
Rehabilitation interventions for weaning from mechanical ventilation in patients with spinal cord injury: A systematic review
Abstract
BACKGROUND:
Despite the fact that weaning from mechanical ventilation (MV) is one of the main rehabilitation goals in patients with spinal cord injury (SCI), controversies are still open about the optimal rehabilitation approach.
OBJECTIVE:
This systematic review aimed at characterizing the rehabilitation interventions currently available to optimize weaning from MV in SCI patients.
METHODS:
On April 12
RESULTS:
Out of 413 records, 14 studies were included (2 randomized controlled trials, 7 observational studies, and 5 case reports). Most of the studies assessed a comprehensive rehabilitation approach, including high tidal volume ventilation, positioning, mechanical lung recruitment maneuvers, secretion management strategies, respiratory muscle training, and electrical stimulation.
CONCLUSION:
Our findings suggested that a comprehensive rehabilitation intervention might have a role in reducing MV duration in patients with SCI. Further studies are needed to better characterize the optimal rehabilitation strategies for enhancing functional recovery of patients with SCI.
1.Introduction
Spinal cord injury (SCI) is a detrimental neurological condition leading to impairment in motor, sensory, and visceral controls [1, 2, 3, 4]. It has been estimated that SCI prevalence ranges from 13.0 per million to 163.4 per million people with a high heterogeneity among countries [5, 6, 7]. In addition, approximately 75% of traumatic SCI involve young adults [5, 6, 7]. Therefore, health-care costs are extremely high, while personal and social costs are inestimable.
In this scenario, rehabilitation plays a pivotal role with growing evidence underlining the needing for a comprehensive rehabilitation approach targeting the multilevel physical and psychosocial disabilities of patients with SCI, reducing not only functional impairment and assistance costs but also improving health-related quality of life (HR-QoL) of patients with SCI [8, 9, 10, 11, 12, 13].
On the other hand, patients with cervical spinal cord lesions may suffer from a higher level of impairment in different body functions, including cough or breathing due to impaired control of abdominal and/or diaphragm muscles [14]. In particular, it has been reported that more than 90% of traumatic cervical SCIs require intubation, while more than 40% of those patients require chronic mechanical ventilation (MV) [15, 16]. Albeit MV is a life-saving intervention in patients with acute respiratory failure, several studies highlighted that prolonged MV crucially affects functional recovery and residual disability, with harmful consequences on length of stay and health-related quality of life (HR-QoL) [17, 18, 19, 20, 21]. Moreover, prolonged MV has been associated with a higher risk for infections, ventilator-associated pneumonia (VAP), and atelectasis [22]. As a result, prolonged MV might significantly affect clinical outcomes of patients with SCI, leading to a higher risk of death and lower survival [23, 24, 25].
Taken together, these findings highlighted the need for effective rehabilitation programs optimizing weaning from MV in patients with SCI not only to improve disability and promote functional recovery but also to reduce clinical complications and improve life expectancy [7, 26].
In recent years, growing evidence highlighted the benefits of respiratory rehabilitation interventions in weaning from MV. More in detail, the recent meta-analysis by Worraphan et al. [27] underlined the effectiveness of inspiratory muscle training (IMT) and early mobilization (EM) in facilitating weaning from MV. However, given the kinesiological differences in respiratory mechanics and the differences in respiratory tract innervation following SCI [28, 29], evidence in this specific population is needed to support the effectiveness of rehabilitation in the weaning process of patients with SCI.
Interestingly, the systematic review by Schreiber et al. [30] assessed the patient’s characteristics that might affect separation from MV in patients with SCI. However, the authors did not focus on rehabilitation approaches aiming at optimizing the weaning process.
Despite the effects of rehabilitative interventions in weaning from MV have been deeply studied [31, 32, 33], there is no clear evidence about specific rehabilitation strategies enhancing the weaning process in patients with SCI. Moreover, to the best of our knowledge, no previous systematic review assessed the effects of different rehabilitation approaches proposed to improve weaning from MV in SCI patients.
Therefore, the aim of this systematic review was to summarize the current evidence about the effects of rehabilitative interventions in reducing MV duration and enhancing the weaning process in patients with SCI.
2.Methods
2.1Registration
This systematic review has been performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement [34]. The international prospective register of systematic reviews (PROSPERO) was preliminary searched for similar review protocols in progress without showing similar reviews. The systematic review was submitted to PROSPERO and accepted on 13
2.2Search strategy
Five databases (PubMed/Medline, Scopus, Web of Science, Cochrane Central Register of Controlled Trials (CENTRAL), and PEDro) were systematically searched simultaneously for studies published until April 12
2.3Selection criteria
In accordance with the PICO model [35], we considered eligible clinical trials satisfying the following criteria:
• P) Participants: mechanically ventilated patients with spinal cord injury, age
• I) Intervention: we considered all rehabilitation and/or physiotherapy interventions administered as exclusive or integrated interventions.
• C) Comparator: any comparator.
• O) Outcome: the primary outcomes were weaning duration (defined as time between first assessment and the absence of MV for 48 hours), MV duration (defined as time between start of MV and successful weaning), and weaning success rate (express as percentage of patients weaned per whole sample). The secondary outcomes were: i) Pulmonary function; ii) Extubation or decannulation time; iii) Length of stay; iv) Safety.
Only studies published in peer-reviewed International Journal were included. The exclusion criteria were: i) studies involving animals; ii) participants with pregnancy, clinical instability (defined as hemodynamic alterations, respiratory events, abnormal laboratory values, reduced level of consciousness or temperature alterations), or palliation; iii) Masters or doctorate theses, conference proceedings, and literature review; iv) language other than English. No publication date restriction was applied.
After duplication removal, the records were screened by two investigators that independently reviewed titles and abstracts. The articles meeting the enrolment criteria proceeded to the full-text review screening phase. Any disagreements were discussed with a third reviewer to reach consensus.
Lastly, relevant full-text records were assessed in by two independent reviewers; in case of disagreement, it was solved by asking a third reviewer.
2.4Data extraction and synthesis
All data were extracted by two independent reviewers through Excel. Any disagreement was solved by discussion between the two reviewers or by consulting a third reviewer.
The following data were extracted: 1) Authors; 2) Journal; 3) Publication year; 4) Nationality; 5) Population characteristics; 6) Intervention characteristics; 7) Comparator characteristics; 8) Outcomes; 9) Main findings.
A descriptive approach was used to synthesize both study characteristics and data extracted. The studies were grouped for the syntheses basing on the outcomes assessed. Moreover, subgroup analysis has been performed based on the type of intervention assessed.
2.5Quality assessment and risk of bias
The quality assessment was performed through Joanna Briggs Institute Critical Appraisal Checklist for Randomized Controlled Trials, JBI Critical Appraisal Checklist for Cohort Studies, JBI Critical Appraisal Checklist for Case Series, or JBI Critical Appraisal Checklist for Case Reports basing on the study design [36]. Two independent reviewers performed independently the quality assessment. A third reviewer was involved in case of disagreement to achieve consensus.
3.Results
3.1Study characteristics
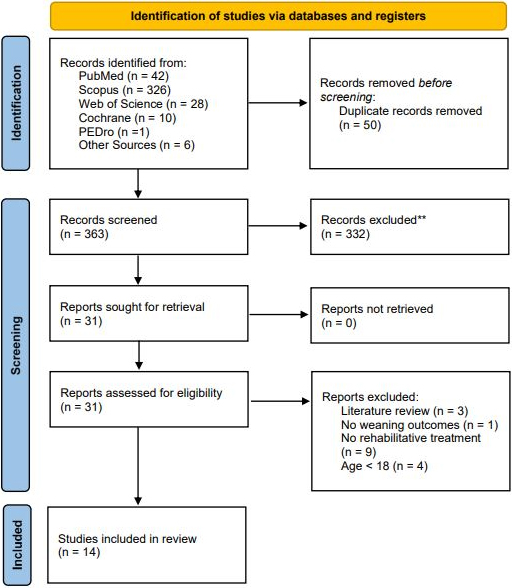
A total of 407 records were identified from 5 databases assessed, while 6 records were identified from other sources. After duplication removal, 363 studies were assessed for eligibility and screened for title and abstract. As a result, 332 records were excluded, and 31 studies were subsequently screened in full text. Lastly, 14 studies [37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53] were included in the present systematic review. Figure 1 shows further details about the article selection process through the PRISMA flow diagram. Supplementary Table 2 shows the list of the 17 full-text studies assessed for eligibility and excluded, reporting the reasons for exclusion.
Figure 1.
PRISMA 2020 flow diagram.
As a result, the following studies were included in the present systematic review: Atito-Narh et al. [37], Duarte et al. [38], Fenton et al. [39], Gundogdu et al. [40], Gutierrez et al. [41], Gutierrez et al. [42], Hatton et al. [43], Kim et al. [44], Korupolu et al. [45], McCaughey et al. [46], Peterson et al. [47], Toki et al. [50], Wong et al. [52], and Zhang et al. [53].
The studies included were published between 1999 [47] and 2021 [38, 43, 45] and were conducted in America (USA
The patients included were characterized by a mean age ranging between 27.24
All studies [37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53] included in this systematic review assessed patients with cervical SCI, while two studies [37, 45] included also patients with thoracic SCI. Interestingly, most of the studies included [37, 38, 40, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53] assessed acute SCI. In contrast, the RCT of Fenton et al. [39] assessed patients with sub-acute traumatic SCI, while the studies by Gutierrez et al. [41, 42] assessed patients with chronic SCI. Asia Impairment Scale (AIS) was used to characterize the functional impairment of SCI in eleven studies [37, 38, 39, 40, 42, 44, 45, 46, 50, 52, 53], while in three studies [41, 43, 47] the functional impairment was not reported. Table 1 summarizes in detail the sample characteristics of both intervention groups and comparator groups of each study included in the present review.
3.2Intervention characteristics
Rehabilitation interventions have been classified as changing in MV settings, mobilization/positioning techniques, respiratory muscle training, abdominal or diaphragmatic electrical stimulation, recruitment manoeuvrers (manual hyperinflation or intermitted positive-pressure breathing – IPPB), and secretion management (clearance of airway, swallowing therapy, tracheal suctioning).
• Changing in MV settings: Five studies [39, 43, 45, 47, 52] assessed the effects of high Vt mechanical ventilation. More in detail, the RCT of Fenton et al. [39] assessed the effects of high Vt at 20 ml kg
• Mobilization/positioning: Two studies [37, 42] assessed mobilization/positioning as a potential treatment for improving weaning of SCI patients. More in detail, the effects of Trendelenburg chest optimization positioning were assessed in the RCT by Gutierrez et al. [42]. Each positioning session was maintained for about 30 minutes. In contrast, Atito-Narh et al. [37] assessed the effects of different positioning strategies in their treatment protocol. More in detail, the positioning protocol
Table 1
Main characteristics of the studies included
Authors journal year Nationality Study design Participants Intervention Comparator Protocol duration Outcomes Main findings Sample size Age (years) Male/Female BMI (kg/m2) Neurological lesion level (Cervical, Thoracic, Lumbar) AIS Chronic/ Acute Complete/ Incomplete Fenton et al. 2016 Spinal Cord. USA RCT IG: 39.31 IG: 14 M/2 F CG: 11 M/6 F NR Cervical IG: C1-3: 4 C4: 6 C5: 5 C6: 1 CG: C1-3: 2 C4: 8 C5: 6 C6: 1 AIS A-B-C AIS A: NR AIS B: NR AIS C: NR Acute NR High-Vt 20 ml kg Standard-Vt 10 ml kg Weaning period – Weaning duration
– Pulmonary function
– Safety
This study reports about 33 SCI patients on MV admitted to ICU (mean age IG: 39.31 Gutierrez et al. 2010 J Rehabil Res Dev. USA RCT 55.00 12 M 23.46 Cervical C3: 2 C4: 5 C5: 5 AIS A-B A: 4 B: 8 Chronic Complete: 4 Incomplete: 8 Trendelenburg chest optimization (TCO) 20 mL/kg of IBW session duration: 30 min Supine chest optimiza-tion (SCO) 20 mL/kg of IBW session duration: 30 min Weaning period – SBT duration
– Pulmonary function
This study reports about 12 SCI patients on MV admitted to ICU (mean age 55.00 Gundogdu et al. 2017 Disabil Rehabil. Turkey Cohort study MV: 27.1 MV: 9 M/1 F TT: 19 M/6 F NR Cervical MV: C1: 3 C2: 1 C3: 1 C4: 2 C5: 2 C6: 1 C7: 0 TT: C1: 0 C2: 0 C3: 2 C4: 7 C5: 9 C6: 4 C7: 3 AIS A-B-C AIS A: 29 AIS B-C: 6 Acute Complete: 22 Incomplete: 13 MV group: Clearance of airway secretions Respiratory muscle training (with threshold IMT device, and was admin-istrated in 10 repetitions, three times a day, five days per week) Swallowing therapy SBT progressively greater in duration and frequency as tolerated TT closure time gradually increased as tolerated TT group: Clearance of airway secretions Ventilator muscle train-ing (with threshold IMT device, and was admin-istrated in 10 repetitions, three times a day, five days per week) Swallowing therapy TT closure time gradually increased as tolerated Weaning or decannulation period – Weaning duration
– Decannulation time
– Pulmonary function
This study reports about 35 SCI patients (mean age: MV: 27.1 Table 1, continued
Authors journal year Nationality Study design Participants Intervention Comparator Protocol duration Outcomes Main findings Sample size Age (years) Male/Female BMI (kg/m2) Neurological lesion level (Cervical, Thoracic, Lumbar) AIS Chronic/ Acute Complete/ Incomplete Hatton et al. 2021 J Spinal Cord Med. USA Cohort study IG: 40 (27–51 IQR) CG: 53 (35–70 IQR) IG: 17 (77%) M CG: 126 (79%) M IG: 27 (25–30) CG: 27 (24–31) Cervical IG: C1: 2 (9%) C2: 3 (14%) C3: 3 (14%) C4: 6 (27%) C5: 5 (23%) C6: 3 (14%) C7: 0 CG: C1: 11 (7%) C2: 26 (16%) C3: 24 (15%) C4: 33 (21%) C5: 42 (26%) C6: 18 (11%) C7: 5 (3%) NR Acute Complete: 77 Incomplete: 104 High-Vt Standard-Vt NR – Ventilator dependence at discharge
– Safety
This study reports about 181 SCI patients on MV admitted to ICU (mean age IG: 40 [27–51 IQR], CG: 53 [35-70 IQR]; mean BMI: IG: 27 [25–30], CG: 27 [24–31]; IG: 79% male, CG: 77% male). IG underwent to High-Vt, while CG underwent Standard-Vt. The main finding is represented by VAP incidence. In particular, 85 patients (47%) developed VAP (68% of patients in High-Vt group and in 44% of patients in standard tidal volumes group; Kim et al. 2007 Spinal Cord. Korea Cohort study 47.6 55 M/7 F NR Cervical C-: 1 C1: 3 C2: 9 C3: 23 C4: 20 C5: 2 C6: 2 C7: 0 C8: 2 AIS A-B A: 49 B: 13 Acute Complete: 49 Incomplete: 13 – Tracheal suction-
ing (MAC and
manually assisted
cough by abdom-
inal thrust) when-
ever necessary or
at least every 2 h
/ Weaning period – Weaning success rate
– Duration from
tracheostomy to
decannulation
This study reports about 62 SCI patients on MV (mean age: 47.6 Korupolu et al. 2021 Spinal Cord. USA Cohort study IG: 43 (26–59 IQR) CG: 33 (21–56 IQR) IG: 24 (71 %) M CG: 41 (82%) M NR Cervical and thoracic IG: C1-C3: 11 (32%) C4-C6: 22 (65%) CG: C1-C3: 22 (44%) C4-C6: 25 (50%) T2-T4: 2 (4%) Unknown: 1 (2%) AIS A-B-C-D IG: A: 19 (56%) B: 7 (20.5%) C: 7 (20.5%) D: 0 Unknown: 1 (3%) CG: A: 30 (60%) B: 9 (18%) C: 7 (14%) D: 2 (4%) Unknown: 2 (4%) Acute Complete: 49 Incomplete: 35 High-Vt 15–20 ml/kg PBW Standard-Vt 8.4–14.9 ml/kg PBW Weaning period – Weaning duration
– MV duration
– Weaning success rate
– Length of stay
– Safety
This study reports about 84 SCI patients on MV (mean age: IG: 43 [26–59 IQR], CG: 33 [21–56 IQR]; IG: 71 % male, CG: 82% male). IG underwent to High-Vt, while CG underwent Standard-Vt. The main finding is represented by the incidence of pneumonia. The risk of pneumonia in IG was 4.3 times higher compared to CG (95%; CI: 1.5–12). Odds of pulmonary adverse events in IG were 5.4 times higher (CI: 1.8–17) compared to CG. There were no significant improvements in weaning duration (IG: 19 [18, 22 IQR]; CG: 19 [18, 21 IQR]; McCaughey et al. 2015 PLoS One. UK Cohort study IG: 48.2 IG: 8 M/2 F CG: 8 M/1 F NR Cervical IG: C0/5: 1 C3/4: 2 C4: 3 C5: 1 C5/6: 1 C6/7: 1 C7: 1 CG: C3: 1 C4: 2 C5: 5 C6: 1 AIS A-B-C IG: A: 5 B: 2 C: 3 CG: A: 7 B: 1 C: 1 Acute Complete: 12 Incomplete: 7 Abdominal Functional Electrical Stimulation Frequency: 5 sessions/week on 4 alternate weeks Volume: 20–40 minutes/session Usual care 8 weeks – Weaning duration
– Pulmonary function
This study reports about 19 SCI patients on MV (mean age: IG: 48.2 Table 1, continued
Authors journal year Nationality Study design Participants Intervention Comparator Protocol duration Outcomes Main findings Sample size Age (years) Male/Female BMI (kg/m2) Neurological lesion level (Cervical, Thoracic, Lumbar) AIS Chronic/ Acute Complete/ Incomplete Peterson et al.1999 Spinal Cord. USA Cohort study IG: 31 37 M/5 F NR Cervical C3-C4 NR Acute Complete High-Vt Mean 25.3 ml/kg (range 20.3–32.2 ml/kg) Low-Vt Mean 15.5 ml/kg (range 11.6–19.4 ml/kg) Weaning period – Weaning duration
– Safety
This study reports about 42 SCI patients on MV (mean age: IG: 31 Wong et al.2012 Top Spinal Cord Inj Rehabil. USA Cohort study 33.4 22 M/2 F 25.82 Cervical C1: 7 C2: 1 C3: 4 C4: 12 AIS A-B-C-D A: 19 B: 3 C: 1 D: 1 Acute Complete: 19 Incomplete: 5 – High-Vt
12–15 ml/kg IBW
– Secretion manage-
ment (HFPV and
MIE) every 2 to 4
hours, for 30 to 45
minutes.
/ Weaning period – Weaning duration
This study reports about 24 SCI patients on MV (mean age: 33.4 Atito-Nahr et al. 2008 British Journal of Intensive Care UK Case series 43.8 10 M/3 F NR Cervical and Thoracic C2: 2 C3: 4 C4: 5 C5: 1 C6: 1 T4: 1 AIS A-B-C A: 9 B: 1 C: 3 Acute Complete: 9 Incomplete: 4 – Ventilatory support
(night: CMV 10–15
ml/kg; day: PC SIMV
– Tracheal cuff deflation
– Mobilisation of se-
cretions with pressure monitored hyperinflation
– Routine bagging
– Positioning (physical
turns from side to
side and back 3–4
hourly and mobilise in wheelchair)
– Swallowing and
speech therapy
– Progressive SBT
– Speaking valve and
deflate cuff if present,
– Monitor vital capac-
ity, combined with
incentive spirome-
try, supine position
initially)
/ Weaning period – Weaning duration
– Pulmonary function
This study reports about 13 SCI patients on MV (mean age: 43.8 Duarte et al.2021 Spinal Cord Ser Cases. Brazil Case series IG: 28 IG: 75% M/25% F CG: 83% M/16% F NR Cervical C3: 1 C2/4: 1 C4/5: 3 C4/6: 1 C5/6: 3 C6/7: 1 AIS A Acute Complete Transcutaneous electric diaphragmatic stimula-tion Setting: frequency of 30hertz, pulse width of 1ms, rise time of 0.7 ms,and current intensity of60 milliamps Frequency: 2 sessions/day for 7 days a week Duration (session): 20 min Standard weaning protocol Weaning period – Weaning duration
– MV duration
– Length of stay
This study reports about 10 SCI patients on MV admitted to ICU (mean age IG: 28 Table 1, continued
Authors journal year Nationality Study design Participants Intervention Comparator Protocol duration Outcomes Main findings Sample size Age (years) Male/Female BMI (kg/m2) Neurological lesion level (Cervical, Thoracic, Lumbar) AIS Chronic/ Acute Complete/ Incomplete Gutierrez et al. 2003 J Rehabil Res Dev. USA Case series Range: 44–68 7 M NR Cervical C2: 2 C4: 1 C5: 2 C5-7: 1 C7: 1 NR Chronic Incomplete Resistance and endurance protocol: – Pretraining Optimization (Position,
Suction, Aerosolize,
Hyperinflate)
– Inspiratory/Expiratory
Resistance Training
(Inspiratory/expi-
ratory trainer, Cuff
deflated and red cap
on trach tube)
– On-Vent Endurance
Training (SIMV rate
of 1–2, PS to maintain
tidal volume
ml on CPAP 5 PS 5
for 2 continuous hours per day for 1 week)
– Off-Vent Endurance
Training (Gas
injection nebulizer
wye-piece as tolerated,
Tracheal gas insuf-
flation device as tol-
erated, Red cap to
trach tube as toler-
ated, Tracheal de-
cannulation unless
contraindicated)
/ Weaning period – Weaning success rate
– Pulmonary function
This study reports about 7 SCI patients on MV (age range: 44–68; 100% male) undergoing resistance and endurance protocol. The main findings are represented by weaning success rate. Low tetraplegic patients completed their prescribed training. Of these, 4/4 (100%) were weaned from mechanical ventilation. Significant changes were reported in terms of MIP ( Toki et al. 2008 Arch Phys Med Rehabil. Japan Case series Case 1: 34 Case 2: 29 Case 1: M Case 2: M NR Cervical Case 1: C1 Case 2: C1 Case 1: A Case 2: A Acute Complete NPPV Noninvasive Positive-Pressure Ventila- tion Case 1: starting from Vt IBW of 9.5 mL/kg Case 2: starting from Vt IBW of 7.8 mL/kg / Hospitalization time – Pulmonary function
– Length of stay
This study reports about 2 SCI patients on MV undergoing NPPV. Both patients were discharged home successfully. At first, they were ventilated through tracheostomy tube, and then were decannulated to NPPV. Improvements were reported in terms of: Vc (Case 1 Table 1, continued
Authors journal year Nationality Study design Participants Intervention Comparator Protocol duration Outcomes Main findings Sample size Age (years) Male/Female BMI (kg/m2) Neurological lesion level (Cervical, Thoracic, Lumbar) AIS Chronic/ Acute Complete/ Incomplete Zhang et al. 2020 Signa Vitae China Case report 48 M NR Cervical C4 A Acute Complete – IMT
– passive training
(stretching of the in-
tercostal muscles, bed
tilting, passive move-
ment of the scapula
and the proximal end
of the upper limbs)
– active training (vari-
ous diaphragmatic fa-
cilitation techniques)
/ Weaning period – Weaning success rate
– SBT duration
– Pulmonary function
This study reports about a male SCI patient on MV (age: 48), with complete cervical spinal cord injury (level C4). The patient underwent IMT. The patient was successfully weaned from mechanical ventilation and discharged from the hospital. The MIP increased to 31.05 cmH2O (vs. 13.88 cmH2O pre-intervention. The diaphragmatic muscle showed a thickness of 0.22 cm (at the admission was 0.17 cm) and a diaphragmatic activity of 2.22 cm (at the admission was 4 cm). Abbreviations: AIS
included physical turns from side to side and back 3–4 hourly and mobilise in wheelchair.
• Respiratory muscles training: Three [40, 41, 53] studies assessed respiratory muscle training proposing different therapeutic strategies. In particular, the case series of Gutierrez et al. [41] assessed the effect of a resistance and endurance training protocol including 4 phases (pretraining optimization, inspiratory/expiratory resistance training, on-vent endurance training, and off-vent endurance training). On the other hand, Zhang et al. [53] assessed the effect of an inspiratory muscle training protocol. In particular, it was composed of passive activities (stretching of the intercostal muscles, bed tilting, passive movement of the scapula and the proximal end of the upper limbs), and strength and endurance training on the diaphragm. Lastly, Gundogdu et al. [40], assessed the effect of an inspiratory muscle training protocol with a threshold IMT device, administered in 10 repetitions, three times a day, five days per week until decannulation.
• Abdominal or diaphragmatic electrical stimulation: Electrical stimulation was assessed in two studies [38, 46]. Duarte et al. [38] assessed the effects of transcutaneous electric diaphragmatic stimulation (TEDS) administrated for 20 minutes per session, twice a day, for 7 days a week. TEDS was administrated with a frequency of 30 hertz, pulse width of 1 ms, rise time of 0.7 ms, and current intensity of 60 milliamps. McCaughey et al. [46] assessed the effects of Abdominal Functional Electrical Stimulation (AFES), 20–40 minutes per session, five sessions per week on 4 alternate weeks, for 8 weeks.
• Lung hyperinflation/recruitment maneuvers: Gutierrez et al. [41, 42] and Atito-Narh et al. [37] assessed lung hyperinflation maneuvers with ventilators or manual resuscitation bag.
• Secretion management (including tracheal suctioning and swallowing rehabilitation): Four studies [37, 40, 44, 52] assessed the effects of secretion management, clearance of airway, swallowing therapy, or tracheal suctioning. In particular, Kim et al. [44] assessed the effects of mechanical insufflation-exsufflation (MI-E) or manually assisted cough (MAC) by abdominal thrust followed by suctioning or self-oral expectoration. Similarly, Wong et al. [52] assessed the effects of high-frequency percussive ventilation (HFPV) and mechanical insufflation-exsufflation (MI-E) for managing secretion, every 2–4 hours, for 30 to 45 minutes.
Interestingly, Atito-Narh et al. [37] included swallowing rehabilitation in their protocol, consisting of bedside assessment of swallow performance with deflated cuff before administering oral intake. Moreover, in the study by Gundogdu et al. [40] patients received daily care for oral hygiene, thermal (cold) and tactile stimulation, head and trunk positioning, dietary modification, swallowing maneuvers and oral motor exercises, including the lip, tongue and jaw movements according to the different patient characteristics for 60 min a day, 5 days a week for 3 to 6 weeks.
All rehabilitation programs assessed in the present systematic review have been summarized in detail in Table 1.
3.3Control characteristics
The intervention groups were compared with standard/low volume mechanical ventilation [39, 43, 45, 47], usual care/standard weaning protocol [38, 46], or positioning [42]. In particular, in the RCT performed by Gutierrez et al. [42], the intervention group, which performed Trendelenburg chest optimization (TCO), was compared with Supine Chest Optimization (SCO), setting the Vt on 20 mL/kg of ideal body weight for 30 min per session. All control protocols assessed in the present systematic review have been summarized in Table 1.
3.4Primary Outcomes – Weaning duration, MV duration, and weaning success rate
Weaning duration has been assessed in eight trials [37, 38, 39, 40, 45, 46, 47, 52], two studies [38, 45] assessed MV duration, and four studies [41, 44, 45, 53] assessed weaning success rate. More in detail, the RCT performed by Fenton et al. [39] showed no significant differences in mean days to wean between high-Vt group and standard-Vt group (IG: 14.5 days, CG: 14 days;
In the case series by Atito-Narh et al. [37] assessing the effects of a comprehensive rehabilitation approach (ventilatory support, tracheal cuff deflation, mobilization of secretions with pressure monitored hyperinflation, routine bagging, positioning, swallowing and speech), the mean weaning duration was 56.1
Wong et al. [52] assessed the effects of high-Vt, MIE and HFPV, 13 (neurological levels C3-C4) were successfully weaned from MV, nine with level of injury at C1, C2, and C3 were not weaned, one patient with C4 AIS B needed night-time ventilation. Gutierrez et al. [41] reported that all tetraplegic patients with low neurological levels and completing the prescribed training underwent successful weaning from MV. Kim et al. [44] showed a weaning success rate of 24.2% in patients with cervical spinal cord injury. Lastly, Zhang et al. [53] reported successful weaning from MV in the patient that underwent to IMT program.
3.5Secondary outcomes – pulmonary function
Pulmonary function was assessed in eight studies [37, 39, 40, 41, 42, 46, 50, 53]. In particular, in the RCT by Fenton et al. [39], no significant differences between groups were reported in terms of FVC values. However, significant within-group differences were reported in both groups (
Concurrently, the RCT by Gutierrez et al. [42] underlined that Spontaneous Breathing Trial (SBT) duration was significantly longer in TCO group compared to SCO group (IG: 87.67
In the cohort study by Gundogdu et al. [40], the means of the maximal inspiratory pressure (MIP), maximal expiratory pressure (MEP) and peak cough flow (PCF) values of MV-dependent patients after the weaning protocol significantly improved (MIP:
3.6Secondary outcomes – extubation or decannulation
In the cohort study by Gundogdu et al. [40], the mean duration of decannulation was 31.7
Table 2
Joanna Briggs Institute Critical Appraisal Checklist for the studies included
| Joanna Briggs Institute Critical Appraisal Checklist for RCTs | ||||||||||||||
| Authors and year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Total score |
| Fenton et al. 2016 | Y | Y | Y | N | N | Y | Y | Y | Y | Y | Y | Y | Y | 11 |
| Gutierrez et al. 2010 | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | 12 |
| Joanna Briggs Institute Critical Appraisal Checklist for RCTs: Q1 | ||||||||||||||
| Joanna Briggs Institute Critical Appraisal Checklist for Cohort Studies | ||||||||||||
| Authors and year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Total score |
| Gundogdu et al. 2016 | Y | N/A | Y | N | N | Y | Y | Y | Y | N | Y | 7 |
| Hatton et al. 2021 | Y | Y | Y | Y | Y | Y | Y | N/A | N/A | N | Y | 8 |
| Kim et al. 2007 | Y | N/A | Y | Y | N | Y | Y | Y | Y | N | Y | 8 |
| Korupolu et al. 2020 | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | 10 |
| McCaughey et al. 2015 | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | 10 |
| Peterson et al. 1999 | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | 10 |
| Wong et al. 2012 | Y | N/A | Y | Y | N | Y | Y | Y | Y | N | Y | 8 |
| Joanna Briggs Institute Critical Appraisal Checklist for Cohort Studies: Q1 | ||||||||||||
| Joanna Briggs Institute Critical Appraisal Checklist for Case Series | |||||||||||
| Authors and year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Total score |
| Atito-Nahr et al. 2008 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 10 |
| Duarte et al. 2021 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 10 |
| Gutierrez et al. 2003 | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | 9 |
| Toki et al. 2008 | Y | Y | Y | N | Y | Y | Y | Y | N | Y | 8 |
| Joanna Briggs Institute Critical Appraisal Checklist for Case Series: Q1 | |||||||||||
| Joanna Briggs Institute Critical Appraisal Checklist for Case Reports | |||||||||
| Authors and year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Total score |
| Zhang et al. 2020 | N | N | Y | Y | Y | Y | Y | Y | 6 |
| Joanna Briggs Institute Critical Appraisal Checklist for Case Reports: Q1 | |||||||||
3.7Secondary outcomes – length of stay
The study by Duarte et al. [38] reported differences in length of stay in ICU between TEDS group and standard weaning protocol group (IG: 31
3.8Secondary outcomes – ventilator dependence at discharge
Hatton et al. [43] showed that ventilator dependence at 30 hospital days or hospital discharge was significantly increased in high-Vt group (82% of patients) compared with standard-Vt group (38% of patients) (
3.9Secondary outcomes – safety
The RCT by Fenton et al. [39] reported no significant differences in incidence of adverse pulmonary events (
3.10Quality assessment
The quality assessment was performed following the Joanna Briggs Institute Critical Appraisal Checklist for Randomized Controlled Trials, JBI Critical Appraisal Checklist for Cohort Studies, JBI Critical Appraisal Checklist for Case Series, or JBI Critical Appraisal Checklist for Case Reports basing on the study design [36]. The studies included [39, 40, 42, 43, 44, 45, 46, 47, 52, 53] presented at least one serious risk of bias, which translated into an overall serious risk of bias for that study. The main quality concerns included the lack of data on baseline characteristics of study participants, nonrandom sampling approaches (convenience samples), missing data, and lack of a reliable tool to estimate and report outcomes. Further details about the quality assessment of each study included in this review are shown in Table 2.
4.Discussion
To date, rehabilitation could be considered as a milestone in the complex management of SCI patients [54, 55, 56], with several studies proposing different approaches to enhance the weaning process in mechanically ventilated SCI patients [37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53]. However, the optimal rehabilitation approach is still a challenge for physicians and researchers, considering that no clear indications are currently available for mechanically ventilated SCI patients.
Therefore, by this systematic review we aimed at providing a broad overview about the current rehabilitation strategies aiming at optimizing the weaning process of these patients, characterizing the specific rehabilitation approaches in order to reduce the weaning duration, improve functional outcomes and minimize MV related complications.
Interestingly, six main rehabilitative strategies have been identified in the scientific literature: i) high-Vt ventilation, ii) positioning, iii) mechanical lung recruitment maneuvers, iv) secretion management strategies, v) respiratory muscle training, and vi) electrical stimulation.
To date, high-VT ventilation in patients with SCI is commonly used in the clinical practice [57] and supported by specific guidelines [58]. In this context, SCI patients were frequently not affected by chronic pulmonary conditions, and “healthy lungs” should not be damaged by relatively high-volume ventilation. Moreover, a tidal volume of up to 1000 ml may represent approximately 30% of the normal inspiratory capacity of a healthy adult [29]. In addition, higher VTs stretch the airways smooth muscles, and promote the production of pulmonary surfactant, the alveolar surface tension with positive implications in the prevention of peripheral collapse of small airways [52]. Our results identified five studies [39, 43, 45, 47, 52] assessing the role of high-Vt compared to low-Vt, highlighting conflicting results. More in detail, two retrospective analyses [47, 52] supported higher VTs (more than 20 ml/kg IBW), suggesting positive implications for weaning process duration and complications rate. In addition, Wong et al. [52] suggested that higher VTs might optimize the respiratory status, vocalization, and participation in rehabilitation programs of patients with SCI, reducing MV duration. On the other hand, it should be noted that all patients underwent a comprehensive pulmonary rehabilitation program including HFPV, MIE and high-VT ventilation. Therefore, it is impossible to draw conclusions about each single rehabilitation intervention. On the contrary, the RCT by Fenton et al. [39] confirmed the safety of high-Vt ventilation (20 ml/kg vs 10 ml/kg IBW), without reporting difference in the weaning duration. Lastly, the more recent studies by Hatton et al. [43] and Korupolu et al. [45] raised doubt about the safety of this rehabilitation approach, since no advantages in weaning duration were found and a higher incidence of pneumonia and pulmonary adverse events were reported. Surprisingly, both studies did not report any interventions for the management of mucus encumbrance or other interventions aimed to prevent secretion stagnation and atelectasis [43, 45].
Altogether, these results underlined some concerns about the effectiveness of high-Vt ventilation. Despite these considerations, high-Vt ventilation should not be proposed alone, but included in a comprehensive rehabilitation intervention targeting the multilevel pulmonary impairment of patients with SCI.
In contrast, secretion management strategies were described in four studies [37, 40, 44, 52] reporting promising results in terms of weaning duration [37, 40, 52] or weaning success rate [44]. Despite the positive data, no study assessed the role of secretion management strategies without other interventions.
Although positioning techniques play a key role in the management of patients with SCI due to their widely documented role in secondary complications prevention [59], only two studies [37, 42] assessed mobilization/positioning as a potential treatment for improving weaning of SCI patients. Intriguingly, the RCT by Gutierrez et al. [42] reported significant differences in patients undergoing Trendelenburg positioning compared to supine chest optimization in terms of SBT duration. However, no significant results were reported in terms of weaning duration and weaning success rate, probably due to the small sample size. On the other hand, the case series from Atito-Nahr et al. [37] reported positive results of a specific positioning protocol included in a comprehensive rehabilitation approach. Further studies might clarify the role of different positioning in the complex rehabilitation program also improving pressure ulcer risk, joint contractures, swallowing optimization and several other disabling conditions that might benefit from positioning or repositioning techniques [60, 61, 62, 63, 64].
Interestingly, respiratory muscle training has been assessed by three studies [40, 41, 53]. In this scenario, a growing interest is rising in the current literature about the role of IMT in prolonged MV. In particular, the recent systematic review and meta-analysis by Vorona et al. [65] highlighted that IMT might be considered a key component of a comprehensive rehabilitation intervention aiming at optimizing weaning duration in difficult-to-wean patients [65]. However, neurological impairment characterizing SCI patients might drastically affect respiratory muscle recruitment and respiratory mechanics [28, 29, 66], with detrimental consequences on respiratory muscle’s response to training. Our results underlined that respiratory muscle training might improve weaning duration [40] or weaning success rate [41, 53]. Despite these considerations, a precise patient’s stratification is mandatory in a specific IMT that should be tailored to SCI level and SCI completeness, along with a precise inspiratory muscle weakness assessment.
To overcome the neurological deficit affecting respiratory muscle recruitment, two studies [38, 46] assessed the effects of electrical stimulations on the diaphragmatic muscle and abdominal muscles. On the other hand, it should be noted that several concerns are still open in the current literature about electrical stimulation in pulmonary rehabilitation and no strong evidence currently support this technique [31, 67]. However, electrical stimulations might be considered a suitable rehabilitation strategy in patients with low compliance levels or with high grade of neurological impairment to prevent muscle atrophy.
Taken together, our findings underlined that most of the studies included in the present review assessed different combinations of pulmonary rehabilitation strategies, integrated in a comprehensive rehabilitation intervention. In this scenario, it has been proposed that a multitarget approach might have a role in implementing the synergisms between different therapeutic interventions, with positive effects on functional outcomes of patients with a pulmonary function impairment [27, 68].
On the other hand, recent research is now focusing on a precise stratification based on patients’ characteristics. In particular, the review by Schreiber et al. [30] recently assessed the factors potentially related to successful weaning and weaning duration in patients with SCI. Interestingly, the authors underlined that It might be partly related to specific consequences on muscle recruitment and ventilation mechanics, which might be significantly influenced by patient’s SCI level and SCI completeness [30]. Moreover, presence of multiple spinal cord lesions and pulmonary comorbidities might be crucial factors that might affect weaning process [30]. In this scenario, a patient-tailored approach should consider these issues in order to better personalize the rehabilitative intervention of patients with SCI. Thus, we deeply characterized the participants of this study to provide a qualitative synthesis about the effectiveness of a precise intervention specific to the patient’s characteristics. To the best of our knowledge, this is the first systematic review that assessed the effects of a pulmonary rehabilitation approach in weaning from MV of patients with SCI, focusing on specific rehabilitation strategies to promote pulmonary function recovery and minimize complications.
Besides these considerations, we are aware that this review is not free from limitations. Firstly, the low number of the study included, and the heterogeneous study design did not allow to draw strong conclusions. However, it should be noted that these results reflect the currently available literature. More in detail, our findings underlined a large gap of knowledge in this field with current evidence still based on low-quality studies with controversial results. In addition, several questions are still open about the optimal rehabilitation approach since most of the rehabilitation strategies have been studied in a comprehensive approach. Moreover, the type of SCI lesion might severely influence the rehabilitation response and functional outcomes. On the other hand, the studies identified by the present review underlined a large heterogeneity of the study participants in terms of AIS classification which might severely limits the implications of the study’s results. In this context, a deeper patient stratification should be considered to address the needing for rehabilitative interventions tailored to patients’ characteristics.
5.Conclusions
Rehabilitation strategies with specific indications for patients with SCI are mandatory to prevent severe complications but also to enhance functional recovery and reduce assistance costs in patients with SCI. The results of the present systematic review supported the effects of a comprehensive rehabilitation approach that might include high-Vt ventilation, positioning, mechanical lung recruitment maneuvers, secretion management, respiratory muscle training and electrical stimulation. Despite the promising results, good-quality studies are mandatory to better characterize the effects of specific rehabilitation interventions reducing MV duration. Moreover, a better patients’ stratification is needed to optimize the weaning process and better address the clinical need for an evidence-based patient-tailored rehabilitation plan for these subjects.
Ethical approval
Not applicable.
Funding
The authors report no funding.
Informed Consent
Not applicable.
Author Contributions
Conceptualization, L.L., A.d.S., and M.I.; methodology, L.L., A.d.S., and M.I.; investigation, L.L., F.D.A., A.F., and A.T.; writing – original draft preparation, L.L. and F.D.A.; writing – review and editing, A.d.S and M.I.; visualization, A.F., A.T., C.C., and A.A.; supervision, A.d.S. and M.I. All authors have read and agreed to the published version of the manuscript.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/BMR-220201.
Acknowledgments
The authors want to thank Enrico Cavallo for his support to this work.
Conflict of interest
The authors declare that they have no conflict of interest.
References
[1] | Lu X, Battistuzzo CR, Zoghi M, Galea MP. Effects of training on upper limb function after cervical spinal cord injury: A systematic review. Clinical Rehabilitation. (2015) ; 29: (1): 3-13. |
[2] | Stampas A, Tansey KE. Spinal cord injury medicine and rehabilitation. Seminars in Neurology. (2014) ; 34: (5): 524-33. |
[3] | Invernizzi M, de Sire A, Renò F, Cisari C, Runza L, Baricich A, et al. Spinal cord injury as a model of bone-muscle interactions: Therapeutic implications from in vitro and in vivo studies. Frontiers in Endocrinology. (2020) ; 11: : 204. |
[4] | Invernizzi M, de Sire A, Fusco N. Rethinking the clinical management of volumetric muscle loss in patients with spinal cord injury: Synergy among nutritional supplementation, pharmacotherapy, and rehabilitation. Current Opinion in Pharmacology. (2021) ; 57: : 132-9. |
[5] | Pickett GE, Campos-Benitez M, Keller JL, Duggal N. Epidemiology of traumatic spinal cord injury in Canada. Spine. (2006) ; 31: (7): 799-805. |
[6] | Winslow C, Rozovsky J. Effect of spinal cord injury on the respiratory system. American Journal of Physical Medicine & Rehabilitation. (2003) ; 82: (10): 803-14. |
[7] | DeVivo MJ, Krause JS, Lammertse DP. Recent trends in mortality and causes of death among persons with spinal cord injury. Archives of Physical Medicine and Rehabilitation. (1999) ; 80: (11): 1411-9. |
[8] | Morone G, De Sire A, Martino Cinnera A, Paci M, Perrero L, Invernizzi M, et al. Upper limb robotic rehabilitation for patients with cervical spinal cord injury: A comprehensive review. Brain Sciences. (2021) ; 11: (12): 1630. |
[9] | Invernizzi M, Carda S, Rizzi M, Grana E, Squarzanti DF, Cisari C, et al. Evaluation of serum myostatin and sclerostin levels in chronic spinal cord injured patients. Spinal Cord. (2015) ; 53: (8): 615-20. |
[10] | Invernizzi M, De Sire A, Carda S, Venetis K, Renò F, Cisari C, et al. Bone muscle crosstalk in spinal cord injuries: Pathophysiology and implications for patients’ quality of life. Current Osteoporosis Reports. (2020) ; 18: (4): 422-31. |
[11] | Solomon RM, Dhakal R, Halpin SJ, Hariharan R, O’Connor RJ, Allsop M, et al. Telerehabilitation for individuals with spinal cord injury in low- and middle-income countries: A systematic review of the literature. Spinal Cord. (2022) ; 60: (5): 395-403. |
[12] | Schultz KR, Mona LR, Cameron RP. Mental Health and Spinal Cord Injury: Clinical Considerations for Rehabilitation Providers. Current Physical Medicine and Rehabilitation Reports. (2022) . |
[13] | de Melo-Neto JS, de Campos Gomes F, de Morais DF, Tognola WA. Spinal cord injury in elderly patients admitted to a tertiary hospital. J Back Musculoskelet Rehabil. (2017) ; 30: (4): 929-36. |
[14] | Zimmer MB, Nantwi K, Goshgarian HG. Effect of spinal cord injury on the respiratory system: Basic research and current clinical treatment options. The Journal of Spinal Cord Medicine. (2007) ; 30: (4): 319-30. |
[15] | Claxton AR, Wong DT, Chung F, Fehlings MG. Predictors of hospital mortality and mechanical ventilation in patients with cervical spinal cord injury. Canadian Journal of Anaesthesia = Journal Canadien D’Anesthesie. (1998) ; 45: (2): 144-9. |
[16] | Como JJ, Sutton ER, McCunn M, Dutton RP, Johnson SB, Aarabi B, et al. Characterizing the need for mechanical ventilation following cervical spinal cord injury with neurologic deficit. The Journal of Trauma. (2005) ; 59: (4): 912-6; discussion 6. |
[17] | Beduneau G, Pham T, Schortgen F, Piquilloud L, Zogheib E, Jonas M, et al. Epidemiology of weaning outcome according to a new definition.The WIND study. Am J Respir Crit Care Med. (2017) ; 195: (6): 772-83. |
[18] | Damuth E, Mitchell JA, Bartock JL, Roberts BW, Trzeciak S. Long-term survival of critically ill patients treated with prolonged mechanical ventilation: A systematic review and meta-analysis. Lancet Respir Med. (2015) ; 3: (7): 544-53. |
[19] | Unroe M, Kahn JM, Carson SS, Govert JA, Martinu T, Sathy SJ, et al. One-year trajectories of care and resource utilization for recipients of prolonged mechanical ventilation: A cohort study. Ann Intern Med. (2010) ; 153: (3): 167-75. |
[20] | Herridge MS, Chu LM, Matte A, Tomlinson G, Chan L, Thomas C, et al. The RECOVER program: Disability risk groups and 1-year outcome after 7 or more days of mechanical ventilation. Am J Respir Crit Care Med. (2016) ; 194: (7): 831-44. |
[21] | Kahn JM, Le T, Angus DC, Cox CE, Hough CL, White DB, et al. The epidemiology of chronic critical illness in the United States*. Crit Care Med. (2015) ; 43: (2): 282-7. |
[22] | Windisch W, Dellweg D, Geiseler J, Westhoff M, Pfeifer M, Suchi S, et al. Prolonged weaning from mechanical ventilation. Dtsch Arztebl Int. (2020) ; 117: (12): 197-204. |
[23] | Goligher EC, Dres M, Fan E, Rubenfeld GD, Scales DC, Herridge MS, et al. Mechanical ventilation-induced diaphragm atrophy strongly impacts clinical outcomes. Am J Respir Crit Care Med. (2018) ; 197: (2): 204-13. |
[24] | DeVivo MJ, Ivie CS, 3rd. Life expectancy of ventilator-dependent persons with spinal cord injuries. Chest. (1995) ; 108: (1): 226-32. |
[25] | Shavelle RM, DeVivo MJ, Strauss DJ, Paculdo DR, Lammertse DP, Day SM. Long-term survival of persons ventilator dependent after spinal cord injury. The Journal of Spinal Cord Medicine. (2006) ; 29: (5): 511-9. |
[26] | Soyupek F, Savas S, Oztürk O, Ilgün E, Bircan A, Akkaya A. Effects of body weight supported treadmill training on cardiac and pulmonary functions in the patients with incomplete spinal cord injury. J Back Musculoskelet Rehabil. (2009) ; 22: (4): 213-8. |
[27] | Worraphan S, Thammata A, Chittawatanarat K, Saokaew S, Kengkla K, Prasannarong M. Effects of inspiratory muscle training and early mobilization on weaning of mechanical ventilation: A systematic review and network meta-analysis. Arch Phys Med Rehabil. (2020) ; 101: (11): 2002-14. |
[28] | Baydur A, Adkins RH, Milic-Emili J. Lung mechanics in individuals with spinal cord injury: Effects of injury level and posture. Journal of Applied Physiology. (2001) ; 90: (2): 405-11. |
[29] | Brown R, DiMarco AF, Hoit JD, Garshick E. Respiratory dysfunction and management in spinal cord injury. Respir Care. (2006) ; 51: (8): 853-68; discussion 69-70. |
[30] | Schreiber AF, Garlasco J, Vieira F, Lau YH, Stavi D, Lightfoot D, et al. Separation from mechanical ventilation and survival after spinal cord injury: A systematic review and meta-analysis. Ann Intensive Care. (2021) ; 11: (1): 149. |
[31] | Lippi L, de Sire A, D’Abrosca F, Polla B, Marotta N, Castello LM, et al. Efficacy of Physiotherapy Interventions on Weaning in Mechanically Ventilated Critically Ill Patients: A Systematic Review and Meta-Analysis. Front Med (Lausanne). (2022) ; 9: : 889218. |
[32] | Bernardes Neto SCG, Torres-Castro R, Lima Í, Resqueti VR, Fregonezi GAF. Weaning from mechanical ventilation in people with neuromuscular disease: A systematic review. BMJ Open. (2021) ; 11: (9): e047449. |
[33] | Yuan X, Lu X, Chao Y, Beck J, Sinderby C, Xie J, et al. Neurally adjusted ventilatory assist as a weaning mode for adults with invasive mechanical ventilation: A systematic review and meta-analysis. Critical Care. (2021) ; 25: (1). |
[34] | Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Bmj. (2021) ; 372: : n71. |
[35] | Huang X, Lin J, Demner-Fushman D. Evaluation of PICO as a knowledge representation for clinical questions. AMIA Annu Symp Proc. (2006) ; 359-63. |
[36] | Institute TJB. JBI Critical Appraisal Tools 2017. Available from: https://jbi.global/critical-appraisal-tools. |
[37] | Atito-Narh E, Pieri-Davies S, Watt JWH. Slow ventilator weaning after cervical spinal cord injury. British Journal of Intensive Care. (2008) ; 18: (3): 95-102. |
[38] | Duarte GL, Bethiol AL, Ratti L, Franco G, Moreno R, Tonella RM, et al. Transcutaneous electrical diaphragmatic stimulation reduces the duration of invasive mechanical ventilation in patients with cervical spinal cord injury: Retrospective case series. Spinal Cord Series and Cases. (2021) ; 7: (1): 26. |
[39] | Fenton JJ, Warner ML, Lammertse D, Charlifue S, Martinez L, Dannels-McClure A, et al. A comparison of high vs standard tidal volumes in ventilator weaning for individuals with sub-acute spinal cord injuries: A site-specific randomized clinical trial. Spinal Cord. (2016) ; 54: (3): 234-8. |
[40] | Gundogdu I, Ozturk EA, Umay E, Karaahmet OZ, Unlu E, Cakci A. Implementation of a respiratory rehabilitation protocol: Weaning from the ventilator and tracheostomy in difficult-to-wean patients with spinal cord injury. Disability and Rehabilitation. (2017) ; 39: (12): 1162-70. |
[41] | Gutierrez CJ, Harrow J, Haines F. Using an evidence-based protocol to guide rehabilitation and weaning of ventilator-dependent cervical spinal cord injury patients. Journal of Rehabilitation Research and Development. (2003) ; 40: (5 Suppl 2): 99-110. |
[42] | Gutierrez CJ, Stevens C, Merritt J, Pope C, Tanasescu M, Curtiss G. Trendelenburg chest optimization prolongs spontaneous breathing trials in ventilator-dependent patients with low cervical spinal cord injury. Journal of Rehabilitation Research and Development. (2010) ; 47: (3): 261-72. |
[43] | Hatton GE, Mollett PJ, Du RE, Wei S, Korupolu R, Wade CE, et al. High tidal volume ventilation is associated with ventilator-associated pneumonia in acute cervical spinal cord injury. The Journal of Spinal Cord Medicine. (2021) ; 44: (5): 775-81. |
[44] | Kim DH, Kang SW, Choi WA, Oh HJ. Successful tracheostomy decannulation after complete or sensory incomplete cervical spinal cord injury. Spinal Cord. (2017) ; 55: (6): 601-5. |
[45] | Korupolu R, Stampas A, Uhlig-Reche H, Ciammaichella E, Mollett PJ, Achilike EC, et al. Comparing outcomes of mechanical ventilation with high vs. moderate tidal volumes in tracheostomized patients with spinal cord injury in acute inpatient rehabilitation setting: A retrospective cohort study. Spinal Cord. (2021) ; 59: (6): 618-25. |
[46] | McCaughey EJ, Berry HR, McLean AN, Allan DB, Gollee H. Abdominal functional electrical stimulation to assist ventilator weaning in acute tetraplegia: A cohort study. PloS One. (2015) ; 10: (6): e0128589. |
[47] | Peterson WP, Barbalata L, Brooks CA, Gerhart KA, Mellick DC, Whiteneck GG. The effect of tidal volumes on the time to wean persons with high tetraplegia from ventilators. Spinal Cord. (1999) ; 37: (4): 284-8. |
[48] | Romero-Ganuza J, García-Forcada A, Vargas E, Gambarrutta C. An intermediate respiratory care unit for spinal cord-injured patients. A retrospective study. Spinal Cord. (2015) ; 53: (7): 552-6. |
[49] | Strakowski JA, Pease WS, Johnson EW. Phrenic nerve stimulation in the evaluation of ventilator-dependent individuals with C4- and C5-level spinal cord injury. American Journal of Physical Medicine & Rehabilitation. (2007) ; 86: (2): 153-7. |
[50] | Toki A, Tamura R, Sumida M. Long-term ventilation for high-level tetraplegia: A report of 2 cases of noninvasive positive-pressure ventilation. Archives of Physical Medicine and Rehabilitation. (2008) ; 89: (4): 779-83. |
[51] | Wallbom AS, Naran B, Thomas E. Acute ventilator management and weaning in individuals with high tetraplegia. Topics in Spinal Cord Injury Rehabilitation. (2005) ; 10: (3): 1-7. |
[52] | Wong SL, Shem K, Crew J. Specialized respiratory management for acute cervical spinal cord injury: A retrospective analysis. Topics in Spinal Cord Injury Rehabilitation. (2012) ; 18: (4): 283-90. |
[53] | Zhang B, Jiang H, Zhang C, Li Y, Zhao Z. Pulmonary rehabilitation throughout the weaning from mechanical ventilation for complete cervical spinal cord injury: A case report. Signa Vitae. (2020) ; 16: (2): 210-4. |
[54] | Dost G, Dulgeroglu D, Yildirim A, Ozgirgin N. The effects of upper extremity progressive resistance and endurance exercises in patients with spinal cord injury. J Back Musculoskelet Rehabil. (2014) ; 27: (4): 419-26. |
[55] | Bhide RP, Solomons C, Devsahayam S, Tharion G. Exercise and gait training in persons with paraplegia and its effect on muscle properties. J Back Musculoskelet Rehabil. (2015) ; 28: (4): 739-47. |
[56] | Yildirim A, Sürücü GD, Karamercan A, Gedik DE, Atci N, Dülgeroglu D, et al. Short-term effects of upper extremity circuit resistance training on muscle strength and functional independence in patients with paraplegia. J Back Musculoskelet Rehabil. (2016) ; 29: (4): 817-23. |
[57] | Korupolu R, Stampas A, Jimenez I, Cruz D, Giusto M, Verduzco-Gutierrez M, et al. Mechanical ventilation and weaning practices for adults with spinal cord injury – An international survey. The Journal of the International Society of Physical and Rehabilitation Medicine. (2021) ; 4: (3): 131-40. |
[58] | Respiratory management following spinal cord injury: a clinical practice guideline for health-care professionals. J Spinal Cord Med. (2005) ; 28: (3): 259-93. |
[59] | Early acute management in adults with spinal cord injury: a clinical practice guideline for health-care professionals. J Spinal Cord Med. (2008) ; 31: (4): 403-79. |
[60] | Kruger EA, Pires M, Ngann Y, Sterling M, Rubayi S. Comprehensive management of pressure ulcers in spinal cord injury: Current concepts and future trends. J Spinal Cord Med. (2013) ; 36: (6): 572-85. |
[61] | Harvey L, Herbert R. Muscle stretching for treatment and prevention of contracture in people with spinal cord injury. Spinal Cord. (2002) ; 40: (1): 1-9. |
[62] | Chaw E, Shem K, Castillo K, Wong S, Chang J. Dysphagia and associated respiratory considerations in cervical spinal cord injury. Topics in Spinal Cord Injury Rehabilitation. (2012) ; 18: (4): 291-9. |
[63] | McRae J, Smith C, Beeke S, Emmanuel A. Oropharyngeal dysphagia management in cervical spinal cord injury patients: An exploratory survey of variations to care across specialised and non-specialised units. Spinal Cord Series and Cases. (2019) ; 5: (1). |
[64] | Lippi L, De Sire A, Desilvestri M, Baricich A, Barbanera A, Cattalani A, et al. Can scoliosis lead to spinal cord ischaemia? Early diagnosis and rehabilitation: A paradigmatic case report and literature review. Journal of Back and Musculoskeletal Rehabilitation. (2021) ; 34: (1): 43-7. |
[65] | Vorona S, Sabatini U, Al-Maqbali S, Bertoni M, Dres M, Bissett B, et al. Inspiratory Muscle Rehabilitation in Critically Ill Adults. A Systematic Review and Meta-Analysis. Ann Am Thorac Soc. (2018) ; 15: (6): 735-44. |
[66] | Lemos JR, da Cunha FA, Lopes AJ, Guimarães FS, do Amaral Vasconcellos FV, Dos Santos Vigário P. Respiratory muscle training in non-athletes and athletes with spinal cord injury: A systematic review of the effects on pulmonary function, respiratory muscle strength and endurance, and cardiorespiratory fitness based on the FITT principle of exercise prescription. J Back Musculoskelet Rehabil. (2020) ; 33: (4): 655-67. |
[67] | Özkul Ç, Kılınç M, Yıldırım SA, Topçuoğlu EY, Akyüz M. Effects of visual illusion and transcutaneous electrical nerve stimulation on neuropathic pain in patients with spinal cord injury: A randomised controlled cross-over trial. J Back Musculoskelet Rehabil. (2015) ; 28: (4): 709-19. |
[68] | Reilly C. Transdisciplinary approach: An atypical strategy for improving outcomes in rehabilitative and long-term acute care settings. Rehabil Nurs. (2001) ; 26: (6): 216-20, 44. |


