed using the independent samples t-test. Statistical significance was set at p < 0.05.
3Results
3.1Response rate
All employees on the university staff email lists (n = 6653) working at the time of the study were alerted to the survey. A total of 1121 responded, giving a response rate of 16.8%. Seventy-six (n = 76) surveys were incomplete and excluded from the analysis, therefore the analysis was based on 1045 responses.
3.2Demographics
The respondents were mostly female (67.7%) and right-handed (90.2%) and were aged 20-29 (7.9%); 30-39 (22.7%); 40-49 (33.5%); 50-59 (23.3%); or 60+ (12.6%). Respondents represented the 3 faculties in the university (31.2% (Arts); 26.3% (Sciences); 24.8% (Engineering)) and the other departments (17.7%), and were administrators (42%), academics (31.9%), researchers (17%), technicians (2.8%), librarians (2.2%), or other (4.1%) staff.
3.3Working environment during COVID-19
The majority of respondents (63.6%; n = 665) reported they worked from home all the time, 33.7% (n = 352) had a hybrid working model combining home and university, and 2.7% (n = 28) reported they worked at the university site all the time. The usual workspace for those who worked from home included a dedicated home workspace (52%), kitchen/dining table (29%) and bedroom (9%).
3.4Pattern of computer use
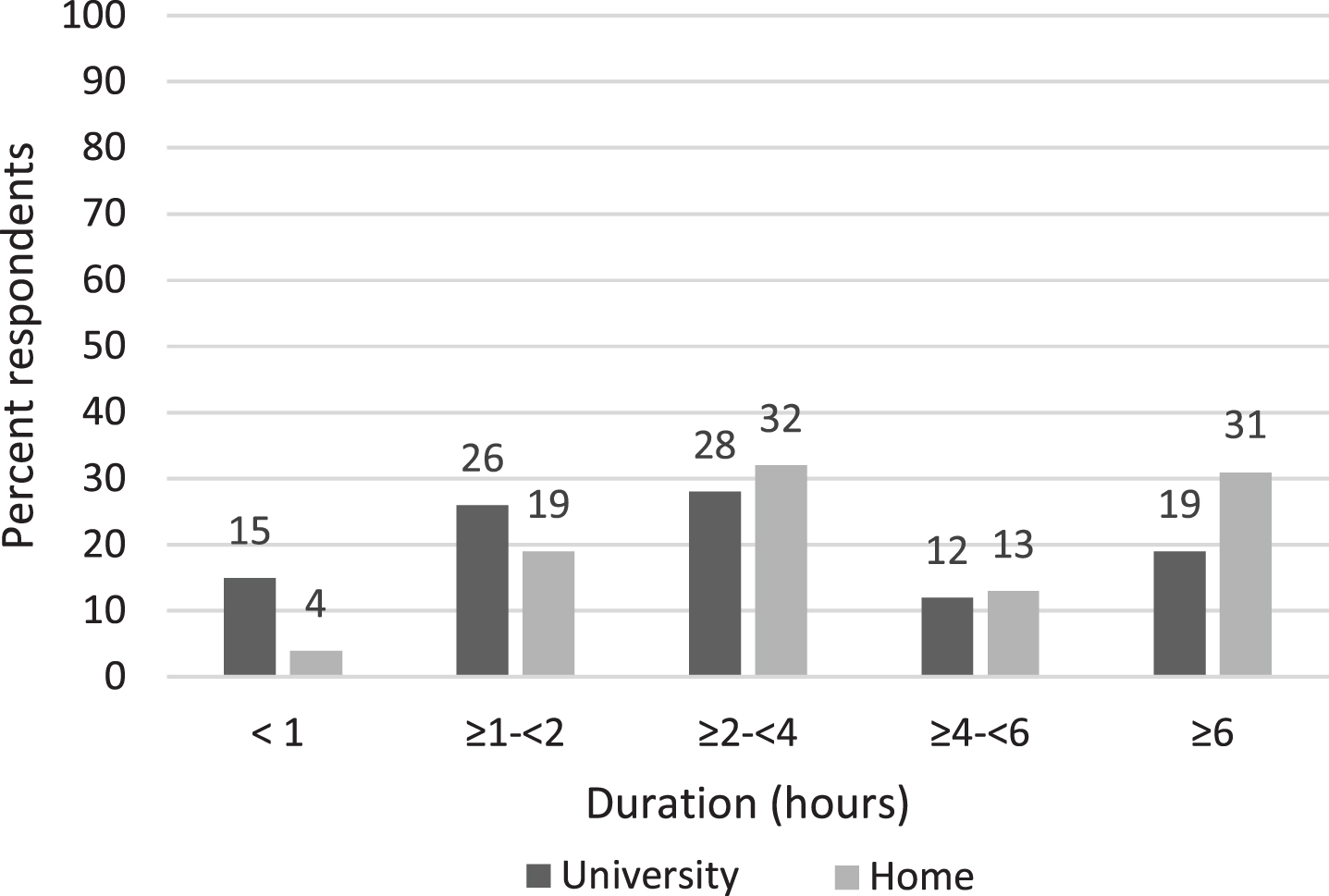
A laptop was more frequently used at home than onsite at the university. When working at the home workspace (n = 1017), 88.1% of respondents used a laptop compared to 50% who used a laptop at their university workspace (n = 380). Desktop computers were used more frequently at the university (68%) than at home (24%). The respondents reported using computers for longer durations daily (Fig. 1) and at any given time (Fig. 2) at home than they were at the university. A significantly greater proportion of respondents took breaks from computer use when working from home (76.4%) compared to when working in the university (68.6%) (p < 0.01).
Fig. 1
Daily duration of computer use.
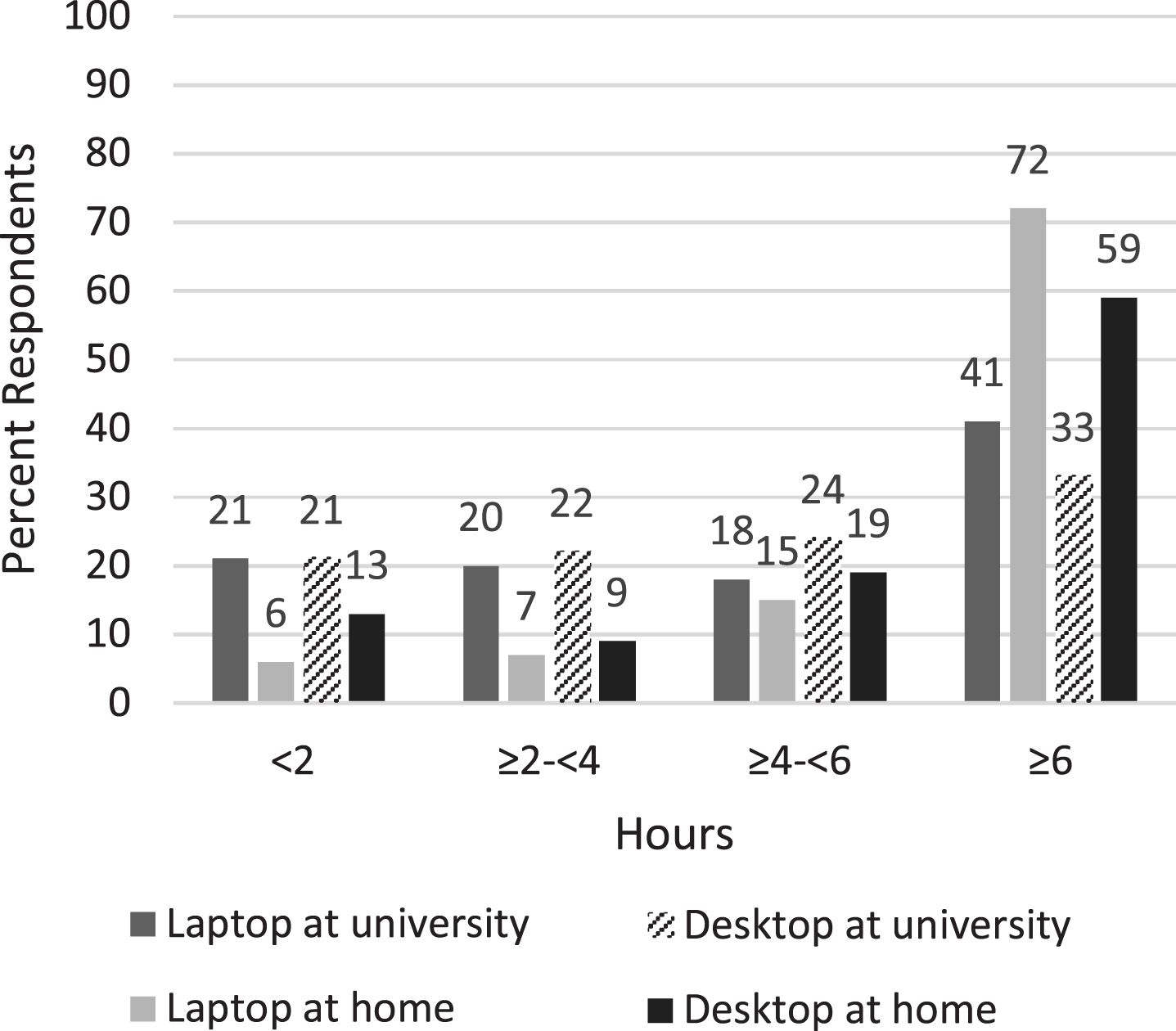
Fig. 2
Computer use at any one time.
3.5Use of equipment
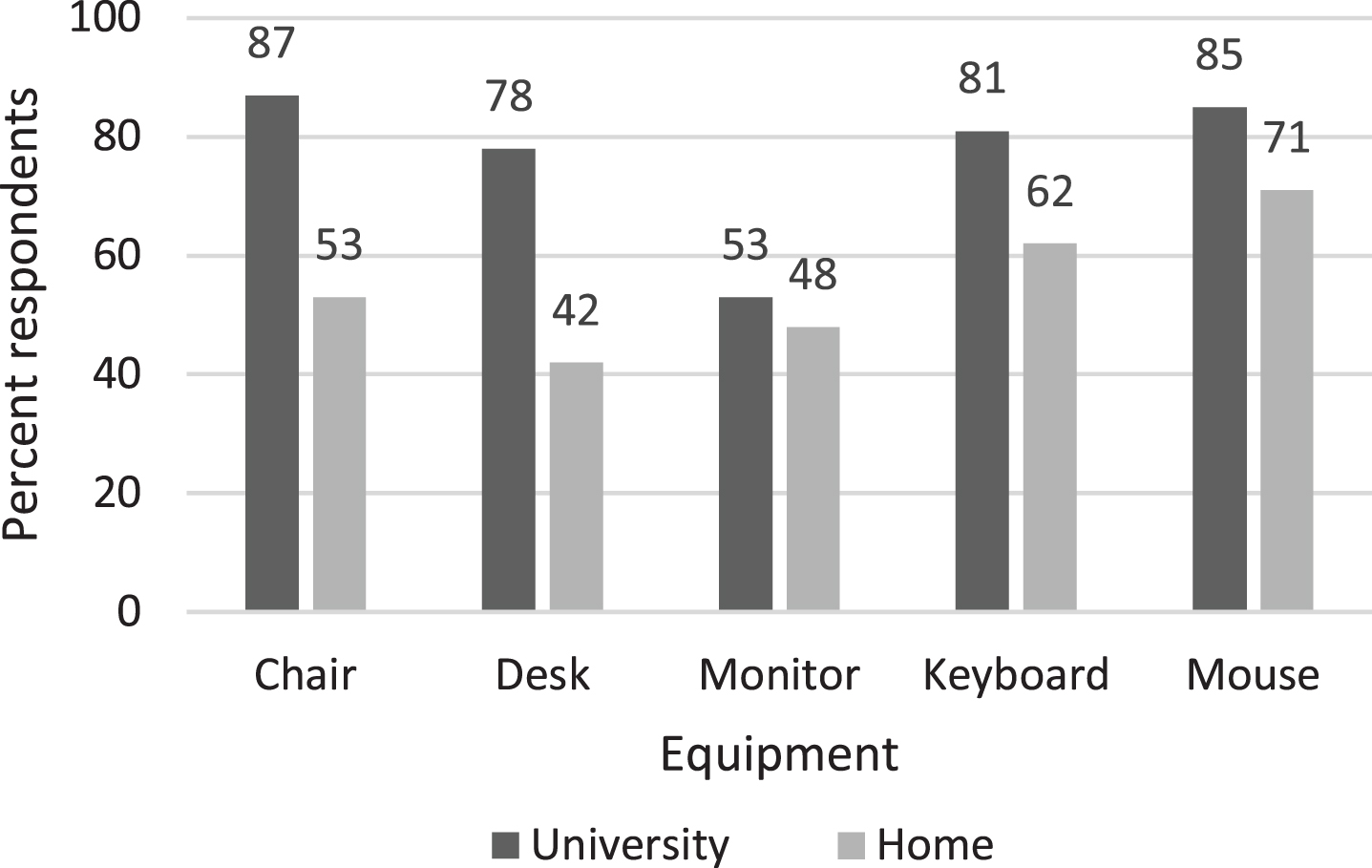
Computer equipment was more likely to be used onsite at the university than at home (Fig. 3), and the difference was significant for using an office chair (p < 0.00001), desk (p < 0.00001), keyboard (p < 0.00001), and mouse (p < 0.00001), but not for a monitor (p = 0.08).
Fig. 3
Use of equipment.
3.6Comfort
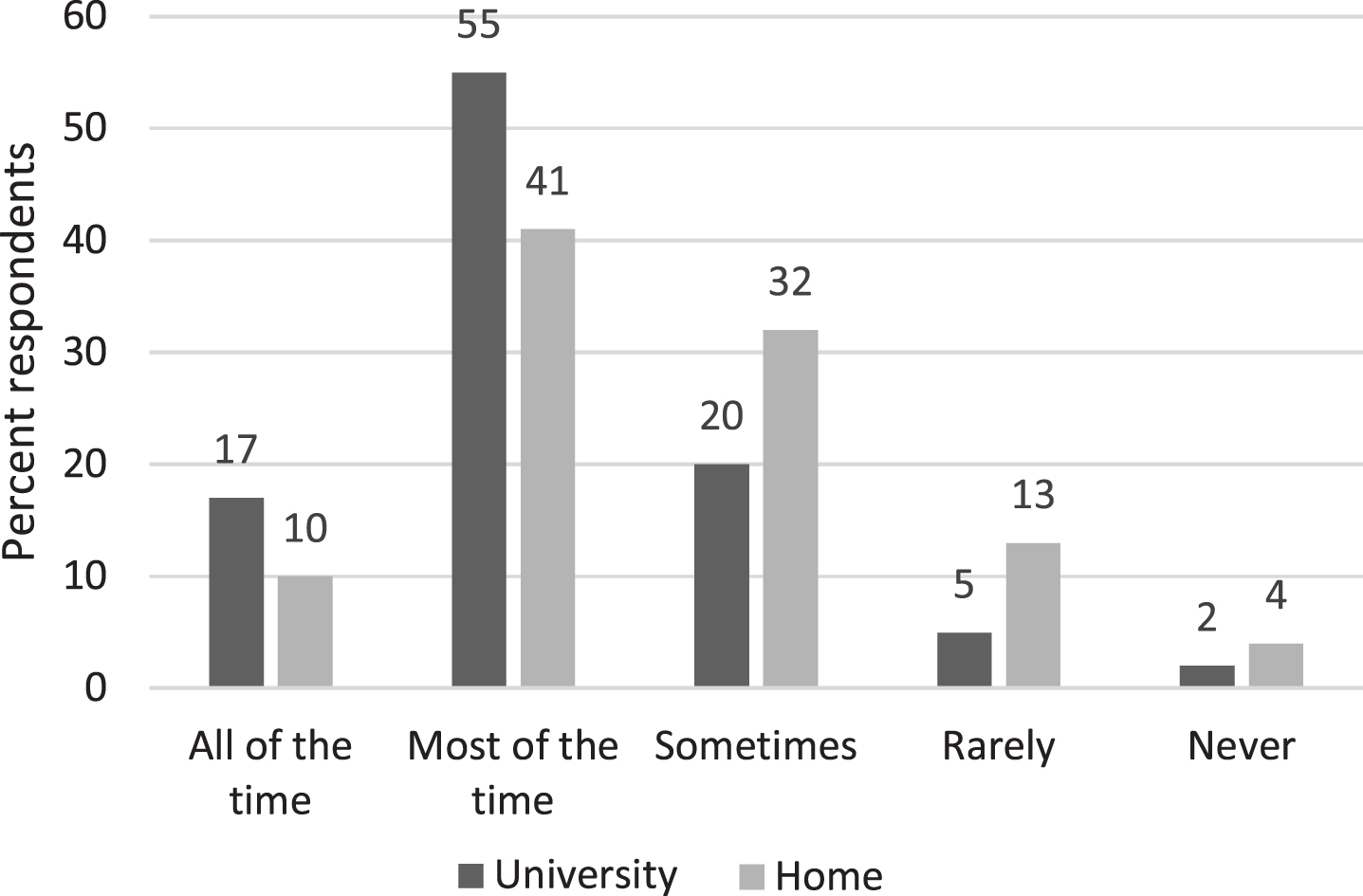
The comfort of the university workspace was reported to be greater than the home workspace (Fig. 4), with significantly more respondents reporting they were comfortable all or most of the time in their workspace onsite at the university (72%) compared to those in their home workspace (51.2%), (p < 0.0001).
Fig. 4
Comfort of the workspace.
3.7Computer-related MSS
Eighty-three percent (83%) of respondents reported computer-related MSS. The most commonly reported body areas were neck (62.4%), shoulder (57%), and lower back (47.3%). Over eighty percent (82.2%) reported MSS related to laptop use and 64.6% reported MSS related to desktop use, and the prevalence of laptop-related MSS was significantly higher than desktop-related MSS for the neck, shoulder, and lower back (Table 1). There was also a significant association between MSS and gender, and between MSS and handedness. Respondents who were female or righthanded were more likely to report computer-related MSS. There was no association between age and computer-related MSS (Table 2). Staff roles were collapsed into 2 categories (academic/research and administration). Chi-square analysis demonstrated there was no significant difference in the prevalence of computer-related MSS between the two groups (p = 0.66). In addition, there was no association between sporting activity (p = 0.53) or playing a musical instrument (p = 0.25) and computer-related MSS. The mean number of hours per week playing sport (p = 0.72), a musical instrument (p = 0.16) or using technology for leisure (p = 0.71) was not significantly different for those who reported computer-related MSS compared to those who did not.
Table 1
Comparison of computer-related MSS for laptop (n = 697) and desktop (n = 260) computer use by body part
| Body part | Type of computer | MSS % (n) | No MSS % (n) | X2 | P |
| Neck | Laptop | 75.6 (527) | 24.4 (170) | 5.145 | 0.0233 |
| Desktop | 68.1 (177) | 31.9 (83) | |||
| Shouder | Laptop | 69.7 (486) | 30.3 (211) | 7.080 | 0.0078 |
| Desktop | 60.4 (157) | 39.6 (103) | |||
| Elbow | Laptop | 18.8 (131) | 81.2 (566) | 0.038 | 0.8453 |
| Desktop | 19.6 (51) | 80.4 (209) | |||
| Wrist/hand | Laptop | 46.9 (327) | 53.1 (370) | 1.997 | 0.1577 |
| Desktop | 41.5 (108) | 58.5 (152) | |||
| Upper back | Laptop | 41.2 (287) | 58.8 (410) | 2.092 | 0.1480 |
| Desktop | 35.8 (93) | 64.2 (167) | |||
| Lower back | Laptop | 57.5 (401) | 42.5 (296) | 35.047 | 0.0001 |
| Desktop | 35.8 (93) | 64.2 (167) | |||
| Hip/thigh | Laptop | 24.2 (169) | 75.8 (528) | 0.588 | 0.4432 |
| Desktop | 26.9 (70) | 73.1 (190) | |||
| Knee | Laptop | 16.2 (113) | 83.8 (584) | 0.423 | 0.5156 |
| Desktop | 14.2 (37) | 85.8 (223) | |||
| Foot/ankle | Laptop | 8.2 (57) | 91.8 (640) | 0.893 | 0.3448 |
| Desktop | 10.4 (27) | 89.6 (233) |
Significant values are italicised and emboldened.
Table 2
Association between computer-related MSS and age, gender* and handedness
| Laptop (n = 891) | Desktop (n = 440) | Laptop or desktop (n = 1015) | ||||
| Risk factors | Symptoms % (n/n) | X2 (p value) | Symptoms % (n/n) | X2 (p value) | Symptoms % (n/n) | X2 (p value) |
| Age n = 1022 | n=891 | X2 = 4.989 | n=440 | X2 = 3.497 | n=1015 | X2 = 2.297 |
| p = 0.288 | p = 0.478 | p = 0.681 | ||||
| 20-29 n = 81 | 85.9(67/78) | 54.1(20/37) | 85.2(69/81) | |||
| 30-39 n = 232 | 84.0(172/206) | 61.4(59/96) | 82.7(191/231) | |||
| 40-49 n = 342 | 84.2(245/291) | 65.6(105/160) | 85(289/340) | |||
| 50-59 n = 238 | 78.9(168/213) | 65.9(60/91) | 80.9(191/236) | |||
| 60+ n = 129 | 77.7(80/103) | 71.4(40/56) | 81.1(103/127) | |||
| Gender n = 1001* | n=876 | X2 = 7.712 | n=433 | X2 = 1.488 | n=1001 | X2 = 6.929 |
| p = 0.005 | p = 0.222 | p = 0.008 | ||||
| Male n = 313 | 76.5(199/260) | 33.8(106/156) | 78.3(245/313) | |||
| Female n = 688 | 84.4(520/616) | 24.9(172/277) | 85(585/688) | |||
| Handedness n = 1011 | n=887 | X2 = 8.243 | n=439 | X2 = 0.000 | n=1011 | X2 = 8.183 |
| p = 0.004 | p = 0.985 | p = 0.004 | ||||
| Left n = 99 | 70.9(61/86) | 64.6(31/48) | 72.7(72/99) | |||
| Right n = 912 | 83.4(668/801) | 64.3(252/391) | 84.1(767/912) | |||
*Males and females only included in the analysis. Significant p values are italicised and emboldened.
There was a significant association between MSS and the use of equipment at home, with a lower prevalence of MSS (laptop or desktop) associated with the use of an office chair (p < 0.05), desk (p < 0.00001) and monitor (p < 0.05), but not with a keyboard (p = 0.58) or mouse (p = 0.52) (Table 3). There were no significant associations between MSS and equipment use onsite at the university. Those who did not have a dedicated home workspace were more likely to have musculoskeletal symptoms (87.4%) than those who had (80.6%) (p < 0.05). There were no associations between daily duration of computer use, but computer use for≥2 hours at any one time at home was associated with MSS (p < 0.05).
Table 3
Association between use of equipment at home and computer-related MSS
| Equipment at home | Computer-related MSS | X2 | p | ||
| Yes n (%) | No n (%) | ||||
| Chair | Yes | 419 (80.7) | 100 (19.3) | 7.2346 | 0.007 |
| No | 410 (87) | 61 (13) | |||
| Desk | Yes | 327 (77.5) | 95 (22.5) | 21.0931 | <0.00001 |
| No | 502 (88.4) | 66 (11.6) | |||
| Monitor | Yes | 380 (80.2) | 94 (19.8) | 8.5045 | 0.004 |
| No | 449 (87) | 67 (13) | |||
| Keyboard | Yes | 511 (83.2) | 103 (16.8) | 0.312 | 0.576 |
| No | 318 (84.6) | 58 (15.4) | |||
| Mouse | Yes | 590 (83.3) | 118 (16.7) | 0.298 | 0.585 |
| No | 239 (84.8) | 43 (15.2) | |||
Laptop n = 697; Desktop n = 260. Significant p values are italicised and emboldened.
3.8Reported impact of computer-related MSS
Eighteen percent of respondents reduced work, 35% reduced non-work-related activities and 24% sought medical attention due to computer-related musculoskeletal symptoms. A significantly higher proportion of males (33.8%) reduced their work due to MSS compared to females (17.9%) (p < 0.001). There was also a significant association between age and having to reduce work due to MSS. A greater proportion of younger respondents (<40 years) had to reduce work due to computer-related MSS (29.6%) than those who were 40-49 (19.2%), 50-59 (18.7%), or 60+ (19.4%) (p < 0.05).
4Discussion
This study was undertaken in March 2021, at a time when employees were continuing to work from home. A new variant of SARS-CoV-2 (B1.1.7) had been identified and the average number of weekly new cases of COVID-19 in Ireland was 3,919 [35]. The study investigated computer use, computer-related workstations and computer-related MSS among university staff working remotely or in the university environment during the COVID-19 pandemic. The prevalence of computer-related musculoskeletal symptoms was high, and was associated with female gender, right handedness, working at home and working on a laptop.
The majority (67.7%) of respondents were female and 90.2% were right-handed. The representation by gender is similar to the proportions reported elsewhere (69.8%) [13] and (60%) [22], and the findings for handedness are comparable to those widely reported in the literature [36].
Almost two-thirds of respondents (63.5%) worked entirely at home, and 34% worked partly in both locations. A similar pattern of work location for employees in Ireland during the COVID-19 pandemic (68% worked remotely, and 24% worked using a hybrid model) was reported [19]. Similar to Gerding et al. [22], who also conducted their study during the COVID-19 pandemic, the current study reported that laptops were more likely to be used than desktop computers at home. This is not surprising bearing in mind that employees had little warning of the need to work from home and it was more straightforward to work on a laptop at such short notice. Of concern is that respondents working at home reported longer use of laptops and desktops per day, and at any one time, than when working in the university workplace. This finding is similar to previous studies that reported longer working and online hours respectively during COVID-19 [19, 37]. This may be a transient finding linked to the pandemic, as the respondents were working in a novel and unprecedented situation. It may have taken longer to complete work online or there may have been more work required during the COVID-19 pandemic. Working from home and working online are likely to be key aspects of employment in the future, and the impact of this transition on the work-life balance and physical and mental wellbeing of employees needs to be addressed. The current study did not find an association between duration of computer use and MSS, however many studies have indicated that increased duration of computer use has been shown to be associated with higher prevalence of MSS [12, 38].
The 3-month prevalence of musculoskeletal symptoms in this study (83%) was similar to other studies of the 12-month prevalence, for example James et al. [13] and Stanam et al. [11] who reported prevalence of 79% and 94% respectively. All of these studies used a modified version of the Nordic Musculoskeletal Questionnaire, but the current study added ‘pins and needles’ to the list of symptoms, and this may account for the comparable prevalence within the shorter time frame. The most common sites of symptoms in the current study were neck (62%), shoulder (57%) and lower back (47%). James et al. [13] reported the same pattern of prevalence of discomfort and these were the main body areas of discomfort reported by university workers [11, 12]. The findings were also consistent with two other studies conducted during COVID-19 that reported the same pattern of prevalence of discomfort [22] and reported discomfort in the same body areas [14].
The prevalence of MSS was significantly associated with female gender. Reports that MSS was higher in females than males have also been made among university populations using computers [12] or tablets [39] and among the general working population [40]. Explanations for gender differences have not been found, but it has been suggested that toleration of levels of fatigue and perception of pain may be different in males in females. Females have also been shown to have higher muscle activity than males when completing the same tasks [41], a factor that could contribute to fatigue and discomfort. Few studies have explored the association between handedness and computer-related MSS. In this study, a significantly greater proportion of right-handed staff reported MSS than those who are left-handed. Right-handedness has been identified as a risk factor for MSS among computer users [2], and for neck and shoulder disorders in university personnel [42].
The current study investigated if the type of computer was associated with MSS. The prevalence of laptop-related MSS was significantly higher for the neck, shoulder, and lower back than desktop-related MSS. Using a laptop can result in poorer posture, and in particular, increased neck flexion [43] which when sustained, has been identified as a risk factor for neck pain [44]. Laptops were used more frequently by those working from home and considering that respondents generally reported a lack of computer equipment at home the poorly designed environment at home may also have contributed to the higher prevalence of MSS. Analysis of video recordings of computer workers identified that the absence of chair features (adjustable height and armrest) was significantly associated with the reporting of MSS [45]. The current study also found that the absence of a dedicated home workspace, an office chair, desk or monitor at home were significantly associated with MSS. Given that remote working is likely to continue for some time for many employees and indefinitely for others, the need for safe and ergonomically compliant home workstations is evident [46]. Policies around remote working/work from home and hybrid working should specifically address workstation set up and equipment provision. Such policies will also have to include pathways for reporting and addressing work-related MSS.
With regard to the impact of MSS, a previous study stated that the ‘majority’ of those who have musculoskeletal discomfort sought medical treatment [13], however only 24% of those who had MSD in the current study sought medical attention. Australian health care is subsidised [13] and therefore more likely to be used compared to university staff in Ireland. Additionally, the influence of COVID-19 on seeking healthcare should be considered, as only those with serious medical complaints may have been likely to seek medical treatment during the pandemic, irrespective of any existing health care subventions.
4.1Limitations
The study design was an online questionnaire survey, and it has been suggested that response bias in online surveys is greater than in paper surveys [47] which is a possible limitation of this study. However, considering the objectives of the study and the timing of the survey, it would not have been possible to conduct a paper survey. The response rate for the study was 16.8%, which although low, is higher than that of two recent similar studies of university employees [13, 22], who reported response rates of 13% and 8.1% respectively. As with all surveys on self-reported musculoskeletal symptoms there is always the risk of selection bias that may affect the observed findings. The limitation of self-reports of computer use [48] is also acknowledged.
5Conclusions
This research was conducted in a unique period under unique circumstances, and this may have influenced the findings. The prevalence of computer-related MSS was high and most frequently reported in the neck, shoulder, and lower back. Computer-related MSS was associated with using a laptop, female gender, right handedness, workspace, and equipment at home. However, future work practices are likely to be influenced by the current pandemic as hybrid models of working are proposed for the future. The policies, regulations and standards around remote workstations and hybrid work practices will have to be addressed. Further research regarding computer-related musculoskeletal symptoms and remote working is warranted.
Ethical approval
Ethics approval was granted by the School of Medicine Research Ethics Committee of the university (Approval no. 20210105).
Informed consent
Informed consent was assumed on completion and submission of the questionnaire.
Conflict of interest
The authors declare that they have no conflict of interest.
Acknowledgments
The authors would like to acknowledge the staff who participated in the study, and those who assisted with the distribution of the survey.
Funding
The authors report no funding.
References
[1] | Waersted M , Hanvold TN , Veiersted KB . Computer work and musculoskeletal disorders of the neck and upper extremity: a systematic review. BMC Musculoskeletal Disorders. (2010) ;11: :79. https://doi.org/10.1186/1471-2474-11-79 |
[2] | Oha K , Animägi L , Pääsuke M , Coggon D , Merisalu E . Individual and work-related risk factors for musculoskeletal pain: A cross-sectional study among Estonian computer users. BMC Musculoskeletal Disorders. (2014) 15: (1). |
[3] | Nunes A , Espanha M , Teles J , Petersen K , Arendt-Nielsen L , Carnide F . Neck pain prevalence and associated occupational factors in Portuguese office workers. International Journal of Industrial Ergonomics. (2021) ;85. https://doi.org/10.1016/j.ergon.2021.103172 |
[4] | Feng B , Chen K , Zhu X , Ip WY , Andersen LL , Page P , et al. Prevalence and risk factors of self- reported wrist and hand symptoms and clinically confirmed carpal tunnel syndrome among office workers in China: a cross-sectional study. BMC Public Health. (2021) ;21: (1):57. https://doi.org/10.1186/s12889-020-10137-1 |
[5] | Wahlstrom J . Ergonomics, musculoskeletal disorders and computer work. Occupational Medicine (Lond). (2005) ;55: (3):168–76. |
[6] | Madeleine P , Vangsgaard S , Hviid Andersen J , Ge HY , Arendt-Nielsen L . Computer work and self-reported variables on anthropometrics, computer usage, work ability, productivity, pain, and physical activity. BMC Musculoskeletal Disorders. (2013) ;14. http://www.biomedcentral.com/1471-2474/14/226 |
[7] | Shuval K , Donchin M . Prevalence of upper extremity musculoskeletal symptoms and ergonomic risk factors at a Hi-Tech company in Israel. International Journal of Industrial Ergonomics. (2005) ;35: , 569–81. |
[8] | Malińska M , Bugajska J , Bartuzi P . Occupational and non-occupational risk factors for neck and lower back pain among computer workers: a cross-sectional study. International Journal of Occupational Safety and Ergonomics (JOSE). (2021) ;27: (4):1108–15. |
[9] | Eltayeb S , Staal JB , Hassan A , de Bie RA . Work related risk factors for neck, shoulder and arms complaints: a cohort study among Dutch computer office workers. The Journal of Occupational Rehabilitation. (2009) ;19: (4):315–22. |
[10] | Ye S , Jing Q , Wei C , Lu J . Risk factors of non-specific neck pain and low back pain in computer-using office workers in China: a cross-sectional study. BMJ Open. (2017) ;7: (4):e014914. |
[11] | Stanam A , Golla V , Vasa S , Taylor R . Exposure to Computer Work and Prevalence of Musculoskeletal Symptoms Among University Employees: A Cross-Sectional Study. Journal of Environmental Health. (2019) ;81: (7):14–9. |
[12] | Collins J , O’Sullivan L . Musculoskeletal disorder prevalence and psychosocial risk exposures by age and gender in a cohort of office based employees in two academic institutions. International Journal of Industrial Ergonomics. (2015) ;45: , 85–97. |
[13] | James C , James D , Nie V , Schumacher T , Guest M , Tessier J , et al. Musculoskeletal discomfort and use of computers in the university environment. Applied Ergonomics. (2018) ;69: , 128–35. |
[14] | Algarni FS , Kachanathu SJ , AlAbdulwahab SS . A Cross-Sectional Study on the Association of Patterns and Physical Risk Factors with Musculoskeletal Disorders among Academicians in Saudi Arabia. Biomed Research International. (2020) ;2020: :8930968. https://doi.org/10.1155/2020/8930968 |
[15] | Kennelly B , O’Callaghan M , Coughlan D , Cullinan J , Doherty E , Glynn L , et al. The COVID-19 pandemic in Ireland: An overview of the health service and economic policy response. Health Policy and Technology. (2020) ;9: (4):419–29. |
[16] | Health Protection Surveillance Centre. Epidemiology of COVID-19 in Ireland 2020. [Available from: https://www.hpsc.ie/az/respiratory/coronavirus/novelcoronavirus/casesinireland/archive/dailyepidemiologyofcovid-19inirelandreports2020/march2020/COVID-19%20Epidemiology%20report%20for%20NPHET%2027.03.2020%20v2-%20website%20version.pdf] |
[17] | Crawford JO , MacCalman L , Jackson CA . The health and well-being of remote and mobile workers. Occupational Medicine (Lond). (2011) ;61: (6):385–94. |
[18] | Di Carvalho Melo L , Bastos Silveira B , Dos Santos JA , de Cena JA , Dame-Teixeira N , Martins MD , et al. Dental Education Profile in COVID-19 Pandemic: A Scoping Review. European Journal of Dental Education : Official Journal of the Association for Dental Education in Europe. (2022) ;00: :1–10. DOI: 10.1111/eje.12798. |
[19] | McCarthy A , Bohle Carbonell K , Ó Síocháin T , Frost D . Remote working during COVID-19: Ireland’s national survey: Phase II report. (2020) . |
[20] | Buckle PW , Devereux JJ . The nature of work-related neck and upper limb musculoskeletal disorders. Applied Ergonomics. (2002) ;33: (3):207–17. |
[21] | Shahwan BS , D’Emeh WM , Yacoub MI . Evaluation of computer workstations ergonomics and its relationship with reported musculoskeletal and visual symptoms among university employees in Jordan. International Journal of Occupational Medicine and Environmental Health. (2022) ;35: (2):141–56. |
[22] | Gerding T , Syck M , Daniel D , Naylor J , Kotowski SE , Gillespie GL , et al. An assessment of ergonomic issues in the home offices of university employees sent home due to the COVID- 19 pandemic. Work-a Journal of Prevention Assessment & Rehabilitation. (2021) ;68: (4):981–92. |
[23] | Jafari-Nodoushan A , Bagheri G , Nodoushan F . Effect of COVID-19 virus on Prevalence of Musculoskeletal Disorders of Facultu Members of Yazd University. Iranian Journal of Ergonomics. (2020) ;8: (3):1–12. |
[24] | Qualtrics. Utah, USA2005 [2020: Available from: https://www.qualtrics.com] |
[25] | Dockrell S , Bennett K , Culleton-Quinn E . Computer use and musculoskeletal symptoms among undergraduate university students. Computers & Education. (2015) ;85: , 102–9. |
[26] | Jacobs K , Baker NA . The association between children’s computer use and musculoskeletal discomfort. Work-a Journal of Prevention Assessment & Rehabilitation. (2002) ;18: (3):221–6. |
[27] | Katz JN , Amick BC , Carroll BB , Hollis C , Fossel AH , Coley CM . Prevalence of upper extremity musculoskeletal disorders in college students. American Journal of Medicine. (2000) ;109: (7):586–8. |
[28] | Schlossberg EB , Morrow S , Llosa AE , Mamary E , Dietrich P , Rempel DM . Upper extremity pain and computer use among engineering graduate students. American Journal of Industrial Medicine. (2004) ;46: (3):297–303. |
[29] | Goes RA , Lopes LR , Cossich VRA , De Miranda VAR , Coelho ON , Do Carmo Bastos R , et al. Musculoskeletal injuries in athletes from five modalities: A cross-sectional study. BMC Musculoskeletal Disorders. (2020) ;21: (1). |
[30] | Wilson IM , Doherty L , McKeown L . Perceptions of Playing-Related Musculoskeletal Disorders (PRMDs) in Irish traditional musicians: a focus group study. Work-a Journal of Prevention Assessment & Rehabilitation. (2014) ;49: (4):679–88. |
[31] | Gómez-Rodríguez R , Díaz-Pulido B , Gutiérrez-Ortega C , Sánchez-Sánchez B , Torres-Lacomba M . Prevalence, disability and associated factors of playing-related musculoskeletal pain among musicians: A population-based cross-sectional descriptive study. International Journal of Environmental Research and Public Health. (2020) ;17: (11. |
[32] | Kourinka IJ,B , Kilbom A , Vinterberg H , Biering-Sorenson F , Andersson G , Jorgensen K . Standardised Nordic Questionnaire for the analysis of musculoskeletal symptoms. Applied Ergonomics. (1987) ;18: (3):5. |
[33] | US Department of Labor. Occupational Safety and Health Administration. Determinants of work-relatedness 2021. [Available from: https://www.osha.gov/laws-regs/regulations/standardnumber/1904/1904.5] |
[34] | Dockrell S , Culleton-Quinn E . Staying well at your computer: computer use and computer- related musculoskeletal symptoms in university staff during COVID-19. (2022) . [Available from: doi.org/10.25546/98021] |
[35] | Health Protection Surveillance Centre. Epidemiology of COVID-19 in Ireland weekly reports- 2021 2021. [Available from: https://www.hpsc.ie/a-z/respiratory/coronavirus/novelcoronavirus/surveillance/epidemiologyofcovid-19inirelandweeklyreports/2021/.] |
[36] | Peters M , Reimers S , Manning JT . Hand preference for writing and associations with selected demographic and behavioral variables in 255,100 subjects: the BBC internet study. Brain and Cognition. (2006) ;62: (2):177–89. |
[37] | Kayabinar E , Kayabinar B , Onal B , Zengin HY , Kose N . The musculoskeletal problems and psychosocial status of teachers giving online education during the COVID-19 pandemic and preventive telerehabilitation for musculoskeletal problems. Work-a Journal of Prevention Assessment & Rehabilitation. (2021) ;68: (1):33–43. |
[38] | Coenen P , Van Der Molen HF , Burdorf A , Huysmans MA , Straker L , Frings-Dresen MHW , et al. Associations of screen work with neck and upper extremity symptoms: A systematic review with meta-analysis. Occupational and Environmental Medicine. (2019) ;76: (7):502–9. |
[39] | Lee SP , Hsu YT , Bair B , Toberman M , Chien LC . Gender and posture are significant risk factors to musculoskeletal symptoms during touchscreen tablet computer use. Journal of Physical Therapy Science. (2018) ;30: (6):855–61. |
[40] | de Zwart BC , Frings-Dresen MH , Kilbom A . Gender differences in upper extremity musculoskeletal complaints in the working population. International Archives of Occupational and Environmental Health. (2001) ;74: (1):21–30. |
[41] | Nordander C , Ohlsson K , Balogh I , Hansson GA , Axmon A , Persson R , et al. Gender differences in workers with identical repetitive industrial tasks: exposure and musculoskeletal disorders. International Archives of Occupational and Environmental Health. (2008) ;81: (8):939–47. |
[42] | Madadizadeh F , Vali L , Rafiei S , Akbarnejad Z . Risk factors associated with musculoskeletal disorders of the neck and shoulder in the personnel of Kerman University of Medical Sciences. Electronic Physician Journal. (2017) ;9: (5):4341–8. |
[43] | Yu Z , James C , Edwards S , Snodgrass SJ . Differences in posture kinematics between using a tablet, a laptop, and a desktop computer in sitting and in standing. Work-a Journal of Prevention Assessment & Rehabilitation. (2018) ;61: (2):257–66. |
[44] | Cagnie B , Danneels L , Van Tiggelen D , De Loose V , Cambier D . Individual and work related risk factors for neck pain among office workers: a cross sectional study. European Spine Journal. (2007) ;16: (5):679–86. |
[45] | Rodrigues MS , Leite RDV , Lelis CM , Chaves TC . Differences in ergonomic and workstation factors between computer office workers with and without reported musculoskeletal pain. Work-a Journal of Prevention Assessment & Rehabilitation. (2017) ;57: (4):563–72. |
[46] | Davis KKS , Daniel D , Gerding T , Naylor J , Syck M . The Home Office: Ergonomic Lessons from the “New Normal?”? Ergonomics in Design. (2020) ;October: :4–10. |
[47] | Sax LJ , Gilmartin SK , Bryant AN . Assessing response rates and nonresponse bias in web and paper surveys. Research in Higher Education. (2003) ;44: (4):409–32. |
[48] | S IJ , Mikkers J , Blatter BM , van der Beek AJ , van Mechelen W , Bongers PM . Test-retest reliability and concurrent validity of a web-based questionnaire measuring workstation and individual correlates of work postures during computer work. Applied Ergonomics. (2008) ;39: (6):685–96. |

