
Gender-based analysis of muscle activation while in a sedentary work posture
Abstract
BACKGROUND:
Many people work in a sitting position where they have to use their upper extremities and hands. Muscle activity in sitting position is affected by the chair height of, the height of the worktable, and the distance to the working target.
OBJECTIVE:
The purpose of this study is to investigate differences in muscle activity between men and wemen at different chair heghts and working distances.
METHODS:
Surface electromyography (EMG) was employed to determine the muscle activity of the upper limbs and the trunk, while an arm-stretching task was performed in a sitting position.
RESULTS:
Women’s muscle activity was higher than that of men in most muscles as the chair height and working distance changed.
CONCLUSIONS:
As the height of the chair or the working distance was changed, muscle activity was greater in women than in men for most of the muscles analyzed. Under the same conditions, women may feel more muscle fatigue than men, so it is necessary to consider gender in the working environment.
1.Introduction
Adults spend most of their waking hours sitting [1]. One study founded people in their 20s–40s were sitting for seven to eight hours a day [2]. In a Southeast Asian study on physical activity, Win et al. [3] found that an average person spends about 6 hours a day in a sitting posture, and that around 37% exceeded eight hours in a sitting posture.
While at work in a sedentary position, men and women typically use the same worktables and chairs of the same height. However, women generally have shorter heights, smaller muscle cross-sectional area, and weak muscle strength than men [4]. This difference in muscle strength produces different performances by men and women [5]. Furthermore, it is known that, during the developmental growth process in women, in mass and strength of the bones are greater than those of the muscles, whereas, in men, muscle mass and strength increase along with the growth of bones [6]. Therefore, men and women will have different muscles and methods of using them in sitting positions.
While writing or working in a sitting position, the body is likely to be bowed forward, leading to a slumping posture. As the distance between the worktable and the trunk increases, the flexion angle of the trunk increases [7], creating a space for the trunk to move forward, which results in a sitting position with a stoop [8]. The muscles of the neck that support the head and the muscles of the back that support the body are extended when the upper body leans forward for a long time, quickly rendering the worker tired. Due to the bent posture, the natural spinal form disappears, causing discomfort to the cervical, thoracic, and lumbar regions [9]. A poor sitting position can be caused by worktables and chairs that do not fit the body structure. Such poor posture can place excessive stress on the musculoskeletal system, including the lumbar spine, leading to deformation of the musculoskeletal system in the body. And ultimately to health impairment [10]. Moreover improper heights of the worktable and chair cause pain in the upper limbs, shoulder, trunk, and back [11]. TThe height of the backrest of the chair, the height of the seat surface, and the width of the seat surface were found to be risk factors for the subjective symptoms of cumulative traumatic diseases. [12]. Women have different muscle characteristics than men. Long-term sitting in chairs that do not fit the human body structure will cause discomfort and musculoskeletal burdens to women.
The aim of this study was to investigate the gender-related effects on muscle activity of the trunk and upper exterimity according to various chair heights and distances between the user and the worktable, which could affect the work performed in a sitting position.
2.Meterials and method
2.1Subjects
The purpose and methods of this study were fully explained to the research subjects by the Declaration of Helsinki before the experiment, and those who voluntarily agreed to the research were targeted. They were informed that they could quit any time if they refused in the middle of the experiment and that there would be no disadvantage. Data from subjects who quit the experiment midway were discarded. It was conducted on 10 healthy men (mean age: 21.90 years, height: 175.30 cm) and 10 women (mean age: 20.73 years, height: 161.36 cm) who voluntarily agreed. The criteria for selecting subjects were people with no problems with sitting posture, cognitive impairment, arm reaching, and hand grasping function. Subjects were those who had no experience with upper extremity-related surgery within the past year. The exclusion criterion for subjects were those with musculoskeletal diseases, such as spinal cord scoliosis, kyphosis, and hip joint contracture, those with congenital anomalies or surgical disease, those with spinal diseases or back pain, and those with neurological deficits and diseases.
2.2Surface electromyography (EMG) system
Surface EMG (Noraxon Telemyo 2400T 2G, USA) was used to determine the muscle activity of the upper extremity and trunk. Surface EMG analogue signals coming from channel were collected, stored and analyzed using the MyoResearch 1.07 program. For EMG data processing, the frequency bandwidth was set to 20–250 Hz, and the sampling rate was set to 1000 Hz. EMG signals were collected, processed by rectification, and analyzed by root mean square (RMS). Among the methods used to normalize the amount of EMG signals, maximal voluntary contraction (MVC) is preferred for an operation involving a large amount of force, whereas a reference voluntary contraction (RVC) method is preferred for an operation involving a small amount of force as a method to enhance sensitivity [13]. In this study, the normalization of the amount of EMG signals was processed as % RVC, representing the ratio of the RMS value obtained during the arm-stretching task to the RMS value obtained during the stable state in a sitting position on the chair.
2.3Water bottle
A commercially available water bottle (500 ml) was used. This water bottle is made of plastic and can be easily accessed in everyday life. Because the extent of the muscle response to weight may vary according to gender and muscle strength, the weight was minimized using an empty bottle.
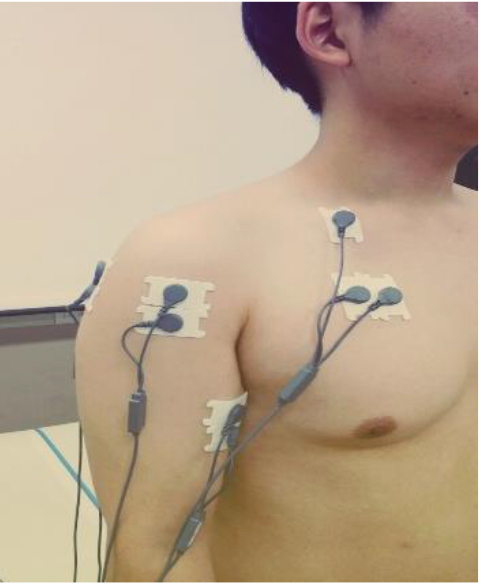
Figure 1.
Surface EMG device attached to the body (front).
2.4Chair and worktables
The used chairs had hard wooden seats with no backrests or armrests. Three types of chairs with varying heights were used, on which subjects could have a sense of security while working with their hips fully supported. After a subject was seated with both feet stably on the floor, their back was stretched to a neutral position, followed by measurement of the knee flexion angle with an electronic goniometer (E-LINK ROM Kit, Biometrics, United Kingdom). The seat height was adjusted to establish knee flexion angles of 80∘, 90∘, and 100∘. The 80∘ knee flexion angle was achieved with a relatively lower seat position than that for the 90∘ knee flexion angle, and the 100∘ knee flexion angle was achieved with a relatively higher seat position than that for the 90∘ knee flexion angle.
The height of the worktable can be adjusted up and down, and the surface of the worktable is non-slip. In the position the subjects sat on a chair, the height was set to allow the object to be moved by bending the elbow 90 degrees.
2.5Experimental procedures
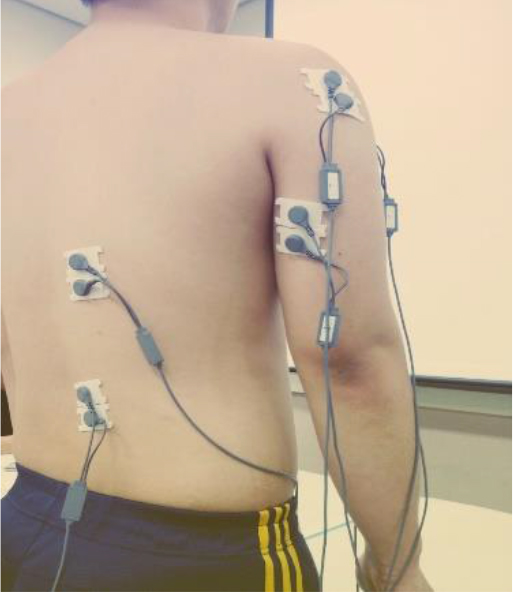
To reduce skin resistance to surface EMG signals, hair was removed, and the skin was wiped off with disinfecting alcohol on cotton where the electrodes were placed. The surface electrodes were attached tightly to the skin in parallel with muscle fibers, with the intervals between each electrode being set to within 20 mm. The surface electrodes were attached to the subject’s dominant hand, with its the pectoralis major, anterior deltoid, posterior deltoid, biceps brachii, triceps brachii long head, thoracic erector spinal muscle and lumbar erector spinal muscles. The ground electrode was attached to the clavicle (Figs 1 and 2).
Figure 2.
Surface EMG device attached to the body (back).
The arm’s length of each subject was measured by raising their arm to their shoulder height and measuring the length from the axilla to the wrist while the shoulder joint was in a flexion state. Distances corresponding to 50%, 70%, 90%, 110%, and 130% of the arm length were established, referring to the study of Yoo et al. [14]. These distances were marked on the worktable. And the mark was the position of the center line when the subject sat in the chair.
The height of the worktable was set so that the elbow angle of the subject could be maintained at 90∘ while the subject sat on the chair with both the ankle joints and knee joints bent at 90∘. The knee width was set to be equal to the width of the pelvis. The distance between the trunk and the worktable was 15 cm, and to prevent the trunk contact with the backrest or worktable. The distance between the base of the chair and the popliteus was set to 8 cm (Fig. 3).
Figure 3.
Initial posture.

Before performing the arm reaching task, the RVC value was first measured to quantify the activity potentials of the muscles being measured. While the subject maintained a natural posture for 15 seconds in a sitting position on the chair, the EMG signals of each muscle were measured three times. The mean value obtained from the middle five seconds of the three repeated measurements was taken as the voluntary reference contraction value.
Each subject, following a voice instruction (“start”) from the investigator, performed an arm-stretching task consisting of grabbing a water bottle with the dominant hand (confirmed in advance) and putting the bottle at a position marked on the worktable. Subjects were given sufficient time to practice beforehand to become accustomed to the movement. The task was performed at three different chair heights, corresponding to knee flexion angles of 80∘, 90∘ and 100∘. Each task was performed three times, and the mean value of the three experiments was used for analysis.
The project was approved by the Kangwon National University (approvalnumber: KWNUIRB-2015-12-001-001).
2.6Data analysis
To verificationof statistical significance of the mean difference in muscle activity according to gender, chair height, and working distance, an analysis was first conducted to determine whether the normal distribution was satisfied. As a result, normal distribution was satisfied, so multivariate analysis (MANOVA) was performed, and an independent t-test was conducted to examine the differences in the mean values between gender groups. The results were presented as mean and standard deviation. The SPSS Statistics 21.0 program was used for statistical analysis of the data. A value of
3.Results
3.1General characteristics of subjects
The subjects who participated in this study were 20 people, 10 men, and 10 women. The mean age of men was 21.90 years, and the mean age of women was 20.73 years. The mean heights of the men and women were 175.30 cm and 161.36 cm, respectively. The mean weights of the men and women were 70.20 kg and 58.00 kg, respectively. The mean arm lengths of the men and women were 53.60 cm and 50.64 cm, respectively (Table 1).
Table 1
Characteristics of the subject groups (Mean
| Male ( | Female ( | |
|---|---|---|
| Age (year) | 21.90 | 20.73 |
| Height (cm) | 175.30 | 161.36 |
| Weight (kg) | 70.20 | 58.00 |
| Arm length (cm) | 53.60 | 50.64 |
3.2Changes in muscle activity associated with changes in chair height
The muscle activity was examined according to chair heights corresponding to knee flexion angles of 80∘, 90∘, and 100∘ (Table 3). The muscle activities of the pectoralis major (
The muscle activity of the pectoralis major was greater in men than in women for all chair heights. On chair heights that created knee flexion angles of 80∘ and 100∘, the muscle activity of the posterior deltoid was greater in women than in men. The muscle activities of the biceps brachii and thoracic erector spinal muscle were greater in women than men when knee flexion angles were 90∘ and 100∘. The muscle activity of the triceps brachii was greater in women than in men when knee flexion angles were 80∘ and 90∘. The muscle activity of the lumbar erector spinal muscle was greater in women than in men, with the chair height that created a knee flexion angle of 100∘. The muscle activity of the anterior deltoid showed no significant difference between men and women at any chair height. Overall, the muscle activity was greater in women than men in most of the muscles analyzed under the experimental conditions.
3.3Changes in muscle activity according to working distancet
Muscle activity was examined according to changes in the distance between the trunk and the worktable (Table 3). The arm-stretching task was performed at working distances of 50%, 70%, 90%, 110%, and 130% of arm length for each subject.
When the working distance was 50% of arm length, the changes in the muscle activities of the posterior deltoid (
When the working distance was
3.4The role of gender on muscle activity at various chair heights or working distances
Gender was found to have a significant effect on muscle activity at various chair heights and working distances. The interaction between gender and chair height statistically significantly affected changes in
Table 2
Changes in muscle activity at various chair heights, according to gender
| PM | PD | AD | BI | TRI | THO | LUM | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female |
| Male | Female |
| Male | Female |
| Male | Female |
| Male | Female |
| Male | Female |
| Male | Female |
| |
| M | M | M | M | M | M | M | M | M | M | M | M | M | M | ||||||||
| Knee flexion angle 80 | 1680.46 | 455.01 | 4.37∗∗∗ | 311.50 | 452.72 | 2645.14 | 2823.21 | 1335.22 | 1157.64 | 1.5 | 440.75 | 518.31 | 133.37 | 129.28 | 0.86 | 155.64 | 156.19 | ||||
| Knee flexion angle 90 | 2146.84 | 367.05 | 5.14∗∗∗ | 320.66 | 345.08 | 2377.30 | 2343.31 | 0.11 | 721.18 | 1177.65 | 453.38 | 562.53 | 114.13 | 154.55 | 161.44 | 166.42 | |||||
| Knee flexion angle 100 | 1428.58 | 433.58 | 4.41∗∗∗ | 287.90 | 374.19 | 2195.56 | 2046.30 | 0.64 | 876.91 | 1286.11 | 432.79 | 487.90 | 110.69 | 137.76 | 135.36 | 163.14 | |||||
Table 3
Changes in muscle activity at various working distances, according to gende
| PM | PD | AD | BI | TRI | THO | LUM | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female |
| Male | Female |
| Male | Female |
| Male | Female |
| Male | Female |
| Male | Female |
| Male | Female |
| |
| M | M | M | M | M | M | M | M | M | M | M | M | M | M | ||||||||
| Working distance 50 | 408.56 | 266.72 | 1.72 | 171.05 | 215.31 | 566.41 | 899.56 | 591.74 | 893.97 | 204.50 | 293.37 | 111.83 | 122.73 | 116.88 | 122.10 | ||||||
| Working distance 70 | 676.72 | 379.39 | 2.08∗ | 199.71 | 293.46 | 1411.31 | 2021.80 | 851.80 | 1263.84 | 292.92 | 450.39 | 127.27 | 133.15 | 127.09 | 139.23 | ||||||
| Working distance 90 | 1331.05 | 430.47 | 3.92∗∗∗ | 263.76 | 353.98 | 2273.94 | 2835.81 | 922.63 | 1269.69 | 370.60 | 519.03 | 126.93 | 144.70 | 138.45 | 154.28 | ||||||
| Working distance 110 | 2375.03 | 563.14 | 4.94∗∗∗ | 328.07 | 488.44 | 3177.65 | 3122.16 | 0.26 | 1111.19 | 1306.67 | 544.38 | 656.58 | 114.51 | 149.84 | 159.48 | 178.09 | |||||
| Working distance 130 | 3489.33 | 497.56 | 5.81∗∗∗ | 524.14 | 680.35 | 4095.27 | 3632.50 | 1.13 | 1264.38 | 1356.94 | 734.51 | 786.78 | 112.93 | 160.24 | 197.23 | 234.84 | |||||
muscle activities of the biceps brachii (
Table 4
Results of the MANOVA(F)
| Gender | Gender | |
|---|---|---|
| PM | 2.91 | 17.99∗∗∗ |
| PD | 2.51 | 1.61 |
| AD | 0.39 | 2.61∗ |
| BI | 12.61∗∗∗ | 1.03 |
| TRI | 0.43 | 1.01 |
| THO | 18.63∗∗∗ | 6.76∗∗∗ |
| LUM | 2.43 | 1.32 |
∗p< 0.05, ∗∗p< 0.01, ∗∗∗p< 0.001. PM: pectoralis major, PD: posterior deltoid, AD: anterior deltoid, BI: biceps brachii, TRI: triceps brachii, THO: thoracic erector spinal muscle, LUM: lumbar erector spinal muscle.
Of the trunk muscles, the muscle activity of the thoracic erector spinal muscle was affected by both the interaction between gender and chair height and the interaction between gender and working distance. Various upper limb muscles were affected by either the interaction between gender and chair height or between gender and working distance.
4.Discussion
In this study, compared muscle activity according to chair height and arm distance to the working target by gender when working in a sitting position.
The study revealed that the muscle activity of the thoracic erector spinal muscle and lumbar erector spinal muscle increased with an increasing distance between the trunk and the working target for both men and women. This result suggests that, as the distance between the trunk and the working target increased, the trunk moved forward to compensate for the difference. When the trunk bends forward, the length of the lumbar erector spinal muscle increases, and their strength changes, and leading to muscle activity higher [15]. Lee et al. [16] reported that when resistance exercise was performed while extending the arm forward, the muscle activity of the lumbar erector spinal muscle increased, which is consistent with the results of the present study. Lee [17] reported that muscle activity in the neck and shoulder muscles was elevated with increased distance between the work table and the trunk. The present study showed that, additionally, the muscle activity of the lumbar erector spinal muscle was elevated. Another study reported that the increasing chair heights correlated with increasing rates of complaints of the subjective symptoms of cumulative traumatic diseases in the upper limbs [12]. However, the present study revealed that not only the upper limb muscles but also the thoracic erector spinal muscle and lumbar erector spinal muscle showed greater muscle activities with increased chair height. Therefore, Therefore, the cumulative muscle fatigue of the trunk muscle as well as the upper extremity muscles will depending on the chair’s height.
In O’Sullivan et al. [18], the electromyographic activities of the thoracic erector spinal muscle and superficial lumbar multifidus were lower during slump sitting than during erect sitting. In contrast to this result, the present study showed that an increase in the distance between the working target and the trunk induced slump sitting, and resulted in the muscle activities of the thoracic erector spinal muscle and the lumbar erector spinal muscle gradually increasing. A reduction in EMG activity of the erector spinal muscle during slump sitting has been reported consistently in the literature, and it seems that postural muscle activity decreases as the lumbopelvic region becomes dependent on its passive structures to maintain the position against gravity at end-range spine flexion. Nevertheless, the elevated muscle activity is believed to be achieved by maintaining lumbopelvic stability to move the upper limbs in the slump posture.
Andrews et al. [19] showed that lumbar pelvic sagittal alignment in a sitting position is affected by gender. Men and women had similar thoracolumbar spinal curves. Still at the lumbar angle, males were flexed more than females were the mean lumbar angle for male participants was slightly more kyphotic in sitting. In men, the pelvis movement rotates posteriorly, and lumbar lordosis is more flattened in a sitting position than in a standing position [20]. In addition, Endo et al. [21] found that the lumbar lordotic angle is markedly greater in women than in men. Women’s lumbar spines exhibited a greater amount of lordosis than did those of the male subjects. This gender difference was associated with higher levels of trunk muscle activity in the iliocostalis lumborum pars thoracic muscles in women than in men [22]. Furthermore, dynamic sitting is associated with changes in lumbar posture [22]. Consistent with previous studies, postural corrections were dependent on lumbopelvic alignment. During dynamic work in a sitting position, women showed higher muscle activity of the lumbar erector spinal muscle muscle than men in 90% and 130% of the arm length from the target. Therefore, it can be seen that women have high activity in the lumbar erector spinal muscle.
In previous studies, the length of time a sitting position was maintained, the flexion angle of the trunk, and the frequency of movements were found to be significant factors in inducing back pain, and keeping a static posture with a large flexion angle for a long time can be a pain-causing factor [23]. The present study showed that more muscle fatigue was accumulated in women than in men while performing the same task. The study by Clarke [24] also found that women feel tired faster than men when performing almost any exercise. Even a small increase in muscle activation can lead to fatigue [25]. Since sitting is inevitable in everyday life, it is essential to correct poor postural habits to avoid daily chronic cumulative trauma and thereby minimize any negative effects. Moreover, given that women may experience more fatigue than men do under the same conditions, it is necessary to consider gender as well as physical conditions in the design of working environments. The heights of chairs, the working distance, and the time spent working are all important workplace considerations.
This study was conducted using chairs without backrests. In modern work environments, chairs with backrests are increasingly becoming popular in consideration of ergonomic design. Because the presence or absence of a backrest affects the activities of the neck and lumbar erector spinal muscles [15], further research on chairs with backrests in various working environments will be needed.
5.Conclusion
The purpose of this study was to investigate the effects of various chair heights and arm reaching distance to the target on muscle activity during sedentary work. And to evaluate the differences in these effects based on gender.
It was found that changes in the chair height or arm reaching distance to the target led to increased muscle activity that was greater in women than in men for most of the muscles analyzed. Considering that women may experience more fatigue than men under the same conditions, gender needs to be considered in the design of working environments.
Conflict of interest
None to report.
References
[1] | Healy GN, Wijndaele K, Dunstan DW, Shaw JE, Salmon J, Zimmet PZ, Owen N. Objectively measured sedentary time, physical activity, and metabolic risk: the Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Diabetes Care. (2008) ; 31: (2): 369-371. doi: 10.2337/dc07-1795. |
[2] | Healy GN, Clark BK, Winkler EA, Gardiner PA, Brown WJ, Matthews CE. Measurement of adults’ sedentary time in population-based studies. American Journal of Preventive Medicine. (2011) ; 41: (2): 216-227. doi: 10.1016/j.amepre.2011.05.005. |
[3] | Win AM, Yen LW, Tan KH, Lim RBT, Chia KS, Mueller-Riemenschneider F. Patterns of physical activity and sedentary behavior in a representative sample of a multi-ethnic South-East Asian population: a cross-sectional study. BMC Public Health. (2015) ; 15: (1): 318. doi: 10.1186/s12889-015-1668-7. |
[4] | Miller AEJ, MacDougall JD, Tarnopolsky MA, Sale DG. Gender differences in strength and muscle fiber characteristics. European Journal of Applied Physiology and Occupational Physiology. (1993) ; 66: (3): 254--262. doi: 10.1007/BF00235103. |
[5] | Salvador EP, Cyrino ES, Gurjão ALD, Dias RMR, Nakamura FY, Oliveira ARD. A comparison of motor performance between men and women in multiple series of weight exercises. Revista Brasileira de Medicina do Esporte. (2005) ; 11: (5): 257-261. doi: 10.1590/S1517-86922005000500002. |
[6] | Lang TF. The bone-muscle relationship in men and women. Journal of Osteoporosis. (2011) ; 2011: . doi: 10.4061/2011/702735. |
[7] | Kim KS, Yoo HS, Jung DH, Jeon HS. Analysis of Movement Time and Trunk Motions According to Target Distances and Use of Sound and Affected Side During Upper Limb Reaching Task in Patients With Hemiplegia. Physical Therapy Korea. (2010) ; 17: (1): 36-42. |
[8] | Caneiro JP, O’sullivan P, Burnett A, Barach A, O’Neil D, Tveit O, Olafsdottir K. The influence of different sitting postures on head/neck posture and muscle activity. Manual Therapy. (2010) ; 15: (1): 54-60. doi: 10.1016/j.math.2009.06.002. |
[9] | Lee SY, In MA. The Analysis of Desk User Suitability For student & Formative Development Study-Focused on Elementary Student-. Korean Society of Basic Design & Art. (2005) ; 6: (4): 333-342. |
[10] | Chaffin DB, Anderson GBJ, Martin BJ. Occupational Biomechanics 4th ed. John wiley & sons; (2006) . |
[11] | Yoon SH, Park SR, An HJ. Study on Physical Symtoms by Postures and Conditions of Used Chairs and Desks in an Elementary School Pupils. Journal of Korean Society for Hygienic Science. (1998) ; 4: (1): 41-54. |
[12] | Jeong HG, Roh YM, Yim HW, Park CY, Jeong CH. A Relationship between Cumulative Trauma Disorder and the Type of Workstatons and chairs in Workers with Repetitive Motion Tasks. Annals of Occupational and Environmental Medicine. (2001) ; 13: (2): 152-163. |
[13] | Park KS, Bak KH, Hong GB. The Effect of Wearable Wrist Rest During Keyboard and Mouse Use. Journal of the Ergonomics Society of Korea. (2008) ; 27: (3): 33-41. doi: 10.5143/JESK.2008.27.3.033. |
[14] | Yoo WG, Park JH, Yoo EY, Shin HK, Choi JD. Effects of Distance of Target on the Movement of Arm and Trunk During Reaching Target Activities. Journal of Korean Society of Occupational Therapy. (2004) ; 12: (2): 61-71. |
[15] | Kim MU, Byeon SJ, Lee GE, Jeong SY, Jo JY, Choi WJ, Choi CY, Kim K. Effects of Position of the Back of a Chair to Muscle Activity during Computer Work. Journal of Rehabilitation Science. (2011) ; 29: (1): 55-68. |
[16] | Lee HO, Bae WS, Shin JW. A Comparison of the Trunk Muscle Activity According to the Direction of Upper Extremity Lifting using Elastic Band. Journal of Korean Society of Physical Medicine. (2016) ; 11: (2): 25-31. doi: 10.13066/kspm.2016.11.2.25. |
[17] | Lee WH. Effect of Distance Between Trunk and Desk on Forward Head Posture and Muscle Activity of Neck and Shoulder Muscles During Computer Work. Journal of the Korean Society of Physical Medicine. (2013) ; 8: (4): 601-608. doi: 10.13066/kspm.2013.8.4.601. |
[18] | O’sullivan PB, Grahamslaw KM, Kendell M, Lapenskie SC, Möller NE, Richards KV. The effect of different standing and sitting postures on trunk muscle activity in a pain-free population. Spine. (2002) ; 27: (11): 1238-1244. |
[19] | Claus AP, Hides JA, Moseley GL, Hodges PW. Thoracic and lumbar posture behaviour in sitting tasks and standing: Progressing the biomechanics from observations to measurements. Applied Ergonomics. (2016) ; 53: : 161-168. doi: 10.1016/j.apergo.2015.09.006. |
[20] | De Carvalho DE, Soave D, Ross K, Callaghan JP. Lumbar spine and pelvic posture between standing and sitting: a radiologic investigation including reliability and repeatability of the lumbar lordosis measure. Journal of Manipulative and Physiological Therapeutics. (2010) ; 33: (1): 48-55. doi: 10.1016/j.jmpt.2009.11.008. |
[21] | Endo K, Suzuki H, Nishimura H, Tanaka H, Shishido T, Yamamoto K. Sagittal lumbar and pelvic alignment in the standing and sitting positions. Journal of Orthopaedic Science. (2012) ; 17: (6): 682-686. doi: 10.1007/s00776-012-0281-1. |
[22] | O’sullivan P, Dankaerts W, Burnett A, Straker L, Bargon G, Moloney N, Perry M, Tsang S. Lumbopelvic kinematics and trunk muscle activity during sitting on stable and unstable surfaces. Journal of Orthopaedic & Sports Physical Therapy. (2006) ; 36: (1): 19-25. doi: 10.2519/jospt.2006.36.1.19. |
[23] | Lee SH. A Study on the Association Between Sitting Posture and Back Pain. The Graduate School of Inha University. Master’s dissertation. (2006) . |
[24] | Clarke DH. Sex differences in strength and fatigability. Research Quarterly for Exercise and Sport. (1986) ; 57: (2): 144-149. doi: 10.1080/02701367.1986.10762190. |
[25] | van Dieën JH, Westebring-van der Putten EP, Kingma I, de Looze MP. Low-level activity of the trunk extensor muscles causes electromyographic manifestations of fatigue in absence of decreased oxygenation. Journal of Electromyography and Kinesiology. (2009) ; 19: (3): 398-406. doi: 10.1016/j.jelekin.2007.11.010. |


