
A systematic review and meta-analysis of educational interventions for children and adolescents with acquired brain injury
Abstract
BACKGROUND:
Children with brain injuries face significant challenges in their recovery. One of the greatest is transitioning from hospital/home to school where they face issues such as reintegration, lack of understanding and catching up with missed work. Many children struggle with their altered circumstances and require additional supports to meet the academic demands of systems which are ill equipped to teach them.
OBJECTIVE:
To summarise the best available evidence for the use of educational interventions to improve academic attainment in childhood survivors of acquired brain injury (ABI).
METHODS:
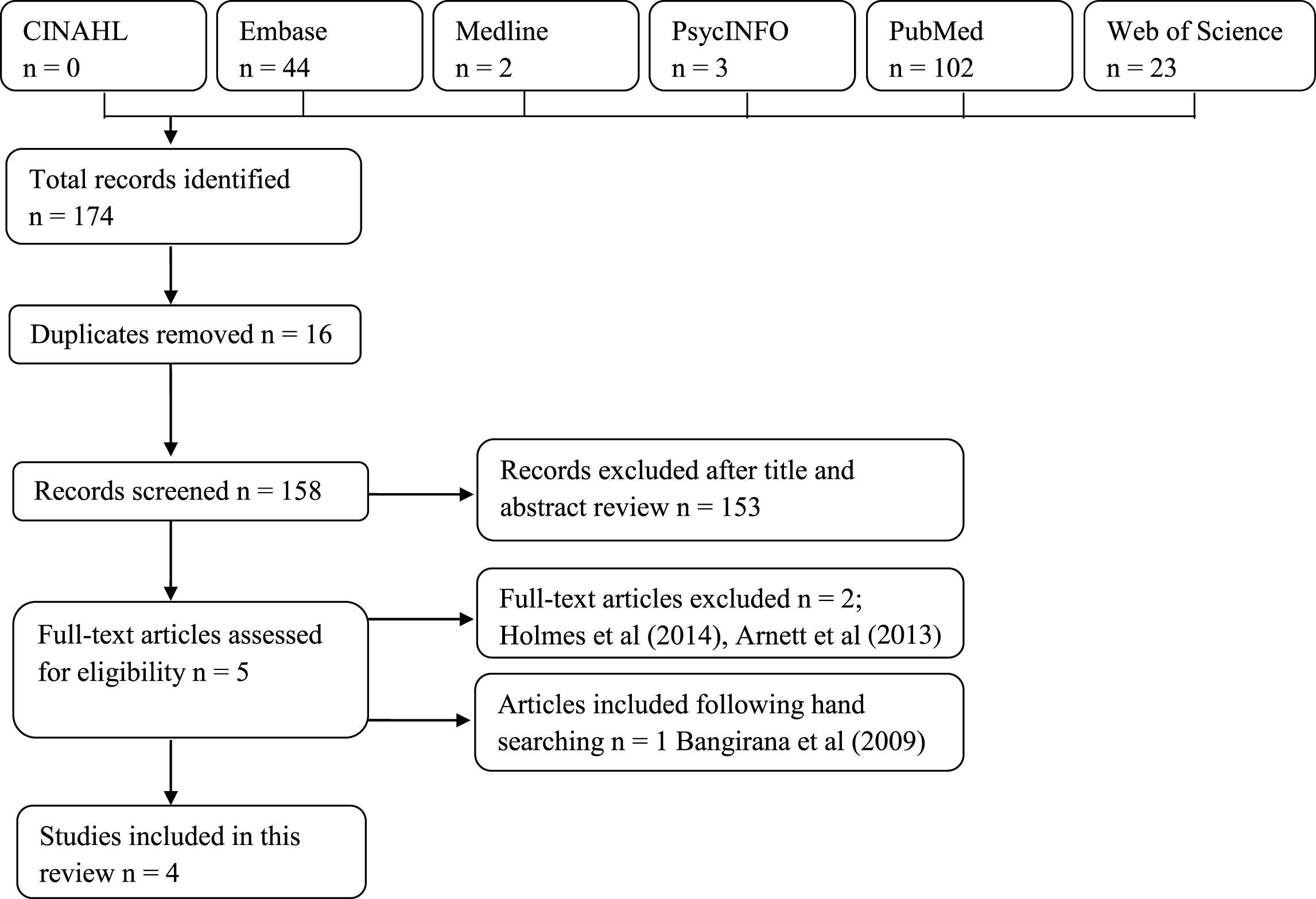
Six electronic databases (Cinahl, Embase, Medline, PsycINFO, Pubmed, & Web of Science) were systematically searched for randomised controlled trials published between 1980 and 2017. Two authors independently reviewed these studies and extracted data on type of intervention, characteristics of participants, outcome measures, findings and recommendations. The Cochrane Collaboration’s Risk of Bias tool was used to assess systematic error in the included studies.
RESULTS:
Four studies met the inclusion criteria (n = 296 children and adolescents). Three studies (n = 287) were included in meta-analysis for the primary outcome which showed no statistically significant difference between the intervention and control conditions on academic attainment (SMD 1.31, 95% CI –0.06 to 2.68, p = 0.06). No statistically significant differences were found which favoured the intervention for the secondary outcomes of attention, internalising or externalising behavior. All effect sizes were considered as small.
CONCLUSIONS:
This review suggests that no currently effective educational interventions exist for children with ABI. Greater efforts are required to produce effective and rigorously tested interventions to improve outcomes for these children.
1Introduction
Return to school following brain injury creates challenges for both the child and the teacher. The child may now have difficulties with behavior (Hawley, Ward, Magnay, & Mychalkiw, 2004), cognition (Anderson, Catroppa, Morse, Haritou, & Rosenfeld, 2005; Halstead et al., 2013; Kurowski et al., 2013) and emotion (Limond, Dorris, & McMillan, 2009; Tonks et al., 2009) which are often long lasting (McKinlay, Dalrymple-Alford, Horwood, & Fergusson, 2002) and negatively affect academic performance (Anderson, Brown, Newitt, & Hoile, 2011; Ransom et al., 2015). Despite the problems faced following injury, children often transition back to school with inadequate supports (Dettmer, Ettel, Glang, & McAvoy, 2013). Further, even if the child’s classroom teacher is informed about the injury, they are unlikely to have received training about what to expect and so may be ill-equipped to meet the child’s needs (Ettel, Todis, & Davies, 2016; Glang et al., 2015). Transitions between school grades, or moving to a new school, can mean the child loses the support of a teacher familiar with their challenges, whilst gaining a new teacher who lacks experience of providing accommodations for a child with brain injury (Hawley et al., 2004). Given the impact of poor educational outcomes on future prospects (Anderson, Brown, Newitt, & Hoile, 2009), it is important that effective interventions are developed that will support the academic achievement of children with brain injury.
The school system is generally viewed as the most natural environment for a child to meet their educational, social and often behavioral needs. However, successful transition to school requires educational interventions which are appropriately developed and delivered. A recent systematic review of parent experiences reported that a number of school factors impede successful integration for children with brain injury. These included: a lack of teacher knowledge, teachers having low expectations of the child with brain injury, or holding negative views towards the child, and/or teachers taking a “wait and see” approach and not attending planning meetings (Andersson et al., 2016). Clinicians and educators echo these same themes, and also note other challenges that affect the quality of educational services for children (e.g., poor communication between medical and educational professionals, lack of clear policies and procedures to guide transition from hospital to school) (Hartman, Duncanson, & Farahat, 2015).
To be effective, teachers need an understanding of the impact of the brain injury on the child’s ability to function in the classroom, both in terms of the environment (e.g. noise, light and distractions associated with a busy classroom), the specific challenges the child experiences, and the social needs that a child with brain injury has. Although many strategies used with children with similar functional impairments can be effective in addressing these challenges (Glang, Ylvisaker, Stein, & Ehlhardt, 2008; Ylvisaker et al., 2001, 2005), teachers can benefit from learning how to modify academic, behavioral and social support strategies for children with brain injury. Further, for a child with brain injury to function effectively, the teacher requires information regarding the roles of other professionals involved in the child’s care, as well as their own role within this team. Long-term, teachers need to be aware of how the brain injury will interact with the expected developmental trajectory of the child, and adapt any educational inputs and strategies to suit these changes (McKinlay et al., 2016). It is clear that the challenges faced by the teacher in supporting a child with brain injury are extensive.
Emerging research of educational interventions that target social, behavioral, academic, and cognitive domains provide limited information regarding their overall effectiveness. The objective of this review was to assess the effectiveness of educational interventions on the academic attainment, as well as cognitive, behavioral and emotional outcomes, for children with acquired brain injuries. The review benefits from the experience of three international authors who provide perspectives from four unique educational contexts (i.e. Australia, New Zealand, UK and USA).
2Methods
2.1Search strategy
Electronic databases (Cinahl, Embase, Medline, PsycINFO, Pubmed, Web of Science) were systematically searched in July 2017. These databases were selected due to their focus on empirical research addressing education and medical conditions. Search terms were selected from the existing literature to reflect the population and outcomes of interest. To ensure the highest level of evidence from selected studies we chose only to include those which employed randomised controlled trial (RCT) designs. We sought to include studies which made reference to acquired brain injury to allow for sufficient scope. Acquired brain injury generally encompasses any type of brain damage that occurs following birth, including oxygen deprivation, accident, stroke, substance abuse, infection or trauma. The reference lists of included studies were screened for relevant articles. The search terms utilised were as follows:
school age* OR pediatric* OR youth OR teen* OR adolescen* OR student* OR pupil* OR child* OR elementary education OR high school OR primary education OR elementary school OR middle school OR primary school.
AND
brain injur* OR head injur* OR brain tumor* OR stroke* OR aneurysm* OR anoxi* OR hypoxi* OR concussion* OR TBI OR mTBI.
AND
clinical trial OR randomized controlled trial OR controlled clinical trial.
AND
academic success OR academic achievement OR academic performance.
2.2Inclusion and exclusion criteria
Our review included publications which evaluated the use of an educational intervention on the academic attainment of children and adolescents with acquired brain injuries. We defined educational intervention as any programme which sought to improve performance on measures of learning e.g. reading, mathematics etc. The intervention may be delivered by researchers, teachers, parents or peers or may be undertaken independently. We made the decision to accept studies which made comparison between the intervention and placebo conditions, the interventions and no treatment conditions and studies which compared two or more types of intervention. As stated above, we wished to review the best available evidence for the effectiveness of educational interventions and so limited our review to RCTs. These could include parallel RCTs, cluster randomised trials or the first phase of randomised cross-over trials. Due to limited resources, we elected to exclude studies which were published in languages other than English.
2.3Selection of included studies
Two authors independently reviewed the titles and abstracts of publications as identified by the search strategy. Any duplicates were removed and both authors reviewed the resulting selection to determine which publications met the inclusion criteria. Those articles deemed most suitable were then retrieved for comprehensive review. In the case of disagreement, the third author made the final decision on the publication’s inclusion. See Fig. 1 for a flowchart of study inclusion.
Fig.1
Flowchart of included studies.
2.4Data extraction and risk of bias
Data extraction was independently conducted by two review authors through use of a standardised data extraction tool created for this review. The tool was piloted prior to use with the included studies to determine any existing problems which were then addressed and refined. When the team felt the tool sufficiently covered the requisite areas, data extraction commenced. In the case of disagreement the third author made the final decision. Where possible we chose to record data on; type of intervention; characteristics of intervention and control participants (e.g. age, gender, severity and type of injury); sample size; outcome measures; study findings & recommendations.
2.5Primary outcome
The primary outcome of interest was academic achievement as measured by psychometrically validated tools. These included tests such as the Wide Range Achievement Test-third edition (Wilkinson 1993), the California Verbal Learning Test – Children’s Version (Delis, Kramer, Kaplan, & Ober, 1994), and any other validated tool.
2.6Secondary outcomes
Included any behavioral, cognitive, or emotional outcome which could impact on academic attainment and was measured by use of psychometrically validated tools. These comprised tests which measured behavior, for example, the Child Behavior Checklist (Achenbach & Rescorla, 2000) or the Strengths and Difficulties Questionnaire (Goodman 1997) aspects of cognition such as memory (e.g. The Rivermead Behavioral Memory Test for Children; Wilson, Ivani-Chalian, & Aldrich, 1991), executive functioning (e.g. Behavior Rating Inventory of Executive Functioning; Gioia, Isquith, Guy, & Kenworthy, 2000), attention (e.g. Wechsler Intelligence Scale for Children-fourth edition; Kaplan, Fein, Kramer, Delis, & Morris, 2000), and emotion (e.g. Child Behavior Checklist; Affect Intensity Scale; Achenbach & Rescorla, 2000; Eisenberg et al., 2016).
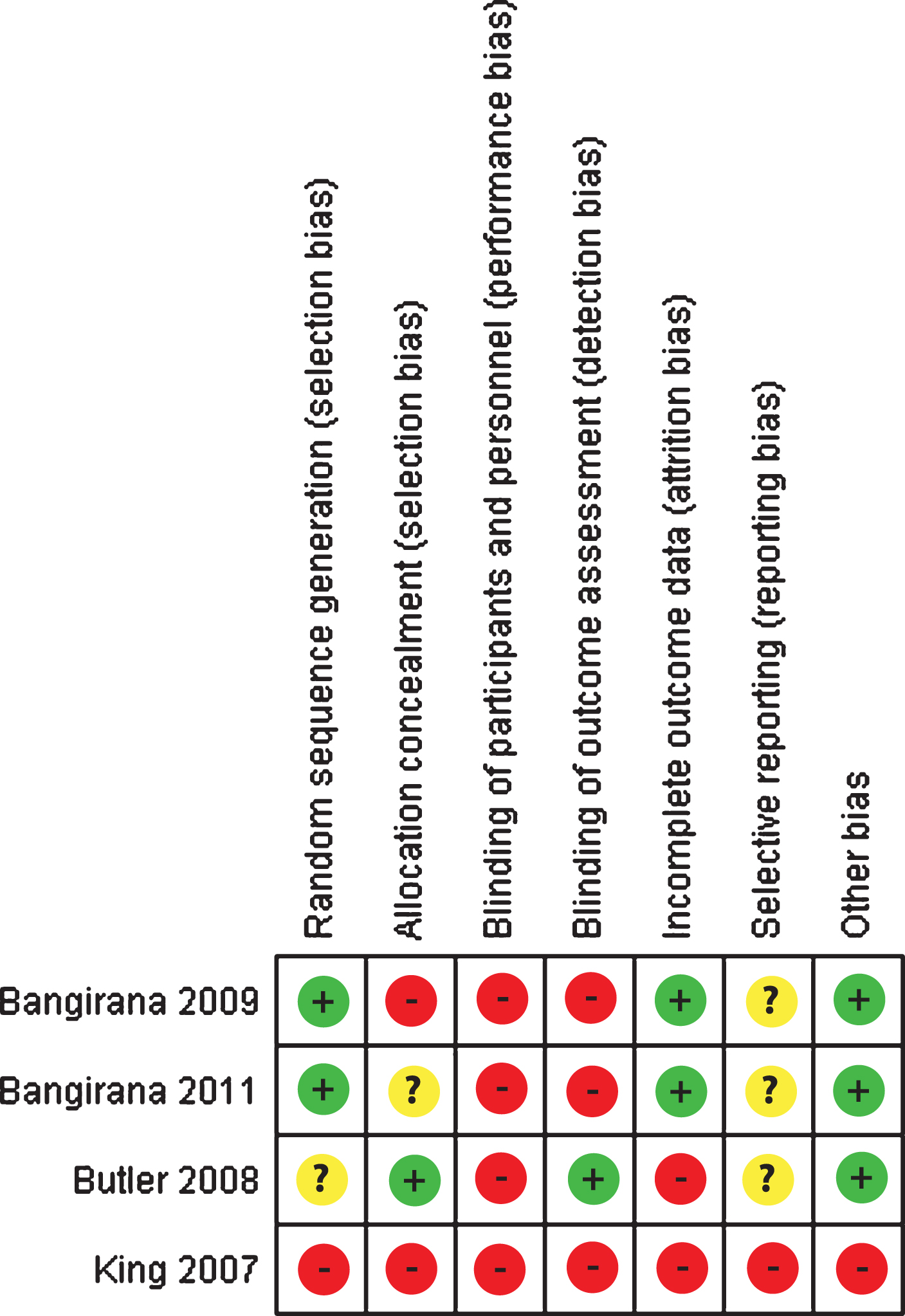
Risk of bias was independently assessed by two authors who judged the included studies on issues such as allocation concealment, blinding of participants and personnel, incomplete outcome data and selective reporting. The RCT risk of bias assessment tool included in Chapter 8 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins, Altman, & Sterne, 2011) was used for this purpose. Each area of bias was judged as ‘high risk’, ‘low risk’ or ‘unclear risk’. See Fig. 2 for risk of bias summary.
Fig.2
Risk of bias summary table.
2.7Data analysis
Data were entered into Review Manager 5.3 for the purposes of conducting meta-analysis. Where data were not reported in full, the lead author of the study was contacted and asked to supply additional detail. One author provided additional data on internalising, externalising behavior and on a measure of attention. Requests for additional data in regards to memory outcomes were unsuccessful. All included studies reported continuous data, therefore, we calculated the standardised mean difference (SMD), for outcomes measured on different scales, with 95% confidence intervals (CI). For outcomes measured on the same scale we used the mean difference (MD) with 95% CI. A random effects model was applied in both instances. Statistical heterogeneity between studies was assessed through visual inspection of forest plots and use of the I2 statistic. Where it was not possible to conduct meta-analysis on all outcomes, results were presented narratively.
3Results
3.1Description of included studies
Four trials (n = 296 participants) were identified which met the inclusion criteria (see Table 1). All of the included studies were randomised controlled trials with the unit of randomisation being the individual child/adolescent. Two trials (Bangirana et al., 2009, 2011) utilised an intervention consisting of computerised cognitive rehabilitation training compared to a no treatment control condition. One trial (Butler et al., 2008) used a cognitive remediation program compared to a wait list control. The remaining trial (King, White, McKinstry, Noetzel, & DeBaun, 2007) employed general academic tutoring for both the intervention and control conditions. The intervention group then received additional memory rehabilitation.
Table 1
Summary of included study characteristics
| Intervention | Sample characteristics: | Outcome measures: | Main findings: | Recommendations: | |
| Bangirana et al. (2009) | Captain’s Log computer software – Exercises were selected from modules relating to Attention skills, Conceptual/Memory skills, Visual Motor Skills and Logic Skills. Two sessions once a week for eight weeks, in the clinic, home or school settings. | 65 participants with ABI following severe malaria. Intervention mean age = 9.7 years, control mean age = 10.1 years. Intervention n = 32, control n = 33 | Primary: CogMed Maze tasks - Groton Maze Chasing Task and Groton Maze Learning Task. Secondary: Child Behavior Checklist. | Children in the intervention condition showed statistically significant improvements in visuomotor processing speed, working memory, learning and internalising problems. | Need to establish the long-term benefit of computerised cognitive rehabilitation in children with cerebral malaria and to provide interventions for children below the age of five years. |
| Bangirana et al. (2011) | Captain’s Log computer software – Exercises were selected from modules relating to Attention, Memory, Visuomotor skills and Reasoning. Two sessions once a week for eight weeks. | 61 participants with ABI following severe malaria. 5–12 years of age. Intervention n = 28, control n = 33. | Primary: Test of Variables of Attention. Secondary: Kaufman Assessment Battery for Children second edition; Child Behavior Checklist; Wide Range Achievement Test-third edition; Middle Childhood Home Observations for the Measurement of the Environment. | Children in the intervention condition showed statistically significant improvements, compared to those in the control condition, on a measure of learning. Children in the control condition made statistically significant improvements on a measure of working memory. | Need to establish whether improvements in cognition in children with severe malaria, following computerised cognitive rehabilitation, are sustained over time. |
| Butler et al. (2008) | Cognitive Remediation Program (CRP) – consisting of three components; (1) hierarchically graded massed practice, (2) strategy acquisition, and (3) cognitive-behavioral interventions. Twenty two-hour weekly sessions over 4–5 months. | 161 survivors of childhood malignancy that involved CNS disease and/or treatment to the CNS. 6–17 years of age. Intervention age 10.8 years, Control age 11.1 years. 108 participants in intervention group. | Primary: Academic achievement = Wide Range Achievement Test-Third Edition; Calculation and Applied Problems; Reading Comprehension; Arithmetic (WISC–III). Brief focused attention = Digit Span; Sentence Memory; Stories (Children’s Memory Scale); Rey Auditory Verbal Learning Test (Trial 1). Working Memory = Digits Backward; Stroop Color–Word Test (Trial 3); Trail Making Test B; Brief Test of Attention. | ||
| Memory Recall = Stories (Delayed Recall); Rey–Osterrieth Complex Figure Test (Delayed Recall); RAVLT (Delayed Recall of Trial). Vigilance = Continuous Performance Test. Secondary: Learning/Learning Strategies = Strategies Assessment Measure. Parent/Teacher Ratings of Attention = Conners’ Parent Rating Scale: Long Version–Revised; Conners’ Teacher Rating Scale: Long Version—Revised. Self-esteem = Culture-Free Self-Esteem Inventory, Second Edition | A statistically significant improvement was shown on tests of academic achievement for the intervention but not the control group. No statistically significant differences were found for measures of attention, working memory, memory recall or vigilance. Statistically significant differences were shown on tests of learning, parent but not teaching ratings of attention with no significant differences on self-esteem. | A holistic approach to rehabilitation is essential. Involvement of caregivers who emphasise skills taught during the CRP may improve outcomes over time. Need for a multidimensional, reliable measure of working memory. | |||
| King et al. (2007) | General academic tutoring, memory rehabilitation training and task preparation strategies. Year one = 1 hour per week, Year two = 2 hours per week. | 9 participants with sickle cell disease and stroke. 8–13 years of age. 5 intervention (3 males), 4 control (1 male). | Memory as measured by a subtest the of Children’s Memory Scale. Wechsler Abbreviated Scale of Intelligence, California Verbal Learning Test–Children’s Version, Digit Span, Wechsler Individual Achievement Tests–Second Edition | Children in the intervention condition made statistically significant improvements, compared to children in the control condition, on tests of verbal learning, memory (digit span backwards but not forwards) and academic achievement (reading but not spelling or mathematics). | None provided |
3.2Sample size
The number of participants randomised to the control and intervention conditions ranged from 9 (King et al., 2007) to 161 (Butler et al., 2008). Bangirana et al. (2011) was alone in conducting and reporting on a sample size calculation (30 participants per group), which was met for the control (n = 33), but not the intervention condition (n = 28). Butler et al. (2008) made reference to using power analysis but failed to report their target sample size. Bangirana et al. (2009) and King et al. (2007) did not perform a sample size calculation prior to recruitment.
3.3Participants and setting
The included studies analysed data from 296 children and adolescents. One of the trials (Bangirana et al., 2009) stated that the intervention was delivered in a clinic, while a second trial (King et al., 2007) was conducted at school. No other trials provided information in regards to setting. Three of the trials recruited from healthcare sites. Bangirana et al. (2009) recruited from a single hospital site in Uganda, while Bangirana et al. (2011) recruited from four hospitals in the same region. Bulter et al. (2008) recruited from healthcare sites in Oregon, Pennsylvania, Tennessee, Texas, California, New York and Ohio in the USA. No recruitment site was described by King et al. (2007). All of the included participants were between 5 and 17 years old.
3.4Excluded studies
Two papers were excluded following full review. The first assessed the implementation of memory training by teachers in a school setting (Holmes & Gathercole, 2014) and was excluded because participants did not possess acquired brain injury. The second explored educational attainment in children and adolescents with traumatic brain injury following an online problem-solving intervention (Arnett et al., 2013). This study was excluded as it was a secondary data analysis which sought to examine the predictive nature of a measure of executive functioning on educational outcomes.
3.5Risk of bias in included studies
Risk of bias was assessed for the four included trials using the domain-based risk of bias tool of the Cochrane Collaboration (Higgins et al., 2011) and is summarised in Fig. 2.
3.6Allocation
Bangirana et al. (2011) employed a table of random numbers for the purposes of allocation, while Bangirana et al. (2009) used random number generation to allocate participants to the intervention or control arms of their trials. King et al. (2007) failed to report how they randomly allocated participants. Butler et al. (2008) employed the services of a data manager to randomly allocate but did not describe the procedures used. We therefore deemed selection bias to be low for Bangirana et al. (2009) and Bangirana et al. (2011), unclear for Butler et al. (2008) and high for King et al. (2007).
3.7Blinding
None of the included studies were able to blind participants from group allocation. However, Butler et al. (2008) did take steps to conceal allocation from the assessors. Performance bias was therefore judged as high for all studies with only Butler et al. (2008) deemed as possessing low detection bias.
3.8Incomplete outcome data
Bangirana et al. (2011) (n = 61 participants) report no drop outs from their study. This study was therefore judged as having low attrition bias. Bangirana et al. (2009) (n = 65 participants) state that 3 children dropped out of the intervention due to a fuel crisis which meant that travel to the assessment centre was difficult. One child died before completing follow-up assessment in the control arm of the trial. The overall attrition rate was 6% and therefore attrition bias was deemed as low. Butler et al. (2008) (n = 163 participants) reports that 9 children refused to complete post-test assessment (no explanation is given), 6 were unable to be contacted and the reason for 3 further incompleters was unknown. One child was deemed ineligible following randomisation and one refused follow-up assessment (no explanation is provided) for the control arm. The overall attrition rate was 19% and therefore attrition bias was deemed as high. King et al. (2007) (n = 11 participants) reported that one child dropped out of the intervention arm of the trial in the first year due to frustration with the reading programme and a lack of parental support. Data are provided on 9 children (attrition rate of 18%) who completed the trial with no explanation given as to why a second child dropped out of the control arm of the trial. This study was therefore judged as having high attrition bias.
3.9Selective reporting
Registered protocols for King et al. (2007), Bangirana et al. (2009) and Butler et al. (2008) could not be found. Bangirana et al. (2009) and Butler et al. (2008) were therefore judged as possessing an unclear risk of reporting bias. A trial protocol was found for Bangirana et al. (2011), however, no explanation is provided for why the data from 5 participants is excluded from analysis of the attention outcome. This trial was deemed as having an unclear risk of reporting bias. King et al. (2007) failed to present the results of inferential statistics for the outcome of memory as measured by the Children’s Memory Scale and omitted a study flowchart as recommended by CONSORT (Moher et al., 2012). This study was therefore judged as having high reporting bias.
3.10Other bias
One study (King et al., 2007) was assessed as having a high risk of bias in relation to the choice of statistics used to test the difference between the intervention and control groups. This study used the repeated measures analysis of variance to assess differences between 4 children in the control condition and 5 children in the intervention condition.
3.11Meta-analysis of academic achievement (primary outcome)
All four included studies (n = 296) reported on the primary outcome of academic achievement. The corresponding author of the King et al. (2007) trial did not provide mean and standard deviation data on request and thus were not included in this meta-analysis. The three studies which reported on this outcome (n = 287) used measures relating to learning (Bangirana et al., 2009, 2011) and arithmetic (Butler et al., 2008). Following meta-analysis the three included studies showed no effect (p = 0.06) of the interventions on academic achievement. The combined SMD for this outcome was 1.31 (95% CI – 0.06 to 2.68) showing an improvement for the intervention group. Heterogeneity was high (I2 = 96%, Tau2 = 1.39) and was statistically significant (p < 0.001) (see Fig. 3). The SMD of 1.31 would be considered as a small effect size. These results suggest that there is no evidence for an effect of the interventions in improving the academic achievement of children and adolescents with ABI.
Fig.3
Forest plot of academic achievement (primary outcome).

3.12Meta-analysis of externalising behavior (secondary outcome)
Two studies (n = 126) examining the same intervention (Captain’s Log computer software) reported on externalising behavior and were included in meta-analysis (Bangirana et al., 2009, 2011). There was a statistically significant effect (p = 0.0005) which favoured the control group over the intervention group. The combined MD for externalising behavior was 1.18 (95% CI 0.52 to 1.85) showing an improvement in externalising behavior for the control group. Heterogeneity was non-existent (I2 = 0%, Tau2 = 0) and non-significant (p = 0.37) (see Fig. 4). The MD of 1.18 would be considered a small effect size. These results suggest that there is no evidence for an effect of improving the externalising behavior of children with ABI following use of Captain’s Log computer software.
Fig.4
Forest plot of externalising behavior (secondary outcome).

3.13Meta-analysis of internalising behavior/emotion (secondary outcome)
Two studies (n = 126) provided data on internalising behavior as measured by the Child Behavior Checklist (Bangirana et al., 2009, 2011). There was no statistically significant effect (p = 0.23) of the interventions on internalising behavior. However, the MD showed a decrease (–1.57, 95% CI –4.14 to 1.00) in internalising behavior which favoured the intervention condition. There was no heterogeneity (I2 = 0%, Tau2 = 0) which was also non-significant (p = 0.63) (see Fig. 5). The MD of 1.57 would be considered as a small effect size. These results indicate that the use of Captain’s Log computer software did not improve the internalising behavior of children with ABI.
Fig.5
Forest plot of internalising behavior/emotion (secondary outcome).

3.14Meta-analysis of attention (secondary outcome)
Bulter et al. (2008) and Bangirana et al. (2011) (n = 217) assessed the outcome of attention using different types of measurement tools. Butler et al. (2008) employed the Brief Test of Attention (Schretlen, 1997) while Bangirana et al. (2011) used the Test of Variables of Attention (Dupuy, & Greenberg, 2005). There was no statistically significant effect (p = 0.58) of the interventions on attention. The SMD showed an increase (0.11, 95% CI –0.28 to 0.50) in attention which favoured the intervention condition. Heterogeneity was moderate (I2 = 40%, Tau2 = 0.03) and non-significant (p = 0.20) (see Fig. 6). The SMD of 0.11 would be considered as a small effect size. These findings suggest that the interventions were not successful in improving attention in children with ABI.
Fig.6
Forest plot of attention (secondary outcome).

4Discussion
Meta-analysis suggests that the educational interventions reported here are not effective in improving academic performance for children and adolescents with ABI. These findings are based on three of the four studies included in the meta-analysis. Two of these studies (n = 126) (Bangirana et al., 2009, 2011) investigated use of a computerised cognitive rehabilitation training package (i.e. Captain’s Log software) on learning, whilst the third (n = 161) (Butler et al., 2008) made use of a Cognitive Remediation Program (CRP) based on an assessment of performance on composite scales relating to reading, arithmetic and spelling. Two studies (Bangirana et al., 2009, 2011) from the same team of researchers in Uganda, assessed children aged between 5 to 12 years of age, whilst the third (Butler et al., 2008) contained a mix of children and adolescents (6 to 17 years) from the USA.
Two studies (n = 126) (Bangirana et al., 2009, 2011) assessed alterations in internalising and externalising behaviors for children with ABI following intervention with Captain’s Log software. Meta-analyses of these data suggest no statistically significant effect of the intervention on either internalising or externalising behaviors. Participants in the control condition showed reduced externalising behaviors when compared to the experimental group. Children in the experimental condition showed improvements in internalising behaviors following the intervention, however, these were non-significant.
Two studies (n = 217) (Bangirana et al., 2011; Butler et al., 2008) included a measure of attention in their assessment of the impact of Captain’s Log software and a CRP. Meta-analysis of this data showed a slight improvement (0.11) in attention following intervention which was not statistically significant.
Three of the four included studies (Bangirana et al., 2009, 2011; King et al., 2007) contained relatively small numbers of participants (9 to 65). As such the findings from these studies must be treated with caution. The largest study (Butler et al., 2008) employed a multi-centre approach, including seven states, to achieve a sample of 161 survivors of childhood malignancy or disease of the central nervous system.
4.1Limitations of this review
Although we made every effort to minimise bias in the selection of studies, it is still possible that we may have omitted some relevant manuscripts in this review. Our focus on the highest level of available evidence for effectiveness of interventions resulted in identification of only four RCTs. Lastly, due to resource limitations it was only possible to include studies published in the English language.
4.2Implications for practice and research
The results from this meta-analysis suggest that there is no evidence for the use of the two educational interventions included here to bring about improvements in academic attainment for children and adolescents with ABI. The tested interventions, Captain’s Log cognitive training software (Bangirana et al., 2009) and the CRP (Butler et al., 2008) both consist of computer-based cognitive training aimed at improving academic achievement and cognitive functioning. Although computer-delivered cognitive training has been shown to result in improved cognitive performance (Linden et al., 2016), this meta-analysis suggests that there are no significant benefits of such training on academic performance.
There was no evidence that the interventions included in this review resulted in improved academic attainment in children with ABI. The importance of fostering academic success for children with ABI on return to school cannot be underestimated if they are to achieve their full potential. As students struggle in the school setting, they progressively disengage from school, which amplifies their academic underachievement (Henry, Knight, & Thornberry, 2012). School disengagement is directly linked to school dropout, which leads to decreased earnings (Rouse, 2005), poor health outcomes (Muennig, 2005), dependence on public assistance (Waldfogel, Garfinkel, & Kelly, 2005), and a significant increase in the likelihood of being incarcerated (Moretti, 2005). The three studies included in meta-analysis were conducted in Uganda and the USA meaning that many countries have yet to trial such interventions. Clearly further work is necessary to develop effective interventions in other regions, however, given the importance of supporting children in their transition back to school on future outcomes, every effort should be made to achieve this.
Recommendations by the International Paediatric Brain Injury Society suggest that children with ABI should be given appropriate educational accommodations which meet their changing needs as their brains continue to develop and grow (McKinlay et al., 2016). As such, a successful educational intervention must adapt to the changing needs of the child whilst also taking into consideration the training deficit which is often present among school teachers (Linden, Braiden, & Miller, 2013). Interventions should focus on functional skills and be responsive to the need for context sensitivity (Ylvisaker et al., 2005).
4.3Future directions
The research included in this review included interventions for children with ABI to improve cognition, behavior and learning. However, a singular focus on the child as the point of intervention fails to acknowledge the multi-faceted nature of interventions intended to improve academic outcomes. The context in which we seek to intervene must be fully understood and taken into consideration. Educational policy, teacher understanding, training and school-based resources represent some of the factors which can impact on the development and delivery of educational programs (Dettmer et al., 2013). To be successfully implemented over the long-term interventions must work within the school environment in order to be fully integrated into the educational curriculum (Ylvisaker et al., 2001, 2005).
The variety in methods of measurement employed in the included studies suggests that no current gold standard exists to measure academic attainment in children with ABI. Future work should seek to provide consensus on those measures which provide the highest levels of validity and reliability to enable future comparison.
Only two countries, Uganda and the USA, have made efforts to develop interventions to work with children with ABI to improve educational outcomes. There is a clear need for other countries to develop evidence-based interventions which work within their available resources and cultural contexts. Efforts should be made to seek collaborative opportunities to standardize these approaches to reduce time to development, overcome common barriers to implementation and reduce costs.
5Conclusions
The small number of included studies indicates that there is a lack of available, rigorously tested interventions which seek to improve academic attainment for children following brain injury. Collectively these studies did not significantly improve academic attainment which indicates that greater efforts are needed to produce effective interventions. These interventions were also shown to be ineffective for rehabilitating the wider spectrum of ABI deficits (i.e. cognition, behavior or emotion) suggesting that such complex difficulties may require specialised approaches. Given the relationship between academic performance and transition to employment and adulthood, there is a critical need for further research in this area.
Conflict of interest
The authors report no conflicts of interest.
Funding
This project was completed with funding from the National Institute on Disability and Rehabilitation Research, grant #H133G140059.
References
1 | Achenbach T. , & Rescorla L. ((2000) ). Manual for the ASEBA preschool forms and profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, and Families. |
2 | Anderson V. , Brown S. , Newitt H. , & Hoile H. ((2009) ). Educational, vocational, psychosocial, and quality-of-life outcomes for adult survivors of childhood traumatic brain injury. Journal of Head Trauma Rehabilitation, 24: (5), 303–312. |
3 | Anderson V. , Brown S. , Newitt H. , & Hoile H. ((2011) ). Long-term outcome from childhood traumatic brain injury: Intellectual ability, personality, and quality of life. Neuropsychology, 25: (2), 176–184. http://doi.org/10.1037/a0021217 |
4 | Anderson V. , Catroppa C. , Morse S. , Haritou F. , & Rosenfeld J. ((2005) ). Attentional and processing skills following traumatic brain injury in early childhood. Brain Injury: [BI], 19: (9), 699–710. http://doi.org/10.1080/02699050400025281 |
5 | Andersson K. , Bellon M. , Walker R. , Andersson K. , Bellon M. , & Walker R. ((2016) ). Parents’ experiences of their child’s return to school following acquired brain injury (ABI): A systematic review of qualitative studies. Brain Injury, 9052: . http://doi.org/10.3109/02699052.2016.1146963 |
6 | Arnett A. B. , Peterson R. L. , Kirkwood M. W. , Taylor H. G. , Stancin T. , Brown T. M. , & Wade S. L. ((2013) ). Behavioral and cognitive predictors of educational outcomes in pediatric traumatic brain injury. Journal of the International Neuropsychological Society: JINS, 19: , 881–889. http://doi.org/S1355617713000635 [pii]10.1017/S1355617713000635 [doi]; 10.1017/S1355617713000635 [doi] |
7 | Bangirana P. , Allebeck P. , Boivin M. J. , John C. C. , Page C. , Ehnvall A. , & Musisi S. ((2011) ). Cognition, behavior and academic skills after cognitive rehabilitation in Ugandan children surviving severe malaria: A randomised trial. BMC Neurology, 11: (1), 96. http://doi.org/10.1186/1471-2377-11-96 |
8 | Bangirana P. , Giordani B. , John C. C. , Page C. , Opoka R. O. , & Boivin M. J. ((2009) ). Immediate neuropsychological and behavioral benefits of computerized cognitive rehabilitation in Ugandan pediatric cerebral malaria survivors. Journal of Developmental and Behoral Pediatrics, 30: (4), 310–318. http://doi.org/10.1097/DBP.0b013e3181b0f01b.Immediate. |
9 | Butler R. W. , Copeland D. R. , Fairclough D. L. , Mulhern R. K. , Katz E. R. , Kazak A. E. , & Sahler O. J. ((2008) ). A multicenter, randomized clinical trial of a cognitive remediation program for childhood survivors of a pediatric malignancy. Journal of Consulting and Clinical Psychology, 76: , Retrieved from http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles//CN-00640184/frame.html |
10 | Delis D. C. , Kramer J. H. , Kaplan E. , & Ober B. A. ((1994) ). California Verbal Learning Test–Children’s Version manual. San Antonio, TX: Psychological Corp. |
11 | Dettmer J. , Ettel D. , Glang A. , & McAvoy K. ((2013) ). Building statewide infrastructure for effective educational services for students with TBI: Promising practices and recommendations. The Journal of Head Trauma Rehabilitation, 29: (3), 224–232. http://doi.org/10.1097/HTR.0b013e3182a1cd68 |
12 | Dupuy T. R. , & Greenberg L. M. ((2005) ). The T.O.V.A Manual for IBM Personal Computer or IBM Compatible Minneapolis, MN: Universal Attention Disorders. |
13 | Eisenberg N. , Fabes R. A. , Murphy B. , Maszk P. , Smith M. , Karbon M. , & Richard A. ((2016) ). The role of emotionality and regulation in children âTM s social functioning: A longitudinal study. Child Development, 66: (5), 1360–1384. |
14 | Ettel D. , Todis B. , & Davies S. C. ((2016) ). Traumatic brain injury: Persistent misconceptions and knowledge gaps among educators. Exceptionality Education International, 26: (1), 1–18. |
15 | Gioia G. , Isquith P. K. , Guy S. C. , & Kenworthy L. ((2000) ). BRIEF: Behavior Rating Inventory of Executive Function. Lutz, FL: Psychological Assessment Resources. |
16 | Glang A. , Ettel D. , Todis B. , Gordon W. A. , Oswald J. M. , Vaughn S. L. , & Brown M. ((2015) ). Services and supports for students with traumatic brain injury: Survey of state educational agencies. Exceptionality, 23: (4), 211–224. http://doi.org/http://dx.doi.org/10.1080/09362835.2014.986612 |
17 | Glang A. , Ylvisaker M. , Stein M. , & Ehlhardt L. ((2008) ). Validated instructional practices: Application to students with traumatic brain injury. Journal of Head, 23: (4), 243–251. |
18 | Goodman R. ((1997) ). The Strengths and Difficulties Questionnaire: A research note. Journal of Child Psychology and Psychiatry, 38: (5), 581–586. |
19 | Halstead M. E. , McAvoy K. , Devore C. D. , Carl R. , Lee M. , & Logan K. ((2013) ). Returning to learning following a concussion. Pediatrics, 132: (5), 948–957. http://doi.org/10.1542/peds.2013-2867 |
20 | Hartman L. , Duncanson M. , & Farahat S. L. S. ((2015) ). Clinician and educator experiences of facilitating students’ transition back to school following acquired brain injury: A qualitative systematic review. Brain Injury, 29: (12), 1387–1399. http://doi.org/10.3109/02699052.2015.1071431 |
21 | Hawley C. A. , Ward A. B. , Magnay A. R. , & Mychalkiw W. ((2004) ). Return to school after brain injury. Archives of Disease in Childhood, 89: (2), 136–142. http://doi.org/10.1136/adc.2002.025577 |
22 | Henry K. L. , Knight K. E. , & Thornberry T. P. ((2012) ). School disengagement as a predictor of dropout, delinquency, and problem substance use during adolescence and early adulthood. Journal of Youth and Adolescence, 41: , 156–166. http://doi.org/10.1007/s10964-011-9665-3 |
23 | Higgins J. P. T. , Altman D. G. , Sterne J. A. C. Chapter: Assessing risk of bias in included studies, In: Higgins J.T. Green S. (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. [updated March 2011]. The Cochrane Collaboration, (2011) . |
24 | Holmes J. , & Gathercole S. E. ((2014) ). Taking working memory training from the laboratory into schools. Educational Psychology, 34: (4), 440–450. http://doi.org/10.1080/01443410.2013.797338 |
25 | Kaplan E. , Fein D. , Kramer J. , Delis D. , & Morris R. ((2004) ). Wechsler Intelligence scale for children fourth edition - integrated. San Antonio, TX: Harcourt Assessment, Inc. |
26 | King A. A. , White D. A. , McKinstry R. C. , Noetzel M. , & DeBaun M. R. ((2007) ). A pilot randomized education rehabilitation trial is feasible in sickle cell and strokes. Neurology, 68: (23), 2008–2011. http://doi.org/10.1212/01.wnl.0000264421.24415.16 |
27 | Kurowski B. G. , Wade S. L. , Kirkwood M. W. , Brown T. M. , Stancin T. , & Taylor H. G. ((2013) ). Online problem-solving therapy for executive dysfunction after child traumatic brain injury. Pediatrics, 132: , e158–66. http://doi.org/http://dx.doi.org/10.1542/peds.2012-4040 |
28 | Limond J. , Dorris L. , & McMillan T. M. ((2009) ). Quality of life in children with acquired brain injury: Parent perspectives 1-5 years after injury. Brain Injury, 23: (7), 617–622. http://doi.org/10.1080/02699050902997870 |
29 | Linden M. , Braiden H. , & Miller S. ((2013) ). Educational professionals’ understanding of childhood traumatic brain injury. Retrieved from Brain Injury, 27: (1), 92–102. http://informahealthcare.com/doi/abs/10.3109/02699052.2012.722262 |
30 | Linden M. , Hawley C. , Blackwood B. , Evans J. , Anderson V. , & Rourke O. C. ((2016) ). Technological aids for the rehabilitation of memory and executive functioning in children and adolescents with acquired brain injury (Review). Cochrane Database of Systematic Reviews, (7). http://doi.org/10.1002/14651858.CD011020.pub2.www.cochranelibrary.com |
31 | McKinlay A. , Linden M. , DePompei R. , Aaro Jonsson C. , Anderson V. , Braga L. , Castelli E. , de Koning P. , Hawley C. A. , Hermans E. , Kristiansen I. , Madden A. , Rumney P. , Savage R. , & Wicks B. ((2016) ). Service provision for children and young people with acquired brain injury. Best practice recommendations: – international paediatric brain injury society (IPBIS). Brain Injury. |
32 | McKinlay A. , Dalrymple-Alford J. C. , Horwood L. J. , & Fergusson D. M. ((2002) ). Long term psychosocial outcomes after mild head injury in early childhood. Journal of Neurology, Neurosurgery, and Psychiatry, 73: (3), 281–288. Retrieved from http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1738032&tool=pmcentrez&rendertype=abstract |
33 | Muennig P. ((2005) ). Health returns to education interventions. Symposium on the social costs of inadequate education conducted at Teachers College; New York, NY. |
34 | Moher D. , Hopewell S. , Schulz K. F. , Montori V. , G??tzsche P. C. , Devereaux P. J. , & Altman D. G. ((2012) ). CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. International Journal of Surgery, 10: (1), 28–55. http://doi.org/10.1016/j.ijsu.2011.10.001 |
35 | Moretti E. ((2005) ). Does education reduce participation in criminal activities? Symposium on the social costs of inadequate education conducted at Teachers College; New York, NY. |
36 | Ransom D. M. , Vaughan C. G. , Pratson L. , Sady M. D. , McGill C. A. , & Gioia G. A. ((2015) ). Academic effects of concussion in children and adolescents. Pediatrics, 135: (6), 1043–1050. http://doi.org/10.1542/peds.2014-3434 |
37 | Rouse C. E. ((2005) ). The labor market consequences of an inadequate education. Symposium on the social costs of inadequate education conducted at Teachers College, New York, NY. |
38 | Schretlen D. ((1997) ). Brief Test of Attention. Odessa, FL: Psychological Assessment Resources. |
39 | Tonks J. , Slater A. , Frampton I. , Wall S. E. , Yates P. , & Williams W. H. ((2009) ). The development of emotion and empathy skills after childhood brain injury. Developmental Medicine and Child Neurology, 51: (1), 8–16. http://doi.org/10.1111/j.1469-8749.2008.03219.x |
40 | Waldfogel J. , Garfinkel I. , & Kelly B. ((2005) ). Public assistance programs: How much could be saved with improved education? Symposium on the social costs of inadequate education conducted at Teachers College; New York, NY. |
41 | Wilkinson G. S. ((1993) ). The Wide Range Achievement Test. Third. Wilmington, DE: Wide Range. |
42 | Wilson B. , Ivani-Chalian R. , & Aldrich F. ((1991) ). Rivermead Behoral Memory Test for Children (RBMT-C) Bury St Edmunds: Thames Valley Test Co. |
43 | Ylvisaker M. , Adelson D. , Braga L. W. , Burnett S. M. , Glang A. , Feeney T. , & Todis B. ((2005) ). Rehabilitation and Ongoing Support After Pediatric TBI Twenty Years of Progress. Journal of Head Trauma Rehabilitation, 20: (1), 95–109. http://doi.org/10.1097/00001199-200501000-00009 |
44 | Ylvisaker M. , Todis B. , Glang A. , Urbanczyk B. , Franklin C. , DePompei R. , & Tyler J. S. ((2001) ). Educating Students with TBI: Themes and Recommendations. Journal of Head Trauma Rehabilitation, 16: (1), 76–93. |


