The importance of work or productive activity in life care planning and case management
Abstract
INTRODUCTION: The importance of work or productive activity for the well-being, community integration, and quality of life of people living with disabilities is addressed, with implications for life care planning and case management.
BACKGROUND: The role of work or productive activity in our society, and consequences of deprivation if rehabilitation services do not address vocational effects of disabilities, is explored. A continuum of productivity options is introduced; types of vocational rehabilitation assessment processes and interventions are described.
PURPOSE: The role of vocational rehabilitation services in life care planning and case management is discussed, focusing on quality of life for people living with disabilities.
CONCLUSION: Rehabilitation and health care professionals should understand the importance of work or other productive activity, and support the development of appropriate plans to address those needs among people who have disabilities.
1Introduction
When people have significant disabilities, the interactions between those disabilities and the environments in which people live have profound implications for quality of life. Those environments extend far beyond the home, and into the community, the workplace, and the world at large. Sander, Clark, and Pappadis (2010) identified three main areas that define community integration of people with disabilities: 1) employment or other productive activity, 2) independent living, and 3) social activity (p. 121). Araten-Bergman and Stein (2014) identified employment as important for “realizing the human rights of individuals with disabilities” (p. 381).
2Life care planning for people living with disability
Life care planning is a systematic process of identifying and quantifying an individual’s multidimensional disability-related needs (Deutsch & Reid, 2003). One of those dimensions of disability-related needs is the effect on work and other productive activities. The life care planning process involves gathering information and evaluating the disability-related needs of an individual in order to project what that person will need into the future to minimize complications and maximize quality of life. It results in a life care plan document, a “roadmap” of options for the individual living with disability and her or his family to use to make informed decisions about those options (Reid, 2011).
3Role of work in our society
Work, and earning the means to take care of one’s own needs and that of one’s family, is highly valued in our society. For most people, work or other productive activity is part of our identities, and gives meaning to our lives. Those who lose that part of their identity often wish to return to it. For example, Farrell (2014) described the growing practice of “unretirement” among retired individuals who choose to return to the workforce, explaining that work has emotional and psychological rewards that have “taken deep roots in our culture” (p. 23). Farrell explained how the value of work is far greater than just the income that can be derived from that work, stating that “The factory, the office, the cubicle, the retail store, and other workplaces are communities with colleagues, cubicle mates, union brothers and sisters, and fellow employees” (p. 15).
Farrell (2014) also described the reciprocally beneficial relationship between work and health, summarizing recent research results with the simple statement, “having a job itself is a force for staying healthy” (p. 43). The effects of unemployment, including not only reduced income but also reduced social interactions and sense of self-worth, could have a negative effect not just on quality of life, but also on life expectancy for people with disabilities. Robinson (2014) and Ditchman et al. (2014) summarized many studies addressing the positive effect of work on physical and mental well-being. Krause (2002) identified important variables that impact life expectancy, including income, access to health care, and psychosocial adaptation; these factors are associated with consequences of unemployment. According to Leahy et al. (2014), “Without a doubt, lack of employment opportunities excludes people with disabilities from full community inclusion and participation, stalls upward mobility, greatly affects their health-related quality of life, and subjective well-being” (p. 148).
4Effects of brain injury on work and productive activity
Traumatic brain injury often results in “distinctive patterns of cognitive, behavioural and physical impairment which impact significantly on independent living skills and participation in work or study” (Ponsford, 2013, p. 803). According to Kolakowsky-Hayner and Kreutzer (2001), return to work after brain injury “has been limited to as little as one-third of the brain injured population, as many as ten years post injury” (p. 41). When Deutsch, Kendall, Daninhirsch, Crimino-Ferguson, and McCollum (2006) followed up with people who had life care plans developed because of brain injury, they expanded their definition of vocational outcomes to include return to work, supported employment, or return to school or training with the anticipation of returning to work; in their sample, about half of the group had positive vocational outcomes. Whether the focus is on paid employment, education with a goal of employment, or some other form of productive activity, Katz, Zazler, and Zafonte (2013) clarified that “Return to some sort of productive activity is an essential part of societal reintegration and life satisfaction after brain injury” (p. 7).
5Continuum of productivity options
There are many varied productivity options for people who have disabilities. At one end of the continuum could be meaningful day activities, designed to get people out of the house and interacting with others, building “social capital” (Condeluci & Fromnech, 2014; Condeluci, Ledbetter, Ortman, Fromknecht, & DeVries, 2008). At the other extreme is competitive employment without any supports. In between are options such as the clubhouse model, sheltered work, customized employment, supported employment, and the identification of natural workplace supports.
The clubhouse model was originally designed for people living with mental illness, but was expanded by Jacobs and DeMello (1996) to work with people who had brain injuries. Jacobs (1997) explained how clubhouses are operated by and for their members. The focus is on each individual’s abilities, not on disabilities. Each member establishes his or her own goals, and is encouraged by staff members to break those goals down into smaller steps that can be accomplished relatively quickly. Members share tasks necessary to run the clubhouse, and provide both social support and accountability to each other. West, Targett, Crockatt, and Wehman (2013) provided an update about contemporary use of this model.
Sheltered work is an option designed to provide employment for people with disabilities in a segregated workshop setting, designed specifically to provide an employment opportunity for them. Sometimessheltered work is considered to be a transitional training step before integrated employment; other times it is considered a long-term continuing employment option. There has been significant debate over time about the efficacy and appropriateness of sheltered work, compared with the supported employment model. An example of a study finding negative effects for sheltered work as a precursor to integrated (supported) employment was published by Nazarov, Golden, and von Schrader (2012).
Customized employment (Citron, et al., 2008; Gower, Rudstam, & Young, 2014; Wehman, Targett, & West, 2014) involves carving out or creating specific jobs within an existing employment setting. For example, suppose an employment specialist approaches a restaurant and interviews people to see what kinds of tasks they would rather not have to do. That specialist finds out that the wait staff members dislike having to wrap silverware to prepare it for placing on tables. To them, it is a boring job that usually has to be done just when they have the least time available to do it (when there is a rush of diners). The specialist then creates a job focused primarily on wrapping silverware for the entire restaurant, and trains an individual with significant intellectual disabilities to perform the job well, with pride, in that restaurant.
Supported employment is a broader term, which encompasses not just customized employment but a broad range of options for empowering people with disabilities to be employed in “real work for real pay” (Wehman, Inge, Revell, & Brooke, 2007). In part as a response to funding limitations in many vocational rehabilitation service delivery systems, a growing emphasis in supported employment is the identification or development of “natural supports” in the workplace (West, Kregel, Hernandez, & Hock, 1997). This approach involves identifying coworkers or other supports already existing in the workplace that can help to empower people with significant disabilities to function well in the workplace without the need for ongoing job coaches or other external assistance.
When workplaces are designed with universal accessibility in mind, many people with disabilities qualify for and are successful in competitive employment without any assistance. The range of services and supports needed to facilitate successful employment or involvement in other meaningful, productive activities varies widely from person to person.
Independent of the continuum of productivity options is the degree to which an individual is paid for his or her productivity. Although “real work for real pay” is possible for many more people with disabilities than most members of the public realize, volunteer work can also be meaningful for those who wish to pursue it. Another dimension that is independent of the continuum of productivity options is the extent to which supports are transitional versus ongoing. An individual with a significant intellectual disability might only need transitional supports to succeed in a customized employment situation (such as wrapping silverware), while a professional accountant who is deaf might need interpreter services or computer-assisted real-time captioning (CART) services for staff meetings throughout her or his career.
6Vocational rehabilitation interventions
Vocational rehabilitation interventions, designed to address vocational barriers experienced by people who have disabilities, can use any of the models along the continuum of productivity options. Chan et al. (1997) described vocational rehabilitation as “a dynamic process consisting of a series of actions and activities that follow a logical, sequential progression of services related to the total needs of a person with a disability” (p. 312) and clarified that the process usually ends with successful placement of the individual in employment. Ditchman et al. (2014) noted strong empirical support for the efficacy of vocational rehabilitation interventions, including counseling, skills training, job placement, and supported employment.
The importance of career counseling interventions, and the centrality of work for individuals with disabilities, was described by Strauser (2014). He explained that the benefits of career counseling include increasing “power, social connection, and self-determination” and are not limited to “the traditional dichotomous outcomes of employed versus unemployed” (p. 8). Career counseling can be beneficial not only for people who are seeking work, but also for those interested in finding volunteer opportunities or other ways to include meaningful, productive activities in their lives. Whether with a goal of paid employment or a goal of other meaningful activity, career counseling can facilitate finding a match between the available opportunities and the needs and interests of the individual. This is important for job satisfaction; without such a match, “just any job” is not likely to meet the individual’s needs. Keeping in mind that lower job satisfaction is associated with decreased mental and physical health (Fritzsche, Dhanani, & Spencer, 2014), this is highly relevant to life care planning and case management with people who have disabilities.
Job development and placement services can help people with disabilities find a “match” between job opportunities and their own abilities and needs. Gower et al. (2014) summarized factors that facilitate successful job placement, with a focus on understanding the needs of employers as well as the needs and assets of people with disabilities. Bissonette (1994) focused on “the art of creating opportunity” (title page) in her classic book about job development.
A job coach (who may also be called a vocational rehabilitation specialist, employment specialist, etc.) can provide “an array of supports to assist a person with a significant disability with obtaining and maintaining competitive employment in the community” (Targett & Wehman, 2011, p. 135). Examples of such supports include on-the-job training, incorporating assistive technology, facilitating communication with coworkers, and designing compensatory memory strategies (Wehman, Targett, & Cifu, 2006). Typically, the involvement of a job coach is most intensive in the early stage, until the worker develops the competencies and strategies needed to be successful on the job; the job coach then fades out involvement in a follow-along phase.
Other interventions that may be needed to achieve the work or other productive activity goals of people with disabilities include educational support and training, as well as assistive technology and rehabilitation engineering services. Education and training could be focused on a specific employment goal, or on a hobby or other productive activity (such as woodworking or photography). Similarly, assistive technology and rehabilitation engineering services could be related directly to work or to other meaningful activities. For example, if a person who becomes blind wants to learn woodworking skills “without chopping off any hands,” both assistive technology and appropriate training would be important.
Supported employment services can incorporate job development and placement, job coaching, assistive technology, and other individualized services into one person-centered approach. Wehman et al. (2014) described a body of research supporting efficacy of the supported employment approach.
7Assessment processes
Strauser, Chan, Wang, Wu, and Rahimi (2014) and Chan et al. (1997) provided overviews of vocational evaluation in rehabilitation practice, including attention to levels of vocational assessment. The first level (Screening) “typically involves one or two interviews with the client and then 2 to 3 hours of testing” (Strauser et al., 2014, p. 185). The second level (Clinical Case Study) adds to the first level information “a detailed psychosocial and vocational history and synthesizing information from other professionals” and often “conducting a transferable skills analysis to address job placement and possible vocational training” (p. 185). The third level (Vocational Evaluation), is the most comprehensive and time consuming, and adds to the previous levels tasks which are specific to the evaluee and his or her situation, including the use of work samples, situational evaluations, on the job evaluations, observations in community settings, and job analyses.
8Role of vocational rehabilitation in life care planning and case management
Planning for appropriate work or other meaningful activity is an essential part of life care planning and case management with people who have significant disabilities. Studying the roles and functions of life care planners, Pomeranz, Yu, and Reid (2010) found that among the 21 themes emerging from the data collected, one was focused on vocational information. This study confirmed that one of the essential tasks of life care planners is to “Assess the need for short/long-term vocational/educational services” (p. 117).
If an individual providing life care planning or case management services doesn’t have expertise in vocational rehabilitation, s/he should be able to refer to and coordinate efforts with other professionals who do have that expertise. Berens and Weed (2010) and Neulicht and Berens (2011) provided overviews of the roles of vocational rehabilitation counselors and consultants for life care planning and case management.
Historically, some life care planners and case managers have not addressed vocational or meaningful activity issues in their work with people who have disabilities, sometimes stating that this is beyond their area of expertise. This tendency may have developed in part from misunderstanding the “optional” nature of including a vocational/educational plan within a life care plan document itself. Weed and Field (2001) mentioned that this page is “optional” in a life care plan, because “Other professionals may choose to complete a narrative and a specific rehabilitation plan that focuses on vocational issues which is located in a separate document” (pp. 176 -177). To be clear: addressing vocational or meaningful activity issues in life care planning and case management is not optional; it is an integral part of maximizing quality of life and minimizing complications for people living with disabilities. What is optional is whether costs of needed vocational rehabilitation services show up in the life care plan document or in a separate vocational analysis and rehabilitation plan.
Another problem that the authors of this article have noticed is that reports from some vocational experts do not address any vocational rehabilitation plan or mention of the need for involvement in any kind of productive activity that can significantly improve the quality of life for an evaluee living with disability. A vocational expert who simply comes to the conclusion that a person is “unemployable” and has a “total loss of earning capacity” without also addressing the need for some type of productive, meaningful activity is missing something important.
Regardless of which professional takes which role in planning with people who have disabilities to include work or other productive activity in their lives, attention to this important aspect of life is essential, and should not be ignored. As a “roadmap” of what to expect in the future and what options are available for a person living with disability to make informed choices about how to navigate that future, a life care plan should definitely address productiveactivity.
9Case example
Examples of vocational rehabilitation interventions have been described in this article. Perhaps less clear are examples of other productive activities. To illustrate, the following is an example from the clinical practice of one of the authors of thisarticle.
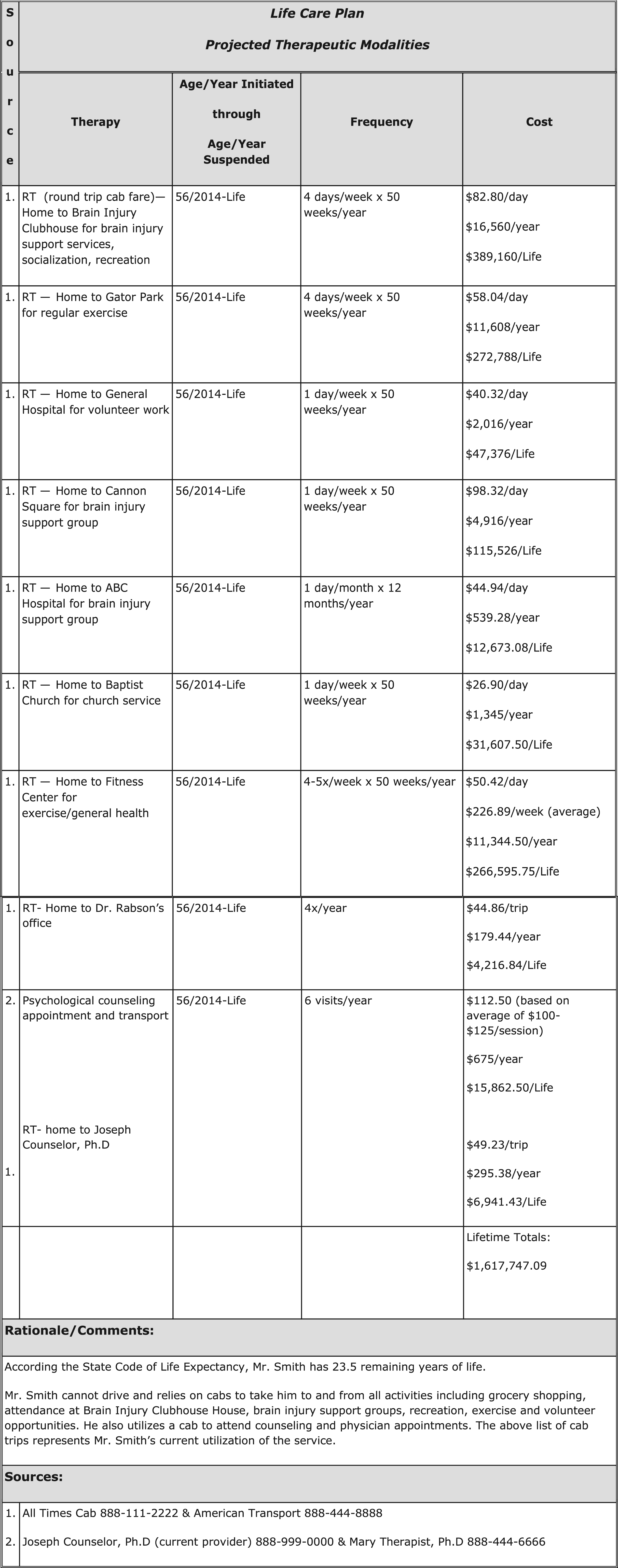
“Mr. Smith” is a 56 year-old male who sustained severe traumatic brain injury in 2004. Following many years of rehabilitation, he has been able to achieve a level of independence that includes living in his own home with family nearby to provide supervision and assistance as needed. He is unable to drive and relies on cab service or family for transportation to and from activities. He volunteers at a local hospital once a week. He also attends a brain injury clubhouse where he enjoys socialization with others and community outings. In order to maintain his general health and wellbeing, he exercises at a local gym. Transportation is also provided to allow him to receive ongoing supportive counseling and physician follow-upcare.
Figure #1 provides a (sanitized) page from Mr. Smith’s life care plan, illustrating some of the services provided and costs of providing those services to incorporate meaningful, productive activity into his life. Many life care planners would include in their life care plans transportation for items that are considered medically necessary (such as counseling and physician follow-up care), but might miss costs for important activities such as Mr. Smith’s volunteer work, participation in the brain injury clubhouse activities, and exercising at the local gym. Those activities support Mr. Smith’s community integration, and greatly enhance his quality of life.
10Conclusion
Attention to work or other productive activity for people with disabilities is essential, but at times missing from life care planning and case management practice. Rehabilitation and health care professionals should understand the importance of work or other productive activity, and support the development of appropriate plans to address those needs among people who have disabilities.
Conflict of interest
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
1 | Araten-Bergman T, Stein MA(2014) Employment, social capital and community participation among Israelis with disabilities. Work48: 38139010.3233/WOR-131779 |
2 | Berens DE, Weed RO(2010) The role of the vocational rehabilitation counselor in life care planningWeed RO, Berens DELife care planning and case management handbook3rd ed4162Boca RatonCRC Press |
3 | Bissonnette D(1994) Beyond traditional job development: The art of creating opportunityMilt Wright & AssociatesGranada Hills. CA |
4 | Chan F, Reid C, Kaskel L, Roldan G, Rahimi M, Mpofu E(1997) Vocational assessment and evaluation of people with disabilitiesPhysical Medicine and Rehabilitation Clinics of North America8: 2311325 |
5 | Citron T, Brooks-Lane N, Crandell D, Brady K, Cooper M, Revell G(2008) A revolution in the employment process of individuals with disabilities: Customized employment as a catalyst for system changeJournal of Vocational Rehabilitation28: 169179 |
6 | Condeluci A, Fromknecht J(2014) Social capital: The key to macro changeLash PublishingYoungsville, NC |
7 | Condeluci A, Ledbetter MG, Ortman D, Fromknecht J, DeFries M(2008) Social capital: A view from the fieldJournal of Vocational Rehabilitation29: 3133139 |
8 | Deutsch PM, Kendall SL, Daninhirsch C, Cimino-Ferguson S, McCollom P(2006) Vocational outcomes after brain injury in a patient population evaluated for Life Care Plan reliabilityNeuroRehabilitation21: 305314 |
9 | Deutsch P, Reid C(2003) Life care planning: A methodology for catastrophic disability analysisAnchor K, Schmerling J, Anchor JThe catastrophic injury handbook: Understanding vocational, economic, legal and clinical aspects of complex physical and mental trauma118131Kendall/HuntDubuque, IA |
10 | Ditchman N, Wu M, Chan F, Fitzgerald S, Lin C, Tu W(2014) Vocational rehabilitationStrauser DRCareer development, employment, and disability in rehabilitation343360SpringerNew York |
11 | Farrell C(2014) Unretirement: How Baby Boomers are changing the way we think about work, community, and the good lifeNew YorkBloomsbury Press |
12 | Fritzsche BA, Dhanani LY, Spencer JM(2014) Empowerment through employment: Job satisfaction theories and researchStrauser DRCareer development, employment,and disability in rehabilitation139159SpringerNew York |
13 | Gower WS, Rudstam H, Young J(2014) Elements of effective job placement: Environmental context, employer relationships,and understanding the job seekerStrauser DRCareer development, employment, and disability in rehabilitation297324SpringerNew York |
14 | Jacobs HE(1997) The Clubhouse: Addressingwork-related behavioral challenges through a supportive social communityJournal of Head Trauma Rehabilitation12: 51427 |
15 | Jacobs HE, DeMello C(1996) The Clubhouse model and employment following brain injuryJournal of Vocational Rehabilitation7: 169179 |
16 | Katz DI, Zazler ND, Zafonte RD(2013) Clinical continuum of care and natural historyZazler ND, Katz DI, Zafonte DBrain injury medicine: Principles and practice2nd ed212Demos, New York |
17 | Kolakowsky-Hayner SA, Kreutzer JS(2001) Return to work after brain injury:Aself- directed approachNeuroRehabilitation16: 4147 |
18 | Krauss JS(2002) Accuracy of life expectancy estimates in life care plans: Consideration of nonbiographical and noninjury factorsTopics in Spinal Cord Injury Rehabilitation7: 45968 |
19 | Leahy MJ, Chan F, Lui J, Rosenthal D, Tansey T, Wehman P, Kundu M, Dutta A, Anderson CA, Del Valle R, Sherman S, Menz FE(2014) An analysis of evidence-based best practices in the public vocational rehabilitation program: Gaps, future directions, and recommended steps to move forwardJournal of Vocational Rehabilitation41: 147163 |
20 | Neulicht AT, Berens DE(2011) The role of the vocational rehabilitation consultant in life care planningRiddick-Grisham S, Deming LMPediatric life care planning and case management2nd ed275318Boca RatonCRC Press |
21 | Nazarov ZE, Golden TP, von Schrader S(2012) Prevocational services and supported employmentwagesJournal of Vocational Rehabilitation37: 11912910.3233/JVR-2012-0605 |
22 | Pomeranz JL, Yu NS, Reid C(2010) Role and function study of life care plannersJournal of Life Care Planning9: 357118 |
23 | Ponsford J(2013) Factors contributing to outcome following traumatic brain injuryNeuroRehabilitation32: 80381510.3233/NRE-130904 |
24 | Reid C(2011) Life care planning, Entry inKreutzer JS, DeLuca J, Caplan BEncyclopedia of clinical neuropsychology14631464SpringerNew York |
25 | Robinson R(2014) Introduction to vocational rehabilitationRobinson RFoundations of forensic vocational rehabilitation112SpringerNew York |
26 | Sander AM, Clark A, Pappadis MR(2010) What is community integration anyway? Defining meaning following traumatic brain injuryJournal of Head Trauma Rehabilitation25: 212112710.1097/HTR.0b013e3181cd1635 |
27 | Strauser DR(2014) Introduction to the centrality of work for individuals with disabilitiesStrauser DRCareer development, employment, and disability in rehabilitation110SpringerNew York |
28 | Strauser DR, Chan F, Wang M, Wu M, Rahimi M(2014) Vocational evaluation in rehabilitationStrauser DRCareer development, employment, and disability in rehabilitation179192SpringerNew York |
29 | Targett PS, Wehman PH(2011) Essentials of transition planningEmployment: Community based choicesWehman PS127144Paul BrooksBaltimore, MD |
30 | Weed RO, Field TF(2001) Rehabilitation Consultant’s Hand bookrevised editionElliott & FitzpatrickAthens, GA |
31 | Wehman P, Inge KJ, Revell WG, Brooke VA(2007) Real work for real payPaul Brookes PublishingBaltimore, MD |
32 | Wehman PH, Targett PS, Cifu DX(2006) Job coaches: A workplace supportAmerican Journal of Physical Medicine & Rehabilitation85: 870410.1097/01.phm.0000228557.69308.15 |
33 | Wehman PH, Targett PS, West MD(2014) Supported employment/customized employmentStrauser DRCareer development, employment, and disability in rehabilitation325342SpringerNew York |
34 | West MD, Kregel J, Hernandez A, Hock T(1997) Everybody&s doing it: A national study of the use of natural supports in supported employmentFocus on Autism and Other Developmental Disabilities12: 3175181 |
35 | West MD, Targett PS, Crockatt SY, Wehman PH(2013) Return to work following traumatic brain injuryZazler ND, Katz DI, Zafonte RDBrain injury medicine:Principles and practice2nd ed13491359Demos,New York |
Figures and Tables
Fig.1
Example of productive activity elements in a life care plan.