
Evidence-based and adverse-effects analyses of cupping therapy in musculoskeletal and sports rehabilitation: A systematic and evidence-based review
Abstract
BACKGROUND:
Cupping therapy has been used to treat musculoskeletal impairments for about 4000 years. Recently, world athletes have provoked an interest in it, however, the evidence to support its use in managing musculoskeletal and sports conditions remains unknown.
OBJECTIVE:
To evaluate the evidence level of the effect of cupping therapy in managing common musculoskeletal and sports conditions.
METHODS:
2214 studies were identified through a computerized search, of which 22 met the inclusion criteria. The search involved randomized and case series studies published between 1990 and 2019. The search involved five databases (Scopus, MEDLINE (PubMed), Web of Science, Academic Search Complete PLUS (EBSCO), and CrossRef) and contained studies written in the English language. Three analyses were included: the quality assessment using the PEDro scale, physical characteristic analysis, and evidence-based analysis.
RESULTS:
The results showed that most studies used dry cupping, except five which used wet cupping. Most studies compared cupping therapy to non-intervention, the remaining studies compared cupping to standard medical care, heat, routine physiotherapy, electrical stimulation, active range of motion and stretching, passive stretching, or acetaminophen. Treatment duration ranged from 1 day to 12 weeks. The evidence of cupping on increasing soft tissue flexibility is moderate, decreasing low back pain or cervical pain is low to moderate, and treating other musculoskeletal conditions is very low to low. The incidence of adverse events is very low.
CONCLUSION:
This study provides the first attempt to analyze the evidence level of cupping therapy in musculoskeletal and sports rehabilitation. However, cupping therapy has low to moderate evidence in musculoskeletal and sports rehabilitation and might be used as a useful intervention because it decreases the pain level and improves blood flow to the affected area with low adverse effects.

1.Introduction
Cupping therapy is a technique that uses one or more glass, plastic, or bamboo cups sucked on the skin with localized negative pressure [1]. Cupping therapy has been used to treat various diseases; including herpes zoster, hypertension, stroke, cough, asthma, and low back pain for more than four thousand years [1]. Recently, professional athletes have increased their interest in using cupping therapy [2]. Michael Phelps, a swimming athlete who has won the most gold medals in history, appeared at the 2016 Olympics with circular red marks on his shoulders due to the application of cupping therapy. Phelps indicated that cupping therapy could relieve his muscle fatigue and soreness [3]. In the National Basketball Association (NBA) of the 2018–2019 season, LeBron James, Russel Westbrook, and James Harden had received cupping therapy to treat their muscle soreness.
Although professional athletes favor cupping therapy in managing their muscle recovery and pain, the mechanism of cupping therapy and its exact effect in treating exercise-induced muscle fatigue and musculoskeletal conditions remain largely unknown [4]. Previous systematic or literature reviews on cupping mainly focused on investigating the effect of cupping therapy in treating musculoskeletal or sports conditions without reporting its evidence in treating these conditions [2, 5]. Also, it is unclear whether cupping therapy is effective in treating muscle recovery after exercise, training, and competition. Furthermore, the adverse effects of cupping therapy have been barely identified in the literature. A previous systematic review discussed the adverse effects of cupping therapy on musculoskeletal conditions [6]; however, this review was limited to a Korean population and did not discuss the adverse effects of cupping therapy on accelerating muscle recovery after exercise, training, and competition.
Several rehabilitation modalities were previously used to improve athletes’ performance and muscle recovery after exercise, training, and competition [7, 8, 9]. Davis et al. demonstrated that massage enhanced the related measures to performance (endurance, strength, jump, sprint, flexibility, or fatigue); however, these improvements are nonsignificant [8]. Rose et al. reported that whole body cryotherapy had a small effect on the recovery from muscle damage with several exposures; while, it significantly improved the recovery from pain, loss of muscle function, and markers of inflammation and damage [9]. Cupping therapy might have a superior role over both massage and cryotherapy because it can promote skin’s blood flow, change skin’s biomechanical properties, increase pain thresholds, improve local anaerobic metabolism, reduce inflammation, and modulate cellular mechanisms of the immune system [10].
Because of the promising role of cupping therapy in musculoskeletal and sports rehabilitation, the purpose of this study is to systematically review the effect of cupping therapy in musculoskeletal and sports rehabilitation, evaluate the evidence level of this effect, measure its adverse effects, and provide insight into the mechanism of cupping therapy on improving musculoskeletal and sports conditions.
2.Methods
2.1Design
Both systematic review and evidence-based analysis designs were used. The comprehensive guidelines of The National Center for The Dissemination of Disability Research with The Preferred Reporting Items for Systematic Reviews [11] were followed. Institutional approval of this systematic review was not necessary due to the nature of the study.
2.2Identification and selection of studies
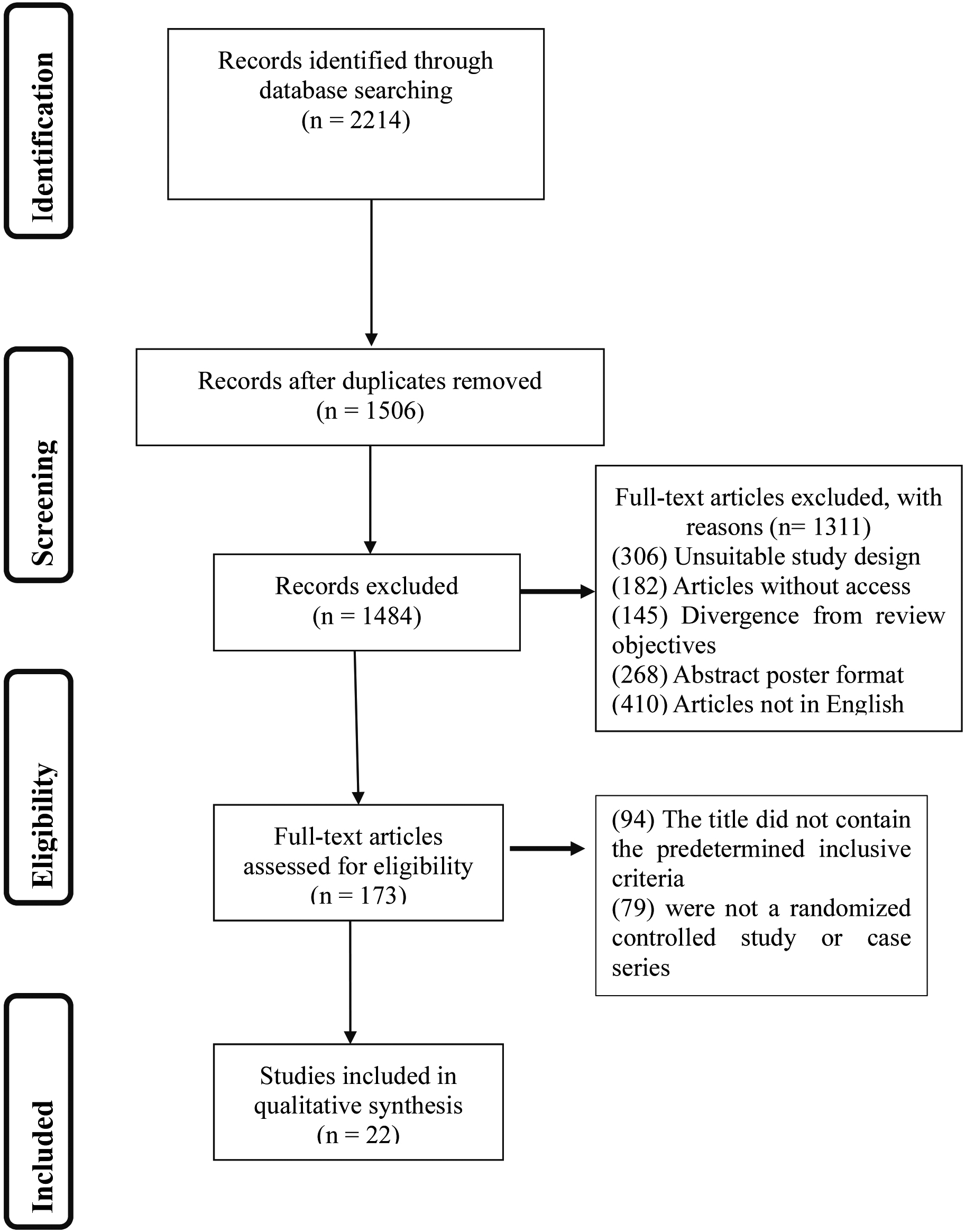
Twenty-two studies were identified through a computerized search. The search involved randomized and case series studies published between 1990 and 2019. The search was conducted through the server of the University of Illinois at Urbana-Champaign, IL, USA. The search strategy and search terms were based on a Patient, Intervention, Comparison, and Outcomes (PICO) design. The search was conducted for testing the effect of cupping therapy alone or in comparison to other rehabilitation modalities in musculoskeletal or sports-related conditions. This search involved five databases (Scopus, MEDLINE (PubMed), Web of Science, Academic Search Complete PLUS (EBSCO), and CrossRef) and contained only papers written in the English language and published in academic journals. The search strategy for the different elements of the PICO design is shown in Table 1. The flowchart of data extraction and search strategy findings is illustrated in Fig. 1.
Table 1
Full search strategy for the different elements of the PICO in the selected databases
| Patient | Intervention | Comparison | Outcomes |
|---|---|---|---|
| Musculoskeletal dysfunction ORsports injuries ORLow back pain ORCervical pain [MeSH] ORNeck pain ORPlantar fasciitis ORStiffness of soft tissues ORFibromyalgia [MeSH] ORMyofascial pain syndrome OROsteoarthritis ORMuscle fatigue ORDelayed onset muscle soreness [MeSH] ORAcute Muscle soreness OR | “Cupping” [MeSH] OR“Cupping therapy” [MeSH] OR“Wet cupping” [MeSH] OR“Dry cupping” [Mesh] OR“suction” [Mesh] OR“Cupping Massage” [Mesh] OR“traditional cupping” [MeSH] OR“Negative pressure” | “Range of motion, articular” [MeSH] OR“Pain” [MeSH] OR“Musculoskeletal Pain” [MeSH] OR“Chronic pain” [MeSH] OR“Muscle soreness” [Mesh] OR“Activities of daily living” [MeSH] OR“Sports” [MeSH] OR“Quality of life” [MeSH] OR“Patient Satisfaction” ORMuscle strength ORFunctionality ORFunctional ability ORActivities of daily living ORSports ORQuality of life ORPatient satisfaction |
Figure 1.
Flowchart of data extraction and search strategy findings.
2.3Eligibility criteria
Studies were selected founded on their goals of treatment. The used intervention should be cupping therapy and the disorder should be musculoskeletal and sports conditions. Inclusion criteria included cupping, musculoskeletal conditions, sports conditions, and randomized and case series studies. The age range of the participants in any study should be over 18 years. In this systematic review, studies were excluded if their participants had neurological or other diseases not related to musculoskeletal or sports rehabilitation. Also, we excluded pilot studies, case reports, letters to editors, opinions, commentaries, conference abstracts, dissertations, theses, or articles without access.
2.4Data collection process
An initial computerized database search was performed by the first author (AM) to find related studies to this review. Included data from each study was the title, journal name, authors, research drive, publication date, study design, randomization, blinding, power, age of participants, inclusion criteria, exclusion criteria, assessment dates, group comparability, homogeneity, examination techniques, and precision of exercise description.
Then, a co-author (XZ) assessed the title and abstract of each study. If any study fits our inclusion and exclusion criteria, the full text was downloaded. After gathering the full text of these studies, an additional reviewer (YJ) independently investigated included studies to see whether they fitted the inclusion and exclusion criteria or not.
2.5Quality assessment
All included studies were evaluated for methodological quality using the PEDro scale, which is a valid measure to assess the methodological quality of clinical trials [12]. Two reviewers (AM and Z.), who were not blinded to the details of studies, independently executed the assessment using a standardized method. Disagreements between both reviewers were solved by consulting a third reviewer (YJ). Methodological qualities of included studies were evaluated from 1 to 10 on a 10-item PEDro scale. The PEDro scale has 10 items, including random allocation, concealed allocation, similarity at baseline, subject blinding, therapist blinding, assessor blinding,
2.6Evidence-based analysis
Items were scored as either present or absent. The risk of bias in the study group, with 95% CI, was dependent on the predicted risk in the comparison group and the relative effect of the study (and its 95% CI). The grades of evidence included:
• High: We are very confident that the true effect lies close to the estimate of the effect;
• Moderate: We are moderately confident that the true effect lies close to the estimate of the effect; however, there is a possibility that it is different;
• Low: The confidence in the effect estimate is limited; the true effect may be different from the estimate of the effect;
• Very low: We have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect.
3.Results
3.1Characteristics of the included studies
The preliminary search in electronic databases revealed 2214 studies. We did not consider 1506 studies because of their duplication. We excluded 1311 studies for several reasons, including 306 studies that had unsuitable study designs, 182 studies that had no access to their full-text, 145 studies that had divergences from review objectives, 268 studies that were in abstract poster format only, and 410 studies not written in the English language. The residual 173 studies were included in this review based on their titles and abstracts. We did not include 151 studies after reading entire articles. The main reasons for this non-selection were: (1) The title did not contain the predetermined inclusive criteria (nighty-four studies), (2) The article was not a randomized controlled study or case series (seventy-nine studies). After reading the complete text of the residual studies, only 22 studies fulfilled the inclusion and exclusion criteria.
The included studies investigated individuals with an age range from18 to 60 years. Most studies used dry cupping, except for five studies, which used wet cupping [13, 14, 15, 16, 17]. Most studies compared cupping therapy to no intervention, three studies compared it to standard medical care, other studies compared it a specific intervention including heat [17], routine physiotherapy [18], electrical stimulation [19], active range of motion (ROM), and stretching [20], passive stretching [21], or acetaminophen [22]. Treatment durations ranged from one day to 12 weeks. The outcome measures included APS-POQ (American Pain Society Patient Outcome Questionnaire), ODQ, NRS (Numerical rating Scale), PPI (Present Pain Questionnaire), PPT (Pressure Pain Threshold), VAS (Oswestry Disability Questionnaire), FFbH-R (Funktionsfragebogen Hannover Rücken’), SF-36 (quality of life questionnaire Short form 36), MQS (Medication Quantification Scale), SF-MPQ (short-form McGill pain questionnaire), the number of acetaminophen tablets, skin surface temperature, blood pressure, functional disability, pain at motion, MDT (Mechanical Detection Threshold), VDT (Vibration Detection Threshold), cervical spine angle, the turtle neck angle, the pain threshold, the cervical ROM, The Levine CTS-score (Carpal tunnel syndrome), DASH-Score (The Disabilities of the Arm, Shoulder and Hand), SS-scale (Symptom Severity Scale), FSS (functional status scale), DSL (Distal Sensory Latency), DML (Distal Motor Latency), FAAM (The Foot and Ankle Ability Measure), LEFS (The Lower Extremity Functional Scale), PSFS (Patient-Specific Functional Scale), muscle strength, EMG (Electromyography), SLR (Straight Leg Raising) angle, popliteal angle, and muscle peak torque at 60
3.2Quality assessment
The PEDro scale was used for assessing the quality of involved studies. The PEDro scale assessment indicated that all included studies are randomized controlled trials except two studies by Hanan and Eman [13] and Yim et al. [26]. No information was included about blinding in the 10 studies by Hanan and Eman [13], Kim et al. [14], Farhadi et al. [15], Akbarzadeh et al. [27], Cramer et al. [28], Saha et al. [29], Lauche et al. [30], Yim et al. [26], Michalsen et al. [17], and Mohammadi et al. [18]. Nine studies included a control group to compare their results to the intervention group. The baseline similarities between groups were achieved in all studies except in the studies by Hanan and Eman [13], Yim et al. [26], and Michalsen et al. [17]. Intention to treat analysis was followed in all studies. The results of the assessment by the PEDro scale are listed in Table 3.
3.3Evidence-based analysis
This review revealed that cupping therapy has low-moderated effects. Cupping therapy had moderate effects on pain level and threshold; knee active and passive ROM; semitendinosus, and biceps femoris EMG in healthy males and females; pain level; and skin surface temperature (SST) at SI 15, GB 21, and LI 15 (acupuncture points) in patients with chronic neck pain.
Cupping therapy had low effects on severity sensation with pain; back disability in patients with low back pain; pain level; foot and ankle function; lower extremity function; pain pressure threshold in patients with plantar fasciitis; current pain level; morning pain; pain pressure threshold at calf and heel areas; foot and ankle function; ankle dorsiflexion ROM; and ankle plantar flexion strength in patients with heel pain. Cupping therapy had low effects on pain at rest; numbness; tingling; pain with pressure; and symptom severity in patients with carpal tunnel syndrome (CTS). Cupping therapy had low effects on neck pain at rest and with movement; neck-related function; physical component scores and mental component scores of SF-36 survey; pain pressure threshold; mechanical detection threshold; and vibration detection threshold in patients with neck pain. Cupping therapy had low effects on neck-related symptom severity; functional status; distal sensory latency; distal motor latency; cervical angle, turtle neck angle pain threshold; neck flexion ROM; neck extension ROM; and neck right and left lateral flexion in patients with carpal tunnel syndrome. Cupping therapy had low effects on pain level and intensity; disability; physical and mental component scores of SF-36 survey; and pain medications in patients with low back pain.
Cupping therapy had very low effects on straight leg raising (SLR); popliteal angle; and knee flexion peak torque at 60
Table 2
Characteristics of the included studies
| Study | Number of participants | Age (years, mean | Exercise methods | Duration of intervention | Outcome measures | Results | |||
|---|---|---|---|---|---|---|---|---|---|
| Study group | Control group | Within-groups | Between-groups | ||||||
| Hanan and Eman [13] | 30 | SG: 35.63 | Wet cupping therapy | No control group | One session | APS-POQ and ODQ |
|
| |
| Kim et al. [14] | 32 | SC: 44.20 | Wet cupping | No intervention | 2 weeks | NRS, PPI, and ODQ |
|
| |
| Teut et al. [23] | 110 | SG (1): 49.00 | Cupping | ||||||
| High pulsatile vacuum | Cupping | ||||||||
| Low pulsatile vacuum | No intervention | 12 weeks | VAS, FFbH-R, and SF-36 |
|
| ||||
| Farhadi et al. [15] | 98 | SG: 44.90 | Wet cupping | Usual care | 12 weeks |
|
|
| |
| Akbarzadeh et al. [27] | 100 | SG: 25.00 | |||||||
| CG: 27.00 | Dry cupping | Routine care | 2 weeks |
|
|
| |||
| AlBedah et al. [16] | 30 | SG: 36.48 | Wet cupping | No intervention | 4 weeks |
|
|
| |
| Chi et al. [32] | 60 | SG: 43.60 | Dry cupping therapy at SI 15, GB 21, and LI 15 acupuncture points | No intervention (20 min rest) | One session | VAS, skin surface temperature, and blood pressure |
| There were significant differences between both groups for all outcome measures | |
| Cramer et al. [28] | 50 | SG: 44.46 | Pulsating cupping therapy | Self-directed standard medical care | 5 sessions | NRS, functional disability, SF-36, PPT, and pain at motion |
| ANCOVA analysis revealed that there were significant differences between both groups for all outcome measures | |
| Saha et al. [29] | 50 | SG: 54.3 | Dry cupping | No intervention | 5 sessions |
|
|
| |
| Lauche et al. [30] | 50 | SG: 54.80 | Dry cupping therapy | No intervention | 1 session | VAS, pain with movement, SF-36, NDI, MDT, VDT, and PPT |
| ANCOVA analysis revealed that there were significant differences between both groups for all outcome measures except for the NDI | |
| Yim et al. [26] | 18 | SG: 22.66 | A Cross-over design in which, the two groups received both the McKenzie stretching and dry cupping therapy at different intervals | 1 session then one week as a washout period and crossover interventions | Cervical spine angle, the turtleneck angle, the pain threshold, and the cervical ROM |
|
| ||
| Michalsen et al. [17] | 52 | SG: 58.50 | wet cupping therapy | Heat over trapezius muscle. | 1 session | VAS, The Levine CTS-score, DASH-Score, and SF-36. |
|
| |
| Mohammadi et al. [18] | 56 | SG: N/A (only age range 18–60 years was written) | Dry cupping therapy and Routine physiotherapy (transcutaneous electrical nerve stimulation and ultrasound) | Routine physiotherapy | 10 sessions | SS-scale, FSS, DSL, and DML |
|
| |
| Weiqing et al. [19] | 29 | SG: 40.10 | |||||||
| CG: 39.30 | Dry cupping therapy | Electrical stimulation therapy | 8 sessions | VAS, FAAM, LEFS, and PPT | There were significant differences in all outcome measures within both groups |
| |||
| AlKhadhrawi and Alshamei [20] | 71 | SG: 41.00 | Dry cupping | Active ankle dorsiflexion exercise and stretching | 1 session |
|
|
| |
|
Table 2, continued | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Study | Number of participants | Age (years, mean | Exercise methods | Duration of intervention | Outcome measures | Results | |||
| Study group | Control group | Within-groups | Between-groups | ||||||
| Kim et al. [21] | 30 | SG: 30.10 | |||||||
| CG: N/A | Heated Dry cupping therapy | Passive stretching | One session |
|
|
| |||
| Murray and Clarkson [24] | 21 | SG: N/A (19 and 31 years) | |||||||
| CG: N/A | Moving cupping therapy | N/A | 1 session |
|
|
| |||
| Williams et1al [82] | 25 | 19.40 | Dry cupping therapy | No intervention | One session | Hamstring flexibility |
| There was a non-significant difference between both groups for hamstring flexibility | |
| Cao et al. [25] | 30 | SG: 53.30 | |||||||
| CG: N/A | Dry cupping | N/A | 15 days |
|
|
| |||
| Lauche et al. [52] | 141 | SG: 54.35 | Dry cupping | Shame cupping | Usual care | 18 days |
|
|
|
| Teut et al. [33] | 40 | SG: 68.10 | |||||||
| CG: 69.3 | Dry cupping | no intervention | 8 sessions | VAS and WOMAC, and SF-36 |
|
| |||
| Khan et al. [22] | 20 | Only age range from30 to 60 years for both groups was written without means | Dry cupping | Acetaminophen 650 mg, twice/day | 3 sessions | Pain, stiffness, tenderness, edema, disability, crepitation, and nocturnal pain scales. These scales were developed by the authors |
|
| |
ROM: Range of motion, PROM: Passive range of motion, AROM: Active range of motion, SG: Study group, CG: Control group, APS-POQ: American Pain Society Patient Outcome Questionnaire, ODQ: Oswestry Disability Questionnaire, VAS: Visual analogue scale, NRS, Numerical rating Scale, PPI: Present Pain Questionnaire, FFbH-R: Funktionsfragebogen Hannover Rücken’, SF-36: quality of life questionnaire Short form 36, MQS: Medication Quantification Scale, SF-MPQ: short-form McGill pain questionnaire, PPT: Pressure Pain Threshold, NDI: Neck Disability Index, MDT: Mechanical Detection Threshold, VDT: Vibration Detection Threshold, DASH-Score: The Disabilities of the Arm, Shoulder and Hand, SS: Symptom Severity Scale, FSS: functional status scale, DSL: Distal Sensory Latency, and DML: Distal Motor Latency, FAAM: The Foot and Ankle Ability Measure, LEFS: The Lower Extremity Functional Scale, PSFS: Patient-Specific Functional Scale, EMG: Electromyography, SLR: Straight Leg Raising, and WOMAC: McMasters Universities Osteoarthritis Index.
Table 3
PEDro scale of the included studies
| Included studies | Eligibility criteria | Randomization | Concealed allocation | Baseline similarity between groups | Blinding of participants | Blinding of therapists | Blinding of all assessors | Key outcome measurements | Intention to treat Analysis | Results of between-group comparisons | Measures of variability |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Hanan and Eman [13] | Yes | No | No | No | No | No | No | Yes | Yes | Yes | Yes |
| Kim et al. [14] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes |
| Teut et al. [23] | Yes | Yes | No | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Farhadi et al. [15] | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes |
| Akbarzadeh et al. [27] | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes |
| AlBedah et al. [16] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Chi et al. [32] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes |
| Cramer et al. [28] | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes |
| Saha et al. [29] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes |
| Lauche et al. [30] | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes |
| Yim et al. [26] | Yes | No | No | No | No | No | No | Yes | Yes | Yes | Yes |
| Michalsen et al. [17] | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Mohammadi et al. [18] | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Weiqing et al. [19] | Yes | Yes | No | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| AlKhadhrawi and Alshamei [20] | Yes | Yes | No | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Kim et al. [21] | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Murray and Clarkson [24] | No | No | No | No | No | No | No | Yes | Yes | No | No |
| Williams et al. [82] | Yes | Yes | No | No | No | Yes | Yes | Yes | No | Yes | No |
| Cao et al. [25] | Yes | No | No | No | No | No | No | Yes | Yes | No | No |
| Lauche et al. [52] | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Teut et al. [33] | Yes | Yes | Yes | No | No | No | No | Yes | Yes | Yes | Yes |
| Khan et al. [22] | Yes | Yes | No | No | No | No | No | Yes | Yes | Yes | Yes |
therapy had very low effects on affective and sensory pain perception, function, physical and mental component scores of SF-36 survey, general and physical fatigue, and sleep period in patients with chronic low back pain.
3.4Adverse effects
This review revealed that the incidence of adverse effects of wet and dry cupping therapy was very low to low. The main adverse effects included hematoma at the site of application of a cupping glass [31]; mild low back pain related to the seated position [32]; muscle soreness for 1–2 days, minor hematoma at the treated site for 2 days, and increased neck pain for 1–5 h [28]; pain, slight reactions such as circulatory instability in the first minute after treatment, tension headaches, migraine attack, reappearing tinnitus, and wound healing itches [30]; an aggravation of pain after the cupping sessions for few hours [33]; headache after cupping lasted for no longer than 60 min [29]; minor burns as a result of the steam in the cups [25]; and mild hematomas at cupping site, self-limiting light tingling sensations for a few minutes, and increased pain [23].
4.Discussion
This systematic and evidence-based review is unique as it is the first review that discusses the evidence level of cupping therapy in musculoskeletal and sports rehabilitation along with providing the mechanisms behind the effect of cupping therapy in each condition. We discussed the included conditions in different sections for a better understanding of the discussion.
4.1Low back pain (evidence: Low to moderate)
Six studies conducted cupping therapy in patients with low back pain [13, 14, 15, 16, 23, 27]. Teut et al. [23] investigated the effect of dry cupping therapy on pain and disability in patients with chronic low back pain. They found that after 4 weeks of cupping therapy, pain and disability significantly decreased, whereas after 12 weeks cupping therapy significantly decreased the pain level only and this decrease continued to be significant. They attributed these results to three mechanisms. The first mechanism included that cupping therapy deformed the skin which could excite A
The results of these studies come in accordance with a recent meta-analysis that reported that cupping therapy is more effective than standard medical care in treating low back pain [34]. Also, Markowski et al. [35] investigated the effect of cupping therapy on pain in patients with low back pain. They found that four sessions of cupping therapy significantly decreased pain and increased straight-leg raise motion, lumbar flexion ROM, and the pain-pressure threshold.
Cupping therapy can be used alone or with other rehabilitative or pharmaceutical interventions in treating cervical or low back pain. Cupping therapy can reduce pain, muscle tenderness, and improve ROM in patients with subacute or chronic low back pain [34]. Cupping therapy can be applied over Ashi acupoints. Ashi acupoints refer to the points which can increase or decrease pain sensation. Ashi points have neither specific terms nor fixed location. Ashi points are selected as acupoints according to where the uncomfortable feeling is located [36].
The evidence-based analysis of the six included studies revealed that the evidence of the effect of cupping therapy in treating low back pain was low to moderate. The included studies have several issues which decreased their evidence. The study by Kim et al. [14] did not include the blinding of therapists and assessors. Also, the authors did not mention where this study was conducted. Furthermore, the study sample size was small. Accordingly, the evidence level of this study was low. The study by Farhadi et al. [15] did not mention within-group analysis and there were no blinding of therapists and assessors. Accordingly, the evidence level of this study was low. The study by AlBedah et al. [16] mentioned that the
4.2Cervical pain (evidence: Low to moderate)
In this review, four studies investigated the effect of cupping therapy on pain inpatient with cervical pain [29, 32, 28, 30]; and one study investigated the effect of cupping therapy on cervical ROM in normal subjects [26]. Saha et al. [29] examined the effect of cupping massage therapy on pain and disability levels in patients with neck pain. They found that dry cupping therapy significantly decreased pain and disability after 2 weeks. Cramer et al. [28] examined the effect of dry cupping therapy on pain at rest and with motion, disability, and pressure, mechanical, vibration thresholds. They found that dry cupping therapy significantly decreased pain at rest and with motion, decreased disability, and increased pressure pain threshold. These studies attributed these results to manual lifting and kneading of muscle tissue produced by cupping therapy which decreased neuromuscular excitability [28, 29]. Cramer et al. [28] reported that applying massage with the cup can produce an inhibitory effect, which helps in reducing muscle spasm. Lauche et al. [30] examined the effect of traditional cupping on pain and mechanical thresholds in patients with chronic nonspecific neck pain. They found that dry cupping therapy significantly decreased pain and increased pressure pain thresholds and quality of life. Also, there was no significant effect of cupping on neck disability, mechanical detection, and vibration detection. Chi et al. [32] investigated the effect of cupping therapy on chronic neck and shoulder pain. They found that cupping therapy significantly decreased neck and shoulder pain. Yim et al. [26] compared the effects of McKenzie stretching exercise to cupping therapy on pain threshold, cervical ROM, cervical spine angle, and turtle neck angle. They found that cupping therapy significantly increased pain threshold and cervical ROM, while McKenzie’s stretching did not. Also, they found that both stretching and dry cupping had no significant effect on the cervical spine angle or the turtleneck angle.
The evidence-based analysis of the five included studies revealed that the evidence of the effect of cupping therapy in treating neck pain was low to moderate. The study by Saha et al. [29] included between-groups and within-group analyses. The mean differences between groups were significant for most outcome measures. There was no blinding of patients and therapists. Accordingly, the evidence level of this study was moderate. The study by Cramer et al. [28] did not write the value of the pain intensity at the baseline as other variables. Additionally, this study did not include concealed allocation, blinding of therapists, blinding of all assessors, or blinding of participants. Accordingly, the evidence level of this study was low. The study by Lauche et al. [30] included between-groups and within-group analyses. The mean differences between groups were significant for most outcome measures. This study did not include concealed allocation, blinding of therapists, blinding of all assessors, or blinding of participants. Accordingly, the evidence level of this study was moderate. The study by Chi et al. [32] compared the results using analysis of covariance (ANCOVA) using the adjusted treatment group for baseline measurements as a fixed factor. In this study, the mean differences for all outcome measures were small. Accordingly, the evidence level of this study was moderate. The study by Yim et al. [26] used a small sample size and performed within-groups analyses only. Accordingly, the evidence level of this study was low. The evidence-based analyses of cupping therapy in neck pain are shown in Supplementary Tables 7-11.
4.3Carpal tunnel syndrome (evidence: Low)
Although CTS might be uncommon among able-bodied athletes, it has been shown in the literature that CTS is very common among athletes with a disability, particularly basketball wheelchair players [37, 38, 39].
In this review, three studies investigated the effect of cupping therapy on CTS and its related symptoms [17, 18]. Michalsen et al. [17] investigated the effect of cupping therapy on symptoms of CTS. They assumed that for better treatment of CTS, cupping therapy should be applied on defined zones (these zones segmentally relate to the median nerve) in the shoulder triangle. They applied wet cupping therapy far from the carpal tunnel on the trapezius muscle. They assessed their patients 7 days after cupping therapy. They found that there were significant improvements in Levine’s CTS score, neck pain, functional disability (DASH Score), and physical quality of life. Mohammadi et al. [18] used dry cupping therapy which was applied on the volar surface of the wrist for 4 min at a pressure of 50 mmHg. They performed cupping therapy for 10 sessions/every alternate day and the assessment was performed after these 10 sessions. They found there were significant improvements in both CTS symptoms and median nerve conduction time. They argued these improvements to the biomechanical effects created by cupping therapy that helped to decrease compression on median nerve.
Results of these two studies come in accordance with the results of the case report study that investigated the effect of cupping therapy on CTS-related symptoms [40]. They found that cupping therapy significantly improved CTS symptoms within the first week and these symptoms progressively decreased with complete resolution of symptoms after 6 to 8 weeks. They reported also that there were significant improvements in median nerve conduction velocity and initial abnormalities presented in the wrist joint.
The evidence-based analysis of these two studies revealed that the evidence of the effect of cupping therapy in treating CTS was low. The study by Michalsen et al. [17] did not include concealed allocation, baseline similarity between groups, or blinding of participants. Additionally, they demonstrated that heat increased pain, which might be difficult to be accepted. Accordingly, the evidence level of this study was low. The study by Mohammadi et al. [18] did not include concealed allocation or blinding of participants. Also, changes between means are very small to be significant. Accordingly, the evidence level of this study was low. The evidence-based analyses of cupping therapy in CTS are shown in Supplementary Tables 12 and 13.
4.4Plantar fasciitis (evidence: Low)
Plantar fasciitis is considered a communal overuse injury in sports, particularly in runners [41, 42]. Lopes et al. demonstrated that the prevalence of plantar fasciitis in runners varies from 4.5 to 10%, and it is considered as the third most common running-related musculoskeletal injury after medial tibial stress syndrome and Achilles tendinopathy [43]. Planter fascia plays an important role in providing static and dynamic supports for arches of the foot by distributing forces placed on the whole foot during weight-bearing activities [44, 45].
In this review, two studies investigated the effect of cupping therapy on plantar fasciitis and heel pain [19, 20]. Weiqing et al. [19] investigated the effect of dry cupping therapy on pain and function in patients with plantar fasciitis. They compared cupping therapy to electrical stimulation. They found that cupping therapy was effective as electrical stimulation in decreasing pain and improving lower limbs function. They argued these improvements to local negative pressure created by dry cupping. This negative pressure increased blood flow which helped in removing exudates and increasing anti-inflammatory substances. AlKhadhrawi and Alshamei [20] examined the effect of dry cupping on pain and function in patients with plantar heel pain. They divided participants into two groups (intervention and control groups). Both groups performed ankle dorsiflexion exercise and stretching exercise for calf muscle and plantar fascia. In addition, the intervention group received dry cupping. They found that pain at rest immediately showed a significant decrease in the intervention group, but not in the control group. Morning pain significantly decreased in both groups after 2 days, with a significant difference between both groups. Pain perceived threshold showed an immediate significant improvement in the intervention group, but not in the control group. Both groups showed significant improvements in patient-specific functional scale and ankle dorsiflexion ROM. Plantar flexor strength showed an immediate significant improvement in the intervention group, but not in the control group.
The results of these two studies come in accordance with the results of the recent study conducted by Escaloni et al. [46] to investigate the effect of the combination of dry cupping therapy and neural glide on peripheral neuropathic plantar foot pain. They applied a 4.5 mm diameter cup positioned fixed on the superior medial tibia at the proximal course of the saphenous nerve. Another large cup was placed on an acupoint called Spleen 9 (SP-9) to provide higher stress at the line among fat and muscle layers. To provide a pull force at the cup, the patient was asked to extend the knee with ankle dorsiflexion while the cup was maintained at SP-9 via negative pressure from the suction. To add more pull at the cup, a cervical flexion was added. After three weeks, they found that there were significant improvements in pain and ankle joint ROM.
The evidence-based analysis of these studies revealed that the evidence of the effect of cupping therapy in treating carpal tunnel syndrome was low. The study by Weiqing et al. [19] did not include blinding of therapists, blinding of all assessors, or concealed allocation. Also, the sample size was small. Accordingly, the evidence level of this study was low. The study by AlKhadhrawi and Alshamei [20] did not include concealed allocation or blinding to participants and therapists. Also, there performed within-group analysis only. Accordingly, the evidence level of this study was low. The evidence-based analyses of cupping therapy in plantar fasciitis are shown in Supplementary Tables 14 and 15.
4.5Stiffness of soft tissues (evidence: Low)
The decrease in flexibility of connective tissues is a common symptom that occurs after either repeated sports injuries [47] or prolonged immobilization [48]. Prolonged immobilization usually follows sport-causing surgeries such as anterior cruciate ligament reconstruction surgery, meniscal repair, or fractures. Delaloye et al. [49] investigated the rate of loss in knee extension ROM after anterior cruciate ligament reconstruction surgery. They found that the rate of loss in knee extension was rapid, and it occurred due to hamstring contracture and quadriceps inactivation more than intra-articular mechanical pathology.
In this review, three studies discussed the effect of cupping therapy on flexibility, tissue stiffness, power, and ROM [50, 21, 24]. Kim et al. [21] examined the effect of cupping therapy on flexibility, knee ROM, pain threshold, and muscle activity of the hamstring muscle. They applied three dry cups on the hamstring muscle for 5 min. They found that cupping therapy significantly improved flexibility, pain threshold, and muscle contraction. They argued this improvement in connective tissues flexibility to the effect of cupping therapy on producing an effective mobilization of connective tissues including muscle, tendon, fascia, and skin. This mobilization increased neurophysiological activity at various levels, including nociceptors, spinal cord, and other nerves. This finally caused a significant relaxation of these connective tissues [51]. Additionally, the negative pressure created by the application of cupping therapy (which reaches about 4 inches) exerted various mechanical effects including relieving of muscular pain, restoration of muscle flexibility, recovery from adhesions, and release of tissues that bounded up within muscle [13]. Williams et al. [50] investigated the effects of cupping on hamstring flexibility in college soccer players. They found that 7 min of therapeutic cupping treatment did not significantly increase hamstring flexibility. This non-significant decrease might be due to the short period of application of cupping. On the contrary, the pilot study by Markowski et al. [35] indicated that cupping significantly increased lumbar flexion and straight leg raise. Murray and Clarkson [24] investigated the effect of cupping therapy on knee ROM. All participants in this study received 15 min of moving cupping therapy to their dominant posterior lower extremity. They found that moving cupping therapy significantly increased hip and knee ROM by 7% in the straight leg raise and 4% in a popliteal angle test. Also, they found that moving cupping had no significant effect on knee flexion power measures.
The evidence-based analysis of these studies revealed that the evidence of the effect of cupping therapy in treating stiffness of soft tissues was low to moderate. The study by Kim et al. [21] did not include blinding of therapists or blinding of all assessors. Also, it did not mention the setting where this study was conducted. Furthermore, the sample size was small. Accordingly, the evidence level of this study was low. The study by Williams et al. [50] did not include blinding of therapists, blinding of all assessors, or concealed allocation. Also, they performed within-group analyses only. Accordingly, the evidence level of this study was low. The study by Murray and Clarkson [24] included one group, had a small sample size, no randomization, no blinding, and non-significant results. Accordingly, the evidence level of this study was low. The evidence-based analyses of cupping therapy on the stiffness of soft tissues are shown in Supplementary Tables 16–18.
4.6Fibromyalgia (evidence: Very low)
Fibromyalgia is a common disorder [53]. Individuals with fibromyalgia exhibit greater sensitivity to a wider range of stimuli, such as cold and heat, besides mechanical and ischemic pressure stimuli. These stimuli yield pain responses in these individuals when applied at intensity levels that do not normally evoke pain responses [54, 55]. The frequency of fibromyalgia among competitive sports professionals is around 2.2% [56].
The main effect of cupping therapy in fibromyalgia may be through reducing pain and increasing its threshold. The effect of cupping therapy on increasing pain threshold may be attributed to several mechanisms. The first mechanism might be due to mechanical effects exerted by the negative pressure produced by cupping therapy. This negative pressure stimulates mechanoreceptors, which their signals are transferred to the spinal cord faster than pain signals. Thus, this mechanism blocks pain signals and increases pain threshold (pain gate control theory) [26, 30, 32]. The second mechanism might be due to the increase in fluid and blood movements presented either during or after removing the cup [57]. This could increase the removal of any excess fluid or toxins beneath the skin. Consequently, an increase in the space between the fascia and lower structures occurs by elevating the fascia over the inflammatory and pain core. Also, increasing the circulation helps in obstructing the accumulation of pain chemicals in the affected area. It has been shown that the increase in the amount of these chemicals decreases the pain threshold and causes rapid development of pain [58]. The third mechanism might be due to the increase in local microcirculation induced by cupping therapy. This increase in local microcirculation improves muscle function in the affected areas. All these discussed effects cause a decrease in the hypersensitivity of trigger points [28, 59], thus an increase in pain threshold could occur in these points.
In this review, two studies (one randomized trial and one case series) investigated the effect of cupping therapy in people with fibromyalgia [25, 52]. Cao et al. [25] investigated the effect of cupping therapy in treating fibromyalgia. In this study, 30 consecutive persons with fibromyalgia were received dry cupping therapy. Pain assessment and decrease in the number of tender points were performed at the 5
The evidence-based analysis of the three included studies revealed that the evidence of the effect of cupping therapy in treating fibromyalgia was very low. The study by Cao et al. [25] included no randomization, concealed allocation, blinding of participants, blinding of therapists, or blinding of all assessors. In addition, changes in all variables were small. Also, Also, they performed within-group analyses only. Accordingly, the evidence level of this study was very low.
Lauche et al. [52] included large sample size and between-groups analyses; however, there was no concealed allocation. Accordingly, the evidence level of this study was moderate. The evidence-based analyses of cupping therapy in fibromyalgia are shown in Supplementary Tables 19 and 20.
4.7Osteoarthritis (evidence: Very low to low)
Osteoarthritis commonly occurs in weight-bearing joints, particularly the knee joint. Knee osteoarthritis associates some sports (e.g., soccer, elite-level long-distance running, competitive weightlifting, wrestling) and can lead it a significant disability and early retirement of sports [61, 62]. Cupping therapy produces significant effects on alleviating most symptoms that accompany knee osteoarthritis [60].
The main effect of cupping therapy in knee osteoarthritis is attributed to its analgesic effect. Cupping therapy acts over neural centers in spinal cord causing a release of some chemical transmitters and endogenous opioids. This helps in blocking pain messages, facilitating nociceptive painful reception, and producing a comfortable feeling [63]. Cupping therapy also improves blood flow around the treated area. Thus, it helps in elevating toxins stuck deep in soft-tissue layers to superficial body surface areas [64]. Furthermore, it has been demonstrated that cupping therapy modulates inflammatory reactions by increasing lymph flow [65]. Furthermore, Dons’koi et al. [66] and Tagil et al. [67] reported that cupping therapy regulates the immune system by eliminating oxidants and decreasing numbers of cytotoxic natural killer cells. These previous effects can significantly relieve the pain and decrease inflammatory reactions present with knee osteoarthritis.
In this review, two randomized studies discussed the effect of cupping therapy on knee Osteoarthritis [33, 22]. Khan et al. [22] investigated the effect of dry cupping on knee osteoarthritis-related symptoms. They found that dry cupping significantly improved pain, tenderness, edema, nocturnal pain, and disability. Teut et al. [33] investigated the effect of dry cupping on pain (assessed by the Visual Analogue Scale) and activities of daily living, functional mobility, gait, general health, and quality of life (assessed by the Western Ontario and McMaster Universities Osteoarthritis (WOMAC) score and SF-36 score). They found that cupping therapy significantly improved pain and activities of daily living, functional mobility, gait, general health, and quality of life. These results contradict the results of the recent systematic review which reported that there is weak evidence to support the hypothesis that cupping therapy has beneficial effects on reducing the pain intensity and improving the physical function in patients with knee osteoarthritis [60].
The evidence-based analysis of the two included studies revealed that the evidence of the effect of cupping therapy in treating knee osteoarthritis is very low to low. The study by Khan et al. [22] did not include concealed allocation, baseline similarity between groups, blinding of participants, or blinding of therapists. In addition, they used self-developed scales that have no validity or reliability. Furthermore, Also, they performed within-group analyses only. Accordingly, the evidence level of this study was very low. Teut et al. [33] did not mention within groups analyses and baseline similarities. Also, the sample size was small. Accordingly, the evidence level of this study was low. The evidence-based analyses of cupping therapy on the stiffness of soft tissues are shown in Supplementary Tables 21 and 22.
4.8Muscle fatigue (evidence: Very low)
In this review, no study directly investigated the effect of cupping therapy on muscle fatigue; however, one study investigated fatigue as an outcome measure in evaluating the effect of cupping therapy on fibromyalgia [52]. They found that cupping therapy has no significant effects on general, physical, or mental fatigue.
Muscle fatigue is common among athletes. Current exercise interventions include either grading exercise intensity, increasing rest period, using mild training intensity, or using massage for the fatigued muscle. The effect of these exercise interventions is still in debate [68, 69]. Animal studies reported that the accumulation of metabolites or decreasing oxygen amount has a major role in the impairment of muscle contraction. Consequently, the occurrence of muscle fatigue at the cellular level [70, 71, 72]. The role of accumulated metabolites in producing muscle fatigue was extensively shown in the literature [72, 73, 74, 75].
When individuals work or exercise, the metabolic rate increases considerably, and a fast increase in metabolites concentration occurs. At the beginning of any exercise or work, the muscle uses oxygen to provide ATP as a source of energy (cellular respiration). After the depletion of oxygen, the glycolysis process begins to provide the needed amount of ATP by converting glucose into pyruvate. Then pyruvate transforms to lactic acid [73]. Intracellular acidosis that occurs due to lactic acid accumulation was reported as the most important cause of skeletal muscle fatigue. The accumulation of lactic acid reduces the PH which reduces the sensitivity of the contractile apparatus to Ca
The effect of cupping therapy on decreasing muscle fatigue might be attributed to two mechanisms. The first mechanism might occur due to the decrease in number of accumulated metabolites produced by the increase in fluid exchange due to the application of cupping therapy. Yoo and Tauskl have demonstrated that cupping therapy increased blood circulation and helped in removing toxins and waste products from the body [64]. This helped in removing these metabolites and decreasing the recovery period after any exercise. The second mechanism might be due to the increase in the oxygen supply to working muscles. Li et al. conducted a study to demonstrate the effect of cupping therapy on increasing oxygen supply to working muscles [76]. They performed a dry cupping therapy placed on the infraspinatus muscle, and they used near-infrared spectroscopy to assess the concentration change in blood volume, deoxyhemoglobin, and oxyhemoglobin. They found that there was a significant decrease in deoxyhemoglobin and a significant increase in the oxy-hemoglobin amount in tissues adjacent to the cupping site. Happle has demonstrated that the increase of oxygen supply to the contracting muscles delayed the occurrence of muscle fatigue and increased the time to exhaustion [77]. Several studies demonstrated that cupping therapy could delay the rate of muscle fatigue during sports performance. This might be attributed to its negative pressure which increases the space between the fascia and lower structures. Thus, better oxygenation and blood flow to working muscles occur during sports performance [58, 78]. Future studies showed be conducted to investigate the effect of cupping therapy on muscle fatigue, particularly in athletes.
4.9Delayed onset muscle soreness (DOMS) (evidence: Very low)
This review could not find any study that directly investigated the effect of cupping therapy on delayed muscle soreness. Delayed onset muscle soreness is a usual experience of novice or elite athletes and it is considered a type of structural muscle injury [79]. It was reported in the literature that there were several possible mechanisms responsible for the development of pain in DOMS including, lactic acid, muscle spasm, connective tissue damage, muscle damage, and inflammation [79, 80, 81].
The effect of cupping therapy on treating or preventing DOMS is similar to its effects on muscle fatigue. Cupping therapy increases blood circulation and fluid exchange which helps in removing excess amounts of lactic acid responsible for developing pain, as previously discussed [28, 57, 76]. The effect of cupping therapy in treating muscle or connective tissues damages might be attributed to either the increase in the blood circulation which enhances the own body’s anti-inflammatory mechanism or the renormalization of the alignment of muscle and connective tissues which helps in a faster improvement and lesser incidence of re-injuries. Also, the effect of cupping therapy on decreasing muscle spasm as a source of DOMS might be due to lifting and kneading effects produced by cupping therapy in spasmed muscles. This can decrease muscle tone through a massage-like effect. Consequently, a relaxation of the spasmed muscle can occur faster. Also, the improvement of muscle spasm can decrease ischemic pain created by muscle spasm. Muscle spasm can lead to pain through exciting mechanosensitive nociceptors or compressing local blood vessels, causing ischemic pain. Prolonged ischemic pain could induce hypersensitivity to noxious stimuli and lower pain thresholds [28]. Future studies showed be conducted to investigate the effect of cupping therapy in individuals with DOMS, particularly in athletes.
5.Conclusion
This review provided the first attempt to analyze the evidence level of cupping therapy in musculoskeletal and sports rehabilitation. The review concluded that the evidence of using cupping therapy in musculoskeletal and sports rehabilitation is low to moderate. The main effects of cupping therapy included decreasing pain and increasing blood supply through negative pressure. This review suggested that however of the low- moderate evidence of the effect of cupping therapy, it is a useful intervention to be performed in musculoskeletal and sports rehabilitation because it decreases pain level and increases pain threshold with a low incidence of adverse effects. In addition, it may improve blood flow to the affected area which includes anti-inflammatory substances.
Funding
There was no funding for this study.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/BMR-210242.
Acknowledgments
All authors contributed to the conceptual design, preparation of the draft, and revision of the paper.
Conflict of interest
None of the authors have any conflict of interest to declare.
References
[1] | Jennifer Brett ND, L. A. Clean needle technique manual. 7th ed. (2016) , the United States of America: Council of Colleges of Acupuncturem and Oriental Medicine. |
[2] | Lee MS, Kim JI, Ernst E. Is cupping an effective treatment? An overview of systematic reviews. Journal of Acupuncture and Meridian Studies. (2011) ; 4: (1): 1-4. |
[3] | Trofa DP, et al. The evidence of common nonsurgical modalities in sports medicine, Part 2: Cupping and blood flow restriction. J Am Acad Orthop Surg Glob Res Rev. (2020) ; 4: (1): e1900105. |
[4] | Lowe DT. Cupping therapy: An analysis of the effects of suction on skin and the possible influence on human health. Complement Ther Clin Pract. (2017) ; 29: : 162-168. |
[5] | Cao HJ, Han M, Zhu XS, Liu JP. An overview of systematic reviews of clinical evidence of cupping therapy. Journal of Traditional Chinese Medical Sciences. (2015) ; 2: (1): 3-10. |
[6] | Kim T-H, et al. Adverse events related to cupping therapy in studies conducted in Korea: A systematic review. European Journal of Integrative Medicine. (2014) ; 6: (4): 434-440. |
[7] | Alawna M, Mohamed AA. Short-term and long-term effects of ankle joint taping and bandaging on balance, proprioception and vertical jump among volleyball players with chronic ankle instability. Phys Ther Sport. (2020) ; 46: : 145-154. |
[8] | Davis HL, Alabed S, Chico TJA. Effect of sports massage on performance and recovery: A systematic review and meta-analysis. BMJ Open Sport Exerc Med. (2020) ; 6: (1): e000614. |
[9] | Rose C, et al. Whole-body cryotherapy as a recovery technique after exercise: A review of the literature. Int J Sports Med. (2017) ; 38: (14): 1049-1060. |
[10] | Aboushanab TS, AlSanad S. Cupping therapy: An overview from a modern medicine perspective. J Acupunct Meridian Stud. (2018) ; 11: (3): 83-87. |
[11] | Page MJ, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst Rev. (2021) ; 10: (1): 89. |
[12] | de Morton NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Australian Journal of Physiotherapy. (2009) ; 55: (2): 129-133. |
[13] | Hanan SA, Eman SE. Cupping therapy (Al-Hijama) – It’s impact on persistent non-specific lower back pain and client disability. Life Science Journal. (2013) ; 10: (4s): 631-642. |
[14] | Kim JI, et al. Evaluation of wet-cupping therapy for persistent non-specific low back pain: A randomised, waiting-list controlled, open-label, parallel-group pilot trial. Trials. (2011) ; 12: : 146. |
[15] | Farhadi K, et al. The effectiveness of wet-cupping for nonspecific low back pain in Iran: A randomized controlled trial. Complement Ther Med. (2009) ; 17: (1): 9-15. |
[16] | AlBedah A, et al. The use of wet cupping for persistent nonspecific low back pain: Randomized controlled clinical trial. J Altern Complement Med. (2015) ; 21: (8): 504-8. |
[17] | Michalsen A, et al. Effects of traditional cupping therapy in patients with carpal tunnel syndrome: A randomized controlled trial. J Pain. (2009) ; 10: (6): 601-8. |
[18] | Mohammadi S, et al. The effects of cupping therapy as a new approach in the physiotherapeutic management of carpal tunnel syndrome. Physiother Res Int. (2019) ; 24: (3): e1770. |
[19] | Weiqing G, Leson C, Vukovic C. Dry cupping for plantar fasciitis: A randomized controlled trial. Journal of Physical Therapy Science. (2017) ; 29: (5): 859-862. |
[20] | AlKhadhrawi N, Alshami A. Effects of myofascial trigger point dry cupping on pain and function in patients with plantar heel pain: A randomized controlled trial. J Bodyw Mov Ther. (2019) ; 23: (3): 532-538. |
[21] | Kim J-E, et al. Effect of cupping therapy on range of motion, pain threshold, and muscle activity of the hamstring muscle compared to passive stretching. Journal of The Korean Society of Physical Medicine. (2017) ; 12: (3): 23-32. |
[22] | Khan AA, Jahangir U, Urooj S. Management of knee osteoarthritis with cupping therapy. J Adv Pharm Technol Res. (2013) ; 4: (4): 217-23. |
[23] | Teut M, et al. Pulsatile dry cupping in chronic low back pain – a randomized three-armed controlled clinical trial. BMC Complement Altern Med. (2018) ; 18: (1): 115. |
[24] | Murray D, Clarkson C. Effects of moving cupping therapy on hip and knee range of movement and knee flexion power: A preliminary investigation. J Man Manip Ther. (2019) ; 27: (5): 287-294. |
[25] | Cao H, et al. Medicinal cupping therapy in 30 patients with fibromyalgia: A case series observation. Forsch Komplementmed. (2011) ; 18: (3): 122-6. |
[26] | Yim J, et al. Comparison of the effects of muscle stretching exercises and cupping therapy on pain thresholds, cervical range of motion and angle: A cross-over study. Physical Therapy Rehabilitation Science. (2017) ; 6: (2): 83-89. |
[27] | Akbarzadeh M, et al. The Effect Dry Cupping Therapy at Acupoint BL23 on the Intensity of Postpartum Low Back Pain in Primiparous Women Based on Two Types of Questionnaires, 2012; A Randomized Clinical Trial. International Journal of Community Based Nursing and Midwifery. (2014) ; 2: (2): 112-20. |
[28] | Cramer H, et al. Randomized controlled trial of pulsating cupping (pneumatic pulsation therapy) for chronic neck pain. Forsch Komplementmed. (2011) ; 18: (6): 327-34. |
[29] | Saha FJ, et al. The effects of cupping massage in patients with chronic neck pain – a randomised controlled trial. Complement Med Res. (2017) ; 24: (1): 26-32. |
[30] | Lauche R, et al. The effect of traditional cupping on pain and mechanical thresholds in patients with chronic nonspecific neck pain: A randomised controlled pilot study. Evid Based Complement Alternat Med. (2012) ; 2012: : 429718. |
[31] | Michalsen A, et al. Effects of traditional cupping therapy in patients with carpal tunnel syndrome – a randomized controlled trial. Evidence-based Complement Alternative Medicine. (2009) ; 10: (1-8): 601-608. |
[32] | Chi LM, et al. The effectiveness of cupping therapy on relieving chronic neck and shoulder pain: A randomized controlled trial. Evid Based Complement Alternat Med. (2016) ; 2016: : 7358918. |
[33] | Teut M, et al. Pulsatile dry cupping in patients with osteoarthritis of the knee – a randomized controlled exploratory trial. BMC Complementary and Alternative Medicine. (2012) ; 12: (1): 1. |
[34] | Yuan QL, Guo TM, Liu L, Sun F, Zhang YG. Traditional Chinese medicine for neck pain and low back pain: A systematic review and meta-analysis. PLoS One. (2015) ; 10: (2): e0117146. |
[35] | Markowski A, Sanford S, Pikowski J, Fauvell D, Cimino D, Caplan S. A pilot study analyzing the effects of Chinese cupping as an adjunct treatment for patients with subacute low back pain on relieving pain, improving range of motion, and improving function. J Altern Complement Med. (2014) ; 20: (2): 113-7. |
[36] | Cui XJ. Terminology. Journal of Acupuncture and Tuina Science. (2003) ; 1: : 63. |
[37] | Jacob T, Hutzler Y. Sports-medical assessment for athletes with a disability. Disability and Rehabilitation. (1998) ; 20: (3): 116-9. |
[38] | Jackson DL, et al. Electrodiagnostic study of carpal tunnel syndrome in wheelchair basketball players. Clinical Journal of Sport Medicine. (1996) ; 6: (1): 27-31. |
[39] | Mauerberg-deCastro E, Campbell DF, Tavares CP. The global reality of the Paralympic Movement: Challenges and opportunities in disability sports. Motriz: Revista de Educação Física. (2016) ; 22: (3): 111-123. |
[40] | Sucher BM. Suction decompression of the carpal tunnel. J Am Osteopath Assoc. (2019) ; 119: (7): 464-468. |
[41] | Warren BL. Plantar fasciitis in runners treatment and prevention. Spons Medicine. (1990) ; 10: (5): 338-345. |
[42] | Petraglia F, Ramazzina L, Costantino C. Plantar fasciitis in athletes: Diagnostic and treatment strategies. A systematic review. Muscles, Ligaments and Tendons Journal. (2017) ; 7: (1): 107-118. |
[43] | Lopes AD, et al. What are the main running-related musculoskeletal injuries? A systematic review. Sports Medicine. (2012) ; 42: (10): 891-905. |
[44] | Thompson JV, et al. Diagnosis and management of plantar fasciitis. J Am Osteopath Assoc. (2014) ; 114: (12): 900-6. |
[45] | Martinelli N, Bonifacini C, Romeo G. Current therapeutic approaches for plantar fasciitis. Orthopedic Research and Reviews. (2014) . |
[46] | Escaloni J, Young I, Loss J. Cupping with neural glides for the management of peripheral neuropathic plantar foot pain: A case study. J Man Manip Ther. (2019) ; 27: (1): 54-61. |
[47] | Gleim GW, McHugh MP. Flexibility and its effects on sports injury and performance. Sports Medicine. (1997) ; 24: (5): 289-299. |
[48] | Williams PE and G. G. Connective tissue changes in immobilised muscle. Journal of Anatomy. (1984) ; 138: (2): 343-350. |
[49] | Delaloye JR, et al. How to rapidly abolish knee extension deficit after injury or surgery: A practice-changing video pearl from the scientific anterior cruciate ligament network international (SANTI) study group. Arthrosc Tech. (2018) ; 7: (6): e601-e605. |
[50] | Williams JG, et al. The effects of cupping on hamstring flexibility in collegiate soccer players. Journal of Sport Rehabilitation. (2017) ; 28: (4): 1-44. |
[51] | Musial F, Spohn D, Rolke R. Naturopathic reflex therapies for the treatment of chronic back and neck pain – Part 1: Neurobiological foundations. Forsch Komplementmed. (2013) ; 20: (3): 219-24. |
[52] | Lauche R, et al. Efficacy of cupping therapy in patients with the fibromyalgia syndrome-a randomised placebo controlled trial. Sci Rep. (2016) ; 6: : 37316. |
[53] | Hauser W, et al. Fibromyalgia. Nat Rev Dis Primers. (2015) ; 1: : 15022. |
[54] | Bradley LA. Pathophysiology of fibromyalgia. Am J Med. (2009) ; 122: (12 Suppl): S22-30. |
[55] | Carli G, et al. Reactivity to superficial and deep stimuli in patients with chronic musculoskeletal pain. Pain. (2002) ; 100: : 259-269. |
[56] | Inanici F, et al. The frequency of fibromyalgia in sport professionals. Rheumatol Int. (2011) ; 31: (8): 1121-2. |
[57] | Al-Bedah AMN, et al. The medical perspective of cupping therapy: Effects and mechanisms of action. J Tradit Complement Med. (2019) ; 9: (2): 90-97. |
[58] | Basbaum AI, et al. Cellular and molecular mechanisms of pain. Cell. (2009) ; 139: (2): 267-84. |
[59] | Bridgett R, et al. Effects of cupping therapy in amateur and professional athletes: Systematic review of randomized controlled trials. J Altern Complement Med. (2018) ; 24: (3): 208-219. |
[60] | Wang YL, et al. Cupping therapy for knee osteoarthritis: A synthesis of evidence. Complement Med Res. (2018) ; 25: (4): 249-255. |
[61] | Driban JB, et al. Is participation in certain sports associated with knee osteoarthritis? A systematic review. J Athl Train. (2017) ; 52: (6): 497-506. |
[62] | Bullock GS, et al. Playing sport injured is associated with osteoarthritis, joint pain and worse health-related quality of life: A cross-sectional study. BMC Musculoskelet Disord. (2020) ; 21: (1): 111. |
[63] | Sajid MI. Hijama therapy (wet cupping) – its potential use to complement British healthcare in practice, understanding, evidence and regulation. Complement Ther Clin Pract. (2016) ; 23: : 9-13. |
[64] | Yoo SS, Tausk F. Cupping: East meets west. International Journal of Dermatology. (2004) ; 43: : 664-665. |
[65] | Lireza Ahmadi DCSaMR. The efficacy of wet-cupping in the treatment of tension and migraine headache. The American Journal of Chinese Medicine. (2008) ; 36: (1): 37-44. |
[66] | Dons’koi BV, et al. Repeated cupping manipulation temporary decreases natural killer lymphocyte frequency, activity and cytotoxicity. Journal of Integrative Medicine. (2016) ; 14: (3): 197-202. |
[67] | Tagila SM, et al. Wet-cupping removes oxidants and decreases oxidative stress. Complementary Therapies in Medicine. (2014) ; 22: : 1032-1036. |
[68] | Mohamed AA. Can proprioceptive training reduce muscle fatigue in patients with motor neuron diseases? A new direction of treatment. Front Physiol. (2019) ; 10: : 1243. |
[69] | Mohamed AA. Can proprioceptive training enhance fatigability and decrease progression rate of sarcopenia in seniors? A novel approach. Curr Rheumatol Rev. (2021) ; 17: (1): 58-67. |
[70] | Theofilidis G, et al. Monitoring exercise-induced muscle fatigue and adaptations: Making sense of popular or emerging indices and biomarkers. Sports (Basel). (2018) ; 6: (4). |
[71] | Debold EP. Potential molecular mechanisms underlying muscle fatigue mediated by reactive oxygen and nitrogen species. Front Physiol. (2015) ; 6: : 239. |
[72] | Enoka RM, Duchateau J. Muscle fatigue: What, why and how it influences muscle function. J Physiol. (2008) ; 586: (1): 11-23. |
[73] | Westerblad H, L. J, Lännergren J, Allen DG. JCellular mechanisms of fatigue in skeletal muscle. American Journal of Physiology. (1991) ; 261: (2 Pt 1): C195-209. |
[74] | Cooke R. Modulation of the actomyosin interaction during fatigue of skeletal muscle. Muscle Nerve. (2007) ; 36: (6): 756-77. |
[75] | Allen DG. Fatigue in working muscles. J Appl Physiol. (2009) ; 106: (2): 358-9. |
[76] | Li T, et al. Significant and sustaining elevation of blood oxygen induced by Chinese cupping therapy as assessed by near-infrared spectroscopy. Biomed Opt Express. (2017) ; 8: (1): 223-229. |
[77] | Hepple RT. The Role of O2 Supply in Muscle Fatigue. Canadian Journal of Applied Physiology. (2002) ; 27: (1): 56-69. |
[78] | Kenzo K, J. W, Tsuyoshi K. Clinical Therapeutic Applications of the Kinesio Taping Method. 2003, Tokyo, Japan: Ken Ikai Co Ltd. |
[79] | Cheung K, Hume PA, Maxwell L. Delayed onset muscle soreness treatment strategies and performance factors. Sports Medicine. (2003) ; 2: (33): 145-164. |
[80] | Poddonones DJ, Q.B. M. Effect of cryotherapy on muscle soreness and strength following eccentric exercise. International Journal of Sports Medicine. (1997) ; 18: (8): 588-593. |
[81] | Hotfiel T, et al. Advances in Delayed-Onset Muscle Soreness (DOMS): Part I: Pathogenesis and Diagnostics. Sportverletz Sportschaden. (2018) ; 32: (4): 243-250. |
[82] | Williams JG, et al. The effects of cupping on hamstring flexibility in college soccer players. J Sport Rehabil. (2017) ; 28: (4): 350-353. |


