
An intervention study through education: The change in attitudes and knowledge of educators about the COVID-19 vaccine
Abstract
BACKGROUND:
Reliable and culturally informed health communication is vital in developing positive health behaviors.
OBJECTIVE:
The aim of this study was to investigate the change in knowledge and attitudes about COVID-19 vaccines by providing training to educators in a province in the east of Turkey.
METHODS:
A questionnaire developed by the researchers on the basis of the literature was used in this intervention study. It consisted of three parts: socio-demographic information, before education knowledge (BEK) and Attitudes Towards the COVID-19 Vaccine (BEATV), and after education knowledge (AEK) and Attitudes Towards the COVID-19 Vaccine (AEATV). There were 99 teachers, 32 public education teachers, and 144 religious officials who participated in the study. The data were analyzed using SPSS Statistics Pack version 22.0 (IBM, Armonk, NY, USA). Statistical significance value was accepted as p < 0.05.
RESULTS:
Among the participants, the number of correct answers to all questions increased as a result of the study. There was a positive increase in most of the ATV items after the training.
CONCLUSION:
Education on COVID-19 vaccines increased awareness as shown by the total number of correct answers and the improved attitude of educators.
1Introduction
The COVID-19 pandemic has brought disease and death, severely disrupting economies worldwide [1]. For these reasons, the necessity of combating the pandemic has arisen. Today, vaccination is still the most powerful way to combat infectious diseases. Vaccination, along with other public health measures, can contribute to reducing the devastating health, economic, and social problems resulting from the global spread of COVID-19. All around the world, vaccines were developed, safety and efficacy studies were carried out, and it was shown that the vaccines were safe and effective [2, 3]. However, studies also revealed that the COVID-19 had side effects [4, 5].
Vaccine acceptance has been negatively affected by the rapid development of the COVID-19 vaccines [6]. The necessity for preliminary preparations for vaccine acceptance was proposed before the development of COVID-19 vaccines. Widespread and equitable access to the vaccine is essential. Widespread vaccination at a level sufficient to provide herd immunity requires strategies to increase trust and acceptance of the vaccine, as well as adequate health system capacity [1]. Vaccine refusal was stated by WHO as one of the top ten global health threats in 2019 [7]. In many countries, vaccine hesitancy due to misinformation poses significant barriers to ensuring herd immunity [8, 9].
Vaccine hesitancy is defined as “delaying in acceptance or refusal of vaccination despite availability of vaccination services” [7]. A careful balance is needed between educating the public on the need for universal vaccination and avoiding any recommendations to enforce a mandate for universal vaccination. Community-based groups and non-governmental organizations considered to not have bias are of crucial importance in building the public’s trust in the COVID-19 vaccine [1].
Reliable and culturally informed health communication is vital in developing positive health behaviors [8, 9]. This includes preparing the public with accurate information and technological support [1]. Educators for a mass vaccination program need local participation of respected civic, religious, and fraternal organizations, as well as other trusted spokespersons [1].
Affecting public health and creating an economic burden, the COVID-19 pandemic caused an increase in mortality and morbidity as well as economic difficulties due to illness and quarantine periods of employees. COVID-19 vaccination rates in eastern Turkey had not reached the levels required for herd immunity.
The aim of this study is to examine the change in the knowledge and attitudes about COVID-19 vaccines by providing training to educators in a province in the east of Turkey.
2Materials and methods
2.1Study design and setting
Teachers, public education teachers (PET), and religious officials (religious educators) were included in the study. Unlike school-based education, public education teachers provide training to acquire professions and hobbies for housewives and other people who do not attend school. In this context, PETs provide training by offering courses in information technologies, animal breeding, sewing and embroidery, and woodworking. An invitation for COVID-19 vaccine education was sent via Elazıg Provincial Health Directorate. As a result, 99 teachers, 32 PETs, and 144 religious officials volunteered to participate in the study.
Ethical permission was obtained from Fırat University Rectorate Non-Interventional Research Ethics Committee (approval no. 2021/12-41 dated 18.11.2021) and written approval from Elazıg Ministry of Health.
The training was prepared using the information page against COVID-19 hesitation on the website of the Ministry of Health of the Republic of Turkey. The training material was based on the literature. The training was given during a two hours session by public health experts working at Elazıg Provincial Health Directorate and Fırat University. The content of the training included COVID-19 vaccine protection, safety and vaccination, as well as the public health rules. The training covered the questions asked in the questionnaire.
2.2Data collection
A questionnaire was developed by the researchers. It consisted of three parts: the socio-demographic information, before education knowledge (BEK) and before education attitudes towards the COVID-19 Vaccine (BEATV), and after education knowledge (AEK) and after education attitudes towards the COVID-19 vaccine (AEATV).
2.2.1Knowledge questions
Questions measuring knowledge were prepared from the training content. The answer options were as follows: yes, no, I don’t know.
Scientifically, the COVID-19 vaccines;
1. Is it protective?
2. Is it safe?
3. Is its development in a short time doubtful?
4. Is it safe for pregnant women?
5. Should mask-distance-hygiene rules be followed after vaccination?
(Correct answers; 1, 2, 4, 5: yes, 3: no)
2.2.2ATV items
The Attitudes Towards the COVID-19 Vaccine (ATV) was used in this study [8]. A 5-point Likert scale is used in the ATV scale. Turkish validity and reliability study was conducted on the ATV [9].
Table 1
Distribution of sociodemographic characteristics by occupation
| Sociodemographic | Teacher | PET | RO | Total | |
| characteristics | % * (n) | % * (n) | % * (n) | % (n) | |
| Sex | Male | 31,6 (87) | 11,6 (32) | 51,6 (142) | 94,9 (261) |
| Female | 4,4 (12) | 0,0 (0) | 0,7 (2) | 5,1 (14) | |
| Marital status | Married | 32,0 (88) | 10,2 (28) | 51,3 (141) | 93,5 (257) |
| Single | 3,3 (9) | 0,7 (2) | 1,1 (3) | 5,1 (14) | |
| Others | 0,7 (2) | 0,7 (2) | 0,0 (0) | 1,5 (4) | |
| Child | Yes | 32,0 (88) | 10,2 (28) | 49,5 (136) | 91,6 (252) |
| No | 4,0 (11) | 1,5 (4) | 2,9 (8) | 8,4 (23) | |
| Kronic disease | Yes | 5,1 (14) | 5,5 (15) | 16,7 (46) | 27,3 (75) |
| No | 30,9 (85) | 6,2 (17) | 35,6 (98) | 72,7 (200) | |
| COVID-19 vaccine | Yes | 33,8 (93) | 10,5 (29) | 44,7 (123) | 89,1 (245) |
| No | 2,2 (6) | 1,1 (3) | 7,6 (21) | 10,9 (30) | |
| COVID-19 PCR+ | Yes | 12,7 (35) | 5,8 (16) | 17,8 (49) | 36,4 (100) |
| No | 23,3 (64) | 5,8 (16) | 34,5 (95) | 63,6 (175) | |
| Relative COVID-19 | Yes | 30,2 (83) | 10,5 (29) | 43,3 (119) | 84,0 (231) |
| No | 5,8 (16) | 1,1 (3) | 9,1 (25) | 16,0 (44) | |
| Childhood vaccinations | Yes | 34,2 (94) | 11,3 (31) | 46,5 (128) | 92,0 (253) |
| No | 1,8 (5) | 0,4 (1) | 5,8 (16) | 8,0 (22) | |
| If domestic production (Turcovac) | Yes | 23,6 (65) | 9,1 (25) | 38,5 (106) | 71,3 (196) |
| No | 10,2 (28) | 2,5 (7) | 11,3 (31) | 24,0 (66) | |
*Percentage of total, RO: Religious officials.
5, 6, 7, 8, 9 items of the ATV scale are opposite items. The scores of the opposite items were translated before analysis.
1. I want my family to have the vaccine to be developed / developed for this disease.
2. I want to have the vaccine to be developed / developed for this disease as much as possible.
3. I think everybody should have the vaccine to be developed / developed for this disease.
4. I trust to explanations made for the vaccine to be developed/developed.
5. The vaccine to be developed / developed may cause spread of the disease.
6. I think the vaccine to be developed / developed will not / does not have a protective effect.
7. The vaccine to be developed / developed is dangerous.
8. I think the effectiveness of the vaccine to be developed / developed will not be/has not been tested adequately.
9. I think I may survive the epidemic without a vaccine.
2.3Data analysis
The data were analyzed using SPSS Statistics Pack version 22.0 (IBM, Armonk, NY). In line with the characteristics of the variables, percentage, mean±standard deviation, Wilcoxon, Mann Whitney U, and chi-square tests were performed. Kruskal Wallis H test was used for comparison between more than two independent groups, and then Dunn- Bonferroni post hoc test was used for binary comparisons to determine which group originated the difference. Statistical significance was accepted as p < 0.05.
3Results
The majority of the participants were men and married. Most of the participants (89.1%) had at least one dose of COVID-19 vaccine. Most participants (92.0%) had received childhood immunizations according to the national immunization schedule (Table 1).
BEK, AEK, BEATV, and AEATV scores were compared with regard to marital status, having children, and occupation. There was no difference in marital status (BEK p = 0.543, AEK p = 0.158, BEATV p = 0.173, AEATV p = 0.078, Kruskal Wallis). There was no difference in having a child (BEK p = 0.827, AEK p = 0.859, BEATV p = 0.714, AEATV p = 0.581, Mann Whitney U). There was no difference in BEK scores according to occupation (p = 0.999). However, teachers had higher mean ranks in AEK (p = 0.036), BEATV (p = 0.033), AEATV (p = 0.004) (Kruskal Wallis, post hoc Dunn Bonferroni).
After the training, the number of people who answered “yes” to the question “Would you recommend the COVID-19 vaccine to the people around you?” increased. The number of correct answers to all knowledge questions also increased (Table 2).
Table 2
Comparison of the answers to the knowledge questions before and after the training
| BE % (n) | AE % (n) | p | ||
| Vaccination offer | Yes | 59,3 (163) | 64,0 (176) | <0,001* |
| No | 20,7 (57) | 16,4 (45) | ||
| I don’t know | 20,0 (55) | 19,6 (54) | ||
| Protective (Q1) | Correct | 73,1 (201) | 77,1 (212) | <0,001* |
| False | 5,1 (14) | 4,0 (11) | ||
| I don’t know | 21,8 (60) | 18,9 (52) | ||
| Safe (Q2) | Correct | 54,5 (150) | 67,4 (178) | <0,001* |
| False | 6,9 (19) | 5,8 (16) | ||
| I don’t know | 38,5 (106) | 29,5 (81) | ||
| Suspicious (Q3) | Correct | 22,9 (63) | 38,9 (107) | <0,001* |
| False | 33,1 (91) | 22,2 (61) | ||
| I don’t know | 44,0 (121) | 38,9 (107) | ||
| Safety pregnant (Q4) | Correct | 27,6 (76) | 43,3 (119) | <0,001* |
| False | 10,2 (28) | 8,0 (22) | ||
| I don’t know | 62,2 (171) | 48,7 (134) | ||
| Hygiene after vaccination (Q5) | Correct | 89,8 (247) | 93,5 (257) | <0,001* |
| False | 4,4 (12) | 4,0 (11) | ||
| I don’t know | 5,8 (16) | 2,5 (7) | ||
| Total correct answers | MR | 49,41 | 66,14 | <0,001** |
| Mean±SD | 2,68±1,467 | 3,17±1,530 |
*Chi square test, **Wilcoxon test, Q: Question.
After the training, there was a positive increase in most of the ATV items (Table 3).
Table 3
Comparison of the ATV items before and after the training
| BE | AE | Z | p* | |||
| Attitude | MR | Mean±SD | MR | Mean±SD | ||
| 1 | 27,02 | 3,71±1,403 | 41,86 | 3,91±1,229 | –3,551 | <0,001 |
| 2 | 29,36 | 3,62±1,357 | 39,44 | 3,83±1,210 | –4,040 | <0,001 |
| 3 | 31,90 | 3,77±1,325 | 35,66 | 3,93±1,191 | –3,177 | 0,001 |
| 4 | 34,76 | 3,46±1,288 | 44,76 | 3,73±1,196 | –5,248 | <0,001 |
| 5 | 52,12 | 3,80±1,099 | 54,55 | 3,96±1,078 | –,101 | 0,019 |
| 6 | 49,87 | 3,90±1,064 | 50,08 | 4,02±1,021 | –,589 | 0,056 |
| 7 | 45,86 | 3,94±1,014 | 46,10 | 4,02±0,968 | –1,650 | 0,144 |
| 8 | 57,68 | 3,57±1,240 | 59,52 | 3,87±1,095 | –1,603 | <0,001 |
| 9 | 55,45 | 3,61±1,262 | 57,92 | 3,81±1,179 | –,147 | 0,009 |
| Total | 81,31 | 33,38±7,678 | 105,42 | 35,19±7,394 | –1,696 | <0,001 |
*Wilcoxon test.
There was a statistically significant increase in the number of correct answers (p < 0.001) and ATV total score (p < 0.001) of teachers. There was an increase in the number of correct answers and ATV total score of PETs. Although the increase in the number of correct answers was not statistically significant (p = 0.205) and increase in the ATV total score was statistically significant (p = 0.001). In addition, there was a statistically significant increase in the number of correct answers (p < 0.001) and ATV total score (p = 0.001) of religious officials (Wilcoxon test). Change through the training in the number of correct answers and total attitude scores according to occupations is given in Fig. 1. A positive correlation was found between age and BEK, AEK, BEATV, AEATV (Table 4).
Fig.1
Change of number of correct answers and total attitude scores according to occupations with education.
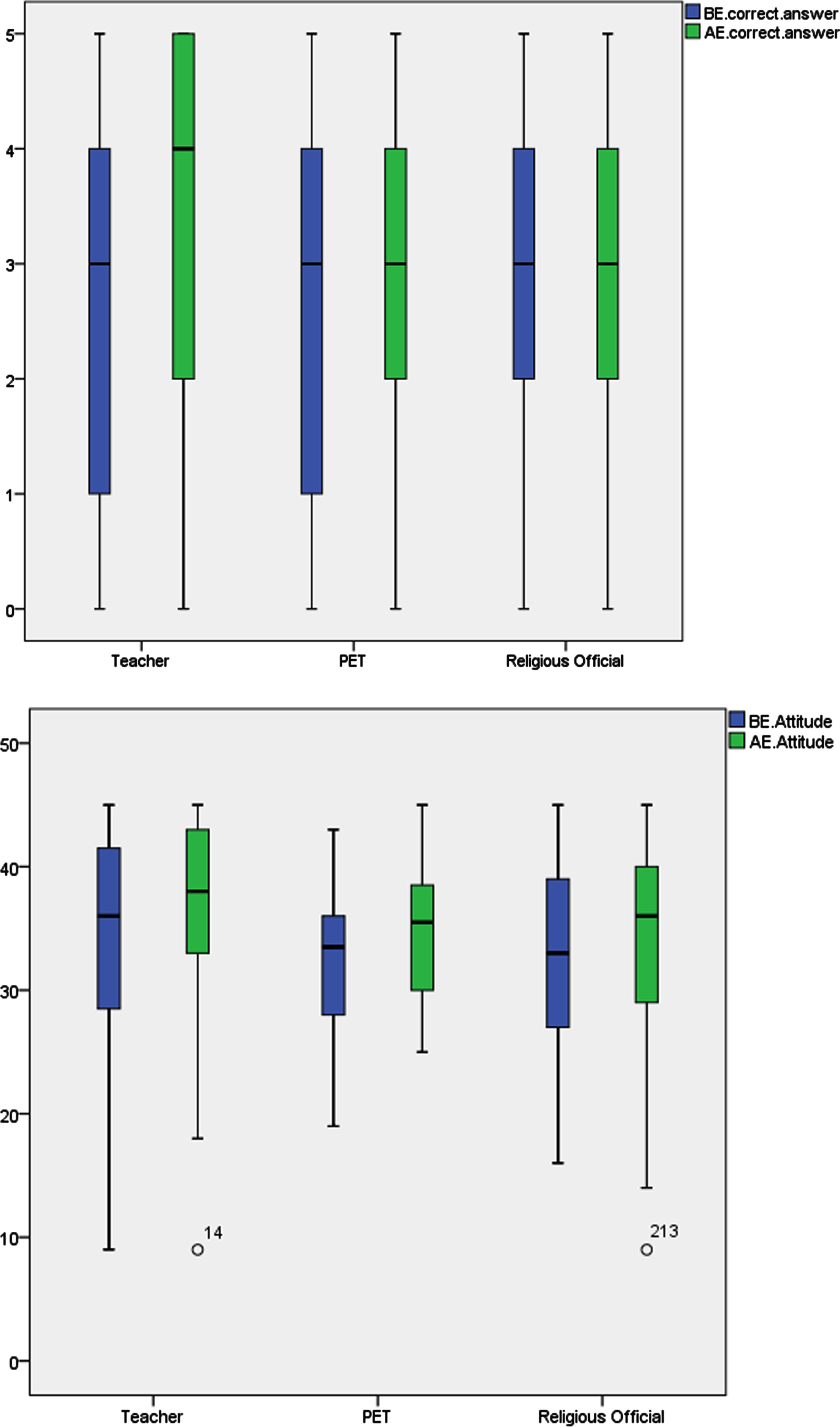
Table 4
Correlation of BEC, AEC, BEATV, AEATV and age (Spearman correlation)
| BEC | AEC | BEATV | AEATV | Age | ||||||
| p | r | p | r | p | r | p | R | P | r | |
| BEC | 1 | |||||||||
| AEC | ,000 | ,680** | ||||||||
| BEATV | ,000 | ,544** | ,000 | ,501** | ||||||
| AEATV | ,000 | ,491** | ,000 | ,525** | ,000 | ,811** | 1 | |||
| Age | ,002 | ,190** | ,004 | ,175** | ,034 | ,128* | ,033 | ,129* | 1 | |
*Correlation is significant at the 0.05 level (2-tailed). **Correlation is significant at the 0.01 level (2-tailed).
4Discussion
Affecting public health, the COVID-19 pandemic caused an increase in mortality and morbidity as well as economic difficulties due to illness and quarantine periods of employees. The vaccine, which is often considered to be one of the most important weapons in the combat of the epidemic, has not received adequate attention. In a study consisting of 19 countries, current levels of willingness to accept a COVID-19 vaccine were found to be insufficient to meet herd immunity requirements in the majority of countries. It was recommended that in order to increase trust among the population, the elements that define and build trust should be understood and interventions should be made accordingly. The ongoing pandemic offers the public health community an important opportunity to support general immunization programs for all vaccine-preventable diseases, as well as to develop vaccine literacy and confidence to support the uptake of COVID-19 vaccines [1]. Inadequate knowledge often leads to a reduction of safe health behaviors, which may adversely affect the preparedness to meet the problems that threaten societies. The effect of pandemic events like COVID-19 are often intense and may completely affect the life of the population [10]. Also, the evidence clearly shows that COVID-19 had an immense impact on the health and welfare of teachers [11].
Our intervention study aimed to create a butterfly effect by providing training on COVID-19 vaccines to occupational groups who have the potential to influence many people in the society. Educators can influence the people around them because teachers and religious officials are considered important by society. Lack of knowledge and religious inconveniences are two important reasons for vaccine refusal, and can be overcome more easily with the participation of teachers, PETs, and religious officials [12, 13].
There was an increase in the total number of correct knowledge answers leading to more positive attitude towards being vaccinated against COVID-19 and the total ATV score increased after the training. These results are expected to increase the rate of vaccination because better awareness of the COVID-19 vaccine is associated with a reduction in hesitancy [14]. Concern about vaccine side effects and lack of information about the effectiveness of vaccines are the most common reasons for vaccine rejection [10]. The training content in the present study included these topics, which the authors believe to be a good step towards reducing vaccine rejection [15].
Teachers, PETs and religious officials volunteered to participate in the training. The necessary permissions were obtained from the local authorities. Majority of the participants were male. Religious officials were the majority of participants. In previous studies, the rate of elderly people stating that they would be vaccinated was found to be higher [1]; although in this study, a positive correlation was determined between age and BEK, AEK, BEATV, AEATV.
This study has some limitations. The results reflect the participating groups and cannot be generalized to the whole population. In addition, the data obtained is limited to the statements of the participants.
5Conclusion
Widespread public acceptance of the COVID-19 vaccine is an important part of controlling the COVID-19 pandemic. Developing strategies to reduce public hesitancy and to increase confidence is vital for the implementation of vaccination programs. It is anticipated that the impact of an intervention to change the attitude of educators will be reflected on the attitudes of the greater society.
Ethical approval
The study was approved by the Fırat University Rectorate Non-Interventional Research Ethics Committee (approval no. 2021/12-41 dated 18.11.2021).
Informed consent
Informed consent was assumed on completion and submission of the questionnaire.
Conflict of interest
The authors have no conflicts of interest to declare.
Funding
None to report.
Acknowledgments
The authors would like to thank Batuhan Selvi for his contribution to the translation and editing process of this article.
Author contributions
Conceptualization: KT, EP, İB, Nİ. Data curation: İB, Nİ. Formal analysis: KT. Methodology: EP, KT. Visualization: KT. Writing–original draft: KT. Writing–review and editing: KT, EP, İB, Nİ.
References
[1] | Lazarus JV , Ratzan SC , Palayew A , Gostin LO , Larson HJ , Rabin K , et al. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. (2021) ;27: (2):225–8. |
[2] | Polack FP , Thomas SJ , Kitchin N , Absalon J , Gurtman A , Lockhart S , et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. The New England Journal of Medicine. (2020) ;383: (27):2603–15. |
[3] | Knoll MD , Wonodi C . Oxford-AstraZeneca COVID-19 vaccine efficacy. Lancet. (2021) ;397: (10269):72–4. |
[4] | Tarawneh O , Tarawneh H . Immune thrombocytopenia in a 22-year-old post COVID-19 vaccine. American Journal of Hematology. (2021) ;96: (5):E133–e4. |
[5] | Franchini M , Liumbruno GM , Pezzo M . COVID-19 vaccine-associated immune thrombosis and thrombocytopenia (VITT): Diagnostic and therapeutic recommendations for a new syndrome. European Journal of Haematology. (2021) ;107: (2):173–80. |
[6] | Fadda M , Albanese E , Suggs LS . When a COVID-19 vaccine is ready, will we all be ready for it? International Journal of Public Health ((2020) ;65: (6):711–2. |
[7] | MacDonald Noni E . Vaccine hesitancy: Definition, scope and determinants. Vaccine. (2015) ;33: (34):4161–4. |
[8] | Geniş B , Gürhan N , Koç M , Geniş Ç , Şirin B , Çırakoğlu OC , et al. Development of perception and attitude scales related with COVID-19 pandemia. Pearson Journal of Social Sciences-Humanities. (2020) ;5: (7):306–28. |
[9] | Uslu Demir Y , Yılmaz E , Altun U . Evaluation of Health Management and Human Resources Management Students’ Perceptions and Attitudes towards the Control and Vaccine of COVID-19. Gümüşhane University Journal of Health Sciences. (2021) ;10: (3):383–97. |
[10] | Zandian H , Sarailoo M , Dargahi S , Gholizadeh H , Dargahi A , Vosoughi M . Evaluation of knowledge and health behavior of University of Medical Sciences students about the prevention of COVID-19. Work. (2021) ;68: (3):543–9. |
[11] | Kotowski SE , Davis KG , Barratt CL . Teachers feeling the burden of COVID- Impact on well-being, stress, and burnout. Work. (2022) ;71: (2):407–15. |
[12] | Quinn SC , Parmer J , Freimuth VS , Hilyard KM , Musa D , Kim KH . Exploring communication, trust in government, and vaccination intention later in the H1N1 pandemic: results of a national survey. Biosecurity and Bioterrorism: Biodefense Strategy, Practice, and Science. (2013) ;11: (2):96–106. |
[13] | Shore DA . Communicating in times of uncertainty: the need for trust. Journal of Health Communication. (2003) ;8 Suppl 1: :13–4. |
[14] | Yigit M , Ozkaya-Parlakay A , Senel E . Evaluation of COVID-19 Vaccine Refusal in Parents. The Pediatric Infectious Disease Journal. (2021) ;40: (4):e134–e6. |
[15] | Goncu Ayhan S , Oluklu D , Atalay A , Menekse Beser D , Tanacan A , Moraloglu Tekin O , et al. COVID-19 vaccine acceptance in pregnant women. International Journal of Gynaecology and Obstetrics: the Official Organ of the International Federation of Gynaecology and Obstetrics. (2021) ;154: (2):291–6. |


