
The effects of the COVID-19 pandemic on healthcare workers’ psychological and mental health: The moderating role of felt obligation
Abstract
BACKGROUND:
The ravages of COVID-19 have created a worldwide emergency in healthcare units. Under these circumstances, the perception of an infection threat is primarily affecting the employees’ performance in reducing contagion effects.
OBJECTIVE:
The purpose of this study is to develop substantial measures of support for healthcare employees to maintain adequacy in job performance.
METHODS:
Data were collected from state-owned hospitals in Pakistan to test the current study’s proposed model. We applied structural equation modeling through a partial least square regression in addition to the blindfolding approach in Smart-PLS. Confirmatory factor analysis was also employed to measure the study’s validity.
RESULTS:
The current study’s findings show that the perception of a threat from COVID-19 and the inadequate protective measures have influenced frontline healthcare workers’ performance levels. The mediating path of depression symptoms indicated the threat of COVID-19 and the absence of protective measures as potential determinants of poor performance. However, an employee’s ability to feel obligated toward their job duties reduces the effect of depression on employee performance.
CONCLUSION:
The current model highlights an individual’s feelings of obligation to maintain their performance level by minimizing the effect of depression and professional anxiety. The present study extensively described the psychological constraints healthcare workers are facing during the current pandemic. Current research addressing healthcare employees’ mental health is vital for better prevention and control during pandemic circumstances. The current study’s findings extend the emerging understanding of employee psychology in such circumstances.
1Introduction
The recent emergence of COVID-19 has devastated many countries’ economies and tarnished the image of health mechanisms among advanced and developing countries [1–3]. The rapid spread of coronavirus (SARS-CoV-2; COVID-19) had disrupted the global healthcare sector. The COVID-19 pandemic has exerted unprecedented pressure on the occupational environment, drastically challenging healthcare employees. The high risk of the pandemic has compelled health professionals to battle against the intensity of COVID-19. The increasing fear caused by the spread of the disease has had significant repercussions for the global health industry, potentially affecting individual health conditions (i.e., physical and psychological). Undoubtedly, the present pandemic consequences are not limited to physical challenges but also extend to psychological and mental well-being [4]. During the pandemic, healthcare workers performed well by risking their lives and fighting at the frontline, combating the intensity of COVID-19. The result shows that the rapid escalation of this pathogenic virus has impacted individuals’ (i.e., nurses’) health conditions, leading to severe physical and mental discomforts [5]. Indeed, COVID-19 caused clinical professionals to experience physical and psychological discomfort, including a high level of depression, anxiety, and pain. These emerging health challenges like fatigue, stress, and mental disorders have affected these individuals’ quality of life, resulting in them reporting numerous health complaints [6].
Furthermore, this study illustrates that the current pandemic had threatened the health system while forcing nurses to exhibit high professional commitment and responsibility. Research shows that their work schedules have become more demanding, increasing their work burden and stress to combat the disease [7]. This increased intensity of the pandemic has led healthcare professionals to face the negative consequences of COVID-19 in the form of an extraordinary workload [8]. Nonetheless, the prevalence of COVID-19 among different occupational environments has made the health employees’ fight firsthand and highly personal. In explaining this notion, a study proposed that despite the advancement in healthcare facilities, the healthcare community is experiencing standardized health challenges, thereby overwhelming the worldwide healthcare infrastructure due to its fatality rates [9].
Pakistan is a developing country with a low-level income. The Pakistani private healthcare sector provides better healthcare workers’ services than the public sector [10]. In Pakistan, the first case of coronavirus 2019 (COVID-19) was registered on February 26, 2020. The Pakistan Ministry of National Health Services Regulations & Coordination reacted to the pandemic by setting up a Disease Outbreak Response System. During March 2020, confirmed cases rose from 471 to 12,723, with increased deaths from 0 to 269. Understanding the psychological impact of the COVID-19 outbreak among healthcare workers is crucial in guiding policies and interventions to maintain their psychological well-being [10]. Recent literature has been emerging worldwide in the context of poor psychological wellbeing and mental health issue during COVID-19 [1, 11, 12].
Meanwhile, it is normal for the general population to enter a state of acute stress and depression in such circumstances [13]. Continuous media reporting and discussions strain the public’s mental state; concurrently, healthcare workers cannot maintain their mental health. As the healthcare industry confronts the severe challenge of the COVID-19 pandemic, health workers are struggling to treat the patients infected by this disease [14]. Among medical professionals, frontline workers (nurses and paramedical staff) face particular psychological disturbance because of the frequent demand for professional flexibility with fewer resources in such divested working environments [15]. Significantly, nurses have observed psychological trauma, which has emerged due to the continuous spawning of infection by infected patients [13]. Yet, despite this, nursing professionals are expected to serve patients in the standard approach [16]. This approach requires nursing professionals to build a consistent attitude toward patients uniformly regardless of case severity and circumstances [17]. Psychological rigidity and mental stability are primary considerations for healthcare professionals in maintaining this standard approach to job performance [18]. Arguably, healthcare workers’ mental health is quite significant for their ability to work efficiency, and it assists in maintaining the sustainability of an organization [19, 20]. Specifically, healthcare workers with vigorous mental health will intensify their psychological endurance, which is ultimately beneficial while treating patients.
Moreover, psychological endurance augments innovative capability and assists in taking rapid decisions during a time of havoc or calamity [21, 22]. In this regard, Berry and Mirabito have worked on employee wellness in the workplace and its impact on employee’s productivity and effectiveness [23, 24]. Their study’s main findings indicate that a consistent workload and pressure to meet job duties can affect an employee’s willingness to perform because of poor psychological wellness. These findings support the notion that job performance and professional productivity may decline because of poor mental health. Healthcare workers’ commitment level, performance effectiveness, and efficiency may be affected due to situational anxiety about being infected by COVID-19 and the absence of psychological protection in workplaces. An extensive review of the literature highlights the idea that effective management or conventional tools can no longer help to maintain an employee’s effectiveness and performance capacity in such situations [25]. Thus, the healthcare sector should consider non-conventional approaches to deal with this scenario [26] (and the negative predictors of job performance). Countering performance issues require better psychological protection for employees, plus winning this war against the COVID-19 pandemic. Specific research regarding COVID-19 and healthcare professionals highlights that the threat perception can trigger depression in healthcare workers, especially frontline workers [27]. In addition, organizations have been unable to provide adequate training and psychological support to deal with this pandemic situation. Relevantly, psychological rigidity and felt obligation among healthcare workers can help them attain performance efficiency [28]. Felt obligation is not limited to a single expectation. The various dimensions of felt obligation coexist during the COVID-19, and the influence of each dimension will change according to the specific phase. As a result, this study provides a potential mechanism that can extensively influence healthcare employees’ performance effectiveness. However, due to the rapid growth of COVID-19, it is quite interesting to contemplate the effectiveness of occupational health, which is also vital for workplace wellness and the workforce.
The economic sustainability of an economy’s growth has a significant dependency on the healthcare sector. The development of this sector can positively contribute to the economy [29]. Healthcare occupations are high-pressure and have long working hours [30]. Further, healthcare centers must provide more facilities and services than other service sectors. They have to respond to consumers/patients as soon as possible. In this unpredictable situation of isolation, quarantine, and medical emergency, a country’s healthcare sector significantly influences its economy. It is difficult for an economy to stabilize during and post-COVID-19 without having a stable and robust healthcare sector [31]. Yet, the COVID-19 illness has no regard for the typical structures and processes of the global health sector. As a result, it has become exceptionally challenging for frontline workers to balance their physical and psychological well-being during the pandemic. Hence, it has become essential to develop and ensure heightened health and safety precautions for the healthcare workforce during the crisis. Critically, this study argues that these unwanted ramifications of the pandemic have radically altered the physical and psychological parameters, adversely affecting an individual’s social and physical well-being [32]. In recent months, the immense increase in COVID-19 cases has demoralized the efforts of health professionals, forcing them to work beyond their capabilities.
The current study focuses on providing support to healthcare management, medical professionals, and policy planners in identifying potential parameters and influencing mechanisms. Additionally, this study highlights the need for nurses’ wellness and recognition of their work in these hard times. Therefore, a timely call to action is proposed to explain how psychological distress, depression, anxiety, and stress experienced by healthcare workers have affected their performance effectiveness during this outbreak [1, 20].
2Theoretical framework and hypothesis development
Healthcare professionals are continually facing a major psychological breakdown worldwide because of this current pandemic situation [33]. In this state, where extreme uncertainty, emotional responses, and epidemiological features are present [34], Pakistan’s healthcare professionals have faced inadequate resources and underprepared health facilities [35]. The current focus of hospital management on providing immediate assistance to the patient has shifted their focus from consistent solutions to swift ones. This approach is natural given the demand of the current situation; however, it has a negative impact on employees’ ability to perform their job duties. Having productive and responsible employees and their willingness to perform well are critical factors for many occupational phenomena [36]. Employees’ performance and functionality depend upon their workplace experiences, job demands, and situational factors [37]. The fear of being infected by this dangerous virus has directly affected individuals’ ability to perform their professional duties, particularly in the healthcare sector [33]. An individual’s disease perception is mainly formed by their surroundings, identifying particular disease causes and related consequences [34, 38]. According to the current study, Rüdell’s disease perception model presented the potential factors that can affect an individual’s mental health and ability or willingness to perform some specific tasks. According to this model, societal and cultural interpretations might influence individual perceptions of a particular illness [39]. The current situation is consistent with this model, given the impact of social surroundings. An extensive review of the brief literature shows that it predicted fear of COVID-19 as one of the substantial factors affecting an employee’s willingness to perform in the desired manner [40]. Perception of the threat of COVID-19 is an emerging concept in the healthcare field, where fear of getting infected, stressful thoughts about leaving the profession, and loss of support all affect the phenomenon of job performance [22, 41]. Constant fear of getting infected, mass quarantine, lack of family support, patients’ poor understanding, constant questioning pressure, and mental exhaustion could affect healthcare professionals’ level of performance and productivity [35]. Employees’ perceptions of stressful experiences influence their mental functionality and effective decision-making ability [42, 43]. It mainly affects the psychological well-being (poor mental health and increased depression symptoms) of the healthcare employees, which could affect their performance in this status quo. As related to COVID-19, the threat is manageable through a significant control model containing perceptions, behaviors, and interpretations [44]. To ensure the substantial performance of healthcare workers, understanding the perception of a threat of COVID-19 could be an effective measure [41]. Therefore, based on the brief literature discussed above, the current study proposed that:
H1: Perceptions of the threat of COVID-19 will have direct effects on job performance.
Addressing COVID-19 specific job performance issues concerning organizational support is as vital as planning better control and prevention measures for this pandemic situation [45]. An increase in mortality rate from this novel disease meant mental catastrophe, and low psychological functioning due to fear of being infected became part of every healthcare professional’s statistics [46, 47]. According to Halcomb, providing mental support and confidence to an individual can increase the tendency to deal with challenging and problematic situations [15]. Apart from professional’s duties, psychological protection by management and similar arrangements can minimize the potential harms of the COVID-19 pandemic. Presently, healthcare units (public and private hospitals), including nursing homes, quarantine centers, and community-based hospitals, fail to provide psychological protection to employees [41]. Psychological protective is a construct that measures the provided facilitates and assistance offered by organizations to protect their employees from mental disturbance [48]. This psychological aspect comprises significant mental support, emotional stability, and better mental functionality. The severity of the current pandemic situation increases its detrimental effects on frontline healthcare workers because of the low anticipation of “psychological protection” by organizational management [49]. In this regard, hospital management is accountable for providing psychological protection, just like other physical support factors. In the current situation, the absence of managerial concerns regarding accommodation, care policies, social support, and flexible work schedules could induce stress. Therefore, based on the discussion mentioned above and literature support, it is pragmatically possible to hypothesize that:
H2: Psychological protection will have direct effects on job performance.
This seriousness, massive infection, and invisible danger of the virus has potentially maintained psychological disorders in fear, stress, panic attacks, and depressing thoughts in the general population. This depression and poor mental functioning level could also significantly influence healthcare employees as they continuously face this pandemic situation. Depression symptoms and poor mental health have a long history of affecting individuals’ ability to perform and execute commands [50]. According to the National Institute of Mental Health (2016), depression is a mental depressive disorder that affects an individual’s working abilities, decision functionality, and, most notably, their ability to respond. A recent study about the current pandemic situation has established its findings related to the perception of getting infected [51]. According to Calvillo et al., perception of the threat of COVID-19 can cause mental preoccupation with the worst scenario [52]. The perception of the threat of COVID-19 has been found to be one of the significant predictors of stress, helplessness, eating disorders, and sleep disturbance, particularly in frontline healthcare workers. It is rationally reasonable that since frontline workers are exposed continuously to infected cases, they develop a fear of being infected more than others [47]. The situation is worst in nurses and other support staff who are vulnerable to being infected and often work with inadequate resources [53]. Meanwhile, changes in job duties, poor psychological support, constant pressures, and depressive thoughts impact mental health [35], imposing a negative impact on employees’ job performance and effectiveness [51].
As mentioned, the unavailability of psychological protective measures’ to healthcare professionals has led to them developing psychological abnormalities [54]. The absence of psychological protection as a support mechanism makes it harder for healthcare professionals to uphold their mental health [20]. It is logically and practically understandable that an individual with a constant fear of COVID-19 and inadequate psychological protective measures cannot maintain their performance level, especially when it comes to caring demands [55]. The care and support provided by hospital management, departmental management, and head nurses as psychological protective measures may save employees from depression, stress, and anxiety [55]. Healthcare providers are the only hope for all those suffering from COVID-19, hospital administration, and state governance. Their decision-making power will affect their services to patients as part of their job duties. Therefore, the current study has assumed that increasing depression symptoms and mental pressure are potential underlying mechanisms that could affect a healthcare professional’s performance. As such, this study proposes:
H3: Perceptions of the threat of COVID-19 will have direct effects on depression symptoms.
H4: Psychological protections will have direct effects on depression symptoms.
H5: Depression symptoms mediate the relationship between perceptions of the threat of COVID-19 and employee performance
H6: Depression symptoms mediate the relationship between psychological protections and employee performance.
Evidence suggests that employees with depression and stress symptoms often fail to reach the desired level of performance even when they are capable of it [56]. In Mental Psychology, an individual’s mental capabilities and psychological stability are a more significant consideration than physical suitability for accomplishing job-oriented tasks [57]. In the current situation, frontline healthcare professionals are the most vulnerable individuals in terms of exhibiting depression symptoms that may affect their tendency to respond with optimal performance. It is difficult to understand and exhibit effective performance when experiencing persistent fear and helplessness [58]. However, the literature supports the notion that those who have feelings of obligation, reciprocation, and social exchange might have a different understanding of performance even in depressing situations [59]. In other words, when employees felt obliged toward their organization because of their previous experiences, organizational efforts, and fair treatment, this made them responsible for their job expectations [60]. Felt obligation is a social exchange phenomenon developed when employees feel themselves repaying an organization separately to the situational factors [61]. In the present scenario, the felt obligation of performing responsibilities include (1) accepting the current situation and maintaining responsive contact with infected patients; (2) avoiding any adverse situations in a workplace; (3) providing assistance to those who need their facilities; (4) self-sufficiency, including their independence from the current pandemic situation; and (5) personal sharing regarding workplace issues with the hospital management [61, 62]. An employee’s sense of belonging and strong bond with the organization can minimize the effect of sudden changes (COVID-19), depressing thoughts (Perception of fear of being infected), and negative feelings because of unrealistic attainments (Psychological Protective). The presence of felt obligation in healthcare professionals would help them to maintain their performance, to the level that is required. It could also help develop a shared culture of managing performance in such situations. As such, there is a need to understand the role of “felt obligation” to minimize the effect of depression and its related symptoms on a healthcare individual’s performance [37]. Currently, most of the present literature is targeting the effects of COVID-19. Instead, a focus is required to highlight a prevention model for maintaining individuals’ efforts and minimizing the dangerous effects of the situation faced. Based on its operationalization and functionality between employee’s depression symptoms and performance, the present study hypothesizes that:
H7: Felt obligation weaken the relationship between depression symptoms and job performance.
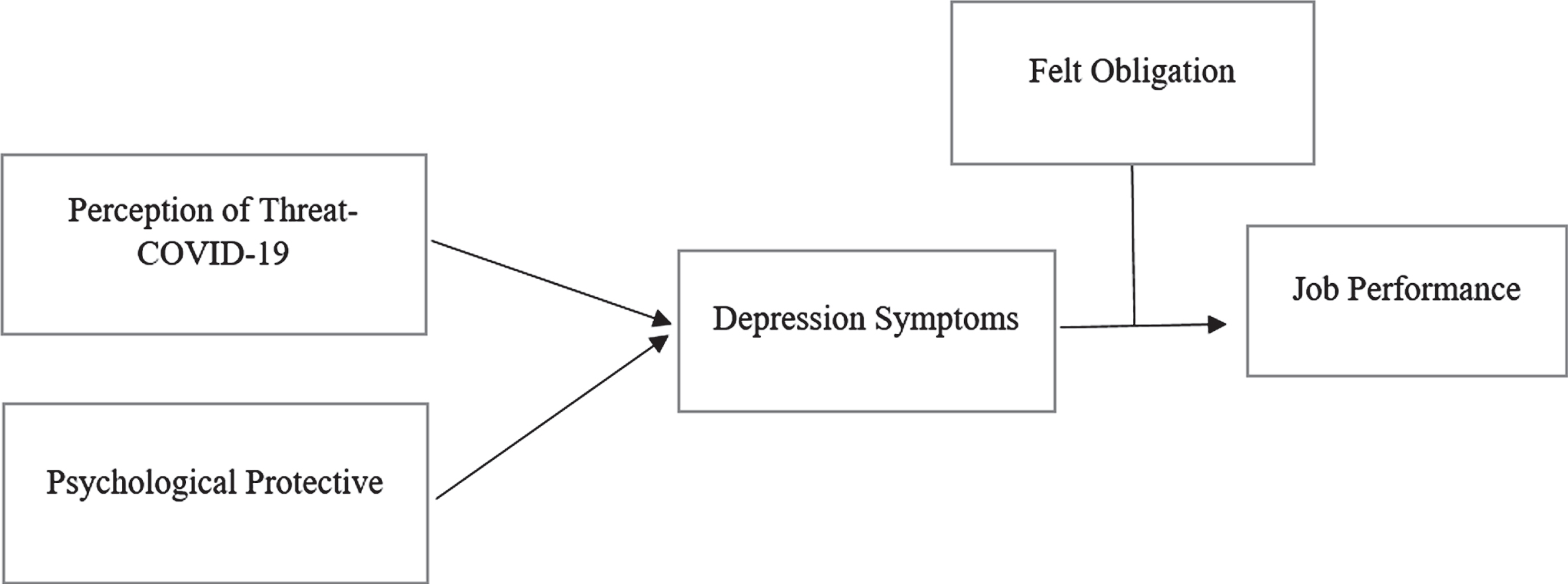
Figure 1 shows the theoretical study framework. Job performance is a dependent variable, and this study’s independent variables are Perception of Threat-COVID-19 and Psychological Protections. Felt obligation is a moderator variable between depression symptoms and job performance.
Fig. 1
Theoretical framework.
3Methodology
3.1Study design
The research objectives were to ascertain the following: a) to what degree can health workers and professionals execute their role despite the prevailing Covid-19 pandemic? b) How effectively are the hospitals’ management providing Personal protective equipment (PPE) kits to ensure a secure environment for their employees to keep them safe from depression and anxiety? The research population consists of health workers and professionals of two metropolises of Pakistan’s critical provinces, including Sindh and Punjab. Sindh has considered it has the most significant number of government hospitals treating COVID-19 patients. In addition, the hospital has all the testing facilities. Punjab was considered for this research as among all the provinces of Pakistan. Punjab has the most significant number of Covid-19 patients in the country. The instrument consisted of sociodemographic information and items from the latent variables, and the scores were evaluated on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). The study participants are directly giving their services to those hospitals where isolation wards are available for COVID-19 patients and COVID-19 test facilities. After developing an English questionnaire, it is sent to the language expert and a local language expert (Urdu). The questionnaire was translated into the local language (Urdu), especially for health workers, including nurses and paramedical staff. Participants were sent a Google questionnaire link via email, WhatsApp, and Viber. The consent form explicitly stated that the participants’ information would be kept confidential and that their participation in the study would not influence their personal or professional life.
All procedures performed were in accord with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standard. The ethical committee approved all the procedures. Informed consent was obtained from all individual participants included in the study.
3.2Study measures
In the current study, Perceptions of COVID-19 threat was measured with five items scale revised [54], and The psychological protective was measured five items scale [41, 54]. The felt obligation scale was measured by seven items adapted from Eisenberger [63]. Items are included (1) I feel a personal obligation to do whatever I can to help my patients cure them. (2) I feel guilty if I did not meet the hospitals’ proper standards. The PHQ-9 items Scale measured depression symptoms. The scale comprised the respondent’s percentage and showed a level of depression and anxiety symptoms. Employee performance was measured with a nine-item questionnaire scale adapted from Abdil gelil Asefa.
3.3Study sample and data collection
In this research, the total population was from two provinces of Pakistan (Punjab and Sindh). The purposive sampling method was applied to gather the primary data based on this aspect. According to Ume Sukan, if the research’s overall population is one million, the sample size must be at least 384 [64]. Since the current study’s total population was lower than a million, roughly 700 questionnaires were distributed online, possibly having a lower return rate than the self-administered survey questionnaire. Of the 700 questionnaires, 490 were received from the participants, thereby registering a 70% return rate. Sekaran and Bougie [64] and Krejcie and Morgan’s [65] sample size specification was attained in the present research.
4Results
Table 1 represents descriptive statics. Data was collected from 490 healthcare workers, out of which 292 are female workers, and 198 are male workers. Most healthcare workers are married and junior doctors with 1-10 years of working experience. Karachi is the epic center of COVID-19 in Pakistan. Two hundred eighty-five healthcare workers participated from Karachi, 120 healthcare workers in Lahore, and 85 workers from other cities.
Table 1
Descriptive of the respondents
| Characteristics | Frequency | Percentage |
| Gender | ||
| Male | 198 | 40.40 |
| Female | 292 | 59.59 |
| Age | ||
| 25 to 35 years | 169 | 34.4 |
| 36 to 45 years | 210 | 42.8 |
| 46 to 55 years | 66 | 13.4 |
| 55 years above | 45 | 9.18 |
| Marital Status | ||
| Single | 126 | 33.2 |
| Married | 335 | 63.3 |
| Others | 29 | 3.47 |
| Job Designation | ||
| Senior Doctors | 120 | 17.3 |
| Junior Doctors | 187 | 32.81 |
| Nurses | 144 | 29.3 |
| Midwives | 25 | 14.6 |
| Others | 14 | 5.7 |
| Education | ||
| Fellow of College of Physicians and Surgeons | 119 | 24.2 |
| Bachelor of Medicine | 118 | 38.3 |
| Nursing Diploma | 101 | 20.6 |
| Health Worker diploma | 46 | 09.3 |
| Others | 36 | 07.3 |
| Work Experience | ||
| 1 to 10 years | 242 | 49.38 |
| 11 to 20 years | 175 | 35.71 |
| 21 to 30 years | 63 | 12.85 |
| Above 30 years | 10 | 02.04 |
| Working Hours | ||
| 6 Hours | 358 | 73.06 |
| 8 Hours | 63 | 12.85 |
| 10 Hours | 00 | 00.00 |
| 12 Hours | 00 | 00.00 |
| Part-time | 40 | 8.16 |
| Location | ||
| Karachi | 85 | 32.81 |
| Lahore | 120 | 46.33 |
| Other | 54 | 20.84 |
The outcomes of Reliability and Validity are mentioned in Table 2, which indicates that all the constructs satisfy the standard for discriminant validity. As per the recommendations of Fornell and Larcker, the discriminant validity was evaluated. According to these authors, every construct’s AVE must be higher than the correlations among the model’s every construct [66].
Table 2
Construct Reliability and Validity
| Construct | Mean | Std | HTMT | VIF | |||||
| DS | EP | FO | POT | PPM | DS | EP | |||
| DS | 3.654 | 0.834 | – | – | – | – | 2.230 | ||
| EP | 3.649 | 0.673 | 0.811 | – | – | – | – | ||
| FO | 3.351 | 0.890 | 0.817 | 0.719 | – | – | 2.230 | ||
| POT | 3.977 | 0.689 | 0.732 | 0.635 | 0.543 | – | 2.561 | ||
| PPM | 4.078 | 0.518 | 0.818 | 0.728 | 0.620 | 0.836 | – | 2.250 | |
DS = Depression Symptoms, EP = Employee performance, FO = Felt Obligation, POT = Perceptions of the threat of COVID-19, PPM = Psychological Protective Measures.
4.1Measurement model results
The outcomes displayed in Table 3 were obtained through the evaluation of the measurement model. Table 3 shows that every loading value should be higher than 0.5, which is the threshold rate [67]. The least average variance value derived must be higher than 0.5 in the present research recommended by Bagozzi and Yie [68]. As per Hair, composite reliability must be higher than 0.7 [69].
Table 3
Measurement model
| Variables | Loadings | CR | AVE |
| Perceptions of the threat of COVID-19 | |||
| POT1 | 0.609 | 0.871 | 0.595 |
| POT2 | 0.739 | ||
| POT3 | 0.822 | ||
| POT4 | 0.790 | ||
| POT5 | 0.725 | ||
| Psychological Protective Measures | |||
| PPM1 | 0.754 | 0.869 | 0.599 |
| PPM2 | 0.831 | ||
| PPM3 | 0.772 | ||
| PPM4 | 0.690 | ||
| PPM5 | 0.768 | ||
| Depression Symptoms | |||
| DS1 | 0.791 | 0.910 | 0.594 |
| DS2 | 0.711 | ||
| DS3 | 0.740 | ||
| DS4 | 0.755 | ||
| DS5 | 0.789 | ||
| DS6 | 0.744 | ||
| DS7 | 0.751 | ||
| DS8 | 0.749 | ||
| DS9 | 0.693 | ||
| Felt Obligation | |||
| FO1 | 0.799 | 0.924 | 0.672 |
| FO2 | 0.810 | ||
| FO3 | 0.824 | ||
| FO4 | 0.847 | ||
| FO5 | 0.833 | ||
| FO6 | 0.796 | ||
| Employee Performance | |||
| EP1 | 0.821 | 0.933 | 0.567 |
| EP2 | 0.782 | ||
| EP3 | 0.754 | ||
| EP4 | 0.778 | ||
| EP5 | 0.739 | ||
| EP6 | 0.845 | ||
| EP7 | 0.687 | ||
| EP8 | 0.710 | ||
| EP9 | 0.734 |
Table 3 represents the study measurement. There are five variables in this study. Perceptions of the threat of COVID-19 have a CR value (0.871) and AVE vale (0.595). Psychological Protective Measures has a CR value (0.869) and AVE value (0.599). Depression Symptoms have a CR value (0.910) and AVE value (0.594). Felt Obligation has a CR value (0.924) and AVE value (0.672). Employee Performance has a CR value (0.933) and AVE value (0.567).
4.2Structural model results
A bootstrapping procedure with 5,000 re-samples was executed to generate the t values for 490 questionnaires [70, 71]. The bootstrapping technique produces more reasonable standard error estimates [72, 72].
Table 4 presents the results of the hypothesis. The results have indicated that the relationship between Perceptions of the threat of COVID-19 and depression symptoms is significant (β= 0.242, p < 0.004); therefore, hypothesis 1 is supported while the relationship between the second hypothesis Psychological Protective Measures, and depression symptoms is also significant (β = 0.559, p < 0.00). Moreover, the statistical link between depression symptoms and employee performance has also proved statistically significant (β = 0.62, p < 0.00); hence, hypothesis 3 is also supported.
Table 4
Path coefficients (structural model path coefficients)
| Hypothesis | Model | Employee performance | CI 5% | CI95% | |||
| Beta | T | Sig. | Results | ||||
| H1 | POT > DS | 0.242 | 3.021 | 0.004 | Supported | 0.089 | 0.444 |
| H2 | PPM > DS | 0.559 | 8.133 | 0.000 | Supported | 0.444 | 0.759 |
| H3 | DS > EP | 0.626 | 10.61 | 0.000 | Supported | 0.519 | 0.701 |
| H4 | POT > DS > EP | 0.131 | 2.790 | 0.003 | Supported | 0.078 | 0.399 |
| H5 | PPM > DS > EP | 0.347 | 6.330 | 0.000 | Supported | 0.239 | 0.439 |
Table 5 describes hypotheses testing for moderating effects. The H7 is significant at 0.004. This study has identified a meaningful negative relationship between depression symptoms and employee performance, inconsistent with past studies. In the current scenario, due to COVID-19 felt obligation, it has been used as a moderator in the present study. A moderator’s role is weakening the relationship between depression symptoms and employee performance. Table 6 shows the model fit summary.
Table 5
Hypotheses testing for moderating effects
| Hypothesis | Model | Employee performance | CI 5% | CI95% | |||
| Beta | t | Sig. | Results | ||||
| H7 | DS*FO > EP | 0.016 | 0.345 | 0.004 | Supported | 0.034 | 0. 380 |
Table 6
Models fit summary
| Fitness criteria | Measurement model | Acceptable range* |
| CMIN/DF | 2.64 | 1–3 |
| GFI | 0.988 | > 0.90 |
| AGFI | 0.873 | > 0.80 |
| CFI | 0.967 | > 0.95 |
| TLI | 0.919 | > 0.90 |
| NFI | 0.932 | > 0.90 |
| RMR | 0.0413 | < 0.09 |
| RMSEA | 0.520 | < 0.08 |
5Discussion
COVID-19 has affected professionals’ capacity to work in these severe conditions. The magnitude and transmission of this impact are strongly negative on frontline healthcare workers. This negative transmission has potentially arisen because of managerial negligence and lack of rapid responses to employees’ concerns. The current study’s findings highlight the need for flexible, adjustable policies and protocols that can play a vital role in reducing nosocomial infection. This is critical as the risk of getting a virus is the main factor imposing pressure on frontline healthcare workers because of their constant and close involvement with COVID-19-affected patients. In this regard, the perception of fear of being infected from COVID-19 is strongly affecting the nurse’s performance at work. The effect is not limited to job duties. However, it also affects their willingness to continue this profession in the future. In addition, the role of psychological protection from healthcare units’ management has been significantly absent in these difficult times. Psychological protection is somehow a new concept to healthcare employees that needs to be understood from the respondents’ side. However, understanding this poor managerial support of frontline healthcare workers points particularly to the absence of psychological protection during COVID-19. Overall, the perception of the likelihood of getting affected and poor psychological protection have noticeably influenced performance standards. Such a negative impression of the situation and the related pressures are potentially occurring because of frontline healthcare workers’ poor psychological and mental health. The presence of depression symptoms associated with COVID-19 infection significantly explains the reason for increased poor performance.
Meanwhile, several young medical staff members infected with COVID-19 whose cases appeared to be mild at the early stage of the disease recently sharply deteriorated and died, further increasing depression symptoms among colleagues in the field. Such factors are causing significant psychosocial stress for medical staff. Constant psychological stress tends to affect workers’ ability to perform even regular tasks. The reason for poor performance by frontline healthcare workers is the mental stress and risk they are confronting in the workplace. Nurses who have a higher absence of psychological protection tend to show more frequent symptoms of anxiety, discomposure, and restlessness. Furthermore, nurses should be protected and evaluated the first moment they feel any discomfort; those with anxiety or insomnia symptoms should be encouraged to seek psychotherapists’ help.
5.1Study implications
The presence of psychological protection and safety from the COVID-19 threat would have strong implications for Hospital administration and policy advisers. The major problem that hospital management and administration have been facing is the fear of getting infected. This study is providing through-provoking managerial implications to provide psychological support to their employees. The tendency to support employees would give a chance to health care management to achieve optimal performance at healthcare units. This study can be implemented in similar scenarios, where employees’ well-being and mental health are needed to stay resilient.
Moreover, its importance for policy planners and executors is suggestively higher. Maintaining psychological protection among healthcare professionals is integral to develop as a central policy for healthcare units. This study has implications for healthcare managers and unit heads in terms of recognizing the importance of psychological support for professionals in avoiding occupational deficiencies. These are regarded as pillars responsible for regulating supportive culture and ensuring a certain level of job performance in healthcare employees. Furthermore, this study would provide valuable insight into financial entitlements, which can occur in the form of paid leaves, insurance claims, medical assistance, and a loss of skilled and experienced human resources.
6Conclusions
The unprecedented outbreak of Covid-19 has affected the psychological wellness of frontline healthcare workers. However, professional pressure, ethical considerations, and feelings of obligations are pushing them to serve those in need. They are predominately struggling psychologically due to the required assistance not being provided because of the emotional challenges and resource scarcity. The presence of fear of being infected and the lack of protective measures in place significantly affect their performance. The current model particularly highlights an individual’s feelings of obligation as crucial to maintaining their performance level by minimizing the effect of depression and professional anxiety. The present study’s extensively described the psychological constraints healthcare workers have faced during the pandemic situation.
Further healthcare employees’ mental health is vital for better prevention and control during pandemic circumstances. It is also evident that peer support and sharing behaviors could reduce the overall effects of mental stress in the healthcare field due to the Covid-19 situation. The current approach will provide eye-opening insights that recognize individuals’ valuable efforts during this crisis period. The study provides valuable contributions, but some limitations need to be addressed in future studies. First, the study was conducted during the lockdown period in Pakistan, and data was collected from the two provinces. In further studies, the data can be cross-national. Secondly, the current study has considered only one moderator variable: felt obligation; future studies may consider other variables such as COVID-19 vaccine and satisfaction with organization COVID-19 responses.
Conflict of interest
The authors declare no conflict of interest.
Data Availability
The data that support the findings of this study are available from the corresponding authors upon reasonable request.
Funding
This research received no external funding.
References
[1] | Li H , Hafeez H , Zaheer MA . COVID-19 and Pretentious Psychological Well-Being of Students: A Threat to Educational Sustainability. Frontiers in Psychology. (2020) ;11: (1):4034. |
[2] | Wu Y-C , Chen C-S , Chan Y-J . The outbreak of COVID-19: an overview. Journal of the Chinese Medical Association. (2020) ;83: (3):217. |
[3] | Sun N , Wei L , Shi S , Jiao D , Song R , Ma L , et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. American Journal of Infection Control. (2020) ;48: (6):592–8. |
[4] | Duan L , Zhu G . Psychological interventions for people affected by the COVID-19 epidemic. The Lancet Psychiatry. (2020) ;7: (4):300–2. |
[5] | Danesh MK , Garosi E , Golmohamadpour H . The COVID-19 Pandemic and nursing challenges: A review of the early literature. Work. 2021;(Preprint):1-14. |
[6] | Arca M , Dönmezdil S , Durmaz ED . The effect of the COVID-19 Pandemic on anxiety, depression, and musculoskeletal system complaints in healthcare workers. Work. 2021;(Preprint):1-8. |
[7] | Potas N , Koçtürk N , Toygar SA . Anxiety effects on quality of life during the COVID-19 outbreak: A parallel-serial mediation model among nurses in Turkey. Work. 2021; (Preprint):1-9. |
[8] | Ünal Ö . During COVID-19, which is more effective in work accident prevention behavior of healthcare professionals: Safety awareness or fatalism perception? Work. 2020;(Preprint):1-8. |
[9] | Prabhu N , Issrani R . Dilemma in the foreign lands during COVID-19: An outlook of expat health care professionals with a take on a social perspective. Work. 2020; (Preprint):1-4. |
[10] | Waris A , Khan AU , Ali M , Ali A , Baset A . COVID-19 outbreak: current scenario of Pakistan. NewMicrobes and New Infections. 2020;100681. |
[11] | Aksoy YE , Koçak V . Psychological effects of nurses and midwives due to COVID-19 outbreak: The case of Turkey. Archives of Psychiatric Nursing. (2020) ;34: (5):427–33. |
[12] | Choi KR , Skrine Jeffers K , Cynthia Logsdon M . Nursing and the novel coronavirus: Risks and responsibilities in a global outbreak. Journal of Advanced Nursing. (2020) ;76: (7):1486–7. doi: 10.1111/jan.14369 |
[13] | While A , Nightingale F . The COVID-19 challenge. British Journal of Community Nursing. (2020) ;25: (5):258. |
[14] | Labrague LJ , de Los Santos JAA . Fear of Covid-19, psychological distress, work satisfaction and turnover intention among frontline nurses. Journal of Nursing Management. 2020; |
[15] | Halcomb E , Williams A , Ashley C , McInnes S , Stephen C , Calma K , et al. The support needs of Australian primary health care nurses during the COVID-19 pandemic. Journal of Nursing Management. (2020) ;28: (7):1553–60. |
[16] | Gupta M , Sharma P . Job satisfaction level among employees: a case study of Jammu region, J&K. IUP Journal of Management Research. (2009) ;8: (5):17. |
[17] | Kalateh Sadati A , Zarei L , Shahabi S , Heydari ST , Taheri V , Jiriaei R , et al. Nursing experiences of COVID-19 outbreak in Iran: A qualitative study. Nursing Open. (2021) ;8: (1):72–9. |
[18] | Glasper A . Potential global pandemics: the role of the WHO and other public health bodies. British Journal of Nursing. (2020) ;29: (5):322–3. |
[19] | Shaw SCK . Hopelessness, helplessness and resilience: the importance of safeguarding our trainees’ mental wellbeing during the COVID-19 pandemic. Nurse Education in Practice. (2020) ;44: :102780. |
[20] | Dickson C , McVittie C , Smith MC . Being conductor of the orchestra: an exploration of district nursing leadership. British Journal of Community Nursing. (2020) ;25: (5):214–21. |
[21] | Al-Rawashdeh S , Alshraifeen A , Alhawamdih S , Ashour A . Wellbeing and quality of life of family caregivers: influence of sleep quality. British Journal of Community Nursing. (2020) ;25: (2):70–5. |
[22] | Khosravi M . Perceived Risk of COVID-19 Pandemic: The Role of Public Worry and Trust. Electron J Gen Med. (2020) ;17: (4):em203.2020. |
[23] | Berry L , Mirabito AM , Baun W . What’s the hard return on employee wellness programs? Harvard Business Review. 2010;2012-68. |
[24] | Mirabito AM , Berry LL . You say you want a revolution? Drawing on social movement theory to motivate transformative change. Journal of Service Research. (2015) ;18: (3):336–50. |
[25] | Hafeez H , Abdullah MI , Riaz A , Shafique I . Prevention of occupational injuries and accidents: A social capital perspective. Nursing Inquiry. (2020) ;27: (4):e12354. |
[26] | Samur M , Seren Intepeler S . Nurses’ view of their work environment, health and safety: A qualitative study. Journal of Nursing Management. (2019) ;27: (7):1400–8. |
[27] | Houghton C , Meskell P , Delaney H , Smalle M , Glenton C , Booth A , et al. Barriers and facilitators to healthcare workers’ adherence with infection prevention and control (IPC) guidelines for respiratory infectious diseases: a rapid qualitative evidence synthesis. Cochrane Database of Systematic Review. (2020) ;(4). https://doi.org//10.1002/14651858.CD013582 |
[28] | Bajnok I , Puddester D , Macdonald C , Archibald D , Kuhl D . Building positive relationships in healthcare: Evaluation of the teams of interprofessional staff interprofessional education program. Contemporary Nurse. (2012) ;42: (1):76–89. |
[29] | Xiao H , Zhang Y , Kong D , Li S , Yang N . The effects of social support on sleep quality of medical staff treating patients with coronavirus disease 2019 (COVID-19) in January and February in China. International Medical Journal of Experimental and Clinical Research. (2020) ;26: :e923549–1. |
[30] | Bojner Horwitz E , Grape Viding C , Rydwik E , Huss E . Arts as an ecological method to enhance quality of work experience of healthcare staff: a phenomenological-hermeneutic study. International Journal of Qualitative Studies on Health and Well-Being. (2017) ;12: (1):1333898. |
[31] | Yang Y , Li W , Zhang Q , Zhang L , Cheung T , Xiang Y . Challenge of mental health services for older adults during the 2019-nCoV outbreak. The Lancet Psychiatry. (2020) ;7: (4):e19. |
[32] | Soheili S , Shariat A , Anastasio AT . Modification of existing occupational therapeutic protocols in response to the ‘new normal’after COVID-19. Work. (2020) ;66: (3):477–8. |
[33] | Xiang Y-T , Yang Y , Li W , Zhang L , Zhang Q , Cheung T , et al. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. The Lancet Psychiatry. (2020) ;7: (3):228–9. |
[34] | Beléndez M , Bermejo Alegría RM , García Ayala MD . Estructura factorial de la versión española del Revised Illness Perception Questionnaire en una muestra de hipertensos. (2005) ;17: (2):318–324. |
[35] | Rana W , Mukhtar S , Mukhtar S . Mental health of medical workers in Pakistan during the pandemic COVID-19 outbreak. Asian Journal of Psychiatry. (2020) ;51: :102080. |
[36] | Anitha J . Determinants of employee engagement and their impact on employee performance. International Journal of Productivity and Performance Managemen. (2014) ;63: (3):308–23. |
[37] | Prasad KD V , Vaidya RW . Association among Covid-19 parameters, occupational stress and employee performance: An empirical study with reference to Agricultural Research Sector in Hyderabad Metro. Sustainable Humanosphere. (2020) ;16: (2):235–53. |
[38] | Broadbent E , Wilkes C , Koschwanez H , Weinman J , Norton S , Petrie KJ . A systematic review and meta-analysis of the Brief Illness Perception Questionnaire. Psychology & Health. (2015) ;30: (11):1361–85. |
[39] | Rüdell K , Bhui K , Priebe S . Concept, development and application of a new mixed method assessment of cultural variations in illness perceptions: Barts Explanatory Model Inventory. Journal of Health Psychology. (2009) ;14: (2):336–47. |
[40] | Lai C-C , Shih T-P , Ko W-C , Tang H-J , Hsueh P-R . Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and corona virus disease-2019 (COVID-19): the epidemic and the challenges. International Journal of Antimicrobial Agents. 2020;105924. |
[41] | Zhu Z , Xu S , Wang H , Liu Z , Wu J , Li G , et al. COVID-19 inWuhan: Immediate Psychological Impact on 5062 Health Workers. MedRxiv. 2020; |
[42] | Ibuka Y , Chapman GB , Meyers LA , Li M , Galvani AP . The dynamics of risk perceptions and precautionary behavior in response to 2009 (H1N1) pandemic influenza. BMC Infect Dis. (2010) ;10: (1):296. |
[43] | van der Weerd W , Timmermans DRM , Beaujean DJMA , Oudhoff J , van Steenbergen JE . Monitoring the level of government trust, risk perception and intention of the general public to adopt protective measures during the influenza A (H1N1) pandemic in the Netherlands. BMC Public Health. (2011) ;11: (1):575. |
[44] | Pérez-Fuentes del M C , Molero Jurado del M M , Oropesa Ruiz NF , Martos Martínez Á , Simón Márquez del M M , Herrera-Peco I , et al. Questionnaire on Perception of Threat from COVID-19. Journal of Clinical Medicine. (2020) ;9: (4):1196. |
[45] | Banerjee D . The COVID-19 outbreak: Crucial role the psychiatrists can play. Asian Journal of Psychiatry. (2020) ;50: :102014. |
[46] | Kang L , Li Y , Hu S , Chen M , Yang C , Yang BX , et al. The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. The Lancet Psychiatry. (2020) ;7: (3):e14. |
[47] | Xiao C . A novel approach of consultation on novel coronavirus (COVID-19)-related psychological and mental problems: structured letter therapy. Psychiatry Investigation. (2020) ;17: (2):175. |
[48] | Leong F , Park YS , Kalibatseva Z . Disentangling immigrant status in mental health: Psychological protective and risk factors among Latino and Asian American immigrants. American Journal of Orthopsychiatry. (2013) ;83: (2pt3):361–71. |
[49] | Dai Y , Hu G , Xiong H , Qiu H , Yuan X . Psychological impact of the coronavirus disease 2019 (COVID-19) outbreak on healthcare workers in China. MedRxiv. 2020 Jan 1. |
[50] | Myklestad I , Røysamb E , Tambs K . Risk and protective factors for psychological distress among adolescents: a family study in the Nord-Trøndelag Health Study. Soc Psychiatry Psychiatr Epidemiol. (2012) ;47: (5):771–82. |
[51] | Pérez-Fuentes del M C , Molero Jurado MDM , Martos Martínez Á , Gázquez Linares JJ . Threat of COVID-19 and emotional state during quarantine: Positive and negative affect as mediators in a cross-sectional study of the Spanish population. PLoS One. (2020) ;15: (6):e0235305. |
[52] | Calvillo DP , Ross BJ , Garcia RJB , Smelter TJ , Rutchick AM . Political ideology predicts perceptions of the threat of covid-19 (and susceptibility to fake news about it). Social Psychological and Personality Science. (2020) ;11: (8):1119–28. |
[53] | Li G , Miao J , Wang H , Xu S , Sun W , Fan Y , Zhang C , Zhu S , Zhu Z , Wang W . Psychological impact on women health workers involved in COVID-19 outbreak in Wuhan: a cross-sectional study. Journal of Neurology, Neurosurgery & Psychiatry. (2020) ;91: (8):895–7. |
[54] | Zhou F , Yu T , Du R , Fan G , Liu Y , Liu Z , Xiang J , Wang Y , Song B , Gu X , Guan L . Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. The Lancet. (2020) ;395: (10229):1054–62. |
[55] | Kong X , Zheng K , Tang M , Kong F , Zhou J , Diao L , Wu S , Jiao P , Su T , Dong Y . Prevalence and factors associated with depression and anxiety of hospitalized patients with COVID-19. MedRxiv. 2020 Jan 1. |
[56] | Mulfinger N , Sander A , Stuber F , Brinster R , Junne F , Limprecht R , Jarczok MN , Seifried-Dübon T , Rieger MA , Zipfel S , Peters M . Cluster-randomised trial evaluating a complex intervention to improve mental health and well-being of employees working in hospital-a protocol for the SEEGEN trial. BMC Public Health. (2019) ;19: (1):1–6. |
[57] | Maben J , Taylor C , Bridges J . Guidance to support nurses’ psychological well-being during Covid-19 crisis. 2020. https://eprints.soton.ac.uk/439503/1/Guidance_to_support_nurses_psychological_well_being_during_Covid_19_crisis_14.04.2020.pdf |
[58] | Grace MK , VanHeuvelen JS . Occupational variation in burnout among medical staff: evidence for the stress of higher status. Social Science & Medicine. (2019) ;232: :199–208. |
[59] | Roch SG , Shannon CE , Martin JJ , Swiderski D , Agosta JP , Shanock LR . Role of employee felt obligation and endorsement of the just world hypothesis: A social exchange theory investigation in an organizational justice context. Journal of Applied Social Psychology. (2019) ;49: (4):213–25. |
[60] | Colquitt JA , Scott BA , Rodell JB , Long DM , Zapata CP , Conlon DE , et al. Justice at the millennium, a decade later: A meta-analytic test of social exchange and affect-based perspectives. Journal of Applied Psychology. (2013) ;98: (2):199. |
[61] | Corso Del AR , Lanz M . Felt obligation and the family life cycle: A study on intergenerational relationships. International Journal of Psychology. (2013) ;48: (6):1196–200. |
[62] | Abraham KM , Stein CH . Staying connected: Young adults’ felt obligation toward parents with and without mental illness. Journal of Family Psychology. (2010) ;24: (2):125. |
[63] | Eisenberger R , Armeli S , Rexwinkel B , Lynch PD , Rhoades L . Reciprocation of perceived organizational support. Journal of Applied Psychology. (2001) ;86: (1):42. |
[64] | Sekaran U , Bougie R . Research methods for business: A skill building approach. John Wiley & Sons; (2016) . |
[65] | Krejcie RV , Morgan DW . Determining sample size for research activities. Educational and Psychological Measurement. (1970) ;30: (3):607–10. |
[66] | Fornell C , Bookstein FL . Two structural equation models: LISREL and PLS applied to consumer exit-voice theory. Journal of Marketing Research. (1982) ;19: (4):440–52. |
[67] | Chin WW . The partial least squares approach to structural equation modeling. Modern Methods for Business Research. (1998) ;295: (2):295–336. |
[68] | Bagozzi RP , Yi Y . On the evaluation of structural equation models. Journal of the Academy of Marketing Science. (1988) ;16: (1):74–94. |
[69] | Hair JF , Ringle CM , Sarstedt M . Partial least squares structural equation modeling: Rigorous applications, better results and higher acceptance. Long Range Plann. (2013) ;46: (1–2):1–12. |
[70] | Hair JF , Ringle CM , Sarstedt M . Partial least squares: the better approach to structural equation modeling? Long Range Planning. (2012) ;45: (5–6):312–9. |
[71] | Henseler J , Ringle CM , Sinkovics RR . The use of partial least squares path modeling in international marketing. In New Challenges to International Marketing. (2009) ;20: (1):277–319. |
[72] | Tenenhaus M , Vinzi VE , Chatelin Y-M , Lauro C . PLS path modeling. Computational Statistics & Data Analysis. (2005) ;48: (1):159–205. |


