
Pedicled ALT-flap for soft tissue reconstruction in the trochanteric area
Abstract
BACKGROUND:
Coverage of soft tissue defects following surgery at the trochanteric area is challenging. Revision surgery in case of compromised wound healing may lead to soft tissue defects requiring reconstruction with pedicled or free flaps. Previous access to the hip joint may jeopardize neurovascular structures relevant to the flap.
OBJECTIVE:
In this study, we evaluated if the use of a pedicled anterior lateral thigh (ALT) flap is a valuable option for soft tissue reconstruction.
METHODS:
In this retrospective study, seven patients were included. Defect etiology was tumor resection in one case, screw osteosynthesis in another case and total hip arthroplasty in three cases. All patients underwent reconstruction by proximal pedicled anterior lateral thigh (ALT) flap.
RESULTS:
Pedicled ALT flap was a safe procedure in all cases. One patient showed delayed wound healing with need for additional surgery. No further complications were observed.
CONCLUSIONS:
Pedicled ALT flap transfer represents a reliable option for soft tissue coverage in the trochanteric area after primary surgery such as hip arthroplasty, osteosynthesis or tumor resection.
1.Introduction
Coverage of soft tissue defects in the trochanteric area is a persistent challenge. While hip arthroplasty or osteosynthesis is often a safe and reliable procedure for fractures of the proximal femur, complications such as infection or postoperative seroma might lead to massive soft tissue defects. Also resection of extensive mesenchymal tumors in this region such as sarcoma, may cause large defects without any reasonable option for local wound closure. Repetitive revision surgery often induces excessive scarring and soft tissue loss, making coverage even more difficult.
Due to demographic change, there are increasing numbers of geriatric and comorbid patients requiring hip arthroplasty and/or tumor resections. Complications such as infections and subsequent soft tissue deficiency are a common problem. While many of these defects are amenable to direct closure, full motion range will lead to dehiscence and repeat breakdown of the instable wound. Thus, a tissue transfer is often indicated to allow tension-free closure. To introduce well vascularized tissue into the defect, pedicled options exist which recruit tissue from the abdomen or thigh such as tensor fasciae latae (TFL), groin flap, vastus lateralis or rectus abdominis (VRAM) [1, 2, 3, 4].
These options are based on an intact and reliable vascular pedicle and intact muscular structures. The TFL, vastus lateralis and pedicled groin flap receive their vascular supply through the ascending branch of the lateral circumflex femoral artery (LCFA), which is often transected by the operative approach [5]. Besides this, there is considerable donor site morbidity, especially when transferring muscular flaps into the defect. In many cases, VRAM requires stabilization of the abdominal wall with surgical mesh and may increase the risk of herniation [6].
In contrast, transfer of perforator-based fasciocutaneous flaps from the anterior thigh (ALT) is a good option as it causes minimal donor site morbidity [7]. Perforators from the descending branch of the LCFA as vascular pedicle are unlikely to have been injured by previous access to the hip joint either through the anterior or lateral approach as the pedicle is found medial and inferior to the hip region (Fig. 3). uperior rotation of the pedicled flap into a proximal defect allows the central region of the flap, including the perforator, to cover the most sensitive area of the defect. This leads to reliable tissue perfusion.
The aim of this study is to outline the benefits of harvesting a pedicled ALT flap to address soft tissue defects secondary to surgery in the trochanteric area after hip arthroplasty or tumor resection.
2.Materials and methods
2.1Study design
In this retrospective cohort study, seven patients that received a pedicled ALT flap in the trochanteric area between 2009 and 2020 were identified in a chart analysis with consent to the ethical committee. Three patients initially underwent total hip arthroplasty, two patients required screw osteosynthesis after a traumatic hip fracture, and all four subsequently showed delayed wound healing and wound dehiscence. Two further patients underwent resection of liposarcoma with consecutive soft tissue deficiency.
Extracted data included age, sex, comorbidities, preoperative defect size, preoperative planning markings, intra- and postoperative complications, infection rate and soft tissue closure (Table 1).
2.2Anatomical background
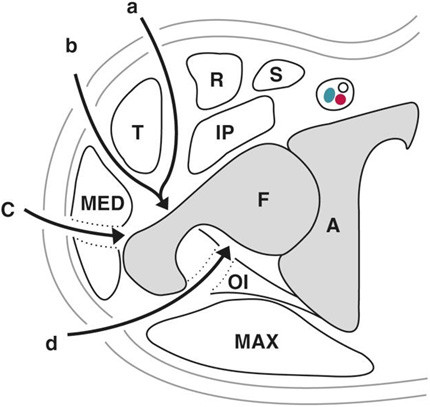
Access to the hip joint via the lateral approach requires transsection of the tractus iliotibialis and/or medial gluteus muscle. Minimally invasive techniques in hip replacement surgery, such as direct anterior approach (DAA), do not require dissection of the gluteus muscle and superior layer of the tractus iliotibialis. When distal extension of the DAA is required, transection of the deep layer may damage the vascular pedicle to the TFL muscle, the ascending branch of the lateral circumflex femoral artery (LCFA), or the vastus lateralis muscle (Figs 1, 3) [5, 8, 9].
Figure 1.
Operative approaches for hip arthroplasty. Direct anterior/anterolateral approach (a,b), lateral approach (c), posterolateral approach (d).
Compartment resections in tumor cases require en-bloc-resection including the vascular pedicle of tractus iliotibialis and femoral quadriceps muscle.
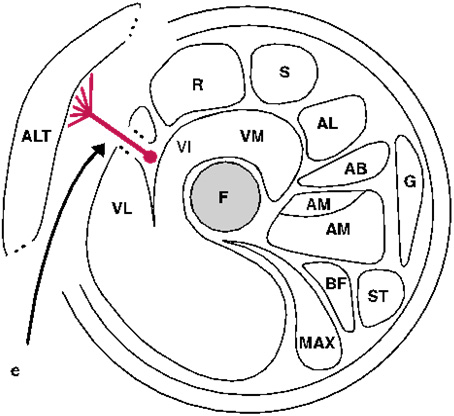
The ALT flap receives its vascular supply from the descending branch of the lateral circumflex artery (LCFA) which is located distally from the operative access area to the hip joint (Figs 1–3). Transsection of the vastus lateralis muscle is required in cases of intramuscular vascular morphology to ensure sufficient preparation of the pedicle (Fig. 2).
Figure 2.
Operative approach to the vascular pedicle of ALT flap (e) F: femur, A: acetabulum, T: tensor fascia latae, MAX: gluteus maximus, MED: gluteus medius, R: rectus femoris, S: sartorius, IP: iliopsoas, OI: obturatorius internus, VL: vastus lateralis, VI: vastus intermedius, VM: vastus medialis, AL: adductor longus, AB: adductor brevis, AM: adductor medius, Am: adductor minimus, G: gracilis, ST: semitendineus, BF: biceps femoris, ALT: anterior lateral thigh.
2.3Operative procedure
To optimize the preoperative defect wound situation, negative-pressure wound therapy (NPWT) conditioning preceded in all cases.
Preoperative planning prior to tissue transfer included localization and marking of potential perforator vessels in the lateral thigh region by use of a handheld doppler ultrasound device. A line from the anterior superior iliac spine to the lateral superior pole of the patella is divided in half. Perforators can be identified in a 3-cm-circle around the middle of this line (Fig. 4).
Figure 3.
Levels of operative approach for hip arthroplasty and anterolateral thigh flap in relation to the ascending and descending branch of the LCFA.
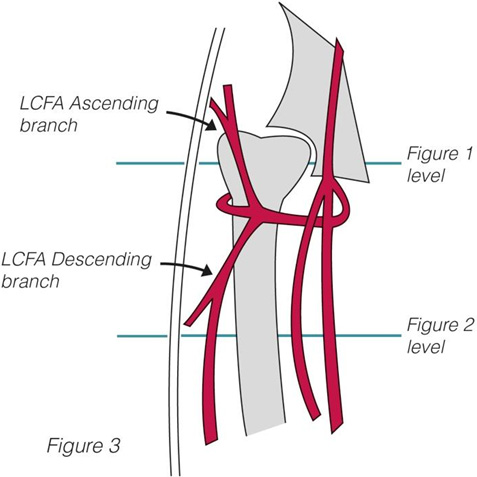
Figure 4.
Peroperative markings.

All cases were performed under general anesthesia. According to defect measurements, flap size was marked around the perforators with additional 1-cm-margin on all sides. Access to the perforator arteries was gained through a medial incision and preparation of the subfascial plane of the thigh. Afterwards the dominant perforator artery was visualized. Locating the vascular pedicle distally ensures sufficient length to allow transposition into the defect. After identifying the marked perforator as a suitable vascular pedicle, the flap was elevated in retrograde position and transferred into the defect through tunneling the subcutaneous tissue between donor and defect side (Fig. 5). After insertion, a drain was placed and the flap was fixed by 3-0-monofil sutures. The donor side defects were closed in primary fashion in all cases (Fig. 6.)
Figure 5.
Proximal located vascular pedicle after flap harvesting.

Figure 6.
Postoperative findings with full defect coverage.

3.Results
Seven patients were included in this study (four female/three male). The mean patient age was 70 years and mean defect size was 46.3 cm2. In five cases, the defect occurred due to periprosthetic infection or osteosynthesis, two patients showed a soft tissue defect after resection of a large liposarcoma (Table 1).
Before reconstruction, all wounds were preconditioned with NPWT. Definite soft tissue reconstruction was performed by a pedicled ALT-flap. The mean operation time was 215.6 minutes. Donor side defect was closed in primary fashion in all cases.
In one case delayed wound healing after tissue transfer was observed, which required secondary closure. Complete flap failure or loss did not occur (Table 1).
4.Discussion
Surgery in the trochanteric area such as hip replacement, osteosynthesis and tumor resections are common procedures. Despite their excellent safety records, complications such as chronic infection and wound healing complications may cause soft tissue defects, which are only amenable to closure by using pedicled or free flaps.
Table 1
Demographic data of the patient cohort
| Pts. No. | Age | Sex | Defect measurements in cm | Defect size in cm2 | Defect etiology | NPWT | Comorbidities | Smoking | Complications | Donor site | ORIF |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 59 | m | 10x4 | 40 | Infect of prosthesis | Yes | Hypertensive disease, diabetes, acne inversa | Yes | None | Primary closure | Total hip endoprosthesis |
| 2 | 79 | m | 10x3 | 30 | Liposarcoma | Yes | Hypertensive disease, Liposarcoma | No | None | Primary closure | – |
| 3 | 82 | f | 5x9 | 45 | Infect of prostesis | Yes | – | No | None | Primary closure | Total hip endoprostesis |
| 4 | 63 | f | 6x5 | 30 | Infect of osteosynthesis | Yes | CML, Thrombophily | No | Delayed healing | Primary closure | Screw osteosynthesis |
| 5 | 71 | f | 11x5 | 55 | Infect of prosthesis | Yes | – | No | None | Primary closure | Total hip endoprosthesis |
| 6 | 62 | m | 12x7 | 84 | Liposarcoma | Yes | Hypertensive disease, arrhythmia | No | None | Primary closure | – |
| 7 | 74 | f | 10x4 | 40 | Infect of osteosynthesis | Yes | Diabetes mellitus | Yes | None | Primary closure | Screw osteosynthesis |
Local advancement flaps often fail due to tissue tension and insufficient perfusion. A prior operative approach makes it even more difficult to get sufficient soft tissue coverage [5, 8, 9]. While numerous reconstructive options have been used in the past, they are often associated with a high rate of complications [1, 2, 3, 4].
The vertical rectus abdominis flap (VRAM) requires abdominal tissue transfer and stabilization of the abdominal wall with mesh grafts. Complications such as herniation of abdominal contents or weakness of the abdominal wall are known and especially troublesome in the elderly population [6]. The pedicled groin flap represents a good locally pedicled option. Its donor side, including the dorsal aspect of the iliac crest is prone to complications. Often, immobile patients are bed-ridden and the harvest site may progress into a pressure sore if a wound healing complication arises. The vascular pedicle (ascending part of LCFA) is prone to traction damage from previous surgeries [5].
The vascular pedicle of the ALT is positioned away from the operative approach to the femur, therefore provides reliable perfusion in these cases.
As shown in previous studies, the ALT flap is a well-established option for coverage of lower extremity soft tissue defects [7, 10].
The free microvascular flap is commonly used in cases where the pedicled ALT flap is not a feasible option, such as for more regional defects in the trochanteric or abdominal wall area [11, 12, 13].
Owing to the complexity of the area, increased safety in tissue transfer can be provided by keeping the original perfusion of the flap without need for microvascular anastomosis.
The autograft is harvested distal to the defect and rotated laterally upwards. Usually, the central area including the perforator covers the most distal aspect of the wound. This is beneficial as the autograft’s well-perfused central area is positioned in the most critical part of the wound (Figs 4–6). As the ALT flap may be harvested up to 7 cm in width, even large defects can be addressed and allow tension-free closure of the donor site. Due to the anterior location of the donor region on the thigh, no pressure occurs throughout the healing phase. This is important as these patients are usually bed-ridden for an extended period of time and this procedure requires immobilization. The abdominal wall is also left undisturbed.
The ALT flap receives its vascular supply through the descending part of the LCFA, which is typically left untouched by primary surgery and provides reliable perfusion. Using this flap as a pedicled variant without need for a microsurgical anastomosis allows shorter operation time and minimizes the risk of postoperative flap loss [12].
5.Conclusion
Pedicled ALT flap can be used not only for soft tissue reconstruction in the lower abdominal or perineal area, but is also a very reliable option for the soft tissue reconstruction of defects resulting from hip surgery [11].
In the hands of experienced microsurgeons, this flap is a safe and swift option. Consequently, we consider this flap to be the prime flap in these difficult revision cases.
Funding
No funding was received for this study.
Ethical approval
All methods were carried out in accordance with relevant guidelines and regulations. All experimental protocols were approved by the ethical committee of University of Wuerzburg. Informed consent was obtained from all subjects. All patient data were used anonymized and were received by the patient chart in consent to the local ethical committee.
Ethical approval
All data generated or analysed during this study are included in this published article.
Conflict of interest
None of the authors declare any conflicts of interest.
References
[1] | Burm YS, Yang WY et al. Distally extended tensor fascia lata flap including the wide iliotibial tract for reconstruction of trochanteric pressure sores. J Plast Aesthet Reconstr Surg. (2011) ; 64: (9): 1197-201. doi: 10.1016/j.bjps.2011.04.010. Epub 2011 Jun 8. |
[2] | Paletta CE, Freedman B, Shehadi SI. The VY tensor fasciae latae musculocutaneous flap. Plast Reconst Surg. (1989) ; 83: (5): 852-7; discussion 858. doi: 10.1097/00006534-198905000-00012. |
[3] | Rodaix C, Auregan J-C, Lhuaire M, Feydy A, Soubeyrand M, Biau D et al. The proximal vastus lateralis flap: An anatomical and radiological study. Morphologie. (2021) ; S1286: -0115(21)00035-7. doi: 10.1016/j.morpho.2021.02.011. |
[4] | Rødgaard JC, Tei TM et al. Delayed Soft Tissue Reconstruction with a Horizontal Rectus Abdominis Musculocutaneous Flap following Hip Exarticulation. Case Rep Surg. (2013) ; 2013: : 670304. doi: 10.1155/2013/670304. Epub 2013 Aug 19. |
[5] | Powers JM, Martinez M, Zhang S, Kale SS. A Description of the Vascular Anatomy of the Tensor Fascia Lata Perforator Flap Using Computed Tomography Angiography. Ann Plast Surg. (2018) ; 80: (6S Suppl 6): S421-S425. doi: 10.1097/SAP.0000000000001424. |
[6] | Schellerer V, Bartholomé L, Langheinrich MC, Grützmann R, Horch RE, Merkel S, Weber K, Donor Site Morbidity of Patients Receiving Vertical Rectus Abdominis Myocutaneous Flap for Perineal, Vaginal or Inguinal Reconstruction. World J Surg. (2021) ; 45: (1): 132-140. doi: 10.1007/s00268-020-05788-5. Epub 2020 Sep 29. |
[7] | Nosrati N. Lower extremity reconstruction with the anterolateral thigh flap. J Reconstr Microsurg. (2012) ; 28: (4): 227-34. doi: 10.1055/s-0032-1306370.. Epub 2012 Mar 7. |
[8] | Putzer D, Haselbacher M, Hörmann R, Klima G, Nogler M. The deep layer of the tractus iliotibialis and its relevance when using the direct anterior approach in total hip arthroplasty: a cadaver study. Arch Orthop Trauma Surg. (2017) ; 137: (12): 1755-1760. doi: 10.1007/s00402-017-2820-x. Epub 2017 Oct 14. |
[9] | Grob K, Monahan R, Gilbey H, Yap F, Filgueira L, Kuster M. Distal extension of the direct anterior approach to the hip poses risk to neurovascular structures: an anatomical study. J Bone Joint Surg Am. (2015) ; 97: (2): 126-32. doi: 10.2106/JBJS.N.00551. |
[10] | Friji MT, Suri MP, Shankhdhar VK, Ahmad QG, Yadav PS. Pedicled anterolateral thigh flap: a versatile flap for difficult regional soft tissue reconstruction. Ann Plast Surg. (2010) ; 64: (4): 458-61. doi: 10.1097/SAP.0b013e3181b4bc70. |
[11] | Jakubietz R, Jakubietz M, Vater A, Kocot A, Kübler H, Kalogirou C. Complex Soft Tissue Defects in Operative Urology: Pedicled Perforator Flaps of the Anterior Lateral Thigh for Tissue Reconstruction of the Lower Trunk. Urol Int. (2021) ; 105: (5-6): 477--482. doi: 10.1159/000512057. Epub 2021 Feb 3. |
[12] | Vijayasekaran A, Gibreel W, Carlsen BT. Maximizing the Utility of the Pedicled Anterolateral Thigh Flap for Locoregional Reconstruction: Technical Pearls and Pitfalls. Clin Plast Surg. (2020) ; 47: (4): 621-634. doi: 10.1016/j.cps.2020.06.011. |
[13] | Hifny M. The pedicled anterolateral thigh flap for trochanteric pressure sore reconstruction: Technical notes to optimize surgical outcome. Arch Plast Surg. (2021) ; 48: (1): 114-120. doi: 10.5999/aps.2020.01270. Epub 2021 Jan 15. |


