
Early findings from the Wisconsin PROMISE project: Implications for policy and practice
Abstract
BACKGROUND:
Promoting the Readiness of Minors in Supplemental Security Income (PROMISE) is a U.S. Department of Education federal demonstration grant in collaboration with Health and Human Services, Labor, and the Social Security Administration. Wisconsin PROMISE is one of six model demonstration sites.
OBJECTIVE:
Through state inter-agency collaboration, the Wisconsin Division of Vocational Rehabilitation implemented Wisconsin PROMISE coordinated services and supports to youth with disabilities receiving supplemental security income (SSI) benefits and their families to improve education and career and financial self-sufficiency outcomes.
METHODS:
Wisconsin PROMISE enrolled 2,024 youth with disabilities receiving SSI benefits and their families who were randomly assigned to usual services or PROMISE services.
RESULTS:
Early data indicates positive results regarding engagement, employment, and earnings outcomes. Wisconsin PROMISE youth employment rates went from 1% in 2013 to 67% in 2018, 10-percentage points higher than observed with the control group.
CONCLUSION:
An overview of early findings from the Wisconsin PROMISE project site related to VR engagement, employment, and earnings outcomes of youth and family participants provides lessons learned that can be applied to VR practice.
1Introduction
Individuals with disabilities are less likely to be employed and are more likely to live in poverty than any other demographic group (Fogg, Harrington, & McMahon, 2011). Poverty and income inequality have dire consequences on the social, mental, and physical well-being of individuals with and without disabilities (Murali & Oyebode, 2004). Further, despite that nearly two-thirds of adults living in long-term poverty have disabilities, poverty and disability have historically been treated as separate issues, addressed by separate advocacy groups, and served by separate government programs (Lustig & Strauser, 2007). In reality, poverty and disability are mutually reinforcing each other in perpetuating inequalities across systems (Pokempner & Roberts, 2001). The struggle for daily survival affects everyday decision making and limits the time flexibility to identify, contact, and access needed services (Spears, 2011). Further, services are not always user friendly, and may not account for the hardships of poverty, including trauma, basic needs, ambivalence, time and opportunity for practical skill development, and adjusting service delivery based on the needs of families and their readiness to engage. Individuals struggling with scarcity will see less benefit, and thus be less likely to engage, with trainings that are more abstract and have delayed benefits. Training or supports need to be applicable to the individual’s current situation, as their current problems regarding scarcity of food, shelter and other basic needs will take precedence over abstract ideas or delayed consequences.
Employment is a key intervention for alleviating poverty among individuals with disabilities (Bonnel, 2004). Lack of employment opportunities excludes people with disabilities from full community inclusion and participation, stalls upward mobility, and greatly affects their health-related quality of life and well-being (U.S. Senate Committee on Health, Education, Labor and Pensions [SCHELP], 2012). As with adults with disabilities, young adults and transition-age youth with disabilities are more likely to be unemployed and have fewer work experiences relative to their peers without disabilities (SCHELP, 2012). Work experiences while in high school are the best predictor of employment as an adult (Carter, Austin, & Trainor, 2011; Test & Cease-Cook, 2012). The Workforce Innovation and Opportunity Act (WIOA) focuses on providing employment services to youth with disabilities for this very reason. The importance of helping young people with disabilities, particularly those receiving Supplemental Security Income (SSI), transition successfully from high school to higher education and into competitive, integrated employment that can lead to quality careers, economic security and the opportunity to join the middle class cannot be understated.
To receive SSI, youth with disabilities must have a Social Security Administration (SSA) disability determination and their households’ income must be deemed low enough. Youth receiving SSI and their families are eligible for a variety of services and supports, but the experience of poverty can limit access and engagement in these services. Prior to WIOA, only 13 percent of youth ages 19 to 23 receiving SSI payments had received services from a state vocational rehabilitation agency, and only 22 percent were employed, compared with 69 percent for all adults ages 20 to 24 (Rangarajan, Reed, Mamun, Martinez, & Fraker, 2009).
Promoting the Readiness of Minors in Supplemental Security Income (PROMISE) is a joint federal research demonstration of the US. Departments of Education (USDOE), Health and Human Services, and Labor, with evaluation support for the demonstration from the Social Security Administration. The USDOE funded six model demonstration projects to implement evidence-based practices in a randomized control trial, to address barriers and obstacles to economic independence and promote successful education and employment post-school outcomes for youth who receive SSI. Youth SSI recipients between the ages of 14 to 16 were eligible to enroll in the PROMISE demonstrations, which were funded for five to six years commencing in October 2013, in Arkansas; California; Maryland; New York; Wisconsin; and a six-state consortium which included Arizona, Colorado, Montana, North Dakota, South Dakota and Utah.
PROMISE was intended to improve the provision and coordination of services and supports for child SSI recipients and their families. Additionally, the intervention was designed to enable them to achieve improved outcomes, including graduating from high school ready for college and a career, completing postsecondary education and job training, obtaining competitive employment in an integrated setting, and increasing youth and family financial self-sufficiency.
Wisconsin PROMISE was one of six model demonstration projects. Wisconsin had a foundational system and partnerships in place, and PROMISE provided a mechanism to ensure that SSI youth were connected to the available services and supports that were most appropriate given their needs. Wisconsin PROMISE was implemented through Wisconsin’s Division of Vocational Rehabilitation (DVR), and Wisconsin PROMISE counselors provided case management to help youth and families navigate through services and connect with needed supports. In addition, the project provided the funding necessary to fill the gaps associated with the needed services and supports. The Wisconsin PROMISE approach promoted a fundamental change in current service delivery systems by creating a step-by-step process and overall individualized coordination to develop youth career interests and encourage families to consider alternatives that otherwise would not have been thought possible. The Wisconsin PROMISE intervention package includedevidence-based service delivery and supports, including rapid engagement, training in motivational interviewing and trauma informed care, and the provision of self-advocacy training, social skills training, paid work experiences, work incentive benefits counseling, and financial coaching. The evidence for each component is outlined below.
Rapid engagement is associated with better employment outcomes when compared to more gradual approaches (Bond, Dietzen, McGrew, & Miller, 1995; Drake, Bond & Becker, 2012). Wisconsin PROMISE case managers were required to have a minimum of monthly contact with participants to support youth and family engagement in the project (Yancey, Ortega, & Kumanyika, 2006). In addition to rapid engagement techniques, case managers implemented a variety of other techniques to promote a positive working alliance with the youth and their families. These techniques included providing additional information about the project, trust-building, motivational interviewing, and trauma informed care (Manthey, Jackson, & Evans-Brown, 2011; Wagner & McMahon, 2004).
Motivational interviewing is an important case management tool when youth and families are not contemplating or prepared to make changes in their educational or career track. Motivational interviewing techniques optimize the likelihood that individuals will begin to see that creating change in their lives is doable and can result in more life satisfaction. When implemented with fidelity, motivational interviewing has been shown to influence change talk, which predicts behavior change (Miller & Rose, 2009). Although motivational interviewing is typically implemented to change substance abuse, health-related behaviors, and gambling (Lundahl, Kunz, Brownell, Tollefson, & Burke, 2010), more recently it has been used to increase employment outcomes (Britt, Sawatzky, & Swibaker, 2018; Larson, Barr, Kuwabara, Boyle & Glenn, 2007; Torres, Frain, & Tansey, 2019).
In addition to motivational interviewing training, Wisconsin PROMISE DVR staff were trained in trauma informed care (Ko et al., 2008) because it was likely that PROMISE youth and their family members have experienced one or more types of trauma (Costello, Erkanli, Fairbank, & Angold, 2002; Marcin, Schembri, He, & Romano, 2003). Trauma informed care is an approach that emphasizes respect, empowerment, and creating connections. It teaches providers methods for enhancing the effectiveness of their work with trauma survivors, who might be easily overwhelmed by barriers. Trauma informed care can significantly impact success in education and employment (National Child Traumatic Stress Network, NCTSN).
Research has found that high expectations are linked to better employment outcomes (McGrew & Evans, 2004; Wagner, Newman, Cameto, Garza, & Levine, 2005). Therefore, PROMISE also provided parents with specific training aimed at increasing their expectations around employment and financial self-sufficiency. Wisconsin PROMISE case management focused on empowering youth and family members because self-advocacy and self-determination are predictors of post school education and employment (Deci & Ryan, 2000; Geenen et al., 2013; Test et al., 2009). To help translate this empowerment to the workplace, participants received social skills training by completing the “Skills to Pay the Bills” curriculum from trained service providers.
Workplace socialization skills are important for job retention and the career development of people with disabilities (Chan, Stauser, Gervey, & Lee, 2010; SHRM, 2012). The curriculum was developed by the U.S. Department of Labor-Office of Disability Employment Policy (ODEP) and is focused on teaching “soft” or workforce readiness skills to youth, including youth with disabilities. It was created for youth development professionals as an introduction to workplace interpersonal and professional skills. The curriculum is targeted for youth ages 14 to 21 in both in-school and out-of-school environments. The basic structure of the program is comprised of modular, hands-on, engaging activities that focus on six key skill areas: communication, enthusiasm and attitude, teamwork, networking, problem solving and critical thinking, and professionalism (http://www.dol.gov/odep/topics/youth/softskills/).
Employers report that knowledge of applied soft skills such as professionalism/work ethic, oral and written communications, teamwork/collaboration, and critical thinking/problem solving to be very important in today’s workplace (SHRM, 2012). Early introduction to soft skills development and application is particularly relevant in improving future employment opportunities for transition-age youth with disabilities (Carter, Trainor, Ditchman, Swedeen, & Owens, 2009; Murray & Doren, 2013; Test & Cease-Cook, 2012). The “Skills to Pay the Bills” curriculum was designed with input and review from youth and covers important areas including skills that promote success not only in jobs but across the span of a career. PROMISE youth had theopportunity to apply the skills directly in their employment experiences.
Although job skills training is important, even more critical is connecting youth to at least one, preferably two, work experiences that are paid at least minimum wage in an integrated community job lasting at least 90 days. This component of the intervention is essential because early, integrated, community work experience is associated with better integrated employment outcomes (Carter, Austin, & Trainor, 2011a&b; Test & Cease-Cook, 2012). The PROMISE DVR Counselor and resource team, which included both the youth and family members, determined the length and number of work experiences based upon the purpose of the work experience. Expectations and goals for the work experience were developed by the team and reviewed after the completion of work experience to determine progress of skill development if goals were met, and if additional work experiences were needed. Supports needed to complete work experiences were provided to ensure success on the job.
As youth and family members work, they may need help navigating the youth and family member public benefits. Work incentive benefits counseling (WIBC) provides informed choice to individuals on how employment income and savings will impact their disability monetary and health benefits (Lui et al., 2010). WIBC is significantly related to increases in beneficiary work and earnings (Delin, Hartman, & Sell, 2012; Kregel, 2012; Schimmel, O’Day, Roche, Livermore, & Harris, 2010; Tremblay, Smith, Xie, & Drake, 2004). Employment is a key component in alleviating poverty among individuals with disabilities, but additional tools, strategies, and supports may be needed (Cook, Burke-Miller, Jonikas, & Swarbrick, 2010; Cook & Elkin, 2010; Davies & Malloy, 2007; Fremstad, 2009). Without targeted financial coaching assistance, individual assets are rarely developed, and in turn, members of this population are at great risk for dislocation and worsening health status. Therefore, both WIBC and financial coaching were important components of Wisconsin PROMISE services.
Wisconsin PROMISE created: (a) access and connection to positive youth activities that developed the skills youth need for success educationally, vocationally, interpersonally, and personally. Support to families to learn how to encourage positive youth development within the family, (b) opportunities for youth, families, educators and providers to develop skills and attitudes necessary for collaborative team planning around educational, vocational and general life goals, (c) increased awareness by youth and their families of the range of vocational and educational opportunities available to both youth and their families if they choose a life path that includes a focus on success in these areas, and (d) access for both youth and their families to resources to address and assist them in attaining their goals.
The purpose of this study was to determine if Wisconsin PROMISE had an impact on early educational attainment and employment outcomes of PROMISE youth and their family members compared to services as usual. The hypothesis was that Wisconsin PROMISE outreach, case management, and wraparound services with an emphasis on connecting youth with paid competitive integrated employment experiences while still in high school was more intensive and more likely to engage SSI youth and their families than services as usual, so would have a positive impact on early educational and employment outcomes for youth and their family members. To better understand the impact of each service component this study explored the relationship of PROMISE specific services on employment outcomes.
2Methods
2.1Participants
Participants in this study were recruited from a list provided by SSA of all eligible participants (9,249 youth) from April 2014 to April 2016. Youth were eligible if they were 14, 15, or 16 years old, receiving SSI and submitted a signed consent to participate and intake form on the day of enrollment. Wisconsin PROMISE enrolled 2,024 teenagers receiving SSI. Once the Wisconsin Promise Formative Evaluation Team received the enrollment packet, they inputted the youth into the online Random Assignment System developed by Mathematica Policy Research (MPR), the national evaluator for PROMISE contracted through SSA. Participants were then randomly assigned to either the treatment or control group. Of those enrolled in the study, 1,018 were randomly assigned to the Wisconsin PROMISE Services group and 1,006 continued services as usual group. Youth randomly assigned to the treatment group were automatically enrolled in Wisconsin’s DVR services (presumed eligible because receiving SSI) where they received both DVR and Wisconsin PROMISE services. Family members who signed the consent form could receive educational, employment, and financial self-sufficiency services and supports through the Family Service Plan (FSP) connected to the youth’s PROMISE DVR case. Youth and family members randomly assigned to the control group received information about Wisconsin’s usual transition services. All participants received two gift cards to a local grocery or retail chain store, $15 for enrolling and $15 for completing the intake form. One youth from the control group and seven treatment youth withdrew from Wisconsin PROMISE.
2.2Measurement
The University of Wisconsin Stout Institutional Review Board (IRB) reviewed the research study design and measurement tools and approved the study for Human Subjects participation. All participants in both the treatment (1,018) and control (1,006) completed the intake form at enrollment. The intake form included identifying and contact information, household related information including income and public assistance; youth information including age, race, ethnicity, gender, and education; youth health status, including self-reported disability type; and parent and other household member information.
Service data. Wisconsin PROMISE service providers reported on service delivery through a secured Data Collection site set up via SharePoint. Wisconsin PROMISE work incentive benefits specialists recorded service length, number of contacts for both consult and analysis, number of service hours, work incentives, overpayments, age 18 redetermination, and challenges. Family advocates recorded completion of family advocacy trainings and if they assisted youth with the completion of the self-advocacy training. In addition, family advocates case noted all their contacts and activities with PROMISE youth and family members, recording activity type and date, number of service and travel hours, topics addressed, and case notes. Financial coaches recorded orientation date, information on the youth and family members PROMISE Individual Development Accounts (IDAs), and case notes.
Administrative data. In addition to the project specific data collected, the PROMISE Management Information System (MIS) included administrative data from multiple administrative data through inter-agency data sharing agreements. The PROMISE consent form included permission to share administrative data from these agencies. Administrative data included PROMISE specific data from Wisconsin DVR’s Integrated Rehabilitation Information System (IRIS) which is the Wisconsin DVR Case Management system that includes all Rehabilitation Service Administration (RSA) 911 data. Additional PROMISE data collected included case note tags (categorizing the nature of the case note), list of the youth’s family members, list of the youth’s resource team, resource team meeting notes, Family Service Plan (services for family members), youth and family member paid work, service completion dates, educational attainment, and engagement ratings.
Tracking rapid engagement and service completion. An effort was made to engage PROMISE youth and family members as quickly as possible, and services were individualized, meeting youth and families where they were at, to help increase the likelihood youth and family members would engage in services. In addition, if youth and family members did not respond to contacts right away, PROMISE staff continued to try to reach out to connect with youth and families to start and continue to engage in services. Wisconsin DVR PROMISE staff effort to implement rapid engagement activity was measured from date of enrollment to date of message, contact or activity where the case note tag of message, consumer contact, counseling, resource team meeting, or authorization of DVR or PROMISE service. This measure includes messages left by voicemail, which may or may not lead to engagement. Therefore, time to consumer engagement was counted by counting the number of days from enrollment to date with a case note with a tag of consumer contact, counseling, resource team meeting, or authorization of DVR or PROMISE service. Wisconsin PROMISE DVR staff also provided a rating of how engaged PROMISE youth and family members were within the PROMISE DVR case management system.
In addition to the DVR data, the PROMISE MIS also included quarterly earnings from the Wisconsin Unemployment Insurance (UI), employment services provided through Wisconsin’s Job Centers, Workforce Innovation and Opportunities Act (WIOA), and Youth Apprenticeship, Medicaid data, including long term care and mental health services, secondary and post-secondary school data, information on food share participation, and family and child welfare data, including Wisconsin Works.
Employment data. Wisconsin UI wage data were used to compare differences in employment rates and wages. Participants were considered to be employed if they had UI wages reported in the time period being studied. Participants were considered to be earning at Substantial Gainful Activity (SGA) if their UI quarterly wages were at least three times the monthly SGA amount. It is important to note that Wisconsin UI wage data only includes wage data from Wisconsin employers, so participants who worked in another state (e.g., Minnesota or Illinois) or for the federal government would not have wages reported in the Wisconsin UI system. Therefore, employment rates and wages are slightly underreported, but this holds equally true for both treatment and control participants allowing for a direct comparison between groups.
Educational attainment. In addition to connecting PROMISE youth and family members to employment opportunities, PROMISE DVR Counselors helped connect youth and family members to post-secondary education opportunities, helping to pay for these opportunities through training grants funded by DVR or PROMISE. Through a data sharing agreement with the National Student Clearinghouse, post-secondary educational enrollments and attainments of all PROMISE participants were added to the PROMISE MIS. Of note, only educational enrollments and attainments from institutions who agree to send their data to the National Student Clearinghouse is included in this data set, although most post-secondary institutions participate in this data sharing effort. Enrollments and attainments included in this report cover spring 2014 to summer 2018 for attainments and fall 2018 for enrollments.
Data Analysis. Differences in employment rates were analyzed in SPSS using a chi-square analysis to detect differences between categorical data (employed yes or no). Visual analysis was used to observe differences over time.
3Results
Due to the large amount of data collected throughout Wisconsin PROMISE, the results that follow are a highlight of early findings. Future articles will provide a more thorough analysis of the depth and breadth of data collected during Wisconsin PROMISE.
3.1Demographics of Wisconsin PROMISE youth
Demographics are summarized in Table 1. At enrollment, Wisconsin PROMISE youth self-reported a primary disability of mental health or behavioral (34 percent), developmental or intellectual (30 percent), and other (e.g., learning, speech, ADHD, etc.; 25 percent), and a smaller percentage reported other disabilities such as sensory, physical, and long-term illness. Other notable demographics included: 49 percent of youth were African American, 36 percent white, 10 percent Hispanic; 67 percent male; 66 percent living in a single parent/guardian household; 85 percent reported good overall health; 70 percent reported an annual household income at or below $25,000; 84 percent had an Individualized Education Plan at enrollment; and 77 percent were attending a traditional high school or middle school. All youth were receiving SSI and Medicaid at the time of enrollment. In addition, 60 percent of families reported someone in the household receiving Social Security Disability Insurance (SSDI), 67 percent reported receiving Food Share (Wisconsin’s version of the Supplemental Nutrition Assistance Program), 22 percent reported other household members receiving SSI, 12 percent reported housing assistance, and 4 percent were receiving Wisconsin Works (W2) or Temporary Assistance for Needy Families (TANF).
Table 1
Wisconsin PROMISE Demographic Information as Reported on the PROMISE Intake Form (n = 1011)
| Primary disability | Percent | Race/ethnicity | Percent | Other demographics | Percent | Age at enrollment | Percent | ||||||
| Mental Health or Behavioral | 34% | African American | 49% | Male | 67% | 14 | 41% | ||||||
| Developmental or Intellectual | 30% | White non-Hispanic | 36% | Single parent/guardian household | 66% | 15 | 27% | ||||||
| Other (e.g., learning, speech, ADHD, etc.) | 25% | Hispanic | 10% | Good overall health | 85% | 16 | 32% | ||||||
| Long-term Illness, Physical/Mobility, Sensory, Head Injury, Not Reported | 11% | Other, Not Reported | 5% | Annual Household Income at or below $25,000 | 70% | ||||||||
3.2Rapid engagement
Wisconsin DVR PROMISE staff effort to engage in rapid engagement as recorded by counselor case notes was most frequently one day (mode) with a median of four days and a mean of eight days. Time to consumer engagement in services was slightly longer with the mode still at one day, a median of eight days, and an average of 26 days. The majority (89 percent) of PROMISE youth had at least one face to face meeting with their Wisconsin PROMISE DVR Counselor. An additional eight percent of PROMISE youth had at least one phone conversation with their counselor. Most PROMISE youth (88 percent) had a signed DVR Individual Plan for Employment (IPE). After the initial IPE was written, engagement ratings ranged from highly engaged in services (50 percent) to mixed engagement (23 percent) to low engagement (27 percent).
3.3PROMISE service completion
Most PROMISE youth (90 percent) had at least one DVR or PROMISE funded service aimed to help them reach their employment goals, and 88 percent of PROMISE youth had an identified resource team. Almost half of the PROMISE youth (48 percent) also had a Family Service Plan serving 652 different family members, and 109 Wisconsin PROMISE treatment family members had their own DVR case compared to 82 control family members. PROMISE treatment youth completed a variety of DVR and PROMISE services including 713 PROMISE youth receiving employment services, 594 met with a PROMISE family advocate, 576 met with a financial coach, 535 met with a work incentive benefits specialist, 532 completed work-related social skills training, 476 completed self-advocacy modules, and 351 completed health promotion fact sheets. In addition, 284 youth and 230 family members had a PROMISE Individual Development Account (IDA).
3.4Work experience
Youth who received Wisconsin PROMISE Services were more likely to have a DVR case, engage in employment services, and have paid work than were youth randomly assigned to services as usual. From April 2014 to September 2018, 100 percent of PROMISE youth in the treatment group had a DVR case, compared to 33 percent youth in the control group. DVR services were correlated with higher employment rates (Kaya et al., 2016; Rumrill et al., 2017), and youth receiving PROMISE services were more likely to be employed.
During PROMISE services, from April 2014 to September 2018, 67 percent of PROMISE treatment youth had reported UI wages compared to 57 percent in the control group. A chi-square test of independence was performed, and PROMISE Services had a significant impact on employment rates, X2 (1, N = 2016) = 23.37, p < .001. About two thirds of control youth never connected to DVR as part of usual services. The employment rate was even lower for youth in the control group without a DVR case at 51 percent. Despite the higher employment rates observed with treatment youth, an equal number of treatment and control youth had SGA equivalent earnings reported in at least one quarter during the service period from April 2014 to September 2018, 78 (eight percent) treatment youth and 78 (eight percent) control youth.
Figure 1 illustrates quarterly employment rates for treatment and control youth over time from prior to enrollment in Wisconsin PROMISE services starting the first quarter of 2013 until the last quarter of Wisconsin PROMISE services the third quarter of 2018. Youth were 14 to 16 years old when they enrolled in Wisconsin PROMISE, so employment rates prior to enrolling in Wisconsin PROMISE were low, one to two percent for both youth in treatment or control groups. After enrollment started in April, the second quarter of 2014, employment rates started to increase for both groups but at a higher rate from treatment group youth compared to control group youth. By the end of the enrollment period in April the second quarter of 2016, 16 percent of treatment youth had UI wages compared 12 percent in the control group. After the enrollment period, differences between the two groups increased. Employment rates by quarter were higher and more variable for youth in the treatment group with higher employment rates observed during quarters that included summer months. June is in the second quarter of the calendar year and even higher employment rates were observed in quarter three, which includes both July and August. By the last quarter of Wisconsin PROMISE service delivery, 41 percent of treatment youth and 35 percent of control youth had reported wages. The percent of control youth with reported wages during this quarter drops to 31 percent when only including youth in the control group without a DVR case.
Fig.1
Percent Youth with UI Wages by Quarter and Treatment Group Figure Caption: Percent of youth who were 14 or older with wages reported to Wisconsin UI in calendar quarters from quarter one of 2013 to quarter three of 2018. Percent of treatment youth with reported wages is represented by the dashed line with closed squares, control group is represented by the solid line with closed triangles, and the subset of the control group without a VR case is represented by the solid line with open circles.
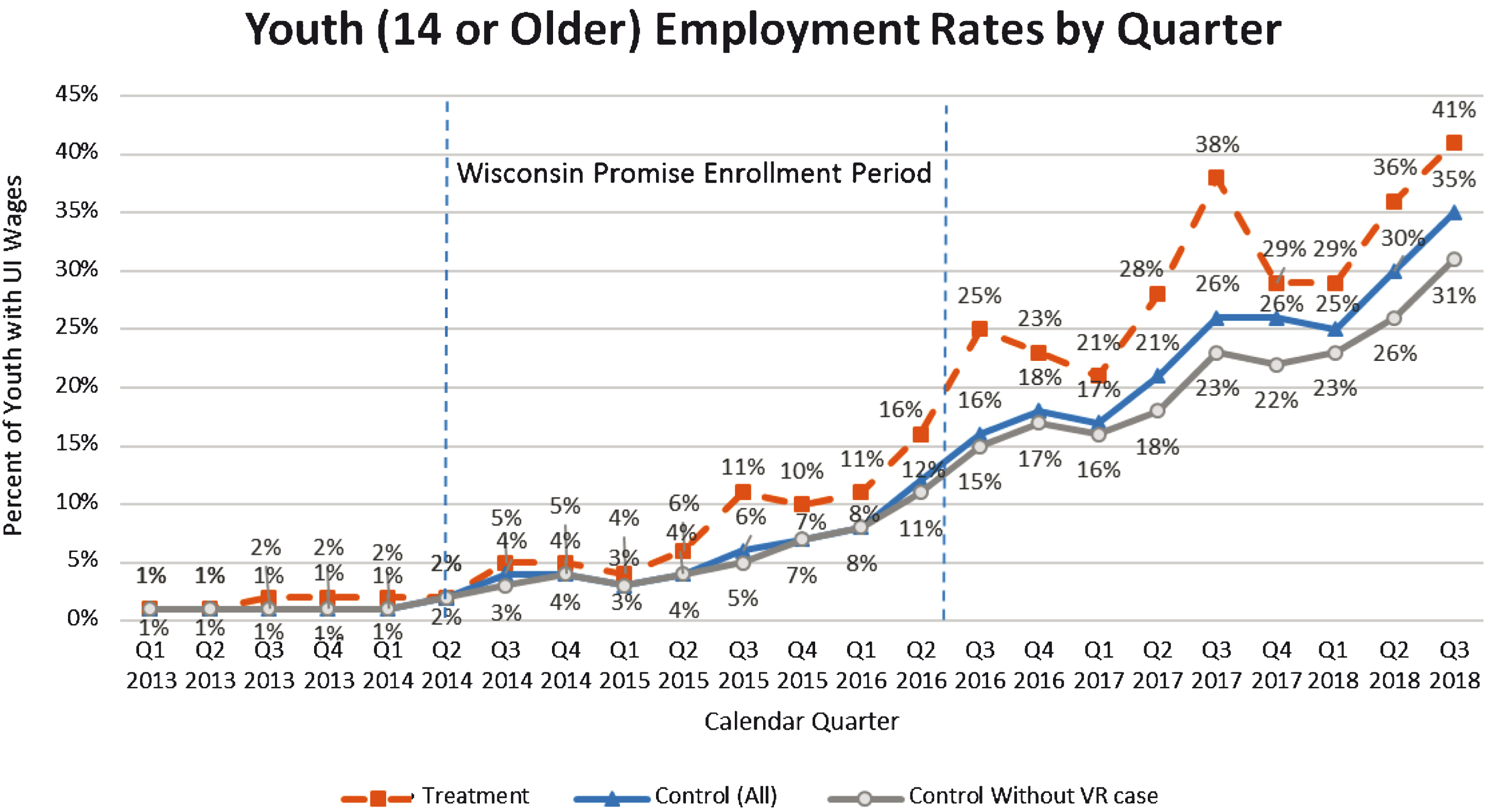
Not only were treatment group youth employment rates higher than observed for the control (usual) services group but PROMISE youth’s employment rate also increased to a rate comparable to youth without disabilities in Wisconsin. According to the Community Population Survey, 53 percent of Wisconsin youth ages 16 to 19 were employed from July 2017 to June 2018. In comparison, 53 percent youth who received Wisconsin PROMISE Services had UI reported wages during this same period compared to 43 percent in the full control group and 38 percent of youth in the control group without a DVR case. In other words, youth with SSI who received PROMISE Services increased their employment rates comparable to the employment rates observed for youth without disabilities.
Employment rates for Wisconsin PROMISE family members increased at similar rates for both treatment and control groups. In the second quarter of 2014, the quarter when Wisconsin PROMISE enrollment began, 39 percent of parents in both the treatment and control groups had Wisconsin reported wages. Employment rates increased for both groups over time, and by the last quarter of services, July through September of 2018, half of the parents had UI wages reported, slightly higher in the control group 50 percent (514 of 1036) than the treatment group 48 percent (512 of 1073). During the full PROMISE service period, from April 2014 to September 2018, 66 percent (685 of 1036) of parents in the control group had a quarterly wage reported in at least one quarter during this period compared to 68 percent (729 of 1073) of parents in the treatment group. A chi-square test of independence was performed, and PROMISE Services did not have a significant impact on parent employment rates, X2 (1, N = 2109) = 0.79, p = .37. According to the Bureau of Labor Statistics, during this period Wisconsin unemployment rates decreased from 5.7 percent in April 2014 to 3.0 percent in September 2018, so increases in parent employment rates may have been related to the improved economy.
Household members experienced similar employment rate increases across treatment and control groups with a few notable differences. It is important to note that household members included both siblings and adult family members, because siblings were usually around high school age their employment rates were lower, so average household employment rates started lower than observed with the parents. In addition, more household members in the treatment group signed the consent form to participate in Wisconsin PROMISE presumably because those in the treatment group could receive services to help them reach their education or employment goals through the PROMISE Family Service Plan. At enrollment, 18 percent (52 of 287) of treatment household members age 14 or older reported UI wages compared to 10 percent (12 of 119) control household members. This increased to 46 percent (159 of 346) for treatment household members and 48 percent (60 of 126) for control household members by the third quarter of 2018. Throughout the PROMISE Services period, 62 percent (178 of 346) of treatment household members and 61 percent of control household members (77 of 126) had reported wages in at least one quarter between April 2014 and September 2018.
3.5Services related to employment rates
Wisconsin PROMISE is a package of services including wraparound case management, which included close collaboration with schools, employment services, financial coaching, work incentive benefits counseling and family and self-advocacy. Each of these services were positively correlated with employment outcomes.
Collaboration with schools. At least one person from school was identified on 614 of the 884 (69 percent) resource teams. Youth with school staff included on their resource team had higher employment outcomes with 70 percent with reported UI wages during the service period compared to 63 percent of youth with reported wages for those with no resource team or a resource team that did not include school staff [X2 (1, N = 1011) = 5.33, p = .021].
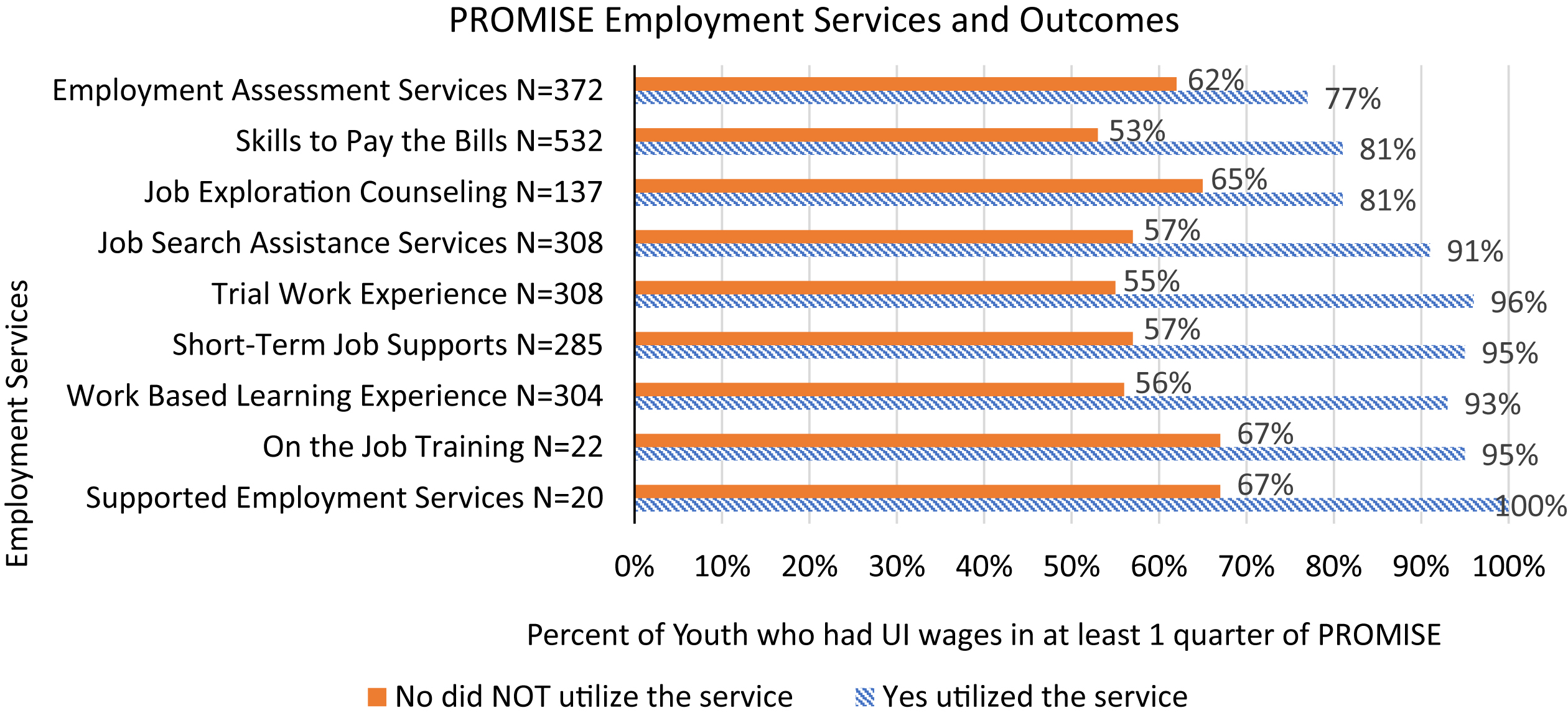
Employment services. Wisconsin PROMISE youth had access to all employment services available through DVR, which allowed for the individualization and customization of employment services. Throughout PROMISE, 713 (71 percent) of PROMISE youth received employments services, which included employment assessment services, Skills to Pay the Bills (soft skills training), job exploration counseling, job search assistance, temporary work experience, short-term job supports, work-based learning, on the job training, and supported employment services. These employment services were positively correlated with employment outcomes. Of the 372 PROMISE youth who received employment assessment services 77 percent had reported wages in at least one quarter between April 2014 and September 2018. In comparison, 62 percent of youth who did not receive employment assessment services had wages reported during this period [X2 (1, N = 1011) = 21.96, p < .001]. Even higher rates were observed for the 532 youth who received Skills to Pay the Bills training with 81 percent of youth who received the training with reported wages compared to 53 percent of youth who did not receive this training [X2 (1, N = 1011) = 88.03, p < .001]. PROMISE youth who received job exploration counseling and job search assistance also had higher employment rates. Of the 137 with job exploration counseling, 81 percent with reported wages compared to 65 percent of youth who did not receive job exploration counseling [X2 (1, N = 1011) = 12.26, p < .001], and 91 percent of the 308 youth who received job search assistance had UI wages [X2 (1, N = 1011) = 109.5, p < .001]. Employment rates were even higher for youth who received on the job supports. More specifically, 96 percent of the 308 youth who received temporary work experience were employed after this work experience [X2 (1, N = 1011) = 150.9, p < .001]; 95 percent of the 285 youth who received short-term job supports had a paid job after receiving these supports [X2 (1, N = 1011) = 127.64, p < .001]; 93 percent of the 304 youth who participated in a work based learning experience had a paid job after this work experience [X2 (1, N = 1011) = 126.03, p < .001]; 95 percent of the 22 youth who received on the job training were working after this training [X2 (1, N = 1011) = 8.03, p = .005]; and 100 percent of the 20 youth who received supported employment services were working before PROMISE services ended in September 2018 [X2 (1, N = 1011) = 9.84, p < .002]. The impact of these services on employment rates are illustrated in Figure 2.
Fig.2
Employment Service Impact on Employment Outcomes Figure Caption. Percent of PROMISE youth who had a job following the receipt of a DVR employment service. N is the count of PROMISE youth who received the service. The number of youth who did not receive the service can be calculated by subtracting 1011 – N.
Financial services. Meeting with a work incentive benefits specialist, financial coach, and having a savings account were all positively correlated with youth employment rates. Of the 535 PROMISE youth who met with a work incentive benefits specialist, 78 percent had reported wages compared to 55 percent of those who did not meet with a benefits specialist [X2 (1, N = 1011) = 58.9, p < .001]. Furthermore, 81 percent of youth earning SGA met with a work incentives benefits specialist. Youth that met with a work incentive benefits specialist had three times as many jobs and three times the total weekly earnings as youth who did not meet with a work incentive benefits specialist. Similarly, 79 percent of the 576 youth who met with a financial coach had reported wages while enrolled in Wisconsin PROMISE compared to 52 percent of the youth who did not meet with a financial coach [X2 (1, N = 1011) = 78.71, p < .001], and 87 percent of youth earning SGA met with a financial coach. Youth who met with a financial coach had five times as many jobs and weekly earnings compared to those who did not meet with a financial coach. Less youth reported having a savings account while in PROMISE, but those who did also reported higher employment rates, with 83 percent of the 377 youth with a savings account with reported wages [X2 (1, N = 1011) = 68.63, p < .001].
Family and self-advocacy. Family and self-advocacy training was also related to increased employment outcomes. Of the 594 youth whose families met with a PROMISE family advocate, 71 percent worked during PROMISE [X2 (1, N = 1011) = 8.43, p < .004]. This employment rate was even higher for youth whose families completed the family advocacy training on navigating transition services and supports and employment possibilities for youth with disabilities with 77 percent of the 414 youth with families who completed the training who had a job while enrolled in PROMISE. Of families who completed the Wisconsin PROMISE family advocacy training, 90 percent agreed the training elevated their expectations of what is possible for their child after high school, 84 percent reported knowing about transition supports for youth, 71 percent reported using more and different resources, and 50 percent reported increases in regular job opportunities for PROMISE youth.
Like family advocacy training, employment rates were correlated with self-advocacy training. Of the 476 PROMISE youth who completed self-advocacy training 79 percent were employed compared to an employment rate of 57 percent for youth who did not complete self-advocacy training [X2 (1, N = 1011) = 52.54, p < .001]. After self-advocacy training, 84 percent of PROMISE youth reported that their abilities help them handle difficult events, and 97 percent reported they know what they need, what they like, and where they excel.
3.6Educational Attainment
Wisconsin PROMISE youth post-secondary enrollment and attainments were similar across both research groups with around 16 percent of youth enrolling in at least one post-secondary program (165 of 1011 treatment youth and 157 of 1005 control youth). Only two treatment youth and one control completed their post-secondary training as of the Summer of 2018, but these low rates may be attributed to the fact that as of August 31, 2018, 34 percent of Wisconsin PROMISE youth were under age 18, 27 percent were 18 years old, 23 percent were age 19, 14 percent were 20, and only one percent were 21 years old. Given that youth with disabilities can remain in high school until they are 21, there simply was not enough time for most PROMISE youth to reach a post-secondary educational attainment during the study period.
Similar to the education enrollments observed for youth, there were slight observable differences in Wisconsin PROMISE parent and household educational enrollments and attainments although these differences were not statistically significant. From spring 2014 to fall 2018, 191 of 1073 (18 percent) treatment parents and 81 of 346 (23 percent) treatment household members had a post-secondary enrollment compared to 177 of 1036 (17 percent) control parents and 26 of 126 (21 percent) control household members. Parent and household members in the treatment group also had more educational attainments from spring 2014 to summer 2018 with 53 of 1073 (5 percent) of treatment parents with 79 educational attainments compared to 41 of 1036 (4 percent) of control parents with 51 educational attainments. There were a wide range of educational attainments ranging from certificates to diplomas to associate degrees to bachelor’s degrees to master’s degrees. Fewer household members had reached an educational attainment by Summer 2018, five treatment household members and two control household members. Again, household members tended to be younger (e.g., siblings), so few were old enough to reach a post-secondary attainment.
4Discussion
Poverty can impact engagement in services (Spears, 2011). Youth and families living day to day with concerns about income, food and shelter insecurity make it difficult to always follow through with program expectations. In addition, traditional training and service approaches did not always account for the hardships of poverty including trauma, basic needs, ambivalence, need for a hands-on learning, and meeting the youth and families where they were at. For these reasons, PROMISE case management included key features that helped to increase engagement in services supports, including bringing services and supports to youth and families and using effective outreach methods including emails, texts, voice mails, and postcards. Case management was employment focused, strength-based with a focus on empowerment and included person centered planning, rapid engagement, motivational interviewing, and trauma informed care. PROMISE DVR counselors also ensured that youth and families were connected with resources to better navigate public benefits and financial concerns. This approach, accompanied with ensuring youth had paid work experiences, led to increased employment outcomes.
The first step is ensuring youth receiving SSI are connected to the service and supports they are eligible for. Knowing that poverty factors can interfere with accessing employment services, service programs and systems need to engage in more targeted outreach through direct mailings, emails, and texts. In Wisconsin PROMISE, we found mailing a postcard directly to youth and families, something that was visually appealing, with few words but contained contact information to learn more was an effective way to get the attention of youth and families and connect with these services and supports. Texts and emails in addition to phone calls were also important tools to support continued communication.
Once youth connected to services and supports by the PROMISE DVR counselors, youth and families were sometimes resistant to change and may have past trauma impacting their engagement in services. As a means of addressing this, PROMISE DVR counselors utilized employment focused person-centered planning along with trauma informed care and motivational interviewing. One of the key reasons that youth and families were resistant to work was fear that working would negatively impact the public benefits they were receiving, including SSI, Medicaid, Food Share, and Housing assistance. To help with these concerns, PROMISE DVR counselors referred youth and families to local work incentive benefits specialists to talk about how they could work, maximize their income and ensure the youth still had the services and supports needed, including healthcare. As youth and families started working, they were also referred to a financial coach to talk about how they could maximize their earnings and build assets to help increase their overall financial self-sufficiency. In addition, youth and families were referred to family advocates to help them navigate transition resources and receive information on what work is possible for youth with disabilities given a good job match and connection with the right supports. Family advocates also helped to teach family and self-advocacy further empowering youth and family members.
Connecting to the right services and supports was also facilitated by identifying local resource teams for each PROMISE youth. Resource teams included the youth, family members, PROMISE DVR counselor, service providers, schools, and other service and supports the youth was connected to such as long-term care, mental health, child welfare, juvenile justice and other local supports including family, friends, neighbors and other supports the youth had in their communities. Ensuring school participation in the resource team was especially important in coordinating the school transition and VR services to better support youth in achieving their post-school education and career goals.
Wisconsin PROMISE demonstrated the importance of connecting youth receiving SSI to employment services available through VR, as youth in both the PROMISE and usual services groups who received employment services through DVR, especially paid work experiences and on the job supports, had higher employment rates. Targeted outreach to youth and their families, along with employment-focused case management, provides a clear strategy for engaging and supporting youth receiving SSI in paid work experiences and employment.
Regarding sustainability of the model, Wisconsin PROMISE has helped inform the design of Pre-Employment Transition Services in Wisconsin, as indicated in WIOA. The establishment of soft skills training using the Department of Labor’s Skills to Pay the Bills Training Curriculum, allowing for a consultation model of providing work incentives benefits counseling that is enhanced when adding financial coaching, informing the implementation of self-advocacy training in an interactive training model, adding text messaging as a way to connect to youth, enhancing relationships with schools, and improving counselor case management through rapid engagement, motivational interviewing, and trauma informed care are all elements informed through PROMISE that have been integrated into DVR policy and practice statewide.
When first implementing services, PROMISE service providers tried implementing group training opportunities for family advocacy training, financial capability training, soft skills training, but found youth and families rarely attended these trainings. In contrast, service engagement was higher when services were delivered in an individual coaching or consultation model. PROMISE youth and families engaged more when services were individualized into work incentive benefits consultation, financial coaching, family and self-advocacy training provided in individualized training sessions with family and youth, and when soft skills training was provided to youth as part of an individually placed student work-based learning opportunity. Similarly, other research has found intensive services were more effective than group trainings in achieving employment outcomes for adult public workforce services (Forston et al., 2017).
4.1Limitations
WIOA implementation occurred while PROMISE enrollment and services were beginning. Because WIOA services have a focus on transition aged youth, the timing of WIOA role out likely had an impact on employment outcomes for PROMISE youth in both the control and treatment groups, thus potentially reducing the overall impact of Wisconsin PROMISE services had in comparison to the new reality of usual services, especially for the third of youth in the control group who received DVR services during the PROMISE service period. In addition, because PROMISE youth enrolled when they were as young as 14, DVR and services providers needed time and training to adjust their service models to better serve younger youth. Prior to PROMISE and WIOA, the service system was more accustomed to serving adults than youth under 18, so implementation of PROMISE services took longer than originally anticipated. For these reasons, the full impact of early work experiences is just starting to be realized. More data needs to be collected over a longer period of time to truly evaluate the long-term impacts PROMISE services had on education, employment, and financial self-sufficiency.
4.2Recommendations for Future VR Practice
Recommendations moving forward include (a) continued data sharing across state agencies to ensure effective inter-agency service coordination, (b) connect youth receiving SSI to employment-focused services and supports through schools, state VR agencies, long-term care, mental health, and others, and (c) continued interagency commitment to supporting employment and career pathways for youth with disabilities, including those receiving or eligible for SSI benefits. Future efforts should include a focus on increasing credentials and measurable skills gains as both lead to better jobs and career development. While entry-level jobs are appropriate while in high school and early adulthood, it is important that youth with disabilities have the opportunity to grow in their careers by working more hours and increase their wages. The goal is to decrease reliance on public benefits and increase the likelihood of financial self-sufficiency in the future, and in order to do so, competitive integrated employment serves as the foundation.
Furthermore, service agencies can learn from PROMISE implementation by ensuring trainings and supports are provided where youth are at whether that be in their homes, in the community, at schools, or on the job, and providing training in an inter-active model that allows for practice and shares information over time as needed rather than trying to share all the information at once in a passive setting. Finally, it is recommended that agencies work together to ensure that family members, not just the youth, have the support needed to navigate services and systems and information on post-school possibilities for all youth with disabilities.
Wisconsin PROMISE has demonstrated that more youth receiving SSI can be connected to employment than typically have been through services as usual. Youth with disabilities continue to show their skills, strengths, and potential can help build a better workforce in all local communities. Models that empower youth and their families while at the same time provide the needed disability related supports and connection to paid work can increase employment outcomes and self-sufficiency.
Conflict of interest
The authors have no conflict of interest to declare.
Acknowledgments
The contents of this paper were developed under a cooperative agreement with the U.S. Department of Education, Office of Special Education Programs, associated with PROMISE Award #H418P140002. Selete Avoke served as the project officer. The views expressed herein do not necessarily represent the positions or policies of the Department of Education or its federal partners. No official endorsement by the U.S. Department of Education of any product, commodity, service or enterprise mentioned in this publication is intended or should be inferred.
References
1 | Bond, G.R. , Dietzen, L.L. , McGrew, J.H. & Miller, L.D. ((1995) ). Accelerating entry into supported employment for persons with severe psychiatric disabilities. Rehabilitation Psychology, 40: , 75–94. |
2 | Bonnel, R. ((2004) ). Poverty reduction strategies: Their importance for disability. GLADNET Collection, retrieved from Cornell University ILR School DigitalCommons@ILR. |
3 | Britt, E. , Sawatzky, R. & Swibaker, K. ((2018) ). Motivational interviewing to promote employment. Journal of Employment Counseling, 55: , 176–189. |
4 | Carter, E. W. , Austin, D. , & Trainor, A. A. ((2011) a). Factors associated with the early work experiences of with severe disabilities. Intellectual and Developmental Disabilities, 49: 233–247. |
5 | Carter, E. W. , Austin, D. , & Trainor, A. A. ((2011) b). Predictors of postschool employment outcomes for young adults with severe disabilities. Journal of Disability Policy Studies, 23: , 50–63. |
6 | Carter, E. W. , Ditchman, N. , Sun, Y. , Trainor, A. A. , Swedeen, B. & Owens, L. ((2010) ). Summer employment and community experiences of transition-age youth with severe disabilities. Exceptional Children, 76: , 194–212. |
7 | Chan, F. , Strauser, D. , Gervey, R. & Lee, E. J. ((2010) ). Introduction to demand-side factors related to employment of people with chronic illness and disability. Journal of Occupational Rehabilitation, 20: , 407–411. |
8 | Cook, J. , Burke-Miller, J. , Jonikas, J. & Swarbrick, M. ((2010) ). Asset development for people with psychiatric disabilities: The essential role of financial security in recovery. Prepared for the U.S. Department of Education, National Institute on Disability and Rehabilitation Research, and the Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, Cooperative Agreement. Retrieved from http://www.cmhsruic.edu/download/NRTC4.IDA%20Project%20Report.10.25.10.pdf. |
9 | Cook, R. & Elkin, S. ((2010) ). Linking people with disabilities to IDAs: Findings from two pilot sites. The Lewin Group report for The Department of Health and Human Services, Office of Community Services. Retrieved from http://www.lewin.com/publications/?published=anytime&expertiseid=27B3D7F0-4310-4F8F-92BC-07763CB66C97. |
10 | Costello, E. J. , Erkanli, A. , Fairbank, J. A. & Angold, A. ((2002) ). The prevalence of potentially traumatic events in childhood and adolescence. Journal of Traumatic Stress, 15: , 99–112. |
11 | Davies, T. & Malloy, J. ((2007) ). Asset development for people with disabilities: A conceptual framework. Prepared for the National Consortium for Health Systems Development. Retrieved from http://www.nchsd.org/library/index.asp?topic=10023. |
12 | Deci, E. L. & Ryan, R. M. ((2000) ). The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychological Inquiry, 11: , 227–268. |
13 | Delin, B. S. , Hartman, E. C. & Sell, C. W. ((2012) ). The impact of work incentive benefits counseling on employment outcomes: Evidence form two return-to-work demonstrations. Journal of Vocational Rehabilitation, 36: , 97–107. |
14 | Delin, B. S. , Reither, A. E. , Drew, J. A. & Hanes, P. ((2004) ). Final project report Wisconsin Pathways to Independence.. |
15 | Drake, R. E. , Bond, G. R. & Becker, D. R. ((2012) ). Individual Placement and Support: An Evidence-Based Approach to Supported Employment. New York: Oxford University Press. |
16 | Fogg, N. , Harrington, P. & McMahon, B. ((2011) ). The underemployment of persons with disabilities during the Great Recession. The Rehabilitation Professional, 19: 3–10. |
17 | Fortson, K. , Rotz, D. , Burkander, P. , Mastri, A. , Schochet, P. , Rosenberg, L. , McConnell, S. & D’Amico, R. ((2017) ). Providing Public Workforce Services to Job Seekers: 30-month Impact Findings on the WIA Adult and Dislocated Worker Programs. Princeton, NJ: Mathematica Policy Research. |
18 | Fremstad, S. ((2009) ). Half in ten: Why taking disability into account is essential to reducing income poverty and expanding economic inclusion. Washington, DC: Center for Economic and Policy Research. Retrieved from http://www.cepr.net/index.php/publications/reports/half-in-ten/. |
19 | Geenen, S. , Powers, L. E. , Powers, J. , Cunningham, M. , McMahon, L. , Nelson, M. , Dalton, L. D. , Swank, P. & Fullerton, A. ((2013) ). Experimental study of a self-determination intervention for youth in foster care. Career Development and Transition for Exceptional Individuals 36: , 84–95. |
20 | Kaya, C. , Chan, F. , Rumrill, P. , Hartman, E. , Wehman, P. , Iwanaga, K. , Pai, C.H. & Avellone, L. ((2016) ). Vocational rehabilitation services and competitive employment for transition-age youth with autism spectrum disorders. Journal of Vocational Rehabilitation, 45: , 73–83. |
21 | Ko, S. J. , Ford, J. D. , Kassam-Adams, N. , Berkowitz, S. J. , Wilson, C. , Wong, M. , Brymer, M. J. & Layne, C. M. ((2008) ). Creating trauma-informed systems: Child welfare, education, first responders, health care, juvenile justice. Professional Psychology: Research and Practice, 39: , 396–404. |
22 | Kregel, J. ((2012) ). Work incentives planning and assistance program: Current program results document the program’s ability to improve employment outcomes, reduce dependence on benefits, and generate cost savings for SSA. Journal of Vocational Rehabilitation, 36: , 3–12. |
23 | Larson, J. E. , Barr, L. K. , Kuwabara, S. A. , Boyle, M. G. & Glenn, T. L. ((2007) ). Process and outcome analysis of a supported employment program for people with psychiatric disabilities. American Journal of Psychiatric Rehabilitation, 39: , 339–353. |
24 | Lequerica, A. H. , Rapport, L. J. , Whitman, R. D. , Millis, S. R. , Vangel S. J. Jr , Hanks, R. A. & Axelrod, B. N. ((2006) ). Psychometric properties of the rehabilitation therapy engagement scale when used among individuals with acquired brain injury. Rehabilitation Psychology, 51: , 331–337. |
25 | Lui, J. W. , Chan, F. , Fried, J. H. , Lin, C. P. , Anderson, C. A. & Peterson, M. ((2010) ). Roles and functions of benefits counseling specialists: A multi-trait analysis. Journal of Vocational Rehabilitation, 32: , 163–173. |
26 | Lundahl, B. W. , Kunz, C. , Brownell, C. , Tollefson, D. & Burke, B. L. ((2010) ). A meta-analysis of motivational interviewing: Twenty-five years of empirical studies. Research on Social Work Practice, 20: , 137–160. |
27 | Lustig, D. C. & Strauser, D. R. ((2007) ). Causal relationships between poverty and disability. RehabilitationCounseling Bulletin, 50: , 194–202. |
28 | Manthey, T. , Jackson, C. & Evans-Brown, P. ((2011) ). Motivational interviewing and vocational rehabilitation: A review with recommendations for administrators and counselors. Journal of Applied Rehabilitation Counseling, 42: , 3–14. |
29 | Marcin, J. P. , Schembri, M. S. , Jingsong, H. & Romano, P. ((2003) ). A population-based analysis of socioeconomic status and insurance status and their relationship with pediatric trauma hospitalization and mortality rates. Research and Practice, 93: , 36–40. |
30 | Martin, D. J. , Garske, J. P. & Davis, M. K. ((2000) ). Relation of the therapeutic alliance with outcome and other variables: A meta-analytic review. Journal of Consulting and Clinical Psychology, 68: , 438–450. |
31 | McGrew, K. S. & Evans, J. ((2004) ) Expectations for students with cognitive disabilities: Is the cup half empty or half full? Can the cup flow over? (Synthesis Report 55.) Minneapolis, MN: University of Minnesota, National Center on Educational Outcomes. |
32 | Miller, W. R. & Rose, G. S. ((2009) ). Toward a theory of Motivational Interviewing. American Psychologist, 64: , 527–537. |
33 | Murali, V. & Oyebode, F. ((2004) ). Poverty, social inequality and mental health. Advances in Psychiatric Treatment, 10: , 216–224. |
34 | Murray, C. & Doren, B. ((2013) ). The effects of working at gaining employment skills on the social and vocational skills of adolescents with disabilities: A school-based intervention. Rehabilitation Counseling Bulletin, 56: , 96–107. |
35 | Pokempner, J. & Roberts, D. E. ((2001) ). Poverty, welfare reform, and the meaning of disability. Ohio State Law Journal, 62: , 1–23. |
36 | Rangarajan, A. , Reed D. , Mamun, A. , Martinez, J. & Fraker, T. ((2009) ) , The Social Security Administration’s youth transition demonstration projects: Analysis plan for interim reports. Princeton, NJ: Mathematica Policy Research. |
37 | Rangarajan, A. , Fraker, T. , Honeycutt, T. , Mamun, A. , Martinez, J. , O’Day, B. & Wittenbrug, D. ((2009) ). The Social Security Administration’s Youth Transition Demonstration Projects: Evaluation Design Report. Available from www.mdrc.org/sites/default/files/full_576.pdf. |
38 | Rumrill, P. D. , Merchant, D. , Kaya, C. , Chan, F. , Hartman, E. & Tansey, T. ((2017) ). Demographic and service-related correlates of competitive employment outcomes among state-federal vocational rehabilitation clients with learning disabilities: A purposeful selection logistic regression analysis. Journal of Vocational Rehabilitation, 47: , 123–134. |
39 | Schimmel, J. , O’Day, B. , Roche, A. , Livermore, G. & Harris, D. ((2010) ). Evaluation of the work incentives planning and assistance (WIPA) program: Beneficiaries served, services provided and program costs (Report No. 08977.160). Washington, DC: Mathematica Policy Research. |
40 | Society for Human Resource Management (SHRM). (May (2012) ). Survey Findings: Employing People with Disabilities: Practices and Policies Related to Retention and Advancement. Cornell University ILR School Employment and Disability Institute. |
41 | Spears, D. ((2011) ). Economic decision-making in poverty depletes behavioral control. Journal of Economic Analysis & Policy, 11: , Article 72. |
42 | Test, D. W. & Cease-Cook, J. . ((2012) ). Evidence-based secondary transition practices for rehabilitation counselors. Journal of Rehabilitation, 78: , 30–38. |
43 | Test, D. W. , Mazzotti, V. L. , Mustian, A. L. , Fowler, C. H. , Kortering, L. & Kohler, P. ((2009) ). Evidence-based transition predictors for improving post school outcomes for students with disabilities. Career Development for Exceptional Individuals, 32: , 180–181. |
44 | Torres, A. , Frain, M. & Tansey, T. N. ((2019) ). The Impact of Motivational Interviewing Training on Rehabilitation Counselors: Assessing Working Alliance and Client Engagement. A Randomized Controlled Trial. Rehabilitation Psychology. |
45 | Tremblay, T. , Smith, J. , Xie, H. & Drake, R. ((2004) ). The impact of specialized benefits counseling services on Social Security Administration disability beneficiaries in Vermont. Journal of Rehabilitation, 5–11. |
46 | U.S. Senate Committee on Health, Education, Labor and Pensions ((2012) ) Unfinished business: Making hiring people with disabilities a national priority. Washington, DC: Author. Retrieved from http://www.harkin.senate.gov/documents/pdf/500469b49b364.pdf. |
47 | Vong, S. , Cheing, G. , Chan, F. , So, E. & Chan, C. C. ((2011) ). Motivational enhancement therapy in addition to physical therapy improves motivational factors and treatment outcomes in people with low-back pain: A randomized controlled trial. Archives of Physical Medicine and Rehabilitation, 92: , 176–183. |
48 | Wagner, C. C. & McMahon, B. T. ((2004) ). Motivational interviewing and rehabilitation counseling practice. Rehabilitation Counseling Bulletin, 47: , 152–161. |
49 | Wagner, M. , Newman, L. , Cameto, R. , Garza, N. & Levine, P. ((2005) ). After High School: A First Look at the Postschool Experiences of Youth with Disabilities. A Report From the National Longitudinal Transition Study-2 (NLTS2), Menlo Park, CA: SRI International. |
50 | Yancey, A. K. , Ortega, A. N. & Kumanyika, S. K. ((2006) ). Effective recruitment and retention of minority research participants. Annual Review of Public Health, 27: , 1–28. |


