
Effects of cooling glove on the human body’s recovery after exercise and improvement of exercise ability
Abstract
BACKGROUND:
After high-intensity exercises, the body’s core temperature increases, affecting the body’s metabolism, increasing thermal stress and muscle fatigue. The most popular technique to maximize post-workout recovery is cryotherapy. However, the cooling effect may vary depending on the body part being cooled since body tissues do not process the same perfusion.
OBJECTIVE:
This study investigates the effects of hand cooling on human body functional recovery and exercise ability improvement by comparing normal rest and rest with hand cooling gloves after high-intensity exercise.
METHODS:
Thirty healthy subjects participated in this study wherein they exercised and used normal rest for one session and hand cooling rest for the next. Blood lactate concentration, heart rate recovery rate, VO
RESULTS:
When hands were cooled after exercise, blood lactate concentration and body temperature significantly decreased, and cardiopulmonary function, muscle strength, and muscular endurance significantly recovered.
CONCLUSION:
Using hand cooling gloves after exercise could attenuate core temperature elevation and improve postexercise recovery. It could also effectively improve athletic performance without using large-scale facilities.
1.Introduction
High-intensity exercise raises core body temperature, resulting in changes in the body’s metabolism and increased thermal stress and muscle fatigue [1, 2]. Elevated core body temperature causes fatigue because of increased blood flow, blood lactate concentration, and oxygen intake. Among numerous postworkout recovery approaches, cryotherapy has become widespread [3]. Cryotherapy is a method applied in sporting events to improve recovery from strenuous exercise by cooling part or all of the body, preventing high fever caused by exercise. Cryotherapy is being studied under various conditions (environment, temperature, exercise intensity) and methods (full-body immersion, half-body immersion, partial immersion). In the related study, the five cooling techniques, including using an air-cooled garment, a liquid-cooled garment, a phase change garment or clothing, hand immersion, and whole-body cooling were compared. Among these, it was found that whole-body cooling was the most effective treatment [4]. Similarly, other studies found that wind cooling was more effective than using ice packs [5], and reported that the core temperature could be reduced through the intake of 12
The cooling effect may vary as different body tissues do not process the same perfusion [8], such as in the arteriovenous anastomosis site, where there is a large area for blood flow. A larger blood flow area enables rapid blood circulation, while the connected reticular veins existing in the dermis layer rapidly transfer core body temperature into the skin [9, 10]. In peripheral areas such as the extremities and ears, there is an arteriovenous anastomosis site where small arteries and veins are directly connected. The hand region with arteriovenous anastomosis is able to satisfy the ease of use and effectiveness of reducing the temperature of the body.
Research has focused on cooling the hand while considering convenience during exercise or rest. The effects of hand cooling and hydration on lowering body temperature after exercise were investigated by comparing the following physiological states: hydrated with passive rest, hydrated with hand cooling on both hands, dehydrated with passive rest, and dehydrated with hand cooling on both hands. Their study showed that body temperature decreased more when both hands were cooled than in passive rest, regardless of hydration [11]. Another study reported that applying local subatmospheric pressure to the entire hand and attaching a heat sink to the palm extracted heat from the circulating blood resulted in exercise endurance [12]. Unfortunately, existing studies are still inconclusive on the effect of hand cooling alone. Thus, further investigation into the efficacy of hand cooling is needed to understand its potential for enhancing postexercise recovery fully.
This study investigates the effects of hand cooling on human body functional recovery and exercise ability improvement by comparing normal rest against rest with hand cooling gloves after high-intensity exercise. Blood lactate concentration with body heat was investigated to determine the efficacy of hand cooling gloves for postexercise recovery after exercise. The heart rate recovery was investigated to check the degree of recovery to resting heart rate related to exercise ability. The VO
2.Method
2.1Study design and participants
Thirty healthy individuals without any disease, 18 males and 12 females, participated in this study (Table 1). Those taking drugs, whether as medication, recreation, or otherwise, and the patients with underlying heart and respiratory diseases were excluded. The purpose and contents of this study were thoroughly explained to the participants, and written consent was obtained before the experiment proceeded.
Table 1
Participants’ physical characteristics
| Sex | Age (years) | Height (cm) | Weight (kg) | BMI (kh/m |
|---|---|---|---|---|
| Male | 31.94 | 179.50 | 78.94 | 24.55 |
| Female | 33.08 | 162.75 | 52.67 | 19.88 |
BMI
Forty-eight hours before the experiment, the participants were prohibited from vigorous exercise, alcohol intake, and caffeine intake. The whole experiment was done in two sessions, one where the participants underwent normal rest (NR) and another where they had cooling rest (CR), which was conducted a week later. For the purpose of this paper, these two sessions are described as the “NR group” and “CR group.” This study was conducted in accordance with the Declaration of Helsinki and was approved by the Kyungpook National University Institutional Review Board (2017-0086).
2.2Facilities and monitoring equipment
The experimental environment was maintained at a temperature of 20
Body heat was measured using an infrared body thermal camera (T-1000 SMART, MESH, South Korea), while blood lactate concentration was measured using a portable lactate analyzer (Accutrend plus, Cobas, Ltd., USA). For analyzing and evaluating the reduction rate of muscle fatigue, the degree of muscle fatigue was determined using the median frequency analysis of an electromyogram (Delsys Bagnoli-8 EMG System, Delsys Inc., USA) measured around the tibialis anterior and gastrocnemius [18]. The median frequency was defined as the spectral edge frequency of 50% (SEF 50) in the power spectrum space. Heart rate was measured using a wireless heart rate measurement system (Polar RS400, Polar, Finland), and the respiration rate was measured using a gas analyzer (Quark CPET, COSMED, Italy). For muscle strength measurement, the torque generated during extension and flexion of the knee joint was measured using isokinetic muscle function evaluation equipment (Biodex System 3, Biodex Medical Systems, Inc., New York, USA).
2.3Cooling gloves
Figure 1.
The customized cooling gloves consisted of a fingerless glove, a heat conduction pouch, a controller and battery pack, a Peltier module with a fan and heat sink, and a wrist pouch.

Customized cooling gloves (Fig. 1) were made and used for the experiment. It consisted of three main components: a glove, a Peltier module, and a controller and battery pack. A fingerless glove’s palm was lined with a heat conduction pouch maintained at 20
2.4Experiment protocol
2.4.1Evaluation of recovery for human body function
The participants performed a high-intensity walking exercise during both sessions at a 15% incline and a speed of 4 km/h on a treadmill for 30 minutes to induce muscle fatigue. The NR group rested without any form of cooling under the same environmental conditions. In contrast, the CR group rested for 20 minutes while wearing cooling gloves immediately after the exercise.
Body heat, changes in blood lactate concentration, reduction in muscle fatigue, and heart rate recovery (HRR) were evaluated to evaluate changes in muscle fatigue and physiological function stabilization with or without cooling. Measurements were performed thrice: before walking, immediately after, and after 20 minutes of rest. The heart rate was measured five times: before the experiment, 15 minutes after walking, 30 minutes after walking, 10 minutes rest, and 20 minutes rest. The maximum oxygen intake before and after the exercise with and without cooling was measured to analyze the respiration rate. Moreover, isokinetic exercise load evaluation was performed to evaluate the effect on muscle strength and muscular endurance.
2.4.2Evaluation of exercise performance and improvement
The participants exercised to exhaustion using the Bruce protocol to evaluate the improvement in cardiorespiratory performance with and without cooling. An initial exercise load was used at 10% inclination, 1.7 mph, for 3 minutes. It was then increased to about 2 to 3 estimated metabolic equivalents (METs) through steadily increasing the incline by 2% and the velocity by 0.8–0.9 mph every 3 minutes until the participant was exhausted [19].
In determining muscle strength, the torque generated during extension and flexion of the knee joint was measured. The measured joint angular velocities were 60
2.4.3Statistical analysis
The mean and standard deviation were calculated before and immediately after the walking exercise, then after resting using the Statistical Package for the Social Sciences (SPSS) v.13.0 (IBM, New York, USA) to verify the significance of the measured data. In addition, to verify the significance of fatigue relief and physiological function recovery effect according to the presence or absence of cooling, a
Figure 2.
Lactate concentration (mean
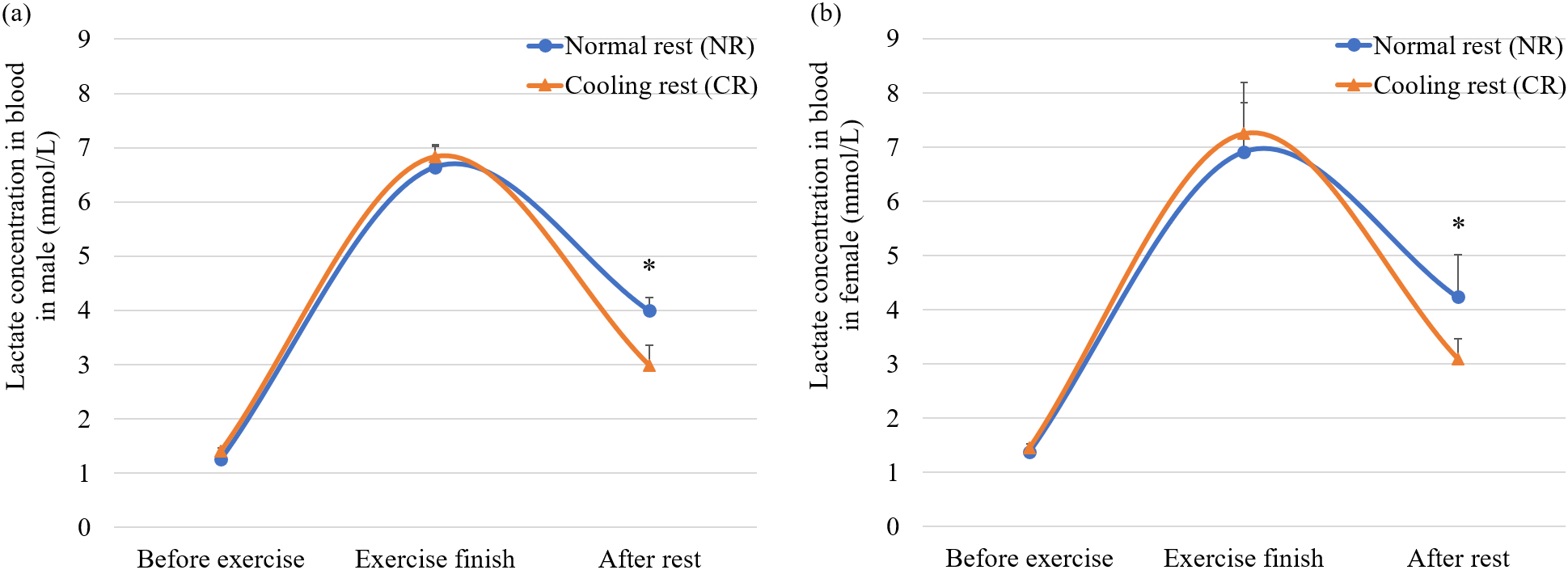
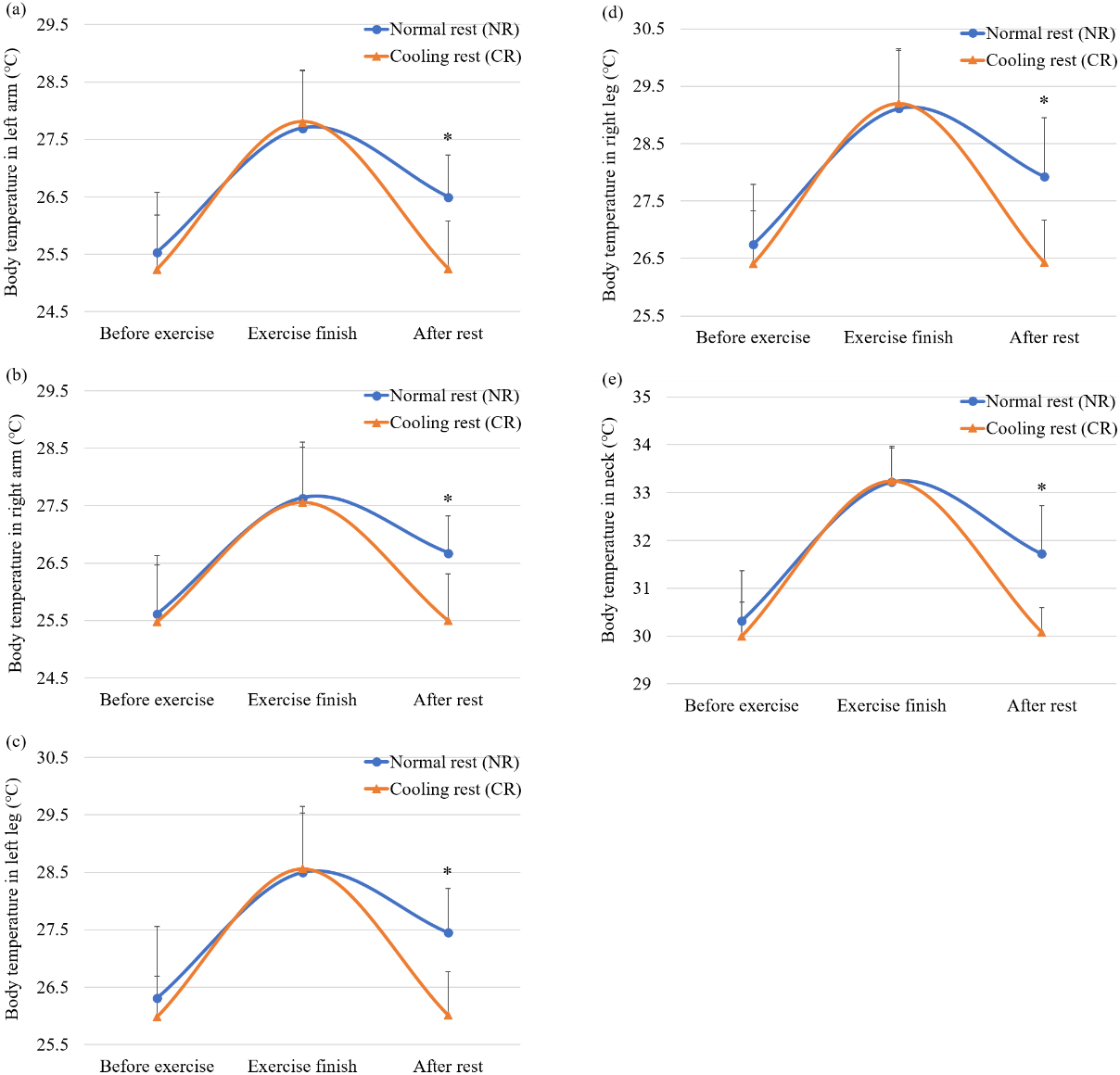
Figure 3.
Body temperatures (mean
3.Results
3.1Lactate concentration
Figure 2a shows the difference in lactate concentration of the male participants when CR and NR were used. Before the exercise, lactate concentration was 0.16
3.2Body temperature
In Fig. 3, a slight difference in body temperature between the CR and NR groups before exercise was observed, and then the body temperature of both groups increased after exercise 20 minutes after the end of the exercise, a significant difference in body temperature recovery rate between the CR and NR groups was observed. With CR, the recovery rate of body temperature for the left arm, right arm, left leg, right leg, and neck was 99.6%, 99%, 98.8%, 99.3%, and 97.2%, respectively. In comparison, with NR, the recovery rate of body temperature for each part was 55.6%, 47.3%, 47.9%, 50.2%, and 51.7%, respectively (
3.3Heart rate recovery (HRR)
Figure 4.
Heart rate recovery (mean
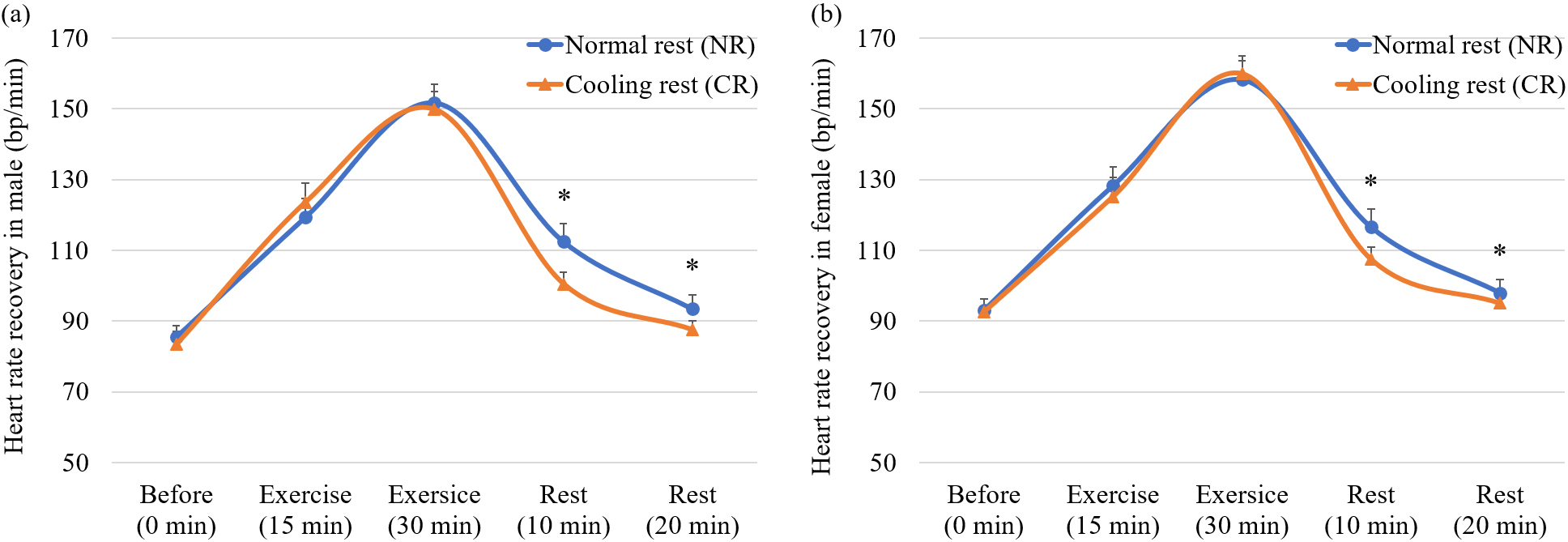
In Fig. 4, the minimal difference in heart rate between the CR and NR groups before the exercise was 2.25
After 20 minutes of rest, the participants’ average heart rate decreased to 87.5
3.4Muscle fatigue
Figure 5.
A comparison of muscle fatigue (mean
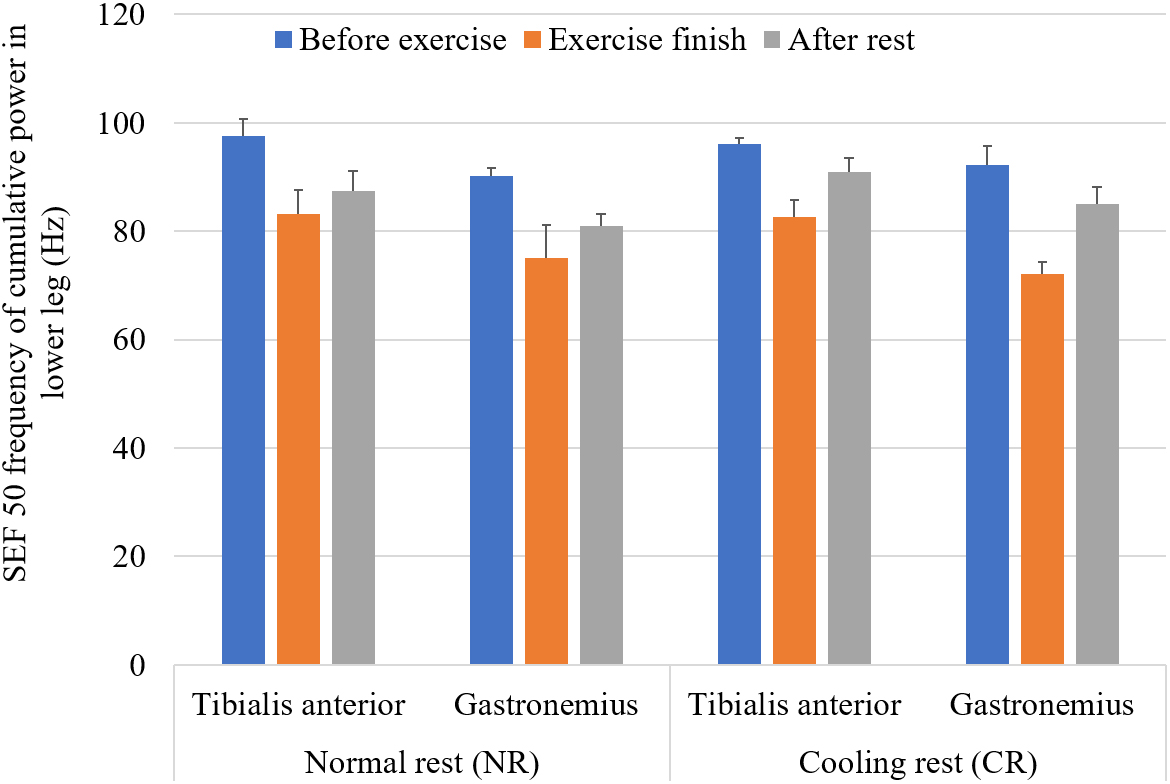
For muscle fatigue analysis, the change in the medium-frequency was observed by power spectrum analysis. The lower the medium-frequency value, the higher the fatigue state. For example, in Fig. 5, the tibialis anterior muscle fatigue test showed that 20 minutes after the exercise, the CR group’s medium-frequency increased from 82.6
3.5Maximal oxygen uptake (VO2
Figure 6.
Maximal oxygen (VO
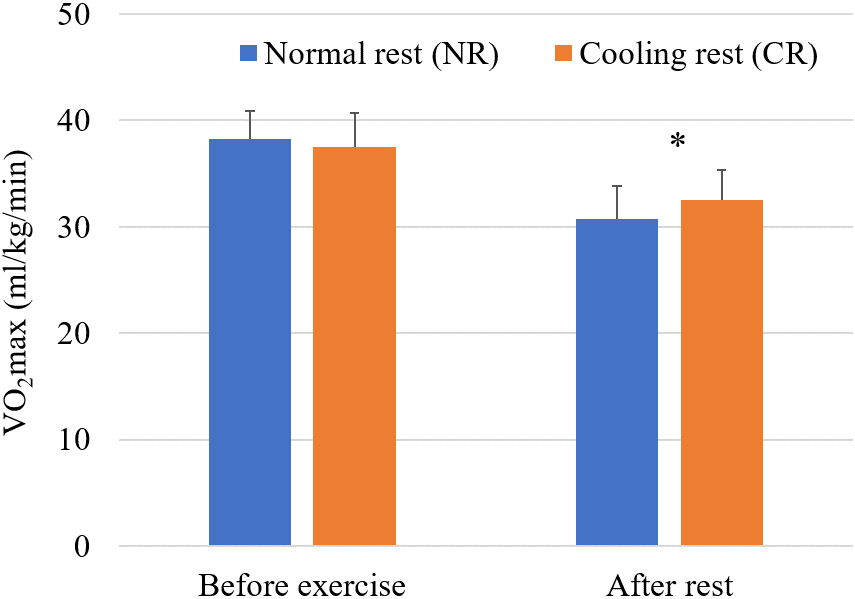
Figure 6 shows that 20 minutes after the exercise, the participants showed a VO
3.6Muscle strength
Figure 7.
Muscle strength (mean
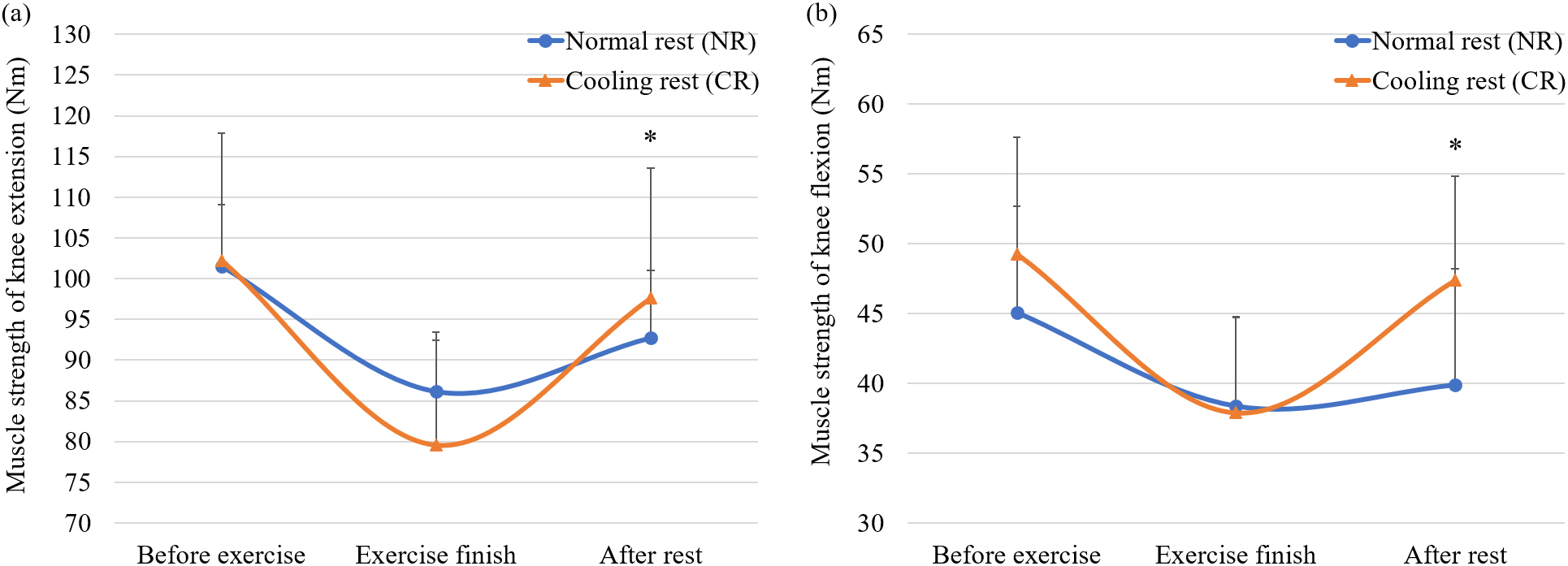
In Fig. 7, with CR, the participants showed increased muscle strength for knee extension, from 79.6
3.7Muscle endurance
Figure 8.
Muscle endurance (mean
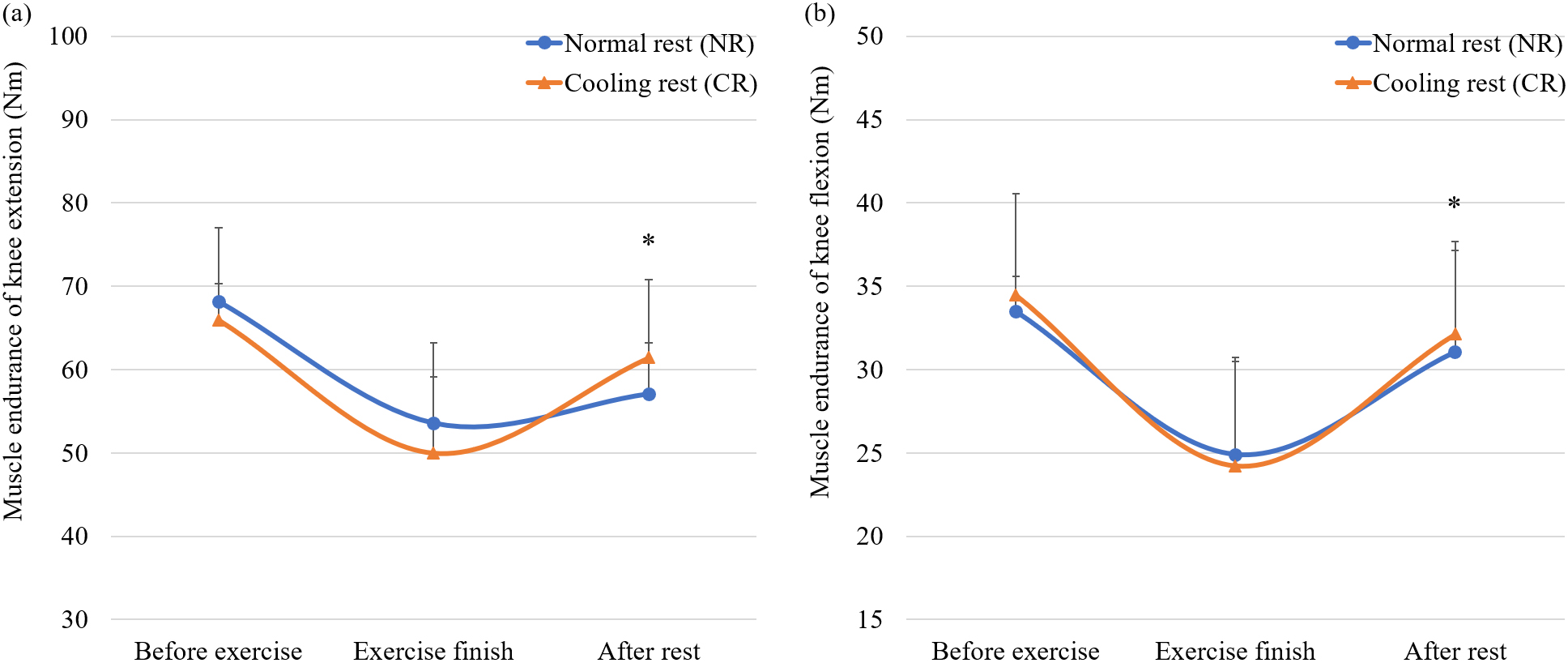
In Fig. 8, the participants with CR showed an increase in muscle endurance for knee extension from 49.99
4.Conclusion
An exercise-induced increase in core temperature can negatively affect exercise performance and lead to heat-related diseases. One notable finding of this study was that the intervention based on local cooling showed a significant difference compared with the control group. Using the palmar cooling technique after exercise could attenuate core temperature elevation and improve exercise performance.
Previous studies have demonstrated cryotherapy as an effective strategy for relieving fatigue symptoms after exercise [21, 22]. In the previous study, the mean body temperature and heart rate after 15 minutes of cold-water immersion (CWI) protocols were compared with passive rest. The mean body temperature and heart rate were significantly reduced when these protocols were followed [23]. In the cycling test, the effect of 15 minutes of CWI was examined, and the blood lactate level after CWI was significantly reduced compared to the passive rest group [24]. In addition, cryotherapy was found to be beneficial for recovery from stressful metabolic exercises by reducing cardiovascular tension [25]. However, there are space constraints and difficulties in maintaining the cooling performance of the cold water immersion method [26]. Similarly, since the blood vessels to the lower extremities are larger, applying this device to the lower extremities, which is another arteriovenous anastomosis in the body, can speed up recovery, but there is discomfort in wearing it.
Cryotherapy can be used as an alternative recovery technique that can be effective without the discomfort associated with CWI by cooling the area of local injury or exercise [27]. Among them, the hand is an arteriovenous anastomosis and can effectively and conveniently reduce the core body temperature [12]. However, the scientific evidence for the effectiveness of recovery after exercise is somewhat lacking.
This study investigates the effect of hand cooling on restoring human body function and improving body ability after exercise. Blood lactate concentration and body heat were measured, and cardiopulmonary function, muscle strength, and muscular endurance were measured to evaluate the improvement in exercise capacity and the recovery of human body function. When hands were cooled after exercise, blood lactate concentration and body temperature were significantly decreased, and cardiopulmonary function, muscle strength, and muscular endurance significantly recovered. Thus, after exercise, the hand cooling technique could attenuate core temperature elevation and improve postexercise recovery.
Conclusively, this study determined the effect of hand cooling gloves on body recovery by lowering body temperature after exercise and improving body function and exercise ability. These results suggest that hand cooling can effectively improve athletic performance without using large-scale facilities, such as cold water immersion. Therefore, hand cooling, which is practical and convenient, could be an alternative to cryotherapy in improving body recovery postexercise.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Kyungpook National University Institutional Review Board (2017-0086).
Conflict of interest
None to report.
References
[1] | Kim DY, Park DH, Kim KH. The comparison of fatigue by different exercise types under hot environment. Exerc Sci. (2008) ; 17: (2): 211-222. doi: 10.15857/ksep.2008.17.2.211. |
[2] | Baek CS, Kim KH, Kwon TD. The effect of the repetitive loaded exercise in a hot environment on body temperature, thermal sensation and ration of perceived exertion. Korean Society of Sports Sciences. (2016) ; 25: (2): 829-838. http://www.dbpia.co.kr/journal/articleDetail?nodeId=NODE06672168. |
[3] | Adams WM, McDermott BP, Schmit C, et al. Body cooling, in Sport and physical activity in the heat, D. J. Casa, Ed. Cham, Springer; (2018) . doi: 10.1007/978-3-319-70217-9_4. |
[4] | Brade C, Dawson B, Wallman K, et al. Postexercise cooling rates in 2 cooling jackets. J Athl Train. (2010) ; 45: (2): 164-169. doi: 10.4085/1062-6050-45.2.164. |
[5] | Leicht AS, Sinclair WH, Patterson MJ, et al. Influence of postexercise cooling techniques on heart rate variability in man. Exp Physio. (2009) ; 94: (6): 695-703. doi: 10.1113/expphysiol.2009.046714. |
[6] | Schniepp J, Campbell TS, Powell KL, et al. The effects of cold water immersion on power output and heart rate in elite cyclists. J Strength Cond Res. (2002) ; 16: (4): 561-566. |
[7] | De Pauw K, De Geus B, Roelands B, et al. Effect of five different recovery methods on repeated cycle performance. Med Sci Sports Exerc. (2011) ; 43: (5): 890-897. doi: 10.1249/MSS.0b013e318200d25f. |
[8] | Douzi W, Dugué B, Vinches L, et al. Cooling during exercise enhances performances, but the cooled body areas matter: A systematic review with meta-analyses. Scand J Med Sci Sports. (2019) ; 29: (11): 1660-1676. doi: 10.1111/sms.13521. |
[9] | Makam M. Glabrous skin regions as thermal portals for human temperature regulation. Stanford, Stanford University, Unpublished data Ph.D. dissertation; (2017) . |
[10] | Walløe L. Arterio-venous anastomoses in the human skin and their role in temperature control. Temperature. (2016) ; 3: (1): 92-103. doi: 10.1080/23328940.2015.1088502. |
[11] | Adams WM, Hosokawa Y, Adams EL, et al. Reduction in body temperature using hand cooling versus passive rest after exercise in the heat. J Sci Med Sport. (2016) ; 19: (11): 936-940. doi: 10.1016/j.jsams.2016.02.006. |
[12] | Grahn DA, Cao VH, Heller HC. Heat extraction through the palm of one hand improves aerobic exercise endurance in a hot environment. J Appl Physiol. (2005) ; 99: (3): 972-978. doi: 10.1152/japplphysiol.00093.2005. |
[13] | Sharma L, Hussain ME, Verma S. Effect of recovery modalities on blood lactate clearance. Saudi J Sports Med. (2017) ; 17: (2): 65. doi: 10.4103/1319-6308.207577. |
[14] | Han SY, Kim H, Lee SH. Effects of basic Taekwondo movement training on body composition, cardiorespiratory of middle-aged women. Korean J Sports Sci. (2007) ; 16: (4): 667-681. |
[15] | Poole DC, Behnke BJ, Musch TI. The role of vascular function on exercise capacity in health and disease. J Physiol. (2021) ; 599: (3): 889-910. doi: 10.1113/JP278931. |
[16] | Wilcock IM, Cronin JB, Hing WA. Physiological response to water immersion: A method for sport recovery? Sports Med. (2006) ; 36: : 747-765. doi: 10.2165/00007256-200636090-00003. |
[17] | Kwon YS, Robergs RA, Kravitz LR, et al. Palm cooling delays fatigue during high-intensity bench press exercise. Med Sci Sport Exer. (2010) ; 42: (8): 1557-1565. doi: 10.1249/MSS.0b013e3181d34a53. |
[18] | Kang SR, Min JY, Yu C, et al. Effect of whole body vibration on lactate level recovery and heart rate recovery in rest after intense exercise. Technol Health Care. (2017) ; 25: (S1): 115-123. doi: 10.3233/THC-171313. |
[19] | Koutlianos N, Dimitros E, Metaxas T, et al. Indirect estimation of VO2max in athletes by ACSM’s equation: Valid or not? Hippokratia. (2013) ; 17: (2): 136. |
[20] | Small K, McNaughton L, Greig M, et al. The effects of multidirectional soccer-specific fatigue on markers of hamstring injury risk. J Sci Med Sport. (2010) ; 13: (1): 120-125. doi: 10.1016/j.jsams.2008.08.005. |
[21] | Ihsan M, Watson G, Lipski M, et al. Influence of postexercise cooling on muscle oxygenation and blood volume changes. Med Sci Sports Exerc. (2013) ; 45: (5): 876-882. doi: 10.1249/MSS.0b013e31827e13a2. |
[22] | Leeder J, Gissane C, van Someren K, et al. Cold water immersion and recovery from strenuous exercise: A meta-analysis. Br J Sports Med. (2012) ; 46: (4): 233-240. doi: 10.1136/bjsports-2011-090061. |
[23] | Vaile J, Halson S, Gill N, et al. Effect of cold water immersion on repeat cycling performance and thermoregulation in the heat. J Sports Sci. (2008) ; 26: (5): 431-440. doi: 10.1080/02640410701567425. |
[24] | Crowe MJ, O’Connor D, Rudd D. Cold water recovery reduces anaerobic performance. Int J Sports Med. (2007) ; 28: (12): 994-998. doi: 10.1055/s-2007-965118. |
[25] | Ihsan M, Watson G, Abbiss CR. What are the physiological mechanisms for post-exercise cold water immersion in the recovery from prolonged endurance and intermittent exercise? Sports Med. (2016) ; 46: (8): 1095-1109. doi: 10.1007/s40279-016-0483-3. |
[26] | Castle PC, Macdonald AL, Philp A, et al. Precooling leg muscle improves intermittent sprint exercise performance in hot, humid conditions. J Appl Physiol. (2016) ; 100: (4): 1377-1384. doi: 10.1152/japplphysiol.00822.2005. |
[27] | Yeargin WS, Casa DJ, McClung JM, et al. Body cooling between two bouts of exercise in the heat enhances subsequent performance. J Strength Cond Res. (2006) ; 20: (2): 383-389. doi: 10.1519/R-18075.1. |


