
The relationship between Turkish women’s self-efficacy for managing work-family conflict and depression, anxiety and stress during the COVID-19 pandemic: A web-based cross-sectional study
Abstract
BACKGROUND:
The COVID-19 pandemic has changed working women’s workplace and family workload. The changing workplace-family workload may cause a decrease in work-family conflict management self-efficacy. The decrease in work-family conflict management self-efficacy in women may increase their depression, anxiety, and stress levels.
OBJECTIVE:
This study aimed to examine the relationship between Turkish women’s self-efficacy for managing work-family conflict and their depression, anxiety, and stress during the COVID-19 pandemic.
METHOD:
This cross-sectional study was conducted with 244 Turkish women via social media (Facebook, Instagram, and WhatsApp). The data were collected online through a questionnaire, the Depression Anxiety Stress Scale-21 (DASS-21), and sub-scales of the Self-Efficacy for Managing Work-Family Conflict Scale (SE-WFC): Work-to-Family Conflict (WFC) and Family-to-Work Conflict (FWC).
RESULTS:
During the COVID-19 pandemic, 87.3% of working women experienced an increase in their family workload (100% increase in cooking and cleaning jobs). On the other hand, workplace workload of 83% of women increased. According to DASS-21, women experienced depression (55.7%), anxiety (49.6%) and stress (63.1%). A negative correlation was found between the mean scores of WFC/FWC and the mean scores of depression, anxiety, and stress. (p < 0.001).
CONCLUSION:
During the COVID-19 pandemic, Turkish women’s self-efficacy for managing work-family and family-work conflict decreased, and their depression, anxiety, and stress levels increased.
1Introduction
The World Health Organization (WHO) declared COVID-19 a pandemic on March 11, 2020. Many countries took strict measures to control the spread of the disease, such as quarantine and increasing the length of stay at home [1, 2]. Although these measures were beneficial for infection control [3], they caused many negative social consequences such as psychological stress [4–6], unemployment [7], age discrimination [8], reductions in female employment, and increased rates of violence against women and children [9–12].
To reduce the spread of the virus during the COVID-19 pandemic, instruction was carried out online. On the other hand, many professions offered flexible working hours [13]. Therefore, women spend much time with their children, and there were changes in the workload of working and non-working women [14]. Fatigue and stress emerged in women who were torn between family and work [15, 16]. COVID-19 increased not only depression, anxiety, and stress levels of working women but also their workplace and family workload [17]. The COVID-19 pandemic, which started in China, caused serious psychological problems as well (i.e., depression, anxiety, and stress) [18, 19]. It was suggested that mental health issues such as depression, anxiety and stress should be considered during the pandemic [20, 21]. WHO issued guidelines in the public interest to address the psychological issues that might arise during the COVID-19 pandemic [22].
One of the reasons for the increase in depression, anxiety and stress during the COVID-19 pandemic is work and family conflict management self-efficacy. Self-efficacy refers to confidence in the ability to control one’s own behaviour and environment. An individual may feel depressed when their self-efficacy level is low. On the other hand, those with high self-efficacy tend to strive to change their lives [23]. Work-family balance means that women have equal work and family responsibilities. To avoid role conflicts between work and family, working women are expected to have a high level of work-family balance [23, 24]. When women’s work and family roles do not conflict, there are no family problems, and their job performance is better. Work-related stress does not occur, and work-family balance is achieved. However, if their work and family roles conflict, there becomes a decrease in work-family conflict management self-efficacy and an increase in stress [25].
Previous research has recommended to increase work-family conflict self-efficacy and reduce the level of depression, anxiety and stress. In order to prevent work-family conflicts, increase self-efficacy and establish the balance between them, regular and scheduled work time, providing title or salary changes at regular intervals during the working time, not including work for the family, doing joint activities with the family, and protective social support systems for the family are recommended. It is stated that working women can be beneficial physically and mentally [19, 24, 25].
Women’s changing work-family balance may cause a decrease in work-family conflict management self-efficacy. Depression, anxiety and stress levels may increase with the decrease of work-family conflict management self-efficacy in women. There is no research on this issue in the literature. Thus, this study aimed to examine the relationship between Turkish women’s self-efficacy for managing work-family conflict and their depression, anxiety and stress during the COVID-19 pandemic.
2Materials and methods
This cross-sectional study was conducted through a web-based online survey between January and June 2021, when the quarantine process continued in Turkey. It was calculated that 244 women were needed in order to analyse the possible low correlation (r = 0.25) between women’s changing work-family conflict management self-efficacy and their depression, anxiety, and stress levels with 5% margin of error and 99% power value using the G*Power software package (version 3.1.9.4). The sample was limitedly representative of the national population. Participants were volunteer, literate, single or married women, who were above 18 years old, using social media (Facebook, Instagram, and WhatsApp), and working in a job.
2.1Data collection tools and data collection
Data collection tools were a questionnaire, the Self-Efficacy for Managing Work-Family Conflict Scale, and Depression Anxiety Stress Scale-21 (DASS-21). After obtaining the necessary permissions for the study, an online survey was created using the Google Forms web application. An electronic online survey was administered to the participants via social media (Facebook, Instagram, and WhatsApp). They were informed about the research on the first page of the online questionnaire. Electronic informed consent was obtained on the first page of the online questionnaire. Besides, they were informed that participation in the online survey was voluntary and that they could withdraw at any time. The online questionnaire consisted of a total of 13 questions (9 questions about the demographic characteristics and 4 questions including features related to work-family workload during the COVID-19 pandemic) [16, 20, 25].
2.1.1Self-Efficacy for Managing Work-Family Conflict Scale (SE-WFC)
The original form of the scale was in Hebrew, and it was adapted into English by Hennessy. The English version involved 8 items and two sub-scales [26, 27]. The sub-scales were Work-to-Family Conflict (WFC) and Family-to-Work Conflict (FWC). WFC reflects the scores of self-efficacy for managing conflicts in situations where work-related difficulties make family life difficult, and FWC represents the scores of self-efficacy for managing conflict, which arises as a result of the reflection of family-related difficulties on work. Since the WFC sub-dimension consists of 5 items and the FWC sub-dimension consists of 3 items, a difference is observed between the mean scores of the sub-dimensions. While the lowest score that can be obtained from the WFC sub-dimension is 0, and the highest score is 45, the lowest score that can be obtained from the FWC sub-dimension is 0, and the highest score is 27. The high scores of WFC and FWC indicate high self-efficacy. The internal consistency coefficients of the original form of the scale were 0.83 for WFC and 0.84 for FWC [28]. In the present study, the internal consistency coefficients of the scale were calculated as 0.98 for WFC and 0.97 for FWC.
2.1.2Depression Anxiety Stress Scale-21 (DASS-21)
Developed by Lovibond and Lovibond, DASS-21 was a short version of DAS-42 [29, 30]. The psychometric properties of the Turkish version of the DASS-21 scale in a “normal and clinical” sample were determined by Sarıçam [31]. The 4-point Likert-type scale measures “depression, anxiety, and stress” and consists of seven questions for each dimension. Getting 5 points or more for depression, 4 points or more for anxiety, and 8 points or more for stress indicates that the individual has a related problem. In the analysis of the study data, participants who scored 5 points or more for depression, 4 points or more for anxiety, and 8 points or more for stress were included in the ‘yes’ group, while those below the specified scores were included in the ‘no’ group. In the study, the internal consistency coefficient was 0.96 for depression, 0.92 for anxiety, and 0.95 for stress. The internal consistency coefficient of the scale was found to be 0.97.
2.2Data analysis
The data were analysed with the SPSS (Statistical Package for Social Sciences) 23.0 program. Descriptive statistical methods, such as frequency, percentage, mean, and standard deviation (SD), were used to analyse the data. Quantitative results of the study were given as mean±standard deviation, and categorical results were presented as numbers (n) and percentages (%). The Shapiro-Wilk test was used for the normal distribution of the data. Spearman’s correlation analysis was used to examine the relationship between scale scores, taking into account distribution characteristics. The statistical significance level was considered as p < 0.05.
2.3Ethical considerations
Ethical approval was obtained from the Trakya University Scientific Research Ethics Committee (Ethics Committee Number: 2021/11).
3Results
The mean age of the women was 40.0±11.6 (min:20 – max:71), 66.8% of them graduated from high school or higher education, and 77.5% were married. Besides, 79.1% of the women participants had children. The average number of children was 2.5±1.7 (min:1 – max:10) and 82.4% of the children are students. Most of them had a nuclear family (88.9%) with equal income and expenditure (70.1%) (Table 1).
Table 1
Demographic characteristics of the women (n = 244)
| Variables |
| |
| Age (year) | 40.0±11.6 | |
| (min:20 – max:71) | ||
| Number of children | 2.5±1.7 | |
| (min:1 – max:10) | ||
| n | % | |
| Marital status | ||
| Married | 189 | 77.5 |
| Single | 55 | 22.5 |
| Has children | ||
| Yes | 193 | 79.1 |
| No | 51 | 20.9 |
| Student status of children | ||
| Yes | 159 | 82.4 |
| No | 34 | 17.6 |
| Education level | ||
| Secondary education and lower | 81 | 33.2 |
| High school and higher | 163 | 66.8 |
| Income status | ||
| Income less than expenditure | 46 | 18.9 |
| Equal income and expenditure | 171 | 70.1 |
| Income more than expenditure | 27 | 11.1 |
| Family type | ||
| Nuclear family | 217 | 88.9 |
| Extended family | 27 | 11.1 |
Note:
During the COVID-19 pandemic, 87.3% experienced an increase in family workload (100% increase in cooking and cleaning jobs). 59% of spouses (n = 188) helped their family workload. 83% stated that their workload increased (Table 2).
Table 2
Characteristics of women regarding family and workload during the COVID-19 pandemic (n = 244)
| Variables | n | % |
| Increase in family workload during the COVID-19 pandemic | ||
| Yes | 213 | 87.3 |
| No | 31 | 12.7 |
| Family workload increase rates during the COVID-19 pandemic | ||
| (n = 244)* | ||
| Cooking | 213 | 100.0 |
| Cleaning | 213 | 100.0 |
| Childcare | 175 | 82.2 |
| Relationship with spouse | 170 | 79.8 |
| Spouse assistance to family workload during the COVID-19 | ||
| pandemic (n = 188) | ||
| Yes | 111 | 59.0 |
| No | 78 | 41.0 |
| Increase in the workload of employees during the COVID-19 | ||
| pandemic | ||
| Yes | 203 | 83.0 |
| No | 41 | 17.0 |
Note: * More than one option has been ticked.
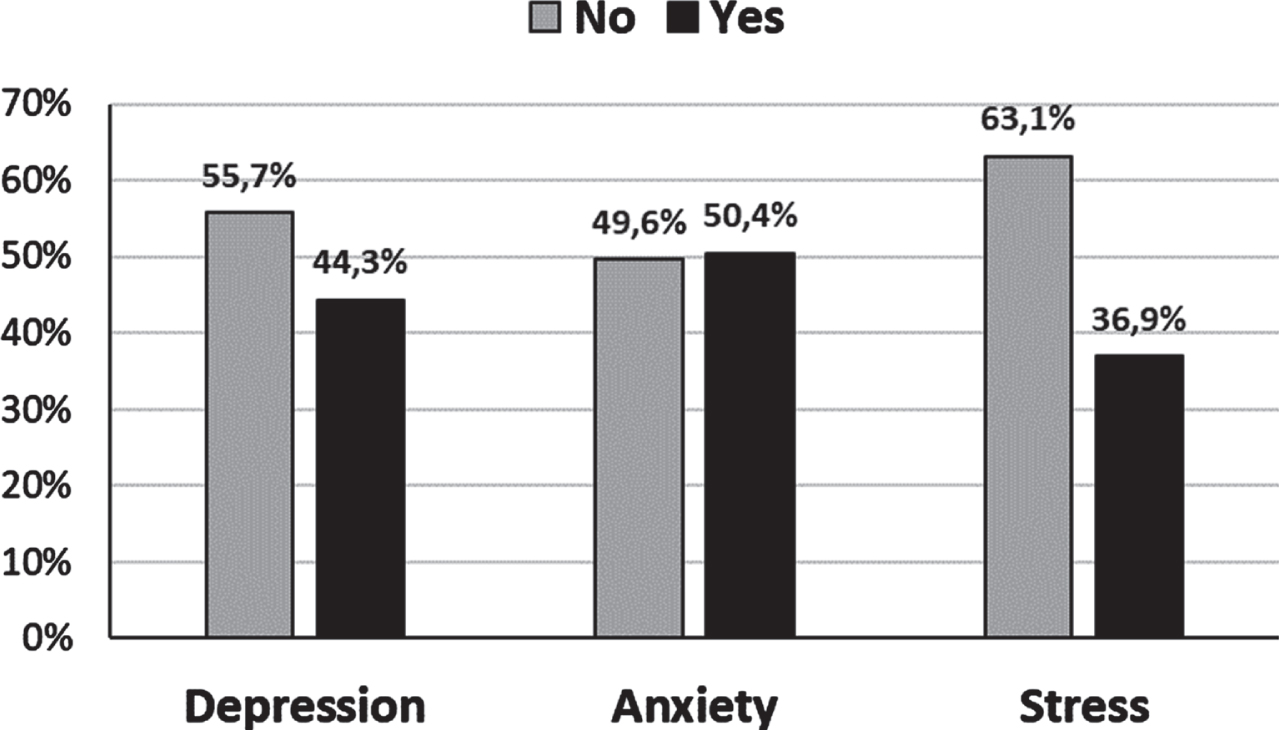
Figure 1 presents the prevalence of depression, anxiety and stress in women. According to DASS-21, women had depression (55.7%, n = 108), anxiety (49.6%, n = 123) and stress (63.1%, n = 90) during COVID-19 pandemic.
Fig. 1
The prevalence of women with depression, anxiety and stress according to DAS-21 during the COVID-19 pandemic.
While the mean score of WFC for women with depression was 25.2±14.4, the mean score of FCW was 15.1±9.1. The mean score of WFC for women without depression was 32.4±14.9, but the mean score of FWC for women without depression was 19.4±8.6. Regarding anxiety, the mean score of WFC was 25.7±14.5, the mean score of FWC was 15.2±8.8. On the other hand, the mean score of WFC for women without anxiety was 32.7±14.9, and the mean score of FWC for women without anxiety was 19.8±8.9. For stress, the mean score of WFC was 25.1±15.1, and the mean score of FWC was 14.9±9.3. The mean score of WFC for women without stress was 31.6±14.6, the mean score of FWC for women without stress was 19±8.6 (Table 3).
Table 3
The mean scores of WFC and WFC of women with depression, anxiety and stress according to DAS-21 during the COVID-19 pandemic (n = 244)
| DAS-21 | No; Yes | SE-WFC | SE-FWC |
| Depression | No (n = 136) | 32.4±14.9 | 19.4±8.6 |
| Yes (n = 108) | 25.2±14.4 | 15.1±9.1 | |
| Anxiety | No (n = 121) | 32.7±14.9 | 19.8±8.9 |
| Yes (n = 123) | 25.7±14.5 | 15.2±8.8 | |
| Stress | No (n = 154) | 31.6±14.6 | 19±8.6 |
| Yes (n = 90) | 25.1±15.1 | 14.9±9.3 |
Note: Abbreviations: DAS-21 = Depression Anxiety Stress Scale-21, SE-WFC = Self-Efficacy for Managing Work-Family Conflict Scale, SE-FWC = Self-Efficacy for Managing Family-Work Conflict Scale.
DASS-21 showed a significant negative correlation between the mean score of sub-scales (depression, anxiety, and stress) and the mean score of WFC and FWC. During the COVID-19 pandemic, as the self-efficacy level of managing work-family and family-work conflict in women decreased, the level of depression, anxiety and stress increased.
Women with depression, anxiety and stress had lower mean scores of WFC and FWC. On the other hand, women without depression, anxiety and stress had higher mean scores of WFC and FWC (p < 0.001) (Table 4).
Table 4
The relationships between the mean scores of women with depression, anxiety and stress according to DAS-21 and the mean scores of WFC and WFC during the COVID-19 pandemic (n = 244)
| DAS-21 | No; Yes | WFC | FWC |
| Depression | r | –0.282 | –0.292 |
| p | <0.001 | <0.001 | |
| Anxiety | r | –0.240 | –0.265 |
| p | <0.001 | <0.001 | |
| Stress | r | –0.239 | –0.253 |
| p | <0.001 | <0.001 |
Note: r, correlation coefficient. Abbreviations: DAS-21 = Depression Anxiety Stress Scale-21, WFC = Self-Efficacy for Managing Work-Family Conflict Scale, FWC = Self-Efficacy for Managing Family-Work Conflict Scale.
4Discussion
During the COVID-19 pandemic, the changing work-family balance may decrease women’s work-family conflict management self-efficacy and increase their depression, anxiety and stress levels. This study aimed to examine the relationship between Turkish women’s self-efficacy for managing work-family conflict and their depression, anxiety as well as stress during the COVID-19 pandemic.
The most important finding of the study was that as women’s self-efficacy in managing work-family and family-work conflict decreased, their depression, anxiety and stress levels increased. This is the only research finding on women working during the COVID-19 pandemic. The literature has shown that participants have different characteristics. River et al. found that when the self-efficacy for managing work-family conflict and family-work conflict in working parents decreased, the level of anxiety increased [32]. Zhang et al. stated that the level of anxiety of female health personnel increased when their self-efficacy for managing work-family conflict and family-work conflict decreased [33]. According to Laster-Loftus, female faculty members’ self-efficacy in managing work-family conflict and family-work conflict decreased as their stress levels increased [34]. Various studies reported that depression, anxiety, and stress levels increased when self-efficacy in managing work-family conflict and family-work conflict decreased [35–37]. The finding of this study confirms the literature. As women’s self-efficacy in managing work-family and family-work conflict decreases, depression, anxiety and stress levels increase. Work and family conflict management inadequacy occurs when depression, anxiety, or stress, which is experienced as a result of being stuck between work and family life, hinders the ability to perform [38]. Besides, Turkish women with depression, anxiety and stress were found to have lower work-family and family-work conflict management self-efficacy. This finding contributes to the literature. Depression, anxiety, and stress reduce working women’s self-efficacy in managing work-family conflict.
During the COVID-19 pandemic, there was an increase in family workload of 87.3% of Turkish women (100% increase in cooking and cleaning jobs) and in their (83%) workplace workload. Suka et al. discovered a 19.5% increase in workplace workload for Japanese women following the onset of the COVID-19 pandemic, as well as a 35.7% increase in home workload for Japanese women [14]. For Boca et al., there was an increase in women’s workload at home and work [39]. According to Adisa et al. there was an increase in family and workplace workload of British working women during the pandemic [40]. Nahdi et al. and Ragasa et al. found that family and workplace workload of women increased during the pandemic [41, 42].
During the COVID-19 pandemic, Turkish women experienced depression (55.7%), anxiety (49.6%) and stress (63.1%). According to DASS-21, the prevalence of depression, anxiety and stress was quite high in Turkish women during the COVID-19 pandemic. During the pandemic, studies were conducted on female health workers in Turkey. In the study by Ozturk et al., 71.1% of Turkish healthcare workers experienced depression, and 35.9% had severe or very severe stress [43]. Sahin et al. found that healthcare workers had depression (77.6%) and anxiety (60.2%) during the COVID-19 pandemic in Turkey [44]. International studies using DASS-21 during the COVID-19 pandemic had various results. For example, a meta-analysis reported the prevalence of stress (48.1%), depression (26.9%), and anxiety (21.8%) in China during the COVID-19 pandemic. The prevalence of depression and anxiety in both women and frontline healthcare workers was higher than the prevalence in the general Chinese population [45]. A study conducted with 1210 Chinese participants concluded that women suffered from depression (16.1%), anxiety (28.8%), and stress (53.8%). The female gender was associated with the great psychological impact of the pandemic and high levels of stress, anxiety, and depression [46]. Shah et al. found that females (aged between 18 and 24) experienced anxiety (50.9%), stress (57.4%), and depression (58.6%) during the COVID-19 pandemic [47]. In their study, Kemal and Othman observed that the prevalence of depression, anxiety, and stress was 45%, 47%, and 18%, respectively, during the pandemic. The female gender was a significant factor in higher levels of depression [48]. In a study on women’s mental health, 57.3% of Tunisian women had extremely severe anxiety and depressive symptoms, and 53.1% had extremely distressing symptoms during COVID-19 [49]. During the COVID-19 pandemic, stress, anxiety, and depression became widespread worldwide. Multiple factors could affect the rates of these mental health problems [47]. Being female and working during the COVID-19 pandemic may be important factors in the increase in the prevalence of depression, anxiety, and stress.
4.1Limitations
The current study has some limitations. First, as the electronic online survey was administered to participants via social media (Facebook, Instagram, and WhatsApp), they were concerned about data security. Second, although the relationship between work-family conflict management self-efficacy in women and depression-anxiety-stress was revealed simultaneously with the quarantine process, long-term causal relationships could not be determined.
5Conclusion
The present study helps identify the relationship between self-efficacy in managing work-family conflicts and depression, anxiety, and stress levels of working women during the COVID-19 pandemic period in Turkey. During the COVID-19 pandemic, women’s changing work and family roles decreased their self-efficacy in managing work and family conflict, increasing the level and prevalence of depression, anxiety, and stress. Increasing workplace and family workload of working women increased depression, anxiety, and stress, revealing the inadequacy of work and family conflict management.
Based on this result, increasing mental health problems of women working during COVID-19 (due to the decrease in work-family conflict management self-efficacy) indicate the necessity of taking serious psychological intervention measures and developing support systems.
Ethical approval
Ethics committee approval was obtained from the Committee for Evaluation of Scientific Research of the Faculty of Medicine at Trakya University (TUTF-BAEK 2021/11).
Informed consent
After the participants who agreed to participate in the study were informed about the research, electronic informed consent was obtained on the first page of the online questionnaire.
Acknowledgments
The authors are grateful to all individuals who participated in the study.
Author contributions
Study design: BK and HKS; Manuscript writing: BK and HKS; Data collection: BK and HKS; Data analysis: BK and HKS; Study supervision: HKS; Critical revisions for important intellectual content: BK and HKS.
Funding
No financial support was received from institutions or organizations.
Conflict of interest
The authors have no conflicts of interest to report.
References
[1] | Xue J , Chen J , Chen C , Hu R , Zhu T . The Hidden Pandemic of Family Violence During COVID-19: Unsupervised Learning of Tweets. J Med Int Res. (2020) ;22: (11):e24361. |
[2] | Sadeghi H , Jehu DA . Exergaming to improve physical, psychological and cognitive health among home office workers: A COVID-19 pandemic commentary. Work. (2022) ;71: (1):13–17. |
[3] | Boxall H , Morgan A , Brown R . The prevalence of domestic violence among women during the COVID-19 pandemic. Australasian Polic. (2020) ;12: (3):38. |
[4] | Gelder N , Peterman A , Potts A , O’Donnell M , Thompson K , Shah N , Gender COVID-19 working group. COVID-19: Reducing the risk of infection might increase the risk of intimate partner violence. EClinical Med. (2020) ;11: :100348. |
[5] | Galea S , Merchant RM , Lurie N . The Mental Health Consequences of COVID-19 and Physical Distancing: The Need for Prevention and Early Intervention. JAMA Intern Med. (2020) ;180: (6):817–818. doi:10.1001/jamainternmed.2020.1562. |
[6] | Li S , Wang Y , Xue J , Zhao N , Zhu T . The Impact of COVID-19 Epidemic Declaration on Psychological Consequences: A Study on Active Weibo Users. Int J Environ Res Public Health. (2032) ;17: (6)–10.3390/ijerph17062032. |
[7] | Su Y , Xue J , Liu X , Wu P , Chen J , Chen C , et al. Examining the Impact of COVID-19 Lockdown in Wuhan and Lombardy: A Psycholinguistic Analysis on Weibo and Twitter. Int J Environ Res Public Health. (2020) ;17: (12). |
[8] | Roje Đapić M , Buljan Flander G , Prijatelj K . Children Behind Closed Doors Due to COVID-19 Isolation: Abuse, Neglect and Domestic Violence. Arch Psychiatry Res. (2020) ;56: (2):181–192. |
[9] | Xiang X , Lu X , Halavanau A , Xue J , Sun Y , Lai P , et al. Modern Senicide in the Face of a Pandemic: An Examination of Public Discourse and Sentiment about Older Adults and COVID-19 Using Machine Learning. J Gerontol B Psychol Sci Soc Sci. (2020) ;12:A: . |
[10] | Bradbury-Jones C , Isham L . The pandemic paradox: The consequences of COVID-19 on domestic violence. J Clin Nurs. (2020) ;29: (13-14):2047–49. doi: 10.1111/jocn.15296. |
[11] | Campbell AM . An increasing risk of family violence during the COVID-19 pandemic: Strengthening community collaborations to save lives. Forens Sci Int Reports. (2020) ;2: :100089. doi: 10.1016/j.fsir.2020.100089. |
[12] | Peterman A , Potts A , O’Donnell M , Thompson K , Shah N , Oertelt-Prigione S , et al. Pandemics and violence against women and children. Center for Global Development. (2020) Apr 1. URL: https://www.cgdev.org/publication/pandemics-and-violence-against-women-and-children [accessed 2022-02-24] |
[13] | Abdullah ZD . The perspective of university academics on remote teaching during COVID-19 pandemic. Malikussaleh J Math Learn (MJML). (2021) ;4: (2):62–9. |
[14] | Suka M , Yamauchi T , Yanagisawa H . Changes in health status, workload, and lifestyle after starting the COVID-19 pandemic: a web-based survey of Japanese men and women. Environm Health Prevent Med. (2021) ;26: (1):1–11. |
[15] | Brown SM , Doom JR , Lechuga-Peña S , Watamura SE , Koppels T . Stress and parenting during the global COVID-19 pandemic. Child Abuse & Neglect. (2020) :104699. |
[16] | Pope J , Olander EK , Leitao S , Meaney S , Matvienko-Sikar K . Prenatal stress, health, and health behaviours during the COVID-19 pandemic: an international survey. Women Birth. (2021) . |
[17] | Hall R , Hall R , Chapman M . The 1995 Kikwit Ebola outbreak: Lessons hospitals and physicians can apply to future viral epidemics. General Hospital Psychiatry. (2018) ;30: (5):446–452. https://doi.org/10.1016/j.genhosppsych.2008.05.003. |
[18] | Wang C , Pan R , Wan X , Tan Y , Xu L , Ho C , et al. Immediate psychological responses and associated factors during the initial stage of the 2019 Coronavirus Disease (COVID-19) epidemic among the general population in China. Int J Environm Res Public Health. (2020) ;17: (5):1729. https://doi.org/10.3390/ijerph17051729 |
[19] | Qiu J , Shen B , Zhao M , Wang Z , Xie B , Xu Y . A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. General Psychiatry. (2020) ;33: (2):e100213. https://doi.org/10.1136/gpsych-2020-100213. |
[20] | Van Bortel T , Basnayake A , Wurie F , Jambai M , Koroma A , Muana A , et al. Psychosocial effects of an Ebola outbreak at individual, community and international levels. Bulletin of the WHO. (2016) ;94: (3):210–214. https://doi.org/10.2471/blt.15.158543. |
[21] | Kumar A , Nayar KR . COVID-19 and its mental health consequences. J Mental Health. (2020) . https://doi.org/10.1080/09638237.2020.1757052. |
[22] | WHO. ((2020) ). Mental health and psychosocial considerations during the COVID-19 outbreak [Ebook]. Retrieved from https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf. |
[23] | Feist J , Feist GJ . Theories of Personality 7th ed. McGraw Hill Education. New York. (2013) . |
[24] | Dhamayanti R . Pengaruh konflik keluargapekerjaan, keterlibatan pekerjaan dan tekanan pekerjaan terhadap kepuasan kerja karyawan wanita studi pada nusantara tour & travel kantor cabang dan kantor pusat semarang. Jurnal Studi Manajemen & Organisasi. (2006) ;3: (2):93–. |
[25] | Mousavinia S , Naami A , Arshadi N , Beshlideh K . The Role of Work-Self Facilitation and Work-Family Conflict Self-Efficacy in decreasing effect of Work-Family Conflicton Family Satisfaction, Couple Relationship Quality and Parenting Quality in Nurses. Iranian J Nurs Res. (2021) ;15: (6):105–120. |
[26] | Cinamon RG , Rich Y . Profiles of attribution of importance to life roles and their implications for the work– family conflict. J Counsel Psychology. (2002) ;49: (2):212–. |
[27] | Hennessy K . Work-family conflict self-efficacy: A scale validation study. (Yayınlanmamış Yüksek Lisans Tezi). University of Maryland, Maryland. 2005–. |
[28] | Amanvermez Y , Denizli S . Iş ve aile çatışmasını yönetme öz-yeterliği ölçeği Türkçe formunun uyarlanması: Yapı geçerliği ve güvenirlik çalışması . Ege Eğitim Dergisi. (2016) ;17: (1):1–17. |
[29] | Lovibond SH , Lovibond PF . Manual for the Depression Anxiety Stress Scales, 2nd ed. Sydney, Australia: Pychology Foundation of Australia; (1995) . |
[30] | Lovibond PF , Lovibond SH . The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Therapy. (1995) ;33: :335–343. |
[31] | Saricam H . The psychometric properties of Turkish version of Depression Anxiety Stress Scale-21 (DASS-21) in health control and clinical samples. J. Cognitive Behav. Psychother. Res. (2018) ;7: (1):19–30. |
[32] | River LM , Borelli JL , Nelson-Coffey SK . Tolerance of infant distress among working parents: Examining the roles of attachment anxiety and work– family conflict. Parenting. (2019) ;19: (1-2):137–159. |
[33] | Zhang H , Tang L , Ye Z , Zou P , Shao J , Wu M , Mu S . The role of social support and emotional exhaustion in the association between work-family conflict and anxiety symptoms among female medical staff: a moderated mediation model. BMC Psychiatry. (2020) ;20: (1):1–9. |
[34] | Laster-Loftus AS . Exploring Work-Family Conflict and Self-efficacy: A Study of Female Online Faculty (Doctoral dissertation, Grand Canyon University). (2018) . |
[35] | Kayaalp A , Page KJ , Rospenda KM . Caregiver burden, work-family conflict, family-work conflict, and mental health of caregivers: A mediational longitudinal study. Work & Stress. (2021) ;35: (3):217–240. |
[36] | Sharififard F , Asayesh H , Hosseini MHM , Sepahvandi M . Motivation, self-efficacy, stress, and academic performance correlation with academic burnout among nursing students. J Nurs Midw Sci. (2020) ;7: (2):88–. |
[37] | El-Kassem RC . Antecedents and Consequences of Work-Family Conflict in Qatar. The J Soc Sci Res. (2019) ;5: (6):1010–1019. |
[38] | Michel JS , Kotrba LM , Mitchelson JK , Clark MA , Baltes BB . Antecedents of work– Family conflict: A meta-analytic review. J Organizational Behav. (2011) ;32: (5):689–725. doi:10.1002/job.695. |
[39] | Del Boca D , Oggero N , Profeta P , Rossi M . Women’s and men’s work, housework and childcare, before and during COVID-19. Rev Econom Household. (2020) ;18: (4):1001–17. |
[40] | Adisa TA , Aiyenitaju O , Adekoya OD . The work– family balance of British working women during the COVID-19 pandemic. J Work-Appl Manag. 2021–. |
[41] | Nahdi K , Taufiq M , Yunitasari D , Lutfi S , Suhartiwi S , Usuludin U , Amrulloh R . Critical discourse analysis in patriarchal society: Covid-19 and increased women workload. JPPI. (2021) ;7: (1):16–27. |
[42] | Ragasa C , Lambrecht I , Mahrt K , Aung ZW , Wang M . Immediate impacts of COVID-19 on female and male farmers in central Myanmar: Phone-based household survey evidence. Agricultural Economic. (2021) ;52: (3):505–523. |
[43] | Öztürk M , Tuncer Ertem G , Kotanoğlu MS , Erdinç Ş , Kınıklı S . COVID-19 pandemisinde görev alan sağlik çalişanlarinin algiladiklari sosyal desteğin depresyon, anksiyete ve stres düzeylerine etkisi. Ankara Eğitim ve Araştırma Hastanesi Tıp Dergisi. (2021) ;54: (1):70–77. |
[44] | Şahin MK , Aker S , Şahin G , Karabekiroğlu A . Prevalence of depression, anxiety, distress and insomnia and related factors in healthcare workers during COVID-19 pandemic in Turkey. J Community Health. (2020) ;45: (6):1168–1177. |
[45] | Bareeqa SB , Ahmed SI , Samar SS , et al. Prevalence of depression, anxiety and stress in china during COVID-19 pandemic: A systematic review with meta-analysis. Int J Psychiatry Med. (2021) ;56: (4):210–227. doi:10.1177/0091217420978005. |
[46] | Wang C , Pan R , Wan X , Tan Y , Xu L , Ho CS , et al. Immediate sychological responses and associated factors during the initial stage of the coronavirus disease (COVID-19) epidemic among the general population in China. Int J Envir Res Public Health. (2020) ;17: (5):1729–. |
[47] | Shah SMA , Mohammad D , Qureshi MFH , et al. Prevalence, Psychological Responses and Associated Correlates of Depression, Anxiety and Stress in a Global Population, During the Coronavirus Disease (COVID-19) Pandemic. Community Ment Health J. (2021) ;57: :101–110. https://doi.org/10.1007/s10597-020-00728-y. |
[48] | Kamal N , Othman N . Depression, Anxiety, and Stress in the time of COVID-19 Pandemic in Kurdistan Region. Iraq Kurdistan J Applied Res. (2020) ;5: (3):37–44. |
[49] | Sediri S , Zgueb Y , Ouanes S , et al. Women’s mental health: acute impact of COVID-19 pandemic on domestic violence. Arch Womens Ment Health. (2020) ;23: :749–756. https://doi.org/10.1007/s00737-020-01082-4. |


