
Reliability of cervical vertebral maturation compared to hand-wrist for skeletal maturation assessment in growing subjects: A systematic review
Abstract
BACKGROUND:
Radiographic methods to assess skeletal maturity (SM) have a key role in adolescent idiopathic scoliosis (AIS) management, allowing to predict risk of spinal curve progression. Cervical vertebral maturation (CVM) has been recently introduced as an alternative tool to assess skeletal maturity; however, its clinical role is still debated.
OBJECTIVE:
This systematic review aimed to investigate the reliability of CVM in the SM assessment of growing subjects, comparing it to hand wrist maturation (HVM).
METHODS:
PubMed, Scopus, and Web of Science databases were systematically searched from inception until 31
RESULTS:
Out of 205 papers, 12 papers were included in the data synthesis. We classified 10 studies (83.3%) as medium-quality studies and 2 studies (16.7%) as high-quality studies. Eight studies reported a significant correlation between CVM Baccetti and different HWM methods.
CONCLUSION:
Taken together, these findings suggested that CVM might be considered as reliable SM assessment method compared to HWM in growing subjects. However, further studies are warranted to confirm these findings.
1.Introduction
Skeletal maturation (SM) is a physiological sequence of body changes characterized by phenomenon in which timing could vary among growing subjects due to a different biologic clock [1]. As a consequence, both somatic maturity and chronological age have been considered as poor indicators of SM, given the wide variation in the onset of pubertal growth spurt (PGS) [2, 3].
The SM assessment is routinely used in the clinical practice of physical and rehabilitation medicine (PRM), orthopedics, pediatrics, and orthodontics to plan an adequate treatment in growing subjects [4, 5, 6]. In this context, SM assessment plays a key role in adolescent idiopathic scoliosis (AIS) management, where an optimal evaluation of skeletal discrepancies may allow PRM physicians to assess the risk of curve progression [7], which might lead to a better postural assessment and consequently to an adequate rehabilitation plan [8]. To date, it has been shown that during the PGS, an increase of scoliosis curvature is exponentially correlated with a severe risk of progression [9].
Furthermore, the spinal curve seems to progress more during the first 2 year of puberty, with several implication on therapeutic management [9, 10, 11, 12]. The overdiagnosis and overtreatment of scoliosis have been considered as rising problems in recent years, taking into account that there is still no agreement in the literature on the effectiveness of bracing or exercise on the curvature progression in adolescents [13]. However, a Cobb’s angle of 20
In this scenario, the gold standard for assessing SM is the hand wrist maturation (HWM), a method that needs an extra hand and wrist X-ray [18, 19, 20, 21, 22, 23, 24, 25]. However, this technique has several limitations, from additional radiation exposure to burden in terms of sanitary costs related to the additional X-rays [26]. Thus, starting from the spine X-ray, among the other SM assessments proposed to overcome this problem, cervical vertebral maturation (CVM) has been started to be frequently used in the common clinical practice [27, 28, 29].
In 1972, Lamparski [27] introduced the CVM as a novel SM evaluation method, that was firstly revised by Hassel and Farman [28], which improved the evaluation of the visible lateral profiles of the second, third and fourth cervical vertebrae, and secondly by Baccetti et al. [29], assessing the shape of the inferior border of C2, C3, and C4, thus providing different CVM stages (CVMS). However, to date, there is no agreement on the correlation among CVMS, HWM stages and the PGS.
The overall growth velocity is related to SM, which might be determined by hand and wrist X-ray evaluation using methods based on both relative growth velocity and percentage of residual growth remaining, instead of using methods aimed at determining the skeletal age [30]. Thus, SM assessment should be widely used in clinical practice by PRM physicians and orthodontists. However, albeit chronological age could not be considered as a valid predictor of skeletal growth velocity, skeletal age and SM are often wrongly not distinguished in the literature [31, 32, 33]. Furthermore, findings of CVM reliability compared to HWM are still controversial in growing subjects [31, 32, 33]. In particular, Santiago et al. [31] did not consider CVM method as appropriate for the SM assessment; conversely, Cericato et al. [32] and Szemraj et al. [33] have more recently reported that CVM might be considered as reliable to evaluate SM, although CVM Hassel and Farman method was not investigated [33].
To date, although CVM is a technique commonly used in the clinical practice, there is still a lack of knowledge on its usefulness in assessing SM in growing subjects to have indications useful for the rehabilitative management of AIS. Therefore, the present systematic review aimed to evaluate the available scientific literature on the reliability of CVM methods compared to HWM methods to assess SM in growing subjects.
2.Materials and msethods
2.1Search strategy
PubMed, Scopus, and Web of Science databases were systematically searched from inception until 31
Table 1
Search strategy for the present systematic review
| PubMed (“hand-wrist”) AND (“cervical vertebral maturation” OR “vertebra” OR “vertebral” OR “cervical vertebral”) AND (“skeletal maturation” OR “maturation” OR “skeletal maturity” OR “maturity” OR “growth peak” OR “growth spurt” OR “pubertal growth peak” OR “pubertal growth spurt” OR “ossification”) AND (“pubertal stage” OR “growing age” OR “pubertal” OR “growth” OR “children” OR “adolescents”) |
| Scopus TITLE-ABS-KEY((“hand-wrist”) AND (“cervical vertebral maturation” OR “vertebra” OR “vertebral” OR “cervical vertebral”) AND (“skeletal maturation” OR “maturation” OR “skeletal maturity” OR “maturity” OR “growth peak” OR “growth spurt” OR “pubertal growth peak” OR “pubertal growth spurt” OR “ossification”) AND (“pubertal stage” OR “growing age” OR “pubertal” OR “growth” OR “children” OR “adolescents”)) |
| Web of Science TS |
This systematic review has been performed in accordance with the PRISMA statement [34] and has been registered on PROSPERO with registration number CRD42020220867.
2.2Selection criteria
Two reviewers (MF, CC) independently screened all potential articles for eligibility after duplication removal. Any disagreement has been resolved through discussion or, if necessary, by a consultation of a third reviewer (AdS).
All observational studies were assessed for eligibility according to the following PICO model:
1. P) Participants consisted of growing subjects;
2. I) Intervention consisted of CVM methods commonly used in the clinical practice for the SM assessment;
3. C) Comparator consisted of HVM methods commonly used in the clinical practice for the SM assessment;
4. O) Outcome measure consisted of the reliability of CVM compared to HWM for the SM assessment.
We included observational cross-sectional studies, written in English language, and available in full text. We excluded studies investigating chronological, skeletal or dental age as primary outcomes, book chapters, posters, conference abstracts, and studies involving animals.
2.3Data extraction
Data extraction was performed by two reviewers independently (MF, CC), assessing eligible full-text papers through a customized data extraction form in Microsoft Excel. Key data were extracted from each study relevant to the specific research questions. We resolved disagreement by a consensus or by the decision of a further experienced reviewer (AdS).
The following data were extracted: 1) authors; 2) scientific journal; 3) publication year; 4) Nationality of study participants; 5) population and number of patients; 6) age of subjects; 7) SM and CVM assessment methods; 8) HWM method; 9) main findings.
2.4Data synthesis
Each selected study has been synthetized describing both extracted data and studies’ characteristics. Then, the study quality was assessed by a 10-item quality scoring adapted by Santiago et al. [31]. The 10 criteria for the quality scoring of the studies included were the following ones: 1. Adequate presentation of study objective; 2. Adequate presentation of study design; 3. Clear description of eligibility criteria of study population; 4. Adequate presentation of methods of assessment; 5. Sample size calculation; 6. Presentation of demographic characteristics of the study population; 7. Adequate reliability assessment; 8. Appropriate statistical analysis; 9. Adequate reporting of results with tables and/or figures; 10. Declared p-values in the results. All of them could be scored as 0 (absence of the criterion) to 1 (presence of the criterion).
Accordingly, two reviewers independently (MF, AdS) provided all studies with a score for the 10 assessment criteria. In case of disagreement, a consensus was achieved involving a further experienced reviewer in the decisional process (MM). Therefore, the studies included were classified as low-quality studies (0–4 points), medium-quality studies (5–7 points) or high-quality studies (8–10 points).
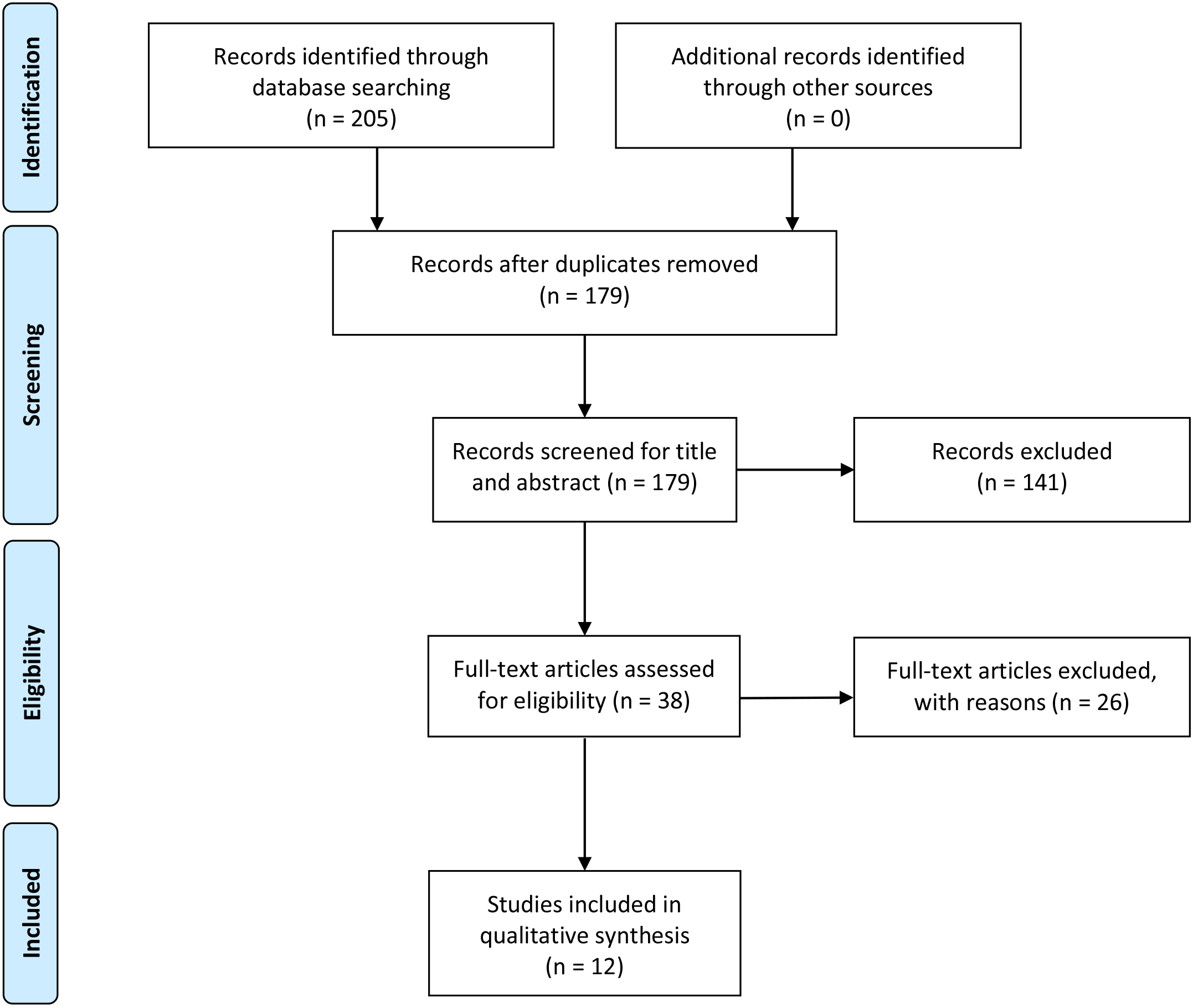
Figure 1.
PRISMA flow diagram.
3.Results
Out of 205 search results, 26 duplicates were removed, and 179 studies were considered as eligible for inclusion and screened for title and abstract. Out of these, we included 38 papers for full-text screening. After the exclusion of 26 articles (25 not respecting eligibility criteria and 1 simultaneously published in two different scientific journals), 12 papers [35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46] were included in the synthesis (see Fig. 1 for the PRISMA flow diagram and Table 2 for further details on the exclusion reasons of 167 articles).
Table 2
Reasons for article exclusion by the present systematic review
|
Articles excluded after title and abstract screening phase ( | |
|---|---|
| Not population of interest | 14 (9.9%) |
| Not intervention of interest | 37 (26.2%) |
| Not comparison of interest | 29 (20.6%) |
| Not outcome of interest | 79 (56.0%) |
|
Articles excluded after full-text screening phase ( | |
| Not population of interest | 2 (7.7%) |
| Not intervention of interest | 3 (11.5%) |
| Not comparison of interest | 2 (7.7%) |
| Not outcome of interest | 13 (50.0%) |
| Full-text unavailability | 2 (7.7%) |
| Full-text in a language different than English | 3 (11.5%) |
| Simultaneous publication in two scientific Journals | 1 (3.9%) |
The exclusion of the articles followed the PICO model defined in the Methods Section. Data are expressed as counts (percentages).
The studies included in the present systematic review [35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46] have been published in the last 19 years (from 2002 to 2017). Most of them (58.3%) were performed in Asia (2 in India [40, 46], 2 in Turkey [39, 45], 1 in Iran [38], 1 in Hong Kong [41], 1 in Qatar [43]), 4 (33.3%) in Europe (2 in Spain [37], 1 in Italy [36], 1 in Poland [35]), and 1 study (8.3%) from Canada [42].
Considering the study population, all 12 studies [35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46] assessed patients of both sexes, although Pichai et al. [40] did not specify the exact number of males and females included. Study cohorts ranged from 30 [35, 36, 37] to 958 [44] subjects, while age of study participants widely varied from 5 [44, 45] to 24 [45] years old; information on subjects age was missing in the study of Flores-Mir et al. [42].
Two studies [37, 40] assessed more than one SM method and were described in detail, accordingly.
Pichai et al. [40] evaluated CVM Baccetti [29] vs HWM Grave and Brown [23] and CVM Hassel and Farman [28] vs HWM Grave and Brown [23]; Camacho-Basallo et al. [37] evaluated CVM methods compared to different HWM methods: CVM Baccetti [29] vs HWM Grave and Brown [23]; CVM Baccetti [29] vs HWM Fishman [21]; CVM Hassel and Farman [28] vs HWM Grave and Brown [23]; CVM Hassel and Farman [28] vs HWM Fishman [21].
In particular, 10 studies evaluated CVM Baccetti [29], compared with different HWM methods: Bjork [35, 36], HWM Grave and Brown [37, 38, 39, 40], HWM Fishman [37, 41, 42] and HWM Hägg and Taranger [43]. Six papers evaluated CVM with Hassel and Farman, comparing it with HWM Grave and Brown [37, 40, 44, 45] and HWM Fishman [37, 46].
Table 3
Quality assessment of the studies included in the present systematic review
| Articles | Criteria for the quality scoring | Score | Quality level | |||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |||
| Durka-Zaja̧c et al. [5] | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 6 | Medium quality |
| Gandini et al. [36] | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 5 | Medium quality |
| Camacho-Basallo et al. [37] | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 7 | Medium quality |
| Hoseini et al. [38] | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 6 | Medium quality |
| Litsas et al. [39] | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | Medium quality |
| Pichai et al. [40] | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 | Medium quality |
| Alkhal et al. [41] | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 5 | Medium quality |
| Flores-Mir et al. [42] | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 | Medium quality |
| Wong et al. [43] | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 5 | Medium quality |
| San Roman et al. [44] | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 8 | High quality |
| Uysal et al. [45] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 | High quality |
| Mahajan et al. [46] | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 6 | Medium quality |
Criteria for the quality scoring of the studies included: 1. Adequate presentation of study objective; 2. Adequate presentation of study design; 3. Clear description of eligibility criteria of study population; 4. Adequate presentation of methods of assessment; 5. Sample size calculation; 6. Presentation of demographic characteristics of the study population; 7. Adequate reliability assessment; 8. Appropriate statistical analysis; 9. Adequate reporting of results with tables and/or figures; 10. Declared
According to the abovementioned 10-item quality scoring for the studies included, 2 studies (16.7%) were classified as high-quality studies [44, 45] and 10 studies (83.3%) as medium-quality studies [35, 36, 37, 38, 39, 40, 41, 42, 43, 46]. No low-quality studies were included in the present systematic review (see Table 3 for further details on quality scoring for each assessment criteria). A meta-analysis could not be performed due to the high clinical heterogeneity of the studies included in terms of variability in both SM assessment and study participants characteristics [47]. The main characteristics of the 12 articles included [35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46] are described in detail in Table 4 and in the following paragraphs.
3.1CVM methods vs HWM methods
3.1.1CVM Baccetti vs HWM Bjork
Two papers [35, 36] compared the CVM Baccetti method [29] with HWM Björk method [20], both show ing consistent results: Durka-Zaja̧c et al. [35] reported a strong statistically significant Pearson’s correlation between the two methods in both sexes (
3.1.2CVM Baccetti vs HWM grave and brown
Four papers [37, 38, 39, 40] compared the CVM Baccetti method [29] with HWM Grave and Brown method [23]; however, there was no agreement on the correlation between the two methods. In particular, Camacho-Basallo et al. [37] showed no significant correlation (
3.1.3CVM Baccetti vs HWM fishman
Three papers [37, 41, 42] compared the CVM Baccetti method [29] with HWM Fishman method [21] showing a significant correlation (
Table 4
Main characteristics of the articles included in the present systematic review
| Authors | Journal | Publication year | Nationality | Population (M/F) | Age (years) | CVM assessment methods | HWM assessment method | Main findings |
|---|---|---|---|---|---|---|---|---|
| Durka-Zaka̧c et al. [35] | Pol J Radiol | 2013 | Poland | 30 (15 M/15 F) | 10-17 | Baccetti [29] | Björk [20] | There was a strong and statistically highly significant ( |
| Gandini et al. [36] | Angle Orthod | 2006 | Italy | 30 (14 M/16 F) | 7–18 | Baccetti [29] | Björk [20] | The authors reduced the stages of growth to five intervals (A–E) to relate the five stages of the CVM Baccetti method to the nine stages of a Björk HVM method. Cohen kappa test index showed a good concordance value (0.783 |
| Camacho-Basallo et al. [37] | Acta Odontol Scand | 2017 | Spain | 202 (104 M/98 F) | 11–14 | Baccetti [29] | Grave and Brown [23] | No significant correlation was found between CVM Baccetti method and HWM Grave and Brown method (CC |
| Hoseini et al. [38] | Iran J Radiol | 2016 | Iran | 133 (67 M/66 F) | 8–18 | Baccetti [29] | Grave and Brown [23] | The authors reduced the stages of growth to five intervals (A–E) to relate the five stages of the CVM Baccetti method to the nine stages of a Björk HVM method. Cohen kappa test revealed a low level of agreement between the two methods (0.312), slightly higher in males (0.33) than in females (0.27) between the stages. |
| Litsas et al. [39] | Eur J Paediatr Dent | 2010 | Turkey | 393 (170 M/223 F) | 8–18 | Baccetti [29] | Grave and Brown [23] | CVM and HVM stages, as well as a 3-stage classification (prepeak/peak/post-peak) are significantly associated in both females (Chi square |
|
Table 4, continued | ||||||||
|---|---|---|---|---|---|---|---|---|
| Authors | Journal | Publication year | Nationality | Population (M/F) | Age (years) | CVM assessment methods | HWM assessment method | Main findings |
| Pichai et al. [40] | J Int Oral Health | 2014 | India | 72 M+F | 7–16 | Baccetti [29] | Grave and Brown [23] | There was a significant correlation between CVM Baccetti method and HWM Grave and Brown method (Kappa |
| Camacho-Basallo et al. [37] | Acta Odontol Scand | 2017 | Spain | 202 (104 M/98 F) | 11–14 | Baccetti [29] | Fishman [21] | CVM Baccetti method was significantly correlated with HVM Fishman method (CC |
| Alkhal et al. [41] | Angle Orthod | 2008 | Hong Kong | 400 (200 M/200 F) | 10–17 | Baccetti [29] | Fishman [21] | The authors found a good correlation between CVM and HWM methods, with a linear relationship between the CVM and the HWM in both male and female. CVM resulted significantly correlated with HWM (Spearman’s r: males |
| Flores-Mir et al. [42] | Angle Orthod | 2006 | Canada | 79 (27 M/52 F) | N/A | Baccetti [29] | Fishman [21] | CVM Baccetti method and HWM Fishman method are significantly correlated ( |
| Wong et al. [43] | Am J Orthod Dentofacial Orthop | 2009 | Qatar | 400 (200 M/200 F) | 10–17 | Baccetti [29] | Hägg and Taranger [2] | A linear relationship was found between the CVM Baccetti method and the HWM Hägg and Taranger in both female (Spearman r: 0.9408) and male (Spearman r: 0.9521). In all subjects investigated, the CVMS3 subjects corresponded mainly to the MP3-FG stage (35 male, 21 female), and a few to the MP3-G stage (1 male, 2 female) in the HWM, that were around the PGS. |
| Camacho-Basallo et al. [37] | Acta Odontol Scand | 2017 | Spain | 202 (104 M/98 F) | 11–14 | Hassel and Farman [28] | Grave and Brown [23] | No significant correlation was found between CVM Hassel and Farman method and HWM Grave and Brown method (CC |
| Pichai et al. [40] | J Int Oral Health | 2014 | India | 72 M+F | 7–16 | Hassel and Farman [28] | Grave and Brown [23] | There was a significant correlation between CVM Hassel and Farman method and HWM Grave and Brown method (Kappa |
| San Roman et al. [44] | Eur J Orthod | 2002 | Spain | 958 (428 M/530 F) | 5–18 | Hassel and Farman [28] | Grave and Brown [23] | There was a good correlation between CVM Hassel and Farman method and HWM Grave and Brown method for SM in females and males ( |
|
Table 4, continued | ||||||||
|---|---|---|---|---|---|---|---|---|
| Authors | Journal | Publication year | Nationality | Population (M/F) | Age (years) | CVM assessment methods | HWM assessment method | Main findings |
| Uysal et al. [45] | Am J Orthod Dentofacial Orthop | 2006 | Turkey | 503 (213 M/290 F) | 5–24 | Hassel and Farman [28] | Grave and Brown [23] | CVM Hassel and Farman method was significantly correlated (p<0.001) with HWM Grave and Brown method, with a Spearman rank-order correlation coefficient of 0.86 (sexes combined); the coefficients for male and female were 0.78 ( |
| Camacho-Basallo et al. [37] | Acta Odontol Scand | 2017 | Spain | 202 (104 M/98 F) | 11–14 | Hassel and Farman [28] | Fishman [21] | CVM Hassel and Farman method was significantly correlated with HWM Fishman method (CC |
| Mahajan et al. [46] | Indian J Dent Res | 2011 | India | 100 (50 M/50 F) | 8–18 | Hassel and Farman [28] | Fishman [21] | CVM Hassel and Farman method was significantly correlated with HWM Fishman method (CC |
Abbreviations: CC
et al. [37] reported a correlation coefficient (CC)
3.1.4CVM Baccetti vs HWM Hägg and Taranger
Only one paper, performed by Wong et al. [43], compared the CVM Baccetti method [29] with HWM Hägg and Taranger method [2] showing a linear relationship between them in both male (Spearman
3.1.5CVM Hassel and Farman vs HWM Grave and Brown
Four papers [37, 40, 44, 45] compared the CVM Hassel and Farman method [28] with HWM Grave and Brown method [23], reporting different findings: Camacho-Basallo et al. [37] reported no significant correlation between the two methods (CC
4.Discussion
SM assessment is a cornerstone in terms of diagnosis, treatment planning, and monitoring treatments in the PRM clinical practice, including patients affected by AIS, playing a key role to guide physicians in the initiation of bracing, timing and hours of brace wear, and eventually its dismission [3, 4, 5, 6, 15, 48, 49]. In this scenario, CVM has been proposed in evaluating the spinal maturity in scoliosis patients representing a tool able to predict spinal growth and curve progression [50, 51]. Overall, the present systematic review summarized the level of evidence behind the reliability of CVM, showing significant correlations between these methods compared to HVM in terms of SM assessment in growing subjects.
Interestingly, all papers included might be considered as at least medium-quality studies, according to the abovementioned 10-item quality scoring [31]. However, there were only two high-quality studies [44, 45] on the topic investigated and both of them have been published more than 15 years ago: San Román et al. in 2002 [44] and by Uysal et al. in 2006 [45]. These findings testified that further studies with a high-level methodology are warranted for assessing the reliability of CVM compared to HWM to assess SM in growing subjects.
At present, there are only three systematic reviews in literature investigating the reliability of CVM compared to HVM [31, 32, 33]. However, Szemraj et al. [33] included only articles investigating CVM Baccetti method [29] as intervention, not providing findings on CVM Hassel and Farman method [28], that is widely used in the common clinical practice and even highly investigated, as shown by this systematic review that included 5 papers comparing the CVM Hassel and Farman method to HWM methods [37, 40, 44, 45, 46].
Furthermore, the three above-mentioned systematic reviews [31, 32, 33] did not distinguish skeletal age and skeletal maturation, albeit it is well known that chronological age is not a valid predictor of skeletal growth velocity [30]. On the other hand, we assessed the reliability of CVM compared to HWM to assess SM in growing subjects, taking into account the absence of a common agreement on the reliability of CVM in literature.
Indeed, Santiago et al. [31] concluded that the CVM was not appropriate for the SM assessment, underlining the low-quality evidence of the papers included. On the other hand, the systematic reviews performed by Cericato et al. [32] and Szemraj et al. [33] reported a high level of correlation between CVM and HWM, concluding that CVM was reliable to evaluate SM and might replace HWM in the next future in the common clinical practice.
Findings highlighted by the present systematic review are in agreement with the last two systematic reviews [32, 33]. We showed that 8 studies [35, 36, 37, 39, 40, 41, 42, 43] showed a high correlation between CVM Baccetti and different HWM methods, and 5 studies [37, 40, 44, 45, 46], comparing CVM Hassel and Farman with different HWM methods, highlighted a significant correlation between these different techniques. However, we should report that 3 studies showed no significant correlation between CVM methods and HWM Grave and Brown: two [37, 38] assessing CVM Baccetti and one [37] evaluating CVM Hassel and Farman.
Moreover, compared to the aforementioned systematic reviews [31, 32, 33], we found a few differences in terms of correlation between CVM and HWM methods. This aspect might be due to the well-known difference in the PGS onset between male and females [1], which has not been adequately assessed by 7 papers included [35, 36, 37, 38, 40, 44, 46]. In this context, Wong et al. [43], considering the crucial difference in the onset of the circumpubertal periods between sexes, stratified their analysis using different age ranges (female: 10–15 years; male: 12–17 years), showing a highly significant correlation between CVM and HWM (Spearman r was 0.9408 in male and 0.9521 in female). Furthermore, it should be noted that CVM showed a low sensitivity for SM assessment in subjects away from the circumpubertal period [43]. This aspect is poorly considered in literature and could generate a major bias (e.g. Uysal et al. [45] included subjects aged from 5 to 24 years).
Furthermore, it was interesting to highlight the findings reported by Litsas et al. [39] suggesting the importance that the gender differentiation might play during the circumpubertal period. The Authors showed that CVMS I and II belong to pre-peak period and CVMS III to the peak period in male; at the same time, the Authors showed that CVMS I belongs to the pre-peak period and CVMS II and III to the peak period in female. CVMS IV and V represent the post-peak period in both sexes.
Taken together, these findings reported that CVM has a significant reliability in the SM assessment and might be considered a valid alternative to HWM in providing an adequate assessment of the growth curve progression. Indeed, in 2020, Zhang et al. [51] firstly showed that CVM could be used as an alternative to Risser sign in determining peak height velocity, reporting a strong correlation between CVM stages and the Risser sign (
Nevertheless, the present systematic review could not be considered as free from limitations: first of all, the high clinical heterogeneity of the studies included in terms of variability in both study population characteristics and the SM assessment methods used that did not consent to perform a meta-analysis; moreover, all papers included had a cross-sectional design that hinders to obtain data on growth analysis; lastly, the literature screening has been limited to articles published in English language, albeit a comprehensive search of the literature was performed. However, the present systematic review firstly evaluated the reliability of CVM methods (both Baccetti and Hassel and Farman) compared to HWM methods to assess the only skeletal maturation (not the skeletal age) in growing subjects, based on the data of studies searched in the main scientific databases from inception until 31st December 2020.
5.Conclusions
Taken together, the findings of this systematic review demonstrated that both CVM Baccetti and Hassel and Farman methods might be considered reliable SM assessment methods compared to HWM in growing subjects. However, further studies with a Level of Evidence 2 according to the OCEBM 2011 [56] are warranted to elucidate the role of CVM in SM assessment, which is a crucial indicator for physicians to plan an appropriate management of AIS in the PRM clinical practice.
Conflict of interest
None of the authors declare any conflict of interests, funding sources or consultant relationships with any organizations involved in this research.
Author contributions
Study design and conceptualization: MF and AdS.
Databases search: AdS.
Data screening: MF, CC, AdS.
Data extraction: MF, CC, AdS.
Data synthesis and interpretation: MF, MM, AdS.
Manuscript drafting: MF and AdS.
Critical revision: AR, MM, MI.
Study supervision: AdS.
Study submission: AdS. All authors read and approved the final version of the manuscript.
References
[1] | Sanders JO, Qiu X, Lu X, Duren DL, Liu RW, Dang D, et al. The Uniform Pattern of Growth and Skeletal Maturation during the Human Adolescent Growth Spurt. Sci Rep. (2017) ; 7: : 16705. |
[2] | Hägg U, Taranger J. Maturation indicators and the pubertal growth spurt. Am J Orthod. (1982) ; 82: : 299-309. |
[3] | Baccetti T, Franchi L, De Toffol L, Ghiozzi B, Cozza P. The diagnostic performance of chronologic age in the assessment of skeletal maturity. Prog Orthod. (2006) ; 7: : 176-188. |
[4] | Sanders JO, Khoury JG, Kishan S, Browne RH, Mooney JF 3rd, Arnold KD, et al. Predicting scoliosis progression from skeletal maturity: a simplified classification during adolescence. J Bone Joint Surg Am. (2008) ; 90: : 540-53. |
[5] | Luk KD, Saw LB, Grozman S, Cheung KM, Samartzis D. Assessment of skeletal maturity in scoliosis patients to determine clinical management: a new classification scheme using distal radius and ulna radiographs. Spine J. (2014) ; 14: : 315-325. |
[6] | Perinetti G. The Third Finger Middle Phalanx Maturation (MPM) Method to Assess Timing of Functional Treatment for Skeletal Class II Malocclusion: Report of Three Cases. Case Rep Dent. (2019) ; 8382612. |
[7] | Dimeglio A, Canavese F. Progression or not progression? How to deal with adolescent idiopathic scoliosis during puberty. J Child Orthop. (2013) Feb; 7: (1): 43-9. doi: 10.1007/s11832-012-0463-6. |
[8] | Bernetti A, Agostini F, Cacchio A, Santilli V, Ruiu P, Paolucci T, et al. Postural Evaluation in Sports and Sedentary Subjects by Rasterstereographic Back Shape Analysis. Appl. Sci. (2020) ; 10: : 8838. doi: 10.3390/app10248838. |
[9] | Charles YP, Dimeglio A, Canavese F, Daures JP. Skeletal age assessment from the olecranon for idiopathic scoliosis at Risser grade 0. J Bone Joint Surg Am. (2007) ; 89: : 2737-2744. |
[10] | Charles YP, Daures JP, de Rosa V, Dimeglio A. Progression risk of Idiopathic Juvenile scoliosis during pubertal growth. Spine. (2006) ; 31: : 1933-1942. |
[11] | Lonstein JE, Carlson JM. The prediction of curve progression in untreated idiopathic scoliosis during growth. J Bone Joint Surg Am. (1984) ; 66: : 1061-1071. |
[12] | Sansur CA, Smith JS, Coe JD, Glassman SD, Berven SH, Polly DW Jr, et al. Scoliosis research society morbidity and mortality of adult scoliosis surgery. Spine (Phila Pa 1976). (2011) ; 36: (9): E593. |
[13] | Dunn J, Henrikson NB, Morrison CC, Blasi PR, Nguyen M, Lin JS. Screening for Adolescent Idiopathic Scoliosis: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. (2018) ; 319: : 173-187. doi: 10.1001/jama.2017.11669. |
[14] | Płaszewski M, Grantham W, Jespersen E. Screening for scoliosis – New recommendations, old dilemmas, no straight solutions. World J Orthop. (2020) ; 11: (9): 364-379. doi: 10.5312/wjo.v11.i9.364. |
[15] | Negrini S, Dincer F, Kiekens C, Kruger L, Varela-Donoso E, Christodoulou N. Evidence based position paper on physical and rehabilitation medicine (PRM) practice for people with spinal deformities during growth. The European PRM position (UEMS PRM Section). Eur J Phys Rehabil Med. (2017) Feb; 53: (1): 125-131. doi: 10.23736/S1973-9087.16.04406-3. |
[16] | Scaturro D, de Sire A, Terrana P, Costantino C, Lauricella L, Sannasardo CE, et al. Adolescent idiopathic scoliosis screening: Could a school-based assessment protocol be useful for an early diagnosis? J Back Musculoskelet Rehabil. (2020) Nov 24. doi: 10.3233/BMR-200215. |
[17] | Lippi L, de Sire A, Desilvestri M, Baricich A, Barbanera A, Cattalani A, et al. Can scoliosis lead to spinal cord ischaemia? Early diagnosis and rehabilitation: A paradigmatic case report and literature review. J Back Musculoskelet Rehabil. (2021) ; 34: (1): 43-47. doi: 10.3233/BMR-200070. |
[18] | Greulich WS, Pyle SI. Radiographic Atlas of Skeletal Development of the Hand and Wrist. Stanford, CA: Stanford University Press, (2004) . |
[19] | Tanner JM, Whitehouse RH, Marshall WA. Assessment of Skeletal Maturity and Prediction of Adult Height: TW 2 Method. New York, NY: Academic Press, (1975) . |
[20] | Bjork A, Helm S. Prediction of the age of maximum pubertal growth in body height. Angle Orthod. (1967) ; 37: : 134-143. |
[21] | Fishman LS. Radiographic evaluation of skeletal maturation; a clinically oriented method based on hand wrist films. Angle Orthod. (1982) ; 52: : 88-112. |
[22] | Nanda R. The rates of growth of several facial components measured from serial cephalometric roentnograms. Am J Orthod. (1955) ; 41: : 658-673. |
[23] | Grave KC, Brown T. Skeletal ossification and the adolescent growth spurt. Am J Orthod. (1976) ; 69: : 611-619. |
[24] | So LL. Correlation of sexual maturation with skeletal age of southern Chinese girls. Aust Orthod J. (1997) ; 14: : 215-217. |
[25] | Beit P, Peltomäki T, Schätzle M, Signorelli L, Patcas R. Evaluating the agreement of skeletal age assessment based on hand-wrist and cervical vertebrae radiography. Am J Orthod Dentofacial Orthop. (2013) ; 144: : 838-847. |
[26] | Shim JJ, Bogowicz P, Heo G, Lagravere MO. Interrelationship and limitations of conventional radiographic assessments of skeletal maturation. Int Orthod. (2012) ; 10: : 135-147. |
[27] | Lamparski DG. Skeletal age assessment utilizing cervical vertebrae. Master Thesis, University of Pittsburgh, Pittsburgh, PA, (1972) . |
[28] | Hassel B, Farman AG. Skeletal maturation evaluation using cervical vertebrae. Am J Orthod Dentofacial Orthop. (1995) ; 107: : 58-66. |
[29] | Baccetti T, Franchi L, McNamara JA. The Cervical Vertebral Maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin Orthod. (2005) ; 11: : 119-129. |
[30] | Flores-Mir C, Nebbe B, Major PW. Use of skeletal maturation based on hand-wrist radiographic analysis as a predictor of facial growth: a systematic review. Angle Orthod. (2004) Feb; 74: (1): 118-24. doi: 10.1043/0003-3219(2004)074<0118:UOSMBO>2.0.CO;2. |
[31] | Santiago RC, de Miranda Costa LF, Vitral RW, Fraga MR, Bolognese AM, Maia LC. Cervical vertebral maturation as a biologic indicator of skeletal maturity. Angle Orthod. (2012) ; 82: : 1123-1131. |
[32] | Cericato GO, Bittencourt MA, Paranhos LR. Validity of the assessment method of skeletal maturation by cervical vertebrae: a systematic review and meta-analysis. Dentomaxillofac Radiol. (2015) ; 44: : 20140270. |
[33] | Szemraj A, Wojtaszek-Słomińska A, Racka-Pilszak B. Is the cervical vertebral maturation (CVM) method effective enough to replace the hand-wrist maturation (HWM) method in determining skeletal maturation-A? systematic review. Eur J Radiol. (2018) ; 102: : 125-128. |
[34] | Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. (2009) ; 339: : b2535. |
[35] | Durka-Zaja̧c M, Marcinkowska A, Mituś-Kenig M. Bone age assessment using cephalometric photographs. Pol J Radiol. (2013) ; 78: : 19-25. |
[36] | Gandini P, Mancini M, Andreani F. A comparison of hand-wrist bone and cervical vertebral analyses in measuring skeletal maturation. Angle Orthod. (2006) ; 76: : 984-989. |
[37] | Camacho-Basallo P, Yáñez-Vico RM, Solano-Reina E, Iglesias-Linares A. Five radiographic methods for assessing skeletal maturity in a Spanish population: is there a correlation? Acta Odontol Scand. (2017) ; 75: : 106-112. |
[38] | Hoseini M, Zamaheni S, Bashizadeh Fakhar H, Akbari F, Chalipa J, Rahmati A. Comparative Evaluation of the Efficacy of Hand-Wrist and Cervical Vertebrae Radiography for the Determination of Skeletal Age. Iran J Radiol. (2016) ; 13: : e21695. |
[39] | Litsas G, Ari-Demirkaya A. Growth indicators in orthodontic patients. Part 1: comparison of cervical vertebral maturation and hand-wrist skeletal maturation. Eur J Paediatr Dent. (2010) ; 11: : 171-175. |
[40] | Pichai S, Rajesh M, Reddy N, Adusumilli G, Reddy J, Joshi B. A comparison of hand wrist bone analysis with two different cervical vertebral analysis in measuring skeletal maturation. J Int Oral Health. (2014) ; 6: : 36-41. |
[41] | Alkhal HA, Wong RW, Rabie AB. Correlation between chronological age, cervical vertebral maturation and Fishman’s skeletal maturity indicators in southern Chinese. Angle Orthod. (2008) ; 78: : 591-596. |
[42] | Flores-Mir C, Burgess CA, Champney M, Jensen RJ, Pitcher MR, Major PW. Correlation of skeletal maturation stages determined by cervical vertebrae and hand-wrist evaluations. Angle Orthod, (2006) ; 76: : 1-5. |
[43] | Wong RW, Alkhal HA, Rabie AB. Use of cervical vertebral maturation to determine skeletal age. Am J Orthod Dentofacial Orthop, (2009) ; 136: : 484.E1-6. |
[44] | San Román P, Palma JC, Oteo MD, Nevado E. Skeletal maturation determined by cervical vertebrae development. Eur J Orthod. (2002) ; 24: : 303-311. |
[45] | Uysal T, Ramoglu SI, Basciftci FA, Sari Z. Chronologic age and skeletal maturation of the cervical vertebrae and hand-wrist: is there a relationship? Am J Orthod Dentofacial Orthop. (2006) ; 130: : 622-628. |
[46] | Mahajan S. Evaluation of skeletal maturation by comparing the hand wrist radiograph and cervical vertebrae as seen in lateral cephalogram. Indian J Dent Res. (2011) ; 22: : 309-316. |
[47] | Cochrane Handbook for Systematic Reviews of Interventions Version 6.1, 2020. Available on www.cochrane-handbook.org (accessed February, 7th 2021). |
[48] | Babaee T, Kamyab M, Ganjavian MS, Rouhani N, Jarvis J. Success Rate of Brace Treatment for Juvenile-Onset Idiopathic Scoliosis up to Skeletal Maturity. Int J Spine Surg. (2020) Oct; 14: (5): 824-831. doi: 10.14444/7117. |
[49] | Babaee T, Kamyab M, Ganjavian MS. Infantile Idiopathic Scoliosis: Outcomes of Brace Treatment until Skeletal Maturity or Spinal Fusion. Arch Bone Jt Surg. (2020) Nov; 8: (6): 696-702. doi: 10.22038/abjs.2020.44975.2253. |
[50] | Demirjian A, Goldstein H, Tanner JM. A new system of dental age assessment. Hum Biol. (1973) ; 45: : 211-227. |
[51] | Zhang Y, Shu S, Gu Q, Liu Z, Zhu Z, Qiu Y, Bao H. Cervical vertebral maturation (CVM) stage as a supplementary indicator for the assessment of peak height velocity (PHV) in adolescent idiopathic scoliosis (AIS). Quant Imaging Med Surg. (2020) Jan; 10: (1): 96-105. doi: 10.21037/qims.2019.11.07. |
[52] | Misterska E, Glowacki J, Kołban M. Does rigid spinal orthosis carry more psychosocial implications than the flexible brace in AIS patients? A cross-sectional study. J Back Musculoskelet Rehabil. (2019) ; 32: (1): 101-109. doi: 10.3233/BMR-181121. |
[53] | Bidari S, Kamyab M, Ahmadi A, Ganjavian MS. Effect of exercise on static balance and Cobb angle during the weaning phase of brace management in idiopathic scoliosis and hyperkyphosis: A preliminary study. J Back Musculoskelet Rehabil. (2019) ; 32: (4): 639-646. doi: 10.3233/BMR-181128. |
[54] | Kavyani M, Nasiri E, Karimi MT, Fatoye F. The effect of spinal bracing on stability in patients with adolescent idiopathic scoliosis. J Back Musculoskelet Rehabil. (2020) ; 33: (1): 139-143. doi: 10.3233/BMR-170908. |
[55] | Çolak TK, Akgül T, Çolak I, Dereli EE, Chodza M, Dikici F. Health related quality of life and perception of deformity in patients with adolescent idiopathic scoliosis. J Back Musculoskelet Rehabil. (2017) ; 30: (3): 597-602. doi: 10.3233/BMR-160564. |
[56] | OCEBM Levels of Evidence – Centre for Evidence-Based Medicine, University of Oxford. Available on https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence. (accessed February, 7th; 2021). |


