
The effects of the COVID-19 pandemic on the mental health of workers and the associated social-economic aspects: A narrative review
Abstract
BACKGROUND:
The COVID-19 pandemic has struck nations worldwide, pushing worldwide health and socio-economic systems to extreme limits. Upon exposure to an exceeding number of patients and supply shortages, the resilience of healthcare resources has been broadly challenged.
OBJECTIVE:
We will firstly discuss the mental health turmoil during the COVID-19 pandemic as the primary focus of this study and delve into the mental health repercussions among the workforce. Also, we debate the risk factors, particularly highlighting the impact of social behaviors and media exposure. We examine the pandemic’s impact on occupational health services. Secondly, we thoroughly discuss the effect of socio-economic and race disparities in the COVID-19 contraction and the related psychologic sequelae. Economic outcomes are also highlighted, particularly alterations in poverty rates and occupational sectors.
METHODS:
Peer-reviewed reports were extracted through Embase, PubMed, and Google Scholar until June 2022.
RESULTS:
A constellation of untoward spillover effects of the pandemic, including dramatic changes in public and workplace environments, enduring curfew, and low wages, have put socio-economic aspects of daily life under exuberant strain. Indeed, occupational and public health stakeholders presume a coinciding social crisis to occur, provided the pandemic’s implications on socioeconomics and psychological wellbeing are not addressed well with evidence-based approaches and peer services.
CONCLUSION:
Evaluating the socio-economic and mental health impact is imperative to cope with the pandemic. Also, we should assess the predisposing and protecting factors in a broad array of life aspects associated with COVID-19.
1Introduction
The World Health Organization (WHO) announced the burgeoning coronavirus 2019 (COVID-19) infection as a pandemic in March 2020, requiring imminent actions. In April 2020, approximately half of the world’s population (3.9 billion) had to abide by the mandatory social distancing policies, including rigorous lockdowns. As of November 2021, more than 256 million confirmed cases were reported worldwide, with over 5.1 million deaths [1]. The scaling toll of COVID-19 is put into context by reviewing previous biologic disasters. For instance, data from the 2003 severe acute respiratory syndrome (SARS) outbreak unfolded 8,000 confirmed cases and 800 deaths. Compelling evidence proposes that the sizable morbidities and mortalities of COVID-19, along with the entailed economic strains, justify the necessity to appraise its repercussion on interconnected psychosocial and economic factors [2].
To fend off the disease spread, most of the world has introduced wide-ranging restrictions, encompassing a concrete curfew, physical distancing policies, the obligatory cessation of mass gathering religious and sports events, shutdown of many business sectors and academic campuses, and the extended travel restrictions [3]. Although the implemented social distancing measures ameliorated the rapidly growing load of cases, public health authorities unraveled the pandemic’s deleterious socio-economic and mental health impacts as the spillover effects.
The International Labor Organization (ILO) assessments at the beginning of the pandemic estimated a steep decline in employment between an approximate array of 5.3 million and 24.7 million, raising the global unemployment rate to 4.89% and 5.65%, respectively (Table 1). For the first time since the 1990s, extreme poverty rates ascend as data from World Bank confirms that more than 150 million people would fall down the absolute poverty limit by 2021. The unprecedented unemployment rates contribute to 2100 to 9600 suicide commitments annually [4]. The malfunctioning health and socio-economic infrastructures in low-income countries (LIC), precisely those confronting fragility, conflict, and violence (FCV) challenges, lay a foundation for their significant vulnerability to the pandemic’s attritions. Interestingly, the coronavirus pandemic has hit economic sectors to various extents. For instance, the effect is particularly clear-cut in healthcare and drug design services, which preserved increasingly onerous efforts to curb the disease. On the other page, other sectors confronted staggering obstacles, such as cessations or supply chain interruptions. An unprecedented state of upheaval challenged sectors facing compulsory adaption to smart working. A growing strand of evidence unfolded the significant downturn in liquidity and stock instability [5]. Overall, the healthcare system downturn might undermine workers’ social and economic aspects [6].
Table 1
The interaction of the strictness of pandemic’s measures and occupation alterations
| Country | Cases | Deaths | Stringency index* | Employment rate | Unemployment rate | ||
| 2019 | 2020 | 2019 | 2020 | ||||
| USA | 39.3 million | 641K | 57.87 | 71.36 | 67.07 | 3.67 | 8.09 |
| India | 32.8 million | 439K | 70.83 | 45.20 | 36.40 | 5.27 | 7.11 |
| Iran | 5 million | 108K | 59.72 | 40.13 | 37.77 | 11.14 | 10.96 |
| UK | 6.8 million | 133K | 43.98 | 76.16 | 75.43 | 3.83 | 4.55 |
| Brazil | 20.7 million | 580K | 51.39 | 57.30 | 46.80 | 11.93 | 13.67 |
| Indonesia | 4.1 million | 133K | 68.98 | 65.64 | 63.72 | 3.62 | 4.11 |
| Turkey | 6.4 million | 57K | 32.41 | 50.30 | 47.50 | 13.73 | 13.14 |
| France | 6.8 million | 114K | 66.67 | 65.58 | 65.30 | 8.43 | 8.03 |
*Government response stringency index; (0–100, 100 = strictest).
Consistently, mental health concerns have arisen due partly to the concomitant financial instabilities, lockdown policies, and the worrying picture of the future. On the same line, investigations on young adult workers in the USA and UK in the first wave of the pandemic disclosed a pronounced accrual in mental distress, as opposed to similar data on 2017-19 [7]. Recent researches estimate that 1 out of five COVID-19 patients shows neuropsychiatric symptomatology, including anxiety, sleep disturbances, posttraumatic stress disorder (PTSD), and major depressive symptoms (MDS). Despite the exponentially rising demands for unparalleled psychological health support programs, WHO emergency response updates attested that less than 10% of countries sustain running mental health services. Hence, public health policymakers draw attention to the significant risk of an impending psychological wellbeing crisis because of the dearth of mental health support services [8].
Taken together, robust responses are required to compensate for the pandemic’s reverberating social and financial effects. However, it should be borne in mind that the psychological wellbeing of the workforce is also in jeopardy, necessitating the development of pragmatic strategies by compiling a range of resources and information. Herein, this review primarily focuses on the mental health alterations in workers caused by COVID-19 in terms of psychological disturbances. Also, we underscore protective and risk factors for these mental disorders and analyze the effects of containment policies on mental wellbeing. Secondly, the impact of COVID-19 on social and economic states is discussed, explaining how COVID-19 has affected everyday life with consequential changes in mental health. Overall, with the evidence presented from epidemiological perspectives, we examine whether and how COVID-19 has impacted the mental health of the labor force in different races and socio-economic positions.
2Methods
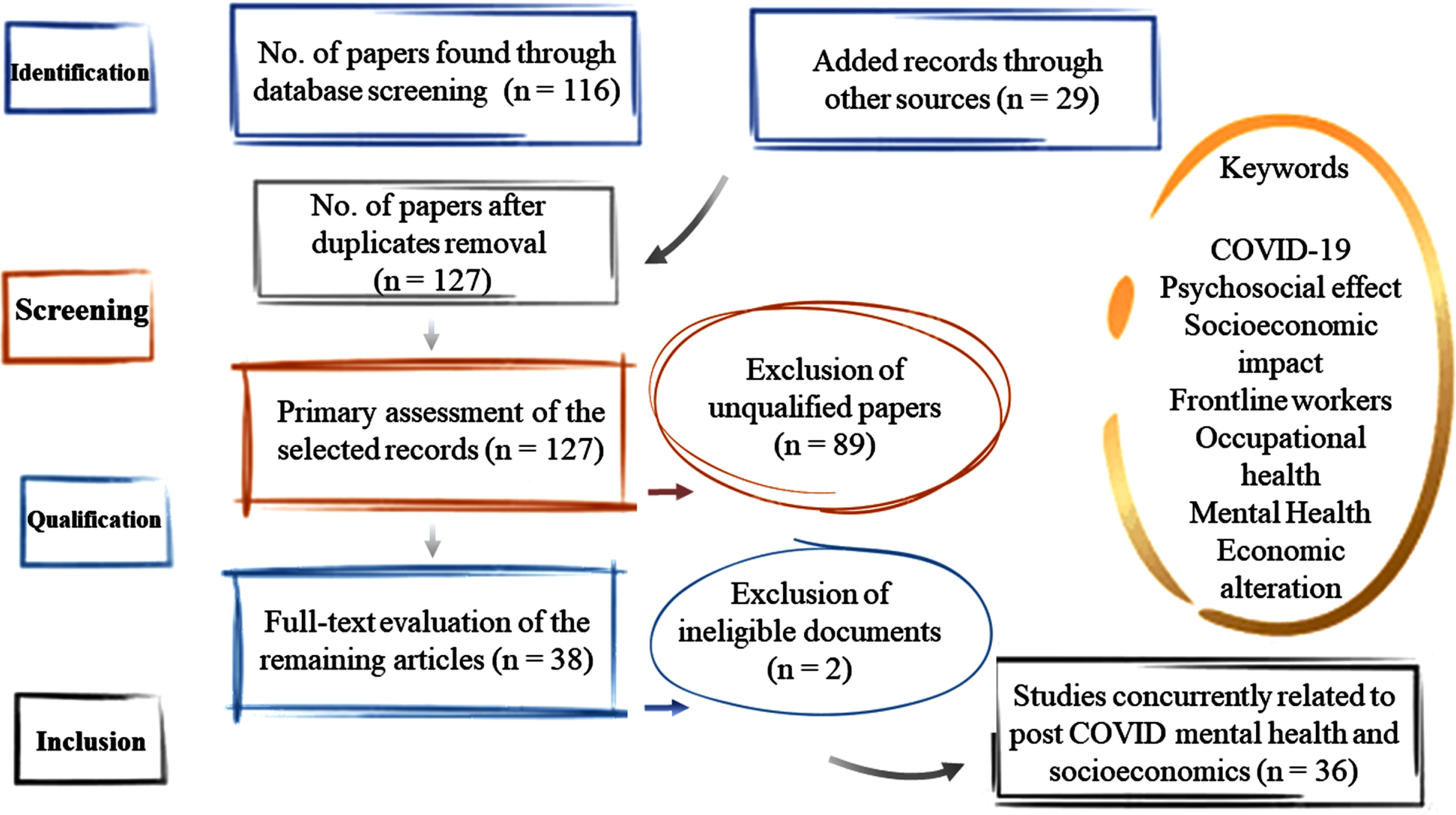
The present manuscript attempts to address the mental health and socio-economic implications of the COVID-19 pandemic on the workforce. To provide a comprehensive review of the current literature, we conducted a thorough database search, including PubMed and PsychInfo, MEDLINE, Web of Science, and Google Scholar. The search term categories included “COVID-19", mental health outcomes (e. g., “mental*", “psych*", “psychology services", “anxiety", “behave*", “depress*", “stress*"), and socioeconomics such as “social isolation", “coping", “lockdown measures", “financial strain", “economy” in different combinations up to June 2022. Figure 1 depicts the quantity of the screened papers in each level of study selection and shows the approach utilized in this article to assess the eligibility of the identified papers and extract data. The authors included only peer-reviewed original papers, published or available as preprints and written in English with relevant content to our selected scope.
Fig. 1
Illustration of the literature search method and review process.
IMental health impacts
3Mental health implications of the SARS-CoV-2 outbreak on the general public
Extensive knowledge has been accumulated concerning the deleterious role of the pandemic on public psychological health. Non-pharmacological interventions (NPIs) commenced by the public health policymakers, such as strict physical distancing decrees and long-term shutdown of educational, recreational, and economic activities, are among the major culprits of these negative emotional instabilities [9]. Besides, massive scales of job losses and furloughs, with consequential low wages and depleted resources, negatively stroke people’s already susceptible mental wellbeing worldwide. Moreover, the abruptness and rapid spread of the infection and its related stigma, as well as the risk of contracting the coronavirus and transmitting it to their loved ones, further spurred mental distress among the public. Concomitant development of these problems provided a fertile ground for various mental disorders, including substance abuse, MDS, insomnia, and fatigue (anxiety symptoms) [10, 11]. Public and occupational health systems are in jeopardy due to the pandemic-related psychologic disturbances as these factors impinge on social resilience, preventing the replenishment of the depleted public resources [12]. Risk factors of the pandemic’s psychologic sequelae and their role in workplace-related distress have been debated. In the following sections, we further discuss these factors to address the pandemic’s mental health impact on workplaces.
3.1Mental health sequelae in the workforce
3.1.1Healthcare workers (HCWs)
Exceeding stress levels among healthcare workers (HCW) may herald a flare in their psychological outcomes. WHO intended that HCWs are vulnerable and prone to the onset of psychological repercussions predisposing them to PTSD, depressive symptoms, and burnout syndrome (BOS) during the pandemic [13]. On the same line, a bulk of data from previous outbreaks corroborate this contention, as a meta-analysis from the 2009 H1N1 pandemic unveiled the two-fold increased risk of disease contraction among HCW and one-fifth of HCW with clinical manifestations of the infection asserted similar symptoms among their family [14]. Besides this, there has been a social stigma against HCWs, including discrimination, insufficient knowledge, and contagion risks. In tandem with accrued working hours, social isolation lays a foundation for physical and mental exhaustion [15]. These findings resonate with a rifle of studies emerging from across the world, intending to the increased prevalence of major depressive syndrome (50%), and a rise in the incidence of an anxiety disorder (ranging between 22% to 45%), sleep disorder (33%), and stress (ranging between 28% to 72%) [16].
The occurrence of these symptoms rests on major risk determinants, including insufficient social support networks, dysfunctional modes of coping, and inadequate preparedness for disaster response plans. Other factors predisposing HCWs to devastating mental health outcomes include female gender, younger age, working as a nurse compared to physicians, and working close to COVID-19 patients. However, controversial investigations have been published regarding other sociodemographic traits. For instance, some studies claimed that living states (alone or with others), education, and geographical location does not affect the outcomes [17]. In contrast, others witnessed more pronounced signs of vicarious traumatic stress among separated, widowed, or married female nurses and those with intermediate work [18].
Studies adjusted for covariates unveiled that particularly frontline caregivers show more severe psychopathological manifestations. Evidence from an observational study among 1257 frontline HCWs mirrored the dramatic rise in depressive symptoms and anxiousness in one-half of the participants, and over three-quarters of the respondents intended work-related distress, while one-third complained about sleep difficulties [19]. Thus, working in patient-facing jobs is considered an independent risk determinant of worse psychiatric outcomes. These results are consistent with Lu et al.’s work, which examined the mental health of 550 HCWs during a period of 36 months post-severe acute respiratory syndrome (SARS) and reported moderate to severe symptoms of PTSD in over 10% of participants [20]. They intended that low SEP and living alone were the significant risk determinants of PTSD. A similar study among HCWs in Hong Kong also declared that over one-quarter needed mental health support following the SARS outbreak [21].
Another point meriting consideration is that WHO explains the burnout syndrome (BOS) as a compilation of adverse mental manifestations resulting from protracted workplace-related distress, encompassing mainly three dimensions. Firstly, the gradual accumulation of feeling worn-out and drained (exhaustion), a sense of detachment from one’s self and job (depersonalization), and reduced professional accomplishment [22]. Intense working schedules and insufficient supporting programs have led to increased exhaustion and detachment among HCWs while lowering their efficacy. Henceforth, the mental fatigue among caregivers would contribute to inefficiency at work and shallowed connections with the surrounding community and patients. Burnout, in essence, aims at accelerating productivity in the workplace; however, it causes several untoward effects, including moral injury and presenteeism [23]. On the personal level, it may impinge on the private lives of caregivers, implicating in suicidal ideation and separation. At the occupational stage, low quality of care, malpractice, and diminished patient satisfaction ensue. Evaluations have unraveled that stress is the cornerstone for developing BOS. Occupational stress has been linked to high workload, long shifts, and a toxic work atmosphere. Consistently, young adult nurses with low work histories are at the highest risk of developing emotional exhaustion and BOS [24].
(1) Moral injury is the consequence of one acting in opposition to their values and ethics, particularly upon abrupt trauma, resulting in psychosocial and behavioral distress. This is a more prevalent concept in military literature; howsoever, upon the burst of SARS-CoV-2 infection, HCWs have been put under strain to implement the limited sources of oxygen therapy and drugs of putative therapeutic value among an accelerating number of patients. Thus, inadvertently implicate in potential deaths that would not take place under stable conditions [25]. Concomitant inadequacy of resources, a need to maintain their safety along with protecting the patients, their families, and colleagues, accompanied by the heavy workloads, have contributed to increased vulnerability in terms of moral principles. Hence, these factors compound their mental health, laying a foundation for various psychologic conditions, such as major depressive disorder (MDD), PTSD, and self-harm [25, 26]. Institutional support has gotten to play a vital role in modulating the depth of these psychopathologies’ burden on HCWs during and post-pandemic [27].
(2) Presenteeism is the culture of continuing to work even with impaired productivity only as a performative measure. It has been attested that workplace upheavals during the pandemic could be accompanied by a pronounced rise in sick leave and employee turnover. However, regarding work ethics among HCWs, they place high values on their professional life and exert work-centered solid moral principles and commitment [28]. Consequently, the excessive workloads to provide healthcare to an exceeding number of patients, along with the common phenomenon of hesitancy and unwillingness to seek support in adverse times among caregivers, particularly physicians, has conjointly led to overarching repercussions, including presenteeism. To add weight to this argument, recently, Webster et al. recorded that among all occupational sectors, physicians exerted the highest rate of sickness presenteeism [29].
Overall, policymakers should consider implementing multidisciplinary psychosocial support groups involving psychotherapists, counselors, and occupational health specialists to improve HCWs’ mental health, particularly during burnout.
3.1.2Teleworkers
Upon the burst of COVID-19, teleworking has led to significant lifestyle changes with conjoint escalates in sedentary behavior, ergonomic risks, and attenuated physical activity. Thus, leading to several adverse events in the workforce, including weight gain, mental distress, and musculoskeletal diseases, such as low back pain [24].
Before the COVID-19 pandemic, an eligible strand of research had focused on the beneficial mental health impact of remote working, including amplified productivity, workflow, and connectivity between the workforce. However, during the lockdowns, teleworking impinged on much broader realms that, in turn, may channel its impact on mental health. Adopting distant-working methods challenged employees to carry on their assigned work among people unaware of their concerns with resultant increased distractions. To make matters worse, work and life are drastically entwined among remote workers due to blurred and indistinguishable boundaries representing work-life integration rather than balance [30]. The British Royal Society for Public Health surveyed how smart working influenced workforce mental health. A pronounced portion of respondents (68%) asserted lower connection with their coworkers, particularly during burdensome responsibilities and working troubles. Also, one-half declared their difficulty switching from work to personal life [24, 31].
Organizational support teams play an impotent role in reducing the isolation feeling and mental health issues among staff and increasing their connectivity. Several preventive plans have been established in this context, such as lucid instructions concerning work-life boundaries, enhanced IT support, and averting heavy workloads [24].
3.2Helping and service professions
3.2.1Social workers
Shelter-in-place orders derived most close-proximity jobs to a halt and continued through smart-working. Researchers unveiled significant alterations in the flow of social workers’ practice during the pandemic. Firstly, an upsurge in the use of technology-based approaches to meet the needs of their clients. Interestingly, healthcare social workers utilized ICT to connect patients in isolation rooms with their families via online platforms while the visits were restricted due to COVID-19 measures. Secondly, social workers have faced a substantial decline in their cases. The rationale is that these practices are commonly associated with referrals and mandatory reports, which have been greatly sabotaged during the pandemic. The paucity of calls has been declared by sexual offenses, child and domestic abuse social workers, owing in part to restricted admissions at medical centers due to the high load of COVID-19 patients and fear of contagion among vulnerable people [32]. In tandem, youth transitional housing social workers asserted they have never met such a nosedive decline in the bulk of cases as of the burst of COVID-19. There is a consensus that the dearth of calls is attributed to a hesitancy to ask for help or refer rather than a preceding number of housing units. Social workers portend an enormous increase in the load of their currently invisible patients beyond the capacity of regular services in the post-COVID-19 era. The predictively pronounced bulk of traumatizing sufferers with inaccessibility to social services will stretch the essential social sectors to the limit, requiring significant interventions to be commenced by policymakers [33].
On the other hand, societal inequities surfaced during the pandemic, and social workers have questioned the underpinnings of wealth distribution. For instance, governments worldwide aided vulnerable individuals with housing and financial aides during the pandemic, which could be continued beyond the pandemic.
3.2.2Teachers
Psychosomatic complications of the current pandemic in the academic sector have been vastly neglected. Implemented physical-distancing measures and associated technostress of ICT use have put unprecedented strains on teachers’ lifestyles. There is an overwhelming body of evidence regarding home teaching and increased work pressures pertaining to a significant rise in the symptomatology of anxiousness, major depressive symptoms, insomnia, and diminished professional satisfaction [34, 35]. In line, Li et al., through a cross-section study among Chinese teachers, witnessed that 14% suffer from anxiousness, with dominance among women of older ages [36]. These observations resonate with parallel streams of the literature that have emerged worldwide, as data from Prado-Gascó et al. reflected the high levels of exhaustion due to increased workloads among Spanish teachers [37].
Moreover, approximately two-thirds intended their positive attitude concerning home-teaching, while 10% of respondents declared the use of medical therapy to control pandemic-related distress. Another study evaluated the prevalence of mental pain among academic staff, revealing that 70% of respondents were distressed, with over 19% being severely pressured [38]. It has been concreted that anxiety symptoms impinge on social connections and play a devastating role in social network engagement. The latter is considered the primary coping method among educators. Others include social media interactions, prayers, and publishing research papers [38]. Common concerns among educators are as follows:
(1) Increased utilization of ICT; Intriguingly, contradictory to evidence from other economic sectors, Gorrochategi et al. demonstrated that among educators, older adults (>45y) are more susceptible to pandemic-related stressors [39]. The rationale for this rests in that compared to younger teachers, the adaption to distance teaching is more challenging for older adults, which constitute the majority of teachers in many parts of the world [40]. Available online platforms for assessing the assignments and preparing for examinations have put further strains on educators, while the risk of cheating in tests increased. These factors, concomitant with privacy issues and a steep decline in the positive teacher-student relationship, have contributed to teachers’ mental turmoil. On the other page, evidence has suggested a correlation between psychological downturn and women, particularly those inexperienced in smart working strategies before the pandemic lockdowns. This might stem from cultural gender inequalities in playing specific roles in the household [40].
(2) The nature of the pandemic; Prompting imminent response measures with undetermined protraction of restrictions. Concomitantly, institutional factors, including inadequate IT resources and support and unpreparedness for online teaching, have placed upheavals on educators. In fact, over one-half of teachers in a study asserted the risk of contagion with COVID-19 as their major source of stress, along with social isolation [32].
(3) Source of infection; A sizable fraction of the teachers’ psychologic disturbances might be the result of fears of predisposing students, particularly children, to SARS-CoV-2 disease in the setting of school classrooms. Indeed, this assumption of schools being the source of infection has been the prevailing notion since the burst of the pandemic leading to mental distress among teachers [41]. In this perspective, the reopening of education centers increased the tension among teachers concerning the health of their students. Arias Gallegos et al., through conducting a survey, drew attention to the higher levels of stress symptomatology in pre-primary and primary school. This is in discordance with observations prior to COVID-19, spotting that high school teachers interacting with adolescents recorded a significantly higher burden of mental distress [42]. A straightforward explanation for this phenomenon might rest on the more profound responsibility toward children more prone to infection, warranting prompt care beyond the normal states to meet their parents’ expectations. Also, bubble classroom management has inclined the school community to further pressures. Controversially, young adult students follow the protection measures themselves. On the other page, teachers’ mental discomfort is negatively associated with having a family, considering increased needs for childcare and homeschooling [43].
(4) Job instability; Cladellas-Pros et al. postulated that irrespective of age, job instability is a significant contributor to MDS and anxiousness among educators even before the pandemic, manifested by impaired psychosomatic health outcomes [44, 45]. Thus, COVID-19-associated furloughs and layoffs, unstable part-time educator works with low wages, compounded by diminished non-medical research funds faced by approximately 44% of teachers, play a devastating role on teachers’ health, warranting urgent actions to ascertain them with secured contracts [46].
3.2.3Psychologists
The gloomy picture of speculative acute and chronic psychological aftermaths during and post-COVID-19 has prompted calls for mental health services. Psychologists have come to play a vitally important role in mitigating the pandemic’s toll, while the pandemic is stretching the mental health resources to the limit. Research from Italy demonstrated that volunteer psychotherapists had been put under strain to remote working adoption and to meet the needs of an exceeding number of sufferers. They concreted this implication by recording unprecedented scores of different categories of BOS [7].
Viewing clinical psychotherapists’ performance through the lens of the five broad personality models enables researchers to investigate the untoward repercussions of the pandemic among them. Neuroticism, defined as a propensity to negative emotions and cognitive distortion, leads to impaired managing capability and a broad range of manifestations, including fatigue, agitation, and restlessness. This emotional instability is the leading predictive determinant of impaired mental health during screening among psychologists [33]. Agreeableness, defined as prosocial behaviors and inclination to cooperative interactions, contributes to more robust social support networks and enhances coping strategies. Openness is described as being prone to embracing fresh experiences and having a positive perception of new ideas. It was witnessed that openness imposes far-reaching effects on abating depersonalization feelings concomitant with boosting professional accomplishments. Hence, increasing job satisfaction among psychologists and dampening mental distance from their job and patients [47].
On the whole, a substantial portion of psychologists was unprepared for distance working, and such abrupt adaption to smart working led to detachment and mental distance from clients to different levels according to their personality traits. The research on insufficient ICT support and resources’ effect on psychologists is scant and controversial, although data exhibited a negative correlation between telematics use and more pronounced depersonalization feelings [32, 33]. Finally, compelling evidence has established that training courses for significant trauma preparation improve the mental well-being of clinical counselors in times of such reverberating disasters.
3.3The great resignation
Considering adjustment disorder from an occupational perspective sheds a bright light on commonly described mental symptomatology, such as MDS, anxiousness, behavioral distress, and PTSD. These workplace-related factors culminate in depleted resilience among the workforce, laying a foundation for employee dissatisfaction, organizational engagement, and poor employee performance (increased absences and sickness presence). Thus, these factors, accompanied by cognitive and affective job insecurity and decreased coworker support, have contributed to increased turnover intention and inadvertent mistakes [48]. In other words, unprecedented work pressure conjointly with implications on work ethics, particularly among HCWs, would exhibit a spillover effect on the workforce’s global social and mental health. These pandemic-associated repercussions compounding the psychosomatic status of the workforce and equipment shortages have contributed to BOS and pronounced turnover levels, particularly among close-proximity jobs, such as the healthcare sector [49]. Consistently, the term “great resignation” was coined by Anthony Klotz, a professor of management at UCL School of Management, to indicate a critical socio-economic trend collectively began in early 2021 in which an unprecedented bulk of the labor force voluntarily quit their jobs. A set of factors, including financial stagnation, enduring reduced job satisfaction, and health concerns, led employees to take early retirement or seek opportunities in organizations with enhanced smart-working strategies [48].
3.4Pandemic hit on mental health programs
The prevalence of mental illness was significantly high even before the pandemic. Data from 2018 claimed that 970 million people (13% of the global burden of diseases) had psychological disorders or substance abuse conditions. COVID-19 compounded the need for mental health services, which were insufficient even before the pandemic. WHO stated that psychological healthcare services in the high-risk groups were inadequate in over 67% of nations globally. Remarkably, more than two-thirds of vulnerable children and younger adults do not receive adequate care in the setting of mental, neurological, and substance use (MNS) programs [50].
Moreover, among women of child-bearing age and young adult students and workers, there is a 60% to 70% decline in their perinatal mental health services, peer support school- and workplace-based mental health programs, respectively. Canceled or postponed, inadequate support programs leave individuals vulnerable to pandemic-related psychological deficits [51]. The rationale for these global disruptions in mental health care lies in the paucity of enough specialists experienced in psychological support (33%). Other etiologies include lack of sufficient amounts of PPE (30%) and the transformation of mental health support facilities to field hospitals and isolation centers (20%). Moreover, community leaders in 116 countries put extended mental health programs in their pandemic response plans, although over 80% of these countries failed to allocate efficient financial resources to such projects [52]. Noteworthy, the costs of psychological therapy programs scaling millions of dollars impede their massive deployment, as the 2013 U.S. data declares that the prescriptions on mental health issues and substance abuse expensed over 188.7 billion USD. WHO reports significant insufficiency in global mental health resources, indicating an impending mental crisis without urgent prompting supportive actions [12, 53]. The voluntary, not-for-profit sector has taken center stage in this realm, raising funds for severely impacted individuals and virtual community support sessions.
3.4.1Occupational health services
Since the early days of the pandemic, workplace health concerns have come to play a progressively prominent role in order to curb infection. Challenging days are on the horizon for occupational health professionals to overcome the raised mental distress and ergonomic issues among the remote-working workforce and burnout in those with public-facing jobs. In this context, Total Worker Health®(TWH) is a set of exemplary plans developed by occupational and public health policymakers to enhance labor force wellbeing and productivity by fending off workplace health hazards concomitant with implementing health promotion and preventive injury measures [54, 55].
Researchers perceive the deployment of disability management and psychosomatic resilience-training projects focusing on personal and professional growth and growing a sense of belonging to a community contribute to increased commitment and productivity of the workforce in the post-COVID era. Exploiting ICT, which has shown great promise during the pandemic, concomitant with innovative and more flexible staffing strategies and collaborative interdisciplinary support teams, are presumed to improve workforce efficiency in times of major trauma [54].
3.5Risk factors for pandemic-related psychological distress
There has been an ongoing debate about the presumed risk determinants of the post-pandemic psychosocial impacts. Research in the UK has unraveled the prominent influence of being younger and women and being considered the high-risk group on the occurrence of psychologic turmoil. Consistently, data from eastern countries exhibited that educated young adults who live alone (single or divorced) and those with high-risk exposure jobs are more vulnerable to these symptoms [56]. On the other hand, it is suggested that the male gender, living in extended families, having a firm salary, having strong trust in HCWs, and minimized exposure to pandemic-related social media are among protective factors against detrimental mental health outcomes [57]. The protecting effect of living in more crowded households might stem from the importance of family support, particularly across Asian cultures [58]. In this realm, we should highlight that although the enacted physical distancing plans minimize the risk of disease transmission in those working in close-proximity jobs to their families, the undermined social bonds adversely affect their psychological wellbeing [59]. Research on the clinical course of the COVID-19 disease demonstrated that across its protean manifestations, coughing, headache, and pharyngitis are most robustly associated with the mental sequelae. Moreover, in concert with the health belief model, which intends that people are more willing to adopt health-promoting behaviors when they perceive themselves at high risk of contracting illness, more willingness toward NPIs, such as personal protective equipment (PPE) and hand hygiene reduces the perceived susceptibility to COVID-19 infection and hence enhances the positive mood [60].
3.6Social media exposure
ICTs and media platforms are harnessed to improve public awareness and keep them in touch with their social support network. However, the pandemic-related infodemic and magnified use of social media platforms culminated in the far-reaching spread of misinformation, stigma, and increased conflicts regarding the efficiency of lockdown measures in contending the disease [56]. Hence, distrust accrual and impinged social cohesion contribute to a decrease in the effectiveness of public health policies [61]. Consistently, ruminating media coverage and the readily available pandemic metrics, such as new cases and death toll on the internet, further devastate the emotional outcomes [62]. Data obtained from China’s healthcare system assessed the impact of social media exposure on mental health. They unveiled that upon curfew enforcement in Wuhan, between half to two-thirds of the citizens with self-reported intense internet surfing were grappled with MDS, and about 25% experienced combined symptomatology of depression and anxiousness, which is two-fold greater than individuals with restricted social media usage during the same period [49, 63].
Strikingly, the rising number of COVID-19 cases heralded flares of uncertainty and a detrimental infodemic, which warranted urgent policies to maintain community resilience by controlling social media exposure [64]. United Nations (U.N.), on May 12, 2020, commenced a set of recommendations to overcome the hostile cyber attempts and groundswell of anti-vaccination ideas. Moreover, WHO declared Resolution WHA73.1 as a pandemic response plan, underscoring the accurate pandemic-related knowledge dissemination and impeding internet content, which undervalues the public health policies [65].
IISocio-economic blow
4Disproportionate racial impact of the pandemic on the workforce
Epidemiologic investigations highlighted a pronounced racial impact in COVID-19 confirmed cases. In the USA, the mortality rate was up to 40% higher among African-Americans compared to Whites, with 178 deaths per 100k, and 124 deaths per 100k population, respectively [66, 67]. Several factors contribute to this finding, including the significant burden of chronic psychosomatic conditions and crowded housing, compounded by the economic strains among Blacks and minorities.
Occupational Information Network (O*NET) in the USA has investigated the adaptability to distance working plans across different organizations and claimed that the construction industry, medical centers, public transport services, accommodation, and food industry failed to show promise in terms of smart working adoption. Interestingly, Blacks and minorities are the predominant employees in these public-facing works, leaving them most vulnerable to COVID-19 exposure in the workplace [68]. To add weight to this argument, the CPS databank regarding pandemic-related unemployment rates underscored the milder impacts on Blacks’ employment status. Workers in low-income high-proximity jobs commonly commuted by public transport services. This is because they hold essential frontline jobs, such as healthcare, retail, and transport. Impaired adherence to physical distancing orders and restricted space in the transport system would increase the risk of COVID-19 contraction [69]. Controversially, UK references unfolded the excess job losses among ethnic minorities during the pandemic [70].
Similarly, substandard housing across low SEP people rendered them vulnerable to disease transmission. The paucity of space due to overcrowded households and patient isolation rooms impeded the efficient implementation of home-working strategies among these communities. Although, stronger interpersonal connections, mental support, and sharing the household costs were advantages of crowded dwellings [71]. Moreover, coinciding with the increase in health care expenses, lower accessibility to health insurance adversely influenced these communities. Overall, the disproportionate bulk of Blacks and minorities in high-physical proximity work, commuting, and unsafe dwellings increase their risk of contraction [72].
5Economic impact of the pandemic
Economic implications of the pandemic have gained prominence from the early waves in April 2020. COVID-19 yielded an intense decline in the gross domestic product (GDP) to the extent the USA had never experienced before. There is a body of ongoing research attempting to shed deep light on the prominent role of the pandemic on welfare metrics, revenue depletion, liquidity, employment rates, and workplace environment [73, 74]. The U.S. Bureau of Labor Statistics (BLS) recorded that global labor force income declined by 8.2%, which is equal to 4.5% of the global GDP and worth 3.7 trillion USD. Compared to 2019, working hours declined by 8.9% in 2020, fourfold greater than the financial crisis of 2008, equal to 227 million full-time jobs (Table 2). Economic analytic organizations, such as OECD indicated the significant cross-country inequalities in the fiscal resuscitating plans and policy responses to help with the pandemic’s blow [75]. Overall, pandemic has surfaced economic inequalities, warranting urgent actions regarding the entangled occupational implications in the post-pandemic era [76].
Table 2
Pandemic effect on lost working hours based on international labor organization (ILO) data in countries with highest confirmed case as of April 2022
| Country | Cumulative cases per 100k population | Total deaths | Income level | Lost (%) working hours – annual (%) | Lost working hours (as number of FTE jobs) – annual (k) | Total weekly hours worked per employed persons | Ratio of total weekly hours worked to population aged 15–64 | ||
| 2019 | 2020 | 2019 | 2020 | ||||||
| USA | 10563.2 | 611,801 | HIC | 9.2 | 13743.3 | 5967668 | 5406437 | 27.8 | 25.1 |
| Brazil | 9380.3 | 553,179 | UMIC | 14.9 | 13321 | 3548451 | 3037976 | 24.1 | 20.5 |
| Spain | 9337.1 | 81,396 | HIC | 13.2 | 2412.9 | 733900 | 632419 | 23.9 | 20.6 |
| France | 9121.5 | 111,923 | HIC | 8.4 | 2111.3 | 1006798 | 918518 | 24.3 | 22.2 |
| UK | 8674.3 | 129,718 | HIC | 12.8 | 3888.7 | 1207879 | 1055314 | 28 | 24.4 |
| Iran | 4573.4 | 89,479 | LMIC | 5.9 | 1632.4 | 1095950 | 1035206 | 19.2 | 17.9 |
| Russia | 4236.4 | 153,620 | UMIC | 8.5 | 5535.4 | 2646815 | 2388351 | 27.2 | 24.7 |
| Malaysia | 3322.3 | 8,551 | UMIC | 11.1 | 1931.3 | 688154 | 621110 | 31 | 27.7 |
| India | 2307.4 | 442,662 | LMIC | 13.7 | 71600.1 | 20682351 | 18071871 | 22.6 | 19.5 |
| Indonesia | 1214.9 | 88,659 | LMIC | 8.2 | 10424.9 | 4994857 | 4639060 | 27.2 | 25 |
FTE: Full-time equivalent, HIC: High-income economies (> $12,696), LMIC: Lower-middle income economies ($1,046 to $4,095), UMIC: Upper-middle income economies ($4,096 to $12,695) (92).
5.1Poverty rates
According to the world data lab, emerging economies face an unprecedented level of extreme poverty rates, which is described as daily income below 1.9 USD for the first time since 1998. World Bank data unveiled that in 2020, extreme poverty entangled approximately 9.5% of the world population grappled with extreme poverty [77]. Over 80% of the people slipping below the extreme poverty rates are across MIC. Individuals living in extreme poverty accrued from 668 million in 2019 to 750 million in 2020 and reached 711 million by the end of 2021, and will stabilize to 690 million in 2022. United Nations (U.N.) had predicted the 2020 escape rate from extreme poverty to be 2.3 people/second; however, this rate was assessed to be – 154.9 people/minute in 2020 [59, 78]. Before COVID-19, the poverty rate was targeted to decrease to 7.9% in 2020. Consistently, halted growth in average income during 2019–2021 shows a steep decrease in shared prosperity, focusing on revenue and consumption progress across the bottom 40% of the population (Table 3). Together, the impoverished individuals’ income inequalities and impinged resilience herald an enduring economic crash [79, 80].
Table 3
Poverty rates and shared prosperity across nations with highest COVID-19 cases as of May 2021 (93)
| Economy | Cases | Deaths | Number of poor (millions) | Poverty rate (%) | Poverty gap (%) | Ratio of poverty gap to poverty rate (%) | Annualized growth in mean consumption income per capita | Mean consumption (income per capita) |
| USA | 95,550,254 | 1,228,725 | 3.2 | 1.0 | 0.86 | 88.8 | 3.08 | 73.95 |
| India | 65,251,257 | 952,552 | 284.6 | 22.5 | 4.6 | 20.6 | N.A | N.A |
| Brazil | 39,254,651 | 822,228 | 9.3 | 4.4 | 1.6 | 37.1 | 0.12 | 20.97 |
| France | 33,859,584 | 523,540 | 0.0 | 0.02 | 0.01 | 39.2 | 0.77 | 52.97 |
| UK | 25,587,326 | 256,201 | 0.1 | 0.2 | 0.1 | 68.9 | 2.66 | 49.40 |
| Russia | 21,558,955 | 752,665 | 0.0 | 0.03 | 0.01 | 16.4 | –2.27 | 19.93 |
| Germany | 20,583,870 | 325,521 | 0.0 | 0.00 | 0.00 | N.A | 0.80 | 54.06 |
| Turkey | 18,551,696 | 254,847 | 0.0 | 0.36 | 0.05 | 13.1 | 1.47 | 19.91 |
| Italy | 17,957,318 | 514,450 | 0.9 | 1.4 | 1.1 | 78.5 | 1.04 | 42.53 |
| Spain | 15,849,254 | 256,911 | 0.3 | 0.7 | 0.5 | 79.4 | 1.81 | 37.77 |
5.2Occupations and workforce
BLS, data demonstrated that U.S. unprecedented levels of unemployment in April 2020 were only comparable to that of the Great Depression in the 1930s, varying between 14.5% and 19.5%. The employment among Americans in their prime working age (25–54y) took a steep decline to 51%, the lowest since 1949. Annual employment metrics in 2020 showed that the employment-to-population ratio decreased by 3.2% across Whites, 4.8% among Blacks, and 5.4% among Hispanics [81].
Through pandemic response plans, public health stakeholders divided occupations as essential, including medical centers and public transit services, which were more prone to COVID-19 contraction, and non-essential, such as recreational services, which exhibited more unemployment rates [82]. Notable, organizations adapt to smart working as an escape plan to increase the safety of their staff while preventing unemployment. Although, as discussed earlier, an array of economic sectors in the USA are not available from home [83]. The interplay between unemployment and disease transmission is critically essential. For instance, food and accommodation sectors are predominantly occupied by a low-wage workforce with low SEP grappled with underfunding, which per se is a risk factor for COVID-19 contraction. However, the number of confirmed cases among these people is not statistically significant. It is believed that enforced curfew by extended closures had contributed to this by putting thousands of workforce on furlough and layoff [84].
6Prospect
The public health stakeholders should channel their plans into three distinct categories. Firstly, emergent and semi-urgent programs warrant a firm response to the pandemic’s acute socio-economic and psychological implications. Secondly, long-term policies to orchestrate the health care and financial supplies to improve the quality of life and keep firms afloat. Thirdly, resilience training services emphasize on improving adaptability, sustainability, and inclusivity in the pandemic era [85]. From an economic lens, financial professionals claim that post-crisis economic policies encompass three primary avenues. They are firstly, commencing a massive scale of short-time work (STW) to improve flexibility in the workplace and maintain employment with lower incomes. Secondly, help self-employed and entrepreneurs by allocating revenue protection programs. Thirdly, prioritizing feedback to ongoing setbacks in the labor market [86].
Since one individual out of five is afflicted by at least one type of psychological disorder and half of the population is at risk, policymakers should implement services to avert a psychological crisis. Indeed, psychological peer support programs by telemedicine, such as online peer support programs, have garnered attention [87]. Cognitive therapies, including motivational interviewing (MI), cognitive behavioral therapy (CBT), limiting exposure to social media, and maintaining productivity in daily living, could improve mental health outcomes [87]. Controlling the psychological impacts in the marketplace is channeled to multiple categories, such as safety measures, using PPE to protect staff, and utilizing resilience training services. The Time to Change program showed promise in precluding stigmatization in the shocked society by training a set of uncomplicated interventions in the workplace. Another firm example of occupational health programs is trauma risk management service (TRiM), which instructs nonclinical staff to evaluate colleagues in terms of mental health through a health crisis and offer simple psychological support as well as referral to specialists in severe cases. Mental health first aid (MHFA) works in concert with TRiM, showing promise in protecting psychological wellbeing in the traumatized workplace [88]. Furthermore, maintaining work/life boundaries, clear communication, and disseminating evidence-based updates will increase workers’ resilience. Risk factors for the workforce’s mental distress, such as bereavement, previously diagnosed mental disorder, shock, isolation, and low SEP, should be considered in response plans [89].
7Limitations
Limitations of this manuscript should be acknowledged before data extraction from the present paper. First, the studies we assessed utilized a vast array of data collection systems such as voluntary questionnaires, commonly susceptible to sampling and respondent bias, thus declining the generalizability of the results. Despite the rapid data analysis in online surveys, participants engaged in the conducted surveys display characteristic sociodemographic traits, including higher education and internet access, with fewer elder population involvements. Furthermore, self-reporting on health and financial instabilities was not confirmed through third-party valuer involvement, inclining studies to reporting bias [90]. Of note, some studies declared the respondent rate of their surveys exhibiting a wide range and relatively low rates. In addition to assay limitations, in many instances, the questionnaires examined categories specific to COVID-19, which exert discordance with established criteria of the constructs of interest. Although we assessed several longitudinal nested case-control and cohort papers to increase the reliability of our data, we obtained some of our data from cross-section studies, which further limit the representativeness over time and cannot rely on to gather a concrete understanding of the potential linkages in the future. The cause-and-effect relationship between the workplace measures and the psychosocial effects is subject to further validation, with studies determining the organizational measures more specifically. Finally, we assessed studies from different regions worldwide displaying various healthcare systems, GDP and economic levels, and even broader, with cultural differences in the face of stressors [91].
However, the present manuscript has several beneficiaries leveraging its impact. It opens a new avenue to link pandemic-related changes in living to the alterations in the psychological and economic states of the population, particularly the workforce. This paper attempts to shed light on the risk determinants among specific populations giving priorities in managing the crisis. Finally, it declares certain relationships across socio-economic states and psychosomatic domains in the field of public health.
8Conclusion
The pandemic burden and exponentially rising cases pushed healthcare services to extreme limits. The triangle of the pandemic health impact, lockdown measures, and socio-economic vulnerabilities contribute to mental distress among the workforce. We attempted to address the potential risk and protective mental health factors in the workplace setting by debating the perturbations in public health services. We emphasized that clear communication, science-based information dissemination, pronounced interpersonal relationships, and resilience training programs help sustain a productive perspective across the workforce. Also, financial instabilities mandate extensive restructuration to primarily resuscitate from the ongoing trauma and provide plans for the future impacts of trauma on economics. This manuscript unfolded the pronounced inequalities across races regarding SEP and employment conditions. We addressed the untoward spillover socio-economic implications of the pandemic by employing poverty rate and employment statistics on occupations and the labor force.
Conflict of interest
The authors declare that they have no conflicts of interest to report regarding the present study.
Author contributions
Study conception and design: HW; Data collection: NS, FF; Analysis and interpretation of results: FF; Draft manuscript preparation: HW, FF, NS. All authors reviewed the results and approved the final version of the manuscript.
Funding
This study was financially supported by the Social Science Program of Hainan Province (HNSK(YB)19-10).
Ethical approval
Not applicable.
Informed consent
Not applicable.
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
[1] | Velavan TP , Meyer CG . The COVID-19 epidemic. Tropical Medicine & International Health. (2020) ;25: (3):278. |
[2] | Paul A , Englert P , Varga M . Socio-economic disparities and COVID-19 in the USA. Journal of Physics: Complexity. (2021) ;2: (3):035017. |
[3] | Covid C , Team VBCI , COVID C , Team VBCI , COVID C , Team VBCI , et al. COVID-19 vaccine breakthrough infections reported to CDC—United States, January 1–April 30, 2021. Morbidity and Mortality Weekly Report. (2021) ;70: (21):792. |
[4] | Demmou L , Franco G , Calligaris S , Dlugosch D . Liquidity shortfalls during the COVID-19 outbreak: Assessment and policy responses. (2021) . |
[5] | Almeida H . Liquidity Management During the Covid-19 Pandemic. Asia-Pacific Journal of Financial Studies. (2021) ;50: (1):7–24. |
[6] | Brunnermeier M , Landau J-P , Pagano M , Reis R . Throwing a COVID-19 liquidity life-line. Economics for Inclusive Prosperity (Econfip). (2020) ;231. |
[7] | McGinty EE , Presskreischer R , Han H , Barry CL . Psychological distress and loneliness reported by US adults in 2018 and April 2020. Jama. (2020) ;324: (1):93–4. |
[8] | Pierce M , McManus S , Jessop C , John A , Hotopf M , Ford T , et al. Says who? The significance of sampling in mental health surveys during COVID-19. The Lancet Psychiatry. (2020) ;7: (7):567–8. |
[9] | He L , Mu L , Jean JA , Zhang L , Wu H , Zhou T , et al. Contributions and Challenges of Public Health Social Work Practice during the Initial 2020 COVID-19 Outbreak in China. The British Journal of Social Work. (2022) . |
[10] | Holmes EA , O’Connor RC , Perry VH , Tracey I , Wessely S , Arseneault L , et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. The Lancet Psychiatry. (2020) ;7: (6):547–60. |
[11] | Wang J , Tian J , Zhang X , Yang B , Liu S , Yin L , et al. Control of Time Delay Force Feedback Teleoperation System With Finite Time Convergence. Frontiers in Neurorobotics. (2022) ;16. |
[12] | Pfefferbaum B , North CS . Mental health and the Covid-19 pandemic. New England Journal of Medicine. (2020) ;383: (6):510–2. |
[13] | Liu CH , Zhang E , Wong GTF , Hyun S . Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: Clinical implications for US young adult mental health. Psychiatry Research. (2020) ;290: :113172. |
[14] | Lietz J , Westermann C , Nienhaus A , Schablon A . The occupational risk of influenza A (H1N1) infection among healthcare personnel during the pandemic: a systematic review and meta-analysis of observational studies. PloS One. (2016) ;11: (8):e0162061. |
[15] | Vani P , Banerjee D . “Feared and Avoided”: Psychosocial effects of stigma against health-care workers during COVID-19. Indian Journal of Social Psychiatry. (2021) ;37: (1):14. |
[16] | Talevi D , Socci V , Carai M , Carnaghi G , Faleri S , Trebbi E , et al. Mental health outcomes of the CoViD-19 pandemic. Rivista di Psichiatria. (2020) ;55: (3):137–44. |
[17] | Gloster AT , Lamnisos D , Lubenko J , Presti G , Squatrito V , Constantinou M , et al. Impact of COVID-19 pandemic on mental health: An international study. PloS One. (2020) ;15: (12):e0244809. |
[18] | Li Z , Ge J , Yang M , Feng J , Qiao M , Jiang R , et al. Vicarious traumatization in the general public, members, and non-members of medical teams aiding in COVID-19 control. Brain, Behavior, and Immunity. (2020) ;88: :916–9. |
[19] | Jalili M , Niroomand M , Hadavand F , Zeinali K , Fotouhi A . Burnout among healthcare professionals during COVID-19 pandemic: a cross-sectional study. International Archives of Occupational and Environmental Health. (2021) ;94: (6):1345–52. |
[20] | Lu Y-C , Shu B-C , Chang Y-Y . The mental health of hospital workers dealing with severe acute respiratory syndrome. Psychotherapy and Psychosomatics. (2006) ;75: (6):370–5. |
[21] | Chua SE , Cheung V , Cheung C , McAlonan GM , Wong JW , Cheung EP , et al. Psychological effects of the SARS outbreak in Hong Kong on high-risk health care workers. The Canadian Journal of Psychiatry. (2004) ;49: (6):391–3. |
[22] | Chirico F , Afolabi AA , Ilesanmi OS , Nucera G , Ferrari G , Sacco A , et al. Prevalence, risk factors and prevention of burnout syndrome among healthcare workers: an umbrella review of systematic reviews and meta-analyses. Journal of Health Social Sciences. (2021) ;6: (4):465–91. |
[23] | CHIRICO F , AFOLABI AA , Stephen O , ILESANMI GN , FERRARI G , SZARPAK L , et al. Workplace violence against healthcare workers during the COVID-19 pandemic: A systematic review. J Health Soc Sci. (2022) ;7: (1):14–35. |
[24] | Albertson AJ , Landsness EC , Tang MJ , Yan P , Miao H , Rosenthal ZP , et al. Normal Aging in Mice is Associated with a Global Reduction in Cortical Spectral Power and a Network-Specific Decline in Functional Connectivity. |
[25] | Litz BT , Stein N , Delaney E , Lebowitz L , Nash WP , Silva C , et al. Moral injury and moral repair in war veterans: A preliminary model and intervention strategy. Clinical Psychology Review. (2009) ;29: (8):695–706. |
[26] | Gong X , Wang L , Mou Y , Wang H , Wei X , Zheng W , et al. Improved Four-channel PBTDPA control strategy using force feedback bilateral teleoperation system. International Journal of Control, Automation and Systems. (2022) ;20: (3):1002–17. |
[27] | Damery S , Draper H , Wilson S , Greenfield S , Ives J , Parry J , et al. Healthcare workers’ perceptions of the duty to work during an influenza pandemic. Journal of Medical Ethics. (2010) ;36: (1):12–8. |
[28] | Goulia P , Mantas C , Dimitroula D , Mantis D , Hyphantis T . General hospital staff worries, perceived sufficiency of information and associated psychological distress during the A/H1N1 influenza pandemic. BMC Infectious Diseases. (2010) ;10: (1):1–11. |
[29] | Webster RK , Liu R , Karimullina K , Hall I , Amlot R , Rubin GJ . A systematic review of infectious illness presenteeism: prevalence, reasons and risk factors. BMC Public Health. (2019) ;19: (1):1–13. |
[30] | Chirico F , Zaffina S , Di Prinzio RR , GIORGI G , FERRARI G , CAPITANELLI I , et al. Working from home in the context of COVID-19: A systematic review of physical and mental health effects of teleworkers. J Health Soc Sci. (2021) ;6: (3):319–32. |
[31] | Chirico F , Sacco A , Nucera G , Ferrari G , Vinci MR , Zaffina S , et al. Lockdown measures and COVID-19 related deaths during the first and second COVID-19 waves in Italy: a descriptive study. J Health Soc Sci. (2021) ;6: (3):379–90. |
[32] | Abrams LS , Dettlaff AJ . Voices from the frontlines: Social workers confront the COVID-19 pandemic. Social Work. (2020) ;65: (3):302–5. |
[33] | CRESCENZO P , CHIRICO F , FERRARI G , SZARPAK L , NUCERA G , MARCIANO R , et al. Prevalence and predictors of burnout syndrome among Italian psychologists following the first wave of the COVID-19 pandemic: A cross-sectional study. Journal of Health and Social Sciences. (2021) ;6: (4):509–26. |
[34] | Besser A , Lotem S , Zeigler-Hill V . Psychological stress and vocal symptoms among university professors in Israel: implications of the shift to online synchronous teaching during the COVID-19 pandemic. Journal of Voice. (2020) . |
[35] | Ozamiz-EtxebarriaN Berasategi SantxoN Idoiaga MondragonN Dosil SantamaríaM. The psychological state of teachers during the COVID-19 crisis: The challenge of returning to face-to-face teaching. Frontiers in Psychology. (2021) ;11: :620718. |
[36] | Li Q , Miao Y , Zeng X , Tarimo CS , Wu C , Wu J . Prevalence and factors for anxiety during the coronavirus disease 2019 (COVID-19) epidemic among the teachers in China. Journal of Affective Disorders. (2020) ;277: :153–8. |
[37] | Prado-Gascó V , Gómez-Domínguez MT , Soto-Rubio A , Díaz-Rodríguez L , Navarro-Mateu D . Stay at home and teach: A comparative study of psychosocial risks between Spain and Mexico during the pandemic. Frontiers in Psychology. (2020) ;11: :566900. |
[38] | de la Fuente J , Peralta-Sánchez FJ , Martínez-Vicente JM , Sander P , Garzón-Umerenkova A , Zapata L . Effects of self-regulation vs. external regulation on the factors and symptoms of academic stress in undergraduate students. Frontiers in Psychology. (2020) ;11: :1773. |
[39] | Gorrochategi MP , Munitis AE , Santamaria MD , Etxebarria NO . Stress, anxiety, and depression in people aged over 60 in the COVID-19 outbreak in a sample collected in Northern Spain. The American Journal of Geriatric Psychiatry. (2020) ;28: (9):993–8. |
[40] | Song Y , Chen YY . Information and communication technology among early and late middle-aged adults in urban China: Daily use and anticipated support in old age. Australasian Journal on Ageing. (2019) ;38: (3):e85–e92. |
[41] | Fitzpatrick KM , Harris C , Drawve G . How bad is it? Suicidality in the middle of the COVID-19 pandemic. Suicide and Life-Threatening Behavior. (2020) ;50: (6):1241–9. |
[42] | Arias Gallegos WL , Huamani Cahua JC , Ceballos Canaza KD . Síndrome de Burnout en profesores de escuela y universidad: un análisis psicométrico y comparativo en la ciudad de Arequipa. Propósitos y Representaciones. (2019) ;7: (3):72–91. |
[43] | Daks JS , Peltz JS , Rogge RD . Psychological flexibility and inflexibility as sources of resiliency and risk during a pandemic: Modeling the cascade of COVID-19 stress on family systems with a contextual behavioral science lens. Journal of Contextual Behavioral Science. (2020) ;18: :16–27. |
[44] | Cladellas-Pros R , Castelló-Tarrida A , Parrado-Romero E . Satisfacción, salud y estrés laboral del profesorado universitario según su situación contractual. Revista de Salud Pública. (2018) ;20: :53–9. |
[45] | Ma D , Zhang C , Hui Y , Xu B . Economic uncertainty spillover and social networks. Journal of Business Research. (2022) ;145: :454–67. |
[46] | Ozamiz-Etxebarria N . Emotional state of school and university teachers in northern Spain in the face of COVID-19. Revista Espanola De Salud Publica. (2021) ;95. |
[47] | Fan X , Wei G , Lin X , Wang X , Si Z , Zhang X , et al. Reversible switching of interlayer exchange coupling through atomically thin VO2 via electronic state modulation. Matter. (2020) ;2: (6):1582–93. |
[48] | CHIRICO F , LEITER M . Journal of Health and Social Sciences (JHSS). J Health Soc Sci. (2022) ;7: (1):9–13. |
[49] | Mokona H , Yohannes K , Ayano G . Youth unemployment and mental health: prevalence and associated factors of depression among unemployed young adults in Gedeo zone, Southern Ethiopia. International Journal of Mental Health Systems. (2020) ;14: (1):1–11. |
[50] | Wei G , Fan X , Xiong Y , Lv C , Li S , Lin X . Highly disordered VO2 films: appearance of electronic glass transition and potential for device-level overheat protection. Applied Physics Express. (2022) ;15: (4):043002. |
[51] | Fadhel FH , Alqahtani MM , Arnout BA . Working with patients and the mental health of health care workers during the COVID-19 pandemic. Work. (2022) (Preprint):1–12. |
[52] | Moreno C , Wykes T , Galderisi S , Nordentoft M , Crossley N , Jones N , et al. How mental health care should change as a consequence of the COVID-19 pandemic. The Lancet Psychiatry. (2020) ;7: (9):813–24. |
[53] | Huang C , Wu X , Wang X , He T , Jiang F , Yu J . Exploring the relationships between achievement goals, community identification and online collaborative reflection. Educational Technology & Society. (2021) ;24: (3):210–23. |
[54] | Chirico F , Sacco A , Ferrari G . Total Worker Health” strategy to tackle the COVID-19 pandemic and future challenges in the workplace. Journal of Health Social Sciences. (2021) ;6: (4):452–7. |
[55] | Ma D , Zhu Q . Innovation in emerging economies: Research on the digital economy driving high-quality greendevelopment. Journal of Business Research. (2022) ;145: :801–13. |
[56] | Han RH , Schmidt MN , Waits WM , Bell AK , Miller TL . Planning for mental health needs during COVID-19. Current psychiatry reports. (2020) ;22: (12):1–10. |
[57] | Yao L , Li X , Zheng R , Zhang Y . The Impact of Air Pollution Perception on Urban Settlement Intentions of Young Talent in China. International Journal of Environmental Research and Public Health. (2022) ;19: (3):1080. |
[58] | Bhar S , Bhattacharya D , Bose S . Analysing mental health of India during COVID using Twitter. (2020) . |
[59] | Chen J-J , Jiang T-N , Liu M-F . Family socioeconomic status and learning engagement in chinese adolescents: the multiple mediating roles of resilience and future orientation. Frontiers in Psychology. (2021) ;12. |
[60] | Leung CC , Lam TH , Cheng KK . Mass masking in the COVID-19 epidemic: people need guidance. Lancet. (2020) ;395: (10228):945. |
[61] | Zhuang M , Zhu W , Huang L , Pan W-T . Research of influence mechanism of corporate social responsibility for smart cities on consumers’ purchasing intention. Library Hi Tech. (2021) . |
[62] | Gao J , Zheng P , Jia Y , Chen H , Mao Y , Chen S , et al. Mental health problems and social media exposure during COVID-19 outbreak. Plos One. (2020) ;15: (4):e0231924. |
[63] | Guo Y , Yang Y , Kong Z , He J . Development of Similar Materials for Liquid-Solid Coupling and Its Application in Water Outburst and Mud Outburst Model Test of Deep Tunnel. Geofluids. (2022) ;2022. |
[64] | Liu S , He X , Chan FT , Wang Z . An extended multi-criteria group decision-making method with psychological factors and bidirectional influence relation for emergency medical supplier selection. Expert Systems with Applications. (2022) ;202: :117414. |
[65] | Almeida M , Shrestha AD , Stojanac D , Miller LJ . The impact of the COVID-19 pandemic on women’s mental health. Archives of Women’s Mental Health. (2020) ;23: (6):741–8. |
[66] | Wiemers EE , Abrahams S , AlFakhri M , Hotz VJ , Schoeni RF , Seltzer JA . Disparities in vulnerability to severe complications from COVID-19 in the United States. National Bureau of Economic Research; (2020) . |
[67] | Fabic MS , Choi Y , Bishai D . Deaths among COVID Cases in the United States: Racial and Ethnic Disparities Persist. MedRxiv. (2020) . |
[68] | Bueno M , Perez F , Valerio R , Areola EMQ . A usability study on google site and wordwall.net: online instructional tools for learning basic integration amid pandemic. Journal of Global Business and Social Entrepreneurship (GBSE). (2022) ;7: (23). |
[69] | Liu S , He X , Chan FT , Wang Z . An Extended Multi-Criteria Group Decision-Making Method with Psychological Factors and Bidirectional Influence Relation for Emergency Medical Supplier Selection. Expert Systems with Applications. (2022) :117414. |
[70] | Brooks MM , Mueller JT , Thiede BC . Rural-urban differences in the labor-force impacts of COVID-19 in the United States. Socius. (2021) ;7: :23780231211022094. |
[71] | Verdery AM , Smith-Greenaway E , Margolis R , Daw J . Tracking the reach of COVID-19 kin loss with a bereavement multiplier applied to the United States. Proceedings of the National Academy of Sciences. (2020) ;117: (30):17695–701. |
[72] | Sarfraz M , Hafeez H , Abdullah MI , Ivascu L , Ozturk I . The effects of the COVID-19 pandemic on healthcare workers’ psychological and mental health: The moderating role of felt obligation. Work. (2022) (Preprint):1–12. |
[73] | <IF-01>. The Global Economic Impact of COVID-19. (2020) . |
[74] | Chen Y , Sivakumar V . Investigation of finance industry on risk awareness model and digital economic growth. Annals of Operations Research. (2021) :1–22. |
[75] | Obayelu AE , Edewor SE , Ogbe AO . Trade effects, policy responses and opportunities of COVID-19 outbreak in Africa. Journal of Chinese Economic and Foreign Trade Studies. (2020) . |
[76] | Wang C , Wang D , Abbas J , Duan K , Mubeen R . Global financial crisis, smart lockdown strategies, and the COVID-19 spillover impacts: A global perspective implications from Southeast Asia. Frontiers in Psychiatry. (2021) ;12. |
[77] | Huang PH . Pandemic Emotions: The Good, The Bad, and The Unconscious-Implications for Public Health, Financial Economics, Law, and Leadership. Nw JL & Soc Pol’y. (2020) ;16: :81. |
[78] | Sumner A , Hoy C , Ortiz-Juarez E . Estimates of the Impact of COVID-19 on Global Poverty: WIDER working paper; (2020) . |
[79] | Tandon A , Roubal T , McDonald L , Cowley P , Palu T , de Oliveira Cruz V , et al. Economic Impact of COVID-19. (2020) . |
[80] | Liu F , Zhang G , Lu J . Multisource heterogeneous unsupervised domain adaptation via fuzzy relation neural networks. IEEE Transactions on Fuzzy Systems. (2020) ;29: (11):3308–22. |
[81] | Coibion O , Gorodnichenko Y , Weber M . Labor markets during the COVID-19 crisis: A preliminary view. National Bureau of economic research; (2020) . |
[82] | Falvey JR , Krafft C , Kornetti D . The essential role of home-and community-based physical therapists during the COVID-19 pandemic. Physical Therapy. (2020) ;100: (7):1058–61. |
[83] | Garnier R , Benetka JR , Kraemer J , Bansal S . Socioeconomic disparities in social distancing during the COVID-19 pandemic in the United States: observational study. Journal of Medical Internet Research. (2021) ;23: (1):e24591. |
[84] | Côté D , Durant S , MacEachen E , Majowicz S , Meyer S , Huynh AT , et al. A rapid scoping review of COVID-19 and vulnerable workers: Intersecting occupational and public health issues. American Journal of Industrial Medicine. (2021) ;64: (7):551–66. |
[85] | Issa UH , Balabel A , Abdelhakeem M , Osman M . Developing a Risk Model for Assessment and Control of the Spread of COVID-19. Risks. (2021) ;9: (2):38. |
[86] | Hijzen A , Martin S . The role of short-time work schemes during the global financial crisis and early recovery: a cross-country analysis. IZA Journal of Labor Policy. (2013) ;2: (1):1–31. |
[87] | Cheng P , Xia G , Pang P , Wu B , Jiang W , Li Y-T , et al. COVID-19 epidemic peer support and crisis intervention via social media. Community Mental Health Journal. (2020) ;56: (5):786–92. |
[88] | Galbraith N , Boyda D , McFeeters D , Hassan T . The mental health of doctors during the COVID-19 pandemic. BJPsych Bulletin. (2021) ;45: (2):93–7. |
[89] | Dewa CS , McDaid D . Investing in the mental health of the labor force: Epidemiological and economic impact of mental health disabilities in the workplace. Work Accommodation and Retention in Mental Health: Springer; (2011) . 33–51. |
[90] | Lv Z , Chen D , Lv H . Smart city construction and management by digital twins and BIM big data in COVID-19 scenario. ACM Transactions on Multimidia Computing Communications and Applications. (2022) . |
[91] | Wu S , Zhang K , Parks-Stamm EJ , Hu Z , Ji Y , Cui X . Increases in anxiety and depression during COVID-19: a large longitudinal study from China. Frontiers in Psychology. (2021) ;12: :2716. |
[92] | Lee S , Schmidt-Klau D , Verick S . The labour market impacts of the COVID-19: A global perspective. The Indian Journal of Labour Economics. (2020) ;63: (1):11–5. |
[93] | Bank W . Poverty and shared prosperity 2018: Piecing together the poverty puzzle. The World Bank; (2018) . |

