
Work ability among employees 2–10 years beyond breast cancer diagnosis: Late treatment effects and job resources - A longitudinal study
Abstract
BACKGROUND:
The number of workers who have previously undergone a cancer treatment is increasing, and possible late treatment effects (fatigue, physical and cognitive complaints) may affect work ability.
OBJECTIVE:
The aim of the study was to investigate the impact of late treatment effects and of job resources (autonomy, supportive leadership style, and colleagues’ social support) on the future work ability of employees living 2–10 years beyond a breast cancer diagnosis.
METHODS:
Data at T1 (baseline questionnaire) and at T2 (9 months later) were collected in 2018 and 2019 (N = 287) among Dutch-speaking workers with a breast cancer diagnosis 2–10 years ago. Longitudinal regression analyses, controlling for years since diagnosis, living with cancer (recurrence or metastasis), other chronic or severe diseases, and work ability at baseline were executed.
RESULTS:
Higher levels of fatigue and cognitive complaints at baseline predicted lower future work ability. The three job resources did not predict higher future work ability, but did relate cross-sectionally with higher work ability at baseline. Autonomy negatively moderated the association between physical complaints and future work ability.
CONCLUSIONS:
Fatigue and cognitive complaints among employees 2–10 years past breast cancer diagnosis need awareness and interventions to prevent lower future work ability. Among participants with average or high levels of physical complaints, there was no difference in future work ability between medium and high autonomy. However, future work ability was remarkably lower when autonomy was low.
1Introduction
The percentage of workers living with or beyond cancer within the working population in the Netherlands is estimated to be considerable [1]. The most commonly diagnosed cancer is female breast cancer [2] and, the incidence is still rising [3]. Furthermore, because of improved survival rates the 5- and 10-year prevalence has almost doubled over the previous 20 years [4]. Moreover, the return-to-work rates have increased [5] for several reasons, such as a greater focus on returning to work. As a result, the percentage of working people who have had a breast cancer diagnosis in the past will continue to rise. Work is important for this population of workers as, 5 years following diagnosis, the quality of life of the employed is greater than that of the unemployed, although it is also possible that a decline in health triggers changes in employment status [6].
Breast cancer is not a single disease. It has many manifestations, with major differences in treatment options and prognoses. Since cancer is a life-threatening disease, possibly even in the short term, both the diagnosis and the undergoing of treatment can be regarded as a serious life event. This represents a difference from many chronic conditions, such as diabetes, or problems with the musculoskeletal system. The period after a cancer diagnosis is often unpredictable and uncertain. Nevertheless, given the high survival rates of various types of breast cancer, it is also important to realize that, for many, there is a working life after diagnosis.
However, post-cancer-diagnosis workers may experience problems, and their work ability requires attention. Several cross-sectional studies among workers more than 2 years beyond their cancer diagnoses have reported that work ability was lower for these workers compared to that of a reference group or a norm group [7–11], although not all studies indicated this result [12]. An important question remains, therefore, which factors influence the work ability of this population of workers.
As workers beyond a breast cancer diagnosis may experience complaints because of the various late effects of cancer treatments [13], it is conceivable that their work ability may be affected by these complaints. A qualitative study reported the late effects of cancer treatment to be a known potential problem in the guidance by managers or by professionals offered to employees who were working more than 2 years beyond their cancer diagnoses [14], but this issue has not been quantitatively investigated to date with a longitudinal design. As work ability is reported to be negatively related to sickness-related absences, future disability status, and withdrawal behaviors [15], it is important to preserve and enhance work ability among all working populations, and specifically among those experiencing late effects of cancer treatments.
During the reintegration process, which, in the Netherlands, normally takes place in the first 2 years after a cancer diagnosis, any necessary concrete facilities in the workplace (such as, different equipment or working in a quiet environment) are expected to have already received attention. However, less visible resources, for instance, the level of autonomy offered to an employee, may also be important and offer targets for interventions. An interview study reported that managers and professionals differ in their opinion on whether autonomy is more important for workers who experience late effects after cancer treatments than for the healthy population [14]. Across studies among general populations, however, resources within the job and the work situation are positively related to work ability [16], and this is also expected to hold true for post-cancer-diagnosis workers. Therefore, these resources are the focus of the present study in order to identify possible targets for intervention.
In summary, this longitudinal study concerns salaried female employees diagnosed with breast cancer 2–10 years ago and focuses on the impact of cancer treatment’s late effects on future work ability. Furthermore, in order to identify possible targets for intervention resources that may be available within the job and the work situation are studied. The aim is to preserve or enhance the work ability of employees confronted with the late effects of breast cancer treatments.
1.1Late effects of cancer treatment and work ability
The acute side effects of cancer treatments are well known, but less known is that several effects can last much longer or even develop after the first 2 years [13]. These late effects include 1) physical complaints [17], 2) fatigue [18–20], and 3) cognitive complaints [21]. These late effects may affect occupational functioning, such as work ability. However, studies concerning the association of the effects of cancer treatment with work ability beyond these first 2 years after cancer diagnosis are scarce and cross-sectional in nature [22].
First, regarding the physical condition of workers who have returned to work beyond or with cancer, several studies report associations with a lower work ability in relation to somatic symptoms [8], functional limitations [23], or poor self-rated health status [24]. Moreover, those with low work ability have reported a reduced level of self-rated health [25]. Among workers beyond breast cancer diagnosis, more breast and arm symptoms have been observed among respondents with a suboptimal work ability than among those with a good or excellent work ability [17]. The results among populations working with or beyond cancer can, to a certain extent, only be compared with populations who have chronic conditions or with healthy populations who have specific complaints. A lower or decreased work ability has been observed among various populations with physical chronic conditions [26, 27]. However, few studies on work ability concern specific complaints, and those types of physical complaints may not match the possible late effects of cancer treatments. Nevertheless, a study into, for instance, menopausal complaints and work ability may be relevant, as these complaints are also experienced by those who have been treated with, as in cases of hormone-sensitive breast cancer, endocrine therapy. Concerning these symptoms, a cross-sectional study among an otherwise healthy population reported lower work ability for higher levels of menopausal complaints [28]. Another example is a study reporting a positive association with work ability of self-perceived health among female Norwegian workers [29].
Second, regarding fatigue, a negative cross-sectional relationship of fatigue with work ability has been reported among workers more than 2 years past cancer diagnosis [11, 17, 25]. Additionally, several studies have reported on the relationship between fatigue and work ability among healthy populations or specific populations with chronic diseases. Examples are two cross-sectional studies that demonstrate a negative association between fatigue and work ability among nursing workers [30] or among a population with systemic sclerosis [31]. Moreover, a prospective cohort study of hospital nurses reported that the level of fatigue at baseline was a predictor of an unfavorable course of self-reported general work ability over 2 years [32].
Third, regarding cognitive complaints, a negative cross-sectional relationship with work ability has been reported among workers more than 2 years past a cancer diagnosis [17, 33–35]. These studies indicate that cognitive complaints can be associated with lower work ability among working cancer survivors. However, longitudinal studies among this population on this issue are lacking [22]. Studies regarding self-reported cognitive complaints and the longitudinal relationship with work ability among other populations with specific conditions are unknown to the authors. However, the need to investigate the effect of cognitive complaints on work ability within the working population beyond cancer diagnosis have been indicated before [36], and the cross-sectional associations of cognitive complaints with work ability among post-cancer-diagnosis populations provide an extra impetus to include this late effect in the present longitudinal study.
Overall, a higher level of fatigue or physical or cognitive complaints is expected to have a lowering effect on work ability beyond the first 2 years after a breast cancer diagnosis. Therefore, our first hypothesis (H1) is as follows:
H1: A higher level of physical complaints (H1a), fatigue (H1b), or cognitive complaints (H1c) at baseline (T1) is associated with lower future work ability (at T2).
1.2Job resources and work ability with or beyond cancer
The late effects experienced by those working with or beyond cancer treatments can be viewed as additional demands on those attempting to fulfill job requirements. It is therefore important to consider factors within the work environment that possibly preserve or even enhance work ability. These so-called job resources are part of the well-established job demands-resources (JD-R) model [37]. This model comprises the idea that job resources have a positive influence on health and motivational processes. Job resources may refer to aspects of the job that may be functional in achieving work goals, reducing job demands or stimulating personal growth, learning, and development. Job resources may be psychological, social, or organizational in nature [38].
The present study focuses on job resources in which adjustments can be made relatively quickly within the organization at the executive level. This means that the resources located at the organizational level (e.g., organizational culture or career opportunities) are not included, but job resources at the interpersonal level (e.g., supervisor and co-worker support or team climate), the organization of work (e.g., role clarity or participation in decision making), and at the level of the task (e.g., autonomy) were potential candidates for inclusion in the present study. However, a recent literature review has reported that the current knowledge regarding the associations of job resources with work ability among workers 2–10 years after cancer diagnosis and possibly experiencing the late effects of treatment, is only based on cross-sectional data. Furthermore, no information concerning the potential moderation by job resources of the possible associations between the late cancer treatment effects and work ability is available [22]. Therefore, the review could only report on the results regarding cross-sectional relationships between higher work ability and a limited set of job resources. These results concerned higher autonomy [39, 40], more social support by the supervisor [10, 11, 39, 41], and more social support by colleagues [10, 11, 39, 41–43]. As a result, the choice in the present study is to focus on autonomy, a supportive leadership style, and social support by colleagues, to investigate the influence of these job resources on work ability. Furthermore, the possible moderation by these job resources of the presumed relationship between physical complaints, fatigue, and cognitive complaints on the one side and lower work ability on the other will be examined.
First, autonomy can be described as the possibility to influence one’s work by, for instance, making autonomous decisions. Autonomy is addressed in several cross-sectional studies among workers living beyond or with cancer using related concepts, such as decision latitude [39, 40], or job control [44], both reported to be positively related with higher work ability. A lack of autonomy is associated with poor work ability among both general populations [45] and employees with chronic diseases [46]. In addition, job control has been stated to be important in enabling workers with decreased work ability to remain productive at work [47].
Second, as far as the authors are aware, the leadership style of the supervisor or manager has not been studied in relation to the work ability of those working more than 2 years after being diagnosed. However, related concepts, such as social support by supervisors and their avoidance behavior, were studied within this population of workers, indicating that male workers with a cancer diagnosis experienced lower work ability when supervisors’ avoidance behavior was higher [10]. In healthy populations, a supportive leadership style is reported to be associated with higher work ability. For instance, a supportive leadership style among others predicted higher work ability 1 year later among IT workers [48], and supervisor support has been reported to be particularly important to work ability in a cross-national examination of health care workers [49]. Moreover, among employees with chronic diseases, a supportive leadership style has been reported to be cross-sectionally associated with higher work ability [46].
Third, social support by colleagues has been investigated in several studies among workers more than 2 years past their cancer diagnoses. Both case-control [10, 11, 42] and cross-sectional studies [39, 41, 43] have indicated positive associations with work ability. Longitudinal studies are unavailable. Furthermore, female workers with a cancer diagnosis in their past experienced lower work ability if perceived avoidance behavior by colleagues was higher [10]. Social support by colleagues has also demonstrated positive associations with work ability among several healthy occupational populations of employees, such as hospital nurses [50].
To summarize, although longitudinal research data among workers more than 2 years past cancer diagnosis are scarce, a higher level of autonomy, a supportive leadership style, or social support by colleagues are expected to be associated with higher future work ability among employees 2–10 years past a breast cancer diagnosis. Hence, our second hypothesis (H2) is as follows:
H2: A higher level of autonomy (H2a), a supportive leadership style (H2b), or social support by colleagues (H2c) at baseline (T1) is associated with higher future work ability (at T2).
1.3Moderation by job resources of the association between late effects and work ability
Advice regarding the management of the late effects of cancer treatments is available among professionals involved in rehabilitation. Examples of such advice include using cognitive compensatory interventions [51] or opportunities to withdraw [14] in the case of cognitive complaints. However, the effect of job resources in a situation of higher levels of late effects of cancer treatment possibly affecting work ability is unknown. No quantitative studies are known to the authors concerning the possible moderating effects of job resources on the on the relationships of complaints (neither physically, nor mentally or cognitive) with work ability among workers past cancer diagnosis. Nevertheless, job resources are relevant factors in the guidance of workers confronted with the late effects of cancer treatments [14]. Certain job resources possibly reduce the negative impact of the late effects of cancer treatment on work ability. All in all, we expect positive moderating effects by the three aforementioned job resources of the presumed negative relationships of the late effects with work ability. In other words, we expect the job resources to have a more favorable effect on work ability with higher levels of the late effects so that the negative influence of the late effects is reduced. Hence, our third hypothesis is as follows:
H3: The relationship between physical complaints, fatigue, or cognitive complaints (late effects) at baseline (T1) and future work ability (at T2) are moderated by autonomy, a supportive leadership style or social support by colleagues at T1, such that when the job resource is high, the negative influence of the late effects on work ability is less than when the job resource is low.
Four covariates are included in the analyses. Years since diagnosis, living with cancer (recurrence or metastasis), and other chronic or severe diseases are taken into account as covariates, as these factors may influence the relationships because of differences in physical and mental burden. However, comparable studies are not known. The level of work ability level at baseline (T1) is controlled for, as it is expected that the individual level of work ability will be within a range that depends on other factors, such as age. In a recent literature review, age has been reported to demonstrate a significant (negative) relationship with work ability in the vast majority of underlying studies [52]. Because of the use of baseline work ability as a control variable, the age factor is not considered as a separate covariate.
All in all, the present study contributes to research in the field of work and cancer, being the first longitudinal study into the late effects of cancer treatment and job resources on work ability among employees who have returned to work after experiencing a breast cancer diagnosis 2 to 10 years ago. Longitudinal designs are necessary to investigate possible targets for interventions to help retain occupational life [53] and to therefore preserve or enhance work ability within this population. The present study addresses this need.
2Methods
The recruitment of the participants, the procedure used, the measuring instruments and the method to analyse the data of the participants are described below.
2.1Procedure
A survey study was carried out between June 2018 and December 2019 and included two questionnaires. The study was reviewed and approved by the Research Ethics Committee (cETO) of the Open Universiteit in the Netherlands who assessed the ethical acceptability of the study and agreed with the study design and method (reference cETO: U2018/03891/MQF).
The invitation for the first questionnaire (baseline, at T1) was addressed to workers 2 to 10 years after cancer diagnosis. Various methods and channels were used to inform (potential) participants about the study such as social media, a short video clip and a website (including the information letter with details regarding storage of the data and confidentiality). It was communicated that the questionnaire was expected to take 20 minutes to complete. No reward was promised. On the first page, before the questionnaire started, it was stated that by clicking on “Next” the respondent indicated to have read the information, to know that participation was voluntarily, that informed consent was given to collect the data during this study for scientific research and that the respondent was older than 18 years. Those who had completed this first questionnaire were approached 9 months later with the request to also complete a second questionnaire. This request was sent out by e-mail, with a reminder one month later, if necessary.
Data from workers with a past breast cancer diagnosis and with exclusively salaried employment at T1 (baseline) and at T2 (nine months after T1) were used in the present study (N = 287).
2.2Measures
The questionnaires included questions concerning demographics and information about health, treatment, and work. For the present study the data to be used were 1) physical complaints, fatigue, cognitive complaints at T1, 2) work ability at T1, and at T2, 3) autonomy, supportive leadership style, and social support by colleagues at T1, 4) years since diagnosis at T1, and living with cancer (recurrence or metastasis), and other chronic or severe diseases at T1 and at T2.
Physical complaints were measured by a question about complaints caused by ten possible conditions (no, some or many complaints, respectively 0, 1 or 2 points). These conditions were neuropathy, hormonal complaints, hot flushes, osteoporosis, heart complaints (due to cancer treatment), scar adhesions, joint pain, lymphedema, lung problems, and bowel and / or bladder problems. For the level of physical complaints, the total score (0 to 20) is used. The scale was constructed by the researchers because there was no adequate scale available to measure possible late physical effects of cancer treatments. Information from the IPSO (Stichting Psychosocial Oncology in the Netherlands) and the NFK (Dutch Federation of Cancer Patient Organizations) was used to justify the choices.
Fatigue was measured by the subjective fatigue subscale (eight items, seven-point Likert scale, 1 to 7) of the Checklist Individual Strength (CIS) [54, 55]. Examples of items are: “I feel tired”, “Physically I feel exhausted” and “I get tired quickly/soon”. The possible total score for fatigue was 8 to 56. The Cronbach’s α was 0.91.
Cognitive complaints were measured by the Cognitive Failure Questionnaire (CFQ) for subjective cognitive functioning (25 items, five-point Likert scale, 0 to 4) about the frequency of everyday cognitive errors [56]. The items are about small, everyday mistakes that everyone makes from time to time. The respondent could indicate whether this occurs or ‘never’, ‘rarely’, ‘occasionally’, ‘often’ or ‘very often’. Items are, for example: 1) reading something and shortly afterwards not remembering what you have read so that you have to read it again, 2) forgetting which street to take if you choose a route that you know well, but that you rarely used, 3) forgot appointments, 4) forgot people’s names, or 5) forgot what you came to buy in a store. The possible total score was 0 to 100. The Cronbach’s α was 0.93. In this study, the score on this scale will be referred to as cognitive complaints.
Work ability was measured by an item derived from the first item from the Work Ability Index (WAI) [57, 58]. The vast majority of the cross-sectional studies focusing on work ability among workers experiencing late effects of cancer treatments measure work ability using the first item of the WAI. The reason for this is that the complete WAI is an extensive questionnaire, while the first item is reported to have a strong correlation with the complete WAI [59]. The item used in the present study is as follows: “Work ability is the extent to which you are physically and mentally able to perform your current and future work. On a scale of 0 to 10, how many points would you rate your work ability right now? (“0” means you are currently completely unable to work)”.
Autonomy, supportive leadership style, and social support by colleagues were measured using one of the scales by Van Poppel and Kamphuis [60]. The Cronbach’s α’s at T1 for autonomy (four items, five-point Likert scale) was 0.86, for supportive leadership style (four items, five-point Likert scale) 0.93, and for social support by colleagues (five items, five-point Likert scale) 0.71. Examples of items regarding autonomy are “I can decide for myself how I approach my work” and “I can regulate my work pace myself”. Examples of items regarding a supportive leadership style are: “For questions and advice I can always contact my direct supervisor” and “In my work I receive sufficient support, advice and feedback from my direct supervisor”. Examples of items regarding social support by colleagues are: “I can ask my colleagues for advice if I can’t figure it out myself” and “I experience the mutual contact between me and my colleagues as pleasant”.
The year of diagnosis was collected using the first questionnaire, on the basis of which the number of years after cancer diagnosis was determined. In both questionnaires, the respondents indicated whether they were living with cancer (recurrence or metastasis) and whether they had other chronic or severe diseases.
2.3Participants
The numbers of employees with a breast cancer diagnosis were 461 at T1 and 287 at T2. Dropouts between T1 and T2 therefore concerned 174 of the participants at T1.
2.4Analysis
The data were analysed using SPSS software, version 25 (IBM Corporation, Armonk NY, USA) for Windows®/Apple Mac®.
Descriptives were analysed for the study sample at T2 (N = 287) and for the dropouts between T1 and T2 (N = 174). Descriptives were demographics (age, gender, and educational level) and years since diagnosis (at T1), living with cancer (recurrence or metastasis) and other chronic diseases (at T1 and at T2), physical complaints, fatigue, cognitive complaints (at T1), work ability (at T1 and at T2), type of tasks at T2, average weekly work hours and workdays at T2, autonomy, supportive leadership style, and social support by colleagues (at T1).
All hypotheses were analyzed by multivariate regression analyses, controlling for years past cancer diagnosis, living with cancer (recurrence or metastasis), other chronic or severe diseases at T2, and baseline work ability (at T1). Missings were not imputed, which could result in lower numbers of respondents to be used in analyses. Physical complaints, fatigue, cognitive complaints, autonomy, supportive leadership style and social support by colleagues were centered at their means, as unstandardized coefficient estimates will be biased particularly in moderation analyses [61]. The hypotheses were tested in seven steps; each of the four covariates in one of the first four steps, then the late effects together in the fifth step, the three job resources in the sixth step, and the interaction terms to test for moderation in the seventh step. Positive moderation by the job resources of the presumed negative relationships between the late effects and future work ability was expected. This means that the outcome of the multivariate regression concerns a significant, positive β for the interaction terms moderating these associations. In other words, we expected that the negative slope of the relationship between a late effect and future work ability across higher levels of each of the job resources will be decreased, and therefore a positive moderation effect [62] resulting in better work ability outcomes.
3Results
First, the descriptive data are presented below, followed by the results of testing the hypotheses.
3.1Descriptives
At T1 the mean age of the study sample (N = 287) was 49.7 years (SD 7.72) and the mean number of years since diagnosis was 4.5 years (SD 2.39). At T2 6% (N = 17) was living with cancer (recurrence or metastasis) and 44% (N = 125) had other chronic or severe diseases. The type of tasks performed in the current job of the study sample (N = 287) at T2 was 64% (N = 183) mainly mentally (psychologically) demanding, 8% (N = 22) mainly physically demanding and 29% (N = 82) both mentally (psychologically) and physically demanding (rounded, therefore not adding up to 100%). The participants worked an average of 27.9 hours per week spread over an average of 4.4 days.
Dropouts between T1 and T2 (N = 174) were significant younger (at 0.05 level) and reported a significant higher level of cognitive complaints (at 0.01 level). The detailed results of the analysis can be found in Table 1.
Table 1
Characteristics of participants at T2 (N = 287) and dropouts between T1 and T2 (N = 174)
| Variables at T1 | Participants at T2 N = 287 | Dropouts between T1 and T2 N = 174 |
| Age M (SD)λ | 49.7 (7.72) | 48.1 (7.30) |
| Female gender (N, %) | 287 (100%) | 174 (100%) |
| Educational level: | ||
| Elementary and secondary education | 77 (27%) | 42(24%) |
| Vocational secondary education | 52 (18%) | 46 (27%) |
| Higher education | 153 (53%) | 84 (48%) |
| Other or missing | 5 (2%) | 2 (1%) |
| Years since diagnosis (M, SD) | 4.5 (2.39) | 4.6 (2.40) |
| Living with cancer (recurrence or metastasis) (N, %) | 15 (5%) | 6 (3%) |
| Other chronic or severe diseases (N, %) | 121 (43%) | 67 (39%) |
| Physical complaints, M (SD) | 5.2 (3.82) | 5.5 (4.29) |
| (0 –20) | ||
| Fatigue, M (SD) | 34.1 (12.01) | 35.9 (12.14) |
| (8 –56) | ||
| Cognitive complaints, M (SD) μ | 39.7 (15.71) | 43.9 (16.10) |
| (0 –100) | ||
| Autonomy, M (SD) | 15.2 (3.47) | 14.9 (3.78) |
| (4 –20) | ||
| Supportive leadership style, M (SD) | 13.9 (4.23) | 14.4 (4.39) |
| (4 –20) | ||
| Social support by colleagues, M (SD) | 20.6 (2.75) | 20.6 (3.26) |
| (5 –25) | ||
| Work ability, M (SD) | 7.4 (1.66) | 7.4 (1.74) |
| (0 –10) | ||
| Variables at T2 | Participants at T2 N = 287 | |
| Living with cancer (recurrence or metastasis) (N, %) | 17 (6%) | |
| Other chronic or severe diseases (N, %) | 125 (44%) | |
| Type of tasks: | ||
| Mentally (psychologically) demanding | 183 (64%) | |
| Physically demanding | 22 (8%) | |
| Both mentally and physically demanding | 82 (29%) # | |
| Average work hours per week, M (SD) | 27.9 (9.04) | |
| Average work days per week, M (SD) | 4.4 (3.70) | |
| Work ability, M (SD) | 7.3 (1.77) | |
| (0 –10) |
Notes: M = mean, SD = standard deviation, N = number of participants. μ = significant difference between participants at T2 and the dropouts (between T1 and T2) at. 01 level. λ = significant difference between participants at T2 and the dropouts (between T1 and T2) at. 05 level. # = numbers do not add up to 100%, due to rounding.
Among the covariates the only significant bivariate correlation was observed for a higher educational level with less other chronic or severe diseases. Work ability at T1 was correlated with work ability at T2 (r = 0.558, p ≤0.01). A paired sample test resulted in no significant difference between work ability at T1 and work ability at T2. The three late effects showed low mutual correlations, and the same was observed for the job resources. The late effects were significantly correlated negatively (at the 0.01 level) with both work ability at T1, and with work ability at T2. The three job resources were significantly correlated positively (also at the 0.01 level) with both work ability at T1, and with work ability at T2. The detailed results of the analysis can be found in Table 2.
Table 2
Correlations of demographics (age, educational level), control variables (years since cancer diagnosis, living with cancer (recurrence or metastasis), other chronic or severe diseases, work ability at T1), dependent variable (work ability at T2), independent variables (physical complaints, fatigue, and cognitive complaints at T1), and autonomy, supportive leadership style or social support by colleagues at T1
| Variables (questionnaire T1 or T2) | N | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
| 1. Age (T1) | 287 | 1 | ||||||||||||
| 2. Educational level (T1) | 287 | –0.113 | 1 | |||||||||||
| 3. Years since cancer diagnosis (T1) | 287 | 0.212** | 0.066 | 1 | ||||||||||
| 4. Living with cancer (recurrence or metastasis) (T2) | 287 | –0.050 | 0.001 | 0.088 | 1 | |||||||||
| 5. Other chronic or severe diseases (T2) | 284 | 0.133* | –0.126* | –0.029 | –0.036 | 1 | ||||||||
| 6. Work ability (T1) | 287 | 0.021 | 0.073 | –0.009 | 0.112 | –0.210** | 1 | |||||||
| 7. Work ability (T2) | 287 | –0.105 | 0.108 | 0.004 | 0.104 | –0.303** | 0.558** | 1 | ||||||
| 8. Physical complaints (T1) | 287 | 0.101 | –0.065 | –0.003 | –0.001 | 0.239** | –0.277** | –0.280** | 1 | |||||
| 9. Fatigue (T1) | 287 | –0.050 | –0.196** | –0.007 | 0.006 | 0.215** | –0.530** | –0.445** | 0.350** | 1 | ||||
| 10. Cognitive complaints (T1) | 278 | –0.139* | –0.093 | 0.020 | –0.064 | 0.143* | –0.332** | –0.343** | 0.369** | 0.428** | 1 | |||
| 11. Autonomy (T1) | 280 | 0.029 | 0.135 | –0.029 | 0.020 | –0.042 | 0.306** | 0.245** | –0.082 | –0.210** | –0.143* | 1 | ||
| 12. Supportive leadership style (T1) | 270 | –0.001 | 0.011 | –0.053 | 0.043 | –0.077 | 0.359** | 0.262** | –0.104 | –0.215** | –0.188** | 0.291** | 1 | |
| 13. Social support by colleagues (T1) | 265 | –0.038 | 0.005 | –0.141* | 0.144* | –0.024 | 0.337** | 0.239** | –0.066 | –0.224** | –0.147* | 0.232** | 0.367** | 1 |
Notes: *Correlation is significant at the 0.05 level (two-tailed). **Correlation is significant at the 0.01 level (two-tailed).
3.2Hypothesis testing
The stepwise multivariate regression analyses excluded cases with missing data and resulted in N = 236. The final model explained 44% of the observed variance.
Each of the four covariates was tested in one of the first four steps. Two covariates showed a significant association with work ability at T2, namely baseline work ability at T1 (β= 0.328, p ≤0.001) and other chronic or severe diseases at T2 (β= –0.141, p≤0.05). Years since diagnosis and living with cancer (recurrence or metastasis) were not associated with work ability at T2. The detailed results of the analysis can be found in Table 3.
Table 3
Multivariate regression analyses for moderation by autonomy, supportive leadership style or social support by colleagues (at T1) of the association of physical complaints, fatigue, or cognitive complaints (at T1) with future work ability (at T2), controlled by years since diagnosis (at T1), living with cancer (recurrence or metastasis) (at T2), other chronic or severe diseases (at T2) and work ability (at T1)
| Step /Variable | F | R2 | Δ R2 | β | β | β | β | β | β |
| Step 1 | 0.103 | 0.000 | 0.000 | ||||||
| Years since diagnosis at T1 | –0.021 | –0.029 | –0.013 | –0.014 | –0.004 | 0.010 | |||
| Step 2 | 1.908 | 0.016 | 0.016 | ||||||
| Living with cancer (recurrence or metastasis) at T2 | 0.125 | 0.016 | 0.032 | 0.026 | 0.011 | ||||
| Step 3 | 7.795 | 0.092 | 0.075 | ||||||
| Other chronic or severe diseases at T2 | –0.171** | –0.151** | –0.158** | –0.141* | |||||
| Step 4 | 30.440 | 0.345 | 0.254 | ||||||
| Work ability at T1 | 0.525*** | 0.383*** | 0.349*** | 0.328*** | |||||
| Step 5 / late effects at T1 | 22.386 | 0.407 | 0.062 | ||||||
| Physical complaints | –0.050 | –0.049 | –0.041 | ||||||
| Fatigue | –0.127 | –0.121 | –0.131* | ||||||
| Cognitive complaints | –0.183** | –0.181** | –0.202*** | ||||||
| Step 6 / job resources at T1 | 15.801 | 0.413 | 0.005 | ||||||
| Autonomy | 0.035 | 0.049 | |||||||
| Supportive leadership style | 0.012 | 0.049 | |||||||
| Social support by colleagues | 0.061 | 0.063 | |||||||
| Step 7 / interaction terms | 8.818 | 0.437 | 0.024 | ||||||
| Physical complaints x Autonomy | –0.151* | ||||||||
| Physical complaints x Supportive leadership style | 0.005 | ||||||||
| Physical complaints x Social support by colleagues | 0.073 | ||||||||
| Fatigue x Autonomy | 0.076 | ||||||||
| Fatigue x Supportive leadership style | 0.012 | ||||||||
| Fatigue x Social support by colleagues | –0.073 | ||||||||
| Cognitive complaints x Autonomy | –0.031 | ||||||||
| Cognitive complaints x Supportive leadership style | –0.020 | ||||||||
| Cognitive complaints x Social support by colleagues | –0.014 |
Notes: Physical complaints, fatigue, cognitive complaints, autonomy, supportive leadership style and social support by colleagues were centered at their means. *Significant at the≤0.05 level. **Significant at the≤0.01 level. *** Significant at the≤0.001 level.
Thereafter hypothesis H1 was tested with physical complaints, fatigue, and cognitive complaints at T1, together in the fifth step of the multivariate regression analyses, as predictors. The degree of the number of physical complaints did not predict lower work ability at T2 in this analysis, however, a higher level of fatigue and a higher level of cognitive complaints did (respectively β= –0.131, p≤0.05 and β= –0.202, p≤0.001). Therefore, hypotheses H1b and H1c were confirmed, but hypothesis H1a was not. See Table 3.
Hypothesis H2 was tested in the sixth step of the above-described multivariate regression analyses, with the three job resources (autonomy, supportive leadership style, social support by colleagues) at T1 as predictors, and work ability at T2 as dependent variable. The hypotheses H2a, H2b, and H2c were not confirmed. The three job resources did not predict the level of future work ability at T2. See Table 3. An additional analysis demonstrated that all three job resources at T1 did significantly predict work ability at T1 (baseline).
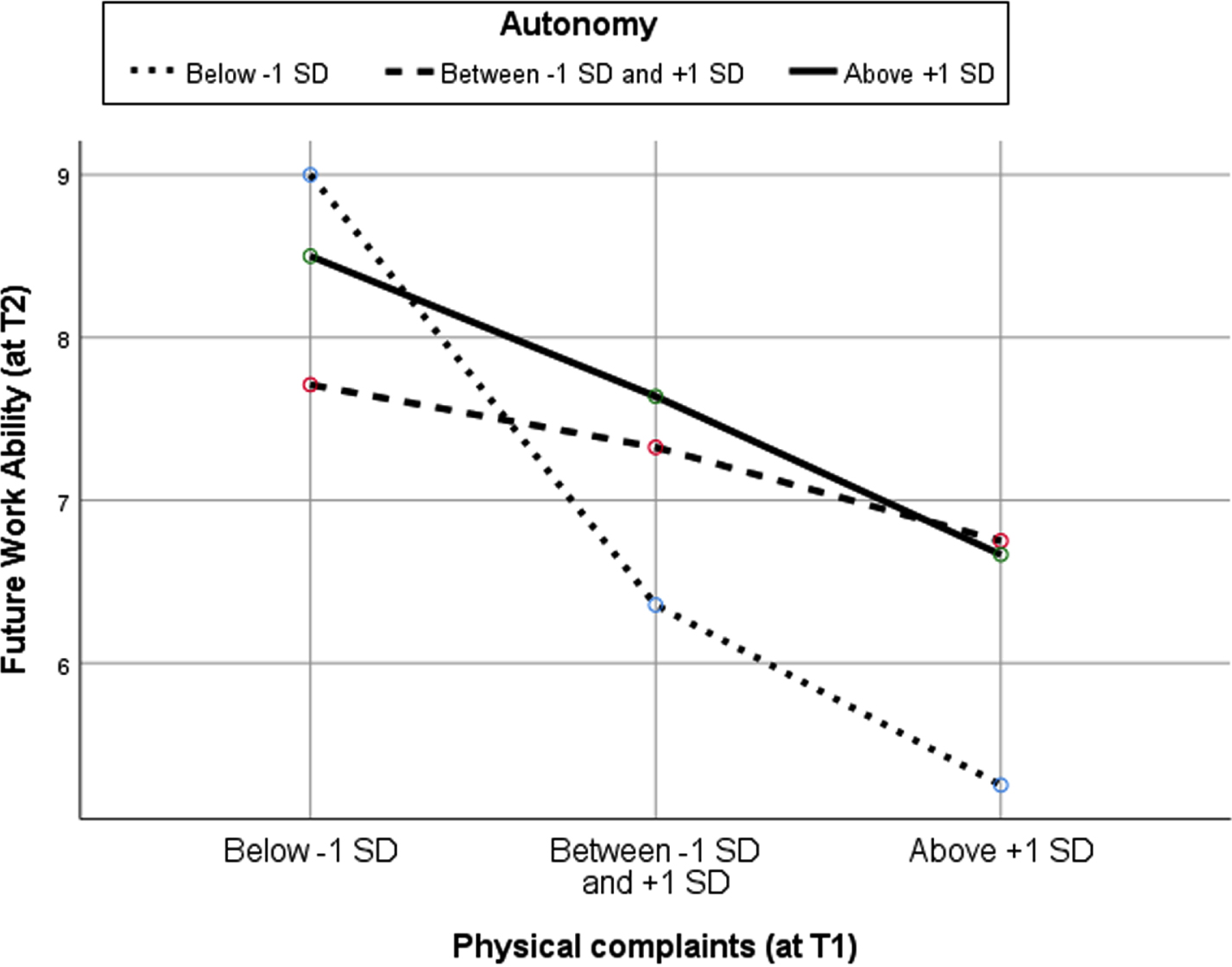
Hypotheses H3 concerned the expected moderation of the job resources (autonomy, a supportive leadership style or social support by colleagues) at T1 of the presumed negative relationships between physical complaints, fatigue, or cognitive complaints (late effects) at T1 and work ability at T2 resulting in better work ability outcomes. This was tested in the seventh step of the multivariate regression analyses. The negative relationships of fatigue and cognitive complaints with work ability were not moderated by job resources, so our expectations were not met. However, there was one case of moderation, as autonomy negatively moderated the association of physical complaints with work ability at T2 (β= –0.151, p ≤0.05), which means a deterioration of work ability outcomes for people with physical complaints. See Table 3. A visual representation shows the different slopes of three lines representing three levels of autonomy for different levels of physical complaints and the associated future work ability. See Fig. 1.
4Discussion
Fig.1
Moderation by autonomy (at T1) of the association of physical complaints (at T1) with future work ability (at T2) among workers 2-10 years beyond breast cancer diagnosis (N = 280).
We found that higher levels of fatigue or cognitive complaints have a longitudinal lowering effect on future work ability among workers more than 2 years beyond breast cancer diagnosis. As far as known, this has not been previously demonstrated. Cross-sectional associations between these late effects and work ability have been reported before [22], in addition to associations between cognitive complaints and fatigue [i.e. 56, 57]. However, the results of the present study cannot be compared with other longitudinal studies, as none are available. The level of physical complaints correlated significantly with lower future work ability, but less strongly than fatigue or cognitive complaints did. Moreover, the three late effects are strongly interrelated and, in this sample, cognitive complaints and fatigue are slightly more strongly related to work ability than physical complaints. This explains why physical complaints showed no significant effect in the regression analyses.
The level of individuals’ work ability was reasonably stable over time, and baseline work ability was predictive of the level of future work ability. Cross-sectionally the three job resources (autonomy, supportive leadership style, and social support by colleagues) at T1 were associated with higher current (baseline) work ability at T1, however the job resources were not predictive of future work ability at T2 (see Table 3). Nor was found that the relationships between late effects and future work ability were moderated by job resources resulting in a change for the better, that is higher future work ability (see Table 3). A possible cause of the latter could be that the factors (that is, the late effects, the job resources and the outcome measure) in the model did not completely match on a cognitive, emotional, or physical level [65]. Up to now, relatively little studies are known about vocational interventions specifically for workers who have had cancer. Other resources, such as within-shift breaks that were found to be beneficial among various employed populations [66] or a modified workstation or schedule especially suggested for workers beyond cancer diagnosis [67] may be important to study as possible moderating resources as well. Generic strategies and elements of the interventions for workers with chronic conditions may be suitable for the post-cancer-diagnosis group, but it is advised to offer working cancer survivors tailored interventions [68].
Although longitudinal research on this issue among workers more than 2 years past a cancer diagnosis is lacking, the available cross-sectional studies among this population have revealed positive correlations of social support of colleagues [39, 41, 43] and concepts related to autonomy [39, 40, 44] with work ability. Furthermore, cross-sectional associations between a supportive leadership style and higher work ability were also observed among employees with chronic diseases [46]. However, in the present study, future work ability (at T2) is not predicted by the level of the job resources at T1, but by baseline work ability and by the late effects fatigue and cognitive complaints at T1. Nevertheless, an additional cross-sectional regression analysis demonstrated that the job resources at T1 did predict work ability at T1, suggesting these job resources may need continual attention.
Furthermore, against expectations, the multivariate regression analyses (controlling for years past cancer diagnosis, living with cancer, other chronic or severe diseases baseline work ability) resulted in a negative moderation by autonomy in the case of physical complaints. Participants with average and high levels of physical complaints and low autonomy experienced a level of future work ability that was much lower than when autonomy was at a medium level. So, a lack of autonomy in the case of average and high physical complaints is not recommended because the lowest level of work ability was experienced in that situation. Furthermore, participants with average and high levels of physical complaints and high autonomy experienced a level of future work ability similar to when autonomy was at medium level. This seems to be in line with the findings that the type and the scope of demands also determine the effect of job control, which even at a high level may not prove to be sufficient to prevent overburdening [69]. Employees with higher levels of physical complaints possibly experience negative effects with too much autonomy and may require less autonomy and different kinds of support when experiencing high levels of physical complaints. It could also be that these workers, as they experience more physical complaints, proceed too far beyond their limits when experiencing more autonomy. This means that, particularly in the case of physical complaints, it is necessary to carefully monitor a balance between physical complaints and the autonomy offered. Autonomy is important, but tailormade advice is particularly necessary in these situations, as the notion that more autonomy will always result in higher work ability may be a misconception.
5Strengths and Limitations
To begin with, it is important to note that this issue has not been studied before. Longitudinal studies of workers who have been diagnosed with cancer more than 2 years ago are rare and have not addressed the impact of late effects of cancer treatments on future work ability at all, as far as the authors of the present study are aware. Furthermore, it is remarkable that large numbers of working participants who fell under the criteria were willing to complete an extensive questionnaire on two occasions. Moreover, professionals indicate that this subject is considered extremely important and that knowledge is lacking in this area [14].
Of course, we must also consider that the study results may have been influenced by certain limitations in the design of the study. First, this study was limited to salaried employees who experienced a breast cancer diagnosis. It is difficult to assess to what extent this may have influenced the results, but it should be mentioned that women with a breast cancer diagnosis in the past have been reported to have a lower work ability than men with testicular cancer and a higher work ability than men with prostate cancer [39]. The late effects of cancer treatment between these populations may be substantially dissimilar and affect work ability differently. Furthermore, cross-sectional studies among workers more than 2 years past cancer diagnosis have reported higher work ability scores among females with a previous breast cancer diagnosis than in the present study. In the present study, work ability was 7.3 at T2, while other studies reported 8.0 (controls 8.6) [8], 8.4 (referents 8.6) [10], 8.7 (controls 9.0) [11] and 8.2 [12]. However, it is unclear to what extent these other studies concerned salaried workers. For example, the latter study also included freelancers and entrepreneurs, and this may have influenced the results. Overall, it is not possible in the present study to make clear inferences regarding the work ability of the entire population of employed women in the Netherlands who were confronted with a breast cancer diagnosis 2–10 years ago. Second, this study did not consider possible differences between the perceived late effects by the worker and the way in which these are perceived by colleagues or professionals. It is particularly important to mention that cognitive complaints were self-reported and not estimated by professionals using neuropsychological testing, while subjective and objective cognitive impairment is known to show little correlation [70]. Furthermore, the results on a self-report scale may show associations with psychosocial factors [51, 71, 72]. Therefore, in future studies on this topic, it would be wise not only to collect data on self-reported cognitive complaints, but also to conduct neuropsychological tests. Third, self-reporting by using a questionnaire may lead to various sources of common method bias [73]. However, we took this into account by using existing, validated scales as much as possible and by carefully determining the order of the scales and other questions to prevent interference. Fourth, profiles are conceivable with specific combinations of certain levels in physical complaints, fatigue and cognitive complaints. These profiles may have different effects. This has not been investigated in this study. Fifth, a moderation analysis requires a number of conditions [61]. One assumption is that distributions include the full range of possible values. This was not always completely the case for the raw scores, however the variables were centered around their means.
This study was conducted with the data of those who wanted to participate and were willing and able to complete two extensive questionnaires within a period of 1 year. Another point in this regard is therefore that the dropouts between questionnaires had significantly more cognitive complaints, and may have caused a so-called healthy worker effect that influenced the results as the selection bias caused a more favorable clinical profile [74]. However, this even further accentuates the results. In addition, nothing is known about the group that did not participate. For these reasons, it is doubtful whether the survey sample is representative of all workers who returned to work and are now 2–10 years past breast cancer diagnosis.
The Covid-19 pandemic started after the data-collection phase of this study. Opportunities for autonomy may have changed during the lockdowns, given the increased prevalence of working at home without a manager or supervisor being physically present. Furthermore, spontaneity in contact with colleagues will have probably diminished during this period, also changing social support. Moreover, job demands may have changed. It is interesting what the effects of these changes may have been among these employees, and future research into these effects is important.
6Conclusions
The present study clearly indicates that cognitive complaints and fatigue may affect future work ability among employees 2–10 years past breast cancer diagnosis. This requires awareness among those who guide employees who were diagnosed with cancer, and among these employees themselves. Interventions by professionals specialized in oncology or psycho-oncology may be preferable. Complaints may be reduced, or compensation mechanisms may be enhanced. Furthermore autonomy, a supportive leadership style, or social support by colleagues may need attention continually as these resources are associated with higher current work ability, but not with future work ability.
The number of workers who have had cancer will continue to increase, and awareness that this is the case and can be associated with the late effects of treatments is important. This is not widely known in the workplace. It is therefore extremely important for professionals and managers or supervisors to be alert and to ask further questions in the case of problems. All in all, the present study is an interesting step toward more awareness about cognitive complaints and fatigue that may affect future work ability. Further research should be conducted into other job resources, such as job crafting or specialized guidance by professionals, as evidence-based targets for interventions available in the workplace are urgently needed.
Acknowledgments
We are grateful to all participants for taking part in this study. We would also like to mention the support of several colleagues from the Faculty of Applied Social Sciences and Law and research trainees of the bachelor Applied Psychology at the Amsterdam University of Applied Sciences. They have played an important role in the development of the flyer and the animation used in the recruitment of the participants and in the creation of the questionnaire.
Ethical approval
The study was reviewed and approved by the Research Ethics Committee (cETO) of the Open Universiteit in the Netherlands who assessed the ethical acceptability of the study and agreed with the study design and method (reference cETO: U2018/03891/MQF).
Informed Consent
The participants provided their written informed consent to participate in this study.
Conflict of interest
TV was employed by the company Loyalis Knowledge & Consult. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. Therefore, the authors declare that they have no conflict of interest.
Funding
The authors report no funding.
References
[1] | Kuijpens JLP Kanker in de beroepsbevolking: aantallen en trends. Tijdschr voor Bedrijfs- en Verzek (2008) ;16: (7):281–4. |
[2] | Ferlay J , Colombet M , Soerjomataram I , Parkin DM , Piñeros M , Znaor A , Bray F . Cancer statistics for the year An overview. Int J Cancer [Internet]. (2021) Aug 15 [cited 2021 Jul 18];149: (4):778–89 Available from: https://onlinelibrary.wiley.com/doi/full/10.1002/ijc.33588 |
[3] | IKNL. Incidentie [Internet]. [cited 2021 Nov 16]. Available from: https://iknl.nl/kankersoorten/borstkanker/registratie/incidentie |
[4] | IKNL. Prevalentie [Internet]. [cited 2021 Jul 18]. Available from: https://iknl.nl/kankersoorten/borstkanker/registratie/prevalentie. |
[5] | Paltrinieri S , Fugazzaro S , Bertozzi L , Bassi MC , Pellegrini M , Vicentini M , Mazzini E , Costi S Return to work in European Cancer survivors: a systematic review [Internet]. Vol. 26, Supportive Care in Cancer. Springer Verlag; 2018 [cited 2020 Jul 5]. p. 2983–94. Available from: https://link.springer.com/article/10.1007/s00520-018-4270-6. |
[6] | Tamminga SJ , Jansen LP , Frings-Dresen MHW , De Boer AGEM Long-term employment status and quality of life after cancer: A longitudinal prospective cohort study from diagnosis up to and including 5 years post diagnosis. Work (2020) ;66: (4):901–7. |
[7] | Gudbergsson SB , Fosså SD , Dahl AA Is cancer survivorship associated with reduced work engagement? A NOCWO Study. J Cancer Surviv [Internet]. (2018) [cited 2018 Jul 13];2: (3):159–68. Available from: https://www.researchgate.net/publication/51428129. |
[8] | Gudbergsson SB , Fosså SD , Dahl AA Are there sex differences in the work ability of cancer survivors? Norwegian experiences from the NOCWO study. Support Care Cancer [Internet]. (2011) Mar 6 [cited 2018 Jul 13];19: (3):323–31. Available from: http://link.springer.com/10.1007/s00520-950010-0820-2. |
[9] | Lee MK , Lee KM , Bae JM , Kim S , Kim YW , Ryu KW , Lee J. H , Noh JH , Sohn TS , Hong SK , Yun YH Employment status and work-relateddifficulties in stomach cancer survivors compared with the generalpopulation. Br J Cancer [Internet]. (2008) Feb 19 [cited 2018 Jul 13];98: (4):708–15. Available from: http://www.nature.com/articles/6604236. |
[10] | Lindbohm ML , Taskila T , Kuosma E , Hietanen P , Carlsen K , Gudbergsson S , Gunnarsdottir H Work ability of survivors of breast, prostate,and testicular cancer in Nordic countries: A NOCWO study. J CancerSurviv [Internet]. (2012) [cited 2018 Dec 10];6: (1):72–81. Available from: https://www.researchgate.net/publication/51760002. |
[11] | Carlsen K , Jensen AJ , Rugulies R , Christensen J , Bidstrup PE , Johansen C , Huitfeldt Madsen IE , Dalton SO Self-reported workability in long-term breast cancer survivors. A population-basedquestionnaire study in Denmark. In: Acta Oncologica [Internet]. (2013) [cited 2018 Jul 13]. p. 423–9 Available from: http://www.ncbi.nlm.nih.gov/pubmed/23282112. |
[12] | Taskila T , Martikainen R , Hietanen P , Lindbohm M Comparative studyof work ability between cancer survivors and their referents. Eur JCancer [Internet]. (2007) Mar 1 [cited 2018 Jul 13];43: (5):914–20. Available from: https://www.sciencedirect.com/science/article/pii/S0959804907000160. |
[13] | Silver JK , Baima J , Newman R , Galantino Lou M , Shockney LD Cancer rehabilitation may improve function in survivors and decrease the economic burden of cancer to individuals and society. Work (2013) ;46: (4):455–72. |
[14] | Boelhouwer IG , Vermeer W , van Vuuren T Late effects of cancer (treatment) and work ability: guidance by managers and professionals. BMC Public Health [Internet]. (2021) Jun 29 [cited 2021 Jul 20];21: (1):1–17. Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-021-11261-2. |
[15] | Cadiz DM , Brady G , Rineer JR , Truxillo DM A review and synthesis of the work ability literature. Work, Aging and Retirement. Oxford Academic (2019) ;5: , 114–38. |
[16] | Brady GM , Truxillo DM , Cadiz DM , Rineer JR , Caughlin DE , Bodner T Opening the Black Box: Examining the Nomological Network of Work Ability and Its Role in Organizational Research. J Appl Psychol 2019. |
[17] | Ho PJ , Hartman M , Gernaat SAM , Cook AR , Lee SC , Hupkens L , Verkooijen HM Associations between work-ability and patient-reported physical, psychological and social outcomes in breast cancer survivors: a cross-sectional study. Support Care Cancer [Internet]. (2018) Aug 6 [cited 2018 Jul 13];26: (8):2815–24. Available from: http://link.springer.com/10.1007/s00520-018-4132-2. |
[18] | Prue G , Rankin J , Allen J , Gracey J , Cramp F Cancer-related fatigue: A critical appraisal. Eur J Cancer (2006) ;42: (7):846–63. |
[19] | Meunier J , Libert Y , Delvaux N , Marchal S , Etienne A , Lienard A , Reynaert C , Razavi D Psychobiological correlates of communication skills use and learning: Preliminary results. Psycho-Oncology J Psychol Soc Behav Dimens cancer (2007) ;16: (9):S25–S25. |
[20] | Reinertsen KV , Cvancarova M , Loge JH , Edvardsen H , Wist E , Fosså SD Predictors and course of chronic fatigue in long-term breast cancer survivors. J Cancer Surviv (2010) ;4: (4):405–14. |
[21] | Wefel JS , Kesler SR , Noll KR , Schagen SB Clinical characteristics,pathophysiology, and management of noncentral nervous systemcancer-related cognitive impairment in adults. CA Cancer J Clin [Internet]. (2015) Mar 1 [cited 2018 Oct 8];65: (2):123–38. Available from: http://doi.wiley.com/10.3322/caac.21258. |
[22] | Boelhouwer IG , Vermeer W , van Vuuren T The associations between late effects of cancer treatment, work ability and job resources: a systematic review. Int Arch Occup Environ Health [Internet]. (2021) Sep 15 [cited 2020 Sep 16];94: (2):147–89. Available from: http://link.springer.com/10.1007/s00420-020-01567-w. |
[23] | Moskowitz MC , Todd BL , Chen R , Feuerstein M Function and friction at work: A multidimensional analysis of work outcomes in cancer survivors. J Cancer Surviv [Internet]. (2014) Jun 26 [cited 2018 Jul 13];8: (2):173–82. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24464639. |
[24] | Torp S , Syse J , Paraponaris A , Gudbergsson S Erratum to: Return to work among self-employed cancer survivors. J Cancer Surviv [Internet]. (2017) Apr 15 [cited 2018 Jul 13];11: (2):201–2. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27981426. |
[25] | Dahl AA , Fosså SD , Lie HC , Loge JH , Reinertsen KV , Ruud E , Kiserud CE Employment Status and Work Ability in Long-Term Young Adult Cancer Survivors. J Adolesc Young Adult Oncol [Internet]. (2019) Jun 1 [cited 2020 Apr 16];8: (3):304–11. Available from: https://www.liebertpub.com/doi/10.1089/jayao.2018.0109. |
[26] | Gould R , Ilmarinen J , Järvisalo J , Koskinen S Dimensions of Work Ability. Results of the Health 2000 Survey [Internet]. (2000) [cited 2018 Aug 26]. Available from: http://www.julkari.fi/bitstream/handle/10024/129167/Dimensionsofworkability.pdf?sequence=1. |
[27] | Leijten FRM , van den Heuvel SG , Ybema JF , van der Beek AJ , Robroek SJW , Burdorf AA The influence of chronic health problems on work ability and productivity at work: a longitudinal study among older employees. Scand JWork Environ Health [Internet]. (2014) ;40: (5):473–82. Available from: http://www.sjweh.fi/showabstract.php?abstractid=3444. |
[28] | Geukes M , Van Aalst MP , Nauta MCE , Oosterhof H The impact of menopausal symptoms on work ability. Menopause [Internet]. (2012) Mar [cited 2021May14] ;19: (3):278–82. Available from: https://journals.lww.com/menopausejournal/Fulltext/2012/03000/The_impact_of_menopausal_symptoms_on_workability.7.aspx |
[29] | Gamperiene M , Nygård JF , Sandanger I , Lau B , Bruusgaard D Self-reported work ability of Norwegian women in relation to physical and mental health, and to the work environment. J Occup Med Toxicol [Internet]. (2008) Apr 22 [cited 2021 May 14] ;3: (1):1–9. Available from: http://www.occup-med.com/content/3/1/8 |
[30] | Da Silva FJ , Felli VEA , Martinez MC , Mininel VA , Ratier APP Association between work ability and fatigue in Brazilian nursing workers. Work (2016) ;53: (1):225–32. |
[31] | Sandqvist G , Scheja A , Hesselstrand R Pain, fatigue and hand function closely correlated towork ability and employment status in systemic sclerosis. Rheumatology [Internet]. (2010) [cited 2021 May 14] ;49: (9):1739–46. Available from: https://academic.oup.com/rheumatology/article/49/9/1739/1787004 |
[32] | Boschman JS , Nieuwenhuijsen K , Frings-Dresen MHW , Sluiter JK Development of hospital nurses’ work ability over a 2 year period. Occup Med (Chic Ill) [Internet]. (2015) Oct 1 [cited 2021 May 14] ;65: (7):542–8. Available from: https://academic.oup.com/occmed/article/65/7/542/1733529 |
[33] | Von Ah D , Storey S , Crouch A , Johns SA , Dodson J , Dutkevitch S Relationship of Self-reported Attentional Fatigue to PerceivedWork Ability in Breast Cancer Survivors. Cancer Nurs [Internet]. (2017) [cited 2018 Jul 13];40: (6):464–70. Available from: http://www.ncbi.nlm.nih.gov/pubmed/2782905 |
[34] | Von Ah D , Storey S , Crouch A Relationship between self reported cognitive function and work-related outcomes in breast cancer survivors. J Cancer Surviv [Internet]. (2018) [cited Apr 8 [cited 2018 Jul 13];12: (2):246–55. Available from: http://www.ncbi.nlm.nih.gov/pubmed/29222703 |
[35] | Hansen JA , Feuerstein M , Calvio LC , Olsen CH Breast cancer survivors at work. J Occup Environ Med [Internet]. (2008) [cited 2021 Aug 1];50: (7):777–84. Available from: https://journals.lww.com/joem/Fulltext/2008/07000/BreastCancerSurvivorsatWork.7.aspx |
[36] | Duijts SFA , Van Der Beek AJ , Boelhouwer IG , Schagen SB Cancer-related cognitive impairment and patients’ ability to work: A current perspective. 11: , Current Opinion in Supportive and Palliative Care. (2017) 19–23. |
[37] | Bakker AB , Demerouti E . The Job Demands-Resources model: State of the art. Journal of Managerial Psychology. (2007) ;22: ;309–28. |
[38] | Bakker AB , Demerouti E The Job Demands-Resources model: State of the art [Internet].. 22 : .Journal of Man agerial Psychology.(2007) [cited 2018 Dec 19].p.309–28. Available from: https://www.emeraldinsight.com/doi/10.1108/02683940710733115 |
[39] | Torp S , Nielsen RA , Gudbergsson SB , Dahl AA Work site adjustments and work ability among employed cancer survivors. Support Care Cancer [Internet]. (2012) Sep 16 [cited 2018 Jul 13];20: (9):2149–56. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22086407 |
[40] | Torp S , Syse J , Paraponaris A , Gudbergsson S Return to work among self-employed cancer survivors. J Cancer Surviv [Internet]. (2017) Apr 12 [cited 2018 Jul 13];11: (2):189–200. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27837444 |
[41] | Musti MA , Collina N , Stivanello E , Bonfiglioli R , Giordani S , Morelli C , Pandolfi P Perceived work ability at return to work in women treated for breast cancer: A questionnaire-based study. Med del Lav (2018) ;109: (6):407–19. |
[42] | Taskila T , Martikainen R , Hietanen P , Lindbohm M-L Com-parative study of work ability between cancer survivors and their referents. Eur J Cancer [Internet]. (2007) 43: (5):914–20. Available from: http://www.sciencedirect.com/science/article/pii/S0959804907000160 |
[43] | Gudbergsson SB , Fosså SD , Dahl AA A study of work changes due to cancer in tumor-free primary-treated cancer patients. A NOCWO study. Support Care Cancer [Internet]. (2008) [cited 2018 Jul 13];16: (10):1163–71. Available from: https://www.researchgate.net/publication/5595058 |
[44] | Cheung K , Ching SYS , Chan A , Cheung D , Cheung SYP The impact of personal-, disease- and work-related factors on work ability of women with breast cancer living in the community: a cross-sectional survey study. Support Care Cancer [Internet].(2017) Nov 14 [cited 2018 Jul 13];25: (11):3495–504. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28612159 |
[45] | Van den Berg TIJ , Elders LAM , De Zwart BCH , Burdorf A The effects of work-related and individual factors on the Work Ability Index: a systematic review. Occup Envi-ron Med [Internet].(2008) Nov 18 [cited 2019 Jul 11];66: (4):211–20. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19017690 |
[46] | Boelhouwer IG , Vermeer W , van Vuuren T Work Ability, Burnout Complaints, and Work Engagement Among Employees With Chronic Diseases: Job Resources as Targets for Intervention? Front Psychol [Internet] 2020 Aug 6 [cited 2020 Sep 16];11. Available from: https://pmc/articles/PMC7424075/?report=abstract |
[47] | Van Den Berg TI , Robroek SJ , Plat JF , Koopmanschap MA , Burdorf A The importance of job control for workers with decreased work ability to remain produc-tive at work. Int Arch Occup Environ Health [Internet].(2011) Aug 16 [cited 2021 Nov 8];84: (6):705–12. Available from: https://link.springer.com/article/10.1007/s00420-010-0588-1 |
[48] | Sugimura H , Thériault G Impact of supervisor support on work ability in an IT company. Occup Med (Chic Ill) (2010) ;60: (6):451–7. |
[49] | McGonagle AK , Barnes-Farrell JL , Di Milia L , Fischer FM , Hobbs BBB , Iskra-Golec I , Kaliterna L , Smith L Demands, resources, and work ability: A cross-national examination of health care workers. Eur J Work Organ Psychol [Internet].(2014) Nov 2 [cited 2018 Dec 19];23: (6):830–46. Available from: http://www.tandfonline.com/doi/abs/10.1080/1359432X.2013.819158 |
[50] | Olsen E , Bjaalid G , Mikkelsen A Work climate and the mediating role of workplace bullying related to job performance, job satisfaction, and work ability: A study among hospital nurses. J Adv Nurs (2017) ;73: (11):2709–19. |
[51] | Feuerstein M . Work and cancer survivors Work and Cancer Survivors. 2011. 1-350 p. |
[52] | Het Concept Werkvermogen –Osagie et al.2019 [Inter-net]. [cited 2019 Jul 10]. Available from: https://tijdschriftvoorhrm.nl/het-concept-werkvermogen/?utmsource=Tijdschrift+voor+HRM+Nieuwsbrief&utmcampaign=1a14722ec9-EMAILCAMPAIGN201906190336&utm medium=email&utm term=0337be68bfe-1a14722ec9-232522021 |
[53] | Wells M , Amir Z , Cox T , Eva G , Greenfield D , Hubbard G , Kyle R , McLennan S , Munir F , Scott S , Sharp L , Taskila T , Wiseman T Time to act: The challenges of working during and after cancer, initiatives in research and practice. Vol. 18, European Journal of Oncology Nursing 2014 1–2. |
[54] | Vercoulen J , Swannik C , Fennis J , Galama J , van der Meer J , Bleijenberg G Checklist Individuele Spankracht (CIS). Gedragstherapie [Internet].(2017) [cited 2020 Dec 28];32: 131–6.Available from: http://www.bsw.ugent.be/VVGP/ficheCIS.pdf |
[55] | Vercoulen JHMM , Swanink CMA , Fennis JFM , Galama JMD , van der Meer JWM , Bleijenberg G Dimensional assessment of chronic fatigue syndrome. J Psychosom Res (1994) ;38: (5):383–92. |
[56] | Ponds R , Van Boxtel MPJ , Jolles J De “Cognitive FailureQuestionnaire” als maat voor subjectief cognitief functioneren. Tijdschr voor Neuropsychol [Internet]. (2006) [cited 2020 Dec 28];2(December 2015):37–45. Available from: https://www.researchgate.net/publication/286212206. |
[57] | Ilmarinen J , Tuomi K , Seitsamo J New dimensions of work ability. Int Congr Ser (1280) 3–7. |
[58] | Ilmarinen J , von Bonsdorff M Work Ability. In: The Encyclopedia of Adulthood and Aging [Internet]. Tijdschr voor Neuropsychol [Internet] Hoboken, NJ, USA: John Wiley & Sons, Inc.;1204 2015 [cited 2018 May 15]. p. 1–5. Available from: http://doi.wiley.com/10.1002/9781118521373.wbeaa2544/27/2022. |
[59] | Ahlstrom L , Grimby-Ekman A , Hagberg M , Dellve L The work ability index and single-item question: Associations with sick leave, symptoms, and health - A prospective study of women on long-term sick leave. Scand J Work Environ Heal (2010) ;36: (5):404–12. |
[60] | Van Poppel J ., &Kamphuis P . Manual School’s Health Measure: Research About Health, Work and Work Conditions in Schools. Tilburg: IVA;2004. |
[61] | Aguinis H , Edwards JR , Bradley KJ Improving Our Understanding of Moderation and Mediation in Strategic Management Research. Organ Res Methods [Internet].(2017) Jan 27 [cited 2021 Dec 26];20: (4):665–85. Available from: https://journals.sagepub.com/doi/abs/10.1177/1094428115627498 |
[62] | Holland SJ , Shore DB , Cortina JM Review and Recommendations for Integrating Mediation and Moderation.. Organ Res Methods [Internet].(2017) Aug 5 [cited 2021 Dec 26];20: (4):686–720. Available from: https://journals.sagepub.com/doi/abs/10.1177/1094428116658958 |
[63] | Dorland HF , Abma FI , Roelen CAM , Smink A , Feuerstein M , Amick BC , Ranchor A V , Bultmann U. , The Cognitive Symptom Checklist-Work in cancer patients is related with work functioning, fatigue and depressive symptoms: a validation study. J Cancer Surviv [Internet].(2016) Jun;10: (3):545–52. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26620817 |
[64] | Todd BL , Feuerstein EL , Feuerstein M When breast cancer survivors report cognitive problems at work. In: International Journal of Psychiatry in Medicine. Baywood Publishing Co., Inc;(2011) ;279–94. |
[65] | De Jonge J , Dormann C Stressors, resources, and strain at work: A longitudinal test of the triple-match principle. J Cancer Surviv [Internet].(2006) Nov [cited 2021 Dec 1238 26];91: (6):1359–74. Available from: https://record/2006-20695-014 |
[66] | Wendsche J , Lohmann-Haislah A , Jürgen J The impact of supplementary short rest breaks on task performance –A meta-analysis. sozialpolitik ch [Internet]. (2016) [cited 2021 Dec 26];2016: (2):Article: 2.3. Available from: https://folia.unifr.ch/global/documents/306065 |
[67] | Alleaume C , Paraponaris A , Bendiane MK , Peretti-Watel P , Bouhnik AD The positive effect of workplace accommodations on the continued employment of cancer survivors five years after diagnosis. Support Care Cancer [Internet]. (2020) [cited 2020 Sep 19];28: (9):4435–43. Available from: https://academic.oup.com/eurpub/article-abstract/29/Supplement4/ckz185.384/5624677 |
[68] | Stapelfeldt CM , Klaver KM , Rosbjerg RS , Dalton SO , Bültmann U , Labriola M , Duijts SFA systematic review of interventions to retain chronically ill occupationally active employees in work: can findings be transferred to cancer survivors? [Internet]. Vol. 58, Acta Oncologica. Taylor & Francis; 2019 [cited 2021 Jul 20]. p. 548–65. Available from: https://www.tandfonline.com/doi/abs/10.1080/0284186X.2018.1559946. |
[69] | Gonzalez-Mulé E , Kim MM , Ryu JW A Meta-Analytic Test of Multiplicative and Additive Models of Job Demands, Resources, and Stress. J Appl Psychol [Internet]. (2021) [cited 2021 Dec 26];106: (9):391–411. Available from: https://record/2020-70963-001. |
[70] | Poppelreuter M , Weis J , Külz AK , Tucha O , Lange KW , Bartsch HH Cognitive dysfunction and subjective complaints of cancer patients: A cross-sectional study in a cancer rehabilitation centre. Eur J Cancer (2004) ;40: (1):43–9. |
[71] | Boscher C , Joly F , Clarisse B , Humbert X , Grellard JM , Binarelli G , Tron L , Licaj I , Lange M Perceived cognitive impairment in breast cancer survivors and its relationships with psychological factors. Cancers (Basel) [Internet]. (2020) Oct 16 [cited 2021 Jul 21];12: (10):1–13. Available from: https://www.mdpi.com/2072-6694/12/10/3000/htm. |
[72] | Pullens MJJ , De Vries J , Roukema JA Subjective cognitive dysfunction in breast cancer patients: A systematic review [Internet]. Vol. 19, Psycho-Oncology.John Wiley & Sons, Ltd; 2010 [cited 2021 Jul 21]. p. 1127–38. Available from: https://onlinelibrary.wiley.com/doi/full/10.1002/pon.1673. |
[73] | Podsakoff PM , MacKenzie SB , Lee JY , Podsakoff NP Com-mon Method Biases in Behavioral Research: A Critical Reviewof the Literature and Recommended Remedies.Vol. 88, Journal of Applied Psychology. 2003.p. 879–903 |
[74] | Chowdhury R , Shah D , Payal A Healthy worker effect phenomenon: Revisited with emphasis on statistical methods-A review [Internet]. Vol. 21, Indian Journal of Occupational and Environmental Medicine. Wolters Kluwer –Medknow Publications; 2017 [cited 2022 Feb 10]. p. 2–8. Available from: http://pmc/articles/PMC5763838/ |


