
The influence of gestational trimester, physical activity practice and weight gain on the low back and pelvic pain intensity in low risk pregnant women
Abstract
BACKGROUND:
Low back and pelvic pain in pregnant women is a clinical condition of which the etiology is multifactorial. Thus, various variables can influence the low back and pelvic pain’s intensity.
OBJECTIVE:
The purpose of this study was to analyze the influence of the gestational trimester, practice of physical activity and weight gain on the intensity of low back and pelvic pain in low risk pregnant women.
METHODS:
Two hundred and sixty-seven pregnant women participated in this study. The gestational age, body mass index, weight gain, physical activity practice and the low back and pelvic pain were evaluated.
RESULTS:
We found a significant difference (
CONCLUSIONS:
Sedentary pregnant women have 30% more chances to have higher pain intensities when compared to the active women, regardless of the gestational trimester and weight gain.
1.Introduction
Low back and pelvic pain (LBPP) are considered the main cause of incapacity in humans [1]. It is defined as a pain located between the ribs and the gluteus area which may irradiate to the lower limbs [2]. Low back and pelvic pain in pregnant women is an important clinical condition that must be considered, since it directly affects these women’s daily activities [3]. The etiology of LBPP is multifactorial and frequently linked to biomechanical, hormonal and vascular changes. In addition to these alterations, the age, economic status, previous pregnancies, body mass index (BMI), familial history of LBPP and history of hypermobility are some of the risk factors that may be associated with this pathology [4, 5].
Studies suggest that LBPP is reported by more than 50% of the pregnant women and the intensity of this pain increases with the gestation’s advance [4, 6, 7]. Despite the prevalence and severity of the symptoms, lots of pregnant women do not search treatment for LBPP, either because of the lack of knowledge about possible treatments or because they consider it a normal or unmanageable pathology [4]. On the other hand, the women who received physiotherapeutic treatment, through orientations about LBPP prevention and treatment, related a better quality of life in pregnancy [8].
Research also reveals the importance of prescribing exercises as a first-line treatment, in order to avoid the use of medication during pregnancy [4, 8]. However, a systematic review about the effect of exercises during and after pregnancy, written by Sd and Pennick in 2015 [9], showed that the results from the controlled and randomized clinical trials are small and not conclusive.
The result of the research has suggested that the weight gain during pregnancy, the advance of pregnancy and practice of physical activity, may influence the LBPP intensity [10, 11]. The lack of physical activity and weight gain are related to back pain. A sedentary lifestyle allied to a deficiency of the musculoskeletal system and a spine overload makes the population more prone to have low back and pelvic pain [12].
In this way, the study of the variables that may influence the low back and pelvic pain’s intensity is an important guiding point to the clinical practice, since it has been shown that this pain may persist throughout pregnancy and, often, during the post-partum [8, 13]. Therefore, the main aim of this study was to analyze the influence of the gestational trimester, practice of physical activity and weight gain on the intensity of low back and pelvic pain in low risk pregnant women.
2.Methods
This study was approved by the Ethics Committee for Research with Humans of Rio Grande do Norte Federal University (UFRN) under protocol number 719.939 e CAAE 30403414.8.0000.5537. All volunteers have signed the Free and Clarified Consent Term (FCCT).
2.1Participants and context
The sampling process was non-probabilistic. The volunteers were recruited, from 16
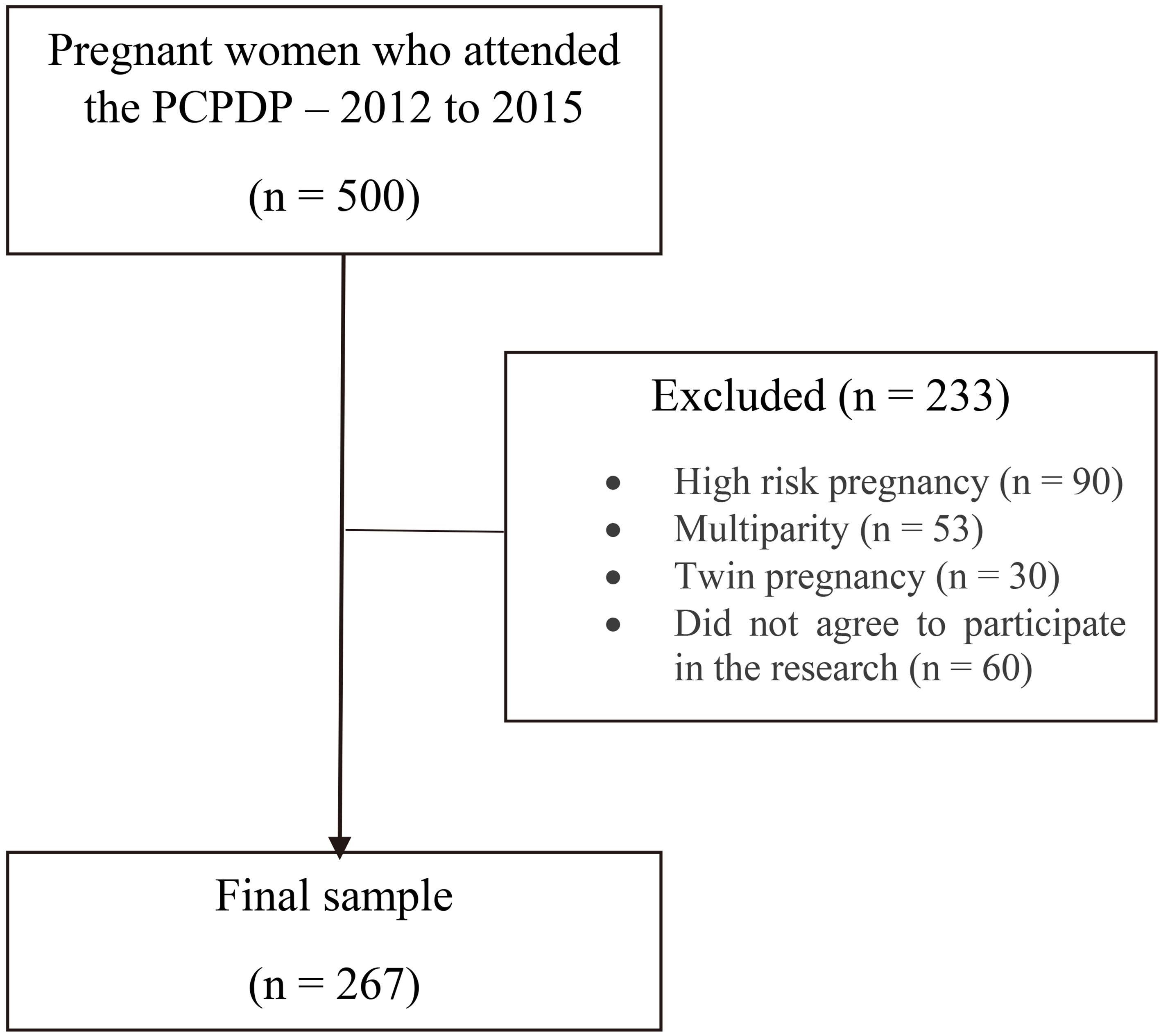
To the sample calculation, we considered the total of pregnant women who attended the PCPDP from 2012 to 2015 (
Figure 1.
Search sample flowchart.
2.2Evaluation tools
The variables were collected using an evaluation form, elaborated by the responsible researchers, and divided into the following groups: sociodemographic data (age, years of education, family income, marital status), obstetric data (gestational age and trimester), anthropometric and lifestyle data (weight, height, BMI, weight gain and physical activity practice).
Table 1
Sociodemographic, obstetric, anthropometric and lifestyle characteristics (
| Variables | Second trimester | Third trimester | Total | |||
|---|---|---|---|---|---|---|
| ( | ( | ( | ||||
| Socialdemographic data | ||||||
| Age (years) | 29.83 | 29.77 | 29.80 | |||
| Years of study | 16.24 | 16.62 | 16.41 | |||
| Marital status | ||||||
| With lifepartner | 94.1% (145) | 92.2% (105) | 93.6% (250) | |||
| Without lifepartner | 1.9% (3) | 0.9% (1) | 1.5% (4) | |||
| Obstetric data | ||||||
| Gestational age (weeks) | 20.7 | 30.05 | 24.68 | |||
| Trimesters | ||||||
| Second | – | – | 57.7% (154) | |||
| Third | 42.3% (113) | |||||
| Anthropometric and lifestyle data | ||||||
| Pre-gestational weight (kg) | 60.04 | 65.47 | 62.32 | |||
| Gestational weight (kg) | 66.05 | 71.30 | 68.26 | |||
| Height (m) | 1.62 | 1.62 | 1.62 | |||
| Pre-gestational BMI (kg/m | 22.79 | 24.78 | 23.62 | |||
| Gestational BMI (kg/m | 24.92 | 27.01 | 25.79 | |||
| Weight gain | 5.97 | 5.86 | 5.92 | |||
| Physical activity | ||||||
| Active | 35.7% (55) | 45.1% (51) | 39.7% (106) | |||
| Sedentary | 63.6% (98) | 54% (61) | 59.6% (159) | |||
Note: there was loss of data for the variable.
The weight gain calculation was made from a subtraction of the weight in the moment of evaluation and pre-gestational weight. For the pre-gestational body mass index (BMI), the weight of the woman before pregnancy was considered and classified as: underweight (BMI, 18.5 Kg/m
Regarding the practice of physical activity, the volunteers were asked: “Do you practice physical activity (low to moderate intensity), at least twice a week, with minimum duration of 50 minutes (by episode)?” If the answer was “yes”, the woman was considered active; otherwise, sedentary [16].
The low back and pelvic pain evaluation was made by asking the volunteer initially “Do you feel low back and/or pelvic pain?”. If the answer was positive, the pregnant woman would indicate the intensity of the pain using the Visual Analogue Scale (VAS) to localize pain in the human figure [17].
2.3Statistical analysis
To characterize the sample, we used descriptive analysis (mean, standard deviation, absolute and relative frequencies). In order to test the quantitative variables normality we used Shapiro-Wilk’s test. The comparison of the pain intensity between active and sedentary pregnant women and between those in the second and third gestational trimester was tested by Mann-Whitney U test. Spearman’s correlation test was used to identify the relation between weight gain and pain intensity.
To analyze the influence of physical activity practice (categorical variable: active versus sedentary), gestational trimester (categorical variable: second versus third) and weight gain (numeric variable) over low back and pelvic pain intensity (numeric variable), we used Poisson regression.
3.Results
Sociodemographic and obstetric characterization of the participants showed that 61.8% (
The bivariate analysis showed a significant difference (
The multivariate analysis indicated that sedentary pregnant women have 30% more chances (
Table 2
Multivariate analysis of the relation among physical activity practice, gestational trimester, weight gain and pain intensity
| Chi-squared |
| Exp (B) | Confidence | ||
| test | interval 95% | ||||
| Lower | Upper | ||||
| Sedentary | 12.44 | 0.001 | 1.30 | 1.12 | 1.50 |
| Active | – | – | 1 | – | – |
| Second trimester | 1.54 | 0.21 | 0.91 | 0.79 | 1.05 |
| Third trimester | – | – | 1 | – | – |
| Weight gain | 3.06 | 0.08 | 0.98 | 0.96 | 1.00 |
4.Discussion
The aim of this study was to analyze the influence of physical activity practice, gestational trimester and weight gain influence on the intensity of low back and pelvic pain. The main result suggests that sedentary pregnant women have 30% more chances to feel more severe pain, when compared to the active women (OR
Physical activity during pregnancy promotes lots of benefits, such as: reducing the risk of overweight, gestational diabetes, pre-eclampsia, preterm birth, varicose veins and deep vein thrombosis [18]. These benefits also include the decrease of low back and pelvic pain intensity, as shown by the study by Da Silva et al. [17], in which they submitted 26 pregnant women to a physical activity protocol for 1 month. The results of this research showed a significant decrease in the LBPP, measured by the Visual Analog Scale (VAS), when compared the values before and after the intervention. A randomized controlled clinical trial with 45 volunteers (20 in the experimental group and 22 in the control group), also showed similar results: pregnant women submitted to a physical activity protocol, which included aerobic and muscle strengthening activities, presented lower pain intensity when compared to the control group [19]. These findings corroborate with the results of our study.
Physiologically, during pregnancy low back and pelvic muscles are gradually overloaded, due to an increase in the total body mass and uterus size [20]. These factors take the abdominal muscles to its maximum stretching, resulting in an unfavorable length tension relationship to the force generation, which causes a decrease in low back and pelvic stability [21, 22]. Thus, although paravertebral muscles are composed mostly by muscle fibers type I, the muscle overload and imbalance, characteristics of the biomechanical changes due to pregnancy, may result in LBPP [22]. Contrary to the pregnant body adaptations, the regular practice of physical activity results in a cardiorespiratory fitness, endurance and muscle strength improvement, and, consequently, decreases low back and pelvic pain intensity [23].
Additionally, the regular practice of physical activity is opposite to a sedentary lifestyle, which is defined as the execution of activities that spend little metabolic energy and is connected to unfavorable health conditions [24]. This concept corroborates with our findings, since sedentary women presented 30% more chances to report greater pain intensities than the active women in our study.
In this way, the professionals responsible for assisting pregnant women should encourage them to keep active during pregnancy, prescribing physical activities that respect the principles of modality, duration, frequency, intensity and progression mode [25].
We did not observe the influence of the third gestational trimester variable over LBPP intensity (OR
Lastly, we found that the weight gain did not influence the LBPP intensity (
4.1Clinical importance and study limitations
This study is important clinically to incite health professionals to encourage pregnant women to adopt a healthy lifestyle, practicing physical activities regularly as a way to prevent low back and pelvic pain or the increase in its intensity. However, we stress that the physical activity should respect the specific characteristics of each pregnancy, as well as the muscular and cardiorespiratory training parameters.
This study’s limitations were the lack of a specific questionnaire to evaluate the volunteers’ level of physical activity and not including pregnant women in the first gestational trimester. Thus, we suggest new longitudinal studies to determinate the risk or protective factors related to the occurrence and intensity of LBPP in pregnant women.
5.Conclusion
Sedentary pregnant women have 30% more chances to have higher pain intensities when compared to the active women, regardless of the gestational trimester and weight gain.
Conflict of interest
None to report.
References
[1] | Ehrlich GE. Low back pain. Bull World Health Organ. (2003) ; 81: (9): 671–6. |
[2] | Gutke A, Betten C, Degerskär K, Pousette S, Fagevik Olsén M. Treatments for pregnancy-related lumbopelvic pain: A systematic review of physiotherapy modalities. Acta Obstet Gynecol Scand. (2015) ; 94: (11): 1156–67. |
[3] | Kendall KD, Emery CA, Wiley JP, Ferber R. The effect of the addition of hip strengthening exercises to a lumbopelvic exercise programme for the treatment of non-specific low back pain: A randomized controlled trial. J Sci Med Sport [Internet]. Sports Medicine Australia. (2015) ; 18: (6): 626–31. Available from: http://dx.doi.org/10.1016/j.jsams.2014.11.006. |
[4] | Mota MJ, Cardoso M, Carvalho A, Marques A, Sa-Couto P, Demain S. Women’s experiences of low back pain during pregnancy. J Back Musculoskelet Rehabil. (2015) ; 28: (2): 351–7. |
[5] | Mann L. Alterações biomecânicas durante o período gestacional: uma revisão. Motriz J Phys Educ. (2010) ; 16: (3): 730–41. |
[6] | Vleeming A, Albert HB, Östgaard HC, Sturesson B, Stuge B. European guidelines for the diagnosis and treatment of pelvic girdle pain. Eur Spine J. (2008) ; 17: (6): 794–819. |
[7] | Ozdemir S, Bebis H, Ortabag T, Acikel C. Evaluation of the efficacy of an exercise program for pregnant women with low back and pelvic pain: A prospective randomized controlled trial. J Adv Nurs. (2015) ; 71: (8): 1926–39. |
[8] | Mazicioglu M, Tucer B, Ozturk A, Serin IS, Koc H, Yurdakos K, et al. Low back pain prevalence in Turkish pregnant women. J Back Musculoskelet Rehabil [Internet]. (2006) ; 19: : 89–96. Available from: http://www.deepdyve.com/lp/ios-press/low-back-pain-prevalence-in-turkish-pregnant-women-nsRX84Qkw3. |
[9] | Sd L, Pennick V. Interventions for preventing and treating low-back and pelvic pain during pregnancy (Review) Summary of Findings for the Main Comparison. (2015) ; (9). |
[10] | Lima AS, et al. Análise da postura e frequência de lombalgia em gestantes: estudo piloto. Journal of the Health Sciences Institute, Volta Redonda. (2011) ; 29: (4): 290–293. |
[11] | Brito JLOP, et al. Lombalgia: prevalência e repercussões na qualidade de vida de gestantes. Revista de Enfermagem da UFSM, Santa Maria. (2014) abr/jun; 4: (2): 254–264. |
[12] | Mann L, Kleinpaul JF, Teixeira CS, Konopka CK. Dor lombo-pélvica e exercício Físico durante a gestação. Fisioter. Mov. (2008) abr/jun; 21: (2): 99–105. |
[13] | Moreira LS, de S Andrade SR, Soares V, De Avelar IS, Amaral WN, Vieira MF. Alterações posturais, de equilíbrio e dor lombar no período gestacional. Femina. (2011) ; 39: (5): 241–4. |
[14] | OMS. Organização Mundial da Saúde, (1995) . Physical Status: The use and interpretation of anthropometry. Technical Report Series, 854. Genebra: OMS. |
[15] | Atalah SE, Castillo CL, Castro RS. Propuesta de um nuevo estandar de evaluación nutricional em embarazadas. Rev Med Chile. (1997) ; 125: : 1429–36. |
[16] | American College Obstetricians and Gynecologists, (2002) . |
[17] | Da Silva SR, Sousa VPS, Bezerra DA, Ribeiro SO, Viana ESR. Influência da Cinesioterapia sobre a dor e qualidade de vida em mulheres grávidas. Fisioterapia Brasil. (2012) ; 13: : 23–28. |
[18] | Evenson KR, et al. Guidelines for physical activity during pregnancy: comparisons from around the world. Am. J. Lifestyle Med. (2014) ; 8: (2): 102–121. |
[19] | Kokic IS, et al. Effect of therapeutic exercises on pregnancy-related low back pain and pelvic girdle pain: secondary analysis of a randomized controlled trial. J Rehabil Med. (2017) ; 49: : 251–257. |
[20] | Gallo-Padillaa D, Gallo-Padilla C, Gallo-Vallejoc FJ, Gallo-Vallejo JL. Lumbalgia durante el embarazo. Abordaje multidisciplinar. Semergen. (2016) ; 42: (6): e59–e64. |
[21] | Sabino J, Grauer JN. Pregnancy and low back pain. Curr Rev Musculoskelet Med. (2008) ; 1: (2): 137–141. |
[22] | De Sousa VPS, Ribeiro SO, Aquino CMR, Viana ESR. Quality of sleep in pregnant woman with low back pain. Fiosterapia em Movimento (on-line). (2015) ; 28: : 319–326. |
[23] | Garland M. Physical activity during pregnancy: a prescription for improved perinatal outcomes. The Journal for Nurse Practitioners – JNP. January (2017) ; 13: (1). |
[24] | Fazzi C, Saunders DH, Linton K, Norman JE, Reynolds RM. Sedentary behaviours during pregnancy: a systematic review. International Journal of Behavioral Nutrition and Physical Activity. (2017) ; 14: : 32. |
[25] | Leitão MB, et al. Posicionamento oficial da sociedade brasileira de medicina do esporte: atividade física e saúde na mulher. Rev Bras Med Esporte. (2000) ; 6: : N |
[26] | Ghaderi F, Jafarabadi MA, Bandpei MAM. Prevalence of musculoskeletal pain and associated factors with low back pain during pregnancy. Iranian Journal of Obstetrics, Gynecology and Infertility. (2013) ; 15: (41): 9–16. |
[27] | Bliddal M, et al. Association of pre-pregnancy body mass index, pregnancy-related weight changes, and parity with the risk of developing degenerative musculoskeletal conditions. Arthritis and Rheumatology. (2016) ; 68: (5): 1156–1164. |


