
An assessment on loss of workforce due to COVID-19 among healthcare personnel: A university hospital experience
Abstract
BACKGROUND:
Healthcare personnel are among the COVID-19 risk groups. For this reason, increased absence from work affects the loss of labor.
OBJECTIVE:
This study aimed to evaluate the workforce loss amongst health personnel working in our hospital due to COVID-19 in a one-year period.
METHODS:
Workforce loss of healthcare workers was assessed via absenteeism and life expectancy. Loss of workforce for COVID-19 PCR positive or PCR negative but CT findings compatible with COVID-19 and personnel with high-risk exposure for COVID-19 were determined with absenteeism. Healthcare personnel who passed away due to COVID-19 was determined with the consideration of the retirement age and expected life years.
RESULTS:
Total lost time from work was 14635 days (excluding deaths). Loss of workforce rates resulting from COVID-19 positivity for male employees was greater in comparison to the results for females (p = 0.018). High-risk exposure of healthcare personnel working in clinical sciences was higher than those in other departments (p < 0.001). Total loss in workforce for 3 people passed away was 14 years 5 months, and total life expectancy was 64 years. Healthcare personnel under the age of 40 had less absenteeism than those over 40 years (p < 0.001).
CONCLUSIONS:
It was observed that all occupational groups working at the hospital were impacted by COVID-19. The two most important factors that influenced absenteeism were the reason for being affected (positivity and high risk) and age. Absenteeism and daily case tracing of healthcare personnel working on the frontlines will aid in both the pandemic control and management of workload for those left behind.
1Introduction
The SARS-CoV-2 virus, identified in China towards the end of 2019 and then spread to the whole world, was termed COVID-19 on February 11, 2020. A pandemic was declared on March 11, 2020 by the World Health Organization (WHO). Throughout the one-year period until March 11, 2021, 118.6 million people acquired the disease globally, as yet 2 835 989 cases, 29 290 deaths associated with COVID-19 were reported in Turkey [1, 2].
Healthcare personnel who have been at the forefront since the beginning of the outbreak are among the first ones mostly affected by the pandemic across occupational groups. A systematic review of occupational risk factors of contracting COVID-19 among healthcare personnel found that overwork, a high-stress work environment, and working on the frontlines increase the risk of infectious disease [3]. In a study assessing the risk of contracting COVID-19 for employees in England, it has been observed that healthcare personnel have a 7 times higher risk in comparison to those working in non-essential jobs during the pandemic [4]. Healthcare personnel are considered among the “very high risk” employment groups by the Occupational Safety and Health Administration (OSHA) [5]. At the 74th World Health Assembly, WHO announced that at least 115,000 healthcare personnel worldwide have died due to COVID-19 [6]. When healthcare personnel are exposed to the virus, apart from their own health, they also pose a risk to their families and colleagues with whom they share the same environment. In addition, as a result of being isolated due to suspicion of exposure or illness and of the threat they present to other healthcare personnel in their work environment, their disruptive impacts on the functioning of health system are multiplied.
Effects of the pandemic on public health may be reviewed in several aspects. Prevalence, incidence, mortality rates are often utilized to reveal the extent of the outbreak. Moreover, there are other consequences of the pandemic such as loss of workforce and decline in health. Loss of workforce may be determined in two ways including absenteeism (being away from work) and presenteeism (decrease in work efficiency). In a study conducted at the beginning of the pandemic in Italy, the total productivity loss within a 2-month period was estimated to be around 300 million Euros [7].
Although the number of cases and deaths are monitored systematically throughout the pandemic, the number of cases based on occupation is not reported. A review on the number of cases and loss of workforce across occupational groups with a high risk of exposure such as healthcare personnel may aid in the monitoring of the coronavirus outbreak as well as facilitating the control of health services, impaired due to absence from work that leads to an increase in workload and stress of other healthcare personnel.
In this study, it is aimed to determine the characteristics loss of workforce respect to COVID-19 among healthcare personnel and evaluate the absenteeism due to COVİD-19 in healthcare personnel at Istanbul University-Cerrahpasa Medical Faculty, one of the largest and tertiary level hospitals in Turkey.
2Methods
2.1Study design and participants
Health personnel with a drop in their workforce due to COVID-19 at our hospital between March 11, 2020 and March 11, 2021 were included in this cross-sectional study.
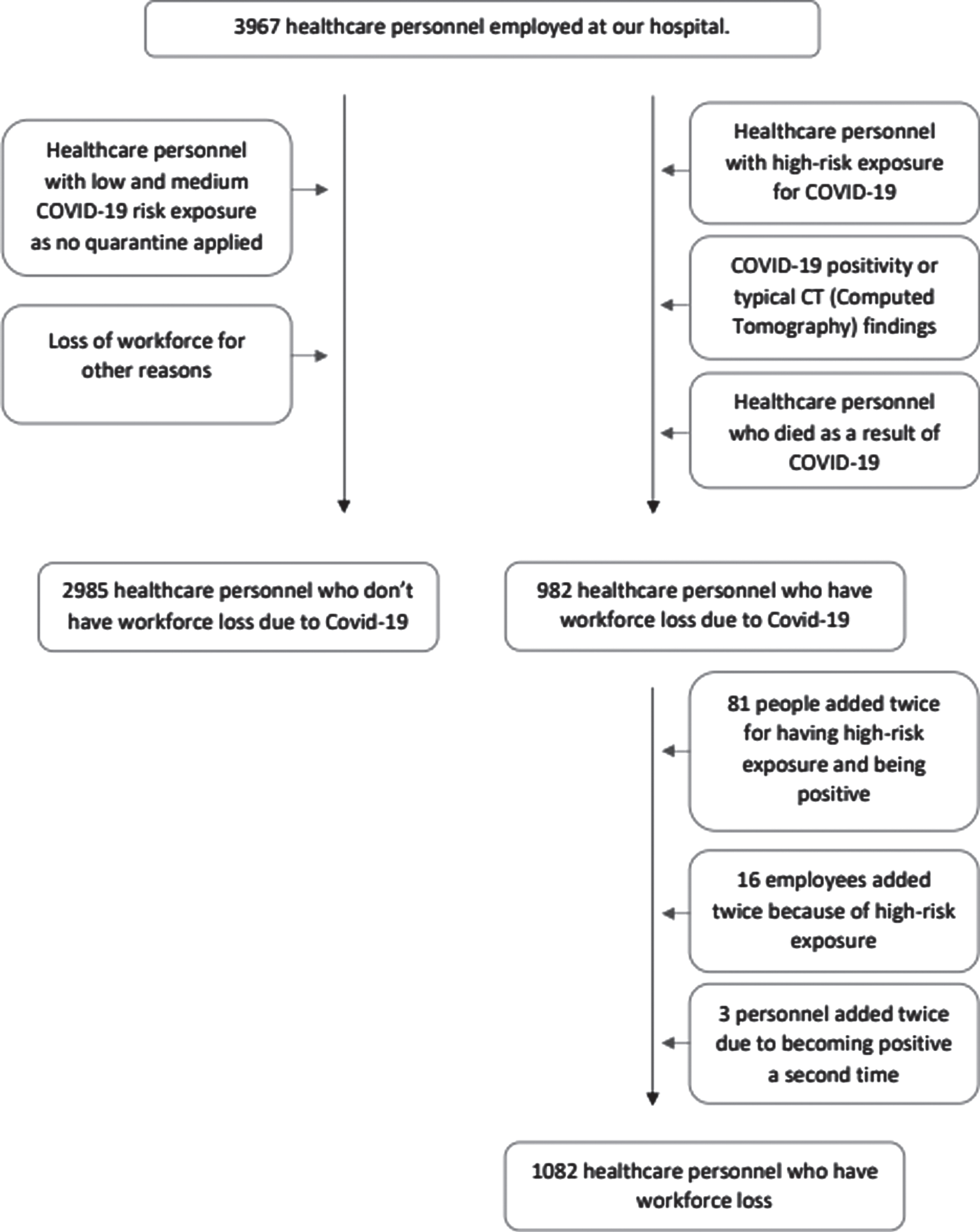
3967 healthcare personnel were employed at our hospital. They were divided in two groups: Healthcare personnel who have workforce loss due to COVID-19 and healthcare personnel who do not have workforce loss due to COVID-19.
Healthcare personnel who have workforce loss due to COVID-19 were selected based on the inclusion criteria: People with high-risk exposure for COVID-19, people with COVID-19 positivity or typical computed tomography (CT) findings, people who died as a result of COVID-19.
Exclusion criteria: Healthcare personnel with low and medium COVID-19 risk exposure as no quarantine applied, loss of workforce for other reasons, and intern doctors and nurse interns.
The data of 982 out of 3967 healthcare personnel with workforce losses resulting from COVID-19 were analyzed. 81 employees experienced absenteeism for having high-risk exposure and being positive, 16 experienced it twice because of high-risk exposure, and 3 experienced twice due to becoming positive a second time. The data pertaining to the second time of these people were evaluated as a separate case of absenteeism (Fig. 1).
Fig. 1
Selection of groups.
2.2Data collection
Workforce loss of healthcare personnel was assessed via absenteeism and life expectancy. Absenteeism was calculated as number of days employees were away from work. The dates of quarantine onset and return to work were documented for patients with COVID-19 polymerase chain reaction (PCR) positive or PCR negative but CT findings compatible with COVID-19 and for those with high-risk exposure for COVID-19, and absenteeism was analyzed based on these data.
The quarantine period according to the current guidelines of the Ministry of Health was applied to the personnel with COVID-19 PCR+ or PCR- but typical chest CT findings (peripheral, bilateral or multifocal round glass opacity). For employees with asymptomatic or mild symptoms, isolation was terminated following a negative PCR test result one day prior to the end of the quarantine. With regards to health personnel with moderate or severe symptoms, a decision for return to work or extension of medical leave was made after the assessment of infectious disease and pulmonary disease specialists.
An outpatient exposure evaluation clinic for healthcare personnel was established at our university and an assessment of the presenting healthcare personnel was carried out with respect to COVID-19 exposure. Personnel with high-risk exposure was recognized as intense exposure of a healthcare personnel who did not comply with the mask and distance rules with the patient or a positive case within the household. Current exposure procedures of CDC (Centers for Disease Control and Prevention) and Department of Health were applied in this review [8, 9]. The quarantine of the healthcare personnel with COVID-19 exposure evaluation demonstrating high risk was initiated from the date of exposure in association with the relevant guidelines. If the oropharyngeal and nasal swap samples obtained throughout the quarantine period were negative and no symptoms developed during the isolation, the quarantine was terminated. Absenteeism rate was calculated as the percentage of absent days per personnel [10].
Loss of workforce for healthcare personnel who passed away due to COVID-19 was determined with the consideration of employment periods up to 65 years of age, the retirement age in Turkey, and life expectancy. Life expectancy by age was based on the 2019 data of Turkish Statistical Institute (TURKSTAT). TURKSTAT annually publishes life tables according to gender and age [11].
Ethics committee approval for our research, dated 08.04.2021 and numbered 70417, was obtained from the Istanbul University-Cerrahpasa Medical Faculty Clinical Research Ethics Committee.
2.3Statistical analysis
SPSS v.21 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Kolmogrov Smirnov tests, histograms and probability plots were utilized for assessing normality. Continuous variables were demonstrated with the use of mean±standard deviation and median (25–75. QR). Categorical variables were expressed via frequency and percentage and comparisons of categorical variables were made using Chi-square test. Comparisons of the groups for continuous variables were made using Mann-Whitney U test for two groups and Kruskal-Wallis test for three and more groups. Whilst investigating the effects of age and other variables on the period of absenteeism, age was identified as a covariate and analyzed utilizing the univariate general linear model. All tests are two-sided and significance level was accepted as p < 0.05.
3Results
Total absenteeism 14 635 days (excluding deaths), 13,5 days per person in healthcare personnel who have workforce loss and 3,7 days per person in all personnel. We found absenteeism rate was % 1,4.
3.1Characteristics of the patients
733 (17.6%) personnel due to COVID-19 positivity, 346 (8.3%) employees as a result of high-risk exposure were quarantined and 3 (0.7%) healthcare personnel died because of COVID-19. The weekly distribution regarding the number of COVID-19 cases in Turkey and at our hospital is provided in Fig. 2. It was observed that it showed similar trends with the total number of patients in our country. 24.8% of women and 28.8% of men experienced loss of workforce due to COVID-19. Loss of workforce rates resulting from COVID-19 positivity for male employees was greater in comparison to the results for females (p = 0.018). The mean age was 38.1±10.6, absenteeism was most commonly noted in the 30–39 age group with a rate of 30.2%. Total lost time from work was 14 635 days (excluding deaths), with a mean of 13.6±8.7. 22.8% of those working in basic sciences, 43.7% of those in clinical medicine, 17.5% of surgical departments, 18.6% of administrative departments experienced workforce loss in the workplace. Personnel with high risk exposure working in clinical sciences was higher than those in other departments (p < 0.001) (Table 1). Total loss in workforce for 3 people passed away was 14 years 5 months, and total life expectancy was 64 years (Table 2).
Fig. 2
Weekly cases at Cerrahpasa Medical Faculty and in Turkey-one year experience.
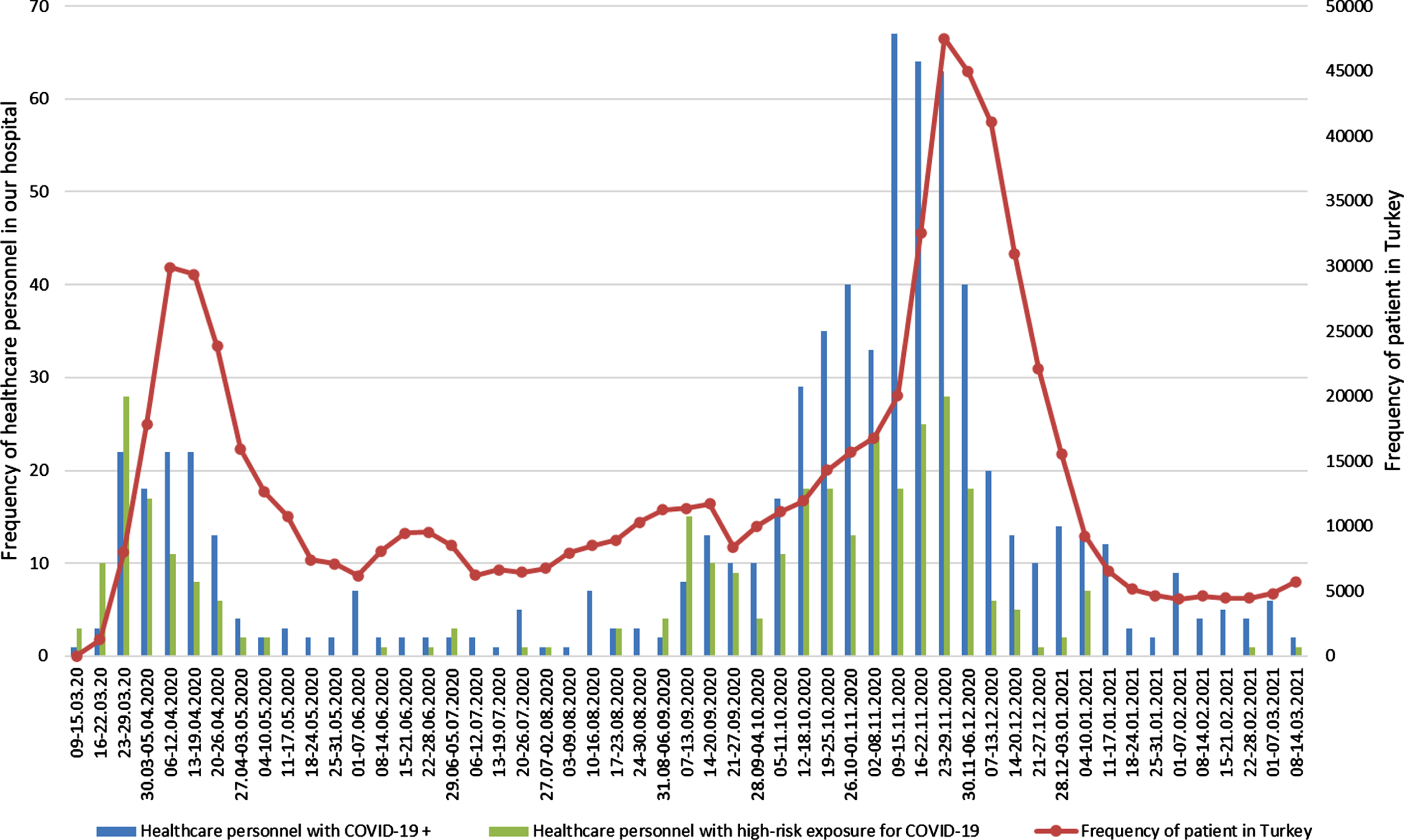
Table 1
Comparison of demographic characteristics concerning all personnel registered in the hospital according to COVID-19 status
| Categories | Healthcare personnel who do not have workforce loss n (%)(2985) | Cause of workforce loss in healthcare personnel n (%) | p1 | |
| COVID-19 positive (736) | High risk exposure (346) | |||
| Sex | ||||
| Female | 1723 (75,2%)a | 388 (16,9)a | 182 (7,9)a | 0,018 |
| Male | 1262 (71,2%)b | 348 (19,5)b | 164 (9,3)a | |
| Age | ||||
| 20–29 | 803 (74,2%)a,b | 202 (18,7)a | 77 (7,1)a | 0,014 |
| 30–39 | 829 (69,8%)b | 241 (20,3)a | 118 (9,9)a | |
| 40–49 | 795 (74,9%)a | 175 (16,5)a | 91 (8,6)a | |
| ≥50 | 558 (75,8%)a | 118 (15,7)a | 60 (8,2)a | |
| Department | ||||
| Basic Sciences | 223 (77,2%)a | 51 (16,8)a | 15 (5,2)a,b | <0,001 |
| Clinical Medicine | 737 (56,3%)b | 351 (26,8)b | 221 (16,9)c | |
| Surgery | 1157 (82,5%)a | 212 (16,9)a | 34 (2,4)b | |
| Administrative | 867 (81,4%)a | 122 (11,5)a | 76 (7,1)a | |
| Professions | ||||
| Academic personnel (Professor, Assoc. Professor, Physicians) | 314 (82%)a | 60 (15,4%)a,b | 10 (2,6%)a | <0,001 |
| Residents | 327 (64,6%)b | 138 (27,3%)c | 41 (8,1%)b,c,d | |
| Nurses | 675 (71,4%)b,c | 198 (20,9%)b,c | 73 (7,7%)d | |
| Health care technician | 324 (79,6%)a | 49 (11,9%)a | 34 (8,4%)b,c,d | |
| Administrative staff | 391 (70,7%)b,c | 86 (15,6%)a,b | 76 (13,7%)c | |
| Others (Cafeteria, Cleaning, Security personnel etc.) | 954 (75,1%)a,c | 205 (16,1%)a | 112 (8,8%)b,d | |
1Chi-square test In group analysis; Each superscript letter denotes a subset of categories whose row value do not differ significantly from each other at the, 05 level. The data pertaining to the second time of people were evaluated as a separate case of absenteeism.
Table 2
Characteristics and workforce loss of patients who died due to COVID-19
| Death number | Age | Sex | Workforce loss | Expected life years |
| 1 | 57 | Male | 7 years 11 months | 22,5 |
| 2 | 61 | Male | 4 years 1 month | 19,3 |
| 3 | 63 | Female | 2 years 5 months | 22,2 |
3.2Differences in characteristics of the participants with absenteeism
The mean for absenteeism in males was greater compared to that for females (p = 0.021). Healthcare personnel who under the age of 40 had less absenteeism than those aged over 40 years (p < 0.001). The personnel employed within clinical departments had lower absenteeism than that of other departments (p < 0.001). The mean for absenteeism in academic staff was higher with respect to nurses and residents (p = 0.003). The absenteeism of healthcare personnel suffering from COVID-19 was greater than those with high risk exposure (p < 0.001). Using age as a covariate, no significant difference was detected between gender, employment unit and assigned duty via the general linear model analysis of univariate, the difference associated with the cause of absenteeism remained the same (Table 3).
Table 3
Comparison of absenteeism among demographic characteristic
| Categories | Absenteeism (day) | p | p | |
| Mean± Standard Deviation | Median (25 –75. QR) | |||
| Sex | ||||
| Femalea | 13,3±9,6 | 12 (9–15) | 0,0211 | 0,9763 |
| Maleb | 13,8±7,7 | 13 (10–15) | ||
| Age | ||||
| 20–29a | 12±5,2 | 11 (10–14) | <0,0012 | |
| 30–39a | 12,5±7 | 12 (9–14) | ||
| 40–49b | 14,7±10,5 | 13 (10–16) | ||
| ≥50b | 16,5±12 | 14 (10–19) | ||
| Department | ||||
| Basic Sciencesa | 13,9±6,3 | 13 (10–18) | <0,0012 | 0,6193 |
| Clinical Medicineb | 12,3±9 | 11 (7–14) | ||
| Surgerya | 15,6±8,2 | 13 (11–18) | ||
| Administrativea | 14,5±8,7 | 13 (10–16) | ||
| Profession | ||||
| Academic personnel (Professor, Assoc. Professor, Physicians)a | 15,1±7,3 | 14 (11–18) | ||
| Residentsb | 11,5±4,3 | 11 (10–14) | 0,0032 | 0,5743 |
| Nursesb | 13,8±9,7 | 12 (9–16) | ||
| Health care techniciana,b | 13,5±7,1 | 13 (8,75–16) | ||
| Administrative staff a,b | 14,2±9,4 | 13 (9–15) | ||
| Others (Cafeteria, Cleaning, Security personnel etc.)a,b | 13,9±9,8 | 13 (10–15) | ||
| Cause of workforce loss | ||||
| COVID-19 positivea | 15,8±9,4 | 13 (11–18) | <0,0012 | <0,0013 |
| High risk exposureb | 8,9±4,2 | 7 (6–13) | ||
1Mann Whitney U test, 2Kruskal Wallis test, 3Univariate general linear model (with age as a covariate). In group analysis; Each superscript letter denotes a subset of categories whose row value do not differ significantly from each other at the, 05 level.
4Discussion
Our study recorded the absenteeism of healthcare personnel related to COVID-19 daily and conducted a review. The overall absenteeism for one year was revealed to be 14,635 days, the total loss of workforce for employees who died was 14 years and 5 months, and the total life expectancy in years was 64. In our study, it was found that age and the cause of absenteeism due to COVID-19 had an impact on absenteeism.
In a study examining 3,398 healthcare personnel with occupational exposure to COVID-19, the risk of becoming COVID-19 positive was 1.82 times higher in males in comparison to females [12]. In another study investigating the prevalence of IgG antibodies against SARS-CoV-2 in healthcare personnel at a health institution, 6.4% of women and 6.9% of men were identified to have positive anti-SARS-CoV-2 IgG antibodies hence no significant difference was demonstrated between genders [13]. Likewise, in our study, COVID-19 positivity was higher in men than in women.
On the review of a study comparing the number of days on medical leave for more than 1,651,305 Spanish workers during the first 3 months of 2020 with those in the first 3 months of previous years, it was noted that diseases of the respiratory system were on the rise in 2020 but there was no difference between genders [14]. Looking into the estimates on 28 April 2020 for disease burden associated with COVID-19 in Italy, it was calculated as 82,020 DALYs for men and 39,429 DALYs for women. Total YLL was demonstrated to be 81,718 in males, 39,096 in females as total YLD was 302 in men and 333 in women [7]. Also in our study, days of absenteeism for male employees were more than female ones yet using age as a covariate, no difference was found between days of absenteeism.
In a study conducted in Korea between the 20th of January 2020 and 24th of April 2020 with a total of 10,708 COVID-19 cases, including 4,323 men and 6,385 women, years of life lost (YLLs) due to premature death were higher in males compared to females [15]. The gender of 2 out of 3 deaths occurring due to COVID-19 at our hospital was male. The total workforce loss of 3 people who passed away was 14 years 5 months, total life expectancy was 64 years.
Reviewing a study that included 9,282 COVID-19 positive healthcare personnel between February 12 and April 9, 2020, in the United States, 55% of patients were aged between 16 to 44 years, 21% aged 45 to 54 years, and 18% aged 55 to 64 years, 6% aged 65 years and older. In addition, the study mentioned the observation of 27 deaths; deaths occurred most frequently in healthcare personnel aged ≥65 years [16]. As for our hospital, the ages of 3 employees who died were 57, 61 and 63 years.
In a study exploring the prevalence of IgG antibodies against SARS-CoV-2 among healthcare personnel in a health facility, the overall prevalence for presence of anti-SARS-CoV-2 IgG antibodies was identified to be 6.6% (95% CI: 5.8–7.3). According to the age group, with the prevalence varying between 5.2% (95% CI: 3.5–7.0) in the 60–64 age group and 10.8% (95% CI: 2.5–19.1) in the group aged 65 and over, it was revealed that there was no significant difference based on age group [13]. In our study, absenteeism was observed most frequently in the 30–39 age group with a rate of 30.2%. Furthermore, we established that the absenteeism of healthcare personnel under the age of 40 was less in comparison to the ones aged 40 years or older.
In consideration of a study performed on healthcare staff, occupational exposure to COVID-19 was detected to be highest among nursing staff (n = 1705; 50.2%). Hospitalization and absenteeism were shown to be more common in healthcare personnel with high-risk exposure in the same study [12]. As for a study conducted in Greece analyzing the cost associated with COVID-19 in healthcare personnel, it was demonstrated that most cases consisted of doctors followed by nurses [17]. Similarly, in our study, resident doctors had the highest exposure rates to COVID-19. Yet, the average absenteeism of academic staff was higher compared to residents and nurses.
Looking into a study done in China, it was indicated that personnel working in surgical branches, intensive care units and departments that intervene in the respiratory tract have a higher risk with regards to COVID-19 [18]. Also in our study, exposure to COVID-19 in clinical sciences was higher than that of other branches, but the duration of absenteeism was lower than the others.
According to CDC and Ministry of Health guidelines, the isolation duration of COVID-19 positivity is longer compared to the quarantine period due to high risk for COVID-19 [8, 9]. Likewise, in the study conducted in Greece performing cost analysis on healthcare personnel, the mean absenteeism of COVID-19 positive personnel was higher than that of the employees exposed to COVID-19 [17]. Similarly, in our study, the absenteeism of COVID-19 positive healthcare personnel was recognized to be more than the personnel with high-risk exposure.
In our study, we found % 1,4 absenteeism rate. The reason why 1.4% was found to be low may be due to the fact that the personnel working in our hospital are mostly young. 1.4% may be an acceptable rate, but absenteeism has not been experienced due to COVID-19 in previous years and we still do not know how COVID-19 affects presenteeism.
4.1Limitations
This study only evaluated the personnel in terms of number of days and an analysis for presenteeism was not performed, which is another important criterion for workforce loss. As the study was carried out in a single center, with the number of deaths at the hospital, we could not complexly prove the impact of COVID-19 on healthcare personnel deaths. Furthermore, we did not evaluate increased workload loss of the personnel who continued to work in the hospital. Future research on this topic may be valuable in showing the importance of workforce loss due to COVID-19.
4.2Strengths
All healthcare personnel at the university were monitored daily from the date of the first case in Turkey. Also, the study was conducted at one of the largest and well-established hospitals of the country.
5Conclusion
Our study is one of the few studies that assesses loss of workforce in healthcare personnel due to COVID-19. The two most important factors having an influence on absenteeism were shown as the reason for being affected (positivity and high risk) and age. Total absenteeism was 14 635 days and 13,5 days per person in healthcare personnel who have workforce loss and 3,7 days per person in all personnel and absenteeism rate was % 1,4.
In our study, it was observed that all occupational groups working at the hospital were impacted by COVID-19. Healthcare personnel are among the first ones to be affected by COVID-19 across the employment groups. The workforce loss experienced may have an effect both on the individual and the other employees as well as workplace operations because total absenteeism was 14 635 days. Absenteeism and daily case tracing of healthcare personnel working on the frontlines will aid in both pandemic control and management of workload for those left behind. Considering the existence of the COVID-19 pandemic in the upcoming years, detection and tracing the effect of the disease on the workforce is critical. This helps to take required precautions regarding workforce loss and maintain the proper working of all healthcare services.
COVID-19 is still not counted as an occupational disease in some countries, including our country. Our study draws attention to the devastating effects of COVID-19 in healthcare personnel from a different perspective.
In further studies, calculating the financial loss of workforce and comparing it with previous years may assist in evaluation of the economic losses related to COVID-19, and its comparison with other occupational groups may also assess the extent of workforce loss in healthcare personnel.
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no external funding.
Ethical approval
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of Istanbul University-Cerrahpasa, Cerrahpasa Faculty of Medicine (protocol code 70417, date 8 April 2021). Permission was obtained from the Republic of Turkey Ministry of Health and faculty administration for the use of patient data in the study.
Informed consent
Since the data of the personnel registered in the hospital were evaluated retrospectively, informed consent was not required.
Acknowledgments
The authors would like to thank the staff of the Cerrahpasa Faculty of Medicine for their devoted work throughout the pandemic.
References
[1] | WHO Coronavirus (COVID-19) Dashboard [homepage on the Internet]. COVID19.who.int; 2021 [cited 16 March 2021]. Available from: https://COVID19.who.int/. |
[2] | T.C. Sağlık Bakanlığı COVID-19 Bilgilendirme Platformu [homepage on the Internet]. T.C. Sağlık Bakanlığı; [cited 16 March]. Available from: 2021. https://COVID19.saglik.gov.tr. |
[3] | Jin H , Chen Y , Fu Q , Qu Q . Occupational risk factors of contracting COVID-19 among health workers: A systematic review. Work. (2021) ;69: :721–34. |
[4] | Van der Plaat DA , Madan I , Coggon D , van Tongeren M , Edge R , Muiry R , et al. Risks of COVID-19 by occupation in NHS workers in England. Occup Environ Med. 2021. |
[5] | COVİD-19/ Hazard Recognition [homepage on the Internet]. Occupational Safety & Health Administra- tion. 2021 [cited 19 September 2021]. Available from: https://www.osha.gov/coronavirus/hazards. |
[6] | WHO/ Director-General’s opening remarks at the World Health Assembly - 24 May 2021 [homepage on the Internet] WHO, 2021 [cited 19 September 2021]. Available from: https://www.who.int/director-general/speeches/detail/director-general-s-opening->. |
[7] | Nurchis MC , Pascucci D , Sapienza M , Villani L , D’Ambrosio F , Castrini F , et al. Impact of the burden of COVID-19 in Italy: Results of disability-adjusted life years (DALYs) and productivity loss. Int J Environ Res Public Health. (2020) ;17: (12). |
[8] | CDC- Interim Guidance for Managing Healthcare Personnel with SARS-CoV-2 Infection or Exposure to SARS-CoV-2 [homepage on the Internet] CDC,2021. [cited 19 september 2021]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-risk-assesment-hchtml?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fhcp%2Fexposure-in-healthcare.html. |
[9] | T.C.Sağlık Bakanlığı- Temaslı Takibi, Salgın Yönetimi, Evde Hasta İzlemi ve Filyasyon [homepage on the Internet] T.C. Sağlık Bakanlığı;[cited 19 september]. Available from 2021 https://COVID19.saglik.gov.tr/Eklenti/40795/0/COVID-19rehberitemaslitakibievdehastaizlemivefilyasyonpdf.pdf>. |
[10] | Cohen Y , Shoval S , Faccio M , Minto R . Deploying cobots in collaborative systems: Major considerations and productivity analysis. International Journal of Production Research. 2021:1-17. |
[11] | Life Tables, 2017-2019 [homepage on the Internet], TURKSTAT, 2020. [cited 4 june 2021]. Available from: https://data.tuik.gov.tr/Bulten/Index?p=Hayat-Tablolari-2017-2019-33711. |
[12] | Maltezou HC , Dedoukou X , Tseroni M , Tsonou P , Raftopoulos V , Papadima K , et al. SARS-CoV-2 infection in healthcare personnel with high-risk occupational exposure: Evaluation of 7-Day exclusion from work policy. Clin Infect Dis. (2020) ;71: (12):3182–7. |
[13] | Gras-Valentí P , Chico-Sánchez P , Algado-Sellés N , Gimeno-Gascón MA , Mora-Muriel JG , Jiménez-Sepúlveda NJ , et al. Sero-epidemiological study of SARS-CoV-2 infection amonghealthcare personnel in a healthcare department. Enferm InfeccMicrobiol Clin. (2021) ;39: (7):319–25. |
[14] | Calvo-Bonacho E , Catalina-Romero C , Fernández-Labandera C , Fernández-Meseguer A , González-Quintela A , Martínez-Muñoz P ,et al. COVID-19 and sick leave: Ananalysis of the ibermutua cohort of over 1,651,305 spanish workersin the first trimester of 2020. Frontiers in Public Health. (2020) ;8: (590). |
[15] | Jo MW , Go DS , Kim R , Lee SW , Ock M , Kim YE , et al. The burden of disease due to COVID-19 in korea using disability-adjusted life years. J Korean Med Sci. (2020) ;35: (21):e199. |
[16] | CDC COVID-19 Response Team. Characteristics of health care personnel with COVID-19 - United States, February 12-April 9, MMWR Morb Mortal Wkly Rep (2020) ;69: (15):477–81. |
[17] | Maltezou HC , Giannouchos TV , Pavli A , Tsonou P , Dedoukou X , Tseroni M , et al. Costs associated with COVID-19 in healthcare personnel in Greece: A cost-of-illness analysis. J Hosp Infect. (2021) ;114: :126–33. |
[18] | Ran L , Chen X , Wang Y , Wu W , Zhang L , Tan X . Risk factors of healthcare workers with coronavirus disease A retrospective cohort study in a designated hospital of wuhan in China. Clinical Infectious Diseases. (2020) ;71: (16):2218–21. |


